Embed Size (px)
Citation preview

Principles of pharmacology inPrinciples of pharmacology innneurology eurology
Presented by:Dr mehran Homam Neurologist & Neurophysiologist
Department of neurologyMashhad azad university

Topics Topics
1-Headache2-Parkinson3-Multiple Sclerosis4-Dementia5-Epilepsy
(from Solomon S, Lipton RB. Headache 1991;31(6):384-7.)

1-Headache1-Headache

HeadacheHeadacheA Common Health ProblemA Common Health Problem
Headache has troubled humankind from the dawn of civilization
Evidence of trepanation, an early form of neurosurgery, was found on skulls from 7000 BC
Migraine symptoms,have been described for over 1,000 years

Primary Headaches Primary Headaches
Benign, recurrent
NOT associated with underlying pathology
The headache is the disease(from Solomon S, Lipton RB. Headache 1991;31(6):384-7.)

Primary Headaches Primary Headaches Migraine (with or without aura)
Tension-type headache (episodic or chronic)
Cluster headache
(from Solomon S, Lipton RB. Headache 1991;31(6):384-7.)

Primary HeadachePrimary Headache
Migraine
TensionCluster

QUESTIONSQUESTIONS
1-SEVERITY 2-QUALITY 3-DURATION 4-ASSOCIATED SYMPTOMS & SIGNS 5-PEAK ONSET 6-FREQUENCY 7-AGGREVATING AND RELIEVING 8-LOCATION

Migraine HeadachesMigraine Headaches

Hildegard von Bingen
Famous people suffering from migraine
Sigmund Freud
Ludwig van Beethoven
Madame de Pompadour

What is Migraine?What is Migraine?
Repeated attacks of throbbing headache – Moderately or severely painful– Frequent or infrequent– Last a few hours to a couple of days
Often only one side of the head hurts Often experience loss of appetite, nausea, and
vomiting;photophobia;phonophobia Periodic familial
World Federation of Neurology

1Migraine originates deep within the brain
2Electrical impulses spread to other regions of the brain.
3Changes in nerve cell activity and blood flow may result in visual disturbance, numbness or tingling, and dizziness.
4Chemicals in the brain cause blood vessel dilation and inflammation of the surrounding tissue
5The inflammation irritates the trigeminal nerve, resulting in severe or throbbing pain
How Migraine WorksHow Migraine Works

MigraineMigraineMajor Forms:Migraine without aura (common) 70%Migraine with aura (classical) 25%Migraine variants and complicated
migraine 5%

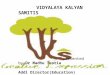
How Migraine Stacks Up Against Other How Migraine Stacks Up Against Other Common DiseasesCommon Diseases
From the Centers for Disease Control and Prevention, the US Census Bureau, and the Arthritis Foundation.
1%
5%6%
7%
12%
Rheumatoid arthritis
Asthma Diabetes Osteoarthritis Migraine
Affected patientss:

0
5
10
15
20
25
30
10 20 30 40 50 60 70 80 90
Women
Men
Age (years)
Per
cent
age
Stewart WF, Lipton RB, et al. JAMA. 1992;267(1):64-69.
Migraine PrevalenceMigraine Prevalence



The Stages of a Migraine AttackThe Stages of a Migraine Attack

1.2% 18.4%
47.2%
33.2%
Mild
Moderately severe
Severe
Extremely severe
Most Patients’ Headaches Are Most Patients’ Headaches Are Severe or Extremely SevereSevere or Extremely Severe
National Headache Foundation. American Migraine Study II: Migraine in the United States: Burden of Illness and Patterns of Treatment

52%39%
9%
Need bed restCan work with some difficulty
Can work as normal
Migraine Takes Quality Time Out Migraine Takes Quality Time Out From Your LifeFrom Your Life
National Headache Foundation. American Migraine Study II: Migraine in the United States: Burden of Illness and Patterns of Treatment

Unnecessary SufferingUnnecessary Suffering
More than half of people with migraine suffer for at least a year before they are diagnosed with migraine
38% suffer for 3 or more years
National Headache Foundation. American Migraine Study II: Migraine in the United States: Burden of Illness and Patterns of Treatment

What You Might Experience What You Might Experience During an AttackDuring an Attack
Nausea Vomiting Diarrhea Sweating Cold hands Sensitivity to light
Sensitivity to sound Scalp tenderness Pale color Pulsing temple Pressure pain

Triggers and Risk Factors
Migraine headaches are often triggered by specific things

Triggers: Changes in Daily CyclesTriggers: Changes in Daily Cycles

Triggers: Environment or DietTriggers: Environment or Diet

Triggers: MentalTriggers: Mental

Protective FactorsProtective Factors
Regular sleepRegular mealsRegular exerciseBiofeedbackHealthy lifestyle

