Embed Size (px)
Citation preview
Current Orthopaedics (2003) 17, 8^16�c 2003 Elsevier Science Ltd. All rights reserved.doi:10.1054/cuor.2000.0316
MINI-SYMPOSIUM:THEELECTIVEHAND
(ii) Principles of tendon transfer in the hand andforearmC.Heras-Palou and F.D.Burke
Pulvertaft Hand Centre,Derbyshire Royal In¢rmary,Derby DE12QY,UK
KEYWORDStendon transfer, handreconstruction, nerveinjury
Summary Tendon transfer is an important technique in the armamentarium of thesurgeon attempting to restore function to the hand. Adiscussion of the principles of thisprocedure and ofthe commonindications and techniques is presented in this paper.�c 2003 Elsevier Science Ltd.Allrights reserved.
INTRODUCTIONTendon transfer is a surgical procedure that involvesmoving the insertion of a tendon^muscle unit from onelocation to another. It is usually a salvage procedure andis part of the reconstructive armamentarium of the sur-geon, along with nerve repair andnerve grafting, tendongrafts, tenodesis, joint arthrodesis and free muscletransfer.
A tendon transfer can be used to restore grasp, im-prove the position of the hand in space, and to preventdeformity, dislocations and contractures. It is indicatedwhen there is a need to replace the function of a paral-ysed muscle (often after nerve injury) or damagedtendon, to splint joints or to prevent or treatcontractures.
Although there was some previous experience,tendon transfers were developed in the second half ofthe19th century,mainly in the lower limb afterpoliomye-litis. The principles were consolidated during the ¢rsthalf of the 20th century.
PRINCIPLESThe principles of tendon transfer are:
K An expendable muscle should be used as a donor.Theobjective is to cause minimal de¢cit when taking thedonormuscle.
K The donor muscle must be of su⁄cient strength1
(Table 1). The power of a donor muscle is usuallysomewhat reduced after transfer. It is thereforeimportant to take a strong muscle in anticipation of
Correspondence to: CH-P.Tel.: +441332 347141 (ex 2396); Fax: +441332254638; E-mail: [email protected]
some weakening arising from transfer (usually MRC 5muscles weaken to MRC 4). If a weak donor is chosen,it will be too weak for useful function after thetransfer.
K The amplitude of a donor muscle is also important(Table 2). Amplitude is the amount a muscle can bestretched from its resting position, plus the amountit contracts.This will be the main determinant of therange of movement.
