PRIMARY PREVENTION OF CVD: Patricia Marr, PharmD ROLE OF
58
PRIMARY PREVENTION OF CVD: ROLE OF ASA AND STATIN THERAPY MAY 2019 Patricia Marr, PharmD Pharmacotherapy Specialist Toronto Western FHT Pharm Course Director, PA Program, UofT PEBC Reviewer
PRIMARY PREVENTION OF CVD: Patricia Marr, PharmD ROLE OF
FOCUSED UPDATE: ASA FOR PRIMARY PREVENTION OF CVD Objectives
Briefly discuss recent trial evidence for the use of ASA in primary prevention of CVD
Briefly review updated clinical guidelines on the use of ASA in primary prevention of CVD
Briefly list ongoing clinical studies and potential future directions Discuss considerations for clinical practice
BACKGROUND ASA has strong evidence for use for secondary prevention of CVD
Previously we had mixed study results on the use of ASA for primary prevention of CVD
Guideline organizations have different recommendations regarding ASA for primary cardiovascular prevention
ASA is commonly used for primary prevention of CVD
Recent studies have helped clarify the role of ASA in this setting
CVD = Cardiovascular Disease
ARRIVE, ASCEND, ASPREE
ARRIVE
Large RCT (~12,500) in 7 Countries ASA 100mg VS placebo Moderate CV risk patients (Mean FRS ~ 14%) No CVD, No Diabetes Mean Age: ~64yrs, Male: ~ 70%, Caucasian ~98% ~43% on STATINS Median follow up 5 years Funding: Bayer
Key Message: No significant difference in any of the efficacy endpoints. Limitation: lower than expected event rate Per Protocol Analysis (Controversial): some benefit in MI reduction
(GU/DU/GI bleeding, NSAIDS, anticoagulants, active reflux esophagitis etc)
ASCEND
Large RCT (~15,500) in UK ASA 100mg VS placebo Diabetes patients without CVD Mostly: Low (~40%) to Moderate CV Risk (~40%) Mean Age: 63yrs, Male: ~ 63%, Caucasian ~97% ~75% on STATINS, by end of trial ~ 25% on PPI Follow up 7.4 years Funded: mainly British Heart Foundation
NEJM Oct 2018 https://www.nejm.org/doi/pdf/10.1056/NEJMoa1804988
Key Message: The CV benefits were largely counterbalanced by bleeding ADRs Total Population: NNT: 91 (for composite), NNH: 111 (Fatal /Major bleed)
SVE = Significant Vascular Event
Presenter
Presentation Notes
A total of 15,480 participants underwent randomization. During a mean follow-up of 7.4 years, serious vascular events occurred in a significantly lower percentage of participants in the aspirin group than in the placebo group (658 participants [8.5%] vs. 743 [9.6%]; rate ratio, 0.88; 95% confidence interval [CI], 0.79 to 0.97; P=0.01). In contrast, major bleeding events occurred in 314 participants (4.1%) in the aspirin group, as compared with 245 (3.2%) in the placebo group (rate ratio, 1.29; 95% CI, 1.09 to 1.52; P=0.003), with most of the excess being gastrointestinal bleeding and other extracranial bleeding. There was no significant difference between the aspirin group and the placebo group in the incidence of gastrointestinal tract cancer (157 participants [2.0%] and 158 [2.0%], respectively) or all cancers (897 [11.6%] and 887 [11.5%]); long-term follow-up for these outcomes is planned. NNH fatal or major bleeding – hosp, transfusion or surger CV composite: MI, Storke, TIA, CV death … excluding ICH) ARI 0.9
Large RCT (~19,000) primarily from Australia ASA 100mg VS placebo Elderly patients without CVD Majority “Not Frail”, ~11% had Diabetes Mean Age: 74, Female: ~ 56%, Caucasian ~91% ~34% on STATINS, ~25% on PPI – at trial entry Median follow up 4.7 years (trial stopped for futility) Funding: mainly National Institute on Aging
NEJM October 2018
NEJM Oct 2018 https://www.nejm.org/doi/pdf/10.1056/NEJMoa1800722?articleTools
No benefit in all cause death, dementia, persistent physical disability But there was increased risk of major bleeding. Major Bleeding NNH =97 Reminder: they excluded patients at “high risk for bleeding”
Presenter
Presentation Notes
ARI 1.03 (about 1% absolute increase risk of bleed_
Increased risk of all cause death (NNH = 143) Surprisingly – death related to cancer was increased (NNH 125) Was this a chance finding?
