Embed Size (px)
Citation preview

Original Studies
Primary Stenting of De Novo Lesions in Small CoronaryArteries: A Prospective, Pilot Study
Rene Koning, 1* MD, Charles Chan, 2 MD, Helene Eltchaninoff, 1 MD, Christophe Tron, 1MD,Satej Janorkar, 1 MD, Vivek Gupta, 1 MD, and Alain Cribier, 1 MD
Technical advancement and new anti-thrombotic regimens have recently shown so muchimprovement in the results of coronary stenting that the conventional contra-indicationfor stenting in small coronary arteries ( F3 mm) needs to be revised. We undertook aprospective pilot study of elective Palmaz-Schatz stenting in de novo lesions located incoronary arteries of less than 3 mm diameter. Fifty consecutive patients (63 6 9 years)with stable (n 5 38) and unstable angina (n 5 12) were included. Philips-DCI quantitativecoronary analysis was used to measure reference diameter, minimal lumen diameter andpercent diameter stenosis before PTCA, after stenting and at 6-month angiographicfollow-up study. All measurements were performed after intracoronary injection ofnitroglycerin (300 mg). All patients received ticlopidine (250 mg/day) and aspirin (100mg/day). The mean lesion length was 9 6 3 mm. The balloon size used for stent deliverywas 2.75 mm in 30 patients and 2.5 mm in 20 patients and the mean balloon inflationpressure used for stent deployment was 12 6 2 atm. All stents were deployed success-fully. In-hospital complications occurred in two patients, diagonal branch occlusion at day2 requiring emergency PTCA in one and a hematoma at the femoral puncture site requiringsurgery in the other. Major adverse cardiac event (MACE) rate remained 2% (nonfatalinfarct in one). Follow-up angiography (n 5 46, 92%) at 6 6 3 months showed a 30%restenosis rate. Target vessel revascularization (TVR) rate was 13%. We conclude thatelective stenting in small coronary arteries is feasible and involves an acceptable risk ofrestenosis. Cathet. Cardiovasc. Diagn. 45:235–238, 1998 . r 1998 Wiley-Liss, Inc.
Key words: coronary stenting; small coronary artery; de novo lesions
INTRODUCTION
Coronary stenting is useful for the treatment of acute orthreatened closure after percutaneous transluminal coro-nary angioplasty (PTCA) and has shown to reduce therestenosis rate in certain subsets of patients. However,stenting in small coronary arteries (,3 mm) has beendeclined by the ACC guidelines [1] in 1996 because ofhigher restenosis and subacute occlusion rates. Neverthe-less, recent advances in stent technology and newlyavailable anti-thrombotic regimens could give us newinsight into the indication of coronary stenting in smallsized coronary arteries. Thus, we conducted a prospectivestudy to assess the feasibility, safety and mid-term resultsof coronary stenting in de novo lesions located in smallcoronary arteries,3 mm in diameter.
METHODS
Patient Selection
Patients with symptomatic ischemic heart diseaseadmitted in our hospital between May 1995 and Decem-ber 1996 were considered for inclusion. The criteria forenrollment were the presence of a significant lesion(.50% diameter stenosis),#15 mm length, suitable for
1Department of Cardiology, Hospital Charles-Nicolle, Universityof Rouen, France.2National Heart Centre of Singapore, Singapore.
*Correspondence to: Dr. Rene´ Koning, MD, Service de Cardiologie,Hopital Charles-Nicolle, 1 rue de Germont, 76000 Rouen, France.
Received 16 March 1998; Revision accepted 4 June 1998
Catheterization and Cardiovascular Diagnosis 45:235–238 (1998)
r 1998 Wiley-Liss, Inc.

stenting and located in a coronary artery with referencediameter of,3 mm on quantitative angiographic measure-ments. Exclusion criteria were myocardial infarctionwithin 15 days, contra-indication to aspirin and/or ticlopi-dine, left ventricular ejection fraction#40%, need of aballoon with $3 mm diameter for stent deployment,evidence of thrombus at the lesion site, ostial lesion,lesion involving a major side branch, severe vesseltortuosity, lesion length.15 mm and reference diameterat the lesion site$3 mm.
The study was approved by the hospital ethical commit-tee. Informed consent was obtained from all the patientsbefore inclusion.
