Embed Size (px)
Citation preview

Primary Cryptococcal Prostatitis in anApparently Uncompromised Host
Romeo L. Caballes1* and Romeo A. Caballes Jr.2
1Department of Pathology and Laboratory Medicine, UMDNJ-New Jersey Medical School,Newark, New Jersey
2Department of Internal Medicine, St. Michael’s Medical Center, Newark, New Jersey
BACKGROUND. Systemic spread from a primary focus of cryptococcal infection commonlyinvolves the central nervous system, manifested as meningitis or meningoencephalitis. Un-treated meningitis and meningoencephalitis are invariably fatal, following a subacute orchronic course of cyclic remission and relapse, followed by progressive deterioration overweeks to months. Occasional patients with fulminating meningoencephalitis die within a fewdays. Incorrect diagnosis may be the most common cause of fatality in this disease. Thoroughhistopathologic examination and blood and body fluid studies should minimize misdiagno-sis.METHODS. We studied the case of an initially misdiagnosed 64-year-old apparently immu-nologically competent man with primary cryptococcal prostatitis that subsequently dissemi-nated to the central nervous system and the left eye. All immunologic findings includingworkup for AIDS viruses were normal. Laboratory studies confirmed cryptococcal infection.RESULTS. After initial misdiagnosis, our patient received improper treatment for 10 months.He developed meningitis and severe left endophthalmitis with optic nerve and retinal in-volvement. Toxic medications led to kidney insufficiency with about 66% loss of function.Following therapy, reevaluation of his immune system showed marked abnormality in cell-mediated immunity.CONCLUSIONS. Cryptococcosis is easily misdiagnosed in uncompromised hosts, both clini-cally and pathologically, because of misconception that the disease affects only immunocom-promised individuals and that primary cryptococcal prostatitis is virtually unheard-of in“normal” males. Prostate 39:119–122, 1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: primary cryptococcal prostatitis; uncompromised; cryptococci; immuno-compromised; central nervous system
INTRODUCTION
Defects in cell-mediated immunity enhance predis-position to cryptococcal infection [1]. Hosts are pre-dominantly human immunodeficiency virus (HIV)-positive individuals clinically suffering from acquiredimmunodeficiency syndrome (AIDS) [2–4].
C. neoformans, a ubiquitous yeast, disseminates andinfects susceptible organs and structures through he-matogenous routes, usually by way of the lower re-spiratory tract. Once in the tissues, the organisms de-velop a thick, clear mucinous (glycosaminoglycans) cap-sule, unique among pathogenic fungi, and requisite toits pathogenicity [5].
Cryptococci are ovoid to spherical single-budding,
thick-walled yeasts, 4–9 micra in diameter, and theyform capsules that may disappear on initial isolationand reappear as the mucoid forms develop. These cap-sules are often more than twice the thickness of theindividual cells [6]. Organisms do not form hyphaebut occasionally develop short abortive germinal tu-bules that disappear on subculture. In tissues and exu-dates, these structures are not observed [7].
The main source of human infection is pigeon ex-creta, chemically alkaline and hyperosmolar, main-
*Correspondence to: Romeo L. Caballes, M.D., 2 Keystone Drive,Livingston, NJ 07039-9207.Received 22 May 1997; Accepted 19 August 1998
The Prostate 39:119–122 (1999)
© 1999 Wiley-Liss, Inc.

taining cryptococci small enough to be inhaled and topenetrate terminal bronchioles [5]. In lower respirato-ry tract involvement, bronchitis and bronchopneumo-nia are the usual clinical presentations. Uncompro-mised hosts may develop silent lung lesions consistingof circumscribed nodules with necrotic centers con-taining many cryptococci, and a fibrotic and granulo-matous wall, known as pulmonary cryptococcoma [5].These lesions rarely calcify and roentgenograms donot suggest a healed infectious process [5].
Systemic spread from a primary focus commonlyinvolves the central nervous system (CNS), clinicallymanifested as meningitis or meningoencephalitis. In-volvement of the brain may extend to the ventricularsystem and any levels of the spinal cord. Brain lesionsare characteristically cystic and may mimic tumors.The tendency of C. neoformans to invade the CNS isbased on its nutritional needs, met by the constituentsof cerebrospinal fluid [7]. Disseminated cryptococcosisalso affects the skin, mucous membrane, eyes, bone,lymph nodes, and visceral organs, such as liver, kid-neys, spleen, and adrenals. India ink preparationsdemonstrate budding, encapsulated yeasts, and latexagglutination tests detect the glycosaminoglycans cap-sule in serum and spinal fluid. In tissue specimens,cryptococci are better identified by special stainingtechniques, such as Mayers mucicarmine, Gomori me-
thenamine silver, and periodic acid-Schiff stains. Or-ganisms may be cultured from these lesions. It hasbeen estimated that the disease is much more preva-lent than is commonly assumed, with approximately2,000 undiagnosed cases for every proven infectiondue to C. neoformans [6].