TreatmentTreatment
Acute:1-nsaids
2-Ergo
3-Triptans
4-Corton
Prophylactic

DHEDHE
Dihydroergotamine – Nasal Spray (Migranal®)– Injectable (D.H.E. )
- Supp
- Tab

Your Symptoms May Affect The Your Symptoms May Affect The Choice of Medication Choice of Medication
Medication Type Pro Con
Oral (tablets) Easy to take Won’t work if you are vomiting
Nasal spray Good for patient with nausea/vomiting, easy
to use
Fewer choices
Injection Works fast Harder to use

1-Ergotamines1-Ergotamines
Ergotamine Ergotamine C Mechanism:Ergots 2-advantages:The most effective 3-Contraindications:Htn-Pregnancy-IHD-Raynoud
disease 4-Disadventages:Ergotism/limitation of Dosage/age 5-Dosage :6 mg in attack 10mg each week Drug reactions:

2-triptans2-triptans
Triptans need to be taken as soon as you recognize an attack– Most patients wait too long – No need to suffer
Triptans work best in the first couple of hours of an attack Mechanism:serotonin agonist Dihydroergotamine works at any time during an attack Available :sumatriptan 50 mg also sc 8mg Dosage; Advantage:faster Effect / Sc injection Disadventage:Relapse/Cost

3-(NSAID)Medicines to Stop a 3-(NSAID)Medicines to Stop a Migraine AttackMigraine Attack
Mechanism:anti inflammatory Adventages: Very effective.tension headache Disadventages:Side effects medications – use with care and tell your doctor
– NSAIDs (eg, ibuprofen, naproxen,indometacin) – Aspirin, acetaminophen, caffeine combination
(avoid using more often than twice a week, especially if using several agents or if you drink a lot of coffee, tea, or caffeinated soda)

Options for Preventive TreatmentOptions for Preventive Treatment
Divalproex sodium/sodium valproate (anticonvulsant) Propranolol (beta-blocker) Timolol (beta-blocker) Methysergide (serotonin antagonist) Other anticonvulsants Other beta-blockers Antidepressants NSAIDs (eg, aspirin)
These are medicines you take every day to prevent headaches

Some Medications May Cause Some Medications May Cause Migraine to Become ChronicMigraine to Become Chronic
May cause chronic headaches:
Opiates Combination analgesics Caffeine Barbiturate-containing
medications Ergotamine tartrate,
isometheptene Triptans Others
Not clearly associated with chronic headaches:
Acetaminophen Aspirin Dihydroergotamine Others

Self Treatment Efforts:Self Treatment Efforts:What You Can Do For Your MigrainesWhat You Can Do For Your Migraines
Rest Biofeedback Ice/heat Massage Exercise Avoid triggers
Seek treatment early
Keep a headache diary
Take medications as directed by your doctor
Many options are available for migraine relief – ask your doctor what’s right for you

Cluster HeadacheCluster Headache Duration
15 to 180 minutes untreated Pain characteristics
Severe unilateral orbital, supraorbital, or temporal pain Associated symptoms (at least 1)
Conjunctival injection, Lacrimation Nasal congestion, Rhinorrhea Forehead and facial swelling Miosis Eyelid Edema
Frequency: between 1 every other day to 8/day

Treatment of Cluster HeadacheTreatment of Cluster HeadacheAcute treatment:
– 100% Oxygen via face mask at 8liters/min given in a seated position
– SL ergotamine at onset of HA and repeated once if needed
– Triptans shown effective in two RCTs– Intranasal administration of a local
anesthetic (4% lidocaine) may be helpful

Treatment of Cluster HeadacheTreatment of Cluster HeadachePreventive Treatment
– Verapamil 80 mg qid– Lithium 300 - 900 mg per day– Prednisone 40 mg per day in divided
doses, tapered over 3 weeks– Ergotamine 2 mg 2 hrs before bedtime to
prevent nocturnal attacks– Divalproex sodium 600 - 2000 mg per day

Tension HeadacheTension Headache Duration
30 min to 7 days Pain characteristics (at least 2)
Pressing/tightening quality Mild to moderate severity Bilateral location No aggravation by routine physical activity
Associate symptoms (Must have both) No vomiting No more than one of: nausea, photophobia, phonophobia
H&P and diagnostic tests do not suggest underlying organic disease


Secondary HeadacheSecondary HeadacheSudden, progressive
Associated with pathology
May require immediate action

PatientPatient
45 years old with HTN and migraine once monthly
1-tab;Ergotamine c twice daily2-tab;valproate Na each night3-tab:advil; when pain qid