Coronary Angiographic Analysis
On-line angiographic measurements (pre-PTCA, post-PTCA, poststenting and at follow-up) were performed intwo nearly orthogonal views after intracoronary adminis-tration of 300 µg of nitroglycerin. A Philips digitalcomputerized system was used for quantitative coronaryangiographic (QCA) analysis. Reference diameter (RD)at the lesion site, minimal lumen diameter (MLD), andpercent diameter stenosis (%DS) were expressed as themean value of the measurements. Vessel edges weredetermined by the computerized algorithm, and lumendimensions were measured using the guiding catheter as ascaling reference. Reference diameter of the vessel wasautomatically calculated by the software. Acute gain wasdefined as the difference between the MLD immediatelyafter stent implantation and the MLD before the proce-dure, and late loss was defined as the difference betweenthe MLD immediately after stent implantation and MLDat follow-up. In addition, the proximal and distal coro-nary artery diameters within 5 mm of the automaticallydetected stenosis edges were measured for confirmationof the ,3 mm vessel size. The lesion morphology wasclassified according to the ACC/AHA classification.
Angioplasty, Stent Placement Protocol andFollow-up
All patients received an intracoronary bolus of 10,000IU of heparin at the beginning of the procedure. Theballoon size was determined according to the referencediameter of the coronary artery to obtain a balloon tocoronary diameter ratio close to 1. Compliant or noncom-pliant balloons of 2.5 mm diameter and noncompliantballoons of 2.75 mm diameter were used. Palmaz-Schatzstents (PS 104, 9 mm length, or PS 153, 15 mm length)were manually crimped over the same balloon which wasused for predilatation. A balloon inflation pressure$8atm (mean, 126 2) was used for stent delivery. Nosecond balloon was used for postdelivery high pressureinflation. Poststent medical management included ticlopi-dine (250 mg/day if weight,85 kg, 500 mg/day if weight
$85 kg) and aspirin (100 mg/day). Ticlopidine wasintroduced at the time of stent implantation and continuedfor 1 month.
Clinical events, electrocardiograms (ECG) and cre-atine kinase-MB (CK-MB) were monitored daily duringhospitalization. Major adverse cardiac events (MACE)included death, myocardial infarction, coronary bypasssurgery or repeat angioplasty during hospitalization.QCA follow-up at 6 months was scheduled. Angiographicrestenosis was defined as a percent diameter stenosis$50% inside and just adjacent to the proximal and distalend of the stent. Target vessel revascularization (TVR)was defined as repeat angioplasty or bypass surgeryperformed because of restenosis during follow-up.
RESULTS
Clinical Characteristics
The study population included 50 consecutive patients,36 men and 14 women with a mean age of 636 9 years.Thirty eight patients presented with stable angina and 12with unstable angina. Sixteen patients had an old Q ornon-Q wave myocardial infarction and three were withprior coronary artery bypass graft surgery. Major riskfactors were diabetes mellitus in 12 patients (24%),hypertension in 23 (46%), hypercholesterolemia in 21(42%) and cigarette smoking in 23 (46%).
Angiographic Characteristics
The lesions according to the ACC/AHA classificationwere type A, 18; type B1, 18; type B2, 11; and type C, 3.The lesion sites were as follows: left anterior descendingartery (n 5 18), circumflex artery (n5 13), rightcoronary artery (n5 13), first diagonal branch (n5 3),obtuse marginal branch (n5 2), and protected left mainartery (n5 1). The mean lesion length was 9.46 3.1 mm.The mean left ventricular ejection fraction was 636 9%.
For stent delivery, 2.75 mm diameter noncompliantballoons were used in 30 patients and 2.5 mm compliantor noncompliant balloons in 20. A 9 mm long Palmaz-Schatz stent (PS 104) was used in 24 patients and a 15mm long articulated stent (PS 153) in 26. The meanballoon inflation pressure used for stent deployment was12 6 2 atm. QCA data are shown in Table I. The meanacute gain in MLD was 1.576 0.44 mm.
In-hospital Course
In-hospital course was uneventful in 48 of 50 patients.Complications occurred in two patients, a non-Q wavemyocardial infarction on the second day due to theocclusion of a stented diagonal branch in one patient anda hematoma at the puncture site in the other. An emer-gency PTCA was carried out in the first and a groinsurgery in the other with a subsequent uneventful out-
236 Koning et al.

come in both the patients. The mean hospital stay of allpatients was 2.66 1.1 days.