K The line of pull should be straight to optimise theworking of the transfer. This is not always possibleand some transfers need to go through a pulley orthrough the interosseous membrane in the fore-arm. Signi¢cant alterations of direction througha pulley weakens the action of a tendon transfer,and therefore a more powerful motor will berequired.
K The correct tension for the transfer should beachieved to provide useful function.This is the criticalstep of the operation, although the patient can adjustthe tension of some transfers to a certain degree byaltering the position of the joints that the transfercrosses. For example, if extensor indicis propius (EIP)is transferred after an extensor pollicis rupture, thepatient can, to some extent, adjust the tension by£exion and extension of the wrist (the tenodesise¡ect).
K Transfer must be across supple joints. Anycontracture must be released ¢rst and joints shouldhave a good passive range of movement. A tendontransfer by itself will not correct a contracture.
K The transfer should lie in unscarred tissue, preferablythrough fatty subcutaneous tissue, to preventadhesions and to provide smooth gliding.
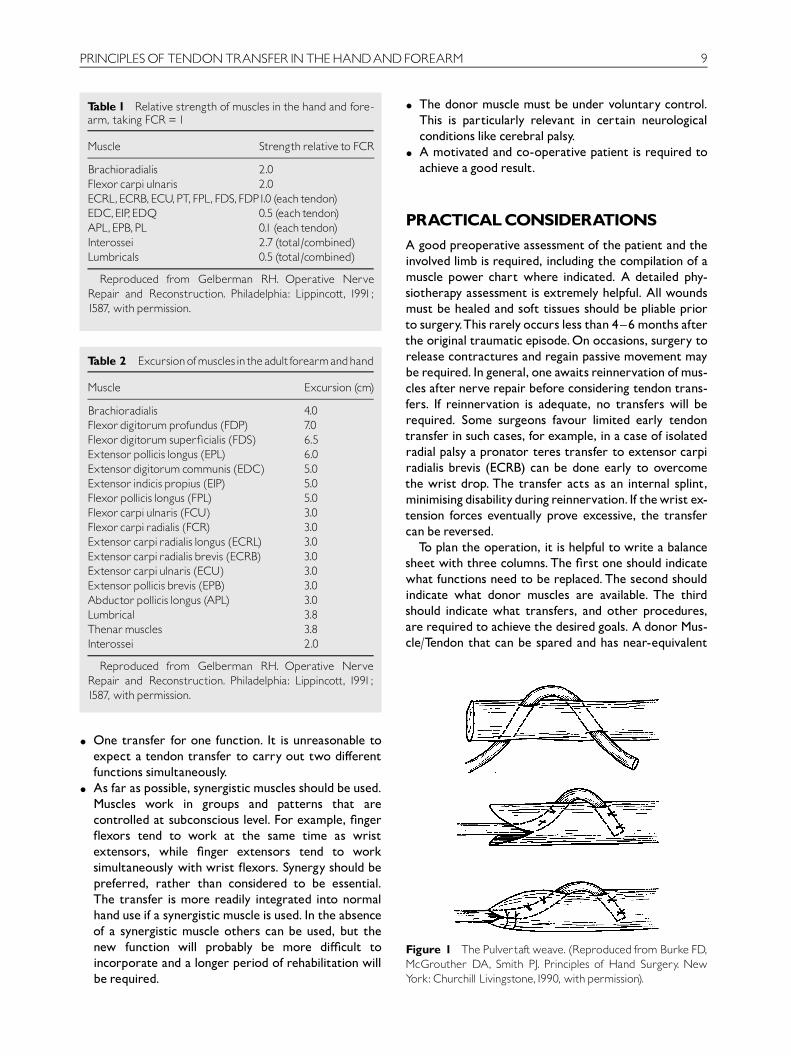
Table 2 Excursionofmusclesinthe adultforearmandhand
Muscle Excursion (cm)
Brachioradialis 4.0Flexordigitorumprofundus (FDP) 7.0Flexordigitorum super¢cialis (FDS) 6.5Extensor pollicis longus (EPL) 6.0Extensordigitorumcommunis (EDC) 5.0Extensor indicis propius (EIP) 5.0Flexor pollicis longus (FPL) 5.0Flexorcarpiulnaris (FCU) 3.0Flexorcarpiradialis (FCR) 3.0Extensorcarpiradialis longus (ECRL) 3.0Extensorcarpiradialis brevis (ECRB) 3.0Extensorcarpiulnaris (ECU) 3.0Extensor pollicis brevis (EPB) 3.0Abductor pollicis longus (APL) 3.0Lumbrical 3.8Thenarmuscles 3.8Interossei 2.0
Reproduced from Gelberman RH. Operative NerveRepair and Reconstruction. Philadelphia: Lippincott, 1991;1587, with permission.
Table 1 Relative strength of muscles in the hand and fore-arm, taking FCR = 1
Muscle Strength relative to FCR
Brachioradialis 2.0Flexorcarpiulnaris 2.0ECRL,ECRB,ECU,PT,FPL,FDS,FDP1.0 (eachtendon)EDC,EIP,EDQ 0.5 (eachtendon)APL,EPB,PL 0.1 (eachtendon)Interossei 2.7 (total/combined)Lumbricals 0.5 (total/combined)
Reproduced from Gelberman RH. Operative NerveRepair and Reconstruction. Philadelphia: Lippincott, 1991;1587, with permission.
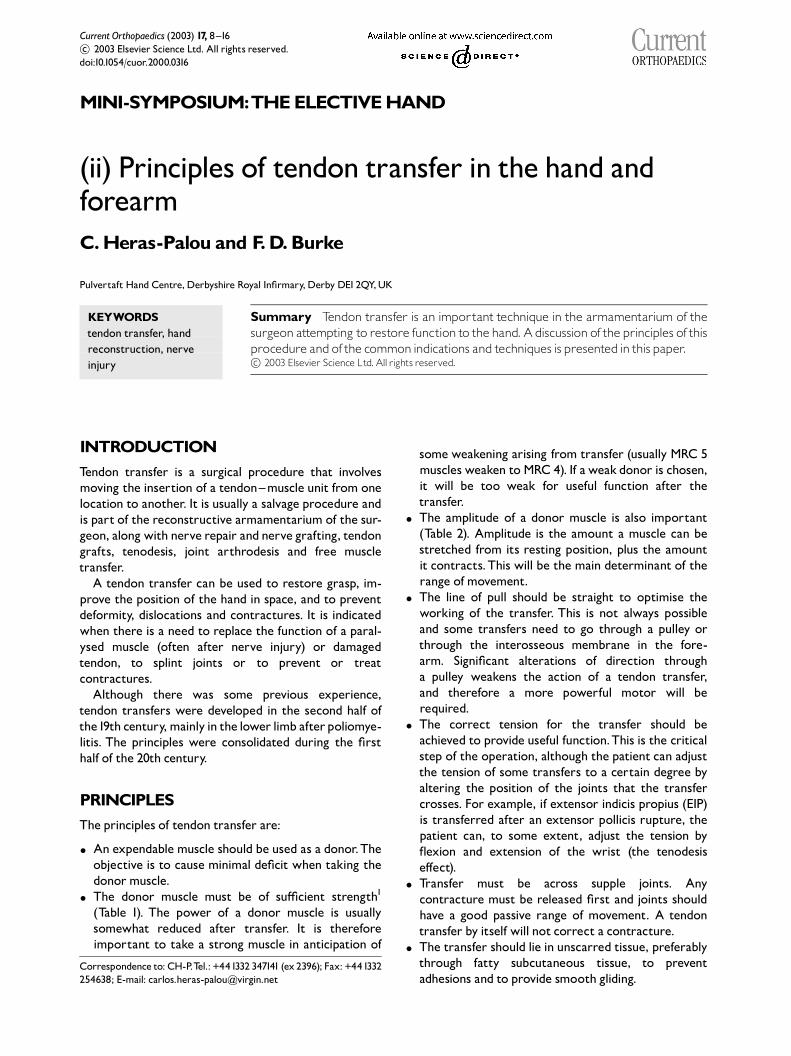
Figure 1 The Pulvertaftweave. (Reproduced from Burke FD,McGrouther DA, Smith PJ. Principles of Hand Surgery. NewYork:Churchill Livingstone,1990, with permission).
PRINCIPLESOF TENDONTRANSFER INTHEHANDANDFOREARM 9
K One transfer for one function. It is unreasonable toexpect a tendon transfer to carry out two di¡erentfunctions simultaneously.
