Embed Size (px)
Citation preview

1354
Primary intra osseous carcinomaChandra Shekar1, Aruna2, Pavankumar B3, Yashwanth4
ABSTRACT:
Primary intra osseous carcinoma (PIOC) is a rare malignant
neoplasm of the jaws which is locally aggressive with quite poor
prognosis. Disease free survival is poor with almost 50% patients
failing within first two years of follow up and reason can be
attributed to the delayed diagnosis. The knowledge of clinical,
radiographic and histopathologic features of PIOC allows
accurate and early diagnosis of the lesion so that an early and
appropriate treatment can be instituted for better prognosis.
Hereby we discuss a typical case of PIOC of the mandible and
an attempt is made to discuss all possible differential and an
update on overview of literature is presented.
Key words: Primary intraosseous carcinoma; jaws; Odontogenictumors; squamous cell carcinoma.
C A S E R E P O R T
doi: 5866/2013.531354
1Reader2Senior Lecturer3Professor4Post Graduate StudentDepartment of Oral SurgeryKamineni Institute of Dental SciencesNarketpally, Nalgonda Dist. A.P. India
Article Info:
Received: April 8, 2013Review Completed: May 10, 2013Accepted: June 10, 2013Available Online: October, 2013 (www.nacd.in)© NAD, 2013 - All rights reserved
Email for correspondence:[email protected]
Quick Response Code
Introduction
Primary intraosseous carcinoma (PIOC) is a very rare but well known lesion affecting the jaw bones. Itwas first described by Loos in 1913 as central epidermoid carcinoma of the jaws. Willis in 1948 renamed it asan intra-alveolar epidermoid carcinoma. The term PIOC was coined by Pindborg in 1971.1-2
According to World Health Organisation (WHO) PIOC is defined as “A Squamous cell carcinoma arisingwithin the jaw, having no initial connection with the oral mucosa and presumably developing from residuesof the odontogenic epithelium”.2
The tumor is locally aggressive and metastasis to lymph nodes. Prognosis further worsens with delayeddiagnosis and treatment. A case report with all the typical features is being presented here.
INDIAN JOURNAL OF DENTAL ADVANCEMENTSJour nal homepage: www. nacd. in
Indian J Dent Adv 2013; 5(3) Suppl 1: 1354-1358

1355
Case report
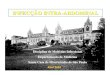
A 70 yr old female patient reported to thedepartment of oral and maxillofacial surgery witha chief complaint of slight painful swelling on theright side of the jaw since three months. The swellinggradually increased to the present size. The patienthad no contributory medical history. However, shehad a habit of smoking chutta since 4 decades. Therewas a gross facial asymmetry with diffuse multiplenodular swelling which was extending from rightside of the mandibular angle region crossing themidline extended to the right side of the corner ofthe mouth.
On palpation two swellings were appearedextraorally. One swelling was extended from theangle of the mandible to the inferior border and wasfixed. The other swelling was grossly oval in shapewith multiple nodules of 4x 5 cm in diameter. Boththe swellings were tender, hard and non-fluctuant.Because of nodular swelling in the midline the lowerlip was inverted (fig 1).
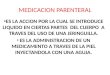
Bilateral submental, submandibular and rightupper jugular nodes were palpable and fixed. Mouthopening was difficult. Intra orally vestibularobliteration was seen extending from left canine toright anterior border of ramus of mandible. The jawwas partially edentulous with hollowing. Themucosa was erythematous and bleeding occurred onpalpation. There was no obvious relation betweenoverlying mucosa and the diseased mass. Onpalpation the inspectory findings were confirmed.The first and second right mandibular molar weremobile and tender(fig 2). A panaromic imagerevealed gross destruction of the left parasymphysis,symphysis, right parasymphysis and right body withfew radiopaque flecks of bone within the body of thelesion. Right first molar shows floating toothappearance (fig 3).
The CT Scan was performed revealing thedestructive lesion in the right half of the mandible
there is complete destruction of the mandible withcortical plates extending from left mandibularcanine region to the right mandibular first molarregion. The whole mandible from the left canine tothe right angle region was destructive in appearance(fig 4).
