Embed Size (px)
Citation preview

FINAL REPORTSeptember 2010
Primary Percutaneous Coronary Intervention
Optimizing Access to Primary PCI for ST Elevation Myocardial Infarction
primary percutaneous coronary intervention 1
table of contents 3 Foreword 4 Introduction 4 Background 6 The Primary Percutaneous Coronary Intervention Subcommittee 7 Methods 7 Findings 7 Primary Percutaneous Coronary Intervention Literature Review 10 Primary Percutaneous Coronary Intervention Service in Ontario 10 Primary Percutaneous Coronary Intervention Program Development
in Ontario: Guiding Principles 10 Current Primary Percutaneous Coronary Intervention Services
Available in Ontario 12 Primary Percutaneous Coronary Intervention Data Collection 12 Staging of Primary Percutaneous Coronary Intervention Services 16 The Challenge: Overcoming Barriers to Access 29 FutureDirection 30 References 34 Bibliography 37 Appendix1:GlossaryofTerms 40 Appendix2:CCNMemberHospitals 55 Appendix3:OntarioCardiacCentresPrimaryPercutaneousCoronary
InterventionPhysicianLeads 56 Appendix4:AccesstoUrgentPercutaneousCoronaryInterventionfor
STeMI:16Recommendations 59 Appendix5:CanadianCardiovascularSocietyCodeSTeMIAlgorithm 60 Appendix6:CCNPCI/STeMICaseReportForm(Draft) 61 Appendix7:PPCI/STeMICaseReportForm/DataDictionary 67 Appendix8:NejM:ACitywideSTeMIProtocol 69 Appendix9:CCNCath/PCIWorkingGroup 69 Appendix10:Acknowledgements

primary percutaneous coronary intervention 2
The Cardiac Care Network of Ontario (CCN) serves an advisory role on adult cardiovascular
care working closely with key stakeholders, including the Ministry of Health and Long-
Term Care, Local Health Integration Networks, hospitals, health care providers, planners
and researchers. Our focus and priority is quality of care, supporting leading practices and
system-wide improvements to achieve excellence in patient care and clinical outcomes. In
addition to monitoring and reporting on wait times and access to advanced cardiac services,
CCN monitors and reports on other key performance metrics to ensure quality and effi ciency
within the system of adult cardiovascular services in Ontario.
CCN is committed to sharing knowledge and information that fosters leading practices and
helps to establish benchmarks and standards for optimal care. We are pleased to provide
you with information relevant to programs providing regionalized care for acute myocardial
infarctions, including primary percutaneous coronary intervention for ST elevation myocardial
infarctions. We hope you fi nd this document informative, and a resource to support your
cardiac program.
Yours truly,
Kori Kingsbury
Chief Executive Officer
Cardiac Care Network of Ontario
Kori Kingsbury

primary percutaneous coronary intervention 3
ForewordAs Chairs of the Primary Percutaneous Coronary Intervention Subcommittee (pPCI-SC) of the
Cardiac Care Network, we are pleased to present this coaching document, Primary Percutaneous
Coronary Intervention: Optimizing Access to Primary PCI for ST Elevation Myocardial Infarction.
The purpose of this document is to provide a vehicle for knowledge transfer that will assist
health care providers and planners in the adoption of leading practices in the provision of ST
segment elevation myocardial infarction (STEMI) care. As part of the CCN’s coaching series
to support leading practices, quality and performance improvement, this document outlines
strategies that are proven to work, identifi es the signifi cant lessons learned and the critical
steps in implementing a successful primary PCI (pPCI) program. We believe that success can be
more broadly achieved by leveraging the experience and sharing the lessons learned of hospital
programs and health care professionals in Ontario that have achieved the requisite level of
services and demonstrated their ability to deliver integrated, regionally supported, 24 hour,
7 days a week (24/7) pPCI services.
Within Ontario, The University of Ottawa Heart Institute, Kingston General Hospital, Hamilton
Health Sciences Centre and Southlake Regional Health Centre were the early adopters of
regional integrated pPCI STEMI programs to meet the needs of their communities. Experts from
these hospitals were brought together by the pPCI-SC, in order to share their experiences and
observations in establishing a 24/7 regional pPCI program with EMS fi eld support. Currently
there are 14 hospitals in Ontario providing some level of pPCI services for STEMI patients. Some
centres are further along in the establishment of their comprehensive regional pPCI programs,
while others are in the earlier stages of development.
Primary angioplasty has been shown to be superior to fi brinolysis when delivered in a timely
manner by experienced operators and teams. Leading practices for pPCI STEMI care are based
on the ACC/AHA guidelines1 that recommend the interval between arrival at the hospital and
intracoronary balloon infl ation (“door-to-balloon” time) to be 90 minutes or less. A review of pPCI
door-to-balloon (D2B) times at Ontario’s PCI centres demonstrated variable median D2B times
with room for improvement across all centres to better align with the ACC/AHA recommendation.
With CCN’s focus on equity, access, and quality of care, this served as a call to action to assess
the alignment of practice with an accepted standard of care and accountability in delivering
quality pPCI services.
Building upon the principle, “the system helping the system,” it is hoped that this document
will be a resource for other PCI centres and regions considering the implementation of a
comprehensive, coordinated pPCI program based on leading practices.
We wish to thank all committee members and CCN staff who assisted in the development of this
document to promote equitable access to quality pPCI care for STEMI patients in Ontario.
Sincerely,
Dr. James Velianou, Dr. Jean Francois Marquis,
Hamilton Health Sciences Centre University of Ottawa Heart Institute
Dr. James Velianou
Dr. Jean Francois Marquis
primary percutaneous coronary intervention 4
IntroductionA signifi cant proportion of patients in Canada are treated with pPCI for STEMI, however
many others continue to be treated with fi brinolysis. Fibrinolysis is demonstrated to improve
survival in a number of large randomized controlled trials when compared to medical
therapy alone, however, pPCI has been shown to be superior to fi brinolysis when delivered
in a timely manner by specially trained cardiologists and catheterization laboratory (cath
lab) teams.2 This superiority is based on the reduction of morbidity (stroke and re-infarction)
and mortality in patients presenting to or transferred to a pPCI capable centre. Patients
not treated with any reperfusion therapy have signifi cantly higher mortality in the range of
15–25%.
Primary PCI (when it can be performed rapidly), as the preferred fi rst treatment for STEMI,
requires services to be delivered by personnel with an appropriate level of experience and
training, in a setting with advanced cardiac diagnostic monitoring available 24/7, with the
availability of immediate access. By leveraging the expertise and lessons learned of those
PCI programs that have achieved this requisite level of service, the CATH/PCI Working Group
of the Cardiac Care Network of Ontario (CCN) endorsed the development of a pPCI coaching
document that could serve as a resource for other PCI centres and regions considering the
provision of pPCI services. This document is to facilitate knowledge transfer by outlining
strategies that have been demonstrated to work, signifi cant lessons learned and the critical
steps in implementing a successful pPCI program.
Background In 2004, CCN released its report, Access to Urgent PCI for ST Segment Elevation Myocardial
Infarction. The report identifi ed 16 recommendations (See Appendix 4) on how pPCI could be
implemented in Ontario along with the following summary recommendation:
“ [where appropriate] pPCI should become the dominant strategy for the reperfusion of
ST Segment Elevation Myocardial Infarction (STEMI) in Ontario.”
The report outlined several key challenges to moving forward with this recommendation,
including:
Lack of an explicit provincial commitment to the systemic delivery of pPCI;
Need for a coordinated approach to advanced cardiac services delivery within a region;
Complexity in the deployment of emergency medical services (EMS) operations at the
municipal level;
Availability of ambulance services and trained paramedics throughout the province; and
Cardiac cath lab resources (particularly human resources) that are necessary to expand
capacity and ensure service availability 24/7;

primary percutaneous coronary intervention 5
Physical resources, such as high acuity beds, to accommodate additional case load at PCI
centres as well as at the referring hospitals;
Geographic limitations that result in transport delays to the nearest PCI centre; and
Repatriation of patients back to their referring centre or community hospital.
In spite of these challenges, four “early adopter” PCI centres in Ontario independently decided
to work with their relevant stakeholders to develop and implement regional and integrated
pPCI STEMI programs to meet the needs of their communities. These centres (in order of fi rst
to most recently implemented) include The University of Ottawa Heart Institute, Kingston
General Hospital, Hamilton Health Sciences Centre, and Southlake Regional Health Centre.
Success is not only defi ned in relation to direct benefi ts, such as improved patient outcomes,
but also in terms of ongoing program evaluation, process improvement, and developing
collaborative relationships. This not only contributes to leading practices with regard to the
recommended ACC/AHA guideline of a 90-minute interval between fi rst medical contact and
intracoronary balloon infl ation (D2B), but also provides a template for system-orientated
care. In addition, from a regional perspective, pPCI STEMI care also establishes the key
infrastructure that is needed to address other cardiovascular care issues, such as early
stroke intervention.
Irrespective of the documented benefi ts, access is a major limitation to a pPCI strategy for
STEMI. With the extensive geography of the province, access to PCI is not available in every
region of the province. In addition, up until recently, some of the PCI programs in Ontario did
not provide 24/7 pPCI or only provided access to pPCI on a limited basis. Since April 2006,
CCN has collected pPCI data to evaluate D2B times for the hospitals in Ontario providing
pPCI. Preliminary analysis of these data suggests there is considerable practice variation and
access to pPCI within the accepted timeframe of 90 minutes or less.
“Time is myocardium” is perhaps one of the most explicit metaphors in cardiac care
describing the imperative for urgency associated with access to the right care at the right
time by the right people. As the pPCI service delivery unfolded across Ontario, there were no
commonly agreed upon standards of practice for the organization of pPCI service delivery
given the regional complexities and unique differences in geography and the Local Health
Integration Networks (LHINs) across Ontario. While PCI providers saw this level of care as
a priority for their centres, they were challenged to provide this level of service and were
often limited by a lack of resources, support and/or infrastructure. With determination,
perseverance and creativity, the majority of the PCI centres in Ontario were able to overcome
these challenges and now provide pPCI with regional models of care.
Subsequent to the work of this subcommittee, several other initiatives have been launched,
and the majority of PCI centres in Ontario now offer pPCI for STEMI.
primary percutaneous coronary intervention 6
Access to, and delivery of, pPCI services to improve patient outcomes demands change in
the organization and deployment of PCI services. There is a shared accountability between
PCI centres, EMS services and referring hospitals. While process improvements can assist
PCI centres to achieve the recommended guidelines for D2B time, leading practices involve
extensive interdisciplinary collaboration and require explicit strategies for overcoming
barriers to implementing organizational change. Organizations that have adopted and learned
from these practices play a key leadership role in assisting other centres to improve patient
access to pPCI services where appropriate.
Since the 2004 publication of the CCN Access to Urgent PCI for ST Segment Elevation
Myocardial Infarction report, several Ontario hospitals embarked on developing and
successfully implementing pPCI programs. The collaboration between partner hospitals in the
LHINs, engagement of key stakeholders in the planning and implementation of the programs
has contributed greatly to the success of the programs. Successful education of EMS
personnel that included ECG interpretation has been one of the main key success factors
in transporting the patient from the fi eld to the cath lab at the pPCI hospitals in a timely
fashion. Today, Ontario has 14 hospitals providing PCI services, 11 full-service cardiac
hospitals with on-site cardiac surgery and three stand-alone centres without cardiac surgery
back-up.
THE PRIMARY PERCUTANEOUS CORONARY INTERVENTION SUBCOMMITTEE
In recognition of what is required to support the successful implementation of integrated
regional pPCI services in Ontario, the CCN CATH/PCI Working Group established the
primary PCI Subcommittee (pPCI-SC) to provide guidance to the broader acute care cardiac
community with regards to service organization and stakeholder collaboration at the system,
organizational and local level. Membership on the pPCI-SC included a multidisciplinary
group experienced with establishing pPCI and representing the 24/7 regional integrated EMS
pPCI programs in Ontario. The scope of the pPCI-SC was to review the four fully operational,
integrated regional pPCI programs in Ontario and identify key success factors and signifi cant
lessons learned, as well as the critical steps required for implementation. The specifi c
deliverables included:
The creation of a coaching document to assist hospitals, LHINs, and policy makers in the
planning and implementation of an integrated pPCI program; and
A document that would be based on the recommendations from the Report on Access to
Urgent PCI, as well as expert opinion relevant to the lessons learned from programs that
had successfully implemented a fully operational, integrated regional model for 24/7 pPCI.
The work of this subcommittee was accountable to the CCN Board of Directors through the
Clinical Services Committee (CSC). The fi nal report and recommendations were presented to the
CSC and the CCN Board of Directors for fi nal review and endorsement prior to distribution to
other cardiac centres and relevant stakeholders, such as the LHINs and the MOHLTC.

primary percutaneous coronary intervention 7
MethodsThe development of this coaching document by the pPCI-SC has been informed through four
specifi c processes that included:
1. A review of the current literature on the evidence supporting pPCI as a preferred
treatment for STEMI;
2. A review of the CCN data on D2B times in Ontario;
3. A survey of a broad range of cardiac care stakeholders at all cardiac hospitals in the
province to assess the priority associated with pPCI services at their centre and identify
any challenges and potential barriers; and
4. An in-depth presentation from each committee member identifying the challenges
and lessons learned in implementing a fully integrated 24/7 regional pPCI service.
Members were asked to prepare a focused and comprehensive summary of their role in
implementation. These were collated into a single document and reviewed by the entire
committee for content and completeness.
From the above activities, common themes, challenges, strategies and lessons learned
emerged to aid in the development of a coaching framework to support the implementation
of pPCI programs.
Findings
PRIMARY PERCUTANEOUS CORONARY INTERVENTION LITERATURE REVIEW
The superiority of pPCI as an intervention for STEMI is based on the reduction of mortality
(7% vs. 9%, p=0.0002), stroke (1% vs. 2%, p=0.0004), non-fatal re-infarction (3% vs. 7%, p<0.0001)
and a composite of these adverse events (8% vs. 14%, p<0.0001) in patients presenting to, or
transferred to, pPCI capable centres.3
A study published by Neilson (2010) demonstrated that pPCI signifi cantly reduced the
composite end-point by an absolute 9.3%, all-cause mortality by 6.6%, and re-infarction by
6.4%. The long-term data thus reinforce that pPCI should be offered to STEMI patients, not
only those admitted to an invasive hospital but also those patients for whom transport from
a referral to an invasive hospital can be completed within 2 hours.4 Clearly, if evidence-based
medicine were to be carried out, then pPCI would be the dominant strategy for most of the
population in the province of Ontario, where all pPCI capable centres provided this service.
As previously stated, this was the recommendation of the CCN consensus panel on pPCI that
published its fi ndings.5
ACC/AHA guidelines recommend that patients treated with fi brinolysis have a door-to-needle
(D2N) time of less than 30 minutes and patients treated by pPCI have a D2B time of less than
90 minutes.6 However, these guidelines were based on the number of randomized controlled
trials that actually had 90- to 120-minute median of D2B times. These studies themselves

primary percutaneous coronary intervention 8
were quite selective since there was not a signifi cant number of patients randomized that
had delays from door to ECG and/or recognition. It is clear that in a signifi cant number of
patients, there was room for improvement for both D2N and D2B times. A more important
value in determining this practice may in fact be limiting the difference between D2N and
D2B times. If D2B times are greater than 60 to 70 minutes over D2N times, then there may be
equivalence in terms of mortality; although stroke and re-infarction reduction would still be
improved with pPCI. However, certain variables such as older age, anterior infarction and late
presentation may in fact extend to a difference of over 110 minutes; thereby extending the
coverage of pPCI to a larger number of eligible patients that could potentially benefi t.7,8
Decreasing D2N and D2B times ultimately enhances access to care for all AMI patients.
This would include AMI patients who cannot be treated with fi brinolysis, who have failed
fi brinolysis therapy, and/or who are in cardiogenic shock; and those treated by a more
aggressive pharmaco-invasive strategy that must travel from a wider geography to access
tertiary cardiac care services.
A system-wide approach to improving D2B times is necessary in attempt to standardize the
coordination of multiple processes involved, from the identifi cation of a STEMI patient in
the fi eld, to the targeted reperfusion intervention. In a survey of 365 hospitals in the U.S., six
processes/strategies were found to be independently associated with improved D2B times.
These six strategies included the following:10,11
1. Emergency department activation of the cardiac cath lab;
2. Single call systems;
3. Early arrival of cath lab teams;
4. Data monitoring and feedback;
5. Administrative support of pPCI program; and
6. System-wide team-based approach from EMS to cath lab.
Multiple medical centres in the United States and Europe have put into place a system of
regional pPCI to improve treatment of STEMI in a given population. These systems provide
24/7 coverage for a population in a given geographic area with prompt transfer of appropriate
patients to the appropriate centres.12,13,14
A CCN consensus panel previously recommended that the dominant strategy for reperfusion
in STEMI in Ontario should be pPCI.15 Unfortunately, not all patients in Ontario are offered
this as a fi rst line reperfusion therapy. Groups from Calgary and Ottawa have published their
experiences with regional pPCI.16,17 Their results reveal that this service can be provided
within a Canadian health system if a system-wide approach is utilized. In fact, many of the
strategies they have utilized have been set out by the D2B: An Alliance for Quality to attain
their results.18,19
primary percutaneous coronary intervention 9
An Ontario Health Technology Advisory Committee (OHTAC) published a report for the
MOHLTC on pPCI in Ontario, which reviewed the evidence and costs associated with pPCI,
and rendered an opinion regarding the widespread implementation of the intervention. This
report agreed that the evidence clearly favored pPCI when compared to fi brinolysis for the
treatment of STEMI. However, this report stated that in order to provide pPCI province-
wide, it would take an inordinate amount of funding (human resources, training and capital
expenses) and time (up to 16 years) to fully implement (the timeline was largely based on EMS
training).20 Despite the report, the Ontario experience has demonstrated that it is possible to
overcome the stated limitations and successfully implement regionalized 24/7 pPCI programs.
In fact, cost analysis from the University of Ottawa Heart Institute and Hamilton Health
Sciences Centre concluded that pPCI, compared with fi brinolysis, resulted in lower
hospitalization costs and decreased adverse events of death, re-infarction, stroke, and repeat
target vessel revascularization.21,22
Clinical evidence indicates that pPCI is the gold standard treatment for patients suffering
from STEMI, and patients should not be disadvantaged due to the time of day they present
with their STEMI. Additional advantages of 24/7 pPCI services include:
Reduced hospital length of stay – a reduction of 1–1.5 days for patients who undergo pPCI
rather than thrombolysis;
All patients receive optimal treatment and best opportunity for optimal clinical outcomes;
Equity of high quality care for all STEMI patients;
Patient care pathways are streamlined and provide more effi cient transition points of care
for all patients;
A reduction in patients requiring emergency inter-hospital transfer for failed
thrombolysis; and
Optimal utilization of available tertiary/quaternary resources within the PCI Centre.
Overall, the evidence from the literature reveals that pPCI can signifi cantly reduce morbidity
and mortality when provided in a timely fashion by experienced teams. Primary PCI is
considered more effective than fi brinolysis at preventing repeat myocardial infarctions
and stroke if done in a timely manner. Improved patient outcomes are also associated with
reduced re-admission rates and decanting emergency departments of AMI patients.
primary percutaneous coronary intervention 10
PRIMARY PERCUTANEOUS CORONARY INTERVENTION SERVICE IN ONTARIO
A recent study led by Dr. William Ghali from the University of Calgary found that 70% of
Ontario residents live within one hour of a hospital that can provide optimal care (pPCI) for
those suffering an MI.23 In Ontario, there are 14 hospitals providing PCI services, 11 full-
service and three stand-alone centres without cardiac surgery services on-site. CCN, in
collaboration with clinical experts from the fi eld, identifi ed a set of general principles to
guide discussions with regard to distinctions between (1) converting a diagnostic cardiac
catheterization lab to a PCI lab; (2) starting up a brand new stand-alone PCI service; and (3)
developing a comprehensive pPCI program.
PRIMARY PERCUTANEOUS CORONARY INTERVENTION PROGRAM DEVELOPMENT IN ONTARIO:
GUIDING PRINCIPLES
Thrombolytic therapy remains a therapeutic option for STEMI patients who are unable to
receive pPCI. Pre-hospital diagnosis of STEMI in the context of a regional program has the
potential to expand the geographic reach of pPCI based on existing capacity. Four key guiding
principles to establish a pPCI program include:
1. Delivering pPCI services requires the advanced skills of a well-established PCI program,
experienced in the care and management of high risk, acutely ill patients;
2. A comprehensive pPCI program should include service availability for STEMI or AMI
patients 24 hours a day, 7 days a week;
3. Ensuring the 24/7 availability of pPCI services does not place extraordinary burden
on hospital system resources, including health human resources; and
4. To optimize effi ciency, pPCI services will require a minimum of two cardiac cath
labs on-site.
CURRENT PRIMARY PERCUTANEOUS CORONARY INTERVENTION SERVICES AVAILABLE IN ONTARIO
As demonstrated in the literature review, leading practices have been established for the
provision of pPCI as part of a regionalized program, with equity in access and better patient
outcomes associated with these best practices, including services that are provided regionally
on a 24-hour, 7 days a week basis and EMS triage in the fi eld. Currently, there is a range of
pPCI services in Ontario including (a) pPCI provided Monday to Friday based on regular
cath lab operating hours and the availability of the lab to accommodate the patient; (b) pPCI
provided to those patients that present in the PCI hospital’s own emergency department; and
c) fully integrated 24/7 service provided on a regional basis with EMS triage fi eld support.
An Ontario example of one model described above is cited in The New England Journal
of Medicine (LeMay et. al., January 17, 2008). Between May 1, 2005 and April 30, 2006, 344
consecutive patients with STEMI were referred to the University of Ottawa Heart Institute for
pPCI: 135 patients directly from the fi eld and 209 patients from emergency departments. pPCI
was performed in 93.6% of patients. Mean D2B time was shorter for patients referred from
the fi eld (69 minutes with a range of 43–87 minutes) than in patients needing inter-hospital
transfer (123 minutes, with a range of 101–153 minutes). D2B times of less than 90 minutes
were achieved in 79.7% of patients who were transferred from the fi eld and in 11.9% of those

