Embed Size (px)
Citation preview
Cheri Lattimer RN, BSNExecutive DirectorNational Transitions of Care CoalitionWashington, DC
Sahil Khanna, MBBSAssociate Professor of MedicineGastroenterology and HepatologyMayo ClinicRochester, MN
Nancy C CarallaFounder and Executive DirectorC Diff FoundationNew Port Richey, FL
James E Lett, II, MD, CMDFamily Medicine PhysicianMedical DirectorAvar ConsultingRockville, MDDirector of the National BoardNational Transitions of Care CoalitionWashington, DC
Kevin W Garey, PharmDProfessor and Chair Department of Pharmacy Practice and Translational ResearchUniversity of HoustonHouston, TX
This activity is provided by PRIME Education. There is no fee to participate. This activity is supported by an educational grant from Merck & Co. Inc.
Interprofessional Steering Committee

© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
Table of Contents
INTRODUCTION....................................................................................................................................................................................
PURPOSE AND SCOPE........................................................................................................................................................
GUIDING PRINCIPLES IN TRANSITIONS OF CARE.........................................................................................................................
THE BURDEN OF CDI ON PATIENTS, HEALTH CARE PROFESSIONALS, AND HEALTHCARE FACILITIES...................................
What is Clostridioides difficile?................................................................................................................................................
How Does CDI Impact Patients’ Lives?.............................................................................................................. ........
What CDI Epidemiology Trends Should Health care Professionals Be Aware Of?...............................................................
What is the Impact of CDI on Healthcare Facilities?..............................................................................................................
GUIDELINE-RECOMMENDED CDI DIAGNOSIS, TREATMENT, AND MANAGEMENT...................................................................
What are the Risk Factors for CDI?.........................................................................................................................................
How can we Prevent CDI in Healthcare and Community Settings?......................................................................................
How is CDI Diagnosed?...........................................................................................................................................................
Point-of-Care Algorithm for CDI Testing.............................................................................................................
How Would You Manage Primary CDI?..................................................................................................................................
How Would You Manage Recurrent CDI?...............................................................................................................................
Point-of-Care Algorithm for CDI Treatment........................................................................................................
CONSIDERATIONS IN TRANSITIONS OF CARE...............................................................................................................................
BARRIERS TO EFFECTIVE CARE TRANSITIONS IN CDI.................................................................................................................
System-Level Barriers..............................................................................................................................................................
Clinician-Level Barriers............................................................................................................................................................
Patient-Level Barriers...............................................................................................................................................................
STRATEGIES FOR OPTIMIZING CDI CARE TRANSITION PATHWAYS...........................................................................................
Identify the Transition Team.....................................................................................................................................................
Empower Patients....................................................................................................................................................................
Point-of-Care Resource for Patient Education..................................................................................................
Create Discharge Management and Protocols......................................................................................................................
Point-of-Care Checklist for Transitions of Care Assessment and Coordination..........................................
REFERENCES........................................................................................................................................................................................
3
3
3
4
4
4
4
5
5
5
6
7
8
9
10
12
13
13
13
14
14
15
15
16
19
20
23
2
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
INTRODUCTIONPURPOSE AND SCOPE
The purpose of this transitions of care (TOC) guide is to describe pathways that enable patients with Clostridioides difficile infection (CDI) and health care professionals managing such patients to coordinate care across multidisciplinary health care settings. The guide—developed by an expert interprofessional steering committee that includes a primary care provider, a gastroenterologist, a pharmacist, a case manager/nurse navigator, and a CDI patient representative—provides strategies, tools, and resources to support the implementation of collaborative team-based approaches for CDI management.
Health care providers, patients, and caregivers can use this guide to learn about strategies that can be applied by the interprofessional team to prevent primary CDI, reduce of the risk of recurrences, and mitigate hospital readmissions following CDI treatment.
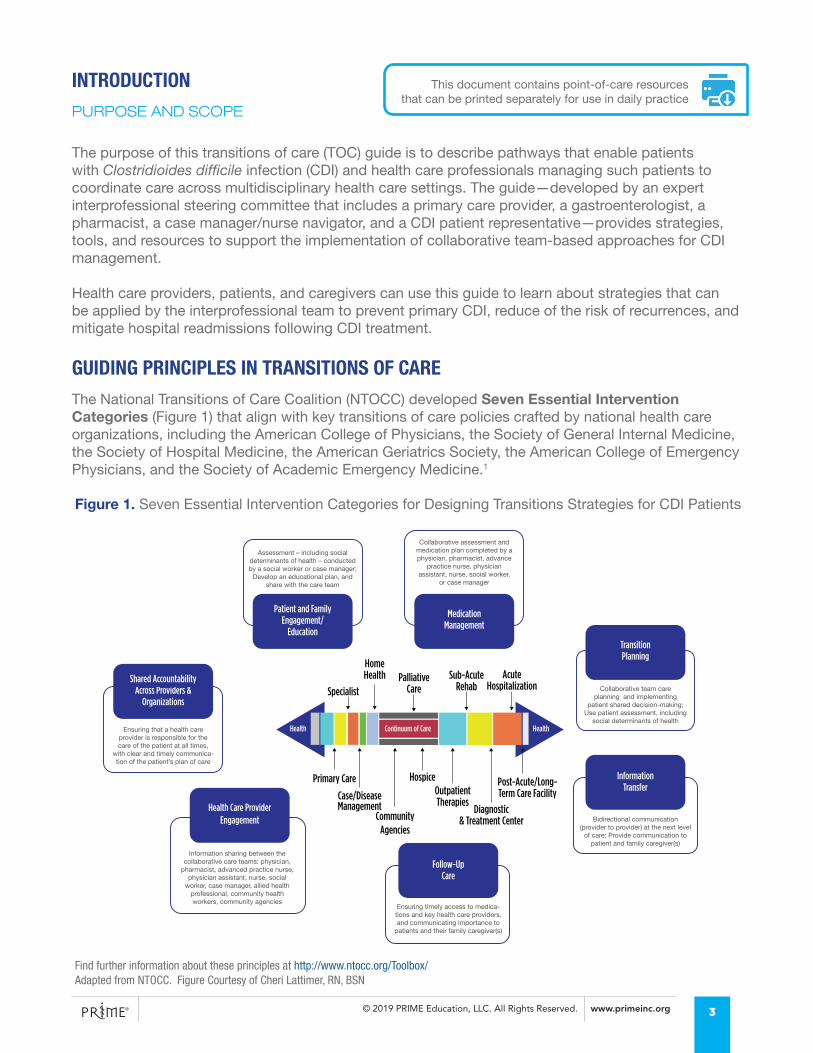
GUIDING PRINCIPLES IN TRANSITIONS OF CAREThe National Transitions of Care Coalition (NTOCC) developed Seven Essential Intervention Categories (Figure 1) that align with key transitions of care policies crafted by national health care organizations, including the American College of Physicians, the Society of General Internal Medicine, the Society of Hospital Medicine, the American Geriatrics Society, the American College of Emergency Physicians, and the Society of Academic Emergency Medicine.1
TransitionPlanning
Specialist
Home Health Palliative
CareSub-Acute
RehabAcute
Hospitalization
Post-Acute/Long-Term Care Facility
Diagnostic& Treatment Center
OutpatientTherapies
Hospice
CommunityAgencies
Case/Disease Management
Primary Care
Shared Accountability Across Providers &
Organizations
Assessment – including social determinants of health – conducted by a social worker or case manager;
Develop an educational plan, and share with the care team
Collaborative assessment and medication plan completed by a physician, pharmacist, advance
practice nurse, physician assistant, nurse, social worker,
or case manager
Collaborative team careplanning and implementing
patient shared decision-making; Use patient assessment, including
social determinants of health
Bidirectional communication (provider to provider) at the next level
of care; Provide communication to patient and family caregiver(s)
Ensuring timely access to medica-tions and key health care providers, and communicating importance to
patients and their family caregiver(s)
Information sharing between the collaborative care teams: physician,
pharmacist, advanced practice nurse, physician assistant, nurse, social
worker, case manager, allied health professional, community health workers, community agencies
Ensuring that a health care provider is responsible for the care of the patient at all times,
with clear and timely communica-tion of the patient’s plan of care
Continuum of Care Health Health
Health Care Provider Engagement
Follow-UpCare
InformationTransfer
MedicationManagement
Patient and Family Engagement/
Education
Figure 1. Seven Essential Intervention Categories for Designing Transitions Strategies for CDI Patients
Find further information about these principles at http://www.ntocc.org/Toolbox/ Adapted from NTOCC. Figure Courtesy of Cheri Lattimer, RN, BSN
This document contains point-of-care resources that can be printed separately for use in daily practice
3
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
THE BURDEN OF CDI ON PATIENTS, HEALTH CARE PROFESSIONALS, AND HEALTH CARE FACILITIES
CASE STUDY: A 29-year-old man presents with diarrhea for 3 days. He was prescribed prophylactic clindamycin for 5 days following dental surgery. His stool test is positive for C. difficile.
WHAT IS CLOSTRIDIOIDES DIFFICILE?
C. difficile infection (CDI) is the most common health care-acquired infection.2
• C. difficile is an anaerobic, gram-positive bacillus that forms heat-, acid-, and antibiotic-resistant spores, and colonizes the intestinal tract via the fecal-oral route3
• CDI can cause diarrhea, colitis, toxic megacolon, and death, depending on the virulence of the bacillus strain, host comorbidities, and the host immune response3
HOW DOES CDI IMPACT PATIENTS’ LIVES?
Studies report decreased functional capacity and considerable anxiety about physical symptoms among people with CDI, many of whom have multiple comorbidities.4–6 People with CDI also experience worsened quality of life, restricted daily activities, reduced work productivity, and increased personal cost burden (e.g., through medication costs).4–6 Such consequences can lead to chain reactions that affect the patient’s social life, work relationships, and income, and are intensified in the presence of recurrences.
WHAT CDI EPIDEMIOLOGY TRENDS SHOULD HEALTH CARE PROFESSIONALS BE AWARE OF?
According to the Centers for Disease Control and Prevention (CDC), approximately half a million individuals in the US were diagnosed with CDI in 2011.7 CDI has also increased considerably in the last two decades in community settings, such as long-term or residential care facilities, as well as in patient populations without prior antibiotic exposure.8–12
• Approximately two thirds of people with CDI had health care-associated infection
• One third had community-associated infection; about 18% of these people had no contact with medical care
• Health care-associated CDI has more severe outcomes than community-associated infection, including higher recurrence rates (20.9% vs 13.5%) and higher mortality (9.3% vs 1.3%).7 Community-acquired CDI may be severe and associated with need for hospitalization11
The CDC defines hospital-acquired CDI as symptom onset more than 48 hours after hospital admission.13 Community-acquired CDI is defined as symptom onset within the community or ≤48 hours after admission to a health care facility, provided that symptom onset was more than 12 hours after the last discharge from a health care facility.