Follow-up
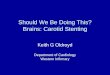
All patients were examined at 6 months follow-upeither at hospital (46; 92%) or by the referring cardiolo-gists (4; 8%) in their clinics. Forty-six patients (92%)underwent an angiographic study at 6.46 3.3 months. Nototal coronary occlusion was observed in any patient.Angiographic restenosis was present in 30% of patients(n 5 14). Of these 14 patients, 12 had in-stent restenosiswhile two had peri-stent restenostic lesions which wereseen just after the distal end of stent. Six patients (13%)underwent repeat revascularization in the form of balloondilation. The mean late loss in MLD was 0.796 0.67mm. Follow-up QCA data are listed in Table I andcumulative distribution of MLD at pre-PTCA, poststentand follow-up is shown in Figure 1. The overall MACErate was 2% including non-Q myocardial infarction inone patient and the TVR rate was 13% (n5 6).
DISCUSSION
Elective stenting of lesions in small coronary arteries isof particular interest because these arteries are frequentlyinvolved in PTCA procedures. To our knowledge, noprospective data are available in this context. The currentstudy demonstrates that coronary stenting is feasible andsafe in the small vessels,3 mm diameter. The restenosisrate of 30% and the TVR of 13% compare favourablywith those reported with the stenting in larger vessels (.3mm diameter). A combination of antiplatelet agents,aspirin and ticlopidine is an effective therapeutic strategyafter coronary stenting in small vessels.
Previous Studies
Scanty data are available in the literature which couldonly be extrapolated to the concept of elective stenting inthe small coronary arteries,3 mm diameter. Roubin etal. [2] have reported a very high (77%) subacute stentthrombosis rate in bail-out situations with the stenting invessels of 2.5 mm diameter. Similarly, poststenting MLDof 3.25 mm was found to be an independent predictor forsubacute thrombosis as well as for restenosis by Fajadet
et al. [3]. Nevertheless, bail-out stenting in small coro-nary arteries did show good immediate results [4]. In theFrench multicentric study [5], stent-thrombosis occurredin 10% patients in whom the balloon used was,3 mmdiameter. Moreover, Goods et al. [6] reported a subacuteclosure rate of 0.9% in a series of 369 patients including ahigh percentage (57%) of small (#3 mm) coronaryarteries.
The BENESTENT and STRESS [7,8] studies whichwere largely designed to treat the coronary arteries.3mm diameter have also made a comparative remark aboutthe stenting in smaller and larger vessels. Since thestudies were multicentric, the data collected from all thecentres happened to show the inclusion of smaller vessels,3 mm diameter but which were treated with theballoons .3 mm diameter. The retrospective meta-analysis of this data showed that the restenosis ratefollowing stenting or PTCA alone was higher in thecoronary arteries,3 mm diameter than those observed inlarger vessels (.3 mm). However, stents had a greaterimpact in increasing the clinical benefits in smaller ratherthan in large coronary arteries [7]. In the extendedconclusion of STRESS I-II, Savage et al. [9] havementioned that elective stent placement provides superiorangiographic and clinical outcomes to balloon angio-
Fig. 1. Cumulative distribution of MLD (minimal lumen diam-eter). Pre-PTCA (percutaneous transluminal coronary angio-plasty), poststenting and at 6 month follow-up.
TABLE I. Quantitative Angiographic Data Pre-PTCA, Post-PTCA, Poststenting and at 6 Months Follow-up
n Reference diameter (mm) Minimal lumen diameter (mm) % Diameter stenosis Proximal diameter (mm) Distal diameter (mm)
Pre-PTCA 50 2.666 0.23 0.876 0.28 666 11 2.766 0.28 2.646 0.33Post-PTCA 50 2.656 0.26 1.696 0.33 366 13 2.796 0.36 2.606 0.32Poststenting 50 2.816 0.24 2.446 0.36 166 9 2.936 0.29 2.776 0.34Follow-up 46 2.656 0.30 1.636 0.56 386 21
No restenosis 32 2.646 0.27 1.916 0.41 266 12Restenosis 14 2.726 0.33 1.016 0.29 636 9
PTCA, percutaneous transluminal coronary angioplasty.
Stenting in Small Coronary Arteries 237

plasty in vessels slightly smaller than 3 mm. But theprospective comparison of stent placement and balloonangioplasty for small coronary arteries remains to bestudied.
Present Study
In our prospective study, the mean RD at the lesion sitewas 2.66 0.2 mm. The proximal and distal coronarydiameters as well as the balloon size chosen for stentdeployment were,3 mm in all cases. The mean ballooninflation pressure for stent delivery was 126 2 atm. Aknown inherent risk of coronary dissection in smallvessels and also a use of conventional 20 mm longballoon for short stent delivery in our series compelled usnot to use higher pressure to deploy a stent. During theinitial part of this experience, we intended to use shorter(9 mm long) Palmaz-Schatz stents to avoid the high riskof thrombogenicity involved with the use of longer stents.However, the satisfactory immediate results of initialexperience encouraged us to use the longer (15 mm)stents in further patients who had longer lesions.