primary percutaneous coronary intervention 11
transferred from emergency departments.24 A copy of the article can be found in Appendix 8.
A complete list of the hospitals in Ontario providing pPCI services, a program overview, and a
list of the program specific highlights is found in Appendix 2.
Table 1 below illustrates the most current distribution of pPCI services across the 14 PCI
centres in Ontario based on: a) regional transport of patients to the PCI centre; b) 24/7
operations; and c) EMS field support.
Table 1. Distribution of Regional, 24/7 and EMS Supported pPCI Services in Ontario
FULL-SERVICE (PCI and CaRdIaC SURGERY) PROGRaM n = PROVIdEd n = nOt PROVIdEd
REGIOnaL tRanSPORt
24/7 OPERatIOnS EMS tRIaGE
Hamilton Health Sciences Centre n n n
Kingston General Hospital n n n
London Health Sciences Centre n n n
Southlake Regional Health Centre n n n
St. Mary’s General Hospital n n n
St. Michael’s Hospital* n n n
Sudbury Regional Hospital n n n
Sunnybrook Health Sciences Centre n n n
Trillium Health Centre n n n
University Health Network n n n
University of Ottawa Heart Institute n n n
Stand-aLOnE PCI CEntRES n = PROVIdEd n = nOt PROVIdEd
REGIOnaL tRanSPORt
24/7 OPERatIOnS EMS tRIaGE
Hôtel-Dieu Grace Hospital – Windsor n n n
Rouge Valley Health System n n n
Thunder Bay Regional Health Sciences Centre n n n
* Also has a partnership program with Toronto East General Hospital.

primary percutaneous coronary intervention 12
PRIMARY PERCUTANEOUS CORONARY INTERVENTION DATA COLLECTION
CCN has been collecting pPCI D2B times since October 2006. Based on a review of the pPCI data
collected, and the availability of new information related to performance metrics to improve D2B
times, CCN undertook a review to enhance the data variables and extend the data collection to
other key aspects relevant to STEMI care and system performance. In addition, CCN focused on
system processes and standard data defi nitions to ensure that data are consistently captured
and comparable between programs. Please refer to Appendix 7 for a sample of a CCN case report
form to track the necessary metrics pertaining to pPCI for STEMI.
STAGING OF PRIMARY PERCUTANEOUS CORONARY INTERVENTION SERVICES
As a PCI program plans to expand their service delivery model to include pPCI services,
phasing services in a step-wise approach to implementation may be preferable as a
deployment strategy. This graduated approach serves to implement the program by starting
pPCI services with STEMI patients presenting within the PCI hospital (either through
the emergency department or other hospital areas). The complexity of managing a patient
experiencing an AMI in the context of a cardiac cath lab should not be understated. Once
skills and baseline competencies have been achieved meeting the needs of patients within the
hospital setting, the service delivery model can then be expanded to accept STEMI patients
as transfers in from other non-PCI hospitals and/or patients brought to the PCI hospital
directly from the fi eld by EMS. This graduated approach to program implementation allows
the PCI centre to refi ne their internal processes and clinical competencies prior to meeting
the many demands and complexities of a regional program to support external stakeholders
and patients from a wider geographical area
Phase 1: PCI Centre 24/7 – Admitted PatientsThe fi rst model of delivery is the management of patients who present with STEMI at the
PCI hospital, either via the emergency department or as a patient admitted with an acute
coronary syndrome that evolves into an acute STEMI.
Typically, PCI hospitals will launch their pPCI program by fi rst providing pPCI services
during regular cath lab operating hours and then work towards expanding their coverage
to support 24/7 operations, through systems of on-call staffi ng and support. This graduated
approach to expanded coverage helps to ensure that internal infrastructure and processes
are established and streamlined prior to adding the complexity of expanded coverage that
can lead to staff and/or program fatigue. In addition, advanced in-hospital protocols such as
“Code STEMI” can be developed and trialed prior to broad scale implementation. Key elements
of a Code STEMI program include:
Timely assessment of STEMI;
Direct notifi cation/activation of cath lab team;
Direct patient transfer to the cath lab; and
Debrief on STEMI cases to determine opportunities for improved effi ciencies.
primary percutaneous coronary intervention 13
Once a PCI hospital has demonstrated its ability to successfully perform pPCI on a 24/7
basis, achieving the recommended targets for D2B times for the majority of STEMI patients
presenting directly to their own emergency department or from within the hospital, it would
be appropriate to expand to Phase 2 or 3 depending on regional resources.
Phase 2: Non-PCI Hospitals 24/7The second model is the coordination of pPCI services for patients originating from non-PCI
hospitals. This requires a system of accelerated referral to expedite the transfer of the patient
between the non-PCI and PCI hospitals. Also included is the timely assessment of STEMI and
rapid transport of the patient to the pPCI hospital. Key elements of this model include:
Timely assessment of STEMI patient at non-PCI hospital;
Rapid communication and activation between non-PCI hospital and PCI hospital;
Agreement to transfer patient in a highly automated and coordinated manner to
expedite care;
Rapid transport by EMS, with direct admission to the cath lab; and
Repatriation of patient back to the non-PCI hospital, once the patient is stabilized
post-procedure.
Phase 3: Field Patients with Direct Transfer to PCI Centre, 24/7In the third model of care, the patient is assessed by the EMS team in the fi eld and then
directly transported to the PCI centre. With evidence of a STEMI by way of the ECG performed
by paramedics in the fi eld, the patient is directly admitted to the cath lab at the nearest PCI
centre. Through direct admission to the cath lab from the fi eld, the patient bypasses a non-
PCI hospital, which expedites D2B time. This model has additional requirements to enable
EMS to bypass other acute care hospitals enroute to the PCI centre. With this model, upon
occasion, a profoundly clinically unstable patient may require stabilization at the closest
acute care hospital prior to transfer to the regional PCI centre (e.g., similar to the trauma
model). This integrated EMS model with identifi cation of STEMI patients in the fi eld requires
the paramedics to have the appropriate skills and training to assess a patient for STEMI by
way of ECG acquisition and/or reading. For regions that are capable of pre-hospital STEMI
diagnosis and bypassing the closest acute care hospital to access PCI centre, this model
achieves treatment times that are considerably shorter than for patients transferred from
other emergency departments.
Key elements of this model include:
Timely assessment of STEMI through acquisition of ECG and diagnosis by paramedic
in the fi eld;
Rapid communication and activation between EMS and PCI hospital;
Bypass protocols established for EMS, authorizing direct transfer to nearest PCI centre
rather than closest acute care hospital;
primary percutaneous coronary intervention 14
Established agreements in place to facilitate direct transfer of patients in a highly
automated and coordinated manner to expedite care;
Rapid transport by EMS, with direct admission to the cath lab; and
Repatriation of patient back to the non-PCI hospital, once the patient is stabilized
post-procedure.
Rather than trying to achieve a full-service, 24/7 regional pPCI service at the early
implementation stages of the program, it is advisable to expand the service delivery models
of pPCI over time. Streamlining the process is paramount to achieving the targets of D2B, or
fi rst medical contact-to-balloon time of <90 minutes.
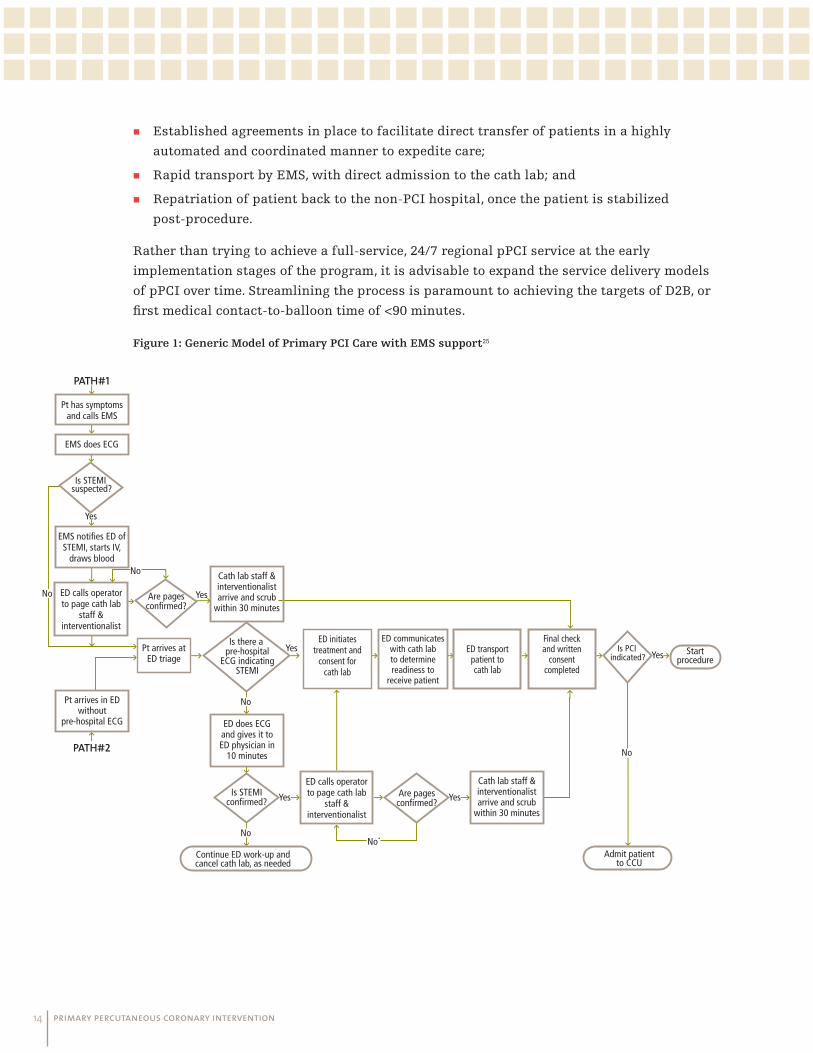
Figure 1: Generic Model of Primary PCI Care with EMS support25
PATH#1
PATH#2
Yes
Yes
Yes
Yes
YesYes
No
No*
No
Admit patientto CCU
No
No
No
Is STEMI suspected?
Pt has symptoms and calls EMS
EMS does ECG
EMS notifies ED ofSTEMI, starts IV,
draws blood
Pt arrives in ED without
pre-hospital ECG
Cath lab staff &interventionalistarrive and scrub
within 30 minutes
Cath lab staff &interventionalistarrive and scrub
within 30 minutes
ED does ECGand gives it to ED physician in
10 minutes
Pt arrives at ED triage
ED calls operatorto page cath lab
staff & interventionalist
ED calls operatorto page cath lab
staff & interventionalist
ED initiates treatment and
consent for cath lab
ED transport patient tocath lab
Final check and written
consent completed
ED communicateswith cath labto determine readiness to
receive patient
Is there a pre-hospital
ECG indicatingSTEMI
Is STEMIconfirmed?
Are pagesconfirmed?
Is PCI indicated?
Startprocedure
Are pagesconfirmed?
Continue ED work-up andcancel cath lab, as needed
primary percutaneous coronary intervention 15
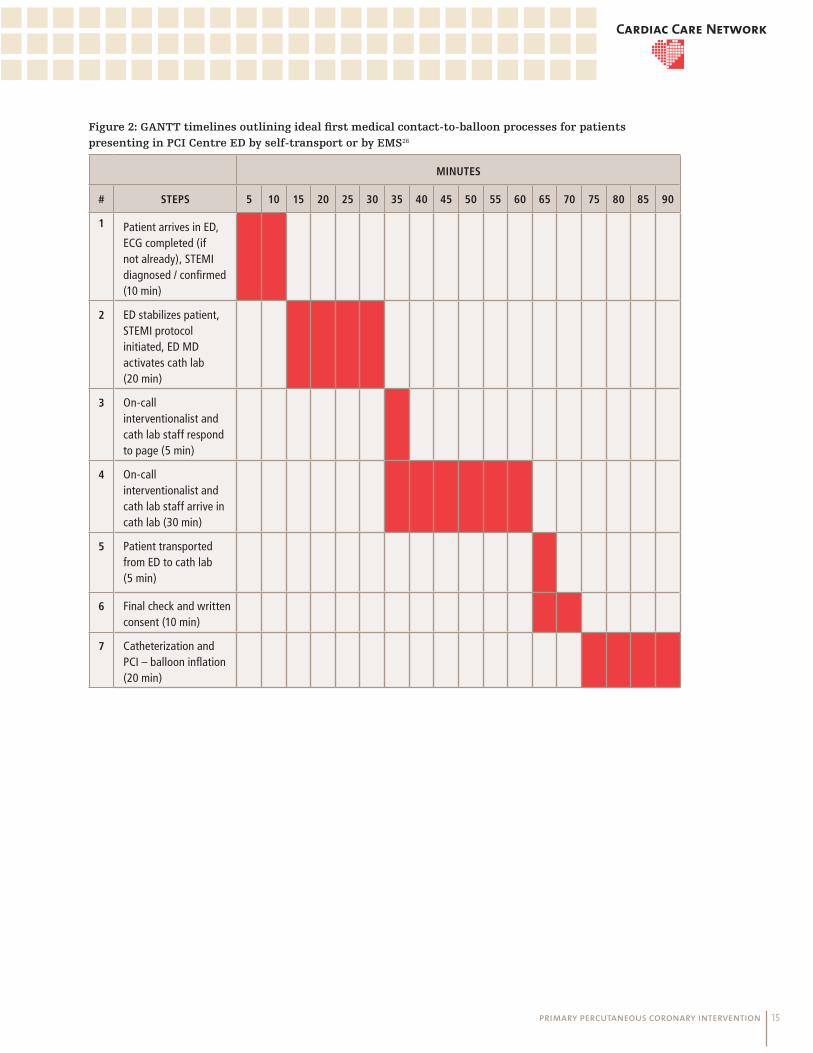
Figure 2: GANTT timelines outlining ideal fi rst medical contact-to-balloon processes for patients
presenting in PCI Centre ED by self-transport or by EMS26
MINUTES
# STEPS 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
1 Patient arrives in ED, ECG completed (if not already), STEMI diagnosed / confi rmed (10 min)
2 ED stabilizes patient, STEMI protocol initiated, ED MD activates cath lab (20 min)
3 On-call interventionalist and cath lab staff respond to page (5 min)
4 On-call interventionalist and cath lab staff arrive in cath lab (30 min)
5 Patient transported from ED to cath lab (5 min)
6 Final check and written consent (10 min)
7 Catheterization and PCI – balloon infl ation (20 min)
primary percutaneous coronary intervention 16
THE CHALLENGE: OVERCOMING BARRIERS TO ACCESS
While the evidence supports the superiority of pPCI as an intervention for STEMI, there are
a number of reasons why PCI programs may be reluctant or unable to completely adopt this
standard of care. While the concept of delivering pPCI services could appear to be simple
in principle to a non-clinician, the challenges in establishing this type of service have been
clearly articulated in the literature and are refl ected in the experiences of the PCI programs
in Ontario that have implemented fully integrated, regional pPCI programs. These challenges
have been categorized accordingly:
The need to rethink established processes;
Leadership and commitment to ensure success and optimal performance;
EMS and paramedic coordination at times requiring amendments to jurisdictional
agreements;
Human resources to ensure appropriate clinical coverage;
Hospital resources to ensure appropriate infrastructure;
Repatriation to accommodate early patient transfers and ensure cath lab availability;
Communication with all stakeholder groups (e.g., within hospital, inter-hospital, EMS).
The following section of this document reviews each of these areas in more detail and
presents strategies that have been successfully deployed to overcome these challenges,
utilizing lessons learned and tools as resources to support best practice for pPCI.
Engagement Processes: Rethinking Established ProcessesImplementation of regional, 24/7 pPCI service requires effective collaboration between
multiple stakeholders. PCI centres seeking to establish pPCI services are encouraged to
work with their regional planning authorities (for Ontario, this could be the Local Health
Integration Network) and other relevant clinical and administrative stakeholders.