Defining Hospital- and Community-Acquired CDI
4
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
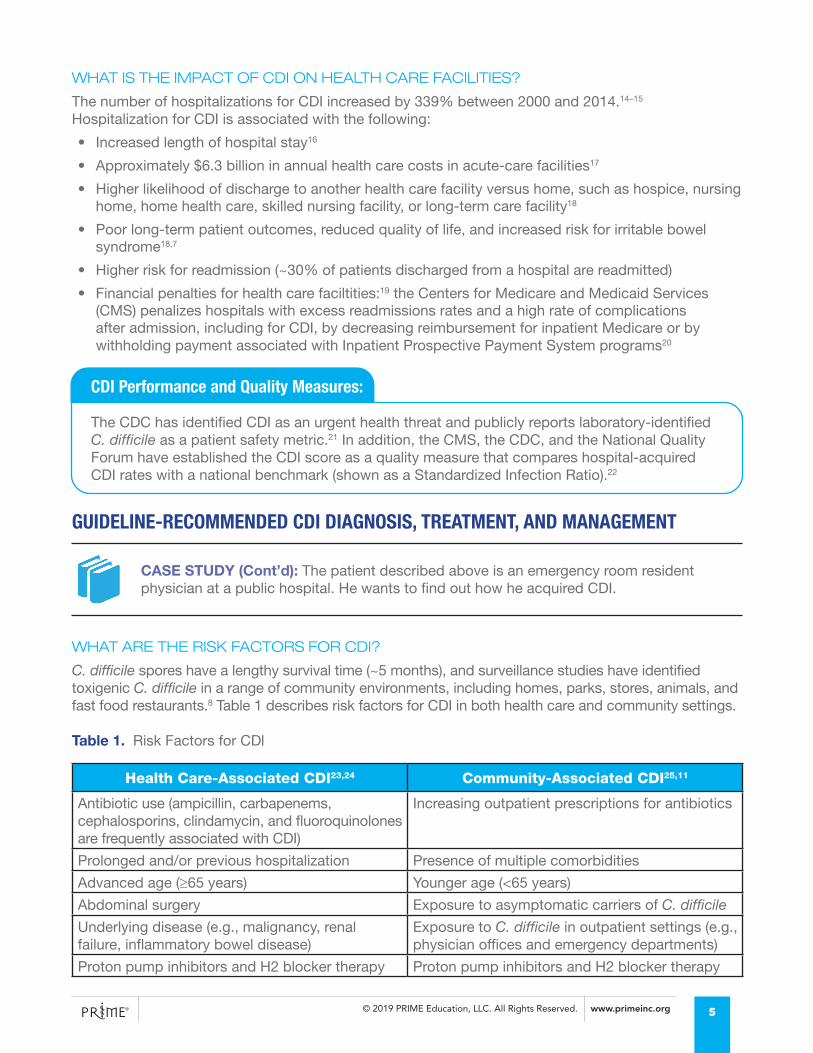
WHAT IS THE IMPACT OF CDI ON HEALTH CARE FACILITIES?
The number of hospitalizations for CDI increased by 339% between 2000 and 2014.14–15 Hospitalization for CDI is associated with the following:
• Increased length of hospital stay16
• Approximately $6.3 billion in annual health care costs in acute-care facilities17
• Higher likelihood of discharge to another health care facility versus home, such as hospice, nursing home, home health care, skilled nursing facility, or long-term care facility18
• Poor long-term patient outcomes, reduced quality of life, and increased risk for irritable bowel syndrome18,7
• Higher risk for readmission (~30% of patients discharged from a hospital are readmitted)
• Financial penalties for health care faciltities:19 the Centers for Medicare and Medicaid Services (CMS) penalizes hospitals with excess readmissions rates and a high rate of complications after admission, including for CDI, by decreasing reimbursement for inpatient Medicare or by withholding payment associated with Inpatient Prospective Payment System programs20
The CDC has identified CDI as an urgent health threat and publicly reports laboratory-identified C. difficile as a patient safety metric.21 In addition, the CMS, the CDC, and the National Quality Forum have established the CDI score as a quality measure that compares hospital-acquired CDI rates with a national benchmark (shown as a Standardized Infection Ratio).22
CDI Performance and Quality Measures:
GUIDELINE-RECOMMENDED CDI DIAGNOSIS, TREATMENT, AND MANAGEMENT
CASE STUDY (Cont’d): The patient described above is an emergency room resident physician at a public hospital. He wants to find out how he acquired CDI.
WHAT ARE THE RISK FACTORS FOR CDI?
C. difficile spores have a lengthy survival time (~5 months), and surveillance studies have identified toxigenic C. difficile in a range of community environments, including homes, parks, stores, animals, and fast food restaurants.8 Table 1 describes risk factors for CDI in both health care and community settings.
Table 1. Risk Factors for CDI
Health Care-Associated CDI23,24 Community-Associated CDI25,11
Antibiotic use (ampicillin, carbapenems, cephalosporins, clindamycin, and fluoroquinolones are frequently associated with CDI)
Increasing outpatient prescriptions for antibiotics
Prolonged and/or previous hospitalization Presence of multiple comorbidities
Advanced age (≥65 years) Younger age (<65 years)
Abdominal surgery Exposure to asymptomatic carriers of C. difficile
Underlying disease (e.g., malignancy, renal failure, inflammatory bowel disease)
Exposure to C. difficile in outpatient settings (e.g., physician offices and emergency departments)
Proton pump inhibitors and H2 blocker therapy Proton pump inhibitors and H2 blocker therapy
5
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
HOW CAN WE PREVENT CDI IN HEALTH CARE AND COMMUNITY SETTINGS?
Antibiotic Stewardship
Antibiotic or antimicrobial stewardship is an important strategy to reduce inappropriate antimicrobial use and lower the chance of primary infection with C. difficile in hospitals. The goals of such stewardship include selecting the optimal dose, duration, and administration route of therapy to ensure the best clinical outcome for treating or preventing infection while maintaining minimal toxicity and impact on resistance.26 Antibiotic stewardship has been shown to reduce CDI, improve patient safety, and optimize resource utilization across the continuum of care. Antibiotic stewardship interventions include auditing, using guideline-recommended empirical therapy, restricting specific antibiotics, limiting treatment duration, de-escalating, cycling or mixing antibiotics, and switching from intravenous (IV) to oral therapy.27
While a physician-pharmacist team might not be available on-site at nursing and skilled nursing facilities, providers can consider other approaches that support the review and optimization of antibiotics, such as telemedicine consults with infectious disease experts.26
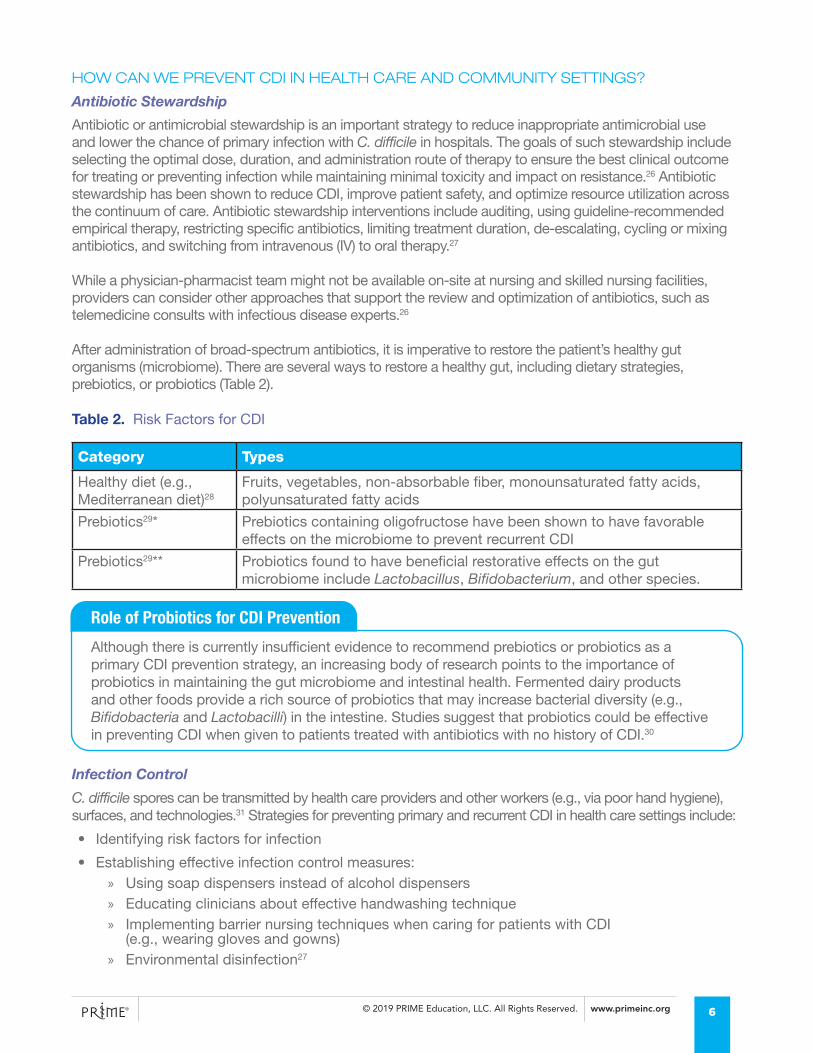
After administration of broad-spectrum antibiotics, it is imperative to restore the patient’s healthy gut organisms (microbiome). There are several ways to restore a healthy gut, including dietary strategies, prebiotics, or probiotics (Table 2).
Table 2. Risk Factors for CDI
Category Types
Healthy diet (e.g., Mediterranean diet)28
Fruits, vegetables, non-absorbable fiber, monounsaturated fatty acids, polyunsaturated fatty acids
Prebiotics29* Prebiotics containing oligofructose have been shown to have favorable effects on the microbiome to prevent recurrent CDI
Prebiotics29** Probiotics found to have beneficial restorative effects on the gut microbiome include Lactobacillus, Bifidobacterium, and other species.
Infection Control
C. difficile spores can be transmitted by health care providers and other workers (e.g., via poor hand hygiene), surfaces, and technologies.31 Strategies for preventing primary and recurrent CDI in health care settings include:
• Identifying risk factors for infection
• Establishing effective infection control measures: » Using soap dispensers instead of alcohol dispensers » Educating clinicians about effective handwashing technique » Implementing barrier nursing techniques when caring for patients with CDI
(e.g., wearing gloves and gowns) » Environmental disinfection27
Although there is currently insufficient evidence to recommend prebiotics or probiotics as a primary CDI prevention strategy, an increasing body of research points to the importance of probiotics in maintaining the gut microbiome and intestinal health. Fermented dairy products and other foods provide a rich source of probiotics that may increase bacterial diversity (e.g., Bifidobacteria and Lactobacilli) in the intestine. Studies suggest that probiotics could be effective in preventing CDI when given to patients treated with antibiotics with no history of CDI.30
Role of Probiotics for CDI Prevention
6
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
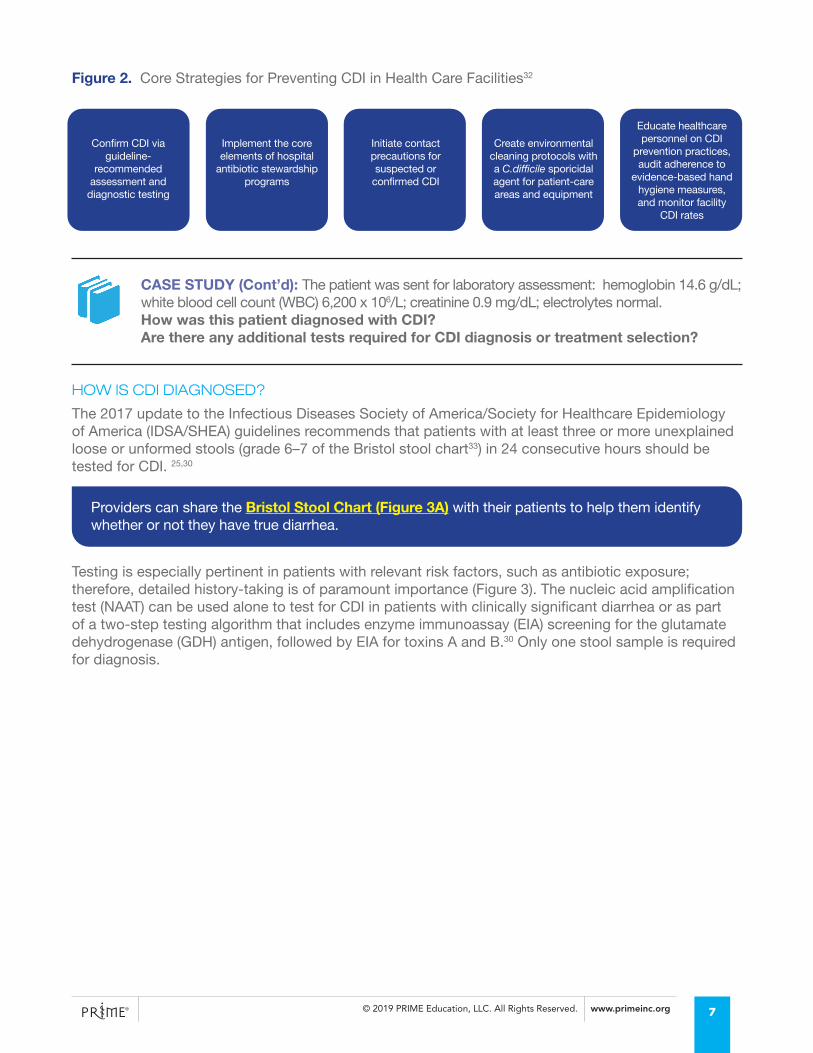
Figure 2. Core Strategies for Preventing CDI in Health Care Facilities32
CASE STUDY (Cont’d): The patient was sent for laboratory assessment: hemoglobin 14.6 g/dL; white blood cell count (WBC) 6,200 x 106/L; creatinine 0.9 mg/dL; electrolytes normal.How was this patient diagnosed with CDI? Are there any additional tests required for CDI diagnosis or treatment selection?
