Embed Size (px)
Citation preview

Proactively Identifying Risk and Medication Errors in Home Infusion: How to Ensure Consistent Learnings When Events OccurMatthew Grissinger, RPh, FISMP, FASCP
Director, Error Reporting Programs, Institute for Safe Medication Practices
Horsham, PA
Laura J. Haynes, PharmD, BCPS, CPHQ, ASQ CSSGB
Manager of Quality and Patient Safety at Penn Medicine at Home – Penn Home Infusion Therapy
King of Prussia, PA

Financial Disclosure
1. Disclosure of Relevant Financial Relationships
I have the following financial relationships to disclose:
Matt Grissinger - Wife is an employee of Johnson & Johnson
Laura Haynes – Husband is an employee of Anthem
2. Disclosure of Off-Label and/or Investigative UsesMatt Grissinger and Laura Haynes - We will not discuss off label use and/or investigational use in
my presentation
2

Learning Objectives
• Explain the concept of system-based causes of medication errors
• Identify examples of latent failures in each phase of the medication use process in the home care setting.
• Describe system enhancements to prevent and detect errors before they reach the patient.
• Review methods to both identify and reports areas of risk associated with home infusion pharmacy.
• Describe the human potential for error and historical prospective of quality/safety within healthcare
• Understand 2 major tools (5 whys and fishbone diagram) needed to identify a root cause for event occurrence
• Identify the root causes from event review examples by using the 2 above tools.
3

Multifactorial nature of errors
• Many factors, latent and active, must be present and in proper alignment for error to occur
• Error investigations always concentrate on sharp (active) end (front line staff) where patient/caregiver interaction occurs
• Contributing factors and blunt end (latent) errors often originate where organizational policies, procedures and resource allocation decisions are made

Formulary,
purchasing
decisions
Inventory
management
Deliver
medications &
Supplies
Medication Use SystemReferral:
Medication-
related History
and Orders
Document
Medication
History
Diagnostic/
Therapeutic
Decisions Made
Medication
Ordered
Receive
Referral;
Evaluate order
Order Entry
Educate patient
regarding
medication
Order verified
and submitted
Prepare
Medication &
Supplies
Educate staff
regarding
medications
History-Taking
Ordering
Pharmacy Management
Education
Select the
correct drug &
supply
Administer
according to
order and
standards for
drug
Document
administration
and associated
information
Assess and
document
patient response
to medication
Intervene as
indicated for
adverse
reaction/error
Administer MedicationMonitor/Evaluate Response Document
Medication Inventory Management
Administration Management
Incident/adverse
event surveillance
and reporting
Surveillance
38%

Key Elements of Medication Use
Patient Information
Drug Information
Communication
Labeling, Packaging &
Nomenclature
Patient Education
Device Acquisition, Use &
Monitoring
Environmental Factors
Staff Competency & Education
Drug Storage, Stock, &
Distribution
Quality & Risk Management

Patient Information
• Lack of critical patient information
• Laboratory values,
• Height,
• Weight,
• Diagnoses,
• Allergies,
• Other drug therapy, etc.
• Patient misidentification
Processes Associated with Patient Information
• Essential patient information is obtained• Is it communicated?
• Readily available in useful form• Where is it documented?
• Considered when prescribing, dispensing, and administering medications
• Lack of drug information systems that merge with patient information

Patient Information• New Referral Intake
• What are you asking for?
• Who does intake?
• Can a patient be admitted without critical information?
• Paper vs Electronic Health Record
9

Communication of Drug Information• Orders
• Handwritten prescriptions
• Verbal/telephone orders
• Ambiguous orders
• Hold orders
• Transmission of Orders
• Fax-related problems
• Electronic prescribing
• Intimidation/Disruptive Behavior
Home Infusion Order Entry Systems
• No clinical decision support (CDS)
• Co-morbidities?
• Allergies and Reactions
• Communication of new reaction/anaphylaxis
• You dispense epi-pens, are they used?
11

Home Infusion Order Entry Systems
• Weights, but is it lbs. or kgs?
• Free texting of drug names
• Pharmacy AND nursing documentation,
• Pharmacy looks at nursing notes?
• Nursing looks at pharmacy notes?
• Supply lists
12

