Embed Size (px)
Citation preview
Co
CLINICAL GUIDELINE
Probiotics for the Prevention of Antibiotic-Associated
Diarrhea in Children�Hania Szajewska, yzRoberto Berni Canani, yAlfredo Guarino, §Iva Hojsak, jjFlavia Indrio,
§Sanja Kolacek, �Rok Orel, #Raanan Shamir, ��Yvan Vandenplas, yyJohannes B. van Goudoever,
pyright 2016 by
and zzZvi W alf of the ESPGHAN Working Group for Probiotics/Prebiotics
available. The quality of e
Recommendations Assess
Received December 7, 20From the �Medical Univ
Laboratory for The I§Department of PaedUniversity Hospital PUniversity Medical CeIsrael, Sackler FacultBrussels, Belgium, thethe zzPediatric Gastro
Address correspondence aWigury 63A, Poland
Supplemental digital conttext of this article on
H.S. has received researchhas participated as aInstitute, Nutricia, Memember for Fundacjainvestigator, and/or spsupported by Biocoderelated to any of the prnot related to the conteclinical investigator, ctopics within the probifee provided to the insrelated clinical studiesAbbott, Danone, NestlMerck/MSD, HospiraBioGaia (ongoing; invAbbvie, and MSD. RInternational, Danoneadvisory board for ASprobiotic related, somNutricia, Mead JohnsoYakult (grants, study,and founder and direclectures by Danone, Nformula. Z.W. has par
Copyright # 2016 byGastroenterology, He
DOI: 10.1097/MPG.0000
JPGN � Volume 62, N
eizman, on Beh
combinations of strains have been tested, but sufficient evidence is still
lacking.
ABSTRACT
This article provides recommendations, developed by the Working
Group (WG) on Probiotics of the European Society for Pediatric Gastro-
enterology, Hepatology, and Nutrition, for the use of probiotics for the
prevention of antibiotic-associated diarrhea (AAD) in children based on a
systematic review of previously completed systematic reviews and of
randomized controlled trials published subsequently to these reviews.
The use of probiotics for the treatment of AAD is not covered.
The recommendations were formulated only if at least 2 randomized
controlled trials that used a given probiotic (with strain specification) were
ESPGHAN and NASPGHAN. Un
vidence (QoE) was assessed using the Grading of
ment, Development, and Evaluation guidelines. If
15; accepted December 10, 2015.ersity of Warsaw, Department of Paediatrics, Warsaw,nvestigation of Food Induced Diseases and CEINGEiatrics, Children’s Hospital Zagreb, University of Zagoliclinico, University of Bari, Bari, Italy, the �Departntre, Ljubljana, Slovenia, the #Institute of Gastroentero
y of Medicine, Tel-Aviv University, Tel-Aviv, Israel,yyDepartment of Pediatrics, Emma Children’s Hospitaenterology and Nutrition Unit, Soroka Medical Centend reprint requests to Hania Szajewska, MD, Departme
(e-mail: [email protected]).ent is available for this article. Direct URL citations appthe journal’s Web site (www.jpgn.org).support (study products only) from Biogaia and Dicofa
speaker on probiotics/microbiota-related subjects for Aad Johnson, Merck, Sequoia, and Yakult; has been a mem
Nutricia (Nutricia Foundation), funding research graeaker for Dicofarm, Heinz, Mead Johnson Nutrition, Mx, Dicofarm, and Mead Johnson Nutrition. Others (sucoducts mentioned in the article and companies using/or snt of the article: Astellas Pharma. I.H. has participated aonsultant, and speaker for Arla Food, Biogaia, Noos, Notic-related fields (never for probiotic product) from Biotitution in the studies related to probiotic product of Dukreceived from Chr. Hansen and Biogaia. Other activitiee, Nutricia and MSD, and nonrestricted educational granand Pharmas. R.O. has participated as a clinical inve
estigator’s initiated study); has participated as a speaker.S. has a clinical investigator, and/or advisory board, Enzymotec, Nestle, Nestle Nutrition Institute, and NuPEN, Ausnutria, Biocodex, Danone Belgium, and Unitetimes not) for Abbott Nutrition, ARLA foods, ASPENn, Merck, Menarini, Orafti, Pfizer, Phacobel, Sari Husa
and advisory fees always paid to the institution). J.B.G.tor of the Dutch Human Milk Bank; his institute receutricia, Nestle Nutrition Institute; he is consultant for Nuticipated as a clinical investigator, speaker, and consuEuropean Society for Pediatric Gastroenterology,patology, and Nutrition000000001081
umber 3, March 2016
the use of probiotics for preventing AAD is considered because of the
existence of risk factors such as class of antibiotic(s), duration of antibiotic
treatment, age, need for hospitalization, comorbidities, or previous episodes
of AAD diarrhea, the WG recommends using Lactobacillus rhamnosus GG
(moderate QoE, strong recommendation) or Saccharomyces boulardii (mod-
erate QoE, strong recommendation). If the use of probiotics for preventing
Clostridium difficile-associated diarrhea is considered, the WG suggests
using S boulardii (low QoE, conditional recommendation). Other strains or
authorized reproduction of this article is prohibited.
Poland, the yDepartment of Translational Medical Science, the zEuropeanAdvanced Biotechnology, University of Naples ‘‘Federico II,’’ Italy, thereb School of Medicine, Zagreb, Croatia, the jjDepartment of Pediatrics,ment of Gastroenterology, Hepatology and Nutrition, Children’s Hospital,logy, Nutrition and Liver Diseases, Schneider Children’s Medical Center ofthe ��Department of Pediatrics, UZ Brussel, Vrije Universiteit Brussel,
l-AMC and VU Universit Medical Center, Amsterdam, The Netherlands, andr. Ben-Gurion University, Beer-Sheva, Israel.nt of Paediatrics, Medical University of Warsaw, 02–091 Warsaw, Zwirki i
ear in the printed text, and links to the digital files are provided in the HTML
rm; has been a clinical investigator for Arla Foods (ongoing), Danone, Nestle;rla, Biogaia, Biocodex, Danone, Dicofarm, Hipp, Nestle, Nestle Nutritionber of Nestle Nutrition Institute faculty; and has served as an advisory board
nts in the field of human nutrition. R.B.C. has participated as a clinicalenarini, Nutricia, and Wyeth (none related to the work submitted). A.G. wash as personal fees for advisory boards, consultancy; personal speakers feeelling them, as well as competitors)—none declared. Other industry relationss a clinical investigator for Biogaia and Chr Hansen. F.I. has participated as aestle, and Nestle Nutrition Institute. S.K. received personal speaker fee for
gaia, Medis, and Arla Foods. Clinical investigator without any personal fee orat. Scientific grants delivered entirely and only to the Institution for probiotic-s nonrelated to probiotics were as follows: personal speaker fee received fromts delivered to the Institution from Nestle, Nutricia, Podravka, AbbVie, Falk,
stigator for United Pharmaceuticals (probiotics were not involved) and forfor Medis, Nutricia, Ewopharma, Biogaia, United Pharmaceuticals, Danone,member, and/or consultant, and/or speaker for Abbott, Danone Institutetricia; none related to the work submitted. Y.V. is consultant or member ofed Pharmaceuticals; has been a clinical investigator and speaker (sometimes, Biogaia, Biocodex, Danone, Dumex, Hero, Hipp, Nestle Nutrition Institute,da, Shire (Movetis), Sucampo, Takeda, United Pharmaceuticals, Wyeth andis member of the Dutch National Health Council, the Breastfeeding Councilived research grants from Danone and MJN; he received compensation fortricia Nederland and holds 3 patents on the amino acid composition of infantltant for Biocodex and Biogaia.Hepatology, and Nutrition and North American Society for Pediatric
495

Co
Key Words: Clostridium difficile, dysbiosis, guideline, infants, microbiota,
probiotics, RCT, systematic review
(JPGN 2016;62: 495–506)
Szajewska et al
A ntibiotic-associated diarrhea (AAD) is a common and chal-lenging complication observed in the ambulatory and hospi-
tal settings alike that occurs in up to a third of all patients treatedwith antibiotics (1). It is defined as diarrhea that occurs in relation toantibiotic treatment with the exclusion of other etiologies. Thisrelation does not necessarily translate into an immediate adversereaction to antibiotics, because AAD may occur after a few weeksand even up to a few months after the administration of theantibiotics (2). Thus, in the latter situation, caution is needed todifferentiate AAD from an episode of infectious gastroenteritis. Therisk of AAD is higher when there is a use of aminopenicillinswithout/with clavulanate, cephalosporins, clindamycin, and, ingeneral, any antibiotic that is active against anaerobes (3). Almostany oral and intravenous antibiotic treatment can, however, causeAAD (3). Clinically, AAD may present as mild diarrhea, but itcan present as well as fulminant pseudomembranous colitis.Usually, no pathogen is identified. In the most severe forms andin an increasing number of patients with chronic conditions such asthose with inflammatory bowel diseases, cystic fibrosis, and cancer,however, the causative agent is often identified as Clostridiumdifficile (4).
The use of probiotics, defined as ‘‘live microorganisms that,when administered in adequate amounts, confer a health benefit onthe host,’’ (5) and/or fermented products such as yogurt has beenreported as a measure to prevent the occurrence of AAD. Therationale for the use of these products relies on the hypothesis thatAAD is caused by dysbiosis that is triggered by antibiotic use andthat the probiotic intervention favorably modulates the intestinalmicrobiota (1).
The aim of this position paper by the European Society forPediatric Gastroenterology, Hepatology, and Nutrition (ESP-GHAN) Working Group (WG) on Probiotics and Prebiotics is toprovide recommendations for the use of probiotics for preventingAAD in children.
METHODSThe same methodology that had been used previously by the
WG for developing guidelines on the use of probiotics for themanagement of acute gastroenteritis (6) was applied for developingthe present position paper. In brief, the document provides a reviewof previously completed systematic reviews and of randomizedcontrolled trials (RCTs) published subsequently to these reviews.For systematic reviews/meta-analyses, the Cochrane Database ofSystematic Reviews and the Database of Abstracts of Reviews ofEffects (DARE) were searched. For subsequently published trials(starting from the date of the most recent search in the includedreviews), CENTRAL (Cochrane Central Register of ControlledTrials), MEDLINE, and EMBASE were searched up to July2015 and again in November 2015.
The focus was on 6 taxonomic groups (Lactobacillus,Bifidobacterium, Saccharomyces, Streptococcus, Enterococcus,and/or Bacillus). The list of individual probiotics to be consideredwas established based on the results of the Cochrane reviewevaluating probiotics for preventing AAD in children (7) and thelist of commonly used probiotics developed by the World Gastro-enterology Organization (8).