primary percutaneous coronary intervention 17
CHALLENGES STRATEGIES COMMENTS
Stakeholder Engagement Host pPCI workshop with teaching/orientation sessions for stakeholder
Ensure clearly defi ned objectives with explicit phased-in approach
Defi ne scope for the intended services
Review of the evidence, data collection and relevant research
Include presentations by clinical and administrative experts from existing pPCI centres
Develop business case, inclusive of all stakeholders
Form a steering committee comprised of key stakeholders (e.g., EMS, ED, administration, cath lab and CCU)
Ensure high level of stakeholder involvement at every level: cath lab, emergency department, inpatient clinical units, Emergency Medical Services, pharmacy, administration, nursing, regional and union stakeholders
Build enthusiasm for the initiative: Regular pPCI meetings with stakeholders, including monthly, to review progress (ED/cath lab and EMS)
Ensure commitment of referring community: Initial meetings with referring community cardiologist/internal medicine, emergency departments, EMS to educate
Provide ongoing education: Education days with emergency department, coronary care unit staff, cath lab staff and Emergency Medical Services to foster collaborative efforts and spirit
Share data with relevant stakeholders: Leverage data to assess progress, drive decision making, discussion evaluation, and quality improvement
Provide information back to stakeholders as soon as possible: Early dissemination of D2B and initially D2N times to chart progress with clearly identifi ed targets and goals
Establish effective communication system as feedback mechanism
Secure commitment and “buy-in” from hospital administration at PCI and non-PCI hospitals
Business Model Develop business case that has clearly defi ned:
Purpose
Implementation model
Benefi ts
Costs
Return on investment
Risks
Specify the type of pPCI implementation model in the scope of the project e.g.:
– Within own hospital – Transfer from non-PCI hospital – Direct transfer from fi eld
Business case must be system-focused and address issues such as:
Quality outcomes for patients/patient centred care
Transfer protocols
Repatriation agreements between hospitals
Information technologies to be leveraged e.g. ECG machines for EMS or BlackBerries for ECG transmission from the fi eld and code STEMI team
Staffi ng models
(continues on next page)

primary percutaneous coronary intervention 18
CHALLENGES STRATEGIES COMMENTS
Project Management Identify project champions (e.g. steering committee members)
Identify project leadership and project execution team
Ensure specifi c project resourcing and budget allocation
Have clearly defi ned timelines and deliverables for implementation
Ensure regular case review to track early performance
Confi rming formal project management and coordination roles is benefi cial to support implementation – identify key physician and administrative leads
Using a project charter endorsed by key stakeholders with executive sponsorship helps to support roll-out strategy
Deploy a clearly defi ned communication plan during implementation to raise awareness, interest and momentum
Step-wise implementation helps to ensure successful deployment of strategy
Keep clinical protocols as simple as possible
Conduct mock Code STEMI scenarios with simulated situations to:
– Assess ECG interpretation skills by EMS
– Test process fl ows and protocols
– Assess staff response times
– Estimate time required to get patient to cath lab
– Determine impact on regular cath lab activity
Use established project management tools: – “To do” checklists
– Accountability/responsibility matrix
– Process fl ow maps/diagrams
Use of a risk management tool – Track all potential risks and mitigation
strategies throughout the life of the project
– Include potential and real risks involving all stakeholder interests
(continued from previous page)
primary percutaneous coronary intervention 19
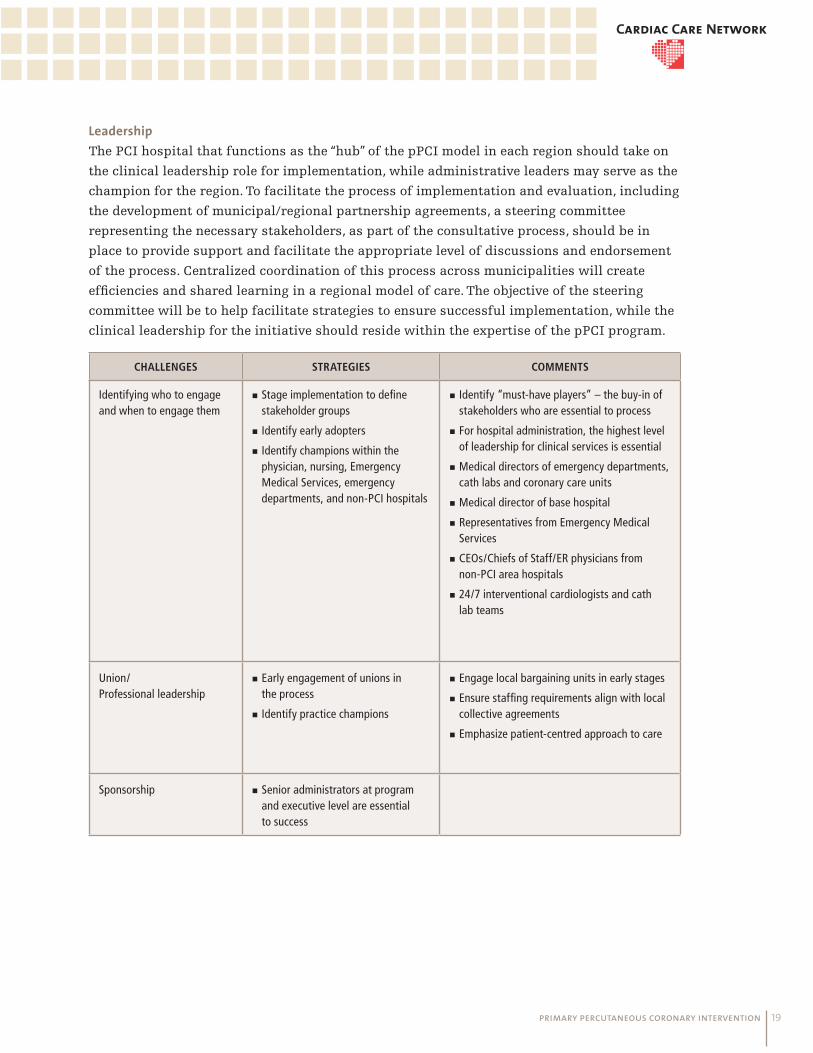
LeadershipThe PCI hospital that functions as the “hub” of the pPCI model in each region should take on
the clinical leadership role for implementation, while administrative leaders may serve as the
champion for the region. To facilitate the process of implementation and evaluation, including
the development of municipal/regional partnership agreements, a steering committee
representing the necessary stakeholders, as part of the consultative process, should be in
place to provide support and facilitate the appropriate level of discussions and endorsement
of the process. Centralized coordination of this process across municipalities will create
effi ciencies and shared learning in a regional model of care. The objective of the steering
committee will be to help facilitate strategies to ensure successful implementation, while the
clinical leadership for the initiative should reside within the expertise of the pPCI program.
CHALLENGES STRATEGIES COMMENTS
Identifying who to engage and when to engage them
Stage implementation to defi ne stakeholder groups
Identify early adopters
Identify champions within the physician, nursing, Emergency Medical Services, emergency departments, and non-PCI hospitals
Identify “must-have players” – the buy-in of stakeholders who are essential to process
For hospital administration, the highest level of leadership for clinical services is essential
Medical directors of emergency departments, cath labs and coronary care units
Medical director of base hospital
Representatives from Emergency Medical Services
CEOs/Chiefs of Staff/ER physicians from non-PCI area hospitals
24/7 interventional cardiologists and cath lab teams
Union/ Professional leadership
Early engagement of unions in the process
Identify practice champions
Engage local bargaining units in early stages
Ensure staffi ng requirements align with local collective agreements
Emphasize patient-centred approach to care
Sponsorship Senior administrators at program and executive level are essential to success
primary percutaneous coronary intervention 20
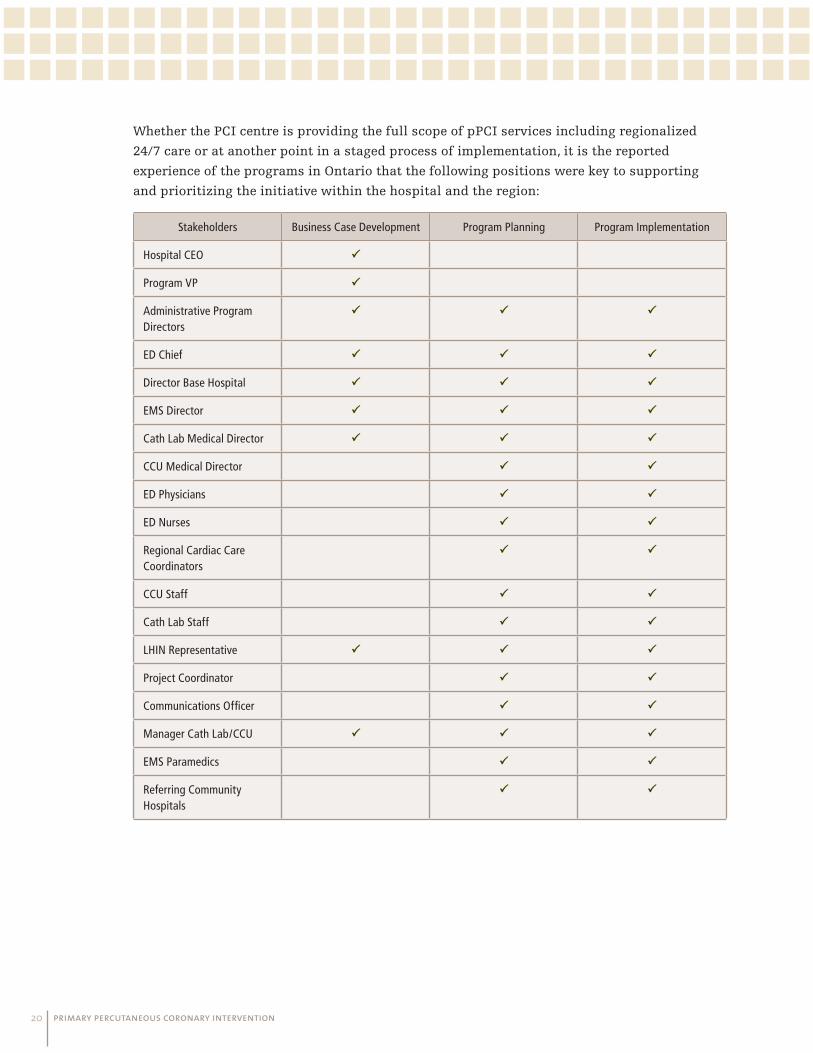
Whether the PCI centre is providing the full scope of pPCI services including regionalized
24/7 care or at another point in a staged process of implementation, it is the reported
experience of the programs in Ontario that the following positions were key to supporting
and prioritizing the initiative within the hospital and the region:
Stakeholders Business Case Development Program Planning Program Implementation
Hospital CEO
Program VP
Administrative Program Directors
ED Chief
Director Base Hospital
EMS Director
Cath Lab Medical Director
CCU Medical Director
ED Physicians
ED Nurses
Regional Cardiac Care Coordinators
CCU Staff
Cath Lab Staff
LHIN Representative
Project Coordinator
Communications Offi cer
Manager Cath Lab/CCU
EMS Paramedics
Referring Community Hospitals

primary percutaneous coronary intervention 21
Emergency Medical Systems and Paramedic ServicesInvolving the Emergency Medical Services (EMS) administrators and paramedic services
early in the planning process was identifi ed as a key requirement to successfully establish
a regional pPCI program. Communication is essential to understand the following:
Local and regional EMS paramedic levels of service;
Paramedic training and skills;
Availability of equipment and support;
Human resources considerations;
Jurisdictional boundaries and regulations; and
Logistics, including dispatch and transportation.
The EMS/ambulance services in Ontario are Upper-Tier Municipality (UTM) based. Thus,
decisions pertaining to the level of service and the majority of funding are from the UTM;
however, the Emergency Health Services Branch of the Ministry of Health and Long-Term
Care (MOHLTC) regulates, accredits, and allocates some of the funding for EMS. One of the
challenges of developing a regional strategy is in part because the UTM boundaries do not
completely align with the LHIN boundaries and are not specifi cally included within the
scope or mandate of the LHIN. Consequently, EMS structures and roles may not be viewed
within the context of a LHIN-wide or regional initiative except through program-specifi c
engagement. Therefore, a critical component of developing a regionalized pPCI program is the
engagement of EMS to ensure the rapid and reliable transport of patients to a pPCI centre.
Overlapping EMS jurisdictions, and balancing the requirements of a STEMI program with
other program obligations and priorities, may require signifi cant dialogue to negotiate service
level requirements and agreements.
In planning for pPCI services, a critical factor is the STEMI patient’s location and proximity
to the nearest PCI hospital, which may or may not align with the LHIN boundaries. The
Ontario Local Health System Integration Act (2006) prohibits LHINs from entering into any
agreement or other arrangement that restricts or prevents an individual from receiving
services based on the geographical area in which the individual resides.
CHALLENGES STRATEGIES COMMENTS
Models for pre-hospital 12-lead ECG interpretation
Equipment
Paramedic
Training
ECG transmission (if required)
Ensure rapid transfer protocols regardless of model
Paramedics with the appropriate training can successfully interpret ECGs (either through transmitted ECG or read in fi eld) to identify STEMI patients in the fi eld and through established protocols execute decision to transport patient direct to pPCI centre
(continues on next page)
primary percutaneous coronary intervention 22
CHALLENGES STRATEGIES COMMENTS
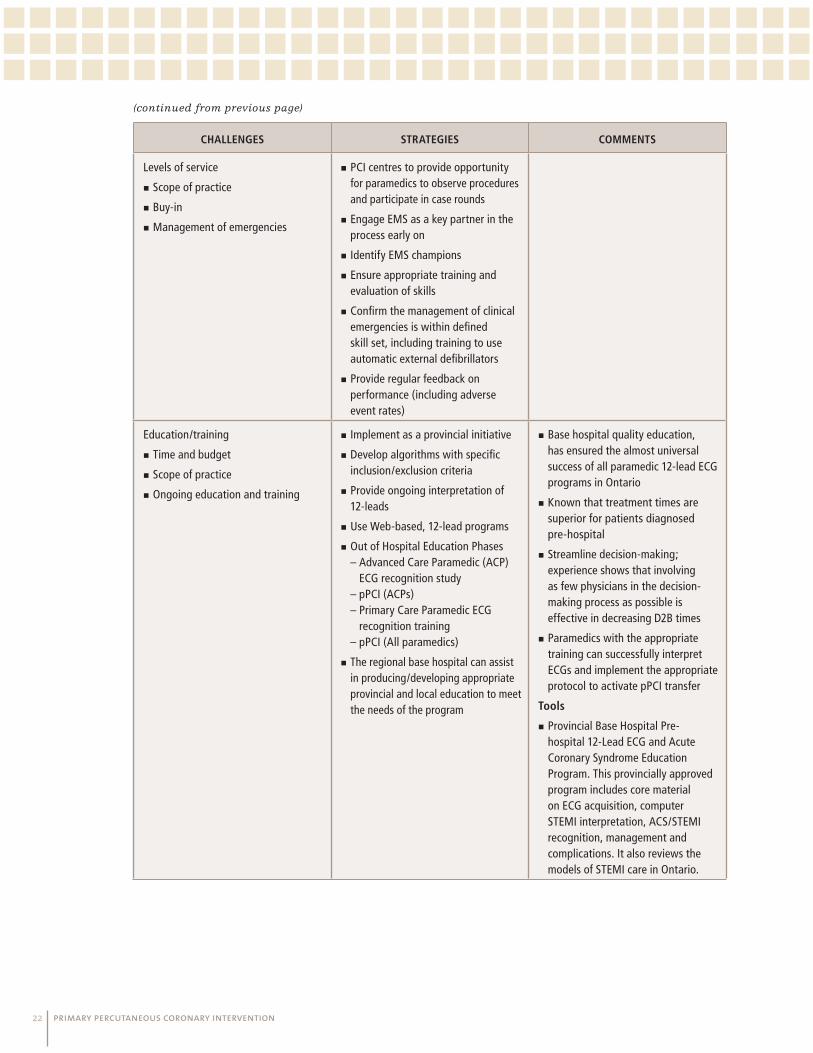
Levels of service
Scope of practice
Buy-in
Management of emergencies
PCI centres to provide opportunity for paramedics to observe procedures and participate in case rounds
Engage EMS as a key partner in the process early on
Identify EMS champions
Ensure appropriate training and evaluation of skills
Confi rm the management of clinical emergencies is within defi ned skill set, including training to use automatic external defi brillators
Provide regular feedback on performance (including adverse event rates)
Education/training
Time and budget
Scope of practice
Ongoing education and training
Implement as a provincial initiative
Develop algorithms with specifi c inclusion/exclusion criteria
Provide ongoing interpretation of 12-leads
Use Web-based, 12-lead programs
Out of Hospital Education Phases – Advanced Care Paramedic (ACP)
ECG recognition study – pPCI (ACPs) – Primary Care Paramedic ECG
recognition training – pPCI (All paramedics)
The regional base hospital can assist in producing/developing appropriate provincial and local education to meet the needs of the program
Base hospital quality education, has ensured the almost universal success of all paramedic 12-lead ECG programs in Ontario
Known that treatment times are superior for patients diagnosed pre-hospital
Streamline decision-making; experience shows that involving as few physicians in the decision-making process as possible is effective in decreasing D2B times
Paramedics with the appropriate training can successfully interpret ECGs and implement the appropriate protocol to activate pPCI transfer
Tools
Provincial Base Hospital Pre-hospital 12-Lead ECG and Acute Coronary Syndrome Education Program. This provincially approved program includes core material on ECG acquisition, computer STEMI interpretation, ACS/STEMI recognition, management and complications. It also reviews the models of STEMI care in Ontario.
(continued from previous page)