Untreated cryptococcal meningitis and meningoen-cephalitis are invariably fatal and usually follow asubacute or chronic course marked by cyclic remissionand relapse followed by progressive deteriorationover weeks to months. However, occasional cases offulminating meningoencephalitis die within a fewdays.
CASE REPORT
A robust, healthy-appearing 64-year-old machinistwith a history of well-controlled diabetes mellitus wasfirst admitted to hospital on January 5, 1988, becauseof difficulty and frequency of urination. He mentionedfrontal headaches and some discomfort and blurringof vision in his left eye, since a month prior to admis-sion. Transurethral prostatectomy was done on Janu-ary 6, 1988. Pathologic diagnosis was “severe xantho-granulomatous prostatitis with areas of acute inflam-mation and microabscess formation.” Postoperatively,
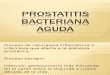
Fig. 1. A: Low-power view of an area of acute granuloma witha microabscess and a dilated and necrotic gland filled with neu-trophils and some cryptococci (hematoxylin-eosin stain, ×175). B:High-power magnification of microabscess containing many cryp-tococci (periodic acid-Schiff stain, ×700). C: Medium-power viewof some cryptococci in lumina of necrotic glands (Gamori methe-namine silver stain, ×440).
120 Caballes and Caballes

frontal headaches became more severe and persistent,accompanied by pain and tenderness, blurred vision,and black scotomata in the left eye. A diagnosis oftoxoplasmosis was made by his ophthalmologist afterhis blood tested positive for T. gondii antibody. He wastreated with daraprim and sulfadiazine for more than2 months with no apparent relief. A pathology con-sultant reviewed the slides and made a diagnosis ofcryptococcal prostatitis. Histopathologically, both he-matoxylin-eosin and special stains (Gomori methena-mine silver, periodic acid-Schiff, and Mayers mucicar-mine) showed an acute granulomatous inflammatoryprocess containing many scattered cryptococci, withmicroabscesses and dilated and necrotic glands filledwith neutrophils and cryptococci (Fig. 1A–C), some ofwhich were budding organisms (Fig. 2). Fibroticchanges were present in granulomatous areas. OnJune 29, 1988, he was readmitted to another hospitalwhere blood and spinal fluid studies confirmed cryp-tococcal infection. His immune system was investi-gated, with some emphasis on ruling out AIDS. Allimmunologic findings were normal. Chest roentgeno-grams were negative. Other laboratory studies on ad-mission showed normal values, except for an elevatedblood glucose of 160 mg/dl. He was already quite ill:toxic, feverish, apprehensive, and, at times, hallucinat-ing when amphotericin B and flucytosine werestarted. A few weeks later, response to amphotericin Bwas determined unsatisfactory. The dose was in-creased from 30 mg to 50 mg/day. Flucytosine wasdiscontinued because of progressive anemia. His con-dition was gradually deteriorating, accompanied byprogressive anemia, renal insufficiency, and persis-tently elevated blood glucose despite insulin therapy.Pertinent laboratory findings were Hgb 7.4 gm/dl,RBC 2.50 × 105, Hct 22.0%, WBC 2.9 × 103, neutrophils96%, lymphocytes 3%, creatinine 2.8 mg/dl, BUN 53
mg/dl, and glucose 357 mg/dl. He was moribund un-til he received 2 units of packed red blood cells, whichimproved his condition remarkably. Pain and tender-ness in the left eye continued to intensify. On July 27,1988, he underwent vitrectomy. The day after surgery,he returned for completion of amphotericin B treat-ment. He never regained vision in the left eye. Duringconvalescence, renal function test demonstrated about66% deficit. Following therapy, reevaluation of his im-mune system revealed marked abnormality in cell-mediated immunity.
DISCUSSION
C. neoformans is an opportunistic organism preyingon individuals with abnormal cell-mediated immunitycaused by a variety of debilitating conditions, such asacquired immunodeficiency syndrome, certain lym-phomas (including Hodgkin’s disease), chronic lym-phocytic leukemia, sarcoidosis, poorly controlled dia-betes mellitus, corticosteroid-secreting lesions of adre-nals, and immunosuppressive drug therapy.
When immunocompromised men with a primarypulmonary focus of cryptococcal infection developeddisseminated disease, the prostate was involved in 6of 23 cases reported by Salyer and Salyer in 1973 [8].On the other hand, an uncompromised man harboringa primary focus of cryptococcal prostatitis is likely tobe misdiagnosed, both clinically and pathologically,because of the misconception that the disease affectsonly immunocompromised individuals, or that pri-mary cryptococcal prostatitis is virtually unheard of in“normal” men.