HOW IS CDI DIAGNOSED?
The 2017 update to the Infectious Diseases Society of America/Society for Healthcare Epidemiology of America (IDSA/SHEA) guidelines recommends that patients with at least three or more unexplained loose or unformed stools (grade 6–7 of the Bristol stool chart33) in 24 consecutive hours should be tested for CDI. 25,30
Testing is especially pertinent in patients with relevant risk factors, such as antibiotic exposure; therefore, detailed history-taking is of paramount importance (Figure 3). The nucleic acid amplification test (NAAT) can be used alone to test for CDI in patients with clinically significant diarrhea or as part of a two-step testing algorithm that includes enzyme immunoassay (EIA) screening for the glutamate dehydrogenase (GDH) antigen, followed by EIA for toxins A and B.30 Only one stool sample is required for diagnosis.
Confirm CDI via guideline-
recommended assessment and
diagnostic testing
Implement the core elements of hospital
antibiotic stewardship programs
Initiate contact precautions for suspected or
confirmed CDI
Create environmental cleaning protocols with a C.difficile sporicidal agent for patient-care areas and equipment
Educate healthcare personnel on CDI
prevention practices, audit adherence to
evidence-based hand hygiene measures, and monitor facility
CDI rates
Providers can share the Bristol Stool Chart (Figure 3A) with their patients to help them identify whether or not they have true diarrhea.
7
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
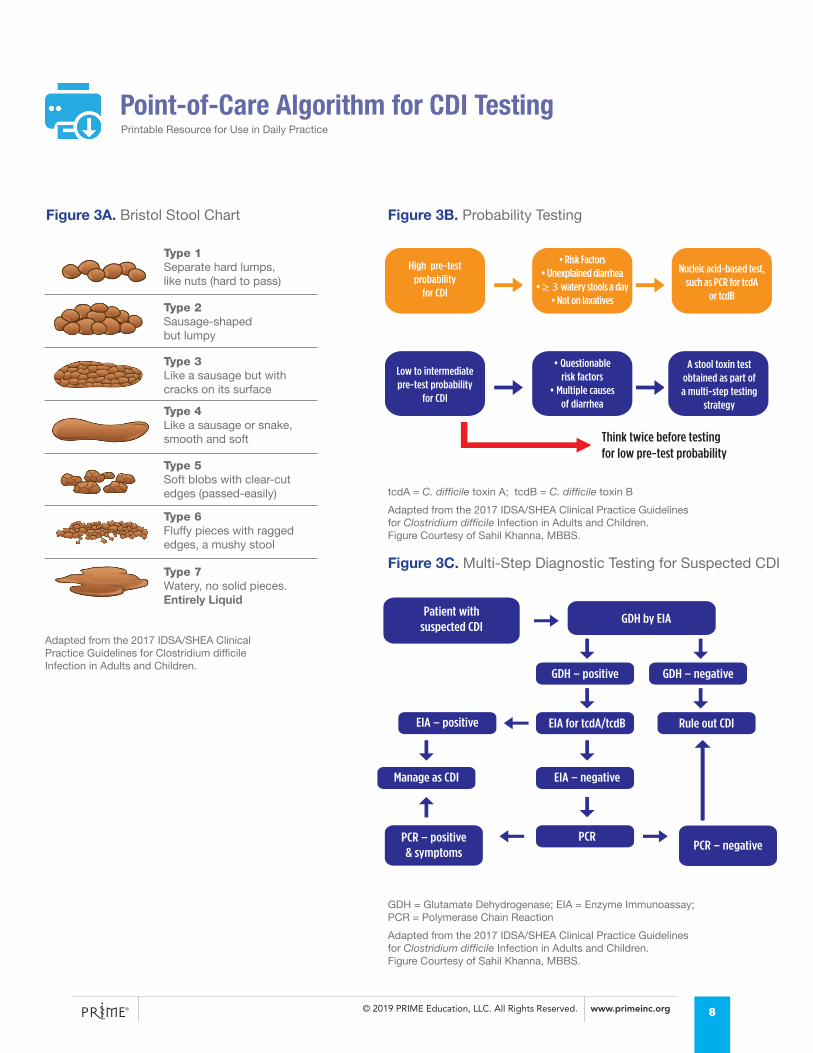
Think twice before testing for low pre-test probability
High pre-testprobability
for CDI
• Risk Factors• Unexplained diarrhea
• ≥ 3 watery stools a day• Not on laxatives
Nucleic acid-based test, such as PCR for tcdA
or tcdB
A stool toxin testobtained as part of a multi-step testing
strategy
Low to intermediate pre-test probability
for CDI
• Questionablerisk factors
• Multiple causesof diarrhea
Patient with suspected CDI
GDH by EIA
GDH – positive
EIA – positive
Manage as CDI
PCR – positive& symptoms
PCR – negative
EIA – negative
PCR
EIA for tcdA/tcdB Rule out CDI
GDH – negative
Point-of-Care Algorithm for CDI TestingPrintable Resource for Use in Daily Practice
GDH = Glutamate Dehydrogenase; EIA = Enzyme Immunoassay; PCR = Polymerase Chain Reaction
Adapted from the 2017 IDSA/SHEA Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children.Figure Courtesy of Sahil Khanna, MBBS.
tcdA = C. difficile toxin A; tcdB = C. difficile toxin B
Adapted from the 2017 IDSA/SHEA Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children. Figure Courtesy of Sahil Khanna, MBBS.
Adapted from the 2017 IDSA/SHEA Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children.
Figure 3B. Probability TestingFigure 3A. Bristol Stool Chart
Figure 3C. Multi-Step Diagnostic Testing for Suspected CDI
8
Type 1Separate hard lumps,like nuts (hard to pass)
Type 2Sausage-shaped but lumpy
Type 3Like a sausage but withcracks on its surface
Type 4Like a sausage or snake,smooth and soft
Type 5Soft blobs with clear-cutedges (passed-easily)
Type 6Fluffy pieces with raggededges, a mushy stool
Type 7Watery, no solid pieces.Entirely Liquid
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
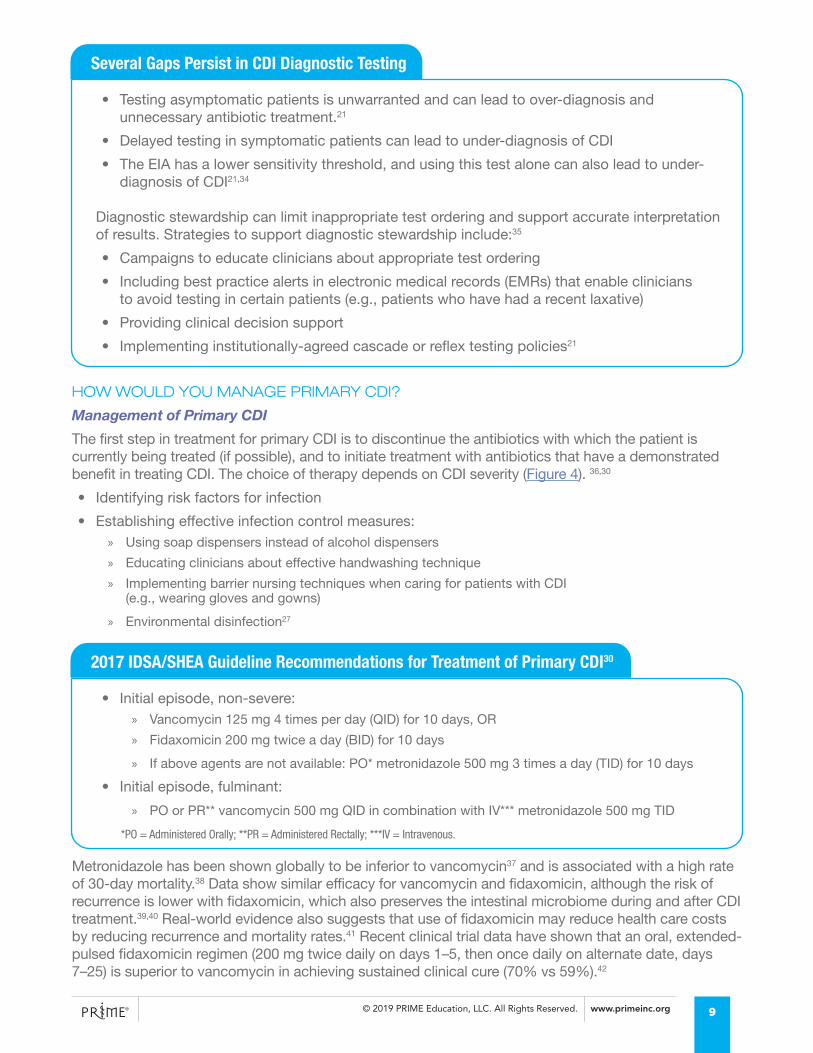
HOW WOULD YOU MANAGE PRIMARY CDI?
Management of Primary CDI
The first step in treatment for primary CDI is to discontinue the antibiotics with which the patient is currently being treated (if possible), and to initiate treatment with antibiotics that have a demonstrated benefit in treating CDI. The choice of therapy depends on CDI severity (Figure 4). 36,30
• Identifying risk factors for infection
• Establishing effective infection control measures: » Using soap dispensers instead of alcohol dispensers
» Educating clinicians about effective handwashing technique
» Implementing barrier nursing techniques when caring for patients with CDI (e.g., wearing gloves and gowns)
» Environmental disinfection27
Metronidazole has been shown globally to be inferior to vancomycin37 and is associated with a high rate of 30-day mortality.38 Data show similar efficacy for vancomycin and fidaxomicin, although the risk of recurrence is lower with fidaxomicin, which also preserves the intestinal microbiome during and after CDI treatment.39,40 Real-world evidence also suggests that use of fidaxomicin may reduce health care costs by reducing recurrence and mortality rates.41 Recent clinical trial data have shown that an oral, extended-pulsed fidaxomicin regimen (200 mg twice daily on days 1–5, then once daily on alternate date, days 7–25) is superior to vancomycin in achieving sustained clinical cure (70% vs 59%).42
*PO = Administered Orally; **PR = Administered Rectally; ***IV = Intravenous.