primary percutaneous coronary intervention 23
CHALLENGES STRATEGIES COMMENTS
Equipment
Education
Funding
12-lead machines are not mandatory equipment for EMS services,
Need to consider ECG machine availability and identify options for funding/implementation
Human Resources
Compensation
Advanced skills
Implications for practice
Identify champions for PCP and ACP
Identify more than a transport team
Recognize advanced level of professional practice and contributions to decreasing mortality and morbidity of AMI
Ensure appropriate training
Recognize that false positive interpretation may be a learning opportunity
Ensure regular review to assess any missed calls (e.g., false negative interpretations)
Start with ECG interpretation and graduate to decision-making
Perform mock Code STEMI scenarios to practice protocol deployment
Skill Set Summary for Primary Care Paramedic, Advanced Care Paramedic, and Critical Care Paramedic
Transportation
Transport of STEMI patient to pPCI centre
Create STEMI transport kit
Ensure prioritization of patients as identifi ed (patients are triaged when ambulance is called) and availability of staff
Develop dispatch algorithms
Integrate with other protocols for other initiatives (stoke, trauma)
Collect data on STEMI patients and outcomes, successes and local challenges
Practice runs
Where possible, start with late-presenters to minimize impact of any potential treatment delays related to transfers
Bypass protocols
Deplete local resources
Not within the Ambulance Act
Change in communications protocol
Requires dispatch support
Ensure hospital-specifi c approvals
Develop as part of base hospital initiative
Cite trauma/stroke protocols
Create alternate dispatch algorithms
(continued from previous page)
primary percutaneous coronary intervention 24
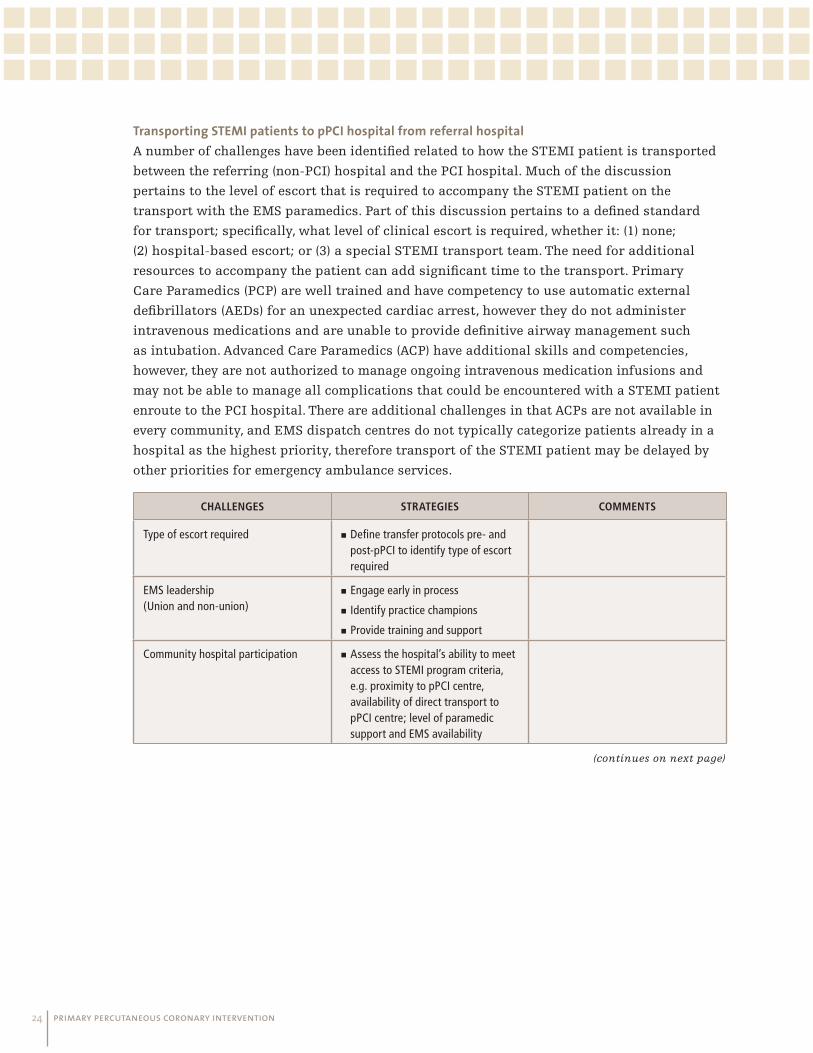
Transporting STEMI patients to pPCI hospital from referral hospitalA number of challenges have been identifi ed related to how the STEMI patient is transported
between the referring (non-PCI) hospital and the PCI hospital. Much of the discussion
pertains to the level of escort that is required to accompany the STEMI patient on the
transport with the EMS paramedics. Part of this discussion pertains to a defi ned standard
for transport; specifi cally, what level of clinical escort is required, whether it: (1) none;
(2) hospital-based escort; or (3) a special STEMI transport team. The need for additional
resources to accompany the patient can add signifi cant time to the transport. Primary
Care Paramedics (PCP) are well trained and have competency to use automatic external
defi brillators (AEDs) for an unexpected cardiac arrest, however they do not administer
intravenous medications and are unable to provide defi nitive airway management such
as intubation. Advanced Care Paramedics (ACP) have additional skills and competencies,
however, they are not authorized to manage ongoing intravenous medication infusions and
may not be able to manage all complications that could be encountered with a STEMI patient
enroute to the PCI hospital. There are additional challenges in that ACPs are not available in
every community, and EMS dispatch centres do not typically categorize patients already in a
hospital as the highest priority, therefore transport of the STEMI patient may be delayed by
other priorities for emergency ambulance services.
CHALLENGES STRATEGIES COMMENTS
Type of escort required Defi ne transfer protocols pre- and post-pPCI to identify type of escort required
EMS leadership (Union and non-union)
Engage early in process
Identify practice champions
Provide training and support
Community hospital participation Assess the hospital’s ability to meet access to STEMI program criteria, e.g. proximity to pPCI centre, availability of direct transport to pPCI centre; level of paramedic support and EMS availability
(continues on next page)

primary percutaneous coronary intervention 25
CHALLENGES STRATEGIES COMMENTS
Availability of EMS transport back to referring hospital recognizing that multiple municipalities may have the jurisdiction to manage the EMS resources
Engage EMS in early phases – including all relevant municipalities if there are multiple service providers within the LHIN
Provide training to EMS paramedics to identify STEMI at point of care (12-lead ECG)
Ensure repatriation is not linked to an in-patient bed but rather based on the agreement from ED physicians to repatriate patient back to referring hospitals post-pPCI (this requires the ED of referring hospital to manage bed requirements as they would for any patient in their ED through their usual processes)
Hold annual updates and CEU hours for EMS personnel and ED physicians and staff from referring hospitals
Deploy a “No Refusal” policy to accept STEMI patient for pPCI despite bed status – if necessary, patients can be maintained in short stay/recovery area overnight or CCU procedure room
Provide opportunities for EMS to be part of the Code STEMI team in cath lab environment
High level of engagement can stimulate interest and priority to augment EMS resources, including equipment/training
Human ResourcesThe availability of human resources impacts all components of pPCI services, given the
requirement to have highly skilled and experienced health care professionals available to
provide care in an acute setting. Additional considerations may be required with respect
to collective agreements, including the rostering and remuneration of staff. Employers
working with local bargaining units will need to address the overall operational needs
of the hospital, including staffi ng the pPCI program, taking into account the dynamics
between the employer and the respective collective agreements. Creative scheduling and
overlapping shifts and coverage may help to meet staffi ng requirements and obviate the
need for overtime.
(continues on next page)
(continued from previous page)

primary percutaneous coronary intervention 26
CHALLENGES STRATEGIES COMMENTS
Number of staff required Ensure appropriate number of staff for the volume of cases completed
Provide training programs to support skills development and cross training (as permitted by professional scope of practice and employment agreements)
Skill and experience Ensure appropriate skills are available, including physicians, nurses, technicians
Scheduling and on-call Creative shift schedules
Extended shifts/on-call services
Availability Car pooling
Buddy system
On-site staff support (e.g., CCU nurse designated to assist with all STEMI)
On-call demands with smaller staff volumes create challenges and can be disruptive to support regularly scheduled cases (e.g., as per collective agreements, staff may be in a position to decline to work next day if called in for emergency pPCI for STEMI during the night)
Implement a one-call number with a designated pager carried by interventional cardiologist on call
Require an immediate response to page and system activation to alert other members of the cath lab team
Test paging system extensively prior to go-live to ensure functional system in place prior to pPCI program implementation
Debrief post-pPCI to determine quality improvement opportunities
Develop system of direct admission to cath lab, bypassing ED
Ensure continued engagement of front-line staff
Review collective agreements
Assess human resource impacts (including staff fatigue/burn out)
Call-back costs can be greater than anticipated – need to consider modifi ed shifts and/or scheduling to meet needs of 24/7 program
Need to identify who is absolutely required for case by call-back, and leverage other hospital staff as resources to support the pPCI care (e.g., nurses from other areas like CCU, emergency, recovery, ICU, etc.)
Ensure data collection to monitor performance, outcomes and trend activity
ED staff can be great champions for direct admission as it helps to ease ER pressures
Help to support presentations by front-line staff (nursing rounds, conferences, etc.)
Post performance times/outcomes with targets to achieve continued success
Be prepared for rapid growth in response to system successes

primary percutaneous coronary intervention 27
Hospital Resources It is important to emphasize that a critical success factor of a pPCI program is the acceptance
of patients for pPCI without being contingent on bed availability. Typically, hospitals are
maintained above occupancy, and rarely is there a physical bed that is open and unoccupied.
Therefore, it is essential to de-link the pPCI patient from the requirement for a CCU bed,
recognizing that there are options available for the patient post-procedure, including care in
other areas of the hospital. In some cases, it may be possible to directly repatriate the patient
back to the non-PCI referring hospital. Requiring pPCI services to be contingent on other
levels of physician acceptance and/or bed availability will result in unnecessary delays to the
patient and will directly impact the D2B times, resulting in excessive treatment times beyond
the targets established for optimal care.
With the exception of very extraordinary circumstances, it is impractical that paramedics
would be required to delay transportation of an acute STEMI patient while awaiting a
decision for the patient to be accepted for pPCI. Eliminating unnecessary and complicated
communication protocols and the implementation of a one-call system will expedite the
transfer process. Successful regional pPCI programs have implemented very simple systems
to alert the pPCI cath lab of a patient in the fi eld or non-PCI hospital referring a STEMI
patient for pPCI.
RepatriationTimely repatriation of the patient back to the referring hospital is also an important success
factor. With successful procedural outcomes, the STEMI patient can be transferred back
to the referring hospital post-pPCI for any additional monitoring that may be required.
Following the successful procedure, a priority for the pPCI program should be to ensure the
availability of pPCI services for the next patient. Therefore, following successful intervention,
stable patients who are free of clinical complications should be considered for transfer and
repatriation back to the referring hospital as soon as possible. Typically, the transfer back
can occur between 8 to 24 hours following the procedure, and in some cases even earlier. Just
as a streamlined referral process expedites the transport of the patient to the pPCI hospital,
a similar level of communication to expedite the repatriation of the stable patient back to
referring hospital post-procedure is required to ensure appropriate patient fl ow. This can be
accommodated by the referring hospital maintaining a bed for the arrival of the patient or
being willing to accept the patient back via the emergency room post-pPCI. It is important to
note that an early repatriation strategy is appropriate for stable patients only; patients who
develop complications or require additional interventions should remain at the PCI hospital,
with transfer back to the referring hospital arranged when the patient is clinically stable and
does not require further intervention.
primary percutaneous coronary intervention 28
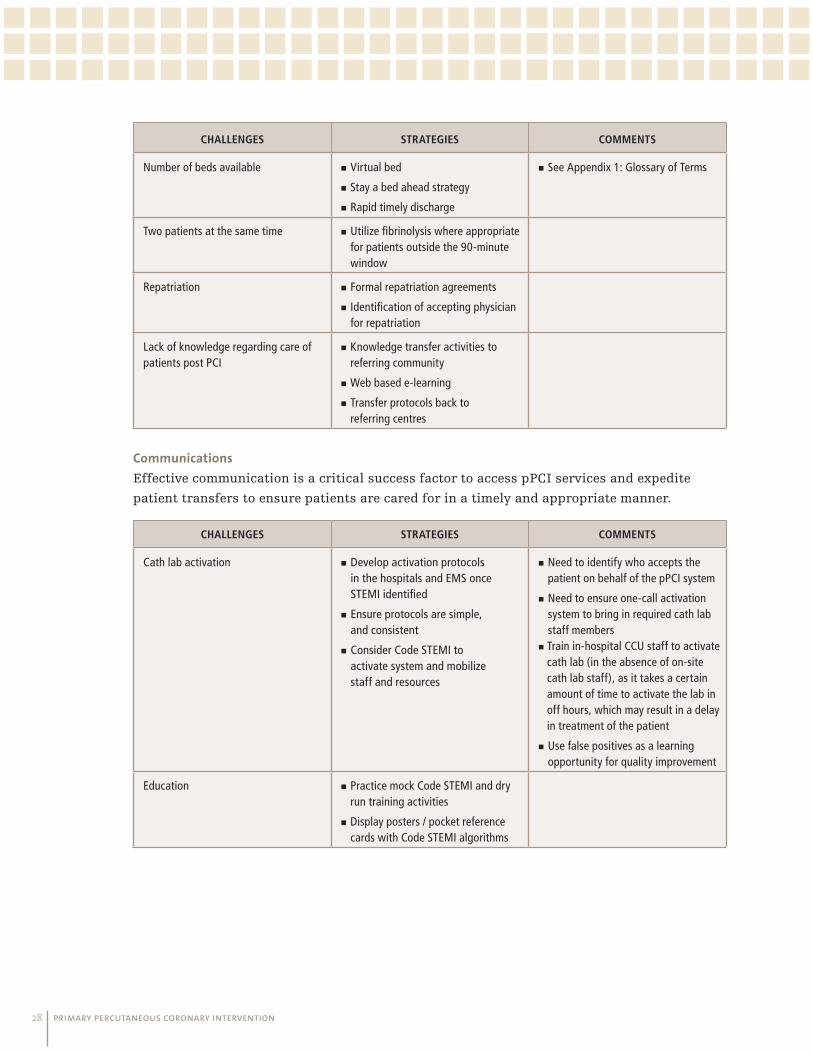
CHALLENGES STRATEGIES COMMENTS
Number of beds available Virtual bed
Stay a bed ahead strategy
Rapid timely discharge
See Appendix 1: Glossary of Terms
Two patients at the same time Utilize fi brinolysis where appropriate for patients outside the 90-minute window
Repatriation Formal repatriation agreements
Identifi cation of accepting physician for repatriation
Lack of knowledge regarding care of patients post PCI
Knowledge transfer activities to referring community
Web based e-learning
Transfer protocols back to referring centres
Communications Effective communication is a critical success factor to access pPCI services and expedite
patient transfers to ensure patients are cared for in a timely and appropriate manner.
CHALLENGES STRATEGIES COMMENTS
Cath lab activation Develop activation protocols in the hospitals and EMS once STEMI identifi ed
Ensure protocols are simple, and consistent
Consider Code STEMI to activate system and mobilize staff and resources
Need to identify who accepts the patient on behalf of the pPCI system
Need to ensure one-call activation system to bring in required cath lab staff members
Train in-hospital CCU staff to activate cath lab (in the absence of on-site cath lab staff), as it takes a certain amount of time to activate the lab in off hours, which may result in a delay in treatment of the patient
Use false positives as a learning opportunity for quality improvement
Education Practice mock Code STEMI and dry run training activities
Display posters / pocket reference cards with Code STEMI algorithms

primary percutaneous coronary intervention 29
Future DirectionThe purpose of this document is to provide information and a vehicle for knowledge transfer
to assist hospitals and health care providers in planning for pPCI as a key treatment for
STEMI across the province. In addition, this document can serve as a resource to hospital
administrators and LHINs in planning health services delivery at a regional level. As part of
the CCN efforts to support leading practices and quality improvement, this document outlines
strategies that have been effective to successfully implement a successful pPCI program, and
shares some of the lessons learned and critical steps in implementing a successful program.
To support this document as a knowledge translation tool, the pPCI-SC recommends the
following next steps:
Develop a pPCI mentorship program aligned with the MOHLTC Coaching Team Model;
Develop strategies to raise LHIN education and awareness;
Develop strategies to raise hospital education and awareness and support pPCI best
practices and performance;
Include information of relevant performance metrics (including D2B times) in CCN
Hospital Reports;
Recommend inclusion of D2B times as a performance indicator for the LHIN and hospital
accountability agreements.

primary percutaneous coronary intervention 30
References1. Krumholz, H.M., Anderson, J.L., Brooks, N.H., Fesmire, F.M., Lambrew, C.T., Landrum,
M.B., Weaver, W.D., Whyte, J. ACC/AHA Clinical Performance Measures for Adults With ST
Elevation and Non–ST Elevation Myocardial Infarction. J Am Coll Cardiol, 2006: 47: 236-
265, doi:10.1016/j.jacc.2005.10.020. pages 236-65
2. Keeley, E.C., Boura, J.A., Grines, C.L. Primary angioplasty versus intravenous thrombolytic
therapy for acute myocardial infarction: a quantitative review of 23 randomized trials.
Lancet 2003: 361:13-20
3. Keeley, E.C., Boura, J.A., Grines, C.L. Primary angioplasty versus intravenous thrombolytic
therapy for acute myocardial infarction: a quantitative review of 23 randomized trials.
Lancet 2003: 361:13-20
4. Nielsen P.H., Maeng M., Busk M., Mortensen L.S., Kristensen S.D., Nielsen T.T., Andersen
H.R. DANAMI-2 Investigators. Circulation. 2010 Apr 6: 121(13):1484-91. Epub 2010 Mar 22.
5. Labinaz, M., Swabey, T., Watson, R., Natarajan, M., Fucile, W., Lubelsky, B., Sawadsky, B.,
Cohen, E., Glasgow, K. CCN Consensus Panel on Access to Urgent PCI for ST Segment
Elevation Myocardial Infarction. Delivery of primary percutaneous coronary intervention
for the management of acute ST segment elevation myocardial infarction: summary of the
Cardiac Care Network of Ontario Consensus Report. Can J Cardio 2006: 22(3):243-50
6. Antman, E.M., Hand, M., Armstrong, P.W., Bates, E.R., Green, L.A., Halasyamani, L.K.,
Hochman, J.S., Krumholz, H.M., Lamas, G.A., Mullany, C.J., Pearle, D.L., Sloan, M.A., Smith,
S.C. Jr., Anbe, D.T., Kushner, F.G., Ornato, J.P., Pearle, D.L., Sloan, M.A., Jacobs, A.K., Adams
C.D., Anderson, J.L., Buller, C.E., Creager, M.A., Ettinger, S.M., Halperin, J.L., Hunt, S.A.,
Lytle, B.W., Nishimura, R., Page, R.L., Riegel, B., Tarkington, L.G., Yancy, C.W. 2007 focused
update of the ACC/AHA 2004 guidelines for the management of patients with ST elevation
myocardial infarction: a report of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines. J Am Coll of Card 2008: 51(2):210-47
7. Nallamothu, B.K., Bates, E.R. Percutaneous coronary intervention versus fi brinolytic
therapy in acute myocardial infarction: is timing (almost) everything? Am J Cardiol 2003:
92(7):824-6
8. Pinto, D.S., Kirtane, A.J., Nallamothu, B.K., Murphy, S.A., Cohen, D.J., Laham, R.J., Cutlip,
D.E., Bates, E.R., Frederick, P.D., Miller, D.P., Carrozza, J.P. Jr., Antman, E.M., Cannon,
C.P., Gibson, C.M. Hospital delays in reperfusion for ST elevation myocardial infarction:
implications when selecting a reperfusion strategy. Circulation 2006: 114(19):2019-25