K As far as possible, synergistic muscles should be used.Muscles work in groups and patterns that arecontrolled at subconscious level. For example, ¢nger£exors tend to work at the same time as wristextensors, while ¢nger extensors tend to worksimultaneously with wrist £exors. Synergy should bepreferred, rather than considered to be essential.The transfer is more readily integrated into normalhand use if a synergistic muscle is used. In the absenceof a synergistic muscle others can be used, but thenew function will probably be more di⁄cult toincorporate and a longer period of rehabilitation willbe required.
K The donor muscle must be under voluntary control.This is particularly relevant in certain neurologicalconditions like cerebral palsy.
K A motivated and co-operative patient is required toachieve a good result.
PRACTICALCONSIDERATIONSA good preoperative assessment of the patient and theinvolved limb is required, including the compilation of amuscle power chart where indicated. A detailed phy-siotherapy assessment is extremely helpful. All woundsmust be healed and soft tissues should be pliable priorto surgery.This rarely occurs less than 4^6months afterthe original traumatic episode.On occasions, surgery torelease contractures and regain passive movement maybe required. In general, one awaits reinnervation ofmus-cles after nerve repair before considering tendon trans-fers. If reinnervation is adequate, no transfers will berequired. Some surgeons favour limited early tendontransfer in such cases, for example, in a case of isolatedradial palsy a pronator teres transfer to extensor carpiradialis brevis (ECRB) can be done early to overcomethe wrist drop. The transfer acts as an internal splint,minimisingdisabilityduringreinnervation. If thewrist ex-tension forces eventually prove excessive, the transfercan be reversed.
To plan the operation, it is helpful to write a balancesheet with three columns. The ¢rst one should indicatewhat functions need to be replaced. The second shouldindicate what donor muscles are available. The thirdshould indicate what transfers, and other procedures,are required to achieve the desired goals. A donor Mus-cle/Tendon that can be spared and has near-equivalent

10 CURRENT ORTHOPAEDICS
strength and excursion to the tendon function that hasbeen lost should be sought. It is helpful if it is also syner-gistic with the dysfunctional tendon.
In the lower limb, it is common to insert the trans-ferred tendon into bone, while in the upper limb it isusually attached to tendon, usually by a weave as de-scribed by Pulvertaft (Fig.1) or by themethod describedby Andersen.2 If there is any possibility of reinnervation,it is prudent to perform end-to-side attachments.
When performing multiple tendon transfers, the do-nor muscles and recipient tendons are exposed at theonset. The motors are freed from their insertions andtransferred via subcutaneous tunnels to the new loca-tion.Care needs to be taken to provide a direction of pullthat is as straight as possible.Wounds that are no longerneeded can be closed at this stage. Transfers are thencompleted by suturing tendons into new insertions,with the correct tension, using the tenodesis test. Theremaining wounds are then closed.Careful haemostasisis required throughout the procedure.
After closing all wounds, the hand is splinted in a posi-tion that will protect the new transfers. On occasions,one positionwill not accommodate all transfers in a pro-tectedmanner.Perhaps one transfer requiring a di¡erentposition to the others may simply be transferred to thenew site at the initial operation, but tendonweavingmaybe delayed for 2 or 3 months until the other transfershave settled in.The ¢nal transfer can then be sutured tothe recipient tendon and splinted in a protectedmannerduring healing.
The tenodesis action and the tenodesis test
The mobility and power of the ¢ngers is created, in themain, by the strong forearmmuscles transmitting forcethrough the longdigital £exors and extensors.The intrin-sic muscles of the hand create additional power, particu-larly those innervated by the ulnar nerve. There isanother importantpower-adjuster available duringman-ual activities: the position of the wrist. Grip is poten-tiated by wrist extension and normal power grip is acombination of digital £exion andwristextension.Digitalextension from a position of power grip is potentiatedbywrist £exion and a normal wrist will drop to neutral ormild £exion during this manoeuvre. A mobile wristallows optimal digital function. The choice of tensionfor tendon transfers is frequently di⁄cult, but evensomewhat inappropriate tension can probably beadjusted by the patient through an alteration in wristposition to optimise the function of the transfer. Onoccasion, wrist fusion may be considered necessary in ahand and forearm reconstruction with tendon transfer.However, it is preferable to try to retain a mobile wristto optimise the results of the transfers.
The tenodesis test is used to assess the tension of atransfer prior to skin closure. The normal cascade ofthe ¢ngers (increasing £exion towards the ulnar borderdigits) moves from a position of £exion in maximal wristextension, to digital extension in maximal wrist £exion.A modest overcorrection of the original deformityshouldbe the aim,with thewristpassing through its nor-mal range of movement. If a digital £exor tendon recon-struction has been performed to the middle ¢nger, thetension should be adjusted so that the posture duringthe tenodesis test mimics the ulnar neighbour digit (i.e.the slightly more £exed ring ¢nger). If an extensor ten-don reconstruction has been performed to the middle¢nger, the tension should be adjusted to mimic the posi-tion of the radial neighbour digit (i.e. the slightly moreextended index ¢nger).
TRANSFERS FORHIGH- ANDLOW-MEDIANNERVEPALSYAttempts to restore continuity of themedian nerve pre-cede attempts to reconstruct the forearm or hand bytendon transfer. Sensibility is as important as power inhand function.
In a low-median nerve palsy, the main function thatneeds to be replaced is opposition of the thumb.Opposi-tion is a combinationmovementwith simultaneous rota-tion of the thumb into pronation and abduction awayfrom the palm. If there is a contracture of theweb space,it should be released before the transfer.