• Testing asymptomatic patients is unwarranted and can lead to over-diagnosis and unnecessary antibiotic treatment.21
• Delayed testing in symptomatic patients can lead to under-diagnosis of CDI
• The EIA has a lower sensitivity threshold, and using this test alone can also lead to under-diagnosis of CDI21,34
Diagnostic stewardship can limit inappropriate test ordering and support accurate interpretation of results. Strategies to support diagnostic stewardship include:35
• Campaigns to educate clinicians about appropriate test ordering
• Including best practice alerts in electronic medical records (EMRs) that enable clinicians to avoid testing in certain patients (e.g., patients who have had a recent laxative)
• Providing clinical decision support
• Implementing institutionally-agreed cascade or reflex testing policies21
• Initial episode, non-severe: » Vancomycin 125 mg 4 times per day (QID) for 10 days, OR
» Fidaxomicin 200 mg twice a day (BID) for 10 days
» If above agents are not available: PO* metronidazole 500 mg 3 times a day (TID) for 10 days
• Initial episode, fulminant:
» PO or PR** vancomycin 500 mg QID in combination with IV*** metronidazole 500 mg TID
Several Gaps Persist in CDI Diagnostic Testing
2017 IDSA/SHEA Guideline Recommendations for Treatment of Primary CDI30
9
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
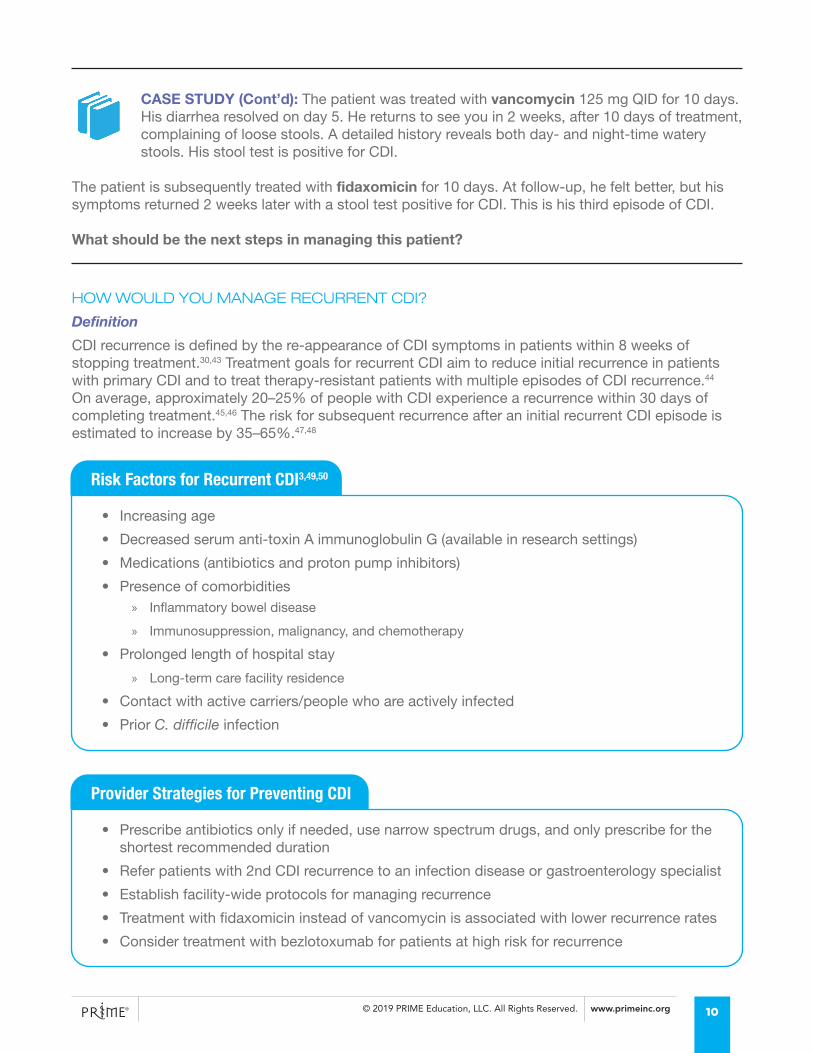
CASE STUDY (Cont’d): The patient was treated with vancomycin 125 mg QID for 10 days. His diarrhea resolved on day 5. He returns to see you in 2 weeks, after 10 days of treatment, complaining of loose stools. A detailed history reveals both day- and night-time watery stools. His stool test is positive for CDI.
The patient is subsequently treated with fidaxomicin for 10 days. At follow-up, he felt better, but his symptoms returned 2 weeks later with a stool test positive for CDI. This is his third episode of CDI.
What should be the next steps in managing this patient?
HOW WOULD YOU MANAGE RECURRENT CDI?
Definition
CDI recurrence is defined by the re-appearance of CDI symptoms in patients within 8 weeks of stopping treatment.30,43 Treatment goals for recurrent CDI aim to reduce initial recurrence in patients with primary CDI and to treat therapy-resistant patients with multiple episodes of CDI recurrence.44 On average, approximately 20–25% of people with CDI experience a recurrence within 30 days of completing treatment.45,46 The risk for subsequent recurrence after an initial recurrent CDI episode is estimated to increase by 35–65%.47,48
• Increasing age
• Decreased serum anti-toxin A immunoglobulin G (available in research settings)
• Medications (antibiotics and proton pump inhibitors)
• Presence of comorbidities » Inflammatory bowel disease
» Immunosuppression, malignancy, and chemotherapy
• Prolonged length of hospital stay
» Long-term care facility residence
• Contact with active carriers/people who are actively infected
• Prior C. difficile infection
• Prescribe antibiotics only if needed, use narrow spectrum drugs, and only prescribe for the shortest recommended duration
• Refer patients with 2nd CDI recurrence to an infection disease or gastroenterology specialist
• Establish facility-wide protocols for managing recurrence
• Treatment with fidaxomicin instead of vancomycin is associated with lower recurrence rates
• Consider treatment with bezlotoxumab for patients at high risk for recurrence
Risk Factors for Recurrent CDI3,49,50
Provider Strategies for Preventing CDI
10
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
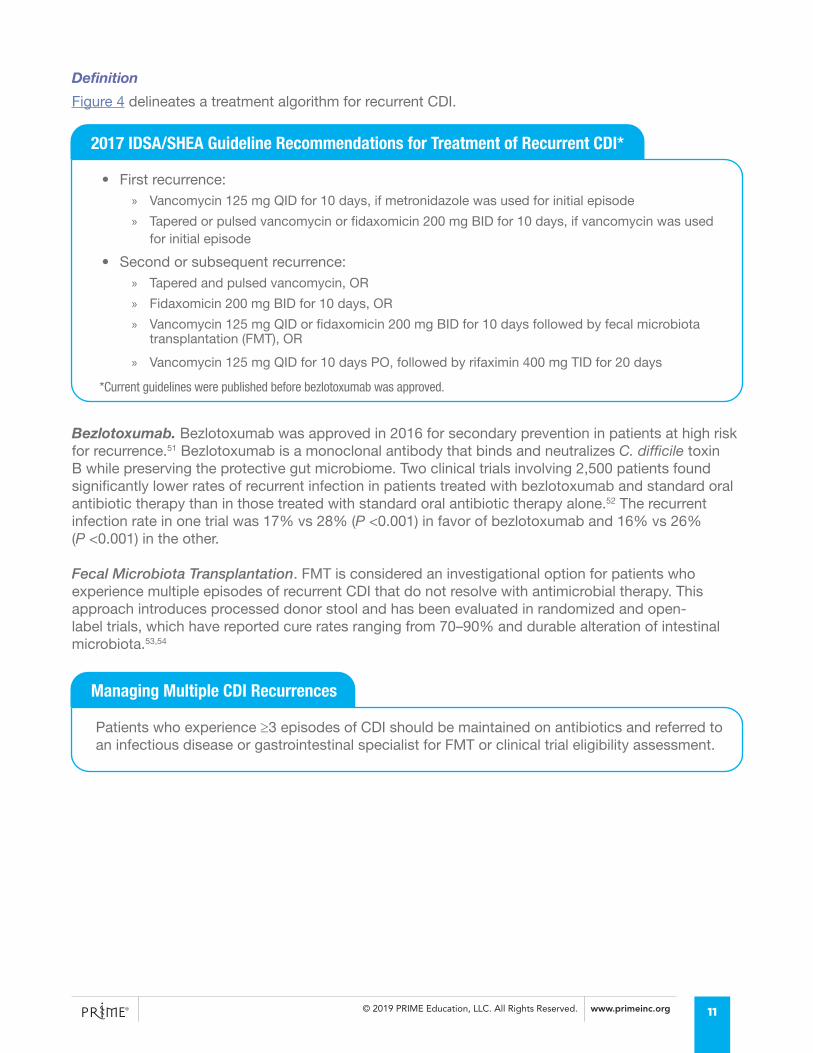
Definition
Figure 4 delineates a treatment algorithm for recurrent CDI.
• First recurrence: » Vancomycin 125 mg QID for 10 days, if metronidazole was used for initial episode
» Tapered or pulsed vancomycin or fidaxomicin 200 mg BID for 10 days, if vancomycin was used for initial episode
• Second or subsequent recurrence: » Tapered and pulsed vancomycin, OR
» Fidaxomicin 200 mg BID for 10 days, OR
» Vancomycin 125 mg QID or fidaxomicin 200 mg BID for 10 days followed by fecal microbiota transplantation (FMT), OR
» Vancomycin 125 mg QID for 10 days PO, followed by rifaximin 400 mg TID for 20 days
Patients who experience ≥3 episodes of CDI should be maintained on antibiotics and referred to an infectious disease or gastrointestinal specialist for FMT or clinical trial eligibility assessment.
2017 IDSA/SHEA Guideline Recommendations for Treatment of Recurrent CDI*
Managing Multiple CDI Recurrences
*Current guidelines were published before bezlotoxumab was approved.
Bezlotoxumab. Bezlotoxumab was approved in 2016 for secondary prevention in patients at high risk for recurrence.51 Bezlotoxumab is a monoclonal antibody that binds and neutralizes C. difficile toxin B while preserving the protective gut microbiome. Two clinical trials involving 2,500 patients found significantly lower rates of recurrent infection in patients treated with bezlotoxumab and standard oral antibiotic therapy than in those treated with standard oral antibiotic therapy alone.52 The recurrent infection rate in one trial was 17% vs 28% (P <0.001) in favor of bezlotoxumab and 16% vs 26% (P <0.001) in the other.
Fecal Microbiota Transplantation. FMT is considered an investigational option for patients who experience multiple episodes of recurrent CDI that do not resolve with antimicrobial therapy. This approach introduces processed donor stool and has been evaluated in randomized and open-label trials, which have reported cure rates ranging from 70–90% and durable alteration of intestinal microbiota.53,54
11
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
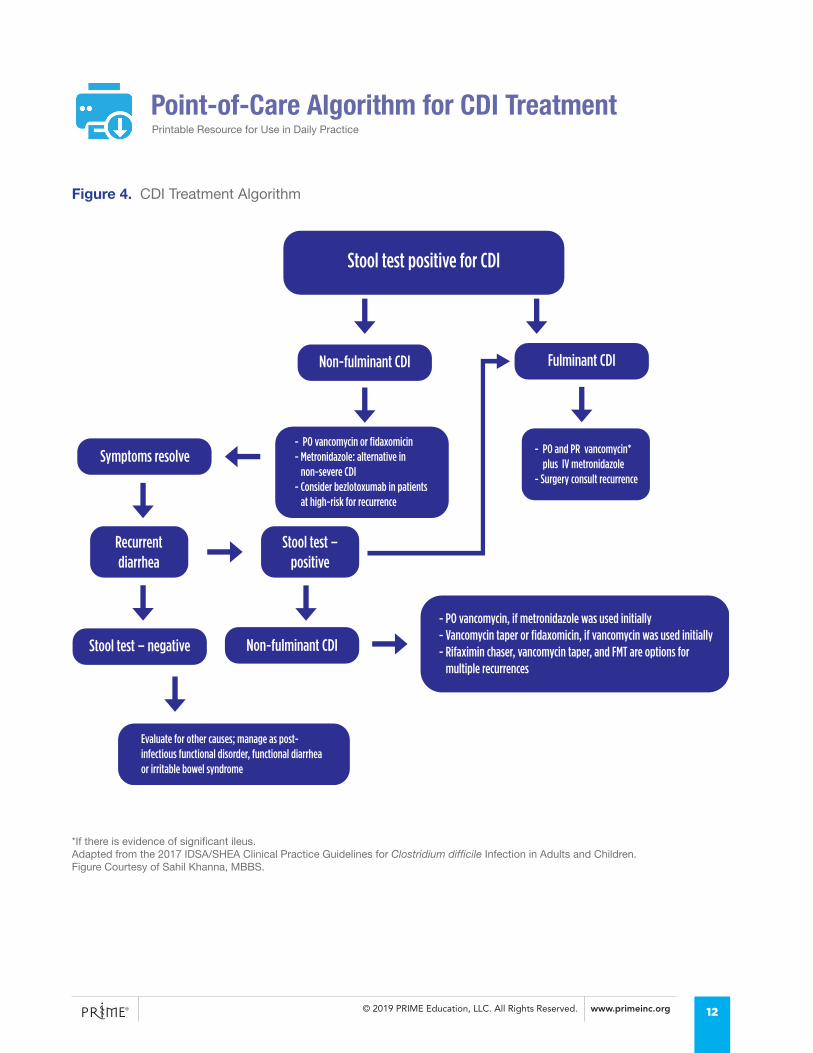
Stool test positive for CDI
Non-fulminant CDI
Symptoms resolve
Recurrentdiarrhea
Stool test – positive
Stool test – negative Non-fulminant CDI
- PO vancomycin or fidaxomicin - Metronidazole: alternative in non-severe CDI- Consider bezlotoxumab in patients at high-risk for recurrence
Evaluate for other causes; manage as post-infectious functional disorder, functional diarrheaor irritable bowel syndrome
- PO vancomycin, if metronidazole was used initially- Vancomycin taper or fidaxomicin, if vancomycin was used initially- Rifaximin chaser, vancomycin taper, and FMT are options for multiple recurrences
- PO and PR vancomycin* plus IV metronidazole- Surgery consult recurrence
Fulminant CDI
Point-of-Care Algorithm for CDI TreatmentPrintable Resource for Use in Daily Practice
*If there is evidence of significant ileus.Adapted from the 2017 IDSA/SHEA Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children.Figure Courtesy of Sahil Khanna, MBBS.