UPDATED META-ANALYSIS
NNT: 333
NNH: 250
NNH: 1000
No significant benefit if limit analysis to recent trials
Presenter
Presentation Notes
Unless provided in the caption above, the following copyright applies to the content of this slide: Published by Oxford University Press on behalf of the European Society of Cardiology 2018.This work is written by US Government employees and is in the public domain in the US. Excluded 2 trials with low ankle brakial index Popadad primary analysis: reduced ankle brakial index … but did secondary analysis and didn’t find a diff Also JAMA meta analysis … similar results … 2019
UPDATED GUIDELINES
2019 ACC/AHA GUIDELINE ON THE PRIMARY PREVENTION OF CVD
Age 40-70yrs Low Dose ASA might be considered for primary prevention in select higher ASCVD adults who are not at increased bleeding risk.
Age > 70yrs Low-dose ASA should NOT be administered on a routine basis for primary prevention
Patients at increased risk of bleeding (any age) Low-dose ASA should NOT be administered for primary prevention
For decades, low-dose aspirin (75-100 mg with US 81 mg/day) has been widely administered for ASCVD prevention. By irreversibly inhibiting platelet function, aspirin reduces risk of atherothrombosis but at the risk of bleeding, particularly in the gastrointestinal (GI) tract. Aspirin is well established for secondary prevention of ASCVD and is widely recommended for this indication, but recent studies have shown that in the modern era, aspirin should not be used in the routine primary prevention of ASCVD due to lack of net benefit. Most important is to avoid aspirin in persons with increased risk of bleeding including a history of GI bleeding or peptic ulcer disease, bleeding from other sites, age >70 years, thrombocytopenia, coagulopathy, chronic kidney disease, and concurrent use of nonsteroidal anti-inflammatory drugs, steroids, and anticoagulants. The following are recommendations based on meta-analysis and three recent trials:Low-dose aspirin might be considered for primary prevention of ASCVD in select higher ASCVD adults aged 40-70 years who are not at increased bleeding risk. Low-dose aspirin should not be administered on a routine basis for primary prevention of ASCVD among adults >70 years. Low-dose aspirin should not be administered Examples Age > 70 years Conditions / PMH: GI bleeding, PUD, history of bleeding from other sites, CKD, coagulopathy, thrombocytopenia Meds: NSAIDs, steroids, anticoagulants for primary prevention among adults at any age who are at increased bleeding risk
FUTURE STUDIES AND OUTSTANDING QUESTIONS Do we need new cardiovascular risk calculators?
Will ASA provide additional benefit to STATIN therapy? Ongoing Study: ACCEPT-D (DM patients on Simvastatin)
Optimal dose of ASA (to balance efficacy VS safety)? Is it the same for everyone? Ongoing: ANDAMAN (Daily VS BID), ADAPTABLE (81mg VS 325mg)
Are there specific populations that may benefit from ASA? Prediction tools to help us select patients? (efficacy + safety).
Will ASA be (partially) resurrected for primary prevention?
Presenter
Presentation Notes
Could lower doses be used? Weight based dosing Prediction tools to help us select patients (factoring in efficacy / safety). Annals of Internal Med 2019
APPLICATION TO PRACTICE
SHARING A REAL LIFE CASE
Presenter
Presentation Notes
pinpointing an individual patient's 10-year CV risk is difficult (given the controversies about accuracies of risk calculators), and individualizing 10-year risk for major bleeding is equally difficult. An alternative perspective would be for clinicians to inform patients that the most-recent trials — performed in contemporary patient populations — weigh against a net benefit for aspirin in primary prevention, regardless of baseline CV risk. https://www.jwatch.org/na48372/2019/02/06/aspirin-primary-prevention-new-meta-analysis
NEJM COMMENTARY: Dr Schwenk and Dr Brett (Deputy editor/ Editor in Chief NEJM)
“pinpointing an individual patient's 10-year CV risk is difficult (given the
controversies about accuracies of risk calculators), and individualizing
10-year risk for major bleeding is equally difficult. An alternative
perspective would be for clinicians to inform patients that the most-recent
trials — performed in contemporary patient populations — weigh
against a net benefit for aspirin in primary prevention, regardless of
“For secondary prevention, in which risk is determined largely by the extent of atherosclerotic disease, the benefits of aspirin outweigh the risks of bleeding. In contrast, for primary prevention, in which risk is determined largely by age and the presence or absence of diabetes, the benefit–risk ratio for prophylactic aspirin in current practice is exceptionally small. Thus, beyond diet maintenance, exercise, and smoking cessation, the best strategy for the use of aspirin in the primary prevention of cardiovascular disease may simply be to prescribe a statin instead.”