Themost commonly used donors are £exor digitorumsuper¢cialis (FDS) (ring), EIP, and palmaris longus (PL)(described by Camitz).
If FDS is chosen, the ring ¢nger super¢cial £exor is di-vided in the ¢nger, withdrawn to the palm and swungradially to the thumb, using palmar fascia or a strip of£exor carpi ulnaris (FCU) as a pulley (Fig. 2). It is anexample of a tendon transfer which does not have astraight pull and therefore needs to be powerful. Thetechnique is popular and e¡ective, but does weaken thegrip to a certain extent. For this reason, some surgeonsprefer to use amore expendable tendon: extensor indicispropius. This tendon (the more ulnar of the two indexextensors) is divided at mid-proximal phalanx level andwithdrawn to wrist level, passed around the ulnar bor-der of the lower forearm and across the £exor surfaceof the wrist and sutured onto the abductor insertion(Fig. 3). The line of pull recreates opposition moree⁄ciently.The skin of the donor ¢nger is closed withoutany repair of the extensor mechanism, which couldobstruct £exion.The remaining communis does not sub-lux radially. A Bunnel suture or a weave to the trans-ferred tendon creates a robust repair. The hand may berested on a volar slab holding the thumb in abduction
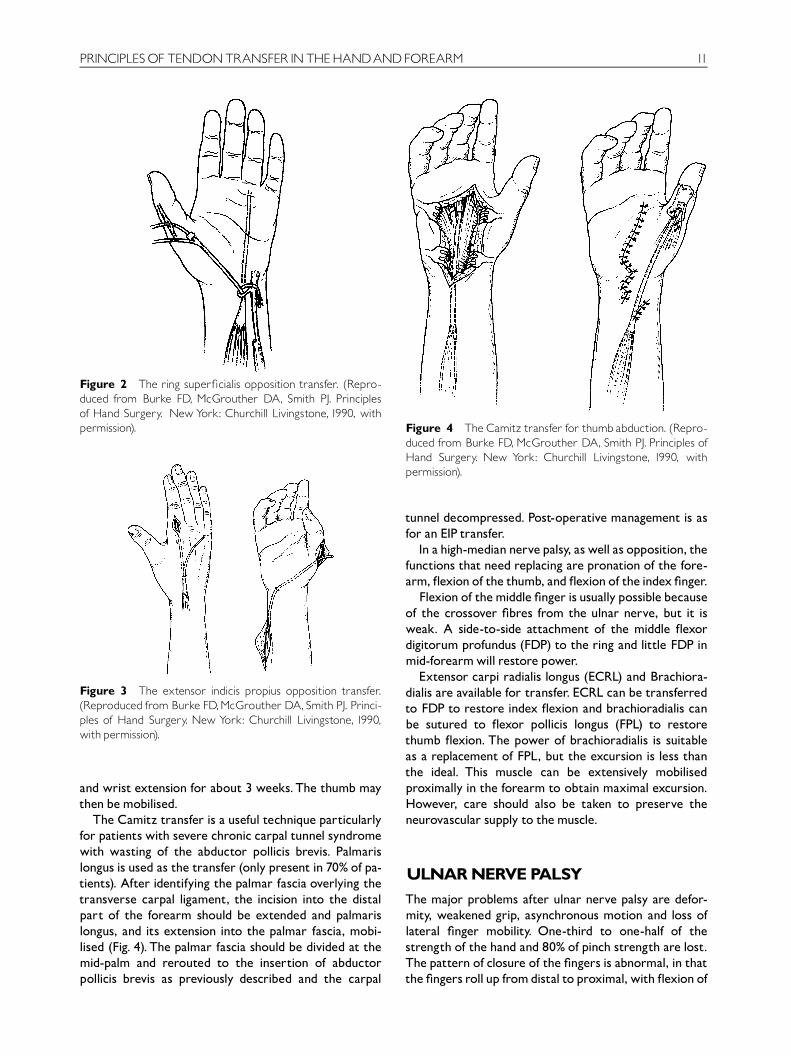
Figure 2 The ring super¢cialis opposition transfer. (Repro-duced from Burke FD, McGrouther DA, Smith PJ. Principlesof Hand Surgery. New York: Churchill Livingstone, 1990, withpermission).
Figure 3 The extensor indicis propius opposition transfer.(Reproduced from Burke FD,McGrouther DA,Smith PJ. Princi-ples of Hand Surgery. New York: Churchill Livingstone, 1990,with permission).
Figure 4 The Camitz transfer for thumb abduction. (Repro-duced from Burke FD, McGrouther DA, Smith PJ. Principles ofHand Surgery. New York: Churchill Livingstone, 1990, withpermission).
PRINCIPLESOF TENDONTRANSFER INTHEHANDANDFOREARM 11
and wrist extension for about 3 weeks.The thumb maythen bemobilised.
The Camitz transfer is a useful technique particularlyfor patients with severe chronic carpal tunnel syndromewith wasting of the abductor pollicis brevis. Palmarislongus is used as the transfer (only present in 70% of pa-tients). After identifying the palmar fascia overlying thetransverse carpal ligament, the incision into the distalpart of the forearm should be extended and palmarislongus, and its extension into the palmar fascia, mobi-lised (Fig. 4). The palmar fascia should be divided at themid-palm and rerouted to the insertion of abductorpollicis brevis as previously described and the carpal
tunnel decompressed. Post-operative management is asfor an EIP transfer.