Figure 4. CDI Treatment Algorithm
12

© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
CONSIDERATIONS IN TRANSITIONS OF CAREBARRIERS TO EFFECTIVE CARE TRANSITIONS IN CDI
Many patients with CDI not only have several comorbidities, but also require care across multiple settings (e.g., sub-acute care facilities, long-term care facilities, primary care, home health). In order to ensure that patients are equipped with knowledge that will enable them to engage in self-care, recognize CDI symptoms should they recur, and continue to receive appropriate treatment with CDI-specific therapies following discharge, it is important to carefully plan the transition to and from hospitals and to coordinate care between patients, caregivers, and members of the clinical team.
Effectively implemented transitions of care processes can reduce the risk for recurrence, hospital readmission, emergency room visits, and complications.55 However, there exist several system-, clinician-, and patient-level barriers to the implementation of effective transitions of care in CDI.
SYSTEM-LEVEL BARRIERS
Lack of Established or Suboptimal Transition Processes
Many health care systems lack comprehensive transition services to support a seamless discharge process from acute to post-acute settings and are focused on rapid versus customized discharge. As a result, patients with CDI may be prematurely discharged without the benefit of a transition plan. Ideally, prior to and at discharge, clinicians would have some designated time to provide verbal patient and caregiver education about hygiene practices, medication management, and symptom recognition that is supported by printed material. However, health care professionals report often feeling rushed at discharge, with little time to educate patients or design a transition plan.20 The expansion of performance measures and other system-level demands reduce the time available to health care providers to effectively plan for transitions.
Inadequate Information Transfer
Gaps in care can emerge when insufficient information is provided from one care setting to the other. Although EMR systems potentially provide a resource to support information-sharing and communication among members of the clinical team, interoperability between systems is not common, and not all EMR platforms support access to CDI discharge information. In addition, if patient discharge education materials on CDI are available in the EMR, they are often in formats that are inaccessible for patients with low literacy.
Suboptimal Medication Management
Suboptimal medication management and education at discharge can pose additional barriers to care transitions. If medications are not reconciled at discharge, clinicians at post-acute facilities may be unaware of patient medications, which can lead to medication errors, adverse events, and rehospitalizations. Additionally, medication cost and formulary issues can create gaps in care. For instance, some skilled nursing facilities are unwilling to accept patients whose medication costs are not fully covered by Medicare plans or avoid working with certain types of Medicare plans.56
13
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
CLINICIAN-LEVEL BARRIERS
Lack of Familiarity with CDI
Many providers are unfamiliar with CDI epidemiology, prevention strategies for primary and recurrent infection, and the implications of health care-acquired CDI for readmissions. Accordingly, they are poorly equipped to provide patient education about primary prevention of CDI and strategies for preventing recurrence in patient-friendly language or formats.
Lack of Familiarity with Transition Roles and Responsibilities
In addition, clinicians in both hospital and post-acute settings may be unfamiliar with their own and others’ roles and responsibilities in the transition process, leading to communication breakdown between different providers. In the event of CDI recurrence following discharge, lack of clarity concerning transition responsibilities can also contribute to blame attribution about whether CDI was acquired in a health care facility or community setting, further fueling communication breakdown and preventing effective transition of care.
Suboptimal Information Transfer
Discharge from hospital settings can also be accompanied by delays in sharing discharge information with community providers. For instance, hospital-based providers may not be familiar with the range of services available for providing home health support or can be reluctant to create a transition plan for outside sites of care over which they have no control. In turn, community providers may be unfamiliar with managing patients who have been or are being treated for CDI. In some cases, patients may be discharged without any information being transferred from the hospital to the post-acute setting, or they may be discharged with instructions from multiple in-hospital providers.
PATIENT-LEVEL BARRIERS
Socioeconomic Factors
Level of income and education, employment status, and access to clean water, food, and housing are all factors that influence health outcomes. Patients with unmet non-medical needs (e.g., food insecurity, low health literacy, lack of transportation) are more likely to be emergency room users or to repeatedly miss medical appointments than patients who do not experience these social determinants of health.
Information Recall
Patients and their caregivers are often unable to recall discharge information or self-care instructions and may be ill-prepared to continue ongoing medication management in the home setting.57 While low health literacy poses a barrier to patient understanding of discharge information, many patients simply do not receive information about self-care or medication management. Some patients might not even be aware of their reason for hospitalization, or be aware that their condition warrants specialist follow-up following discharge.57 Caregivers and community providers are often excluded from the transition planning process, which makes it difficult for them to reinforce any patient education provided at discharge.
Medication Cost
Medication cost is an additional barrier to effective transition, and paying for medications is a primary challenge for patients, whether they are transitioning to their own home or another health care facility. If medication costs are not covered, community- or post-acute facility providers are likely to prescribe less expensive, inappropriate antibiotics and increase the risk of recurrence. These factors, together with ongoing comorbidities and likely polypharmacy, can lead to lower adherence of medications for managing CDI.
14
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
There are many resources that you can direct your patients toward to assist with medication access and lowering medication cost/copays.
• C Diff Foundation: https://cdifffoundation.org/
• Medicare Pharmaceutical Assistance Program: https://www.medicare.gov/pharmaceutical-assistance-program/
• GoodRx: https://www.goodrx.com/
• Pharmaceutical industry-sponsored patient assistance programs
STRATEGIES FOR OPTIMIZING CDI CARE TRANSITION PATHWAYSSafe transitions of patients from hospital to home or another care facility require the successful completion of several tasks, including patient education about key elements of self-care and medication management, medication reconciliation, specialist referral if warranted, comprehensive transition planning documentation, and communication with staff at post-acute health care facilities.
IDENTIFY THE TRANSITION TEAM
• Identify the range of health care providers that need to be involved in care transitions, such as pharmacists, infection preventionists, primary care providers, case managers, and in-home/long-term care staff.58,59,60
» Clarify interprofessional roles and responsibilities in facilitating care transitions from acute to community settings and vice versa
» Establish a transition coach whenever possible to support post-discharge patient engagement and self-management. Social workers, case managers, patient navigators, or transition nurses are more likely to be equipped to lead transition planning than floor nurses or pharmacists61
• Designate a discharge team charged with establishing a patient-centered transition process. Of paramount importance, this team should:
» Create and deliver a consistent message to patients, caregivers, and post-acute facility providers
» Identify the information and formats necessary for a streamlined discharge packet
» Educate patients to engage in self-care and medication management at home
• Expand the composition of the transition team in rural areas and equip them with appropriate resources: » Use telehealth—an emerging strategy for sharing information with community providers (e.g., via
online and web-based video messaging)—and establish regular surveillance of vitals, virtual visits, and medication review62
» Liaise with first responders, such as paramedics and firefighters, who may be able to help with transportation, if patients are moving from one post-acute setting to another
Resources
15
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
EMPOWER PATIENTS
• Educate and empower patients to be their own advocates by providing resources to enable them to know which questions to ask providers at discharge and throughout the transition process. Such questions might include:
» What do I need to know about my illness?
» How can I prevent spreading C. difficile to friends and family?
» What precautions can I take when I return home after discharge?
» What symptoms do I need to watch for?
» What is the best way to wash my hands?
» What should I know about cleaning my home?
» Who should I contact if I have questions or concerns about my illness?
• Engage patients in self-care and medication management by individualizing patient and caregiver education:
» Educate patient about precautions to take in the home environment to prevent recurrence and provide time for patients and caregivers to ask questions (the transition coach or nurse can do this when a patient with health care-acquired CDI is scheduled for discharge)
» Maximize patient/caregiver involvement in all phases of an intervention by promoting self-determination and informed decision-making
» Provide educational information to support the patient/caregiver’s participation in the plan of care (Table 3)
» Use specific health literacy best practices and communication models
The C diff Foundation provides resources for patients regarding home care and strategies for maintaining the home environment (https://cdifffoundation.org/cdiff-infection-homecare/)
The National Patient Safety Foundation’s Ask Me 3, or other teach-back methods, ensure patients are knowledgeable about their condition and feel supported to engage in self-care.63
Ask Me 3
1. What is my main problem?2. What do I need to do?3. Why is it important for me to do this?
C Diff Foundation Resources for Home Care
Engaging Patients in Self-Care
16
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
CREATE DISCHARGE MANAGEMENT AND PROTOCOLS
• Consolidate discharge instructions into one document with simple instructions than can also be circulated to post-acute providers and incorporated into the hospital EMR:64
» Optimize information technology systems (e.g., EMR) and processes to support accurate and timely information transfer from site to site58
» A consolidated discharge summary can help to reduce communication deficits65,66,67
• Create a checklist for patients/providers or refer to the checklist provided at the end of this section to ensure that discharge is appropriately supported. Use this checklist to support discussions with patients about strategies to:
» Find medication payment assistance
» Manage medications as prescribed
» Reduce risk of transmission to household members
» Identify risk factors for recurrence
» Recognize symptoms of CDI: a color-coded symptom guide (e.g., Table 3) can help patients identify when they need to contact a provider
» Identify which provider to contact should symptoms occur
• Offer strategies to support medication adherence: » Begin the patient assistance process at diagnosis
» Initiate the prior authorization process at diagnosis
» Collaborate with in-hospital pharmacist(s) to develop and implement a plan for managing medications
• Social determinants of health—such as housing, food security, literacy, and occupational security—influence patient outcomes:
» Prior to discharge, transition planners can work with patients to uncover underlying social needs and identify their concerns, preferences, and needs
» If patients are transitioning to their own home, planners should assess their needs to determine home-based resources, such as community referrals and social work support
» Patients who lack functional literacy, live alone, are visually impaired, or lack food/medicine security or transport are likely to have additional needs about which transition planners should be aware
The CMS and the American Academy of Family Physicians have created assessment tools for social determinants of health that providers can use to support transition planning and identify potential resources for patients with social and environmental needs (e.g., Meals on Wheels).