The WG is aware that taxonomically equivalent probiotic
pyright 2016 by ESPGHAN and NASPGHAN. Un
microorganisms may be supplied by different manufacturers.At least 1 study indicated that the manufacturing process may
496
influence properties of probiotic bacteria (9). At present, whetheror not these manufacturing differences translate into differences invivo, as well as clinical outcomes, however, remains unclear.Consequently, the taxonomically equivalent probiotics are pre-sented jointly, regardless of the manufacturer. The WG alsorealizes that the same brand may have a different compositionin different locations; nevertheless, this position paper deals withstrain(s) rather than brands or commercial names. Finally, depend-ing on the country, the same probiotic microorganism(s) may beavailable as food supplements, available as registered pharmaceu-tical products, and/or incorporated into foods (10). In this docu-ment, the effectiveness of probiotics was analyzed regardless of theregistration status. Health care professionals and consumersshould, however, be aware of possible variations in the manufac-turing and safety profiles of the products, which may be differentwhen the strain is registered as a drug and also with regard to theclaims allowed.
The primary outcome measures were diarrhea/AAD andC difficile-associated diarrhea (all as defined by the investigators).
To assess the methodological quality of the included RCTs(included in the previously published meta-analyses and sub-sequently published RCTs not included in the systematic reviews),the Cochrane Collaboration’s tool for assessing risk of bias wasused. This tool includes the following criteria: adequacy ofsequence generation, allocation concealment, and blinding ofparticipants, personnel and outcome assessors; incomplete outcomedata; and selective reporting (11).
For reporting the effect, the results for individual studiesand pooled statistics are reported as the risk ratio (RR) betweenthe experimental and control groups with 95% confidence intervals(95% CIs). In other circumstances, we report the findings asreported by the authors of the included studies.
When synthesizing the evidence, each section presentsa summary of the evidence followed by the key recommen-dations. The GRADE system, developed by the Grading ofRecommendations Assessment, Development and EvaluationsWorking Group (12), was used to grade the strength of evidenceand grades of recommendations used in these guidelines. In brief,the GRADE system offers 4 categories of the quality of theevidence (ie, high, moderate, low, and very low) and 2 categoriesof the strength of recommendation (ie, strong or conditional[weak]) (Table 1). The GRADE system suggests presentingrecommendations in the active voice (13). Thus, we used thewording ‘‘the WG recommends’’ for strong recommendations,and ‘‘the WG suggests’’ for conditional [weak] recommen-dations.
As in our previous document (6), the WG adopted theposition of the US Food and Drug Administration Guidance forIndustry (14) that at least 2 adequate and well-controlled studies,each convincing on its own, are needed to establish the effec-tiveness of an intervention. Consequently, the recommendationswere formulated only if at least 2 RCTs that used a given probioticwere available. If there was only 1 RCT, regardless of whether ornot it showed a benefit, no recommendation was formulated.Moreover, if the strain specification was not given and/or theprobiotic product was not otherwise identifiable, no recommen-dation was made.
For the sake of completeness, we report the pooled data(meta-analysis) of all probiotic trials. No recommendation onthe use of probiotics in general was, however, made, becausepooling data on different probiotics has been repeatedly ques-tioned (15). Instead, because various probiotic strains differ intheir effects, preference was given to reporting evidence and
JPGN � Volume 62, Number 3, March 2016
authorized reproduction of this article is prohibited.
recommendations related to a specific probiotic strain or theircombinations separately.
www.jpgn.org

Co
of C difficile-associated diarrhea (4 RCTs, n¼ 938, RR 0.34, 95%
QUALITY OF EVIDENCE: Moderate.
TABLE 1. The grades of the quality of evidence and strength of recommendation set by the GRADE Working Group
Quality of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate quality We are moderately confident in the effect estimate: the true effect is likely to be close to the
estimate of the effect, but there is a possibility that it is substantially different.
Low quality Confidence in the effect estimate is limited: the true effect may be substantially different from
the estimate of the effect.
Very low quality Very little confidence in the effect estimate: the true effect is likely to be substantially different
from the estimate of the effect.
Strength of recommendation Strong When the evidence showed that the benefit of the intervention clearly outweighs the
undesirable effects.
Conditional (weak) When the trade-offs were less certain (either because of the low quality of evidence or because
the evidence suggests that desirable and undesirable effects are closely balanced).
GRADE¼Grading of Recommendations Assessment, Development and Evaluations.
JPGN � Volume 62, Number 3, March 2016 Probiotics for the Prevention of AAD
A draft of the position paper was sent to the WG members forreview and further comments. All of the critical feedback wasdiscussed through e-mail or during personal contacts, and changeswere incorporated as necessary. Recommendations were formulatedand graded. The WG members voted anonymously on each recom-mendation using an online electronic survey tool (SurveyMonkeyInc, Palo Alto, CA, www.surveymonkey.com). Any disagreementfollowing voting was resolved by discussion, and for all recom-mendations, a full consensus was reached. A finalized documentwas submitted to the ESPGHAN Council for final acceptancebefore publication.
The WG recommendations may need to be modified bydifferent countries considering differences in health care systems,local values and preferences, including availability, quality, andcosts of probiotics, and should help local policy makers to decidewhether to use routinely probiotics with documented efficacy forpreventing AAD in children receiving antibiotics based on localcost-effectiveness analysis. This is particularly important in low-and middle-income countries.
Clearly, an individual patient’s risk of developing AAD or Cdifficile-associated diarrhea depends on a number of factors such asclass of antibiotic(s), duration of antibiotic treatment, age, need forhospitalization, comorbidities, and previous episodes of AAD or Cdifficile-associated diarrhea (1–3). These risk factors should beconsidered when making decisions on the use of probiotics inchildren for preventing AAD or C difficile-associated diarrhea.The WG acknowledges that the judicious use of antibiotics remainsthe best method of preventing AAD.
The conclusions of this document may require revision in thefuture as new information becomes available. It is the intention ofthe WG to revise the recommendations not later than 5 years fromnow and produce an updated document.
PROBIOTICS OVERALLA number of systematic reviews and meta-analyses have
shown that probiotics as a group are effective in preventing AAD(7,16,17).
A 2012 meta-analysis by Hempel et al (16) collecteddata from 82 RCTs that evaluated the efficacy of probiotics forpreventing AAD in subjects of all ages. Probiotics, as a group,reduced the risk of AAD (63 RCTs, n¼ 11,811 participants, RR0.58, 95% CI 0.50–0.68). Sixteen RCTs were carried out in infantsand young children and reported a reduced risk of AAD withprobiotic administration (RR 0.55, 95% CI 0.38–0.80). In themajority of trials, Lactobacillus-based interventions, alone or in
pyright 2016 by ESPGHAN and NASPGHAN. Un
combination with other genera, were used. Strains were poorlydocumented. The quality of evidence was low. Of 63 included
www.jpgn.org
trials, 59 lacked adequate information to assess the overall risk ofbias. There was no placebo group in some trials. Included trialsused different definitions of diarrhea/AAD, and in some, nodefinition of these outcomes was provided. Moreover, significantheterogeneity between trials for both primary and secondary out-comes was detected. The authors concluded that the evidence isinsufficient to determine whether this association varies system-atically by population, antibiotic characteristic, or probioticpreparation.
A 2013 systematic review with a meta-analysis assessedthe efficacy and safety of probiotics for preventing C difficile-associated diarrhea or C difficile infection in adults and children(17). A complete case analysis (ie, participants who completedthe study) showed that compared with placebo or no treatment,administration of probiotics reduced the risk of C difficile-associated diarrhea by 64% (23 RCTs, n¼ 4213, RR 0.36, 95%CI 0.26–0.51) in adults and children. In children, probioticadministration reduced the risk of C difficile-associated diarrheafrom 5.9% to 2.3% (3 RCTs, n¼ 605, RR 0.40, 95% CI 0.17–0.96)(17).