In a high-median nerve palsy, as well as opposition, thefunctions that need replacing are pronation of the fore-arm, £exion of the thumb, and £exion of the index ¢nger.
Flexion of themiddle ¢nger is usually possible becauseof the crossover ¢bres from the ulnar nerve, but it isweak. A side-to-side attachment of the middle £exordigitorum profundus (FDP) to the ring and little FDP inmid-forearmwill restore power.
Extensor carpi radialis longus (ECRL) and Brachiora-dialis are available for transfer. ECRL can be transferredto FDP to restore index £exion and brachioradialis canbe sutured to £exor pollicis longus (FPL) to restorethumb £exion. The power of brachioradialis is suitableas a replacement of FPL, but the excursion is less thanthe ideal. This muscle can be extensively mobilisedproximally in the forearm to obtain maximal excursion.However, care should also be taken to preserve theneurovascular supply to themuscle.
ULNARNERVEPALSYThe major problems after ulnar nerve palsy are defor-mity, weakened grip, asynchronous motion and loss oflateral ¢nger mobility. One-third to one-half of thestrength of the hand and 80% of pinch strength are lost.The pattern of closure of the ¢ngers is abnormal, in thatthe ¢ngers roll up fromdistal to proximal, with £exion of
Figure 5 Zancolli volar plate ree¢ng. (Reproduced fromBurke FD,McGrouther DA,Smith PJ.Principlesof Hand Surgery.NewYork:Churchill Livingstone,1990, with permission).
Figure 6 Zancolli super¢cialis lasso. (Reproduced fromBurke FD,McGrouther DA,Smith PJ.Principlesof Hand Surgery.NewYork:Churchill Livingstone,1990, with permission).
12 CURRENT ORTHOPAEDICS
the proximal interphalangeal joint (PIPJ) and distal inter-phalangeal joint (DIPJ) before £exion of the MCP joint.This prevents normal grasp. Weak pinch is particularlydisabling, due to the paralysis of adductor pollicis.Thereis a characteristic claw deformity of the ring and little¢ngers.This is due to imbalance of the forces at the threejoints of each ¢nger.The lumbricalmuscles, and the inter-ossei, £ex the MCPJ and extend the PIPJ and DIPJ. If theyare notworking, the action of theunmodi¢ed long £exorsand extensors produces hyperextension of the MPJ and£exion of the IP joints. The little ¢nger is often ulnar-deviated in extension due to an unbalanced ulnar deviatingforce of the EDQ.This is called theWatenberg sign.
Whenever possible, nerve release or nerve repair isthe treatment of choice. Static or dynamic splints can beused as conservative treatment to correct the deformityof intrinsic paralysis. If there is irreversible paralytic lossof intrinsics, two types of surgical procedures are avail-able. One prevents MPJ hyperextension and includes adorsalboneblock, volar capsulorrhaphy (Fig. 5) or capsu-lodesis.The other augmentsMPJ £exion and interphalan-geal extension by sling tenodesis or tendon transfers.
Capsulodesis and tenodesis for ulnar claw deformity donot require a tendon transfer, but commonly stretch outwith the passage of time.Tendon transfers are preferablefor improving the function of thehand, since theyo¡er thebest chance of correcting the clawing, thereby improvinggrip strength andrestoring synchronousmotion at theMPand IP joints. All ulnar claw deformity tendon transfersmust pass volar to the deep transverse metacarpalligament. In the Stiles^Bunnell tendon transfer, two FDStendons are used, split and rerouted along the lumbricalcanal and sutured to the transverse ¢bres of theradial digital band. For patients with irreparabledistalulnarnerve lesions, this transfer remains anexcellentchoice.
Zancolli described the Lasso procedure where theFDS of each clawed ¢nger is detacheddistally andpassedthrough a transverse incision made in the A1 pulley,looped and sutured to itself in the distal palm.The FDSthen becomes a £exor of the MP joint (Fig. 6).
If clawing is not severe, surgical reconstruction mightbest be directed at improving power pinch. Restorationof a powerful pinch is an important aspect of ulnar nervepalsy reconstruction, yet it rarely gets the attention thatit merits. ECRB or brachioradialis can be augmentedwith a tendon graft which is passed through the thirdintermeta-carpal space and inserted into the radial sideof the thumb MCP joint, adducting and pronating thethumb (Fig. 7). An alternative is to transfer the FDS fromthe middle or ring ¢ngers to the abductor insertion inthe thumb, although grip strength is somewhat under-mined by this procedure. Index ¢nger abduction canbe recreated using a slip of abductor pollicis longusaugmentedwith a tendon graft, inserted into the lateralband of the index ¢nger.
TRANSFERS FORRADIALNERVEPALSYNerverepair is the treatmentof choice after radial nerveinjury, with tendon transfers held in reserve if reinnerva-tion does not occur.Digital andwrist extension aremassactions rather than precision activities and nerve repairoften produces satisfactory function.
