Embed Size (px)
Citation preview

Primary Linitis Plastica of the Colon:
R e p o r t of a Case a n d R e v i e w of the L i t e r a t u r e *
JAYANTA R.OY CHOWDHURY, M.B.B.S., M.R.C.P. (U.K.),
KAMALA DAS, M.B.B.S., M.R.C.O.G. (LONI~.), KIRON M. DAS, M.D., Ph.D. t
From the Nassau County Medical Center, East Meadow, New York
"LINITIS PLASTICA" iS a term commonly used to describe a diffusely infiltrating car- cinoma of a hollow organ, which retains its shape, but becomes thick, rigid and dimin- ished in diameterA The lesion was first recognized in the stomach by Lieutaud 12 in 1779, and Andral 3 reported the first case in 1829 as a case of simple hypertrophy of the stomach. Because of the similarity of the interweaving collagen tissue of the lesion to linen cloth, Brinton s named the condition "linitis plastica" (Greek mean- ing: linen cloth or net) in 1865. Brinton, s however, was not sure of the neoplastic nature of the disease. It remained for Howard 9 to emphasize the malignant nature of the lesion in 1933. Since the his- tologic appearance of the lesion is so vari- able, 21, it seems reasonable to base the diag- nosis on its morphologic appearance which is so characteristic.
The stomach is the most common site of the linitis plastica type of carcinoma, and accounts for 99 per cent of this kind of lesion. 22 Approximately 10 to 15 per cent of all gastric carcinomas fall in this cate- gory. 17 The large bowel contributes 0.9 per cent and the gallbladder and breast together, 0.1 per cent. 22
In a series of 12,000 cases of carcinoma of the colon, only 11 cases of linitis plastica were found, an incidence of less than one
*Received for publication September 13, 1974. t Present address: Albert Einstein College of Medi-
cine, Bronx, New York. Address reprint requests to Dr. Chowdhury,
Nassau County Medical Center, 2201 Hempstead Turnpike, East Meadow, New York 11554.
Dis. Col. & Reet. May-June 1975
in 1,000.7 The majority of the cases of linitis plastica of the colon are secondary to similar lesions of the stomach and gall- bladder�9 About I00 cases of secondary linitis plastica of the colon have been reported so far. 2 Primary linitis plastica of the colon is even more rare, there being only 14 unequivocal cases in medical litera- ture.a, 2. 11, 13, 14, lS, 19, 21, 22 In addi t ion to
these, six cases 3, 6. s, 10 that the authors thought were examples of primary linitis plastica of the colon have been reported. But no definite evidence of absence of neo- plastic lesions of the stomach and gall- bladder is available in these reports, it is difficult to include these as primary lesions of the colon. In their report of 11 cases of linitis plastica-type carcinomas of the colon, Fahl et al. 7 did not differentiate be- tween primary and secondary lesions.
The purpose of the present paper is to review the features of the 14 cases reported in the literature, and in addition, to report a new case of primary iinitis plastica of the
colon.
Repor t of a C a s e
A 38-year-old Negro woman was admitted with complaints of episodic abdominal pain, diarrhea alternating with constipation, and gross rectal bleeding for three weeks. She had had no bowel problem in the past, and there was no history of weight loss. Menstrual periods were regular, but during the period prior to admission she had experienced dysmenorrhea, which was unusual for h e r ,
The past history was unremarkable, except that the patient had recurrent superficial thrombophle- bids from varicose veins of the leg during the preceding six years.
332 Volume 18
�9 Number 4

Volume 18 PRIMARY LINITIS PLASTICA OF T H E COLON 333 Number 4
FIG. 1. Bar ium-enema study, showing long, constricted segment of sigmoid colon.
Physical examinat ion showed that the pat ient was grossly obese, with slight pallor, bu t no cyanosis, jaundice or edema. There was no lym- phadenopathy . She had a deep diffuse tenderness over the left iliac fossa and the left lumbar region. Shifting dullness was present on percussion, but marked obesity precluded estimation of the exact quant i ty of ascitic fluid. Except for a positive test for occult blood in the stool, the rectal examinat ion was negative.