https://innovation.cms.gov/Files/worksheets/ahcm-screeningtool.pdf
https://www.aafp.org/dam/AAFP/documents/patient_care/everyone_project/physician-short.pdf
Assessment Tools for Social Determinants of Health
17
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
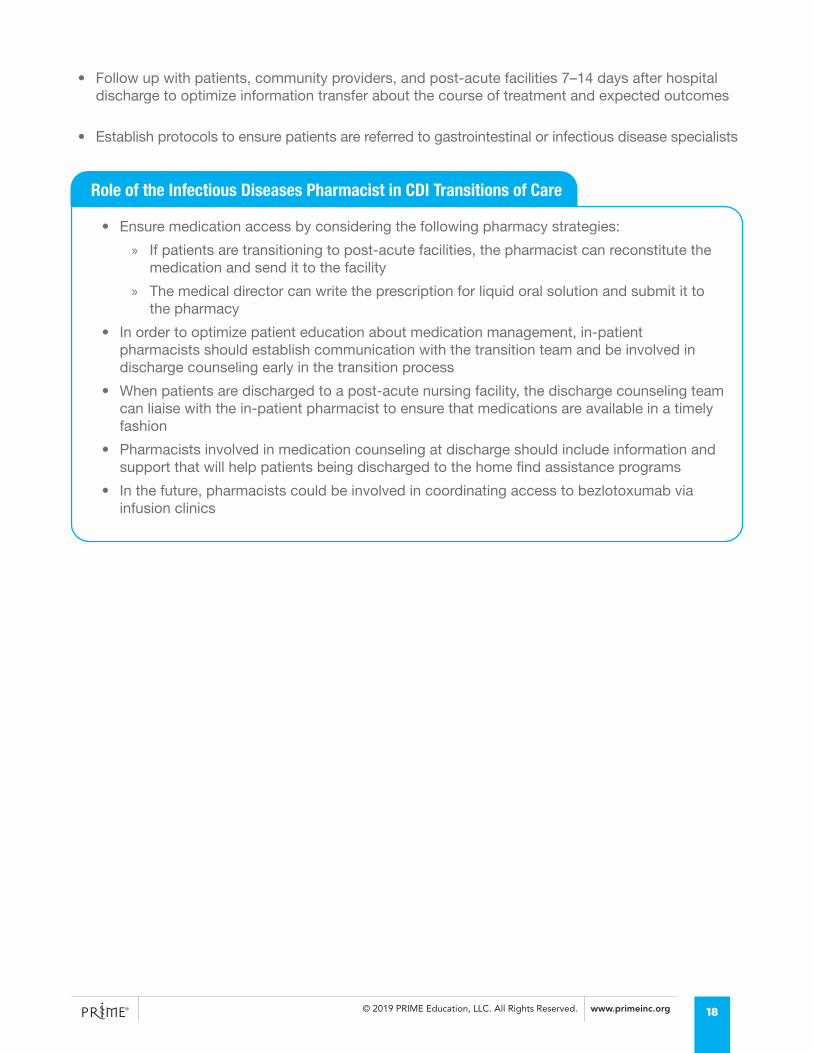
• Follow up with patients, community providers, and post-acute facilities 7–14 days after hospital discharge to optimize information transfer about the course of treatment and expected outcomes
• Establish protocols to ensure patients are referred to gastrointestinal or infectious disease specialists
• Ensure medication access by considering the following pharmacy strategies:
» If patients are transitioning to post-acute facilities, the pharmacist can reconstitute the medication and send it to the facility
» The medical director can write the prescription for liquid oral solution and submit it to the pharmacy
• In order to optimize patient education about medication management, in-patient pharmacists should establish communication with the transition team and be involved in discharge counseling early in the transition process
• When patients are discharged to a post-acute nursing facility, the discharge counseling team can liaise with the in-patient pharmacist to ensure that medications are available in a timely fashion
• Pharmacists involved in medication counseling at discharge should include information and support that will help patients being discharged to the home find assistance programs
• In the future, pharmacists could be involved in coordinating access to bezlotoxumab via infusion clinics
Role of the Infectious Diseases Pharmacist in CDI Transitions of Care
18
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
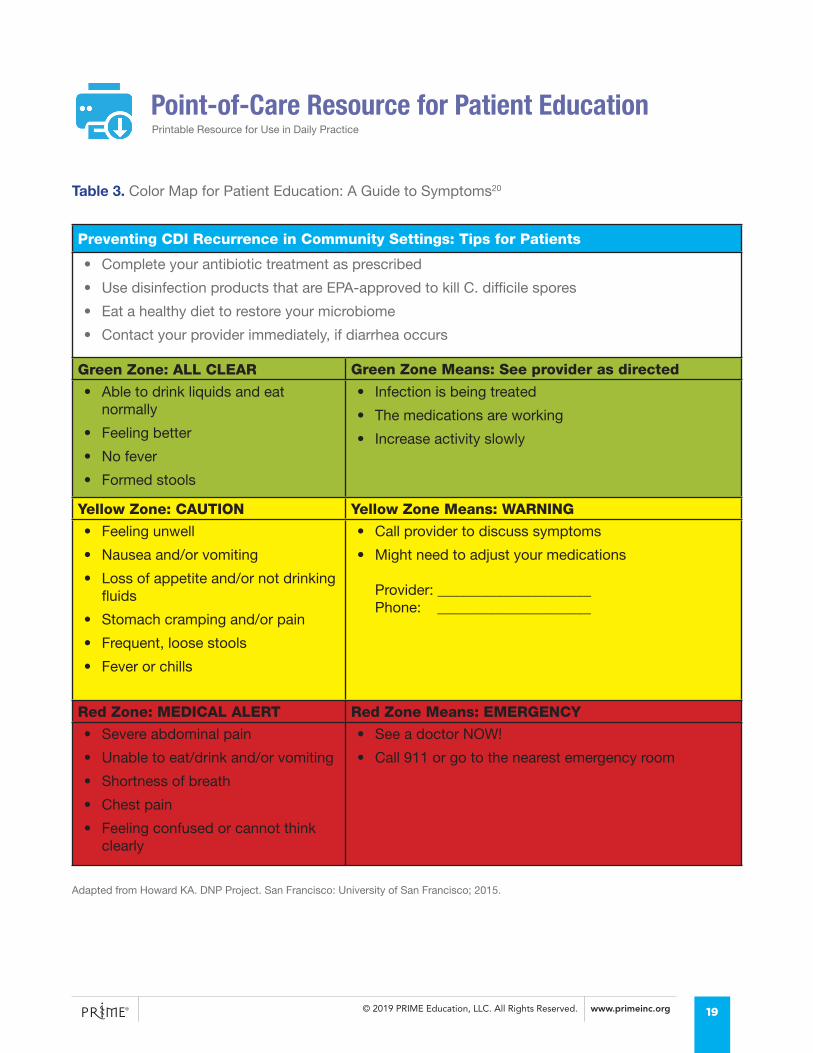
Preventing CDI Recurrence in Community Settings: Tips for Patients
• Complete your antibiotic treatment as prescribed
• Use disinfection products that are EPA-approved to kill C. difficile spores
• Eat a healthy diet to restore your microbiome
• Contact your provider immediately, if diarrhea occurs
Green Zone: ALL CLEAR Green Zone Means: See provider as directed
• Able to drink liquids and eat normally
• Feeling better
• No fever
• Formed stools
• Infection is being treated
• The medications are working
• Increase activity slowly
Yellow Zone: CAUTION Yellow Zone Means: WARNING
• Feeling unwell
• Nausea and/or vomiting
• Loss of appetite and/or not drinking fluids
• Stomach cramping and/or pain
• Frequent, loose stools
• Fever or chills
• Call provider to discuss symptoms
• Might need to adjust your medications
Provider: _____________________Phone: _____________________
Red Zone: MEDICAL ALERT Red Zone Means: EMERGENCY
• Severe abdominal pain
• Unable to eat/drink and/or vomiting
• Shortness of breath
• Chest pain
• Feeling confused or cannot think clearly
• See a doctor NOW!
• Call 911 or go to the nearest emergency room
Table 3. Color Map for Patient Education: A Guide to Symptoms20
Adapted from Howard KA. DNP Project. San Francisco: University of San Francisco; 2015.
Point-of-Care Resource for Patient Education Printable Resource for Use in Daily Practice
19
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
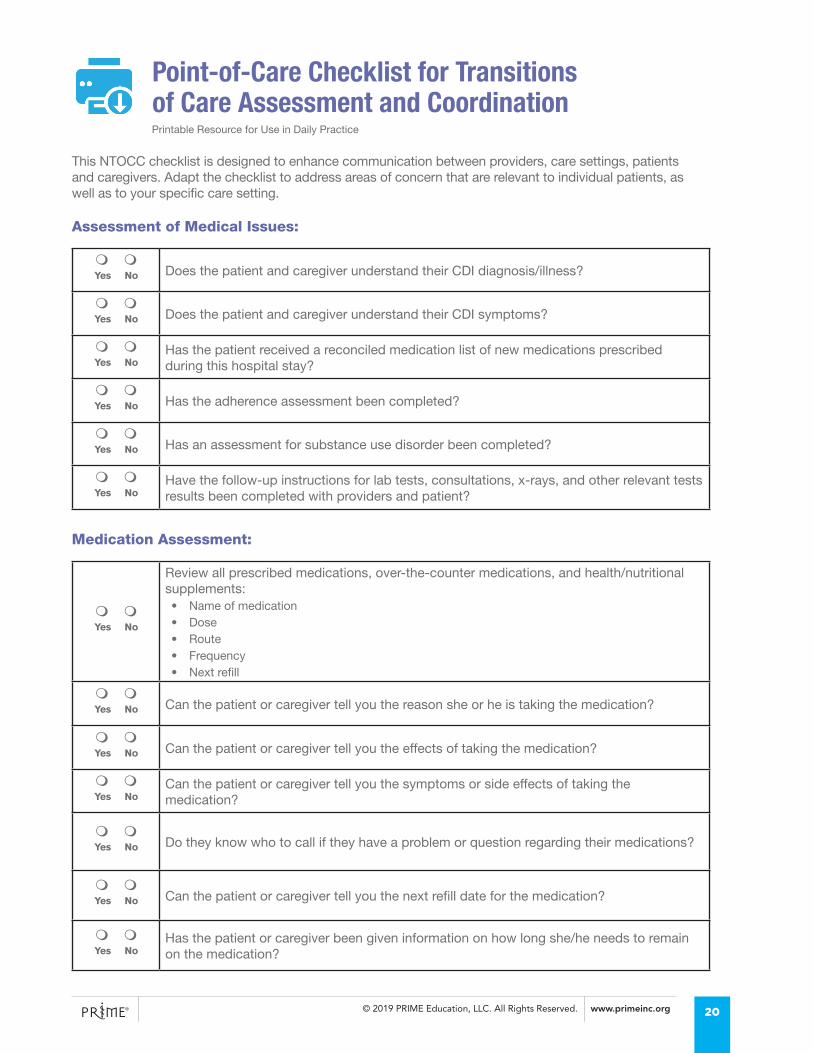
Point-of-Care Checklist for Transitions of Care Assessment and Coordination
m mYes No Does the patient and caregiver understand their CDI diagnosis/illness?
m mYes No Does the patient and caregiver understand their CDI symptoms?
m mYes No
Has the patient received a reconciled medication list of new medications prescribed during this hospital stay?
m mYes No Has the adherence assessment been completed?
m mYes No Has an assessment for substance use disorder been completed?
m mYes No
Have the follow-up instructions for lab tests, consultations, x-rays, and other relevant tests results been completed with providers and patient?
m mYes No
Review all prescribed medications, over-the-counter medications, and health/nutritional supplements:• Name of medication• Dose• Route• Frequency• Next refill
m mYes No Can the patient or caregiver tell you the reason she or he is taking the medication?
m mYes No Can the patient or caregiver tell you the effects of taking the medication?
m mYes No
Can the patient or caregiver tell you the symptoms or side effects of taking the medication?
m mYes No Do they know who to call if they have a problem or question regarding their medications?
m mYes No Can the patient or caregiver tell you the next refill date for the medication?
m mYes No
Has the patient or caregiver been given information on how long she/he needs to remain on the medication?
This NTOCC checklist is designed to enhance communication between providers, care settings, patients and caregivers. Adapt the checklist to address areas of concern that are relevant to individual patients, as well as to your specific care setting.