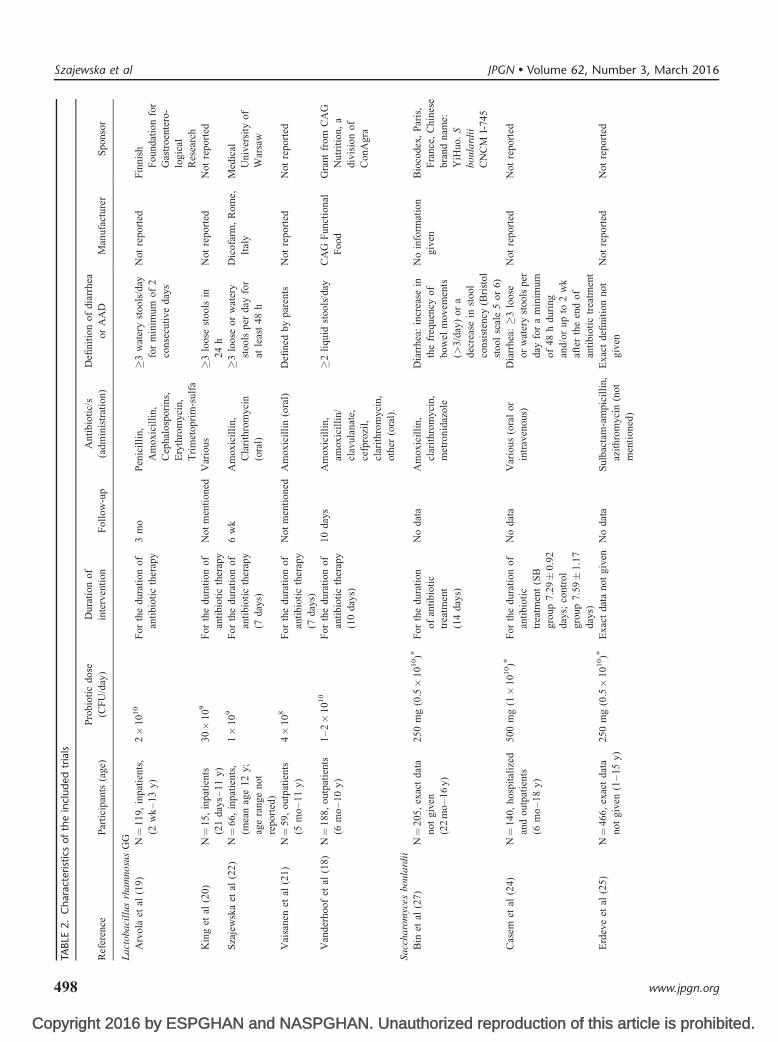
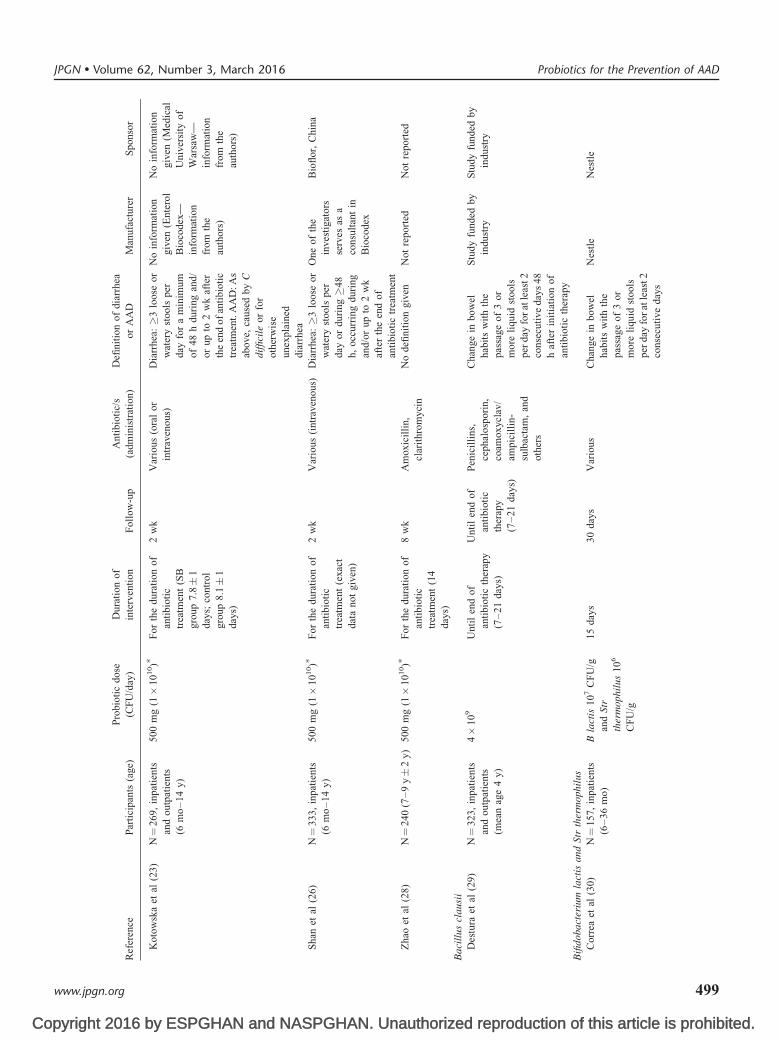
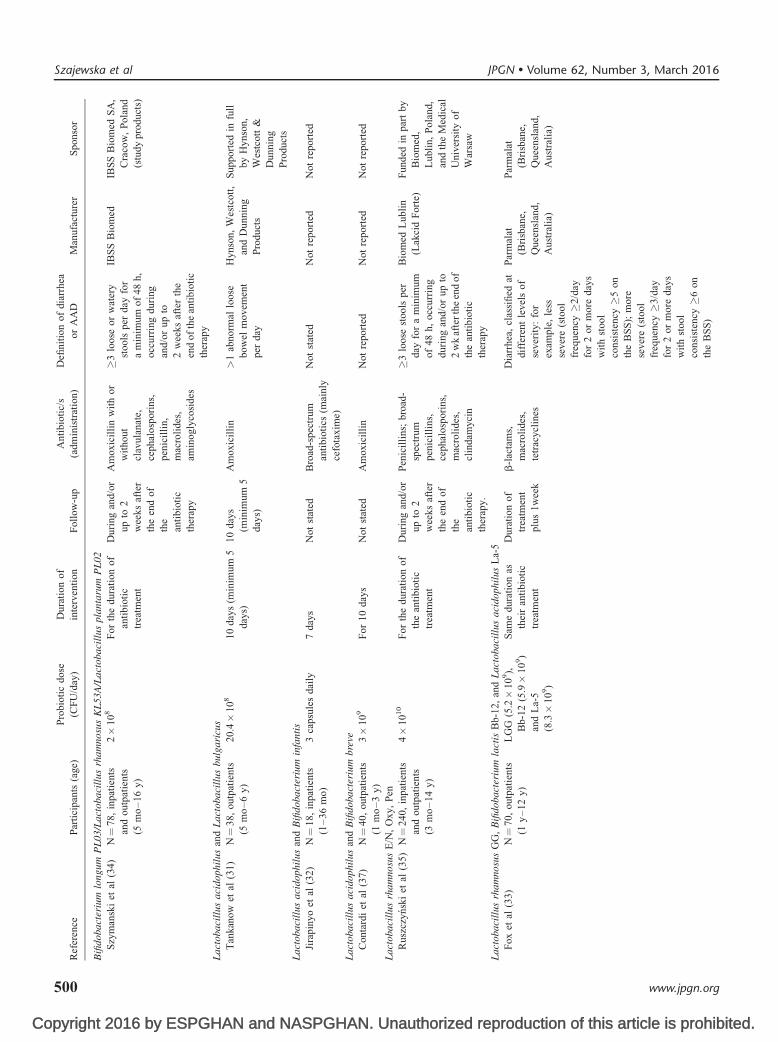
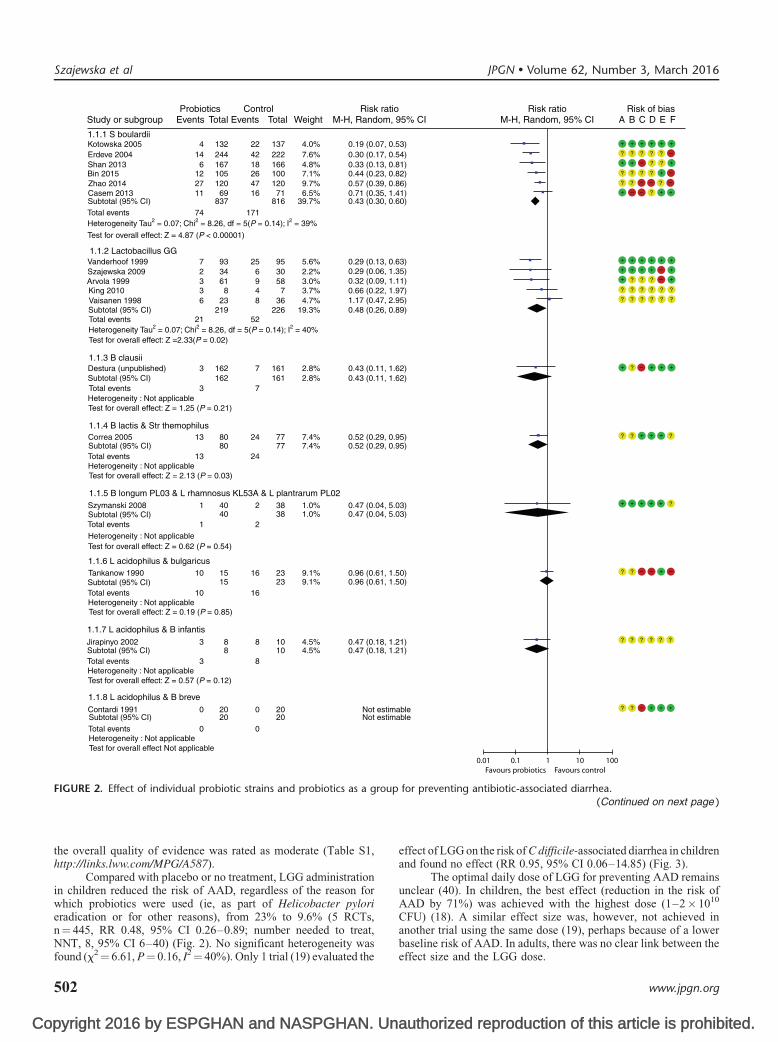
For this report, 21 RCTs involving 3255 children wereincluded (18–38). Among them, 11 RCTs were included in 2strain-specific systematic reviews initiated as part of the develop-ment of these guidelines (39,40). One unpublished study (29) wasidentified in the systematic review by Johnston et al (7). Forcharacteristics of the included RCTs, see Table 2, and for amethodological quality summary, see Figure 1. The pooled resultsof 21 RCTs showed that compared with placebo or no intervention,probiotics as a class reduced the risk of AAD by 52% (21.2% vs9.1%, respectively; RR 0.48, 95% CI 0.37–0.61) (Fig. 2). Only 2probiotics were evaluated in >1 RCT. These were Lactobacillusrhamnosus GG (LGG) and Saccharomyces boulardii. Comparedwith placebo, the administration of probiotics also reduced the risk
CI 0.15–0.76) (Fig. 3).
PROBIOTICS WITH RECOMMENDATIONS
L rhamnosus GG (LGG)
RECOMMENDATION. If the use of probiotics forpreventing AAD in children is considered, the WGrecommends using L rhamnosus GG.
authorized reproduction of this article is prohibited.
STRENGTH OF RECOMMENDATION: Strong
497
Copyright 2016 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
TABLE
2.
Ch
ara
cterist
ics
of
the
incl
ud
ed
tria
ls
Ref
eren
ceP
arti
cip
ants
(age
)
Pro
bio
tic
do
se
(CF
U/d
ay)
Du
rati
on
of
inte
rven
tio
nF
oll
ow-u
p
An
tib
ioti
c/s
(ad
min
istr
atio
n)
Defi
nit
ion
of
dia
rrhea
or
AA
DM
anuf
actu
rer
Sp
onso
r
La
cto
ba
cill
us
rha
mno
sus
GG
Arv
ola
etal
(19
)N¼
11
9,
inp
atie
nts
,
(2w
k–
13
y)
2�
10
10
Fo
rth
ed
ura
tio
no
f
anti
bio
tic
ther
apy
3m
oP
enic
illi
n,
Am
ox
icil
lin
,
Cep
halo
spo
rin
s,
Ery
thro
my
cin
,
Tri
met
op
rim
-su
lfa
�3
wat
ery
stoo
ls/d
ay
for
min
imu
mo
f2
con
secu
tiv
ed
ays
No
tre
po
rted
Fin
nis
h
Fo
un
dat
ion
for
Gas
troen
tero
-
log
ical
Res
earc
h
Kin
get
al(2
0)
N¼
15
,in
pat
ien
ts
(21
day
s–1
1y
)
30�
10
9F
or
the
du
rati
on
of
anti
bio
tic
ther
apy
Not
men
tioned
Var
ious
�3
loo
sest
ools
in
24
h
No
tre
po
rted
No
tre
port
ed
Sza
jew
ska
etal
(22
)N¼
66
,in
pat
ien
ts,
(mea
nag
e1
2y
;
age
ran
ge
no
t
repo
rted
)
1�
10
9F
or
the
du
rati
on
of
anti
bio
tic
ther
apy
(7d
ays)
6w
kA
mox
icil
lin,
Cla
rith
rom
yci
n
(ora
l)
�3
loo
seo
rw
ater
y
sto
ols
per
day
for
atle
ast
48
h
Dic
ofa
rm,
Rom
e,
Ital
y
Med
ical
Un
iver
sity
of
War
saw
Vai
san
enet
al(2
1)
N¼
59
,o
utp
atie
nts
(5m
o–
11
y)
4�
10
8F
or
the
du
rati
on
of
anti
bio
tic
ther
apy
(7d
ays)
No
tm
enti
on
edA
mox
icil
lin
(ora
l)D
efin
edb
yp
aren
tsN
ot
rep
ort
edN
ot
repo
rted
Van
der
ho
ofet
al(1
8)
N¼
18
8,
ou
tpat
ien
ts
(6m
o–
10
y)
1–
2�
10
10
Fo
rth
ed
ura
tio
no
f
anti
bio
tic
ther
apy
(10
day
s)
10
day
sA
mox
icil
lin,
amox
icil
lin/
clav
ula
nat
e,
cefp
rozi
l,
clar
ith
rom
yci
n,
oth
er(o
ral)
.