NEJM COMMENTARY: Dr Paul Ridker, Center for CV Disease Prevention, Brigham and Women’s Hospital, Boston
“Thus, beyond diet maintenance, exercise, and smoking cessation,
the best strategy for the use of aspirin in the primary prevention of
cardiovascular disease may simply be to prescribe a statin instead.”
https://www.nejm.org/doi/pdf/10.1056/NEJMe1812000
Presenter
Presentation Notes
“For secondary prevention, in which risk is determined largely by the extent of atherosclerotic disease, the benefits of aspirin outweigh the risks of bleeding. In contrast, for primary prevention, in which risk is determined largely by age and the presence or absence of diabetes, the benefit–risk ratio for prophylactic aspirin in current practice is exceptionally small. Thus, beyond diet maintenance, exercise, and smoking cessation, the best strategy for the use of aspirin in the primary prevention of cardiovascular disease may simply be to prescribe a statin instead.”
https://www.aafp.org/fpm/2017/0500/p5.html What is not Shared Decision Making Shared decision making is simply a process that aids a physician and patient in selecting the optimal test or treatment for the patient. It involves a bidirectional flow of information. (See “Shared decision making vs. usual care.”) The physician provides information about the disease, the screening service, and risks and benefits; the patient provides his or her thoughts and values; and together they make a decision. Shared decision making is distinct from informed decision making, where the physician provides information to the patient and then the patient makes the decision. Enlarge Print SHARED DECISION MAKING VS. USUAL CARE Although shared decision making is not appropriate in clinical scenarios where the medical treatment is clear, such as antibiotics for meningitis or anticoagulation for a pulmonary embolus, it proves beneficial in situations where more than one treatment or screening decision is valid A recent Cochrane review found that, compared with regular care, use of decision aids had the following results:7 Increased patients' knowledge, Increased the proportion of people who had an accurate risk perception of the disease, Increased the proportion of people who chose an option that was in line with their values, Decreased decisional conflict, Had a positive effect on clinician-patient communication, Had a variable effect on length of visit (from −8 minutes to +23 minutes, with a median increase of 2.5 minutes per visit).
STATINS FOR PRIMARY PREVENTION OF CVD
FOCUSED UPDATE: STATINS FOR PRIMARY PREVENTION OF CVD Objectives: Briefly review efficacy of STATIN therapy for Primary Prevention of CVD
Describe new evidence related to the use of STATINs for primary prevention in elderly patients
Briefly review potential safety risks with STATIN therapy
Introduce select controversies throughout the talk
Discuss considerations for clinical practice
Presenter
Presentation Notes
Objectives Review recent trial evidence for the use of ASA in primary prevention of CVD Review updated clinical guidelines on ASA use for primary prevention of CVD Briefly review ongoing clinical studies and potential future directions Discuss considerations for clinical practice
BACKGROUND: STATINS
Statins are the single most commonly prescribed class of treatment in the developed world
One of the most studied therapeutic classes of medications
Secondary prevention: standard of care. Strong evidence
Statins are the single most commonly prescribed class of treatment in the developed world, (10s of millions if not hundreds of millions) - https://www.bmj.com/content/348/bmj.g3306/rr/759401 Heated discussions about the role of Guidelines have tended to expand the number of people eligible for the drugs Almost 2/3 of people taking statins for primary prevention (BMJ Open 2019 Byrne Guidelines from the US, UK, Europe and Canada – have differing recommendations regarding which patients to treat with medications for primary preventions Diversity may reflect controversies and remaining gaps in literature
RATIONAL PRESCRIBING
Indication
Efficacy
Safety
Dosing / Monitoring / Targets
Adherence and Other Factors
WHAT IS THE RIGHT RISK THRESHOLD? Guidelines from the around the world have different recommendations for STATIN use for primary prevention
What is the right risk threshold to recommend (offer) STATIN therapy? (And is there a best way to calculate risk?)