Assessment of Medical Issues:
Medication Assessment:
Printable Resource for Use in Daily Practice
20
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
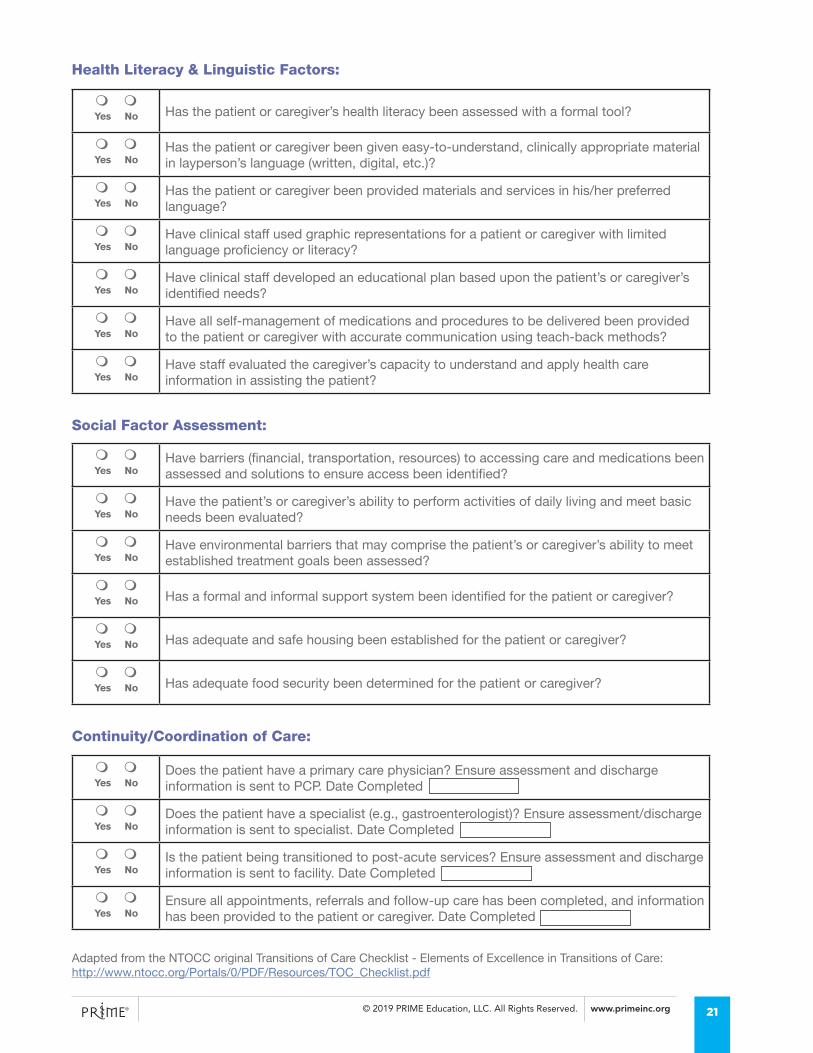
m mYes No Has the patient or caregiver’s health literacy been assessed with a formal tool?
m mYes No
Has the patient or caregiver been given easy-to-understand, clinically appropriate material in layperson’s language (written, digital, etc.)?
m mYes No
Has the patient or caregiver been provided materials and services in his/her preferred language?
m mYes No
Have clinical staff used graphic representations for a patient or caregiver with limited language proficiency or literacy?
m mYes No
Have clinical staff developed an educational plan based upon the patient’s or caregiver’s identified needs?
m mYes No
Have all self-management of medications and procedures to be delivered been provided to the patient or caregiver with accurate communication using teach-back methods?
m mYes No
Have staff evaluated the caregiver’s capacity to understand and apply health care information in assisting the patient?
m mYes No
Have barriers (financial, transportation, resources) to accessing care and medications been assessed and solutions to ensure access been identified?
m mYes No
Have the patient’s or caregiver’s ability to perform activities of daily living and meet basic needs been evaluated?
m mYes No
Have environmental barriers that may comprise the patient’s or caregiver’s ability to meet established treatment goals been assessed?
m mYes No Has a formal and informal support system been identified for the patient or caregiver?
m mYes No Has adequate and safe housing been established for the patient or caregiver?
m mYes No Has adequate food security been determined for the patient or caregiver?
m mYes No
Does the patient have a primary care physician? Ensure assessment and discharge information is sent to PCP. Date Completed
m mYes No
Does the patient have a specialist (e.g., gastroenterologist)? Ensure assessment/discharge information is sent to specialist. Date Completed
m mYes No
Is the patient being transitioned to post-acute services? Ensure assessment and discharge information is sent to facility. Date Completed
m mYes No
Ensure all appointments, referrals and follow-up care has been completed, and information has been provided to the patient or caregiver. Date Completed
Health Literacy & Linguistic Factors:
Social Factor Assessment:
Continuity/Coordination of Care:
Adapted from the NTOCC original Transitions of Care Checklist - Elements of Excellence in Transitions of Care: http://www.ntocc.org/Portals/0/PDF/Resources/TOC_Checklist.pdf
21
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
RESOURCES TO SUPPORT TRANSITIONS OF CARE PATHWAYS IN CDI
• National Transitions of Care Coalition
• Institute for Healthcare Improvement
• Care Transitions Program
• Project BOOST (Better Outcomes for Older Adults Through Safer Transitions)
• Project RED (Re-Engineering the Discharge)
• Post-Acute Care Transitions (PACT) Toolkit
• Partnership for Patients Inter-Facility Infection Control Form
• C Diff Foundation (Education and advocacy resources for patients and healthcare facility providers)
TOOLS TO REDUCE PRIMARY CDI
• CDC Core Elements of Hospital Antibiotic Stewardship Program and checklist
• CDC Get Smart: When Antibiotics Work/Get Smart for Healthcare
• AHRQ Healthcare-Associated Infections Program
• National Action Plan to Prevent Health Care-Associated Infections: Road Map to Elimination
• Quality scores (CMS quality reporting since 2013; Quality Innovation Networks)
• Appropriate controls (State Antibiotic Resistance Prevention Programs)
• National Strategy to Combat Antibiotic Resistant Bacteria
• Hospital Antibiotic Stewardship Program
• CMS Quality Innovation Network National Coordinating Center
22
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
REFERENCES1. Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement American
College of Physicians-Society of General Internal Medicine-Society of Hospital Medicine-American Geriatrics Society-American College of Emergency Physicians-Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976. doi:10.1007/s11606-009-0969-x
2. Magill SS, O’Leary E, Janelle SJ, et al. Changes in Prevalence of Health Care–Associated Infections in U.S. Hospitals. N Engl J Med. 2018;379(18):1732-1744. doi:10.1056/NEJMoa1801550
3. Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. 2015;372(16):1539-1548. doi:10.1056/NEJMra1403772
4. Garey KW, Aitken SL, Gschwind L, et al. Development and validation of a clostridium difficile health-related quality-of-life questionnaire. J Clin Gastroenterol. 2016;50(8):631-637. doi:10.1097/MCG.0000000000000473
5. Wilcox MH, Ahir H, Coia JE, et al. Impact of recurrent Clostridium difficile infection: Hospitalization and patient quality of life. J Antimicrob Chemother. 2017;72(9):2647-2656. doi:10.1093/jac/dkx174
6. Heinrich K, Harnett J, Vietri J, Chambers R, Yu H, Zilberberg M. Impaired Quality of Life, Work, and Activities Among Adults with Clostridium difficile Infection: A Multinational Survey. Dig Dis Sci. 2018;63(11):2864-2873. doi:10.1007/s10620-018-5222-1
7. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile Infection in the United States. N Engl J Med. 2015;372(9):825-834. doi:10.1056/NEJMoa1408913
8. Alam MJ, Walk ST, Endres BT, et al. Community Environmental Contamination of Toxigenic Clostridium difficile. Open forum Infect Dis. 2017;4(1):ofx018-ofx018. doi:10.1093/ofid/ofx018
9. Khanna S, Pardi DS, Aronson SL, et al. The Epidemiology of Community-acquired Clostridium difficile infection : A population-based study. Am J Gastroenterol. 2012;2011(1):89-95. doi:10.1038/ajg.2011.398.The
10. Chitnis AS, Holzbauer SM, Belflower RM, et al. Epidemiology of community-associated Clostridium difficile infection, 2009 through 2011. JAMA Intern Med. 2013;173(14):1359-1367. doi:10.1001/jamainternmed.2013.7056
11. Gupta A, Khanna S. Community-acquired clostridium difficile infection: An increasing public health threat. Infect Drug Resist. 2014;7:63-72. doi:10.2147/IDR.S46780
12. Ofori E, Ramai D, Dhawan M, Mustafa F, Gasperino J, Reddy M. Community-acquired Clostridium difficile: epidemiology, ribotype, risk factors, hospital and intensive care unit outcomes, and current and emerging therapies. J Hosp Infect. 2018;99(4):436-442. doi:10.1016/j.jhin.2018.01.015
13. Tschudin-Sutter S, Kuijper EJ, Durovic A, et al. Guidance document for prevention of Clostridium difficile infection in acute healthcare settings. Clin Microbiol Infect. 2018;24(10):1051-1054. doi:10.1016/j.cmi.2018.02.020
14. Lee RM, Fishman NO. Increasing Economic Burden of Inpatient Clostridium difficile Infection in the United States: National Trends in Epidemiology, Outcomes, and Cost of Care from 2000 to 2014. Open Forum Infect Dis. 2017;4(Suppl 1):S392-S392. doi:10.1093/ofid/ofx163.976
15. Centers for Disease Control and Prevention. Nearly half a million Americans suffered from Clostridium difficile infections in a single year. https://www.cdc.gov/media/releases/2015/p0225-clostridium-difficile.html.
16. Zhang D, Prabhu V, Burrell E, Marcella S. Attributable Health Care Resource Utilization and Costs for Patients With Primary and Recurrent Clostridium Difficile Infection in the United States. Clin Infect Dis. 2018;66(9):1326-1332. doi:10.1016/j.jval.2016.03.1213
17. Zhang S, Palazuelos-Munoz S, Balsells EM, Nair H, Chit A, Kyaw MH. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect Dis. 2016;16(1). doi:10.1186/s12879-016-1786-6
18. Reveles KR, Dotson KM, Gonzales-Luna A, et al. Clostridioides (Formerly Clostridium) difficile Infection During Hospitalization Increases the Likelihood of Nonhome Patient Discharge. Clin Infect Dis. 2019;68(11):1887-1893. doi:10.1093/cid/ciy782
19. Chopra T, Neelakanta A, Dombecki C, et al. Burden of Clostridium Difficile Infection on Hospital Readmissions and Its Potential Impact under the Hospital Readmission Reduction Program. Vol 43. 2015. doi:10.1016/j.ajic.2014.11.004
20. Howard KA. Preventing 30-Day Readmissions of Clostridium difficile Patients Utilizing Targeted Discharge Instructions [Doctor of Nursing Practice project]. San Francisco: University of San Francisco; 2015.
21. Rock C, Pana Z, Leekha S, et al. National Healthcare Safety Network laboratory-identified Clostridium difficile event reporting: A need for diagnostic stewardship. Am J Infect Control. 2018;46(4):456-458. doi:10.1016/j.ajic.2017.10.011
22. National Healthcare Safety Network (NHSN) Facility-wide Inpatient Hospital-onset Clostridium difficile Infection (CDI) Outcome Measure
23

© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
23. Brown KA, Khanafer N, Daneman N, Fisman DN. Meta-analysis of antibiotics and the risk of community-associated Clostridium difficile infection. Antimicrob Agents Chemother. 2013;57(5):2326-2332. doi:10.1128/aac.02176-12
24. Agency for Healthcare Research and Quality. The Evaluation and Research on Antimicrobial Stewardship’s Effect on Clostridium Difficile (ERASE C. Difficile) Project Toolkit for Reduction of Clostridium Difficile Through Antimicrobial Stewardship.; 2012.
25. Ofori E, Ramai D, Dhawan M, Mustafa F, Gasperino J, Reddy M. Community-acquired Clostridium difficile: epidemiology, ribotype, risk factors, hospital and intensive care unit outcomes, and current and emerging therapies. J Hosp Infect. 2018;99(4):436-442. doi:10.1016/j.jhin.2018.01.015
26. Barlam TF, Cosgrove SE, Abbo LM, et al. Executive summary: Implementing an antibiotic stewardship program: Guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin Infect Dis. 2016;62(10):1197-1202. doi:10.1093/cid/ciw217
27. Baur D, Gladstone BP, Burkert F, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(9):990-1001. doi:10.1016/S1473-3099(17)30325-0
28. Hills RD, Pontefract BA, Mishcon HR, Black CA, Sutton SC, Theberge CR. Gut Microbiome: Profound Implications for Diet and Disease. Nutrients. 2019;11(7):1613. doi:10.3390/nu11071613
29. Patel R, Dupont HL. New approaches for bacteriotherapy: Prebiotics, new-generation probiotics, and synbiotics. Clin Infect Dis. 2015;60(Suppl 2):S108-S121. doi:10.1093/cid/civ177
30. McDonald LC, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018;66(7):e1-e48. doi:10.1093/cid/cix1085
31. Gerding DN, Muto CA, Owens RC. Measures to control and prevent Clostridium difficile infection. Clin Infect Dis. 2008;46 Suppl 1(s1):S43-9. doi:10.1086/521861
32. Prevention. USC for DC and. Strategies to Prevent Clostridioides difficile Infection in Acute Care Facilities. https://www.cdc.gov/hai/prevent/cdi-prevention-strategies.html.
33. Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32(9):920-924. doi:10.3109/00365529709011203
34. Gupta A, Cifu AD, S. K. Diagnosis and treatment of Clostridium difficile infection. JAMA - J Am Med Assoc. 2018;320(10):1031-1032.
35. Morgan DJ, Malani P, Diekema DJ. Diagnostic stewardship - leveraging the laboratory to improve antimicrobial use. JAMA - J Am Med Assoc. 2017;318(7):607-608. doi:10.1001/jama.2017.8531
36. Surawicz CM, Brandt LJ, Binion DG, et al. Guidelines for diagnosis, treatment, and prevention of clostridium difficile infections. Am J Gastroenterol. 2013;108(4):478-498. doi:10.1038/ajg.2013.4
37. Johnson S, Louie TJ, Gerding DN, et al. Vancomycin, metronidazole, or tolevamer for Clostridium difficile infection: results from two multinational, randomized, controlled trials. Clin Infect Dis. 2014;59(3):345-354. doi:10.1093/cid/ciu313
38. Stevens VW, Nelson RE, Schwab-Daugherty EM, et al. Comparative effectiveness of vancomycin and metronidazole for the prevention of recurrence and death in patients with clostridium difficile infection. JAMA Intern Med. 2017;177(4):546-553. doi:10.1001/jamainternmed.2016.9045
39. Louie TJ, Cannon K, Byrne B, et al. Fidaxomicin preserves the intestinal microbiome during and after treatment of clostridium difficile infection (CDI) and reduces both toxin reexpression and recurrence of CDI. Clin Infect Dis. 2012;55(SUPPL.2):132-142. doi:10.1093/cid/cis338
40. Cornely OA, Nathwani D, Ivanescu C, Odufowora-Sita O, Retsa P, Odeyemi IAO. Clinical efficacy of fidaxomicin compared with vancomycin and metronidazole in Clostridium difficile infections: A meta-analysis and indirect treatment comparison. J Antimicrob Chemother. 2014;69(11):2892-2900. doi:10.1093/jac/dku261
41. Goldenberg SD, Brown S, Edwards L, et al. The impact of the introduction of fidaxomicin on the management of Clostridium difficile infection in seven NHS secondary care hospitals in England: a series of local service evaluations. Eur J Clin Microbiol Infect Dis. 2016;35(2):251-259. doi:10.1007/s10096-015-2538-z
42. Guery B, Menichetti F, Anttila VJ, et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. Lancet Infect Dis. 2018;18(3):296-307. doi:10.1016/s1473-3099(17)30751-x
43. Aitken SL, Joseph TB, Shah DN, et al. Healthcare resource utilization for recurrent Clostridium difficile infection in a large university hospital in Houston, Texas. PLoS One. 2014;9(7):5-9. doi:10.1371/journal.pone.0102848
44. Dieterle MG, Rao K, Young VB. Novel therapies and preventative strategies for primary and recurrent Clostridium difficile infections. Ann N Y Acad Sci. 2018. doi:10.1111/nyas.13958
24

© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
45. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile Infection in the United States. N Engl J Med. 2015;372(9):825-834. doi:10.1056/NEJMoa1408913
46. Gerding DN, Kelly CP, Rahav G, et al. Bezlotoxumab for Prevention of Recurrent Clostridium difficile Infection in Patients at Increased Risk for Recurrence. Clin Infect Dis. 2018;67(5):649-656. doi:10.1093/cid/ciy171
47. Dubberke ER, Olsen MA. Burden of clostridium difficile on the healthcare system. Clin Infect Dis. 2012;55(SUPPL.2):88-92. doi:10.1093/cid/cis335
48. Desai K, Gupta SB, Dubberke ER, Prabhu VS, Browne C, Mast TC. Epidemiological and economic burden of Clostridium difficile in the United States: Estimates from a modeling approach. BMC Infect Dis. 2016;16(1). doi:10.1186/s12879-016-1610-3
49. Seekatz AM, Young VB. Clostridium difficile and the microbiota. J Clin Invest. 2014;124(10):4182-4189. doi:10.1172/jci72336
50. Peniche AG, Savidge TC, Dann SM. Recent insights into Clostridium difficile pathogenesis. Curr Opin Infect Dis. 2013;26(5):447-453. doi:10.1097/01.qco.0000433318.82618.c6
51. Drug approval package: Zinplava injection (bezlotoxumab). US Food and Drug Administration. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2016/761046_toc.cfm
52. Wilcox MH, Gerding DN, Poxton IR, et al. Bezlotoxumab for Prevention of Recurrent Clostridium difficile Infection. N Engl J Med. 2017;376(4):305-317. doi:10.1056/NEJMoa1602615
53. Hota SS, Sales V, Tomlinson G, et al. Oral vancomycin followed by fecal transplantation versus tapering oral vancomycin treatment for recurrent clostridium difficile infection: An open-label, randomized controlled trial. Clin Infect Dis. 2017;64(3):265-271. doi:10.1093/cid/ciw731
54. Kelly CR, Khoruts A, Staley C, et al. Effect of fecal microbiota transplantation on recurrence in multiply recurrent clostridium difficile infection a randomized trial. Ann Intern Med. 2016;165(9):609-616. doi:10.7326/M16-0271
55. Hussey PS, Schneider EC, Rudin RS, Fox DS, Lai J, Pollack CE. Continuity and the costs of care for chronic disease. JAMA Intern Med. 2014;174(5):742-748. doi:10.1001/jamainternmed.2014.245
56. Gadbois EA, Tyler DA, Shield RR, et al. Medicare Advantage Control of Post-Acute Costs: Perspectives From Plans, Hospitals, and Skilled Nursing Facilities. Innov Aging. 2018;2(suppl_1):409-409. doi:10.1093/geroni/igy023.1525
57. Horowitz LI. Quality of discharge practices and patient understanding at an academic medical center. JAMA Intern Med. 2013;71(2):233-236. doi:10.1038/mp.2011.182.doi
58. Hansen LO, Young RS, Hinami K, Leung A, Williams M V. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med. 2011;155(8):520-528. doi:10.7326/0003-4819-155-8-201110180-00008
59. Kripalani S, Theobald CN, Anctil B, Vasilevskis EE. Reducing Hospital Readmission: Current Strategies and Future Directions. Ann Rev Med. 2014;65:471-485.
60. Kooyman CDA, Witry MJ. The developing role of community pharmacists in facilitating care transitions: A systematic review. J Am Pharm Assoc. 2019;59(2):265-274. doi:10.1016/j.japh.2018.11.009
61. Rosenbek S, Coleman EA. The Care Transitions Intervention. Compr Care Coord Chronically III Adults. 2013;166:261-275. doi:10.1002/9781118785775.ch13
62. Noel K, Yagudayev S, Messina C, Schoenfeld E, Hou W, Kelly G. Tele-transitions of care. A 12-month, parallel-group, superiority randomized controlled trial protocol, evaluating the use of telehealth versus standard transitions of care in the prevention of avoidable hospital readmissions. Contemp Clin Trials Commun. 2018;12(July):9-16. doi:10.1016/j.conctc.2018.08.006
63. Oh EG, Lee HJ, Yang YL, Kim YM. Effectiveness of Discharge Education With the Teach-Back Method on 30-Day Readmission: A Systematic Review. J Patient Saf. 9000;Publish Ah.
64. Halasyamani L, Kripalani S, Coleman E, Schnipper J, van Walraven C, Nagamine J, Torcson P, Bookwalter T, Budnitz T MD. Transition of Care for Hospitalized Elderly. J Hosp Med. 2006;6:354-360. doi:10.1002/jhm.129.
65. Kripalani S, LeFevre F, Phillips CO, Williams M V., Basaviah P, Baker DW. Deficits in Communication and Information Transfer Between Hospital-Based and Primary Care Physicians. Jama. 2007;297(8):831. doi:10.1001/jama.297.8.831
66. Centers for Medicare and Medicaid. The Hospital Conditions of Participation and Interpretive Guidelines.; 2004.
67. O’Leary KJ, Liebovitz DM, Feinglass J, et al. Creating a better discharge summary: Improvement in quality and timeliness using an electronic discharge summary. J Hosp Med. 2009;4(4):219-225. doi:10.1002/jhm.425
25
© 2019 PRIME Education, LLC. All Rights Reserved. www.primeinc.org
Learning Objectives
� Apply evidence-based and expert consensus strategies for closing critical gaps in Clostridioides difficile infection (CDI) care transitions and coordination
� Incorporate evidence- and guideline-informed approaches for assessing risk in, diagnosing, and treating patients with primary or recurrent CDI
� Develop comprehensive hospital discharge plans that account for individual patient factors, including comorbidities and socioeconomic factors
� Apply interprofessional strategies for patient-centered CDI care, including patient/caregiver education, shared decision-making, and adherence promotion
Instructions to obtain credit:
1. Complete the activity in its entirety.
2. Visit PRIME®’s Credit Center at www.primeinc.org/credit.
3. Enter program code 72PR191.
4. Upon completion of the learner assessment tools, you will be able to print your certificate.
Release Date: September 16, 2019 Expiration Date: September 16, 2020
This activity is provided by PRIME Education. There is no fee to participate. This activity is supported by an educational grant from Merck & Co. Inc.
Accreditation Statements
In support of improving patient care, PRIME® is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the healthcare team. This activity was planned by and for the healthcare team, and learners will receive 1.0 Interprofessional Continuing Education (IPCE) credits for learning and change.
Physician Credit Designation Statement PRIME Education, LLC (PRIME®) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. PRIME® designates this Enduring material for a maximum of 1.0 AMA PRA Category 1 Credits™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
Physician Assistant Accreditation Statement PRIME® has been authorized by the American Academy of PAs (AAPA) to award AAPA Category 1 CME credit for activities planned in accordance with AAPA CME Criteria. This activity is designated for 1.0 AAPA Category 1 CME credit. PAs should only claim credit commensurate with the extent of their participation.
Nurse Practitioner Accreditation Statement PRIME® is accredited by the American Association of Nurse Practitioners as an approved provider of nurse practitioner continuing education. Provider number: 060815. This activity is approved for 1.0 contact hour of continuing education (which includes 0.2 hours of pharmacology).
Pharmacist Accreditation Statement This Application-based activity has been approved for 1.0 contact hour (0.1 CEUs) by PRIME® for pharmacists. The Universal Activity Number for this activity is JA0007144-0000-19-080-H01-P. Pharmacy CE credits can be electronically submitted to the NABP upon successful completion of the activity. Pharmacists with questions can contact NABP customer service ([email protected]).
Nurse Accreditation Statement PRIME Education, LLC (PRIME®) is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. PRIME® designates this activity for 1.0 contact hour.
Case Manager Accreditation Statement The Commission for Case Manager Certification designates this educational activity for 1.0 contact hour for certified case managers. Credits for this program are pre-approved.
26
Cheri Lattimer RN, BSNExecutive DirectorNational Transitions of Care CoalitionWashington, DC
Sahil Khanna, MBBSAssociate Professor of MedicineGastroenterology and HepatologyMayo ClinicRochester, MN
Nancy C CarallaFounder and Executive DirectorC Diff FoundationNew Port Richey, FL
James E Lett, II, MD, CMDFamily Medicine PhysicianMedical DirectorAvar ConsultingRockville, MDDirector of the National BoardNational Transitions of Care CoalitionWashington, DC
Kevin W Garey, PharmDProfessor and Chair Department of Pharmacy Practice and Translational ResearchUniversity of HoustonHouston, TX
The following individuals have identified relevant financial relationships with commercial interests to disclose:
Kevin W Garey, PharmD, MS, FASHP (Contributing Author)
Consultant – Merck and CoPrincipal Investigator of Research Grant – Merck and Co
Sahil Khanna, MBBS (Contributing Author)
Consultant – Premier IncPrincipal Investigator of Research Grant – Ferring Pharmaceuticals
The following individuals have no relevant financial relationships with commercial interests to disclose:
Cheri Lattimer, RN, BSN (Author)
James E Lett, II, MD, CMD (Author)
Nancy C Caralla (Author)
Kathleen A Jarvis, MS, RN, CCM (Reviewer)
Joyce M Knestrick, PhD, CRNP, FAANP (Planner)
Mark A Rubin, MD (Planner)
All PRIME staff participating in planning and content development have no relevant financial relationships with commercial interests to disclose.
Contributing Authors