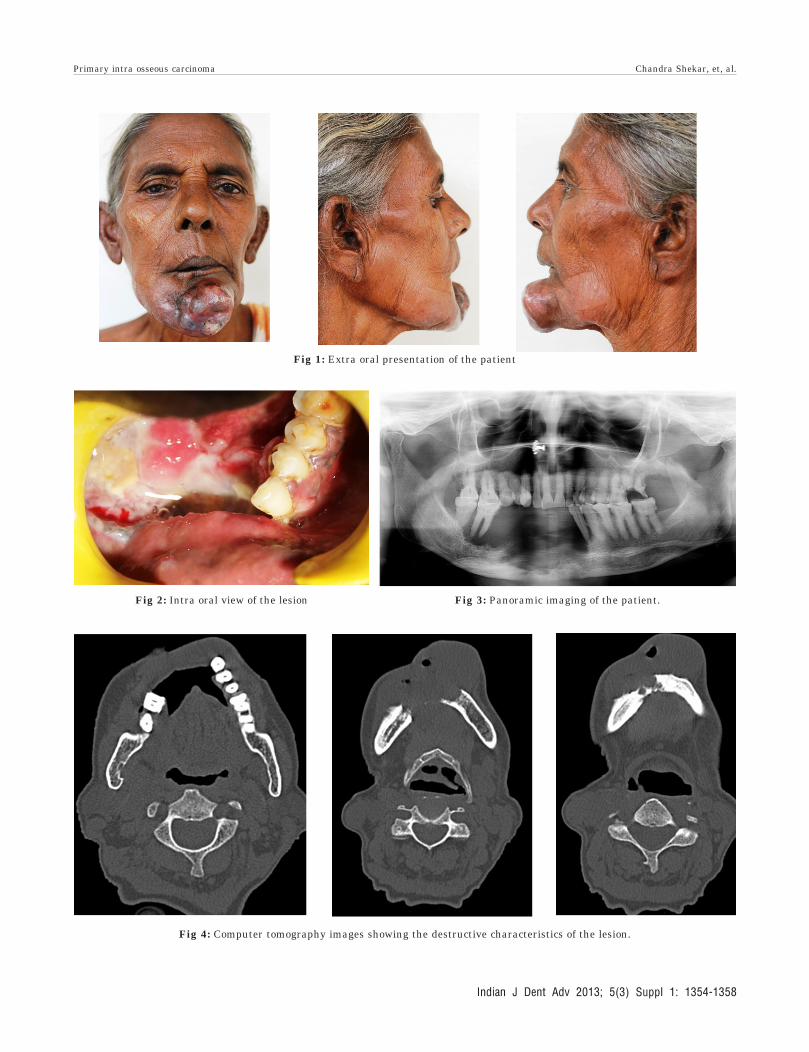
On MRI studies there was evidence of anirregular ill-defined heterogeneously hyper-intenselesion located across the lower jaw occupying thespace between lower right buccal/lingual mucosaanteriorly and the mandible posteriorly with itsepicentre across the labial frenal region. The lesionalmost reaches anteriorly up to the skin withcomplete loss of subcutaneous fat planes. Posteriorlyit is seen to erode the anterior mandibular body, upto the alveolar process of 2ndmolar tooth, causingdeficiency to the bone on the right side and on theleft side it penetrates through its alveolar processnear the 2nd pre molar tooth and covering theanterior and posterior aspects of its alveolar processnear the first molar tooth. The adjacent body andthe base of the ramus on the right side demonstratehyperintense marrow signals. Findings of the boneerosions were being correlated with complementaryCT sections. Inferiorly the lesion is seen to involvethe base of the mandible almost reaching up to theskin with the loss of subcutaneous fat planes. Therewas evidence of few bilateral submandibular lymphnodes, the largest one across the left side (2.4 x 1.2cm), and another adjacent node measuring 1.2 x 0.6cm. the largest node on the right side measuring1.4 x 0.5 and right supraclavicular lymph node 1.8x 1 cm were appreciated. Few smaller cervical lymphnodes across level I level II and level III, largest onthe right side measuring up to 0.7 x 0.4 cm and onthe left side measuring up to 0.6 x 0.4 cm werenoted(fig 5). An impression of squamous cellcarcinoma were featured.