�2
liq
uid
stoo
ls/d
ayC
AG
Fu
ncti
on
al
Fo
od
Gra
nt
fro
mC
AG
Nu
trit
ion
,a
div
isio
no
f
Co
nA
gra
Sa
cch
aro
myc
esb
ou
lard
ii
Bin
etal
(27
)N¼
20
5,
exac
td
ata
no
tg
iven
(22
mo
–1
6y
)
25
0m
g(0
.5�
10
10)�
Fo
rth
ed
ura
tio
n
of
anti
bio
tic
trea
tmen
t
(14
day
s)
No
dat
aA
mox
icil
lin,
clar
ith
rom
yci
n,
met
ron
idaz
ole
Dia
rrh
ea:
incr
ease
in
the
freq
uen
cyo
f
bo
wel
mo
vem
ents
(>3
/day
)o
ra
dec
reas
ein
sto
ol
consi
sten
cy(B
rist
ol
sto
ol
scal
e5
or
6)
No
info
rmat
ion
giv
en
Bio
cod
ex,
Par
is,
Fra
nce
,C
hin
ese
bra
nd
nam
e:
YiH
uo.
S
bo
ula
rdii
CN
CM
I-74
5
Cas
emet
al(2
4)
N¼
140,
hosp
ital
ized
and
ou
tpat
ien
ts
(6m
o–
18
y)
50
0m
g(1�
10
10)�
Fo
rth
ed
ura
tio
no
f
anti
bio
tic
trea
tmen
t(S
B
gro
up
7.2
9�
0.9
2
day
s;co
ntr
ol
gro
up
7.5
9�
1.1
7
day
s)
No
dat
aV
ario
us
(ora
lor
intr
aven
ous
)
Dia
rrh
ea:�
3lo
ose
or
wat
ery
stoo
lsp
er
day
for
am
inim
um
of
48
hd
uri
ng
and
/or
up
to2
wk
afte
rth
een
do
f
anti
bio
tic
trea
tmen
t
No
tre
po
rted
No
tre
port
ed
Erd
eve
etal
(25
)N¼
46
6,
exac
td
ata
no
tg
iven
(1–
15
y)
25
0m
g(0
.5�
10
10)�
Ex
act
dat
an
ot
giv
enN
od
ata
Su
lbac
tam
-am
pic
illi
n,
azit
hro
myci
n(n
ot
men
tio
ned
)
Ex
act
defi
nit
ion
no
t
giv
en
No
tre
po
rted
No
tre
port
ed
Szajewska et al JPGN � Volume 62, Number 3, March 2016
498 www.jpgn.org
Copyright 2016 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Ref
eren
ceP
arti
cip
ants
(age
)
Pro
bio
tic
do
se
(CF
U/d
ay)
Du
rati
on
of
inte
rven
tio
nF
oll
ow-u
p
An
tib
ioti
c/s
(ad
min
istr
atio
n)
Defi
nit
ion
of
dia
rrhea
or
AA
DM
anuf
actu
rer
Sp
onso
r
Ko
tow
ska
etal
(23
)N¼
26
9,
inp
atie
nts
and
ou
tpat
ien
ts
(6m
o–
14
y)
50
0m
g(1�
10
10)�
Fo
rth
ed
ura
tio
no
f
anti
bio
tic
trea
tmen
t(S
B
gro
up
7.8�
1
day
s;co
ntr
ol
gro
up
8.1�
1
day
s)
2w
kV
ario
us
(ora
lor
intr
aven
ous
)
Dia
rrh
ea:�
3lo
ose
or
wat
ery
stoo
lsp
er
day
for
am
inim
um
of
48
hd
uri
ngan
d/
or
up
to2
wk
afte
r
the
end
of
anti
bio
tic
trea
tmen
t.A
AD
:A
s
abo
ve,
cau
sed
by
C
dif
fici
leo
rfo
r
oth
erw
ise
un
expl
ain
ed
dia
rrh
ea
No
info
rmat
ion
giv
en(E
nte
rol
Bio
cod
ex—
info
rmat
ion
from
the
auth
ors
)
No
info
rmat
ion
giv
en(M
edic
al
Un
iver
sity
of
War
saw
—
info
rmat
ion
fro
mth
e
auth
ors
)
Sh
anet
al(2
6)
N¼
33
3,
inp
atie
nts
(6m
o–
14
y)
50
0m
g(1�
10
10)�
Fo
rth
ed
ura
tio
no
f
anti
bio
tic
trea
tmen
t(e
xact
dat
an
ot
giv
en)
2w
kV
ario
us
(intr
aven
ous)
Dia
rrhea
:�
3lo
ose
or
wat
ery
stoo
lsp
er
day
or
du
rin
g�
48
h,
occ
urr
ing
du
ring
and
/or
up
to2
wk
afte
rth
een
do
f
anti
bio
tic
trea
tmen
t
On
eo
fth
e
inve
stig
ators
serv
esas
a
con
sult
ant
in
Bio
cod
ex
Bio
flo
r,C
hin
a
Zh
aoet
al(2
8)
N¼
24
0(7
–9
y�
2y
)5
00
mg
(1�
10
10)�
Fo
rth
ed
ura
tio
no
f
anti
bio
tic
trea
tmen
t(1
4
day
s)
8w
kA
mox
icil
lin,
clar
ith
rom
yci
n
No
defi
nit
ion
giv
enN
ot
rep
ort
edN
ot
repo
rted
Ba
cill
us
cla
usi
i
Des
tura
etal
(29
)N¼
32
3,
inp
atie
nts
and
ou
tpat
ien
ts
(mea
nag
e4
y)
4�
10
9U
nti
len
do
f
anti
bio
tic
ther
apy
(7–
21
day
s)
Un
til
end
of
anti
bio
tic
ther
apy
(7–
21
day
s)
Pen
icil
lin
s,
ceph
alo
spo
rin
,
coam
ox
ycl
av/
ampi
cill
in-
sulb
acta
m,
and
oth
ers
Ch
ang
ein
bo
wel
hab
its
wit
hth
e
pas
sag
eo
f3
or
mo
reli
qu
idst
oo
ls
per
day
for
atle
ast2
con
secu
tiv
ed
ays
48
haf
ter
init
iati
on
of
anti
bio
tic
ther
apy
Stu
dy
fun
ded
by
indu
stry
Stu
dy
fun
ded
by
ind
ust
ry
Bifi
dobact
eriu
mla
ctis
and
Str
ther
mophil
us
Cor
rea
etal
(30
)N¼
15
7,
inp
atie
nts
(6–
36
mo
)
Bla
ctis
10
7C
FU
/g
and
Str
ther
mophil
us
10
6
CF
U/g
15
day
s30
day
sV
ario
us
Chan
ge
inbow
el
hab
its
wit
hth
e
pas
sag
eo
f3
or
mo
reli
qu
idst
oo
ls
per
day
for
atle
ast2
con
secu
tiv
ed
ays
Nes
tle
Nes
tle
JPGN � Volume 62, Number 3, March 2016 Probiotics for the Prevention of AAD
www.jpgn.org 499
Copyright 2016 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Ref
eren
ceP
arti
cip
ants
(age
)
Pro
bio
tic
do
se
(CF
U/d
ay)
Du
rati
on
of
inte
rven
tio
nF
oll
ow-u
p
An
tib
ioti
c/s
(ad
min
istr
atio
n)
Defi
nit
ion
of
dia
rrhea
or
AA
DM
anuf
actu
rer
Sp
onso
r
Bifi
do
ba
cter
ium
lon
gu
mP
L0
3/L
act
ob
aci
llu
srh
am
no
sus
KL
53
A/L
act
ob
aci
llu
sp
lan
taru
mP
L0
2
Szy
man
ski
etal
(34
)N¼
78
,in
pat
ien
ts
and
ou
tpat
ien
ts
(5m
o–
16
y)
2�
10
8F
or
the
du
rati
on
of
anti
bio
tic
trea
tmen
t
Du
ring
and
/or
up
to2
wee
ks
afte
r
the
end
of
the
anti
bio
tic
ther
apy
Am
oxic
illi
nw
ith
or
wit
ho
ut
clav
ula
nat
e,
ceph
alo
spo
rin
s,
pen
icil
lin
,
mac
roli
des
,
amin
og
lyco
sid
es
�3
loo
seo
rw
ater
y
sto
ols
per
day
for
am
inim
um
of
48
h,
occ
urr
ing
du
ring
and
/or
up
to
2w
eeks
afte
rth
e
end
of
the
anti
bio
tic
ther
apy
IBS
SB
iom
edIB
SS
Bio
med
SA
,
Cra
cow
,P
ola
nd
(stu
dy
pro
duc
ts)
La
cto
ba
cill
us
aci
do
ph
ilu
san
dL
act
oba
cill
us
bu
lga
ricu
s
Tan
kan
ow
etal
(31
)N¼
38
,o
utp
atie
nts
(5m
o–
6y
)
20
.4�
10
81
0d
ays
(min
imu
m5
day
s)
10
day
s
(min
imu
m5
day
s)
Am
oxic
illi
n>
1ab
no
rmal
loos
e
bo
wel
mo
vem
ent
per
day
Hy
nso
n,
Wes
tcott
,
and
Du
nn
ing
Pro
duct
s
Su
ppo
rted
infu
ll
by
Hy
nso
n,
Wes
tcott
&
Du
nn
ing
Pro
duct
s
La
cto
ba
cill
us
aci
do
ph
ilu
san
dB
ifid
oba
cter
ium
infa
nti
s
Jira
pin
yo
etal
(32
)N¼
18
,in
pat
ien
ts
(1–
36
mo
)
3ca
psu
les
dai
ly7
day
sN
ot
stat
edB
road
-sp
ectr
um
anti
bio
tics
(mai
nly
cefo
tax
ime)
No
tst
ated
No
tre
po
rted
No
tre
port
ed
La
cto
ba
cill
us
aci
do
ph
ilu
san
dB
ifid
oba
cter
ium
bre
ve
Con
tard
iet
al(3
7)
N¼
40
,o
utp
atie
nts
(1m
o–
3y
)
3�
10
9F
or
10
day
sN
ot
stat
edA
mox
icil
lin
No
tre
port
edN
ot
rep
ort
edN
ot
repo
rted
La
cto
ba
cill
us
rha
mno
sus
E/N
,O
xy
,P
en
Rus
zczy
nsk
iet
al(3
5)
N¼
24
0,
inp
atie
nts
and
ou
tpat
ien
ts
(3m
o–
14
y)
4�
10
10
Fo
rth
ed
ura
tio
no
f
the
anti
bio
tic
trea
tmen
t
Du
ring
and
/or
up
to2
wee
ks
afte
r
the
end
of
the
anti
bio
tic
ther
apy.