Order Entry• Pharmacist #1 enters order. Who checks that?
• Patient
• Order
• Allergies
• Comorbidities
• Weight-based dosing?
• Supplies (and who fixes them?)
13

Chemotherapy• New orders for each cycle or do you just refill based on the
original order?
• How do you know if there is a change in the order?
• What course is the patient on?
• Preparing drugs ahead of time without confirming labs (and drug gets delivered)
14

Compounding Environment
• Overall workflow• Does delivery take precedence over safety
• Environment for compounding• Are you 797 or 800 compliant?
• Space to prepare
• Counter space to check
• Doors going in/out of clean room
• Where is final product stored?
15

Pharmacy Preparation• Labels of bottles on compounder facing forward?
• Double check of restocking vials on compounder
• Barcode verification on compounder vs patient• Open vials cluttering the hood
• “just in case”
• When are labels applied?
• What is included in the final check? • Focus on looking for particulate matter, but is it the right patient?
16


Checking of Final Product
• Pullback method = proxy method • ISMP TMSBP
• How many vials? All or just one? With a pulled back syringe
• Vials, syringes, order, label, final product segregated from others
• Eric Cropp
• IDC when on-call or not on-call
18

ISMP Targeted Best Practices • ……perform an independent verification to ensure that the
proper ingredients are added, including confirmation of the proper volume of each ingredient prior to its addition to the final container.
• Specifically, eliminate the use of proxy methods of verification for compounded sterile preparations of medications
• e.g., the “syringe pull-back method,”
19https://www.ismp.org/sites/default/files/attachments/2019-01/TMSBP-for-Hospitalsv2.pdf
Staff Competency and Education
• Knowledge and skills related to safe medication practices
• Inadequate orientation• Workload for trainers
• Individualized time for orientation
• Inadequate baseline competency evaluation
• Specialties• Oncology

Staff Education and Competency
• What does training include?• Are pharmacists only doing order entry but expected to check
OR prepare when on-call?
• What is competency?
• Ongoing education• News/ISMP updates/changes to your practice
• Internal newsletter
21

Quality Process and Risk Management• How are you identifying risk/unsafe processes?
• Hazardous condition/error reporting
• Ask your employees
• Measures
• Waste
• Interruptions
• Returned pumps
• # of calls
• Changes in workflow, did it work?
22

Pharmacy Huddles• Who is going out today?
• Any hold-ups?
• New admits
• Discharged patients• What should be picked up?
• Drug shortages
23

Human Potential for Error

Institute of Medicine / National Academy of Medicine
• Part I - To Err is Human
• Part 2 – Crossing the Quality Chasm
• Preventing Medication Errors with the Quality Chasm

• “Whatever humans have learned had to be learned as a consequence only of trial and error experience. Humans have learned only through mistakes.”
- R. Buckminster Fuller
26

Science of Improvement
• Based on 2 main types of knowledge
• Subject Matter Knowledge
• Profound Knowledge
27http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx

Profound Knowledge
Appreciation of a System
Psychology
Understanding Variation
Theory of Knowledge
28http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx

Pioneers in Quality and Safety Methodologies
29
• W. Edwards Deming
• Daniel Kahneman
• George Box
• Joseph M. Juran
http://www.ihi.org/resources/Pages/HowtoImprove/default.aspxW.E. Deming, The New Economics, 1994, Chapter 4

“We are making progress against medical errors but much more effort is needed… No one should ever expect perfection, zero errors, or ‘six sigma’. What we should expect, and what I believe is attainable, are zero patient injuries.”
- Michael Cohen
30

A Tool for Event Review – 5 Whys
31

5 Whys
• What is it?
• When do you do it?
• Who does it?
• Why do you do it?
• How is it done?
32http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx

5 Why Example
• Problem Statement: You are on your way home from work and your car stops in the middle of the road.
• 1. Why did your car stop?
Because it ran out of gas.
• 2. Why did you run out of gas?Because you didn’t buy any gas on my way to work.
• 3. Why didn’t you buy any gas this morning?Because you didn’t have any money.
• 4. Why didn’t you have any money?Because you lost it all last night in a poker game.
• 5. Why did you lose your money in last night’s poker game?Because you’re not very good at “bluffing” when I don’t have a good hand.
33