primary percutaneous coronary intervention 31
9. Cantor, W.J., Fitchett, D., Borgundvaag, B., Heffernan, M., Cohen, E.A., Morrison, L.J.,
Ducas, J., Langer, A., Mehta, S., Lazzam, C., Schwartz, B., Dzavik, V., Casanova, A., Singh,
P., Goodman, S.G., for the TRANSFER-AMI Investigators. Trial of Routine Angioplasty
and Stenting After Fibrinolysis to Enhance Reperfusion in Acute Myocardial Infarction
(TRANSFER-AMI). SCAI Annual Scientifi c Sessions in partnership with ACC i2 summit.
Late Breaking Clinical Trials II: Acute Myocardial Infarction Presentation Number 2404-
9. March 30-April 1, 2008 Chicago
10. Bradley, E.H., Herrin, J.. Wang, Y., Barton, B.A., Webster, T.R., Mattera, J.A., Roumanis,
S.A., Curtis, J.P., Nallamothu, B.K., Magid, D.J., McNamara, R.L., Parkosewich, J., Loeb,
J.M., Krumholz, H.M. Strategies for reducing the door-to-balloon time in acute myocardial
infarction. N Engl J Med 2006: 355(22):2308-20
11. Krumholz, H.M., Bradley, E.H., Nallamothu, B.K., Ting, H.H., Batchelor, W.B., Kline-Rogers,
E., Stern, A.F., Byrd, J.R., Brush, J.E. A campaign to improve the timeliness of primary
percutaneous coronary intervention. Door-to-balloon: An alliance for quality. J Am Coll
Cardiol Intv 2008: 1:97-104
12. Ting, H.H., Rihal, C.S., Gersh, B.J., Haro, L.H., Bjerke, C.M., Lennon, R.J., Lim, C.C.,
Bresnahan, J.F., Jaffe, A.S., Holmes, D.R., Bell, M.R. Regional systems of care to optimize
timeliness of reperfusion therapy for ST elevation myocardial infarction: the Mayo Clinic
STEMI Protocol. Circulation 2007: 116(7):729-36
13. Jollis, J.G., Roettig, M.L., Aluko, A.O., Anstrom, K.J., Applegate, R.J., Babb, J.D., Berger,
P.B., Bohle, D.J., Fletcher, S.M., Garvey, J.L., Hathaway, W.R., Hoekstra, J.W., Kelly, R.V.,
Maddox, W.T. Jr., Shiber, J.R., Valeri, F.S., Watling, B.A., Wilson, B.H., Granger, C.B.
Reperfusion of Acute Myocardial Infarction in North Carolina Emergency Departments
(RACE) Investigators. Implementation of a statewide system for coronary reperfusion for
ST segment elevation myocardial infarction. JAMA 2007: 298(20):2371-80
14. Henry, T.D., Sharkey, S.W., Burke, M.N., Chavez, I.J., Graham, K.J., Henry, C.R., Lips, D.L.,
Madison, J.D., Menssen, K.M., Mooney, M.R., Newell, M.C., Pedersen, W.R., Poulose, A.K.,
Traverse, J.H., Unger, B.T., Wang, Y.L., Larson, D.M. A regional system to provide timely
access to percutaneous coronary intervention for ST elevation myocardial infarction.
Circulation 2007: 116(7):721-8
15. Labinaz, M., Swabey, T., Watson, R., Natarajan, M., Fucile, W., Lubelsky, B., Sawadsky, B.,
Cohen, E., Glasgow, K. CCN Consensus Panel on Access to Urgent PCI for ST Segment
Elevation Myocardial Infarction. Delivery of primary percutaneous coronary intervention
for the management of acute ST segment elevation myocardial infarction: summary of the
Cardiac Care Network of Ontario Consensus Report. Can J Cardio 2006: 22(3):243-50

primary percutaneous coronary intervention 32
16. de Villiers, J.S., Anderson, T., McMeekin, J.D., Leung, R.C., Traboulsi, M. Foothills
Interventional Cardiology Service. Calgary STEMI QIHI group. Expedited transfer
for primary percutaneous coronary intervention: a program evaluation. CMAJ 2007:
176(13):1833-8
17. Le May, M.R., So, D.Y., Dionne, R., Glover, C.A., Froeschl, M.P.V., Wells, G.A., Davies, R.F.,
Sherrard, H.L., Maloney, J., Marquis, J.F., O’Brien, E.R., Trickett, J., Poirier, P., Ryan, S.C.,
Ha, A., Joseph, P.G., and Labinaz, M. A City-wide Protocol for Primary PCI in ST Segment
Elevation Myocardial Infarction. N Engl J Med 2008: 358(3):231-40
18. Bradley, E.H., Herrin, J., Wang, Y., Barton, B.A., Webster, T.R., Mattera, J.A., Roumanis,
S.A., Curtis, J.P., Nallamothu, B.K., Magid, D.J., McNamara, R.L., Parkosewich, J., Loeb,
J.M., Krumholz, H.M. Strategies for reducing the door-to-balloon time in acute myocardial
infarction. N Engl J Med 2006: 355(22):2308-20
19. Krumholz, H.M., Bradley, E.H., Nallamothu, B.K., Ting, H.H., Batchelor, W.B., Kline-Rogers,
E., Stern, A.F., Byrd, J.R., Brush, J.E. A campaign to improve the timeliness of primary
percutaneous coronary intervention. Door-to-balloon: An alliance for quality. J Am Coll
Cardiol Intv 2008: 1:97-104
20. Primary angioplasty for the treatment of ST segment elevated myocardial infarction.
Health Technology Scientifi c Review. The MOHLTC. August 2004.
21. Le May, M.R., Davies, R.F., Labinaz, M., Sherrard, H., Marquis, J.F., Laramee, L.A., O’Brien,
E.R., Williams, W.L., Beanlands, R.S., Nichol, G., Higginson, L.A. Hospitalization costs of
primary stenting versus thrombolysis in acute myocardial infarction: cost analysis of the
Canadian STAT Study. Circulation 2003: 108(21):2624-30
22. Jolly, S.S., Yuan, F., Wang, S., Lamy, A., Welsford, M., Velianou, J., Teo, K., Natarajan, M.K.
Cost Effectiveness of primary percutaneous coronary intervention vs. fi brinolysis in
patients with ST elevation myocardial infarction – a contemporary experience in Canada.
Can J Card. 2008: 24 (Suppl SE):109
23. Patel, A.B., Tu, J.V., Waters, N.M., Ko, D.T., Eisenberg, M.J., Huynh, T., Rinfret, S., Knudtson,
M.L., Ghali, W.A. Access to primary percutaneous coronary intervention for ST segment
elevation myocardial infarction in Canada: a geographic analysis. Open Medicine Vol 4,
No 1 (2010). http://www.openmedicine.ca/article/viewArticle/302/298
24. Le May, M.R., So, D.Y., Dionne, R., Glover, C.A., Froeschl, M.P.V., Wells, G.A., Davies, R.F.,
Sherrard, H.L., Maloney, J., Marquis, J.F., O’Brien, E.R., Trickett, J., Poirier, P., Ryan, S.C.,
Ha, A., Joseph, P.G., and Labinaz, M. A City-wide Protocol for Primary PCI in ST Segment
Elevation Myocardial Infarction. N Engl J Med 2008: 358(3):231-40

primary percutaneous coronary intervention 33
25. Bradley, E.H., Roumanis, S.A., Radford, M.J., Webster, T.R., McNamara, R.L., Mattera,
J.A., Barton, B.A., Berg, D.N., Portnay, E.L., Moscovitz, H., Parkosewich, J., Holmboe,
E.S., Blaney, M., Krumholz, H.M. Achieving Door-to-Balloon Times That Meet Quality
Guidelines. How Do Successful Hospitals Do It? Journal of the American College of
Cardiology, Volume 46, Issue 7, Pages 1236-1241
26. Bradley, E.H., Roumanis, S.A., Radford, M.J., Webster, T.R., McNamara, R.L., Mattera,
J.A., Barton, B.A., Berg, D,N., Portnay, E.L., Moscovitz, H., Parkosewich, J., Holmboe,
E.S., Blaney, M., Krumholz, H.M. Achieving Door-to-Balloon Times That Meet Quality
Guidelines. How Do Successful Hospitals Do It? Journal of the American College of
Cardiology, Volume 46, Issue 7, Pages 1236-1241
27. Cardiac Care Network. Access to Urgent PCI for ST Segment Elevation Myocardial
Infarction. Final Report and Recommendations. April 30, 2004. Pages 13-17
28. Welsh, R.C., Travers, A., Huynh, T., Cantor, W.J. Canadian Cardiovascular Society Working
Group: Providing a perspective on the 2007 focused update of the American College of
Cardiology and American Heart Association 2004 guidelines for the management of ST
elevation myocardial infarction. Can J Cardiol Vol 25 No 1 2009: 13-48

primary percutaneous coronary intervention 34
BibliographyAntman, E.M., Hand, M., Armstrong, P.W., Bates, E.R., Green, L.A., Halasyamani, L.K.,
Hochman, J.S., Krumholz, H.M., Lamas, G.A., Mullany, C.J., Pearle, D.L., Sloan, M.A., Smith,
S.C. Jr., Anbe, D.T., Kushner, F.G., Ornato, J.P., Pearle, D.L., Sloan, M.A., Jacobs, A.K., Adams
C,D., Anderson, J.L., Buller, C.E., Creager, M.A., Ettinger, S.M., Halperin, J.L., Hunt, S.A., Lytle,
B.W., Nishimura, R., Page, R.L., Riegel, B., Tarkington, L.G., Yancy, C.W. 2007 focused update of
the ACC/AHA 2004 guidelines for the management of patients with ST elevation myocardial
infarction: a report of the American College of Cardiology/American Heart Association Task
Force on Practice Guidelines. J Am Coll of Card 2008: 51(2):210-47
Bradley, E.H., Herrin, J. Wang, Y., Barton, B.A., Webster, T.R., Mattera, J.A., Roumanis, S.A.,
Curtis, J.P., Nallamothu, B.K., Magid, D.J., McNamara, R.L., Parkosewich, J., Loeb, J.M.,
Krumholz, H.M. Strategies for reducing the door-to-balloon time in acute myocardial
infarction. N Engl J Med 2006: 355(22):2308-20
Bradley, E.H., Roumanis, S.A., Radford, M.J., Webster, T.R., McNamara, R.L., Mattera, J.A.
Barton, B.A., Berg, D.N., Portnay, E.L., Moscovitz, H., Parkosewich, J., Holmboe, E.S., Blaney,
M., Krumholz, H.M. Achieving Door-to-Balloon Times That Meet Quality Guidelines. How Do
Successful Hospitals Do It? J Am Coll Cardiol, 2005: 46:1236-1241
Cardiac Care Network. Access to Urgent PCI for ST Segment Elevation Myocardial Infarction.
Final Report and Recommendations. April 30, 2004. Pages 13-17
Cantor, W.J., Fitchett, D., Borgundvaag, B., Heffernan, M., Cohen, E.A., Morrison, L.J., Ducas,
J., Langer, A., Mehta, S., Lazzam, C., Schwartz, B., Dzavik, V., Casanova, A., Singh, P., Goodman,
S.G., for the TRANSFER-AMI Investigators. Trial of Routine Angioplasty and Stenting After
Fibrinolysis to Enhance Reperfusion in Acute Myocardial Infarction (TRANSFER-AMI). SCAI
Annual Scientifi c Sessions in partnership with ACC i2 summit. Late Breaking Clinical Trials II:
Acute Myocardial Infarction Presentation Number 2404-9. March 30-April 1, 2008 Chicago
de Villiers, J.S., Anderson, T., McMeekin, J.D., Leung, R.C., Traboulsi, M. Foothills
Interventional Cardiology Service. Calgary STEMI QIHI group. Expedited transfer for primary
percutaneous coronary intervention: a program evaluation. CMAJ 2007: 176(13):1833-8
Henry, T.D., Sharkey, S.W., Burke, M.N., Chavez, I.J., Graham, K.J., Henry, C.R., Lips, D.L.,
Madison, J.D., Menssen, K.M., Mooney, M.R., Newell, M.C., Pedersen, W.R., Poulose, A.K.,
Traverse, J.H., Unger, B.T., Wang, Y.L., Larson, D.M. A regional system to provide timely access
to percutaneous coronary intervention for ST elevation myocardial infarction. Circulation
2007: 116(7):721-8
primary percutaneous coronary intervention 35
Jollis, J.G., Roettig, M.L., Aluko, A.O., Anstrom, K.J., Applegate, R.J., Babb, J.D., Berger, P.B.,
Bohle, D.J., Fletcher, S.M., Garvey, J.L., Hathaway, W.R., Hoekstra, J.W., Kelly, R.V., Maddox,
W.T. Jr., Shiber, J.R., Valeri, F.S., Watling, B.A., Wilson, B.H., Granger, C.B. Reperfusion of
Acute Myocardial Infarction in North Carolina Emergency Departments (RACE) Investigators.
Implementation of a statewide system for coronary reperfusion for ST segment elevation
myocardial infarction. JAMA 2007: 298(20):2371-80
Jolly, S.S., Yuan, F., Wang, S., Lamy, A., Welsford, M., Velianou, J., Teo, K., Natarajan, M.K. Cost
Effectiveness of primary percutaneous coronary intervention vs. fi brinolysis in patients with
ST elevation myocardial infarction – a contemporary experience in Canada. Can J Card. 2008:
24 (Suppl SE):109
Keeley, E.C., Boura, J.A., Grines, C.L. Primary angioplasty versus intravenous thrombolytic
therapy for acute myocardial infarction: a quantitative review of 23 randomized trials. Lancet
2003: 361:13-20
Krumholz, H.M., Bradley, E.H., Nallamothu, B.K., Ting, H.H., Batchelor, W.B., Kline-Rogers,
E., Stern, A.F., Byrd, J.R., Brush, J.E. A campaign to improve the timeliness of primary
percutaneous coronary intervention. Door-to-balloon: An alliance for quality. J Am Coll
Cardiol Intv 2008: 1:97-104
Krumholz, H.M., Anderson, J.L., Brooks, N.H., Fesmire, F.M. Lambrew, C.T., Landrum,
M.B., Weaver, W.D., Whyte, J. ACC/AHA Clinical Performance Measures for Adults With ST
Elevation and Non–ST Elevation Myocardial Infarction. J Am Coll Cardiol, 2006: 47:236-265,
doi:10.1016/j.jacc.2005.10.020. pages 236-65
Labinaz, M., Swabey, T., Watson, R., Natarajan, M., Fucile, W., Lubelsky, B., Sawadsky, B.,
Cohen, E., Glasgow, K. CCN Consensus Panel on Access to Urgent PCI for ST Segment Elevation
Myocardial Infarction. Delivery of primary percutaneous coronary intervention for the
management of acute ST segment elevation myocardial infarction: summary of the Cardiac
Care Network of Ontario Consensus Report. Can J Cardio 2006: 22(3):243-50
Le May, M.R., Davies, R.F., Labinaz, M., Sherrard, H., Marquis, J.F., Laramee, L.A., O’Brien, E.R.,
Williams, W.L., Beanlands, R.S., Nichol, G., Higginson, L.A. Hospitalization costs of primary
stenting versus thrombolysis in acute myocardial infarction: cost analysis of the Canadian
STAT Study. Circulation 2003: 108(21):2624-30
Le May, M.R., So, D.Y., Dionne, R., Glover, C.A., Froeschl, M.P.V., Wells, G.A., Davies, R.F.,
Sherrard, H.L., Maloney, J., Marquis, J.F., O’Brien, E.R., Trickett, J., Poirier, P., Ryan, S.C., Ha, A.,
Joseph, P.G., and Labinaz, M. A City-wide Protocol for Primary PCI in ST Segment Elevation
Myocardial Infarction. N Engl J Med 2008: 358(3):231-40

primary percutaneous coronary intervention 36
Nallamothu, B.K., Bates, E.R. Percutaneous coronary intervention versus fi brinolytic therapy
in acute myocardial infarction: is timing (almost) everything? Am J Cardiol 2003: 92(7):824-6
Nielsen, P.H., Maeng, M., Busk, M., Mortensen, L.S., Kristensen, S.D., Nielsen, T.T., Andersen,
H.R. DANAMI-2 Investigators. Circulation. 2010 Apr 6: 1 21(13):1484-91. Epub 2010 Mar 22.
Patel, A.B., Tu, J.V., Waters, N.M., Ko, D.T., Eisenberg, M.J., Huynh, T., Rinfret, S., Knudtson,
M.L., Ghali, W.A. Access to primary percutaneous coronary intervention for ST segment
elevation myocardial infarction in Canada: a geographic analysis. Open Medicine Vol 4, No 1
(2010). http://www.openmedicine.ca/article/viewArticle/302/298
Pinto, D.S., Kirtane, A.J., Nallamothu, B.K., Murphy, S.A., Cohen, D.J., Laham, R.J., Cutlip, D.E.,
Bates, E.R., Frederick, P.D., Miller, D.P., Carrozza, J.P. Jr., Antman, E.M., Cannon, C.P., Gibson,
C.M. Hospital delays in reperfusion for ST elevation myocardial infarction: implications when
selecting a reperfusion strategy. Circulation 2006: 114(19):2019-25
Primary angioplasty for the treatment of ST segment elevated myocardial infarction. Health
Technology Scientifi c Review. The MOHLTC. August 2004.
Ting, H.H., Rihal, C.S., Gersh, B.J., Haro, L.H., Bjerke, C.M., Lennon, R.J., Lim, C.C., Bresnahan,
J.F., Jaffe, A.S., Holmes, D.R., Bell, M.R. Regional systems of care to optimize timeliness of
reperfusion therapy for ST elevation myocardial infarction: the Mayo Clinic STEMI Protocol.
Circulation 2007: 116(7):729-36
Welsh, R.C., Travers, A., Huynh, T., Cantor, W.J. Canadian Cardiovascular Society Working
Group: Providing a perspective on the 2007 focused update of the American College of
Cardiology and American Heart Association 2004 guidelines for the management of ST
elevation myocardial infarction. Can J Cardiol Vol 25 No 1 2009: 13-48

primary percutaneous coronary intervention 37
Appendix 1: Glossary of Terms12-lead ECG: A procedure where leads are attached to patient’s arms, legs and chest wall to
record the electrical activity (rhythm) of the heart.
Advanced Cardiac Life Support (ACLS): A specialty (certifi cation) in advanced life support
measures usually retested bi-annually.
ALS Paramedic: Advanced Life Support Paramedic. This level of paramedic has received
advanced training in emergency medical service delivery.
American Heart Association (AHA): Mission – The American Heart Association is a national
voluntary health agency whose mission is to reduce disability and death from cardiovascular
diseases and stroke.
Angina: Chest pain caused by lack of oxygen (blood fl ow) to the heart.
Angioplasty (PTCA, PCI): A technique used in the treatment of coronary artery diseases.
The plaque that develops in the arteries of the heart is fl attened against the arterial walls,
resulting in improved circulation. The procedure involves threading a catheter through the
coronary arteries to the location of the plaque and infl ating and defl ating a small balloon at
the tip several times, then removing the catheter.
BCLS: A certifi cation in basic life support.
Canadian Cardiovascular Society (CCS): The mission of the Canadian Cardiovascular Society is
to advance the cardiovascular health and care of Canadians through leadership in professional
development, advocacy, and the promotion and dissemination of research.
Canadian Institute of Health Information (CIHI): Mandate was established jointly by
federal and provincial/territorial ministers of health – to coordinate the development and
maintenance of a comprehensive and integrated approach to health information for Canada,
and to provide and coordinate the provision of accurate and timely data and information.
Cardiac Care Network of Ontario (CCN): An advisory body to the MOHLTC that is dedicated
to improving quality, effi ciency, access and equity in the delivery of the continuum of adult
cardiac services in Ontario.
Cardiac catheterization: A diagnostic procedure in which a catheter is introduced into the
coronary artery to determine blockage. This is also referred to as coronary artery angiogram.
Cardiovascular disease (CVD): Diseases affecting the heart and major blood vessels.
CABG (Coronary artery bypass graft): Heart surgery in which a procedure is done to bypass
a narrowing or blockage in a coronary artery. This surgical procedure is used to restore blood
fl ow around previously blocked arteries.