Pen
icil
lin
s;b
road
-
spec
tru
m
pen
icil
lin
s,
ceph
alo
spo
rin
s,
mac
roli
des
,
clin
dam
yci
n
�3
loo
sest
ools
per
day
for
am
inim
um
of
48
h,
occ
urr
ing
du
rin
gan
d/o
ru
pto
2w
kaf
ter
the
end
of
the
anti
bio
tic
ther
apy
Bio
med
Lu
bli
n
(Lak
cid
Fo
rte)
Fu
nded
inp
art
by
Bio
med
,
Lu
bli
n,
Po
lan
d,
and
the
Med
ical
Un
iver
sity
of
War
saw
La
cto
ba
cill
us
rha
mno
sus
GG
,B
ifid
ob
act
eriu
mla
ctis
Bb-
12
,an
dL
act
oba
cill
us
aci
do
ph
ilu
sL
a-5
Fo
xet
al(3
3)
N¼
70
,o
utp
atie
nts
(1y
–1
2y
)
LG
G(5
.2�
10
9),
Bb
-12
(5.9�
10
9)
and
La-
5
(8.3�
10
9)
Sam
ed
ura
tio
nas
thei
ran
tib
ioti
c
trea
tmen
t
Du
rati
on
of
trea
tmen
t
plu
s1
wee
k
b-l
acta
ms,
mac
roli
des
,
tetr
acycl
ines
Dia
rrhea
,cl
assi
fied
at
dif
fere
nt
lev
els
of
sev
erit
y:
for
exam
ple
,le
ss
sev
ere
(sto
ol
freq
uen
cy�
2/d
ay
for
2o
rm
ore
day
s
wit
hst
ool
consi
sten
cy�
5o
n
the
BS
S);
mo
re
sev
ere
(sto
ol
freq
uen
cy�
3/d
ay
for
2o
rm
ore
day
s
wit
hst
ool
consi
sten
cy�
6o
n
the
BS
S)
Par
mal
at
(Bri
sban
e,
Qu
een
slan
d,
Au
stra
lia)
Par
mal
at
(Bri
sban
e,
Qu
een
slan
d,
Au
stra
lia)
Szajewska et al JPGN � Volume 62, Number 3, March 2016
500 www.jpgn.org
Copyright 2016 by ESPGHAN and NASPGHAN. Un
Ref
eren
ceP
arti
cip
ants
(age
)
Pro
bio
tic
do
se
(CF
U/d
ay)
Du
rati
on
of
inte
rven
tio
nF
oll
ow-u
p
An
tib
ioti
c/s
(ad
min
istr
atio
n)
Defi
nit
ion
of
dia
rrhea
or
AA
DM
anuf
actu
rer
Sp
onso
r
La
cto
ba
cill
us
aci
do
ph
ilu
san
dL
act
oba
cill
us
rha
mno
sus
and
La
cto
ba
cill
us
bu
lga
ricu
sa
nd
La
cto
ba
cill
us
case
ian
dStr
ther
mophil
us
and
Bifi
do
ba
cter
ium
infa
nti
san
dB
ifid
oba
cter
ium
bre
ve
Kh
od
adad
etal
(38
)N¼
66
,in
pat
ien
ts
(3–
14
y)
1�
10
9C
FU
/day
Fo
rth
ed
ura
tio
no
f
Hel
ico
ba
cter
pyl
ori
erad
icat
ion
ther
apy
(4w
k?;
no
tcl
earl
yst
ated
)
No
tst
ated
Am
oxic
illi
n,
fura
zoli
done
No
tst
ated
Pro
tex
inC
o,U
KN
ot
repo
rted
Kefi
r
Mer
enst
ein
etal
(36
)N¼
12
5,
ou
tpat
ien
ts
(1–
5y
)
At
leas
th
alf
of
a
15
0m
Ld
rin
k
con
tain
ing
7to
10
9C
FU
bac
teri
a
and
yea
st
Fo
rth
ed
ura
tio
n
of
anti
bio
tic
trea
tmen
t
(10
day
s)
14
day
sA
nti
bio
tics
for
up
per
resp
irat
ory
trac
t
infe
ctio
ns
(no
t
spec
ified
oth
erw
ise)
No
tre
port
edP
robu
gs
(Lif
eway
Fo
ods,
Inc,
Chi
cag
o,
IL)
Lif
eway
Fo
od
s,
Inc
AA
D¼
anti
bio
tic-
asso
ciat
edd
iarr
hea
;B
SS¼
Bri
sto
lS
too
lS
cale
;C
FU¼
colo
ny
-fo
rmin
gu
nit
s;S
B¼
Sb
ou
lard
ii.
�A
sca
lcu
late
db
yth
eau
tho
rs.
Arvola 1999
Ran
dom
seq
uenc
e ge
nera
tion
(sel
ectio
n bi
as)
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
Blin
ding
of p
artic
ipan
ts a
nd p
erso
nnel
(pe
rfor
man
ce b
ias)
Blin
ding
of o
utco
me
asse
ssm
ent (
dete
ctio
n bi
as)
Inco
mpl
ete
outc
ome
data
(at
triti
on b
ias)
Sel
ectiv
e re
port
ing
(rep
ortin
g bi
as)
Bin 2015
Casem 2013
Contardi 1991
Correa 2005
Destura (unpublished)
Erdeve 2004
Fox 2015
Jirapinyo 2002
Khodadad 2013
King 2010
Kotowska 2005
Merenstein 2009
Ruszczynski 2008
Shan 2013
Szajewska 2009
Szymanski 2008
Tankanow 1990
Vaisanen 1998
Vanderhoof 1999
Zhao 2014
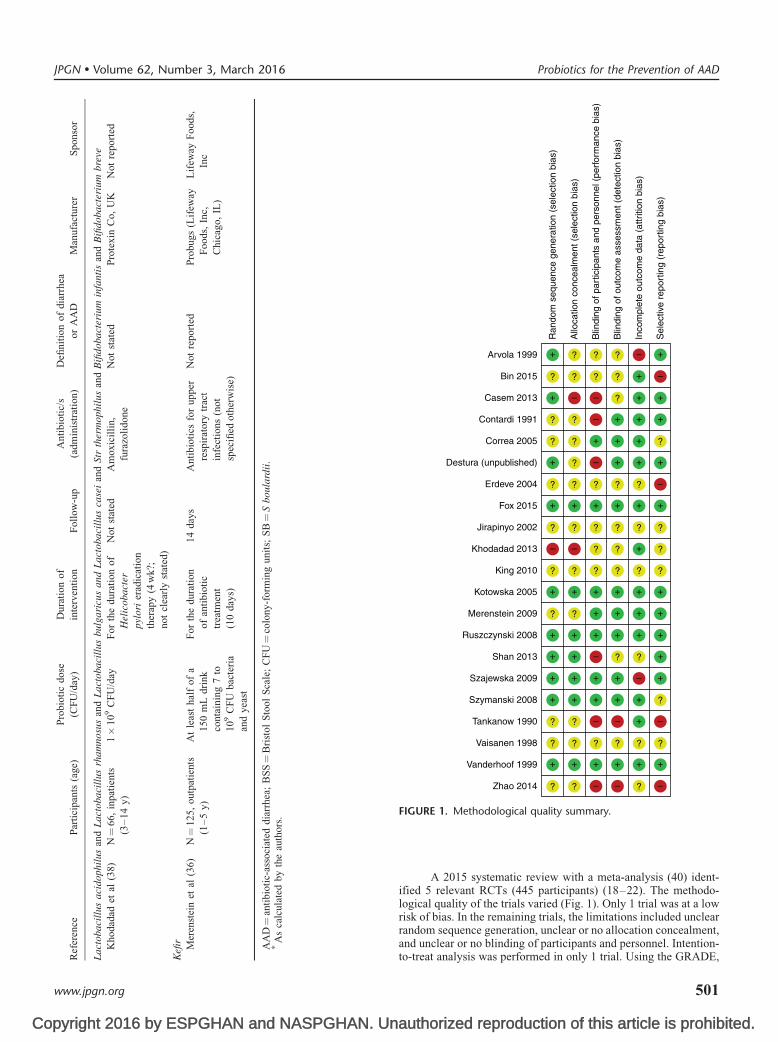
FIGURE 1. Methodological quality summary.
JPGN � Volume 62, Number 3, March 2016 Probiotics for the Prevention of AAD
www.jpgn.org
A 2015 systematic review with a meta-analysis (40) ident-ified 5 relevant RCTs (445 participants) (18–22). The methodo-logical quality of the trials varied (Fig. 1). Only 1 trial was at a lowrisk of bias. In the remaining trials, the limitations included unclearrandom sequence generation, unclear or no allocation concealment,
authorized reproduction of this article is prohibited.