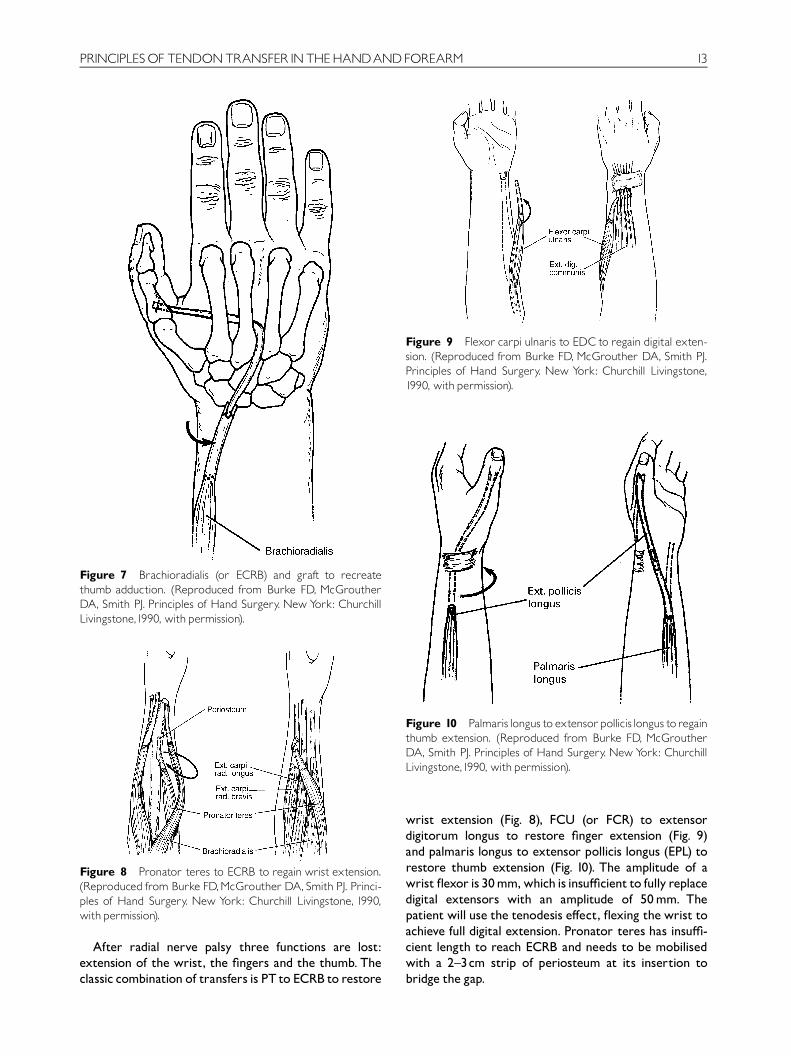
Figure 7 Brachioradialis (or ECRB) and graft to recreatethumb adduction. (Reproduced from Burke FD, McGroutherDA, Smith PJ. Principles of Hand Surgery. New York: ChurchillLivingstone,1990, with permission).
Figure 8 Pronator teres to ECRB to regain wrist extension.(Reproduced from Burke FD,McGrouther DA,Smith PJ. Princi-ples of Hand Surgery. New York: Churchill Livingstone, 1990,with permission).
Figure 9 Flexor carpi ulnaris to EDCto regain digital exten-sion. (Reproduced from Burke FD, McGrouther DA, Smith PJ.Principles of Hand Surgery. New York: Churchill Livingstone,1990, with permission).
Figure 10 Palmarislongus to extensorpollicislongus toregainthumb extension. (Reproduced from Burke FD, McGroutherDA, Smith PJ. Principles of Hand Surgery. New York: ChurchillLivingstone,1990, with permission).
PRINCIPLESOF TENDONTRANSFER INTHEHANDANDFOREARM 13
After radial nerve palsy three functions are lost:extension of the wrist, the ¢ngers and the thumb. Theclassic combination of transfers is PT to ECRB to restore
wrist extension (Fig. 8), FCU (or FCR) to extensordigitorum longus to restore ¢nger extension (Fig. 9)and palmaris longus to extensor pollicis longus (EPL) torestore thumb extension (Fig. 10). The amplitude of awrist £exor is 30mm,which is insu⁄cient to fully replacedigital extensors with an amplitude of 50mm. Thepatient will use the tenodesis e¡ect, £exing the wrist toachieve full digital extension. Pronator teres has insu⁄-cient length to reach ECRB and needs to be mobilisedwith a 2^3cm strip of periosteum at its insertion tobridge the gap.
14 CURRENT ORTHOPAEDICS
Transferring £exor carpi radialis (FCR) may cause aradial deviation of the wrist, particularly with a poster-ior interosseous nerve palsy, where the innervation toECRL is preserved. Flexor carpi ulnaris (FCU) seems too¡er an advantage in this situation, allowing thewrist tomove into a more suitable position of ulnar deviation. IfPL is absent, the option is to use FDS of middle and ring¢ngers through the interosseous membrane to motorextensor digitorum and EPL and, as before, PT to ECRB.This is known as Boyes transfer.
A patient with a radial nerve palsy may develop anadaptive functional pattern consisting of wrist £exion toachieve ¢nger extension. There are several types ofsplints that can be used, but all of them are cumbersomeand, at times, they need to beworn for a very long time.An option is to use the‘internal splint’procedurewhere aPT to ECRB transfer is carried out at the time of nerverepair in an end-to-side fashion, eliminating the need towear a splint during nerve regeneration. If wrist reinner-vation subsequently produces overactive wrist exten-sion, the transfer can be taken down.
TRANSFERSAFTERTRAUMAOccasionally tendon transfers are required to treat se-quelae of tendon trauma.The most common procedureis the transfer of EIP to EPL to regain thumb extensionafter rupture of EPL, seen occasionally after a distalradial fracture.