primary percutaneous coronary intervention 38
Coronary Care Unit (CCU): A specialized unit that provides intensive care to patients
suffering from coronary/cardiac diseases.
Efficacy: The outcome/effectiveness of a treatment regime, study, or protocol.
Facilitated PCI: The practice of combining early pharmacological reperfusion therapy prior to
a planned PCI for STEMI (i.e. all patients receive PCI).
Fibrinolytics (fibrinolytic therapy, fibrinolysis): Medication given to dissolve clots in the
immediate acute phase of myocardial infarction.
First Response: The fi rst health care provider on the scene. Usually paramedic/EMS.
Health Planning Regions: Geographical areas by which health care planning and funding
are categorized.
Infarction: See Myocardial infarction.
Ischemia: A decreased supply of blood to a body organ or part often marked by pain or organ
dysfunction.
Ischemic heart disease (coronary heart disease): A type of heart disease caused by a lack
of oxygen reaching the tissue cells. Angina is a common symptom of ischemic heart disease
(see Angina).
Ministry of Health and Long-Term Care (MOHLTC): The ministry responsible for
administering the health care system and providing services to the Ontario public through
such programs as health insurance, drug benefi ts, assistive devices, care for the mentally ill,
long-term care, home care, community and public health, and health promotion and disease
prevention. It also regulates hospitals and nursing homes, operates psychiatric hospitals
and medical laboratories, and coordinates emergency health services.
Myocardium: Heart muscle.
Myocardial infarction (MI): Damage or necrosis of a region of the myocardium caused by an
interruption in the supply of blood to the heart, usually as a result of occlusion of a coronary
artery.
Necrosis: Cell death caused by lack of blood fl ow.
Ontario Health Technology Advisory Committee (OHTAC): An arm’s-length expert committee
that makes recommendations to the Ontario health care system and the Ontario Ministry
of Health and Long-Term Care (MOHLTC) about the best health technologies for Ontario.
Established in October 2003, OHTAC bridges the worlds of science and health care decision-
making by applying the best available evidence, from around the world and across the
province, to the unique needs of Ontario patients, providers, facility administrators and
policy decision-makers. Decisions are based on evidence-based analyses conducted by the
Medical Advisory Secretariat of the Ministry of Health and Long-Term Care.

primary percutaneous coronary intervention 39
PCP: Primary Care Paramedic. This level of paramedic is an entry level into basic life support
for emergency medical service delivery.
Percutaneous coronary intervention (PCI): see Angioplasty.
Percutaneous transluminal coronary angioplasty (PTCA): See Angioplasty.
Primary PCI: Performing acute angioplasty immediately for the treatment of a STEMI as the
primary form of reperfusion.
Rescue PCI: Performing angioplasty for STEMI after fi brinolytics have been given but where
it has failed to reperfuse the infarct related artery. The decision to perform rescue PCI is
generally made 60 to 90 minutes following the administration of fi brinolysis.
Reperfusion: The restoration of blood fl ow, as in coronary reperfusion after fi brinolytics
(drug).
Revascularization: The restoration of blood fl ow by increasing vessel diameter, as in
angioplasty.
Secondary prevention (of cardiovascular disease): Relates to rehabilitative interventions,
both physiological and behavioral, to minimize disease progression and reduce the risk of
recurrent CV events.
Shock: An imbalance between oxygen supply and myocardial demand causing increased heart
rate, decreased blood pressure and organ failure.
Stay a Bed Ahead Strategy: The American College of Emergency Physicians (ACEP) and the
American Hospital Association (AHA) list in their Strategies for Overcrowding to Stay a Bed
Ahead. Hospitals are encouraged to set a benchmark to stay a bed ahead so there will always
be an open [inpatient hospital] bed to accommodate an ED patient requiring admission.
STEMI (ST elevation myocardial infarction): On a 12-lead ECG, evidence of myocardial
damage causing ST segment elevation.
Stent: A metal device used to hold open an artery after it has been dilated with an
angioplasty balloon.
Thrombus: A blood clot causing interruption of blood fl ow. A thrombus in a coronary artery
can cause a heart attack.
Virtual beds: This term is used to denote a nominal location that the patient is held against
in the hospital’s patient administration system. This is because, in the patient administration
system, each admitted patient needs to be held against a bed, whether or not they are in a
physical bed.
primary percutaneous coronary intervention 40
Appendix 2: CCN Member Hospitals
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Hamilton Health Sciences CentrepPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
Hamilton Health Sciences – General Site (HGH) is the PCI site for LHIN IV (HNHB LHIN). The pPCI
initiative began in 2003 with offering primary PCI initially to patients presenting at the HGH
during cath lab operational hours. The current model consists of two types of patients. Patients
in Hamilton and Burlington presenting by EMS, where a 12-lead ECG demonstrates STEMI, are
transported directly to the HGH. There is a plan to expand the direct fi eld-to-HGH transfer to
other areas of the LHIN over the next year. For patients presenting by self-transportation, or by
EMS where no ECG is obtained in the fi eld, pPCI is offered 24/7 where immediate transportation
is available, or for high risk STEMI and fi brinolysis contraindication patients. In this latter
group, once the STEMI is diagnosed by the Emergency Physician, the Interventionalist on call is
notifi ed via the “PCI Hotline” and the patient accepted for transfer to the HGH.
In 2010, the Primary PCI Initiative has evolved into the Strategic Management of Reperfusion
and Therapies in Acute Myocardial Infarction (SMART-AMI). The SMART-AMI initiative is
focusing on the development of an integrated strategy to deliver optimal medical care for all
patients with STEMI in LHIN IV. This involves collaboration with Hamilton Health Sciences,
regional hospitals, Emergency Medical Services, the LHIN IV Cardiac Working Group and the
LHIN IV Emergency Services Steering Committee. Through improved communication, data
collection, and a rapid feedback loop of key indicators, our goal is to enhance the uptake of
evidence-based best practices in managing patients with STEMI in the region.
HIGHLIGHTS:
The program was implemented in January 2003, using a staged approach to offering
pPCI for STEMI patients within the region.
The program services Burlington to Fort Erie and Burford to Cayuga and includes
more than 1.3 million residents. Approximately 70 percent of the population resides
in the Hamilton or Niagara areas.
The program incorporates strategies for both patients who present by ambulance
(including fi eld-to-PCI centre transport when ECG acquisition is performed in the fi eld)
and by self-transportation.
The program incorporates strategies for patients in whom primary PCI is not readily
available, i.e., rescue PCI post-fi brinolysis.
primary percutaneous coronary intervention 41
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Hôtel-Dieu Grace HospitalpPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Cardiac Catheterization and PCI Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
Hôtel-Dieu Grace Hospital (HDGH) implemented a stand-alone angioplasty program for the
Southwest Ontario region serving primarily Windsor and Essex County at this time. Since
2007, the program has expanded to include two interventional cardiologists and a 12-hour
operational day. The hospital is planning a daytime primary angioplasty program to begin the
fall of 2010.
The hospital is currently seeking approval for expansion through the construction of an
additional wing that will include a two-suite angioplasty lab to allow for a third interventional
recruit and 24/7 primary angioplasty program.
HIGHLIGHTS:
Stand-alone program established May 2007 with rotation of physicians from London
Health Sciences Centre.
Medical Director recruited, leading program at HDGH March 2008.
Second Interventionalist recruited and joined the team May 2010.
Current patient population served is primarily Windsor and Essex County.
(Windsor Regional Hospital and Leamington District Memorial Hospital).
Primary PCI offered during daytime hours but process is not formalized.
On-site pre- and post-PCI clinic established 2008.
Integrated IVUS program established October 2009 decreasing need for additional
transfers to London.
Collaboration with Schulich Medical School – cardiology residents rotate in lab.
Collaborative revascularization rounds held weekly via videoconference with LHSC
reviewing complicated patient cases.
Strong commitment to fundraising to support cath lab expansion project with over
$8 million raised thus far.
Long-term plan for administering lytics and immediate transfer for Chatham/Kent region,
but currently unable to accommodate infl ux of patients due to limited CCU beds and cath
lab capacity.

primary percutaneous coronary intervention 42
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Kingston General Hospital pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
The STEMI (ST Elevated Myocardial Infarction) program represents a partnership between
Frontenac County EMS and the Departments of Emergency Medicine and Cardiology at
Kingston General Hospital (KGH). It provides emergent and urgent treatment for patients
in the region who experience STEMI. Only KGH provides immediate access to angioplasty
services between Ottawa, Peterborough and Oshawa.
The STEMI initiative supports primary PCI treatment for patients/hospitals that can ensure
transportation to KGH in less than 90 minutes predominantly within the immediate Kingston,
Frontenac, Lennox and Addington area and including Napanee and Gananoque. Both basic
and advanced care paramedics were taught how to interpret 12-lead ECGs and to diagnose a
STEMI. Paramedics call ahead to the Emergency Department at Kingston General Hospital when
transporting a STEMI patient to ensure the cardiac catheterization lab is ready for the patient
before the patient arrives. Patients are taken directly to the cardiac catheterization lab at KGH.
HIGHLIGHTS:
The program was started in April 2005 and KGH was the fi rst Ontario hospital to provide
primary PCI 24 hours a day, 7 days a week.
The program operates out of southeastern Ontario, home to close to 500,000 people across
all of Hastings County, Lennox and Addington, Prince Edward County, Frontenac County,
and the City of Kingston. It has a sizeable rural population with 44 percent of its residents
living in communities of fewer than 10,000 people. One-quarter of the population resides
in Kingston.
Nearly 100 paramedics with the Frontenac Paramedic Services are trained to provide on-
site electrocardiogram for patients with chest pain and anginal symptoms.
primary percutaneous coronary intervention 43
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: London Health Sciences CentrepPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
The primary PCI program is a partnership between London Health Sciences Centre, Thames
EMS, the Southwest Ontario Regional Base Hospital, the Central Ambulance Communication
Centre and the London-Middlesex County Department of Emergency Services. Its purpose is
to treat patients experiencing an ST elevation myocardial infarction (STEMI) within
90 minutes of the onset of chest pain.
BCLS and ACLS paramedics based in Middlesex County have been trained to interpret
12-lead electrocardiograms (ECGs) performed in the community. Once a potential STEMI has
been diagnosed, EMS communicates directly with the interventional cardiologist on call who
makes the fi nal diagnosis and assembles the primary PCI team in the cardiac catheterization
lab at University Hospital, a site of London Health Sciences Centre. As the primary PCI team
is assembling in the lab, the patient is transported directly to the cardiac catheterization lab
bypassing emergency departments along the route using a bypass protocol.
The ability of BCLS and ACLS paramedics to interpret 12-lead ECGs, and initiate contact
with the interventionalist on call, has been in effect for a year. Plans are underway to expand
the program to better serve STEMI patients in surrounding communities.
HIGHLIGHTS:
The original program was implemented in 2006. It has expanded three times to better
serve our patient population. We currently offer service 24 hours a day, 7 days a week to
the residents of London-Middlesex regardless of whether they call 911, present at their
local emergency department, or have a STEMI while an inpatient of a local hospital.
The program serves a population of 460,000.
primary percutaneous coronary intervention 44
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Rouge Valley Health System pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
Rouge Valley (RVHS) Cardiac Care Program is a regional program in the Central East LHIN
(CELHIN), one of the largest demographic LHINs in the province, serving Scarborough and
Durham. Stand-alone PCI without on-site cardiac surgery was fi rst trialed at RVHS in January
2003. Rouge Valley had a well-established cardiac catheterization laboratory prior to this.
In 2005, RVHS systematically introduced pPCI with a continued focus on improved patient
clinical outcomes. RVHS completed a pilot Code STEMI project (within Scarborough only) from
February 2009 to April 2010. Through CELHIN funding support, RVHS expanded the Code STEMI
service to Scarborough and Durham as of April 27, 2010.
A multidisciplinary pPCI collaborative committee meets regularly and includes both Toronto and
Durham Region EMS, The Scarborough Hospital, Lakeridge Health Corporation and Rouge Valley
Health System. Evidence-based protocols, algorithms, pre-printed order sets, policies, and D2B data
collection tools were developed by the RVHS pPCI committee, and continuous quality improvements
made to maximize care delivery. Inter-hospital communication and support between EDs, MDs,
nurses and EMS services are critical to the optimization of patient clinical outcomes. Critical
care capacity, regional repatriation, staffi ng challenges, and patient awareness of cardiac infarct
symptomology and the urgency of early reperfusion are important success factors. Despite some of
the challenges of providing pPCI 24/7 the RVHS pPCI program continues to thrive and promote
leading practices and to deliver gold-standard therapy for AMI. This is achieved by the dedication
and cooperation of the RVHS cardiac team and its regional partners.
The collaboration with our partner hospitals and EMS was a critical success factor to ensure
a consistent and standardized approach to the care of all cardiac patients in the CELHIN.
HIGHLIGHTS:
RVHS is a large community hospital within the CELHIN that services a population of 1.5
million people or 11 percent of Ontario’s population. Almost half of its population resides in
Scarborough, however the CELHIN has a mix of rural, urban, and remote communities.
We have a full service cardiac program including cardiac diagnostic testing, coronary
intervention, advanced arrhythmia, inpatient coronary care, cardiac rehabilitation and
secondary prevention.
Rouge Valley was the fi rst stand-alone PCI centre in Ontario to provide pPCI .
The Rouge Valley Cardiac Care Program currently has two catheterization labs, with strategic
direction to expand to service the needs of the CELHIN, specifi cally East Toronto and West Durham.

primary percutaneous coronary intervention 45
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Southlake Regional Health CentrepPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
The program provides 24-hours, 7 days a week primary PCI for the region. All paramedics
have been taught to perform and interpret 12-lead electrocardiograms and diagnose STEMI
using standard criteria. An EMS bypass system is employed, where patients diagnosed with
a STEMI, with onset of symptom < 12 hours and within 45 minutes of SRHC, are brought
directly to the cath lab for primary PCI. Code STEMI can be activated by EMS or the regional
ER physician without the cardiologist’s approval. Cath lab and on-call interventional
cardiologists are called to provide primary angioplasty. A reserved, guaranteed regional
STEMI bed is always available. Repatriation agreements are in place with regional hospitals
to return patients to their closest hospital post-PCI.
A joint program of Newmarket-based SRHC and York Region Emergency Medical Services
(EMS) employs technology that allows paramedics in York Region to wirelessly transmit
an electrocardiogram – which they perform in the ambulance – to SRHC cardiologists.
The physicians then review the electrocardiogram on a hospital computer screen or on
their Personal Digital Assistant (PDA) to confi rm the patient’s diagnosis and recommend
the appropriate treatment, including authorizing paramedics to immediately administer
intravenous clot-busting drugs (for STREAM study patients only).
HIGHLIGHTS:
The ER bypass for primary PCI program was implemented in January 2007.
The program and serves over 1.6 million residents that reside primarily in northern
Toronto and the suburban communities north of the city located in the “905” and “705”
areas, including the Highway 400 corridor.
Southlake Regional Health Centre has successfully collaborated with the three paramedic
services in the Region, offering primary PCI services to all patients meeting set criteria
following a STEMI algorithm.
Southlake Regional Health Centre and York Region are participating in an international
study – the STREAM Trial – wherein patients who are more than 45 minutes from the
hospital and who are given clot-busting medications in the ambulance are compared to
those patients who undergo an angioplasty within one hour of the diagnosis of a STEMI.
primary percutaneous coronary intervention 46
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: St. Mary’s General Hospital
pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
St. Mary’s General Hospital provides a regional approach to STEMI care where patients
are admitted directly to the cath lab for primary angioplasty. The program is a partnership
between St. Mary’s Regional Cardiac Centre and the Region of Waterloo EMS. St. Mary’s
General Hospital has provided advanced ECG training and a train-the-trainer program to
all Region of Waterloo EMS paramedics. EMS has developed a STEMI Protocol and Directive
that allows the paramedics to make the diagnosis from the 12-lead ECG to call direct to
St. Mary’s Cath Lab and to activate the STEMI Protocol. The External Code STEMI protocol
allows advanced care paramedics to review the results of the 12-lead and activate the team
at St. Mary’s directly. The interventional cardiologist speaks with the EMS on route, and if
appropriate, the patient bypasses the hospital’s emergency department and proceeds directly
to the cardiac catheterization lab. The External Code STEMI protocol operates 24/7.
HIGHLIGHTS:
The St. Mary’s program was implemented in 2007.
The program operates within southwestern Ontario, a mix of rural and urban geography
that covers 4,800 square kilometers with a population of 750,000.
The program received the Ontario Hospital Association Best Award in Use of Technology as
a “fi rst” in Canada to adopt wireless RIM technology for diagnosing STEMI.
Recently, EMS paramedics have received advanced training and now do a diagnosis in the
fi eld and implement the Code STEMI Protocol directly. They call one STEMI number, which
activates the on-call team and communication with the interventional cardiologist.

primary percutaneous coronary intervention 47
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: St. Michael’s HospitalpPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
St. Michael’s Hospital is a member of the Toronto Heart Attack Collaborative (THAC). THAC is
a partnership between the hospitals in the Toronto Central LHIN, EMS and the MOHLTC that
provides timely treatment to patients experiencing STEMI.
St. Michael’s Hospital provides a comprehensive 24-hour, 7 days a week approach to STEMI
care where patients are brought directly to the cath lab for primary angioplasty. St. Michael’s
Hospital collaborates with Toronto East General Hospital (TEGH) and St. Joseph’s Health
Centre to facilitate inter-hospital transfers of STEMI patients to St. Michael’s Hospital.
HIGHLIGHTS:
The St. Michael’s Hospital program was implemented in 2008.
The program operates within Canada’s most urban area with a population of 1.15 million
people of diverse ethno-racial, social and religious backgrounds.
The program is one of three centres in Toronto Central LHIN that provides 24-hour access
to PCI.
Level III paramedics are dispatched based on a citywide process called Code STEMI
The Toronto EMS diagnoses STEMI wherever they assess the patient, bypass the local ED
and take the patient directly to the St. Michael’s Hospital cath lab.
Patients from the St. Joseph and TEGH catchment areas are repatriated post pPCI within
6-8 hours for post-procedure recovery.
primary percutaneous coronary intervention 48
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Sudbury Regional Hospital pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
The Sudbury Regional Hospital boasts a primary PCI program. Once a diagnosis of ST
elevation MI (STEMI) has been established, the patient is promptly transferred to the cardiac
catheterization lab and primary PCI takes place. This service is available to all residents who
present to the emergency department shortly after onset of chest pain and are then diagnosed
with an evolving STEMI. Because of the geographical challenges of the North East LHIN, it is
not possible to offer primary PCI to residents who may be hours away. It is therefore prudent
to treat these patients with thrombolysis and then transfer them to our tertiary centre for
rescue PCI if warranted.
Primary PCI service is available 24/7 with cardiologists and interventional cardiologists on
call at all times.
HIGHLIGHTS:
The program supports communities in northeastern Ontario, home to a population of
567,900 people, or 4.6 percent of the population of Ontario. Just over 28 percent of the
North East area is highly concentrated in Greater Sudbury with Sault Ste. Marie and North
Bay the next most populous areas.
Plans are underway to expand the program, a Working Group has been established and
work is in progress.
As of April 2010 the Greater Sudbury Emergency Services, Sudbury Regional Hospital,
Northeastern Ontario Pre-hospital Care Program and the MOHLTC CACC have collaborated
to develop a STEMI Bypass/Alert process by which patients presenting in the pre-hospital
environment with STEMI can be transported by paramedics directly to the cath lab. This
program currently runs Monday to Friday during 0700–1700 hours. After-hours patients
are seen in ED fi rst.