and unclear or no blinding of participants and personnel. Intention-to-treat analysis was performed in only 1 trial. Using the GRADE,
501
Co
1.1.1 S boulardiiKotowska 2005Erdeve 2004Shan 2013Bin 2015Zhao 2014Casem 2013Subtotal (95% CI)Total eventsHeterogeneity Tau2 = 0.07; Chi2 = 8.26, df = 5(P = 0.14); I2 = 39%
Test for overall effect: Z = 4.87 (P < 0.00001)
Vanderhoof 1999Szajewska 2009Arvola 1999King 2010Vaisanen 1998
Total events
1.1.3 B clausiiDestura (unpublished)
Heterogeneity : Not applicable
Heterogeneity : Not applicable
Total events
Total events
Total events 13
Subtotal (95% CI)
Test for overall effect: Z = 1.25 (P = 0.21)
Test for overall effect: Z = 2.13 (P = 0.03)
Heterogeneity : Not applicableTest for overall effect: Z = 0.62 (P = 0.54)
Total eventsHeterogeneity : Not applicableTest for overall effect: Z = 0.19 (P = 0.85)
1.1.4 B lactis & Str themophilus
1.1.6 L acidophilus & bulgaricus
1.1.5 B longum PL03 & L rhamnosus KL53A & L plantrarum PL02
Correa 2005Subtotal (95% CI)
Subtotal (95% CI)Szymanski 2008
Tankanow 1990
Total eventsHeterogeneity : Not applicableTest for overall effect: Z = 0.57 (P = 0.12)
Jirapinyo 2002
1.1.7 L acidophilus & B infantis
Total eventsHeterogeneity : Not applicableTest for overall effect Not applicable
Contardi 1991
1.1.8 L acidophilus & B breve
Subtotal (95% CI)
Subtotal (95% CI)
Subtotal (95% CI)
4146
122711
72336
21
3
3
1
10
13
1
10
3
3
0
0
13224416710512069
837
9334618
23219
162162
8080
4040
1515
88
2020
224218264716
74 171
256948
52
7
7
24
24
2
2
16
16
8
8
0
0
137222166100120
71816
9530587
36226
161161
7777
7.4%7.4%
3838
2323
1010
2020
Not estimableNot estimable
4.0%7.6%4.8%7.1%9.7%6.5%
39.7%
0.19 (0.07, 0.53)0.30 (0.17, 0.54)0.33 (0.13, 0.81)0.44 (0.23, 0.82)0.57 (0.39, 0.86)0.71 (0.35, 1.41)0.43 (0.30, 0.60)
5.6%2.2%3.0%3.7%4.7%
19.3%
0.29 (0.13, 0.63)0.29 (0.06, 1.35)0.32 (0.09, 1.11)0.66 (0.22, 1.97)1.17 (0.47, 2.95)0.48 (0.26, 0.89)
2.8%2.8%
0.43 (0.11, 1.62)0.43 (0.11, 1.62)
0.52 (0.29, 0.95)0.52 (0.29, 0.95)
1.0%1.0%
0.47 (0.04, 5.03)0.47 (0.04, 5.03)
9.1%9.1%
0.96 (0.61, 1.50)0.96 (0.61, 1.50)
4.5%4.5%
0.47 (0.18, 1.21)0.47 (0.18, 1.21)
Test for overall effect: Z =2.33(P = 0.02)Heterogeneity Tau2 = 0.07; Chi2 = 8.26, df = 5(P = 0.14); I2 = 40%
Subtotal (95% CI)
1.1.2 Lactobacillus GG
Study or subgroup Events Total EventsProbiotics
Total WeightControl
M-H, Random, 95% CIRisk ratio
M-H, Random, 95% CIRisk ratio
A B C D E FRisk of bias
0.01 0.1Favours probiotics Favours control
1 10 100
FIGURE 2. Effect of individual probiotic strains and probiotics as a group for preventing antibiotic-associated diarrhea.
(Continued on next page )
Szajewska et al JPGN � Volume 62, Number 3, March 2016
the overall quality of evidence was rated as moderate (Table S1,http://links.lww.com/MPG/A587).
Compared with placebo or no treatment, LGG administrationin children reduced the risk of AAD, regardless of the reason forwhich probiotics were used (ie, as part of Helicobacter pylorieradication or for other reasons), from 23% to 9.6% (5 RCTs,n¼ 445, RR 0.48, 95% CI 0.26–0.89; number needed to treat,
pyright 2016 by ESPGHAN and NASPGHAN. Un
NNT, 8, 95% CI 6–40) (Fig. 2). No significant heterogeneity wasfound (x2¼ 6.61, P¼ 0.16, I2¼ 40%). Only 1 trial (19) evaluated the
502
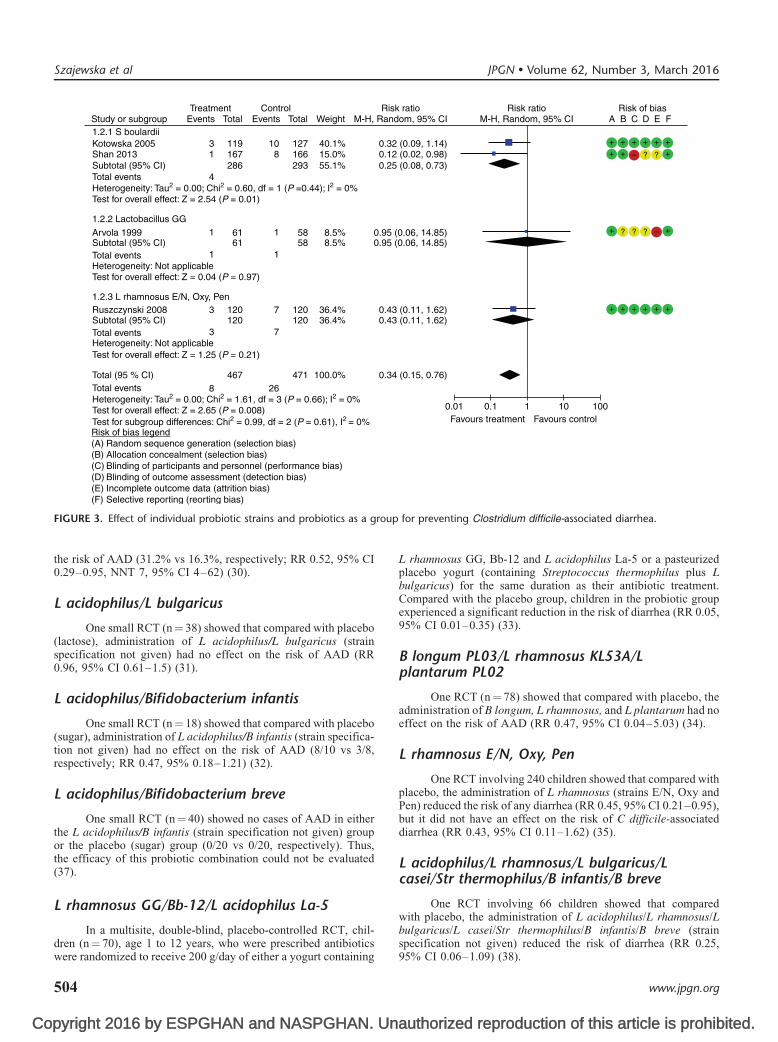
effect of LGG on the risk of C difficile-associated diarrhea in childrenand found no effect (RR 0.95, 95% CI 0.06–14.85) (Fig. 3).
The optimal daily dose of LGG for preventing AAD remainsunclear (40). In children, the best effect (reduction in the risk ofAAD by 71%) was achieved with the highest dose (1–2� 1010
CFU) (18). A similar effect size was, however, not achieved inanother trial using the same dose (19), perhaps because of a lower
authorized reproduction of this article is prohibited.
baseline risk of AAD. In adults, there was no clear link between theeffect size and the LGG dose.
www.jpgn.org
Co
Total eventsHeterogeneity : Not applicableTest for overall effect: Z = 1.85 (P = 0.06)
Test for overall effect: Z = 2.10 (P = 0.04)
Test for overall effect: Z = 3.00 (P = 0.003)
1.1.11 L rhamnosus GG & Bb12 & L acidophilus
1.1.9 L acidophilus & L rhamnosus & L bulgaricus & L casei & Str therophilus & B infantis & B breve
Subtotal (95% CI)Khodadad 2013
Total eventsHeterogeneity : Not applicable
Total eventsHeterogeneity : Not applicable
Test for overall effect: Z = 0.53 (P = 0.60)
Test for overall effect: Z = 5.80 (P < 000001)
1.1.12 Kefir
Total events
Total events
Heterogeneity : Not applicable
Heterogeneity Tau2 = 0.13; Chi2 = 34.51, df = 19 (P = 0.02); I2 = 45%
Test for subgroup differences: Chi2 = 16.82, df = 10 (P = 0.08); I2 = 40.6%
1.1.10 L rhamnosus E/N, Oxy, PenRuszczynki 2008
Fox 2015
Subtotal (95% CI)
Subtotal (95% CI)
Subtotal (95% CI)
Total (95% CI)
Merenstein 2009
2
2
9
1
11
148
9
1
11
3333
120120
3434
5757
1625
8
8
20
20
21
21
14
14
343
3333
120120
3636
6060
1620
2.4%2.4%
0.25 (0.06, 1.09)0.25 (0.06, 1.09)
6.0%6.0%
0.45 (0.21, 0.95)0.45 (0.21, 0.95)
1.5%1.5%
0.05 (0.01, 0.35)0.05 (0.01, 0.35)
6.4%6.4%
0.83 (0.41, 1.67)0.83 (0.41, 1.67)
100% 0.48 (0.37, 0.61)
Risk of bias legend
Random sequence generation (selection bias)Allocation concealment (selection bias)Blinding of participants and personnel (performance bias)Blinding of outcome assessment (detection bias)Incomplete outcome data (attrition bias)Selective reporting (reporting bias)
(A)(B)(C)(D)(E)(F)
0.01 0.1Favours probiotics Favours control
1 10 100
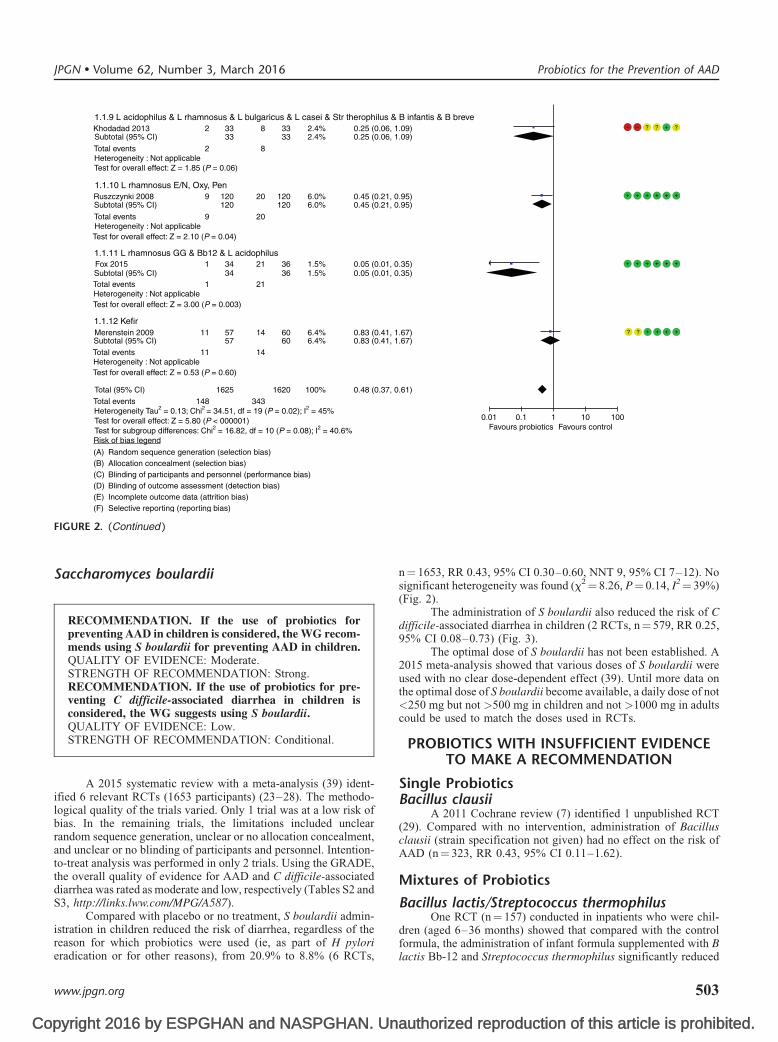
FIGURE 2. (Continued )
JPGN � Volume 62, Number 3, March 2016 Probiotics for the Prevention of AAD
Saccharomyces boulardii
RECOMMENDATION. If the use of probiotics forpreventing AAD in children is considered, the WG recom-mends using S boulardii for preventing AAD in children.QUALITY OF EVIDENCE: Moderate.STRENGTH OF RECOMMENDATION: Strong.RECOMMENDATION. If the use of probiotics for pre-venting C difficile-associated diarrhea in children isconsidered, the WG suggests using S boulardii.QUALITY OF EVIDENCE: Low.STRENGTH OF RECOMMENDATION: Conditional.