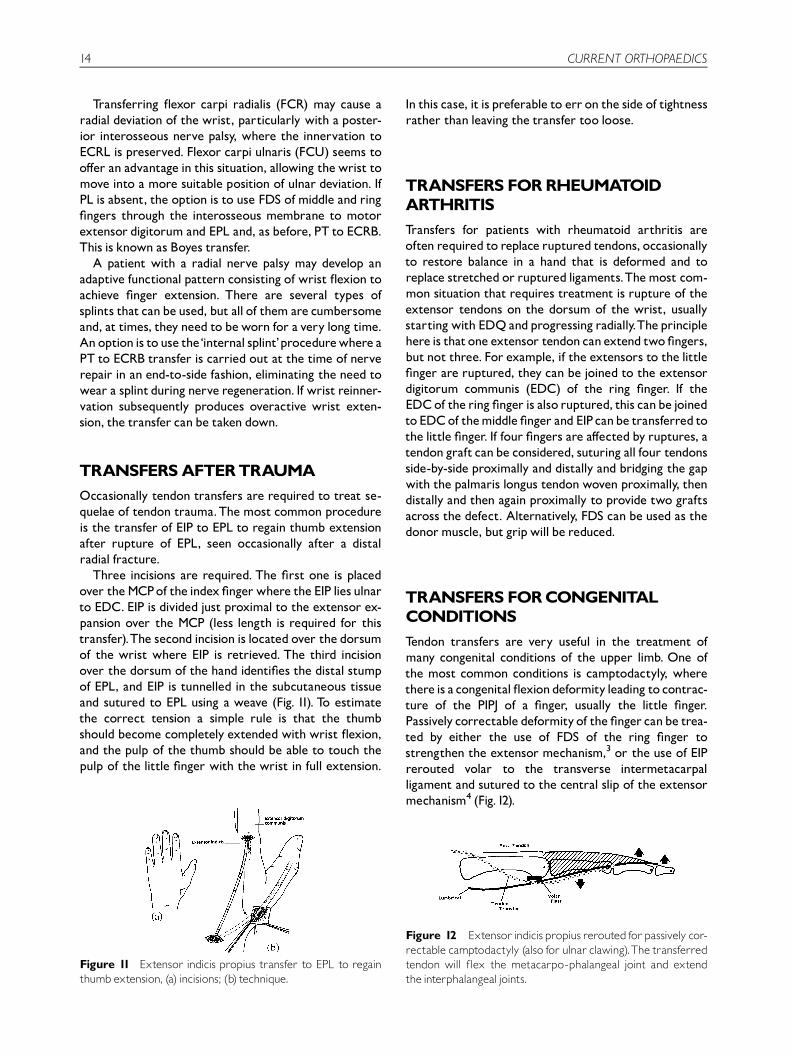
Three incisions are required. The ¢rst one is placedover theMCPof the index ¢nger where the EIP lies ulnarto EDC. EIP is divided just proximal to the extensor ex-pansion over the MCP (less length is required for thistransfer).The second incision is located over the dorsumof the wrist where EIP is retrieved. The third incisionover the dorsum of the hand identi¢es the distal stumpof EPL, and EIP is tunnelled in the subcutaneous tissueand sutured to EPL using a weave (Fig. 11). To estimatethe correct tension a simple rule is that the thumbshould become completely extended with wrist £exion,and the pulp of the thumb should be able to touch thepulp of the little ¢nger with the wrist in full extension.
Figure 11 Extensor indicis propius transfer to EPL to regainthumb extension, (a) incisions; (b) technique.
In this case, it is preferable to err on the side of tightnessrather than leaving the transfer too loose.
TRANSFERS FORRHEUMATOIDARTHRITISTransfers for patients with rheumatoid arthritis areoften required to replace ruptured tendons, occasionallyto restore balance in a hand that is deformed and toreplace stretched or ruptured ligaments.Themost com-mon situation that requires treatment is rupture of theextensor tendons on the dorsum of the wrist, usuallystarting with EDQ andprogressing radially.The principlehere is thatone extensor tendon can extend two ¢ngers,but not three. For example, if the extensors to the little¢nger are ruptured, they can be joined to the extensordigitorum communis (EDC) of the ring ¢nger. If theEDCof the ring ¢nger is also ruptured, this canbe joinedto EDCof themiddle ¢nger and EIPcanbe transferred tothe little ¢nger. If four ¢ngers are a¡ected by ruptures, atendon graft canbe considered, suturing all four tendonsside-by-side proximally and distally and bridging the gapwith the palmaris longus tendon woven proximally, thendistally and then again proximally to provide two graftsacross the defect. Alternatively, FDS can be used as thedonormuscle, but gripwill be reduced.
TRANSFERS FORCONGENITALCONDITIONSTendon transfers are very useful in the treatment ofmany congenital conditions of the upper limb. One ofthe most common conditions is camptodactyly, wherethere is a congenital £exiondeformity leading to contrac-ture of the PIPJ of a ¢nger, usually the little ¢nger.Passively correctable deformityof the ¢nger canbe trea-ted by either the use of FDS of the ring ¢nger tostrengthen the extensor mechanism,3 or the use of EIPrerouted volar to the transverse intermetacarpalligament and sutured to the central slip of the extensormechanism4 (Fig.12).
Figure 12 Extensor indicis propiusrerouted forpassively cor-rectable camptodactyly (also for ulnar clawing).The transferredtendon will £ex the metacarpo-phalangeal joint and extendthe interphalangeal joints.