primary percutaneous coronary intervention 49
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Sunnybrook Health Sciences Centre pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
Sunnybrook Health Sciences Centre (SHSC) is a member of the Toronto Heart Attack
Collaborative (THAC). THAC is a partnership between the hospitals in the Toronto Central
LHIN, EMS and the MOHLTC that provides timely treatment to patients experiencing an
ST elevation myocardial infarction (STEMI).
At SHSC, the hospital provides 24/7 STEMI care with EMS triage support. If a STEMI is
confi rmed, paramedics call SHSC’s cardiac care unit using a dedicated STEMI hotline where
information regarding the patient is relayed to a CCU nurse. A Code STEMI is immediately
initiated which activates the catheterization laboratory team members (interventional
cardiologists and nursing staff). When the patient arrives at SHSC, they are taken directly to
the cath lab where an emergency angioplasty is performed. Following the angioplasty, the
patient is transferred to a CCU bed at SHSC for monitoring and nursing care.
HIGHLIGHTS:
The Sunnybrook Health Sciences Centre Code STEMI program was implemented in 2008.
The program operates within Canada’s most urban area with a population of 1.15 million
people of diverse ethno-racial, social and religious backgrounds.
The program is one of three centres in Toronto Central LHIN that provides 24-hour access
to PCI.
Level III paramedics are dispatched based on a citywide process called STAT (STEMI
ALS Transport) and provide provisional diagnosis of MI using manual 12-lead ECG
interpretations in addition to monitor interpretation.
SHSC is the primary referral centre for STEMI patients at North York General and Humber
River Regional Hospital.
primary percutaneous coronary intervention 50
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Thunder Bay Regional Health Sciences Centre pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Cardiac Catheterization and PCI Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
Thunder Bay Regional Health Sciences Centre (TBRHSC) offers a stand-alone PCI program (no
cardiac surgery on site) to the northwest region of Ontario including the district of Kenora,
Rainy River and Thunder Bay, incorporating signifi cant distances of approximately 1000 km.
Expansion of the program to include 24/7 primary PCI for the residents of Thunder Bay
is planned for the fall of 2010. EMS and community hospitals will be an integral part of a
pharmaco-invasive approach of administration of lytics and direct transport for STEMI
patients at distances greater than 90 minutes away from TBRHSC.
HIGHLIGHTS:
Stand-alone angioplasty program established October 2007 through the mentorship of the
University of Ottawa Heart Institute. A partnership developed with St. Luke’s Hospital,
Duluth Minnesota, provides cardiac surgery as back-up for the program.
TBRHSC currently offers primary PCI for selected cases such as thrombolytic failure,
thrombolytic ineligibility and cardiogenic shock.
TBRHSC serves a vast Northwestern Ontario region of isolated communities, including 30
percent First Nations communities.
Signifi cant fi nancial burden due to travel costs is lessened through the on-site cardiac
intervention program at TBRHSC.
TBRHSC supports the Northern Ontario Medical School that was initiated in 2005.

primary percutaneous coronary intervention 51
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Toronto East General Hospital pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Cardiac Catheterization Program in partnership with SMH for PCI Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
TEGH is a large community hospital in Toronto’s east end and historically, our Emergency
Department has seen amongst the highest volumes of patients with acute coronary syndrome
in the Greater Toronto Area. Our primary catchment area encompasses one of the most
ethnically diverse areas of the province, many from lower socioeconomic backgrounds.
We have had a diagnostic cardiac catheterization laboratory since December, 2001, with
volumes of 1800-2000 cases per year, but our unit has not as yet gained approval to provide
coronary interventional services.
Toronto East General Hospital (TEGH) has been a member of the Toronto Heart Attack
Collaborative (THAC) since June, 2008 and our physicians and administration have played
a central role at THAC in establishing an effective and sustainable model for collaboration
between PCI centres and community hospitals in Toronto.
In support of the paradigmatic shift towards primary PCI for the management of patient
with STEMI, we have developed a partnership with Toronto EMS and our colleagues at
St. Michael’s Hospital (SMH) to ensure timely 24/7 access to primary PCI for Toronto East
General patients.
HIGHLIGHTS:
TEGH’s Primary PCI partnership (Code STEMI program) became operational
on April 1, 2009.
In the fi rst 18 months of operation, 128 Code STEMI patients have been transported
to St. Michael’s Hospital.
Of these, 88 patients (69%) have originated from the TEGH Emergency Department.
This high percentage of ER transfers underscores the vital role played by ER nurses
and physicians at TEGH in recognizing and expediting care.
Median door to balloon times of close to 90 minutes for these ER transfers have been a
testament to the effectiveness of the partnership and the excellent lines of communication
and critical feedback between all involved.

primary percutaneous coronary intervention 52
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: Trillium Health Centre pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
Following a number of years of supported-for-rescue and facilitated pPCI, in December
2008, Trillium launched the regional pPCI Direct process with Halton Region EMS and the
Sunnybrook Osler Centre for Pre-Hospital Care (SOCPC) with a 24 hour, 7 days a week ST
Elevated Myocardial Infarction (STEMI) bypass protocol. We decided to stage our approach
in recognition of the complexity of the process and the fact that we support three EMS
services that operate within our LHIN. Following the successful outcomes with Halton EMS
we launched the process with Toronto EMS in May 2009, followed by Peel EMS in two phases
(south Peel in August 2009 and north Peel in March 2010). Our data shows our average time
from door to fi rst device being 70 minutes. Our performance has been sustained despite the
addition of each EMS service, which has increased our volumes and the travel distances.
EMS has been able to sustain their time target of under 60 minutes from arrival to patient to
arrival at Trillium 98–100 percent of the time.
HIGHLIGHTS:
The STEMI Direct program was implemented in 2008.
The program serves over 1 million residents in the municipalities of South Etobicoke,
Mississauga, Halton Hills, Oakville, and Milton, and covers approximately
900 square kilometers.
As of the end of March 2010 STEMI Bypass for pPCI Direct has partnered Peel and Toronto
EMS as well as Halton EMS. Our partnerships now include Halton Healthcare (Oakville,
Milton, Georgetown sites) and William Osler Health Centre (Brampton Civic and Etobicoke
General sites) as well as the catchment area of Trillium Mississauga and West Toronto sites.
primary percutaneous coronary intervention 53
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: University Health Network – Toronto General Site (TGH)pPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
The University Health Network (UHN) is a member of the Toronto Heart Attack Collaborative
(THAC). THAC is a partnership between the hospitals in the Toronto Central LHIN, EMS and
the MOHLTC that provides timely treatment to patients experiencing a STEMI.
UHN, the Peter Munk Cardiac Centre, provides a comprehensive 24-hour, 7 days a week approach
to STEMI care where patients are brought directly to the cath lab at Toronto General Hospital
(TGH) site for primary angioplasty. The STEMI team is activated by a call placed by a physician
or EMS team member to an emergency number at the hospital’s switchboard. This activates
the STEMI pager system that sends a Code STEMI text message with the patient’s location
to the CICU team (who assess the patient) and cath lab team. Patients are taken directly to
CICU and the cath lab for primary angioplasty. Immediately following primary PCI the patient
is transferred to a dedicated CICU STEMI bed for monitoring and nursing care. The Toronto
Western (TWH) site also does primary PCI during the day Monday through Friday.
HIGHLIGHTS:
The TGH Code STEMI program was implemented in 2008.
The program operates within Canada’s most urban area with a population of 1.15 million
people of diverse ethno-racial, social and religious backgrounds.
The program is one of three centres in Toronto Central LHIN that provides 24-hour access
to PCI.
Level III paramedics are dispatched based on a citywide process called STAT (STEMI
ALS Transport).
The Toronto EMS diagnoses STEMI wherever they assess the patient and bypass the ED.
In collaboration with Mount Sinai Hospital (MSH), STEMI patients are transferred through
the underground tunnel joining MSH and TGH. The EMS transfers patients from the
Toronto Western to the cath lab at TGH.

primary percutaneous coronary intervention 54
CCN Member Hospital Primary PCI Program Profile
CCN Member Hospital: University of Ottawa Heart InstitutepPCI Program Service Level:
CARDIAC PROGRAM TYPE SERVICE MODEL = PROVIDED = NOT PROVIDED
Full Service PCI and Cardiac Surgery Program
Regional Transport 24/7 Operations EMS Triage Support
PROGRAM OVERVIEW:
When an Ottawa patient calls 911 complaining of chest pain, advanced care paramedics
trained to interpret the results of an ECG and recognize ST elevation myocardial infarction,
are immediately dispatched. If a STEMI is confi rmed, the patient is transported to UOHI
where the STEMI cardiology team, on 24/7 standby, has been alerted to the pending arrival
of the patient based on a Code STEMI protocol. On receiving the patient, the cardiology team
is primed to perform an emergency angioplasty. The STEMI protocol, developed by the Heart
Institute, represents an extraordinary collaboration between front-line health care workers,
cardiologists, base hospital physicians and support staff. A collaborative alliance established
among Ottawa’s health care leaders enables advanced care paramedics to bypass conventional
emergency room procedures and transport STEMI patients directly to the Heart Institute’s
STEMI lab. The alliance includes the four local Ottawa hospitals, 12 regional and community
hospital sites, along with an immense base of emergency physicians, cardiologists and GPs,
whose co-operation is essential. Because a suspected heart attack patient can also appear in the
emergency department of another Ottawa hospital, the STEMI team relies on ER staff of that
hospital to identify a STEMI and transfer the patient quickly to the Heart Institute.
HIGHLIGHTS:
A total of 344 STEMI patients were transported to the Heart Institute between May 2005
and May 2006 – the fi rst full year of operation.
The mortality rate of patients delivered to the Heart Institute was 1.9 percent, compared
to 8.9 percent in patients transported to emergency departments of the local hospitals
between July 2001 and January 2004.
The primary PCI program has realized many positive impacts, such as a shorter length of
time in hospital, reducing the burden on emergency rooms and critical care units, where
beds and resources are in high demand.
For the fi rst time in Ontario, the UOHI program ensures urgent standardized treatment
regardless of geography. Heart Institute specialists have collaborated with 16 regional
and community hospital sites to develop the fi rst LHIN-wide program in Ontario for
STEMI patients.

primary percutaneous coronary intervention 55
Appendix 3: Ontario Cardiac Centres Primary Percutaneous Coronary Intervention Physician Leads
CaRdIaC CEntRE PRIMaRY PCI LEad PhYSICIan
Hamilton Health Sciences Centre Dr. Madhu Natarajan
Hôtel-Dieu Grace Hospital Dr. Amr Morsi
Kingston General Hospital Dr. Waitak Kong
London Health Sciences Centre Dr. Kumar Sridhar
Rouge Valley Health System Dr. Saleem Kassam
Southlake Regional Health Centre Dr. Warren Cantor
St. Mary’s General Hospital Dr. Danielle Leddy
St. Michael’s Hospital, Toronto* Dr. Neil Fam
Sudbury Regional Hospital Dr. Gami Ravi
Sunnybrook Health Sciences Centre Dr. Sam Radhakrishnan
Thunder Bay Regional Health Sciences Centre Dr. Mark Henderson
Trillium Health Centre Dr. Randy Watson
Univeristy Health Network Dr. Vlad Dzavik
University of Ottawa Heart Institute Dr. Michel LeMay
* Also has a partnership program with Toronto East General Hospital.

primary percutaneous coronary intervention 56
Appendix 4: Access to Urgent Primary Percutaneous Coronary Intervention for STEMI: 16 Recommendations27
Recommendation 1 – That primary PCI for STEMI patients, presenting within 12 hours of
symptom onset, be the preferred therapy for:
All eligible patients presenting to a hospital with on-site PCI facilities with an experienced
interventional team, with a maximum D2B time of less than 90 minutes.
All eligible patients who can be transferred from an acute care hospital to a primary
PCI centre with a maximum D2B time of less than 90 minutes.
All patients who have contraindications to fi brinolytic therapy, regardless of distance,
as long as the procedure is performed within 12 hours of symptom onset.
Patients who present after 12 hours of symptom onset to be managed on a case-by-case basis.
Recommendation 2 – That all centres providing primary PCI services maintain an
infrastructure that enables it to perform to high standards of safety and effi cacy, including:
A minimum standard of 150 PCI procedures per operator per year.
An annual review process to ensure that:
– All operators achieve minimum procedure volumes; and
– The centre performs a minimum of 500 diagnostic catheterization procedures and 400
interventional procedures per year of which greater than 50 must be primary PCI.
Suffi cient number of operators and catheterization laboratory staff performing PCI to
ensure the availability of PCI services 24 hours a day, seven days a week.
Recommendation 3 – That fi brinolytics be administered to STEMI patients who present to
hospital within 12 hours of symptom onset and who cannot receive primary PCI within the
recommended D2B times, or for whom PCI is contraindicated. Patients who present after 12
hours of symptom onset are to be managed on a case-by-case basis.
Recommendation 4 – Patients presenting within 2 hours of symptom onset represent a
special subset of STEMI patients who derive particular benefi t from early reperfusion
therapy. Careful case-by-case consideration of treating these patients with fi brinolytic
therapy rather than primary PCI should occur, weighing the risk of fi brinolytic therapy with
the potential delay in performing primary PCI.
Recommendation 5 – Rescue angioplasty should be performed for patients with acute STEMI
who receive fi brinolytic therapy but continue to present with on-going ischemic symptoms
and ECG changes 90 minutes following the administration of the fi brinolytics.
Recommendation 6 – Patients less than 75 years of age, who present with cardiogenic
shock within 18 hours of symptom onset, should be transferred immediately to an advanced
cardiac centre with on-site cardiac surgery for immediate angiography and revascularization.
Patients over 75 years of age are to be managed on a case-by-case basis. The use of
fi brinolytics has not been proven effective in this setting and its use should be individualized.
primary percutaneous coronary intervention 57
Recommendation 7 – Primary PCI should be performed in centres with on-site cardiac
surgical capability or in established stand-alone PCI centres with demonstrated ability to
transport patients to a cardiac surgical centre within 90 minutes of decision to transport.
Recommendation 8 – That a regional MI system, involving PCI hospitals, referring acute
care hospitals and municipal emergency medical services, be developed to provide effective,
effi cient and quality patient management for STEMI patients from patient assessment
through to post-MI care.
Recommendation 9 – That a working group be convened with a focus on emergency medical
services comprised of representatives from CCN, LHINs, hospitals and the MOHLTC
to identify strategies, processes and resources necessary to overcome current EMS
transportation challenges and to support the pPCI model and recommendations described
in this report.
Recommendation 10 – That suffi cient funding is available to support transportation
infrastructure that is capable of providing medically appropriate, reliable and effi cient
service to allow for optimal utilization of advanced services and regionalized systems.
Recommendation 11 – That all PCI hospitals implement the following processes and
infrastructures to support the delivery of pPCI for patients with STEMI presenting at PCI
hospitals on a 24/7 basis:
The development of emergency room care maps that ensure the timely diagnosis of STEMI
and transfer of the patient directly to the catheterization laboratory.
The development of direct communication links from the emergency room to the
responsible interventional cardiologist.
The development of processes/algorithms to accept patients directly to the cardiac cath
laboratory prior to obtaining a CCU bed (e.g., de-linking the CCU from the cath laboratory).
Early discharge policy for stable patients with uncomplicated myocardial infarction
diagnosis who have undergone PCI.
Referral to cardiac rehabilitation (which includes secondary prevention programs).
Recommendation 12 – That the MOHLTC plan for funding to support the infrastructure and
resource requirements at PCI hospitals with implementation provincially by 2008/09, which
would include:
Incremental funding for additional primary PCI cases.
Recruitment, hiring and training of additional catheterization laboratory and post-PCI
care staff.
Funding to support additional CCU beds where warranted, adding the needed fl exibility to
de-link the CCU from the catheterization laboratory.
Recommendation 13 – That a pilot project involving several regional MI centres, which include
the PCI hospital, referring acute care hospitals, and emergency medical services, be established
to support primary PCI for patients transferred from non-PCI acute care hospitals to PCI sites