Pelvic examinat ion revealed a nodular mass in the pouch of Douglas and fullness of both fornices. It was possible to introduce the sigmoidoscope up to 18 cm only. Up to this level the mucosa of the rectum and sigmoid colon was normal, but blood was seen coming from above this level. Varicose veins were observed in the lower extremities, but no deep venous thrombosis was present. The rest of the physical examinat ion was within normal limits.
T h e initial blood studies showed: hemoglobin 12 g/100 ml; hematocr i t 36 per cent; leukocyte count 7,200 cu ram. neutrophils 73 per cent, lym- phocytes 26 per cent, and monocytes 1 per cent. P ro th rombin time was 13.9 sec (control 11.8 sec). Blood glucose was 107 rag/100 ml; blood urea ni t rogen 10 rag/100 ml; sodium 136 mEq/1, potas- s ium 3.8 mEq./1, bicarbonate 24 mEq/1, chloride 98 mFq/1; total protein 7.4 g/100 ml, a lbumin 4.33 g/100 ml; calcium 9.8 rag/100 ml; inorganic phos-
phorus 2.6 mg/100 ml; creatinine I mg/100 ml: bi l i rubin 0.4 mg/100 ml; alkaline phosphatase 57 IU; lactic dehydrogenase 194 IU; serum glutamic oxaloacetic acid transaminase 100 IU. Urinalysis was within normal limits.
Barium-enema studies showed a stricture of the proximal sigrnoid colon, 8 to 10 cm long, with minimal mucosal destruction. T h e out l ine of the colonic wall at the region of the str icture was gen. erally smooth, but on some views an appearance of shelving was suggested (Fig. 1). T h e radiologic picture was thought to be consistent with an inflammatory lesion of the colon, or an extracolonic neoplastic lesion enveloping and constrict ing the colon. T h e rest of the colon and the terminal i leum were normal. An upper gastrointestinal series and small bowel fol low-through were nor- mal, and so was the chest x-ray. An intravenous pyelogram revealed an extrinsic pressure defect on the dome of the ur inary bladder, bu t subsequent cystoscopy showed no abnormali ty .
During the following two weeks moderately se- vere ascites developed. T h e ascitic fluid was grossly bloody, with a protein content of 4.6 g/100 ml. Cytologic examinat ion of the fluid revealed malig. nant cells of adenocarcinomatous type ("Pap" class V). Cytology of the uter ine cervical smear was also positive for adenocarcinoma ("Pap" class V). Uter ine cervical biopsy, however, was negative for malignancy. At this stage a pr imary colonic neo-

334 CHOWDHURY, ET AL. Dis. Col. & Reef. May-J'une 1975
mass on the right side of the pelvis. A skeletal survey was unrevealing.
Immediately following completion of these in- vestigations, while the pat ient was being prepared for operation, she suddenly died of massive pul- monary embolism. This was approximately four weeks after her initial admission.
Postmortem examination showed a massive pul- monary embolism with infarction. T h e sigmoid colon contained an area of thickened, rigid wall, 10 cm long, with a smooth glistening inner lining, devoid of normal mucosal pat tern (Fig. 2). Tu- mor-like masses were found in both ovaries (Fig. 3). There was evidence of lymph-node metastasis in the intra-abdominal, para-aortic, and lower thoracic para-aortic lymph nodes. T h e peritoneum was seeded with numerous sites of metastasis.