34
A Tool for Event Review – Fishbone
Diagramming

Fishbone Diagrams
• AKA - Cause and Effect or Ishikawa diagrams
What is it?
When do you do it?
Who does it?
Why do you do it?
How is it done?
35http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx

Fishbone Example
36

37
Case Review

Case #1
• Patient called into triage noting that their 46 hour chemo regimen had stopped after 4 hours of infusion that was hooked up by field home infusion RN.
38

5 Whys
39

Fishbone
40

Case #2
• RPH working on refills for TPN patients and notices that 10 mL of multi-trace elements (MTE) was added to TPN versus 1 mL standard.
41

5 Whys
42
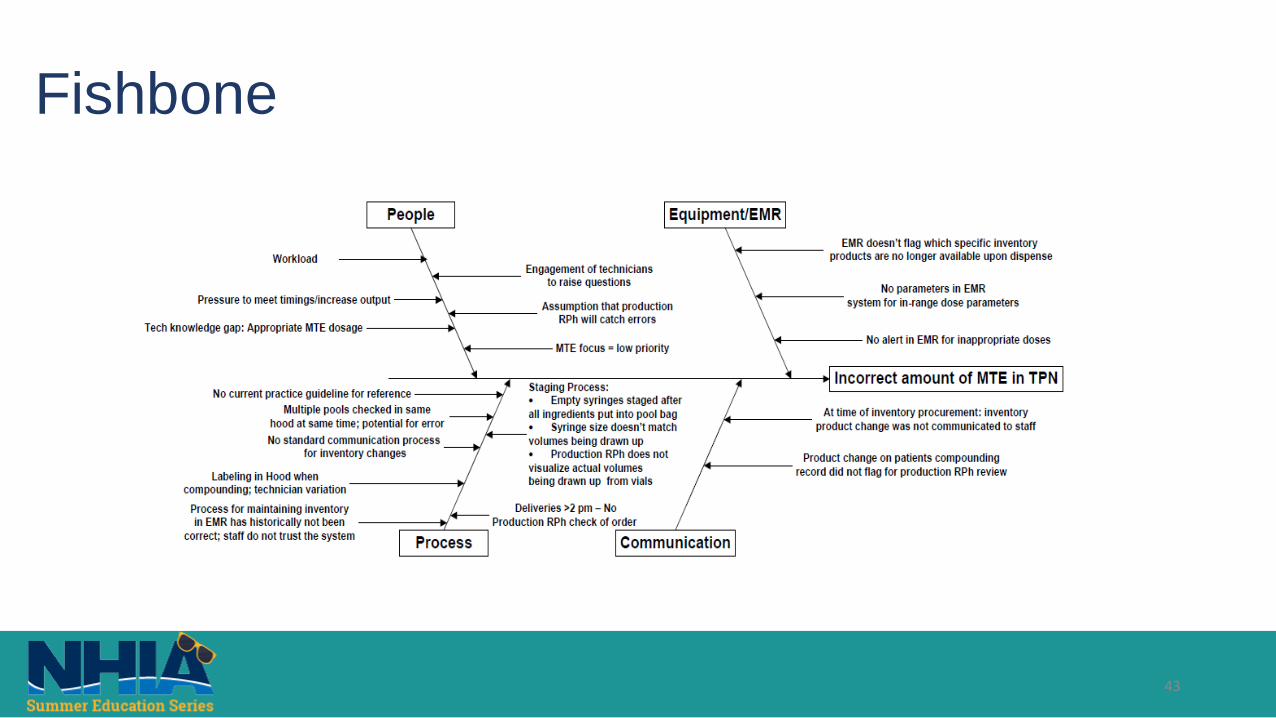
Fishbone
43

Conclusions
• Humans and their infallibly is a component of healthcare
• Ensuring that everyone learns from events that occur in your organization provides the foundation for improvement
• 5 Whys and Fishbone diagrams are tools for understanding how you can improve your current processes based on events that happen
44

• “We must accept human error as inevitable – and design around that fact.”
- Donald Berwick
45