primary percutaneous coronary intervention 58
by 2005/06. These pilot projects will include the development of tripartite agreements between
PCI sites, referring hospitals and emergency medical services (including municipal operations,
base hospitals and dispatch centres) to ensure:
The development and achievement of standards for transportation of STEMI patients from
the referring hospital to the PCI hospital.
The development of timely and cost-effective transportation systems for patients being
repatriated back to the referring hospital.
The development and monitoring of emergency room patient care management algorithms
for the rapid triage, diagnosis and management of STEMI patients.
The development of post-PCI care maps for repatriation, acute- and recovery-care
management, early discharge and rehabilitation.
The development of effi cient and rapid communication processes.
Prior to implementation, the pilot PCI centre should have implemented, at a minimum,
Model A of the primary PCI model (see reference #6).
Recommendation 14 – That the MOHLTC support a pilot project to evaluate a model of
“First Response” for primary PCI in Ontario, where patients are assessed at the point of
presentation of the STEMI and are transferred directly to the closest PCI hospital for
primary PCI. The pilot project should involve both urban and non-urban municipalities to
appropriately assess the generalizability of the model. Prior to implementation, the pilot PCI
centres should have successfully implemented, at a minimum, Phase I of the primary PCI
Recommendation 15 – That the MOHLTC plan for funding to support the infrastructure and
resource requirements for the pilot projects which would include:
Incremental funding for additional primary PCI cases.
Increased catheterization laboratory staff and post-PCI care nursing.
Funding for expanded emergency medical services (vehicles, staff, equipment, medications)
and training for paramedics to a level appropriate to meet the assessment and transport
needs of the STEMI patients.
Increased CCU/STEMI beds at PCI centres.
Enhanced access and delivery of secondary prevention cardiac rehabilitation programs.
Recommendation 16 – That a provincial monitoring system for STEMI in Ontario be
implemented that would include:
Monitor the treatment of STEMI in Ontario and the implementation of the proposed
models of care.
Monitoring of D2B and D2N times.
Monitor new changes in the treatment of STEMI as they develop, such as the use of
pre-hospital fi brinolytics and the use of pharmaco-invasive strategies.
Monitor access, safety and effi cacy of the STEMI model in Ontario through the tracking
and reporting of data.
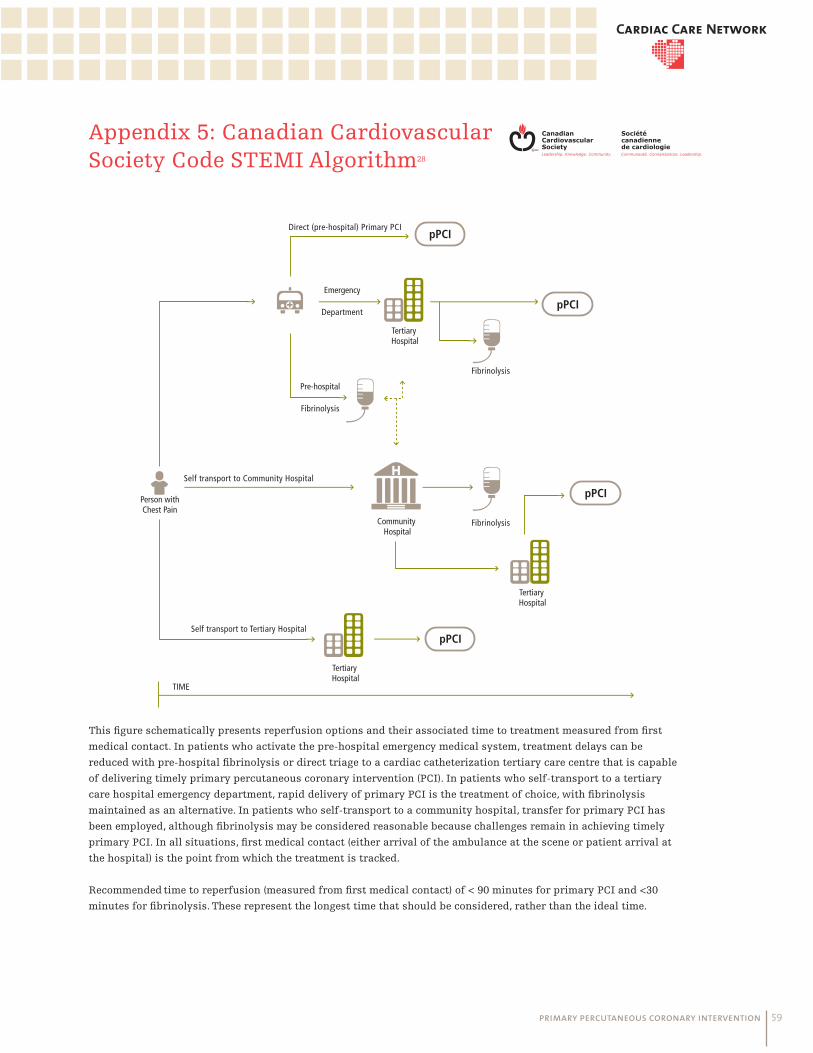
primary percutaneous coronary intervention 59
Appendix 5: Canadian Cardiovascular Society Code STEMI Algorithm28
pPCI
pPCI
pPCI
pPCI
Person withChest Pain
TIME
Community Hospital
Pre-hospital
Fibrinolysis
Emergency
Department
Fibrinolysis
Direct (pre-hospital) Primary PCI
Self transport to Community Hospital
Self transport to Tertiary Hospital
Fibrinolysis
Tertiary Hospital
Tertiary Hospital
Tertiary Hospital
This fi gure schematically presents reperfusion options and their associated time to treatment measured from fi rst
medical contact. In patients who activate the pre-hospital emergency medical system, treatment delays can be
reduced with pre-hospital fi brinolysis or direct triage to a cardiac catheterization tertiary care centre that is capable
of delivering timely primary percutaneous coronary intervention (PCI). In patients who self-transport to a tertiary
care hospital emergency department, rapid delivery of primary PCI is the treatment of choice, with fi brinolysis
maintained as an alternative. In patients who self-transport to a community hospital, transfer for primary PCI has
been employed, although fi brinolysis may be considered reasonable because challenges remain in achieving timely
primary PCI. In all situations, fi rst medical contact (either arrival of the ambulance at the scene or patient arrival at
the hospital) is the point from which the treatment is tracked.
Recommended time to reperfusion (measured from fi rst medical contact) of < 90 minutes for primary PCI and <30
minutes for fi brinolysis. These represent the longest time that should be considered, rather than the ideal time.
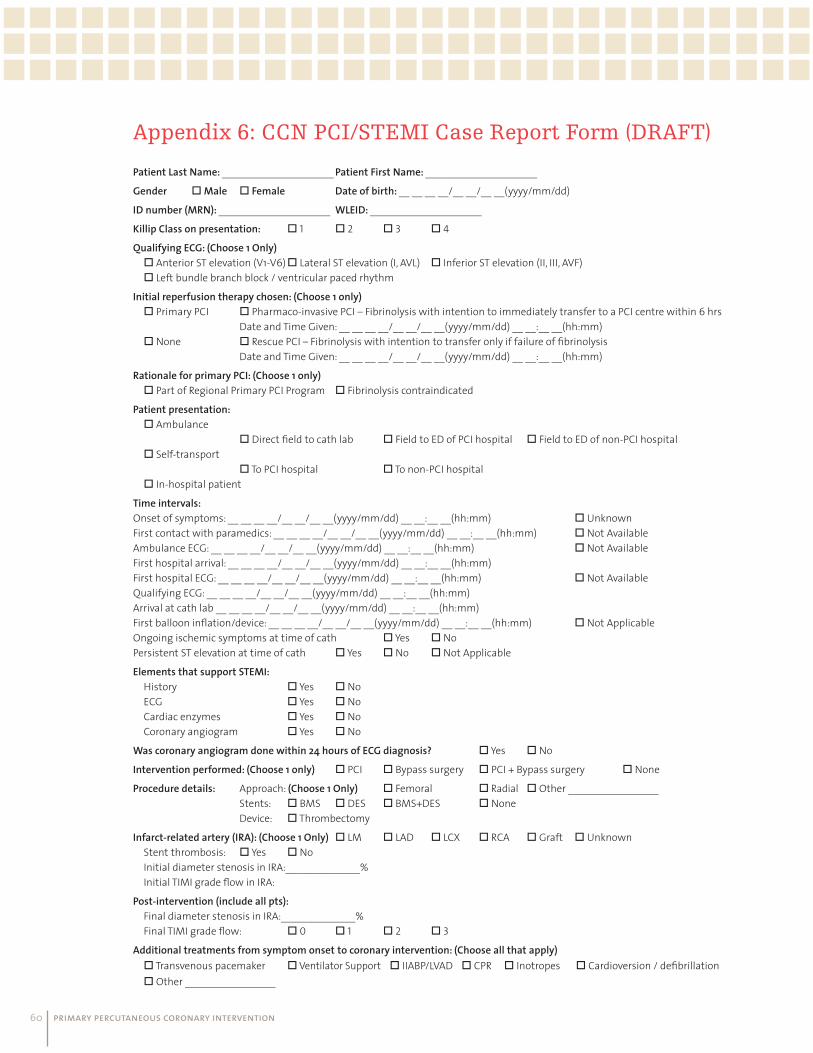
primary percutaneous coronary intervention 60
Appendix 6: CCN PCI/STEMI Case Report Form (DRAFT)
Patient Last Name: _____________________ Patient First Name: _____________________Gender Male Female Date of birth: __ __ __ __/__ __/__ __(yyyy/mm/dd)ID number (MRN): _____________________ WLEID: _____________________Killip Class on presentation: 1 2 3 4Qualifying ECG: (Choose 1 Only) Anterior ST elevation (V1-V6) Lateral ST elevation (I, AVL) Inferior ST elevation (II, III, AVF) Left bundle branch block / ventricular paced rhythmInitial reperfusion therapy chosen: (Choose 1 only) Primary PCI Pharmaco-invasive PCI – Fibrinolysis with intention to immediately transfer to a PCI centre within 6 hrs Date and Time Given: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) None Rescue PCI – Fibrinolysis with intention to transfer only if failure of fi brinolysis Date and Time Given: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm)Rationale for primary PCI: (Choose 1 only) Part of Regional Primary PCI Program Fibrinolysis contraindicatedPatient presentation: Ambulance Direct fi eld to cath lab Field to ED of PCI hospital Field to ED of non-PCI hospital Self-transport To PCI hospital To non-PCI hospital In-hospital patientTime intervals:Onset of symptoms: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) UnknownFirst contact with paramedics: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) Not AvailableAmbulance ECG: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) Not AvailableFirst hospital arrival: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm)First hospital ECG: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) Not AvailableQualifying ECG: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm)Arrival at cath lab __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) First balloon infl ation/device: __ __ __ __/__ __/__ __(yyyy/mm/dd) __ __:__ __(hh:mm) Not ApplicableOngoing ischemic symptoms at time of cath Yes No Persistent ST elevation at time of cath Yes No Not ApplicableElements that support STEMI: History Yes No ECG Yes No Cardiac enzymes Yes No Coronary angiogram Yes NoWas coronary angiogram done within 24 hours of ECG diagnosis? Yes NoIntervention performed: (Choose 1 only) PCI Bypass surgery PCI + Bypass surgery NoneProcedure details: Approach: (Choose 1 Only) Femoral Radial Other _________________ Stents: BMS DES BMS+DES None Device: ThrombectomyInfarct-related artery (IRA): (Choose 1 Only) LM LAD LCX RCA Graft Unknown Stent thrombosis: Yes No Initial diameter stenosis in IRA:______________% Initial TIMI grade fl ow in IRA:Post-intervention (include all pts): Final diameter stenosis in IRA:______________% Final TIMI grade fl ow: 0 1 2 3
Additional treatments from symptom onset to coronary intervention: (Choose all that apply) Transvenous pacemaker Ventilator Support IIABP/LVAD CPR Inotropes Cardioversion / defi brillation Other _________________

primary percutaneous coronary intervention 61
Appendix 7:
Version: V. 01–02Last Update: July 20, 2010
Cardiac Care Network
PPCI/STEMI Case Report FormData Dictionary

primary percutaneous coronary intervention 62

primary percutaneous coronary intervention 63
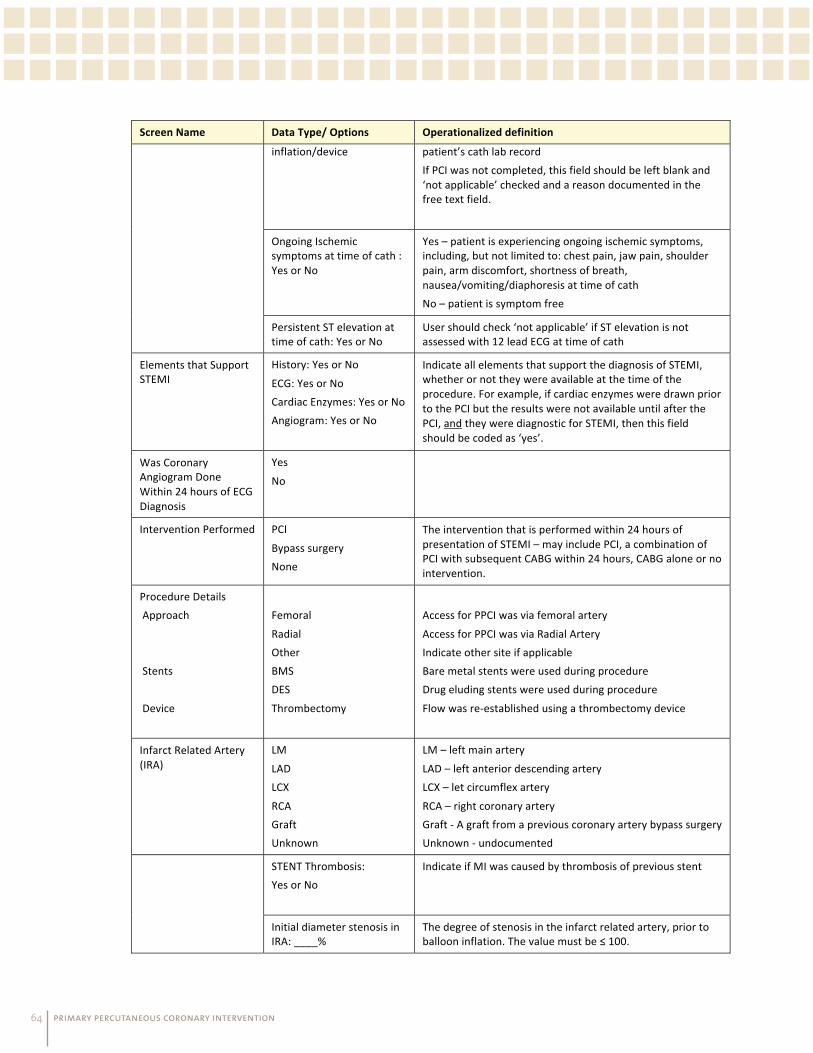
primary percutaneous coronary intervention 64

primary percutaneous coronary intervention 65

primary percutaneous coronary intervention 66

primary percutaneous coronary intervention 67
Appendix 8: NEJM: A Citywide STEMI ProtocolA Citywide Protocol for Primary PCI in ST Segment Elevation Myocardial Infarction
Michel R. Le May, M.D., Derek Y. So, M.D., Richard Dionne, M.D., Chris A. Glover, M.D., Michael
P.V. Froeschl, M.D., George A. Wells, Ph.D., Richard F. Davies, M.D., Heather L. Sherrard, R.N.,
Justin Maloney, D.D., Jean-François Marquis, M.D., Edward R. O’Brien, M.D., John Trickett,
R.N., Pierre Poirier, A.C.P., Sheila C. Ryan, B.Sc., Andrew Ha, M.D., Phil G. Joseph, M.D., and
Marino Labinaz, M.D.
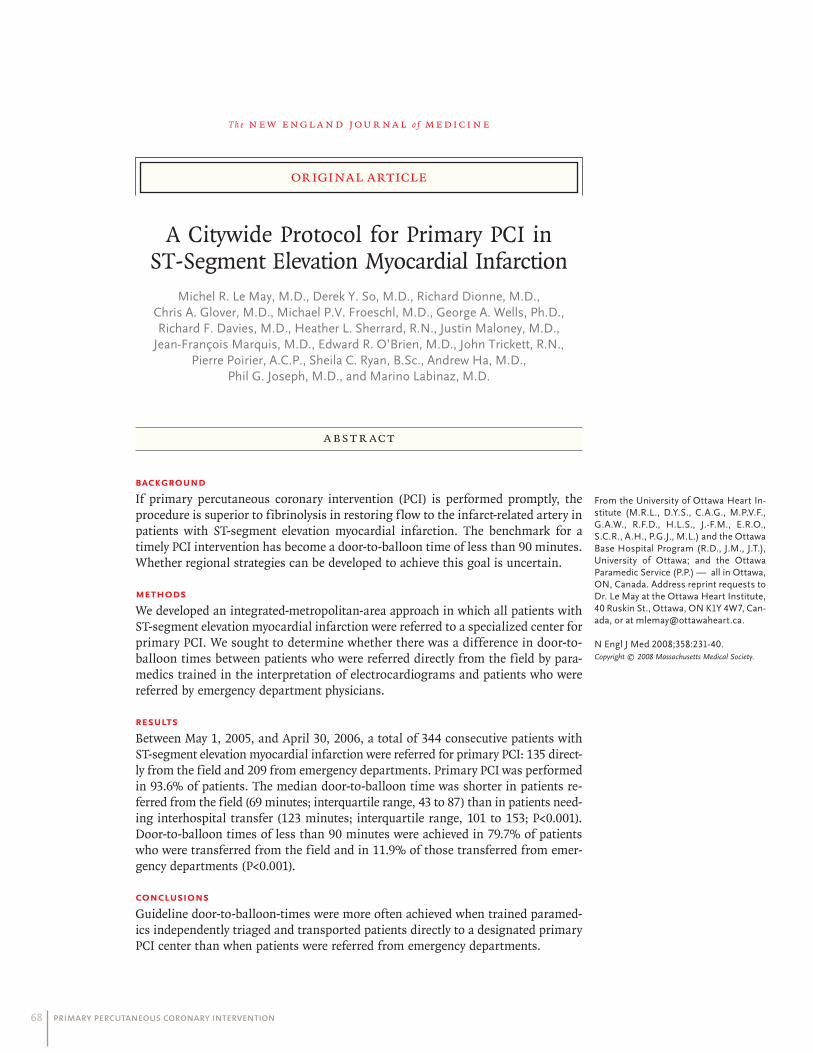
primary percutaneous coronary intervention 68
Th e n e w e ng l a nd j o u r na l o f m e dic i n e
original article
A Citywide Protocol for Primary PCI in ST-Segment Elevation Myocardial Infarction
Michel R. Le May, M.D., Derek Y. So, M.D., Richard Dionne, M.D., Chris A. Glover, M.D., Michael P.V. Froeschl, M.D., George A. Wells, Ph.D., Richard F. Davies, M.D., Heather L. Sherrard, R.N., Justin Maloney, M.D.,
Jean-François Marquis, M.D., Edward R. O’Brien, M.D., John Trickett, R.N., Pierre Poirier, A.C.P., Sheila C. Ryan, B.Sc., Andrew Ha, M.D.,
Phil G. Joseph, M.D., and Marino Labinaz, M.D.
From the University of Ottawa Heart In-stitute (M.R.L., D.Y.S., C.A.G., M.P.V.F., G.A.W., R.F.D., H.L.S., J.-F.M., E.R.O., S.C.R., A.H., P.G.J., M.L.) and the Ottawa Base Hospital Program (R.D., J.M., J.T.), University of Ottawa; and the Ottawa Paramedic Service (P.P.) — all in Ottawa, ON, Canada. Address reprint requests to Dr. Le May at the Ottawa Heart Institute, 40 Ruskin St., Ottawa, ON K1Y 4W7, Can-ada, or at [email protected].
N Engl J Med 2008;358:231-40.Copyright © 2008 Massachusetts Medical Society.
A bs tr ac t
Background
If primary percutaneous coronary intervention (PCI) is performed promptly, the procedure is superior to fibrinolysis in restoring flow to the infarct-related artery in patients with ST-segment elevation myocardial infarction. The benchmark for a timely PCI intervention has become a door-to-balloon time of less than 90 minutes. Whether regional strategies can be developed to achieve this goal is uncertain.
Methods
We developed an integrated-metropolitan-area approach in which all patients with ST-segment elevation myocardial infarction were referred to a specialized center for primary PCI. We sought to determine whether there was a difference in door-to-balloon times between patients who were referred directly from the field by para-medics trained in the interpretation of electrocardiograms and patients who were referred by emergency department physicians.
Results
Between May 1, 2005, and April 30, 2006, a total of 344 consecutive patients with ST-segment elevation myocardial infarction were referred for primary PCI: 135 direct-ly from the field and 209 from emergency departments. Primary PCI was performed in 93.6% of patients. The median door-to-balloon time was shorter in patients re-ferred from the field (69 minutes; interquartile range, 43 to 87) than in patients need-ing interhospital transfer (123 minutes; interquartile range, 101 to 153; P<0.001). Door-to-balloon times of less than 90 minutes were achieved in 79.7% of patients who were transferred from the field and in 11.9% of those transferred from emer-gency departments (P<0.001).
Conclusions
Guideline door-to-balloon-times were more often achieved when trained paramed-ics independently triaged and transported patients directly to a designated primary PCI center than when patients were referred from emergency departments.
primary percutaneous coronary intervention 69
Appendix 9: CCN Cath/PCI Working Group
COMMITTEE MEMBER AFFILIATION
Dr. Jean-Francois Marquis – Chair University of Ottawa Heart Institute
Dr. Warren Cantor Southlake Regional Health Centre
Dr. Eric Cohen Sunnybrook Health Sciences Centre
Dr. Vladimir Dzavik University Health Network
Ms. Nancy Elford Toronto East General Hospital
Dr. Dennis Ko Institute for Clinical and Evaluative Studies
Dr. Madhu Natarajan Hamilton Health Sciences Centre
Dr. James Velianou Hamilton Health Sciences Centre
Appendix 10: AcknowledgementsCCN would like to acknowledge the following people who were instrumental in the
development of the Primary Percutaneous Coronary Intervention: Optimizing Access to
Primary PCI for ST Elevation Myocardial Infarction document.
James Velianou, Hamilton Health Sciences
Jean-François Marquis, University of Ottawa Heart Institute
Mae Squires, Kingston General Hospital
Michel LeMay, University of Ottawa Heart Institute
Michelle Welsford, Hamilton Health Sciences, Paramedic Base Hospital Program
Pat Doucette, University of Ottawa Heart Institute
Pierre Poirier, Deputy Chief, Operations, Ottawa Paramedic Service
Warren Cantor, Southlake Regional Health Centre