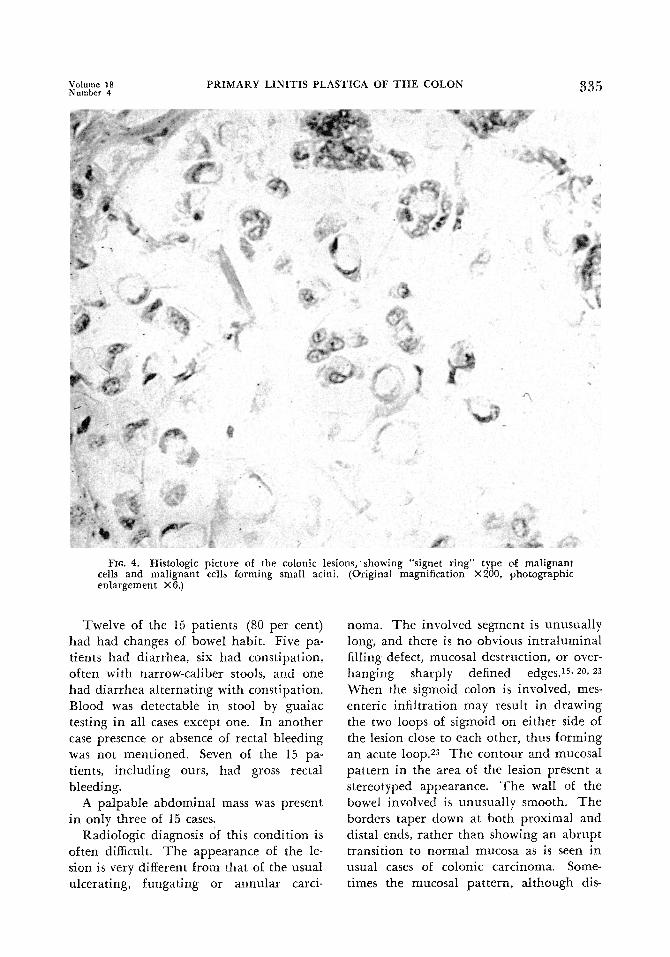
Microscopic examination of the colonic lesion showed a large number of darkly stained malignant cells, with large nuclei and scanty cytoplasm. Some malignant cells contained a large amount of amorphous mucoid material, giving them a "signet ring" appearance. Other malignant cells were seen in small glandular formation (Fig. 4). A similar histologic picture was found in the ovarian metastases.
The stomach, gallbladder, liver, and other ab- dominal viscera were normal both macroscopically and microscopically.
FIG. 2. Autopsy specimen of the involved area of the sigmoid colon.
plasm involving the ovary or a primary ovarian neoplasm involving the colon was suspected. A repeat barium-enema study three weeks after the initial study showed the same picture as before. A B-mode sonogram showed ascites, a large solid mass on the left side of the pelvis, and a smaller
D i s c u s s i o n
T h e c l i n i c a l d a t a o f 15 cases o f p r i m a r y
l i n i t i s p l a s t i c a o f t h e c o l o n a n d r e c t u m
a re p r e s e n t e d i n T a b l e 1. A n a l y s i s of t h e
d a t a d o e s n o t s h o w a n y sex p r e p o n d e r a n c e ,
t h e r e b e i n g s e v e n m a l e a n d e i g h t f e m a l e
p a t i e n t s . Ages of t h e p a t i e n t s r a n g e d f r o m
24 to 72 years .
Fro. 3. Metastatic in- volvement of bo th ova- r i~ .
Volume 18 PRIMARY LINITIS PLASTICA OF THE COLON 3 3 5 Number 4
FIG. 4. Histologic picture of the colonic lesions, showing "signet ring" type of malignant cells and malignant cells forming small acini. (OTiginaI magnification • photographic enlargement ?<6.)
Twelve of the 15 patients (80 per cent) had had changes of bowel habit. Five pa- tients had diarrhea, six had constipation, often with narrow-caliber stools, and one had diarrhea al ternat ing with constipation. Blood was detectable in stool by guaiac testing in all cases except one. In another case presence or absence of rectal bleeding was not mentioned. Seven of the 15 pa- tients, including ours, had gross rectal bleeding.
A palpable abdominal mass was present in only three of 15 cases.
Radiologic diagnosis of this condition is often difficult. T h e appearance of the le- sion is very different from that of the usual ulcerating, fungating or annular carci-
noma. T h e involved segment is unusually long, and there is no obvious in t ra luminal filling defect, mucosal destruction, or over- hanging sharply defined edgesAS, 20, 23 When the sigmoid colon is involved, rues- enteric infiltration may result in drawing the two loops of sigmoid on either side of the lesion close to each other, thus forming an acute loop33 T h e contour and mucosal pat tern in the area of the lesion present a stereotyped appearance. T h e wall of the bowel involved is unusually smooth. T h e borders taper down at both proximal and distal ends, ra ther than showing an abrupt transition to normal mucosa as is seen in usual cases of colonic carcinoma. Some- times the mucosal pat tern, al though dis-

336
,r
~
~
'-a
~ ~
"~ v
C H O W D H U R Y , E T A L .