A 2015 systematic review with a meta-analysis (39) ident-ified 6 relevant RCTs (1653 participants) (23–28). The methodo-logical quality of the trials varied. Only 1 trial was at a low risk ofbias. In the remaining trials, the limitations included unclearrandom sequence generation, unclear or no allocation concealment,and unclear or no blinding of participants and personnel. Intention-to-treat analysis was performed in only 2 trials. Using the GRADE,the overall quality of evidence for AAD and C difficile-associateddiarrhea was rated as moderate and low, respectively (Tables S2 andS3, http://links.lww.com/MPG/A587).
Compared with placebo or no treatment, S boulardii admin-istration in children reduced the risk of diarrhea, regardless of the
pyright 2016 by ESPGHAN and NASPGHAN. Un
reason for which probiotics were used (ie, as part of H pylorieradication or for other reasons), from 20.9% to 8.8% (6 RCTs,
www.jpgn.org
n¼ 1653, RR 0.43, 95% CI 0.30–0.60, NNT 9, 95% CI 7–12). Nosignificant heterogeneity was found (x2¼ 8.26, P¼ 0.14, I2¼ 39%)(Fig. 2).
The administration of S boulardii also reduced the risk of Cdifficile-associated diarrhea in children (2 RCTs, n¼ 579, RR 0.25,95% CI 0.08–0.73) (Fig. 3).
The optimal dose of S boulardii has not been established. A2015 meta-analysis showed that various doses of S boulardii wereused with no clear dose-dependent effect (39). Until more data onthe optimal dose of S boulardii become available, a daily dose of not<250 mg but not >500 mg in children and not >1000 mg in adultscould be used to match the doses used in RCTs.
PROBIOTICS WITH INSUFFICIENT EVIDENCETO MAKE A RECOMMENDATION
Single ProbioticsBacillus clausii
A 2011 Cochrane review (7) identified 1 unpublished RCT(29). Compared with no intervention, administration of Bacillusclausii (strain specification not given) had no effect on the risk ofAAD (n¼ 323, RR 0.43, 95% CI 0.11–1.62).
Mixtures of Probiotics
Bacillus lactis/Streptococcus thermophilusOne RCT (n¼ 157) conducted in inpatients who were chil-
dren (aged 6–36 months) showed that compared with the control
authorized reproduction of this article is prohibited.
formula, the administration of infant formula supplemented with Blactis Bb-12 and Streptococcus thermophilus significantly reduced
503
Co
Study or subgroup Events TotalTreatment
Events Total WeightControl
M-H, Random, 95% CIRisk ratio
M-H, Random, 95% CIRisk ratio
A B C D E FRisk of bias
Risk of bias legendRandom sequence generation (selection bias)Allocation concealment (selection bias)Blinding of participants and personnel (performance bias)Blinding of outcome assessment (detection bias)Incomplete outcome data (attrition bias)Selective reporting (reorting bias)
(A)(B)(C)(D)(E)(F)
Kotowska 20051.2.1 S boulardii
1.2.3 L rhamnosus E/N, Oxy, Pen
1.2.2 Lactobacillus GG
Shan 2013Subtotal (95% CI)
119167
108
286
127166293
40.1%15.0%55.1%
0.32 (0.09, 1.14)0.12 (0.02, 0.98)0.25 (0.08, 0.73)
Subtotal (95% CI) 61 58 8.5% 0.95 (0.06, 14.85)Arvola 1999 61 58 8.5% 0.95 (0.06, 14.85)
Subtotal (95% CI) 120 120 36.4% 0.43 (0.11, 1.62)
467 471 100.0% 0.34 (0.15, 0.76)
Ruszczynski 2008 120 120 36.4% 0.43 (0.11, 1.62)
Total eventsHeterogeneity: Tau2 = 0.00; Chi2 = 0.60, df = 1 (P =0.44); I2 = 0%Test for overall effect: Z = 2.54 (P = 0.01)
Total events
Total events
Total (95 % CI)
Heterogeneity: Tau2 = 0.00; Chi2 = 1.61, df = 3 (P = 0.66); I2 = 0%
Heterogeneity: Not applicable
Test for overall effect: Z = 2.65 (P = 0.008)
Test for overall effect: Z = 1.25 (P = 0.21)
Heterogeneity: Not applicableTest for overall effect: Z = 0.04 (P = 0.97)
Test for subgroup differences: Chi2 = 0.99, df = 2 (P = 0.61), I2 = 0%
3
73
73
Total events 11
11
268
1
4
0.01 0.1Favours treatment Favours control
1 10 100
oup
Szajewska et al JPGN � Volume 62, Number 3, March 2016
the risk of AAD (31.2% vs 16.3%, respectively; RR 0.52, 95% CI0.29–0.95, NNT 7, 95% CI 4–62) (30).
L acidophilus/L bulgaricus
One small RCT (n¼ 38) showed that compared with placebo(lactose), administration of L acidophilus/L bulgaricus (strainspecification not given) had no effect on the risk of AAD (RR0.96, 95% CI 0.61–1.5) (31).
L acidophilus/Bifidobacterium infantis
One small RCT (n¼ 18) showed that compared with placebo(sugar), administration of L acidophilus/B infantis (strain specifica-tion not given) had no effect on the risk of AAD (8/10 vs 3/8,respectively; RR 0.47, 95% 0.18–1.21) (32).
L acidophilus/Bifidobacterium breve
One small RCT (n¼ 40) showed no cases of AAD in eitherthe L acidophilus/B infantis (strain specification not given) groupor the placebo (sugar) group (0/20 vs 0/20, respectively). Thus,the efficacy of this probiotic combination could not be evaluated(37).
L rhamnosus GG/Bb-12/L acidophilus La-5
In a multisite, double-blind, placebo-controlled RCT, chil-
FIGURE 3. Effect of individual probiotic strains and probiotics as a gr
pyright 2016 by ESPGHAN and NASPGHAN. Un
dren (n¼ 70), age 1 to 12 years, who were prescribed antibioticswere randomized to receive 200 g/day of either a yogurt containing
504
L rhamnosus GG, Bb-12 and L acidophilus La-5 or a pasteurizedplacebo yogurt (containing Streptococcus thermophilus plus Lbulgaricus) for the same duration as their antibiotic treatment.Compared with the placebo group, children in the probiotic groupexperienced a significant reduction in the risk of diarrhea (RR 0.05,95% CI 0.01–0.35) (33).
B longum PL03/L rhamnosus KL53A/Lplantarum PL02
One RCT (n¼ 78) showed that compared with placebo, theadministration of B longum, L rhamnosus, and L plantarum had noeffect on the risk of AAD (RR 0.47, 95% CI 0.04–5.03) (34).
L rhamnosus E/N, Oxy, Pen
One RCT involving 240 children showed that compared withplacebo, the administration of L rhamnosus (strains E/N, Oxy andPen) reduced the risk of any diarrhea (RR 0.45, 95% CI 0.21–0.95),but it did not have an effect on the risk of C difficile-associateddiarrhea (RR 0.43, 95% CI 0.11–1.62) (35).
L acidophilus/L rhamnosus/L bulgaricus/Lcasei/Str thermophilus/B infantis/B breve
One RCT involving 66 children showed that comparedwith placebo, the administration of L acidophilus/L rhamnosus/Lbulgaricus/L casei/Str thermophilus/B infantis/B breve (strain
for preventing Clostridium difficile-associated diarrhea.
authorized reproduction of this article is prohibited.
specification not given) reduced the risk of diarrhea (RR 0.25,95% CI 0.06–1.09) (38).
www.jpgn.org

Co
Kefir
One RCT evaluated the effect of kefir (ie, a fermented milkcontaining Lactococcus lactis, Lactococcus plantarum, Lacto-coccus rhamnosus, Lactococcus casei, Lactococcus lactis sub-species diacetylactis, Leuconostoc cremoris, B longum, B breve,Lactobacillus acidophilus, and 1 yeast, Saccharomyces florentinus)on the risk of AAD. There was no significant difference between thekefir group and the group receiving heat-treated kefir (RR 0.83,95% CI 0.41–1.67) (36).
Yogurt
Yogurt is a form of fermented milk that contains symbioticcultures of Streptococcus thermophilus and L delbrueckii subsp.bulgaricus. A 2015 systematic review with a meta-analysis ident-ified 2 relevant RCTs, both low in methodological quality. Com-pared with no intervention, yogurt consumption had no effect on therisk of AAD (2 RCTs, n¼ 314, RR 0.45; 95% CI 0.11–1.75) (41).
SAFETYThe WG abstained from evaluating the safety of probiotics,
as this was thoroughly reviewed in 2011 by the US Agency forHealthcare Research and Quality (for review, (42)). Althoughprobiotics are safe for use in otherwise healthy populations, cautionshould be taken in specific patient groups. Risk factors for adverseevents include immunosuppression, prematurity, critical illness,presence of structural heart disease, presence of a central venouscatheter, and the potential for translocation of probiotics across thebowel wall. There is a lack of data that specifically address thesafety of probiotics for preventing AAD in these vulnerable popu-lations. The risk of side effects is, however, greater in people whohave severe underlying health conditions.