PRINCIPLESOF TENDONTRANSFER INTHEHANDANDFOREARM 15
TRANSFERS FORCEREBRALPALSYCerebral palsy is a permanent, non-progressive abnorm-ality ofmuscle function causedby injury to the immaturebrain. Before o¡ering surgery to a patient with cerebralpalsy, themusculoskeletal, sensory, functional, psycholo-gical, and social aspectsmust be considered.The patternof deformity is variable, but the most common one isshoulder adduction and internal rotation, elbow £exion,forearm pronation, wrist £exion, ¢nger extension andthumb £exion and adduction.
Successful tendon transfer in cases with varying tonein spasticity of the muscles is very di⁄cult to achieve.With these patients, it is better to err on the side of cau-tion, since over-doing the treatment andcreating the op-posite deformity is worse than the initial problem.However, at present, surgery is probably underused inthis group of patients, and considerable improvementcan be obtained.The best candidates for surgery are co-operative children with spastic condition (rather thanathetoid) with predominantly upper limb involvement,good hand sensibility, without general neurologicalde¢cit and with good family support. A review of themanagement of the upper limb in cerebral palsy hasbeen published in this journal.5
TRANSFERS FORTETRAPLEGIAPatients with tetraplegia are usually young adults, whowere previously very active, and no longer have the useof their legs, minimal hand function, and have no boweland bladder control. Improving the function of theirhands can revolutionise their lives. In a survey of patientswith tetraplegia,6 76% expressed the view that theirpriority would be to have restored hand function, overlower limb function (8%), normal bowel and bladder(14%), and normal use of sexual organs (3%).
The de¢cit is di¡erent in every patient and must becarefully assessed, including assessment of power andsensation. The de¢cit does not necessarily correspondto the skeletal injury level of the cervical spine.The goalsof treatment depend to a large extent on the level of dis-ability.With high lesions the priority is to regain elbowextension, so that the patient is able to transfer from awheelchair, to propel the wheelchair and to reach out.The next priority is grasp.When there are few musclesworking in the forearm, it is best to try to achieve keypinch and claw grip.Wrist arthrodesis and multiple MPand IP arthrodesis are best avoided. Reconstruction hasa better chance of success in hands that have activewristextension, or when active extension can be achieved.Hands with poor sensibility are very limited in theirpotential for recovery of useful function.
A review of the management of the upper limb intetraplegia has been published in this journal.7
OTHERINDICATIONSTendon transfers can also be applied to a variety of othersituations, including combined nerve injuries, brachialplexus palsy involving the shoulder and elbow or thehand and forearm, or after polio and leprosy. Each pa-tientwill have his or her ownuniquemotor de¢cit whichmustbe assessed and treated following theprinciplesde-scribed at the beginning of this paper. Patients withmus-cular dystrophy and other progressive neuromusculardiseases are only considered for tendon transfer if therate of progression is su⁄ciently slow, so that the trans-fer is likely to be of bene¢t formore than 2 or 3 years.
POST-OPERATIVECAREPost-operative care is crucial to the outcome of tendontransfers and close co-operationwith thehand therapistis essential. Immobilisation is usually indicated for amini-mum of 3 weeks after tendon transfers and tenodesis.Oedema will translate into sti¡ness. Oedema can beminimised by careful surgical technique, meticuloushaemostasis, appropriate dressings and splinting, andelevation of the limb, particularly during the ¢rst 48hafter surgery. If oedema develops, it can be treated withelevation, exercises (if appropriate), coban bandages oran air-pressure glove. If the joints are sti¡ post-operatively, they must be mobilised but joint manipula-tion must be avoided. The period of immobilisation willdepend, to an extent, on the robustness of repair. Astout Pulvertaft weave permits early mobilisation withless risk of adhesions.
The patient will need to train the tendon transfer towork in the new position. If the objective is to returnthe limb to functional activities, the best therapy is topractise those tasks, or very similar ones. The patientneeds to be encouraged to use the hand. Occasionallyelectrical stimulation can be of help, since simultaneousmuscle contraction and joint motion can provide thefeedback necessary to induce the transferredmuscle tocontract at the appropriate time.The best therapy is touse the hand for normal and useful activities as soon aspossible after the wounds are healed and the tendonjunctures are secure.
REFERENCES
1. Gelberman R H. Operative Nerve Repair and Reconstruction.
Philadelphia: Lippincott, 1991; 1587.
2. Brand P W, Hollister A. Clinical Mechanics of the Hand. St Louis:
Mosby, 1993; 386.
3. McFarlane RM, Curry GI, Evans H B. Anomalies of the intrinsic
muscles in camptodactyly. J Hand Surg 1983; 8: 531–544.
4. Gupta A, Burke F D. Correction of camptodactyly. J Hand Surg
1980; 15B: 168–170.
5. Tonkin M A. The upper limb in cerebral palsy. Curr Orthop 1995;
9: 149–155.

16 CURRENT ORTHOPAEDICS
6. Hamlin C. Upper extremity reconstruction in the tetraplegic
patient. Techn Hand Upper Extrem Surg 2001; 5: 91–104.
7. Gschwind C R Surgical management of the upper limb in
tetraplegia. Curr Orthop 1999; 13: 1–8
FURTHERREADINGSmith RJ. Tendon Transfers of the Hand and Forearm.Boston: Little, Brown&Co.,1987; 337.
![Design of a Hand Tendon Injury Rehabilitation System using ...based tendon-driven wearable robotic hand [22] Characterisation and evaluation of soft elastomeric acuators for hand assistive](https://img.pdfslide.net/doc/110x75/60b7d0894b1269644e0a4ff0/design-of-a-hand-tendon-injury-rehabilitation-system-using-based-tendon-driven.jpg)