Most RCTs have included patients with ≥ 2 risk factors … although many patients who qualify for drug therapy may not have 2 risk factors
Should age alone be reason enough to initiate treatment?
Controversial: Swiss Modeling Study Suggests STATINs are overprescribed for primary prevention. Looked at benefits VS risks of therapy Suggest a higher risk threshold be used Annals of Internal Med 2019 https://annals.org/aim/article-abstract/2717730/finding-balance-between-benefits-harms-
Used an approach developed by investigators at the National Cancer Institute, the authors projected disease related events and drug related adverse events over time while accounting for competing mortality Criticized – incl 10 year risk fo CVD at which STATINS provide at least a 60% probability of net benefit was 14% uded a wide range of adverse events such as hemorrhagic stroke, acute kindney injustry Guidelines vary on their proposed risk thresholds for treatment Whether they single out lipid levels as a key factor to guide initiation How to calculate risk And also desireable targets JAMA article ACC / AHA would lead to treatment of an estimated 10 million more patients VS USPSTF guideline UPSTF would recommend statins more than Canadian guidelines or European For instance the ACC / AHA risk calculation leatds to treatment as men become older even if they have no risk factos other ahan their unmodificiable age and sex To many it sounds absurd that there is no such things as healthy aging and that everyone eventually will need some medication Nice guidelines do so up to the age of 84 yrrs … because everyone > 75 years of age exceeds the 10% 10 year QRISK2 threshold – the NICE guidliens indirectely provide a strong universal statin indication over the range of 76 – 84. This guideline also provides a specific treatment recommendation for Atorva 20mg in patients >85 … reduce risk of non-fatal MI Most RCTs have included patients with at least 2 or more risk factors … although many patients who qualify for drug therapy may not have 2 risk factors ___________ ACC/ AHA 2019 – 20-75 etc
Dr John P.A. Ioannidis (Stanford): Response to the New ACC / AHA Guidelines (2013)
“It is uncertain whether this would be one of the
greatest achievements or one of the worst disasters
of medical history”
More Than A Billion People Taking STATINs? Potential Implications of the New Cardiovascular Guidelines. https://jamanetwork.com/journals/jama/fullarticle/1787389
RD = Risk differences were the number of events that wold be prevented or increased per 1000 people treated with statins over 10 yrs Systematic review published in family practice 2018 -
EFFICACY: SELECT CONTROVERSIES Quality of Trial data? Influence of Drug Industry?
True Mortality Benefit?
Composite outcomes?
Should we be pooling data from heterogenous studies?
Should we analyze / present data based on level of CVD risk?
What is the True (Real World) Efficacy? Trial F/U generally < 5 years. But for many patients STATIN is lifelong.
Data for Populations: Elderly, Women, Non-Caucasian?
Presenter
Presentation Notes
Quality of the Studies (particulary pre 2005/2006)
Geriatric Experts Across Canada Drug Classes Identified As A High Priority For Deprescribing Guideline Development
Presenter
Presentation Notes
65 Geriatrics Experts From Across Canada (Pharm, Family MD, Geriatricians, NPs_ - participated in the survey Underwent modified delphi process Literature review to identify list of potentially inappopriate medications Expert panel developed survey Survey administered to geriatric experts across canada. Survey 1: 29 drug classes – 14 reaching consensus (> 70%) Survey 2: Survey 3 Interestingly #11 is bisphosponates – 17% …. Need at least 70% concensus 3
~ 6500 patients > 75 without CVD ie, major coronary events, strokes, and coronary revascularisations) Interpretation Statin therapy produces significant reductions in major vascular events irrespective of age, but there is less direct evidence of benefit among patients older than 75 years who do not already have evidence of occlusive vascular disease. This limitation is now being addressed by further trials.