JPGN � Volume 62, Number 3, March 2016
pyrig
�
�
�
�
www
SUMMARY
The WG questions pooling different probiotic strains togetherin a meta-analysis. Probiotic effects against AAD are strainspecific; thus, the efficacy and safety of each should be
e stablished and recommendations for using these strainsshould be made accordingly.� T
he safety and clinical effects of 1 probiotic microorganismshould not be extrapolated to other probiotic microorganisms.A lack of evidence regarding the efficacy of a certain �p robiotic(s) does not mean that future studies will notestablish efficacy in preventing AAD.There is a lack of data that specifically address the safety of �p robiotics for preventing AAD in children who have severeunderlying health conditions.The WG recommends choosing a probiotic, the efficacyof which has been confirmed in well-conducted RCTs,from a manufacturer who has a regulated quality control of f actors including the composition and content of theprobiotic agent.Risk factors for the occurrence of AAD or C difficile-associated diarrhea such as class of antibiotic(s), duration ofantibiotic treatment, age, need for hospitalization, comorbid-ities, and previous episodes of AAD or C difficile-associated d iarrhea should be considered when making decisions on theuse of probiotics in children for preventing AAD.If the use of probiotics for preventing AAD is considered, theht 2016 by ESPGHAN and NASPGHAN. Un
WG recommends using L rhamnosus GG or S boulardii(moderate quality of evidence; strong recommendation).
.jpgn.org
auth
prca
If the use of probiotics for preventing C difficile-associated
Probiotics for the Prevention of AAD
�diarrhea is considered, the WG suggests using S boulardii(low quality of evidence; conditional recommendation).
REFERENCES1. Barbut F, Meynard JL. Managing antibiotic associated diarrhoea. BMJ
2002;324:1345–6.2. McFarland LV. Epidemiology, risk factors and treatments for antibiotic-
associated diarrhea. Dig Dis 1998;16:292–307.3. McFarland LV, Surawicz CM, Stamm WE. Risk factors for Clostridium
difficile carriage and C. difficile-associated diarrhea in a cohort ofhospitalized patients. J Infect Dis 1990;162:678–84.
4. McFarland LV. Meta-analysis of probiotics for the prevention of anti-biotic associated diarrhea and the treatment of Clostridium difficiledisease. Am J Gastroenterol 2006;101:812–22.
5. Hill C, Guarner F, Reid G, et al. Expert consensus document. TheInternational Scientific Association for Probiotics and Prebiotics con-sensus statement on the scope and appropriate use of the term probiotic.Nat Rev Gastroenterol Hepatol 2014;11:506–14.
6. Szajewska H, Guarino A, Hojsak I, et al., European Society for PediatricGastroenterology, Hepatology, and Nutrition. Use of probiotics formanagement of acute gastroenteritis: a position paper by the ESPGHANWorking Group for Probiotics and Prebiotics. J Pediatr GastroenterolNutr 2014;58:531–9.
7. Johnston BC, Goldenberg JZ, Vandvik PO, et al. Probiotics for theprevention of pediatric antibiotic-associated diarrhea. Cochrane Data-base Syst Rev 2011CD004827.
8. Guarner F, Khan AG, Garisch J, et al., World Gastroenterology Orga-nization. World Gastroenterology Organisation Global Guidelines:probiotics and prebiotics October 2011. J Clin Gastroenterol 2012;46:468–81.
9. Grzeskowiak Ł, Isolauri E, Salminen S, et al. Manufacturing processinfluences properties of probiotic bacteria. Br J Nutr 2011;105:887–94.
10. Sanders ME, Guarner F, Guerrant R, et al. An update on the useand investigation of probiotics in health and disease. Gut 2013;62:787–96.
11. Higgins JPT, Altman DG, Sterne AC. Assessing risk of bias in includedstudies. In: Higgins JPT, Green S, eds. Cochrane Handbook for Sys-tematic Reviews of Interventions. Version 5.1.0. www.cochrane-handbook.org. Published 2011. Accessed July 2015.
12. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensuson rating quality of evidence and strength of recommendations. BMJ2008;336:924–6.
13. Andrews J, Guyatt G, Oxman AD, et al. GRADE guidelines: 14. Goingfrom evidence to recommendations: the significance and presentation ofrecommendations. J Clin Epidemiol 2013;66:719–25.
14. Center for Drug Evaluation and Research; Center for Biologics Eva-luation and Research. Guidance for industry: providing clinical evi-dence of effectiveness for human drug and biological products. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm078749.pdf. Published May 1998. AccessedJuly 2015.
15. Rijkers GT, Bengmark S, Enck P, et al. Guidance for substantiatingthe evidence for beneficial effects of probiotics: current status andrecommendations for future research. J Nutr 2010;140:671S–6S.
16. Hempel S, Newberry SJ, Maher AR, et al. Probiotics for the preventionand treatment of antibiotic-associated diarrhea: a systematic review andmeta-analysis. JAMA 2012;307:1959–69.
17. Goldenberg JZ, Ma SS, Saxton JD, et al. Probiotics for the preventionof Clostridium difficile-associated diarrhea in adults and children.Cochrane Database Syst Rev 2013;5:CD006095.
18. Vanderhoof JA, Whitney DB, Antonson DL, et al. Lactobacillus GG inthe prevention of antibiotic-associated diarrhea in children. J Pediatrics1999;135:564–8.
19. Arvola T, Laiho K, Torkkeli S, et al. Prophylactic Lactobacillus GGreduces antibiotic-associated diarrhea in children with respiratoryinfections: a randomized study. Pediatrics 1999;104:e64.
20. King SN, Chung AM, Vidal R. Randomized, double blind, placebocontrolled trial to assess the efficacy of Lactobacillus GG in the
orized reproduction of this article is prohibited.
evention of antibiotic-associated diarrhea in the pediatric internsivere unit (PICU). Pharmacotherapy 2010;30:457–8.
505

Co
21. Vaisanen LM, Leskinen M, Siitonen A, et al. Occurence of diarrhea inchildren receiving oral antibiotics with or without probiotic supple-mentation with Lactobacillus GG. Microb Ecol Health Dis 1998;10:199–200.
22. Szajewska H, Albrecht P, Topczewska-Cabanek A. Randomized, double-blind, placebo-controlled trial: effect of lactobacillus GG supplementationon Helicobacter pylori eradication rates and side effects during treatmentin children. J Pediatr Gastroenterol Nutr 2009;48:431–6.
23. Kotowska M, Albrecht P, Szajewska H. Saccharomyces boulardii in theprevention of antibiotic-associated diarrhea in children: a randomizeddouble-blind placebo-controlled trial. Aliment Pharmacol Ther 2005;21:583–90.
24. Casem RAO. Saccharomyces boulardii in the prevention of antibioticassociated diarrhea in children: a randomized controlled trial. PediatrInfect Dis Soc Philipp J 2013;14:70–6.
25. Erdeve O, Tiras U, Dallar Y. The probiotic effect of Saccharomycesboulardii in a pediatric age group. J Trop Pediatr 2004;50:234–6.
26. Shan LS, Hou P, Wang ZJ, et al. Prevention and treatment of diarrhoeawith Saccharomyces boulardii in children with acute lower respiratorytract infections. Benef Microbes 2013;4:329–34.
27. Bin Z, Ya-Zheng X, Zhao-Hui D, et al. The efficacy of Saccharomycesboulardii CNCM I-745 in addition to standard Helicobacter pylorieradication treatment in children. Pediatr Gastroenterol Hepatol Nutr2015;18:17–22.
28. Zhao HM, Ou-Yang HJ, Duan BP, et al. Clinical effect of triple therapycombined with Saccharomyces boulardii in the treatment of Helico-bacter pylori infection in children. Zhongguo Dang Dai Er Ke Za Zhi2014;16:230–3.
29. Destura RV. Bacillus clausii in preventing antibiotic-associated diarrheaamong Filipino infants and children: a multi-center, randomized, open-label clinical trial of efficacy and safety. Unpublished.
30. Correa NBO, Peret Filho LA, Penna FJ, et al. A Randomized formulacontrolled trial of Bifidobacterium lactis and Streptococcus thermophi-lus for prevention of antibiotic-associated diarrhea in infants. J ClinGastroenterol 2005;39:385–9.
31. Tankanow RM, Ross MB, Ertel IJ, et al. A double-blind, placebo-
Szajewska et al
pyright 2016 by ESPGHAN and NASPGHAN. Un
amoxicillin-induced diarrhea. DICP 1990;24:382–4.
506
32. Jirapinyo P, Densupsoontorn N, Thamonsiri N, et al. Prevention ofantibiotic-associated diarrhea in infants by probiotics. J Med Assoc Thai2002;85(suppl 2):S739–42.
33. Fox MJ, Ahuja KDK, Robertson IK, et al. Can probiotics yogurt preventdiarrhea in children on antibiotics? A double-blind, randomized,placebo-controlled study. BMJ OPEN 2015;5:e006474.
34. Szymanski H, Armanska M, Kowalska-Duplaga K, et al. Bifidobacter-ium longum PL03, Lactobacillus rhamnosus KL53A, andLactobacillus plantarum PL02 in the prevention of antibiotic-associateddiarrhea in children: a randomized controlled pilot trial. Digestion2008;78:13–7.
35. Ruszczynski M, Radzikowski A, Szajewska H. Clinical trial: effective-ness of Lactobacillus rhamnosus (strains E/N, Oxy and Pen) in theprevention of antibiotic-associated diarrhoea in children. Aliment Phar-macol Ther 2008;28:154–61.
36. Merenstein DJ, Foster J, D’Amico F. A randomized clinical trialmeasuring the influence of kefir on antibiotic-associated diarrhea: themeasuring the influence of Kefir (MILK) Study. Arch Pediatr AdolescMed 2009;163:750–4.
37. Contardi I. Oral bacterial therapy in prevention of antibiotic-induceddiarrhea in childhood [Batterioterapia orale quale prevenzione delladiarrea da antibiotici in eta pediatrica]. Clinica Terapeutica 1991;136:409–13.
38. Khodadad A, Farahmand F, Najafi M, et al. Probiotics for the treatmentof pediatric Helicobacter pylori infection: a randomized double blindclinical trial. Iran J Pediatr 2013;23:79–84.
39. Szajewska H, Kołodziej M. Systematic review with meta-analysis:Saccharomyces boulardii in the prevention of antibiotic-associateddiarrhoea. Aliment Pharmacol Ther 2015;42:793–801.
40. Szajewska H, Kołodziej M. Systematic review with meta-analysis:Lactobacillus GG in the prevention of antibiotic-associated diarrhoea.Aliment Pharmacol Ther 2015;42:1149–57.
41. Patro-Gołab B, Sharmi R, Szajewska H. Yogurt for treating antibiotic-associated diarrhea: systematic review and meta-analysis. Nutrition2015;31:796–800.
42. Hempel S, Newberry S, Ruelaz A, et al. Safety of probiotics used
JPGN � Volume 62, Number 3, March 2016
to reduce risk and prevent or treat disease. Evid Rep Technol Assess
controlled study of the efficacy of Lactinex in the prophylaxis ofauthorized reproduction of this article is prohibited.
(Full Rep) 2011;200:1–645.
www.jpgn.org