Our patient had been worked up for HIV-1 andHIV-2 infection during month 11 (July 17, 1988) of hisillness and was found to be negative for both viruses.Similarly, T-cell studies showed normal immunologi-cal findings with a CD4/CD8 (helper/suppressor) ra-tio of 1.28.
In the English-language literature, we found noprevious report of primary cryptococcal prostatitis inuncompormised hosts. The 2 patients with primarycryptococcal prostatitis reported by Hinchey andSomeren [9] and O’Connor et al. [10] were most likelyimmunocompromised hosts. Although the status oftheir immune systems was not clearly defined, it isnevertheless probably safe to assume that both ofthem were immunosuppressed, based on concurrentpredisposing and debilitating conditions: one patienthad pulmonary tuberculosis and diabetes mellitus,and the other had long-standing chronic lymphocyticleukemia.
The presenting complaints of difficult and frequenturination caused by urinary obstruction, secondary toprostatic enlargement, preceded evidence of dissemi-
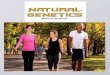
Fig. 2. High-power view of many cryptococci and some buddingorganisms in a microabscess (Mayers mucicarmine stain, ×700).
Primary Cryptococcal Prostatitis in Normal Host 121

nation, e.g., headaches, discomfort, and blurring of vi-sion in the left eye in our present case, by at least 3months. He developed no pulmonary symptoms be-fore or during this illness, and chest roentgenogramsremained clear. By the time amphotericin B and flu-cytosine were started, he was already quite toxic and,at times, hallucinating. The clinical course was char-acterized by gradual deterioration, accompanied byprogressive anemia, renal insufficiency, and persis-tently elevated blood glucose despite insulin therapy.Although his general health appeared remarkably im-proved after blood transfusion, the pain and tender-ness in his left eye continued to intensify due to severeendophthalmitis with optic nerve and retinal involve-ment, ending in complete loss of vision. During con-valescence, the toxic effect of medication used in com-bating the infection had worsened. The kidneys lostabout 66% function. Also following therapy, a repeatimmunologic workup, including T-cell subsets, quan-titative immunoglobulin, and mitogen and antigenproliferation studies showed a significant decline intotal T cells (absolute T-cell count of 290), most notice-able in the CD4/CD8 (helper/suppressor) ratio of 0.13.Normally this ratio is usually between 1.0–3.0, indi-cating an overall T-cell imbalance in favor of immu-nosuppression. Consistent with this interpretationwere the significantly reduced T-cell mitogen re-sponses (Con-A, PHA), while B-cell responses wereonly slightly diminished and immunoglobulin levelswere normal.
REFERENCES
1. Levitz SM. The ecology of Cryptococcus neoformans and the epi-demiology of cryptococcosis. Rev Infect Dis 1991;13:1163–1169.
2. Chuck SL, Sande MA. Infections with Cryptococcus neoformans inthe acquired immunodeficiency syndrome. N Engl J Med 1989;321:794–799.
3. Saag MS, Powderly WG, Cloud GA, Robinson P, Grieco MH,Sharkey PK, Thompson SE, Sugar AM, Tuazon CU, Fisher JF,Hyslop N, Jacobson JM, Hafner R, Dismukes WE, NIAID My-coses Study Group, AIDS Clinical Trials Group. Comparison ofamphotericin B with fluconazole in the treatment of acute AIDS-associated cryptococcal meningitis. N Engl J Med 1992;326:83–89.
4. Powderly WG, Saag MS, Cloud GA, Robinsin, P, Meyer RD,Jacosbson, JM, Graybill JR, Suger AM, McAuliffe VJ, FollansbeeSE, Tuazon CU, Stern JJ, Feinberg J, Hafner R, Dismukes WE,NIAID AIDS Clinical Trials Group, NIAID Mycoses StudyGroup. A controlled trial fluconazole or amphotericin B to pre-vent relapse of cryptococcal meningitis in patients with ac-quired immunodeficiency syndrome. N Engl J Med 1992;326:793–798.
5. Rubin E, Farber JL. Pathology. Philadelphia: Lippincott; 1988. p426.
6. Bailey WR, Scott EG. Diagnostic microbiology, 4th ed. St. Louis:Mosby; 1974. p 257.
7. Moss ES, McQuown AL. Atlas of medical mycology, 2nd ed.Baltimore: Williams and Wilkins; 1960. p 56.
8. Salyer WR, Salyer DC. Involvement of kidney and prostate incryptococcosis. J Urol 1973;109:695–698.
9. Hinchey WW, Someren A. Cryptococcal prostatitis. Am J ClinPathol 1981;75:257–260.
10. O’Connor FJ, Foushee JHS Jr, Cox CE. Prostatic cryptococcosis.J Urol 1965;94:160–163.
122 Caballes and Caballes