Immediate clinical and angiographic results (100%) inthis study were as good as those observed in coronaryarteries$3 mm diameter. The 6 month restenosis rate of30% and TVR of 13% are clearly comparable with that ofstenting in coronary arteries$3mm diameter.
Limitations
The patients in this study had moderately small vessels(2.50 to 2.75 mm). This study does not address the benefitand risk of stenting in very small vessels (,2.5 mm). Thisstudy is nonrandomized, prospective study without acontrol group of patients not receiving stents. The relativeimportance of the factors responsible for the resultsachieved, i.e., the use of ticlopidine or that of high-pressure inflation, cannot be determined from presentstudy. Intravascular ultrasound-guided stent deploymentwas not used in this study. In demonstrating that coronarystenting is effective in establishing and maintaining smallcoronary artery (,3 mm diameter) patency withoutsignificant ischemic or vascular complications, the pre-sent study may be considered a pilot study before
randomized clinical trials can evaluate the short- andlong-term efficacy of stenting in small coronary arteries.
REFERENCES
1. Pepine CJ, Holmes DR, Block PC, Mullines CE, Brinker JA, MarkDB, Mullins CE, Nissen SE, Topol EJ, Williams DO, Goldberg S,Hirshfeld JW, Serruys PW: Coronary artery stents: ACC ExpertConsensus Document. J Am Coll Cardiol 28:782–794, 1996.
2. Roubin GS, Cannon AD, Agarwal SK, Macander PJ, Dean LS,Baxley WA, Breland J: Intracoronary stenting for acute andthreatened closure complicating percutaneous transluminal coro-nary angioplasty. Circulation 85:916–927, 1992.
3. Fajadet F, Doucet S, Caillard J, Cassagneau B, Robert G, Marco J:Predictors of restenosis after Palmaz-Schatz implantation (abstract).Circulation 86:I-531, 1992.
4. Chan CN, Tan AT, Koh TH, Koh P, Lau KW, Gunawan SA,Chakroborty B, Ng A: Intracoronary stenting in the treatment ofacute or threatened closure in angiographically small coronaryateries (,3 mm) complicating percutaneous transluminal coronaryangioplasty. Am J Cardiol 75:23–25, 1995.
5. Karrillon GJ, Morice MC, Benveniste E, Bunouf P, Aubry P, CattonS, Chevalier B, Commeau P, Cribier A, Eiferman C, Grollier G,Guerin Y, Henry M, Lefevre T, Livarek B, Louvard Y, Marco J,Makowski S, Monassier JP, Pernes JM, Rioux P, Spaulding C,Zemour G: Intracoronary stent implantation without ultrasoundguidance and with replacement of conventional anticoagulation byantiplatelet therapy: 30 day clinical outcome of the French Multicen-ter registry. Circulation 94:1519–1527, 1996.
6. Goods CM, Al-Shaibi KF, Yadav SS, Liu MW, Negus BH, Iyer SS,Dean LS, Jain SP, Baxley WA, Parks MJ, Sutor RJ, Roubin GS:Utilization of the coronary balloon-expandable coil stent withoutanticoagulation or intravascular guidance. Circulation 93:1803–1808, 1996.
7. Wong SC, Hirschfeld J, Teirstein P, Schatz R, Shaknovich A,Nobuyoshi M, Satler LF, Chuang YC, Leon MB: Differential impactof stent versus PTCA on restenosis in large (.3 mm) and small (,3mm) vessels in the stent restenosis study (abstract). J Am CollCardiol 25:375A, 1995.
8. Azar AJ, Detre K, Goldberg S, Kiemeneij F, Leon MB, Serruys PWon behalf of the Benestent and Stent Restenosis study. A meta-analysis on the clinical and angiographic outcomes of stents vs ptcain the different coronary vessel sizes in the Benestent-1 andStress-I/II trials (abstract). Circulation 92 (suppl 1):I-475, 1995.
9. Savage MP, Fischman DL, Rake R, Leon MB, Schatz RA, Penn I,Nobuyoshi M, Moses J, Hirshfeld J, Heuser R, Baim D, Cleman M,Brinker J, Gebhardt S, Goldberg S for the STRESS investigators:Efficacy of coronary stenting versus balloon angioplasty in smallcoronary arteries. J Am Coll Cardiol 31:307–311, 1998.
238 Koning et al.