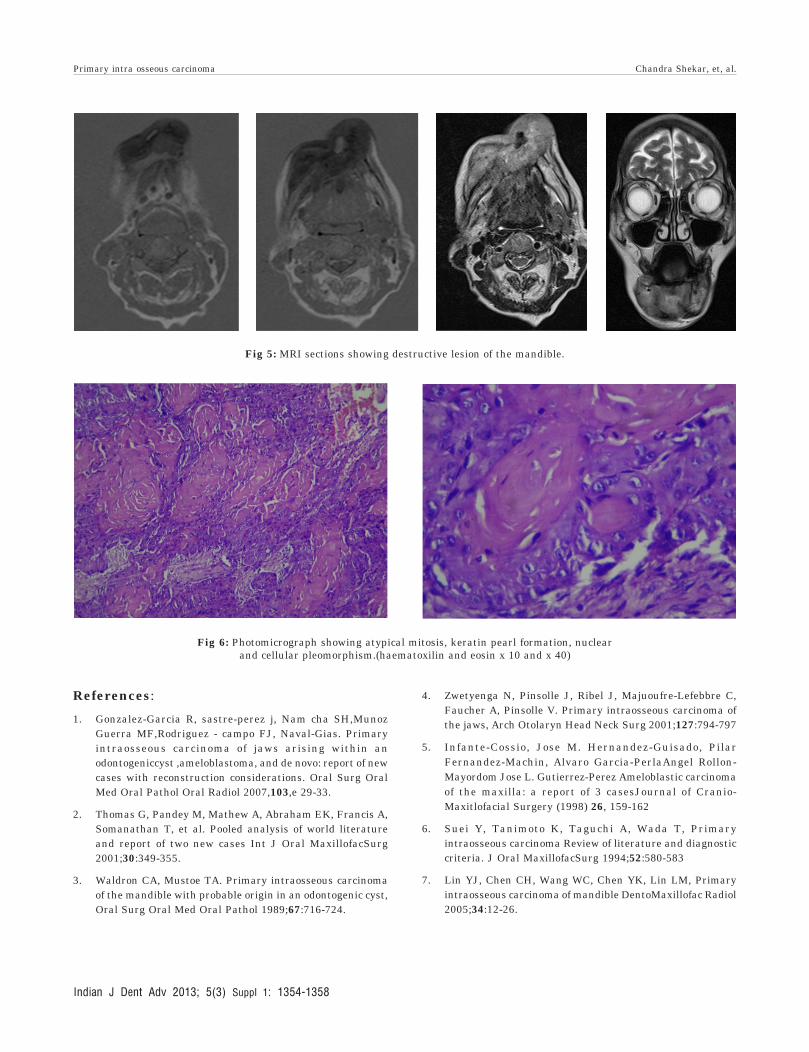
Incisional biopsy was done and histologicalfindings showed dense cellular connective tissuestroma showing malignant epithelial cells in the
Primary intra osseous carcinoma Chandra Shekar, et, al.
Indian J Dent Adv 2013; 5(3) Suppl 1: 1354-1358

1356
arrangement of sheets and strands. Individual cellsscattered across the stroma was also seen.Malignant epithelial cells show severe dysplasticchanges such as atypical mitosis, keratin pearlformation and increased mitotic activity along withnuclear and cellular pleomorphism. There is alsopresence of chronic inflammatory cell infiltrationand moderate cell vascularity and finally featuressuggestive of primary intra-osseous carcinoma denovo- keratinizing type was reported (fig 6).
Discussion
Primary intra-osseous carcinoma is difficult todetermine owing to insufficient data to conclusivelysupport the diagnosis. Approximately more thn 150cases of PIOC have been documented till now1. PIOCaffects patients ranging from 4-90 years of age witha mean age of 57 years. It is more frequently seenin the mandible with a striking predilection for theposterior regions. In maxilla the lesions are mostlyseen in the anterior region and crossing themidline.1-4 Since the initial WHO classificationsystemfor Odontogenic Tumors (Pindborget al.,1972), variousrevisions of this classification havebeen published (Elzay, 1982), that of SlootwegandMiiller(1984)being the most widely accepted.
The latter classification by Kramer in 2005differentiates the following categories of odontogeniccarcinomas: Type 1. Primary intraosseous carcinomaex :odontogeniccyst.Type 2. (A)Malignantameloblastoma. (B) Ameloblastic carcinoma, arisingdenovo, ex:ameloblastoma or ex:odontogenic cyst.Type 3. Primary intraosseous carcinoma arisingdenovo. (A) Non-keratinizing. (B) Keratinizing. In thenew WHO classification (Kramer et al.,1992) it isincluded, as follows, among theodontogeniccarcinomas: A) Malignantameloblastoma. B) Primary intraosseous carcinoma.C) Malignant variants of other odontogenicepithelialtumours.