Only group to benefit: patients 75-84yrs with Type 2 DM
Presenter
Presentation Notes
Retrospective study, researchers in Spain used a primary care database to determine whether initiating statins for primary prevention lowers risks for atherosclerotic CVD and all-cause death in old and very old adults. Participants were 47,000 elders (age, ≥75) without clinically recognized atherosclerotic CVD. 16% started statins. Median follow-up was 7.7 years. After multivariable adjustment, statins did not lower risks for atherosclerotic CVD and all-cause death among participants without diabetes. Among participants with type 2 diabetes who were 75 to 84, statins significantly lowered risks for atherosclerotic CVD (from 29 to 24 events/1000 person-years) and all-cause death (from 55 to 42 deaths/1000 person-years); among participants with type 2 diabetes who were 85 or older, statins did not lower risks for CVD and all-cause death.
STAREE: STATIN THERAPY FOR REDUCING EVENTS IN THE ELDERLY Randomized Control Trial
Healthy elderly people (≥70 years). No history of CVD. N =18,000
Intervention: Atorvastatin 40mg/day VS placebo
Primary Outcomes: Death, development of dementia, development of disability Major fatal or non-fatal CV event.
Estimated completion 2023
https://clinicaltrials.gov/ct2/show/NCT02099123
Presenter
Presentation Notes
The STAREE study will examine whether treatment with statin (atorvastatin 40mg) compared with placebo will prolong overall survival or disability free survival amongst healthy elderly people (≥70 years).�
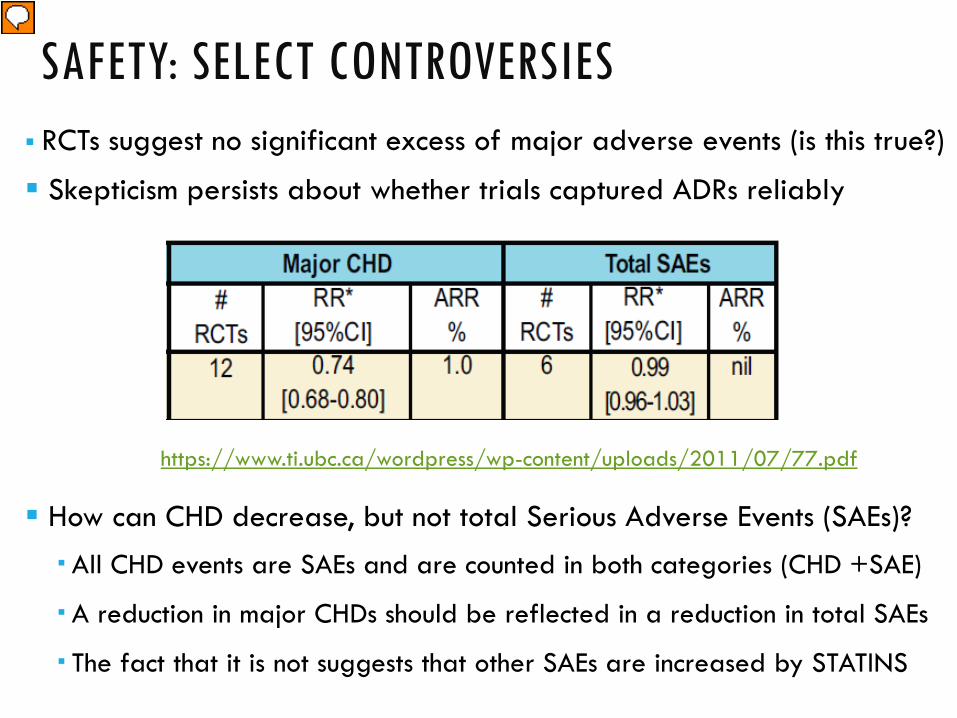
https://jamanetwork.com/journals/jama/fullarticle/2645741 All CHD events are serious adverse events and are counted in both categories, A reduction in major CHD SAEs should be reflectied in a reduction in total SAEs The fact that it is not suggests that other SAEs are increased by STATINS
MAYO Clinic Shared Decision Aid Video: https://www.bing.com/videos/search?q=statin+shared+decision+aid&&view=detail&mid=550673C6C6530976E302550673C6C6530976E302&&FORM=VRDGAR Online Tool: https://statindecisionaid.mayoclinic.org/
Best CV risk Calculator: http://chd.bestsciencemedicine.com/calc2.html