0
o -~= ~ ~ ~ .=e~ =
i = ~ .. .~ ~ ~ =
�9 =~" .~E . ~ ~
{:m
~g ..~, =.=~'"
+ + + + + +
"8
~a e~ ~
~ z
<
0 z
+ + 4-
•a• M
, ~ ~ ~ ~ e ~ , ~
0 z
+ + +
O
8
"O
a e~ O
O,I
g
D i s . CoL & R e e t . M a y - J u n e 1975
a
0 , - .~
Z
g
0
+ + +
g
z
+
0 0
o~ . ~
8 t"4

Volume I8 PRIMARY LINITIS PLASTICA OF THE COLON 337 Number 4
c~ ,A
H
O
~ . ~ o
0
~ ~ ~ e ~ .
~ Z
O
+ + + + +
+ + +
O
~7
.~. s-~ ._~
<
torted, may persist, giving a deceptive appearance to an extracolonic lesion con- stricting the colon. Only occasionally the diagnosis may be made obvious by a filling defect or mucosal destruction within the lesion.
Th e demonstration of a very thick co- lonic wall, or a mass in contact with the colonic lesion, would help greatly in mak- ing the diagnosis of a neoplastic lesion? 3 but this is often not possible by barium- enema examination of the colon. In our patient ultrasonographic B-mode scanning demonstrated a solid pelvic mass of large size in the region of the sigmoid colon and the left adnexa. This helped us to diag- nose a neoplastic lesion, but not in decid- ing whether the lesion was primarily of the ovary or of the sigmoid colon.
Th e gross pathology of the lesion is char- acterized by an undetectable or insignifi- cant primary tumor mass, and spread along the submucosal plane, involving a long segment of the intestine. 16 Th e mucosa is usually smooth and devoid of the normal folds. Occasionally areas of ulceration may be seen. Microscopically, significant inflam- matory infiltration, mucoid deposition, and variable fibrosis coexist with the malignant cells. The malignant tissue itself consists of three elements: 1) darkly stained round malignant cells with large nuclei and sparse cytoplasm; 2 ) the signet-ring cell, with the nucleus pushed to the periphery by intracellular deposits of mucoid mate- rial; 3) malignant ceils arranged in glandu- lar formation.
As linitis plastica is more often secondary to a similar lesion in the stomach or gall- bladder than it is a primary lesion of the colon, the stomach and gallbladder must be closely examined in these patients. Only in the absence of a malignant lesion of these organs can the colonic lesion be diag- nosed as primary.
In all 12 cases, including ours, in which autopsy findings were reported, the pa-

338 CHOWDHURY, ET AL. Dis. Col. & Reet. May-J'une 1975
t ients had per i tonea l metastasis. Seven of
the 12 pa t i en t s had lymph-node involve- m e n t as well. Of the seven female pa t ients
autopsied, six had metasta t ic i nvo lvemen t of the ovaries. Hepat ic metastasis, which is
so c o m m o n in the usual forms of colonic carcinoma, is conspicuous by its rar i ty i n
p r imary l in i t i s plastica of the colon. Only
one of 12 autopsied pa t ients had hepat ic metastasis, a I n one o ther pa t i en t hepat ic metastasis was found at operat ion. 19
T h e prognosis of pa t ien ts who have this cond i t i on has been un i fo rmly poor, the
periods of survival r ang ing from two weeks
to 27 m o n t h s after in i t i a l admiss ion to the hospital . One-year survival has been re- por ted to occur in only two cases.l, is One
of the two pat ients survived 27 months .
Th i s pa t i en t had been treated wi th 5-fluoro- uracil , xs T h e poor prognosis appears to
be re la ted to the fact that the lesion is very
rare, and of ten is confused wi th inf lamma- tory bowel diseases, r e su l t ing in delay in
diagnosis. As the neop la sm spreads very
rap id ly by both local invas ion and metasta- sis, any delay in i n s t i t u t i o n of defini t ive
therapy greatly reduces the chances of survival.