D) Malignant changes in odontogenic cysts.5
To define the lesions in the jaws as PIOC three
specific criteria may be present4-7
1. Histological evidence of squamous cell
carcinoma.
2. Absence of ulcer formation on the overlying
mucosa.
3. Absence of a distant primary tumor at the
time of diagnosis and at least 6 months
during the follow up period.
Etiology of PIOC is not clear probably it arises
from the remnants of odontogenic tissue, either the
epithelial rests of malassez or the remnants of dental
lamina. These epithelial remnants proliferate and
transform into odontogenic carcinoma, a process that
is potentially triggered by an inflammatory process.
It does not have its origin from the epithelial linig
of a pre-existing odontogenic cyst or the epithelial
component of an odontogenic tumor.2-3
Surgery is the treatment of choice and in most
cases consisted of en-bloc resection or radical
resection of the involved bone. Distraction
osteogenesis of mandibular segmental defect maybe
a valid alternative in those patients who are not
candidates for more aggressive surgical procedures.
Radiotherapy and chemotherapy should be
considered only in lesions that cannot be surgically
controlled.2-4 However the effectiveness of these
modalities is unclear because of less number of cases
and documented follow up. Our case highlights that
radiographic examination is one of the most effective
methods for detecting early lesions of PIOC s. hence
accurate knowledge of this rare entity is must toprevent delayed diagnosis.
Primary intra osseous carcinoma Chandra Shekar, et, al.
Indian J Dent Adv 2013; 5(3) Suppl 1: 1354-1358
1357
Fig 1: Extra oral presentation of the patient
Fig 2: Intra oral view of the lesion Fig 3: Panoramic imaging of the patient.
Fig 4: Computer tomography images showing the destructive characteristics of the lesion.
Primary intra osseous carcinoma Chandra Shekar, et, al.
Indian J Dent Adv 2013; 5(3) Suppl 1: 1354-1358
1358
Fig 5: MRI sections showing destructive lesion of the mandible.
Fig 6: Photomicrograph showing atypical mitosis, keratin pearl formation, nuclearand cellular pleomorphism.(haematoxilin and eosin x 10 and x 40)
References:
1. Gonzalez-Garcia R, sastre-perez j, Nam cha SH,MunozGuerra MF,Rodriguez - campo FJ, Naval-Gias. Primaryintraosseous carcinoma of jaws arising within anodontogeniccyst ,ameloblastoma, and de novo: report of newcases with reconstruction considerations. Oral Surg OralMed Oral Pathol Oral Radiol 2007,103,e 29-33.
2. Thomas G, Pandey M, Mathew A, Abraham EK, Francis A,Somanathan T, et al. Pooled analysis of world literatureand report of two new cases Int J Oral MaxillofacSurg2001;30:349-355.
3. Waldron CA, Mustoe TA. Primary intraosseous carcinomaof the mandible with probable origin in an odontogenic cyst,Oral Surg Oral Med Oral Pathol 1989;67:716-724.
4. Zwetyenga N, Pinsolle J, Ribel J, Majuoufre-Lefebbre C,Faucher A, Pinsolle V. Primary intraosseous carcinoma ofthe jaws, Arch Otolaryn Head Neck Surg 2001;127:794-797
5. Infante-Cossio, Jose M. Hernandez-Guisado, PilarFernandez-Machin, Alvaro Garcia-PerlaAngel Rollon-Mayordom Jose L. Gutierrez-Perez Ameloblastic carcinomaof the maxilla: a report of 3 casesJournal of Cranio-Maxitlofacial Surgery (1998) 26, 159-162
6. Suei Y, Tanimoto K, Taguchi A, Wada T, Primaryintraosseous carcinoma Review of literature and diagnosticcriteria. J Oral MaxillofacSurg 1994;52:580-583
7. Lin YJ, Chen CH, Wang WC, Chen YK, Lin LM, Primaryintraosseous carcinoma of mandible DentoMaxillofac Radiol2005;34:12-26.
Primary intra osseous carcinoma Chandra Shekar, et, al.
Indian J Dent Adv 2013; 5(3) Suppl 1: 1354-1358