W i d e resection of the lesion, wi th re-
moval of an a b u n d a n t a m o u n t of mesen- tery in its vicini ty, has been recommended . In add i t i on to this, Sizer et al. ~8 advised
hysterosalpingo-oophorectomy, i n view of
the h igh incidence of early metastasis to these organs. T o o few pat ients have been
treated wi th cytostatic therapy to establish
its role i n the t r ea tment of this condi t ion , bu t in one case 5-fluorouracil led to in-
vo lu t i on of the lesion, which p rompt ly re- curred fo l lowing wi thdrawal of the drug. ~s
W i t h increas ing fami l ia r i ty wi th this
condi t ion , it is hoped that earl ier diagnosis
will be possible in the future, l ead ing to
bet ter prognosis.
References
1. Andersen JA: Primary linitis plastica of the colon and rectum. Acta Pathol Microbiol Scand A 78:227. 1970
2. Andersen JA, Hansen BF: Linitis plastica of the colon and rectum: Report of two cases. Dis Colon Rectum 15:217, 1972
3. Andral: Quoted by Dixon CF, Stevens GA: Carcinoma of linitis plastica type involving the intestine. Ann Surg 103:263, 1936
4. Btoquiaux W: Primaire linitis plastica van her colon. Tijdschr Gastroenterol 13:309, 1970
5. Brinton W: Lectures on the Diseases of the Stomach. London, John Churchill and Sons, 1864, 136 pp
6. David VC: Malignancy in linitis plastica. Surg Clin North Am 11:47, 1931
7. Fahl J.C, Dockerty MB, Judd ES: Scirrhous carcinoma of the colon and rectum. Surg Gynecol Obstet 1t1:759, 1960
8. Fontaine R, Wafter P, Franck P, et al: Linite plastique primitive du rectum: Apropos de deux observations. J Radiol Electrol Med Nucl 39:586, 1958
9. Howard CP: Linitis plastica: A study of ten cases. Q J Med ns 2:59, 1933
10. Jacobi MA: Primary linitis p!astica carcinoma of the colon. Wis Med J 69:211. 1970
11. Laufman H. Saphir O: Primary linitis plastica type carcinoma of the colon. Arch Surg 62: 79, 1951
12. Lieutaud: Quoted by Dixon CF, Stevens GA: Carcinoma of linitis plastica type involving the intestine. Ann Surg 103:263, 1936
13. McQueeny AJ, Olson RW, Medwid A: Primary scirrhous carcinoma of colon: Roentgeno- logic diagnosis. Am J Roentgenol Radium Ther Nucl Med 101:306, 1967
14. Nelson PG: Primary linitis plastica carcinoma of the colon. Aust NZ J Surg 34:288, 1965
15. Phalke IM, Smallwood CJ, Wright FW: Linitis plastica of the colon. Clin Radiol 20:224, 1969
16. Saphir O, Parker ML: Linitis plastica type of carcinoma. Surg Gynecol Obstet 76:206, 1943
17. Schenken JR, Burns EL: The gastrointestinal tract. In: Anderson WAD (ed): Pathology. Ed 3, St. Louis, The C. V. Mosby Company. 1957. Pt. 2, Chapt. 26, p 745
18. Sizer JS, Frederick PL, Osborne MP: Primary linitis plastica of the colon: Report of a case and review of the literature. Dis Colon Rectum 10:339, 1967
19. Speer C8: Linitis plastica carcinoma of the colon: Report of a case. Dis Colon Rectum 14:389, 1971
20. Sussman ML: Coincident scirrhous lesions of the stomach and colon: Report of cases. Am J Roentgenol Radium Ther Nucl Med 33: 205, 1935
21. Turnbull RB, Fisher ER, Rosenak BD: Pri- mary linitis plastica carcinoma of the colon. Cleveland Clin Q 18:210, 1951
22. Weintraub LR, Littman L: Primary linitis plastica of the rectum: Report of a case. Dis Colon Rectum 5:105, 1962
23. Wolf BS, Marshak RH: Linitis plastica or diffusely infiltrating type of carcinoma of the colon. Radiology 81:502, 1963





























