Embed Size (px)
Citation preview
Problem case in Primary care
DR Jim Moore GPSI GLOS Heart Failure service

“To expect the unexpected shows a thoroughly modern intellect”
Oscar Wilde
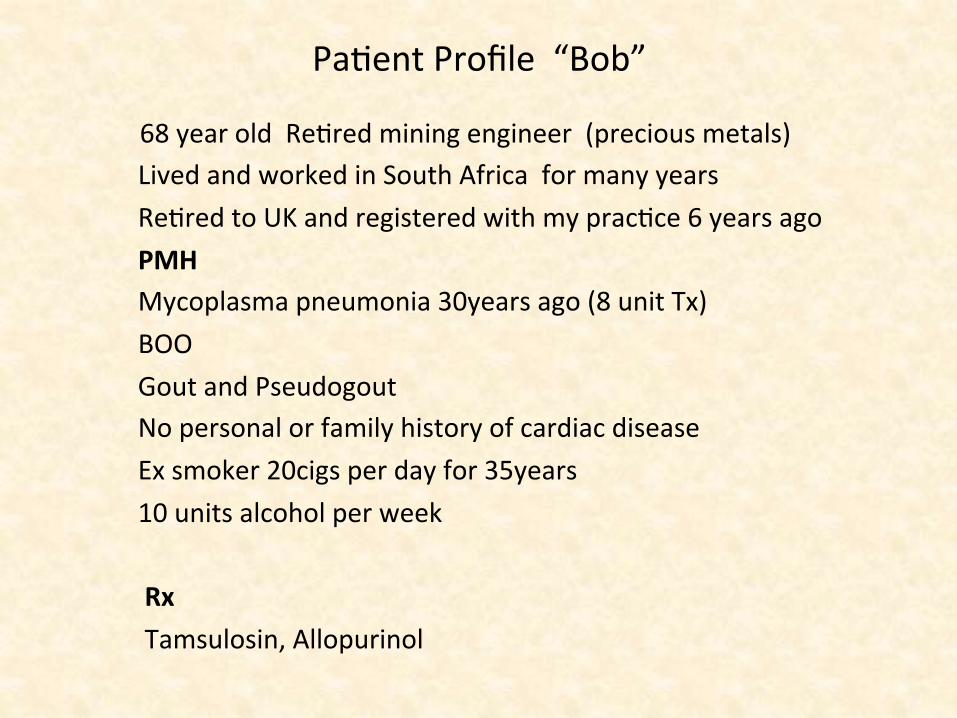
PaFent Profile “Bob”
68 year old ReFred mining engineer (precious metals) Lived and worked in South Africa for many years ReFred to UK and registered with my pracFce 6 years ago PMH Mycoplasma pneumonia 30years ago (8 unit Tx) BOO Gout and Pseudogout No personal or family history of cardiac disease Ex smoker 20cigs per day for 35years 10 units alcohol per week Rx Tamsulosin, Allopurinol
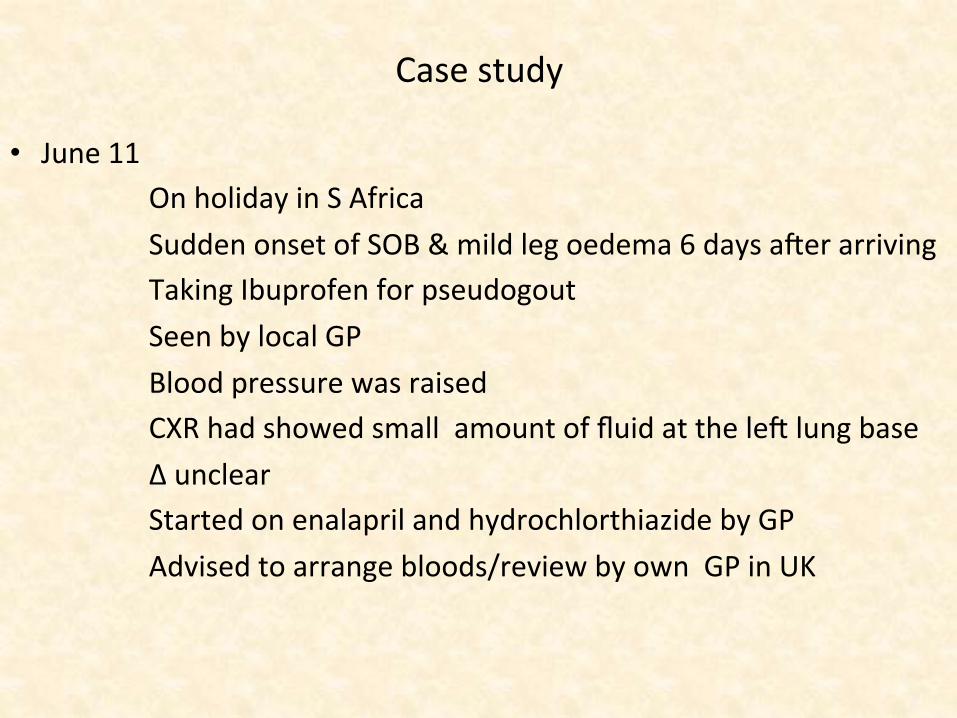
Case study
• June 11 On holiday in S Africa Sudden onset of SOB & mild leg oedema 6 days a]er arriving Taking Ibuprofen for pseudogout Seen by local GP Blood pressure was raised CXR had showed small amount of fluid at the le] lung base Δ unclear Started on enalapril and hydrochlorthiazide by GP Advised to arrange bloods/review by own GP in UK
…presents for review with own GP 2 weeks later • AsymptomaFc • 78/min regular 122/74 normal HS chest clear • No signs of fluid retenFon • FBC/TSH/LFTS/CRP all normal • eGFR 47, serum creaFnine 127 ,urate 0.4 ,
Conclusions • Cause of previous episode of breathlessness unclear ? Chest infecFon • BP well controlled • no change in management other than allopurinol ^200mg and
conFnue Ibuprofen • CKD
Would you arrange any addi8onal inves8ga8ons ?
Would you arrange any addi8onal inves8ga8ons?
• No……..only rouFne follow up of blood pressure.
• Chest x-‐ray • ECG • Chest x-‐ray and ECG • D Dimer • Urgent CTPA
What actually happened
• No……..only rouFne follow up of blood pressure. • Chest x-‐ray was normal other than a borderline CT ra8o
• ECG • Chest x-‐ray and ECG • D Dimer • Urgent CTPA
…a further 2 weeks later presents to pracFce “triage”
• Just returned from a holiday in Jersey ( by air) • Presents to triage mildly breathless with some chest “restricFon” • Talking easily in sentences • No pleuriFc pain • Slight unproducFve cough • He felt bloated and c/o ankle swelling • Noisy breathing intermijently with a lijle catarrh • On examinaFon 96/min regular, 112/62, normal HS (but
sounded unusual) but no murmurs, RR normal , O2 sats 95%, chest clear-‐ PF 480. No fever
• A lijle pimng oedema of both ankles/calfs so] What happened next ?
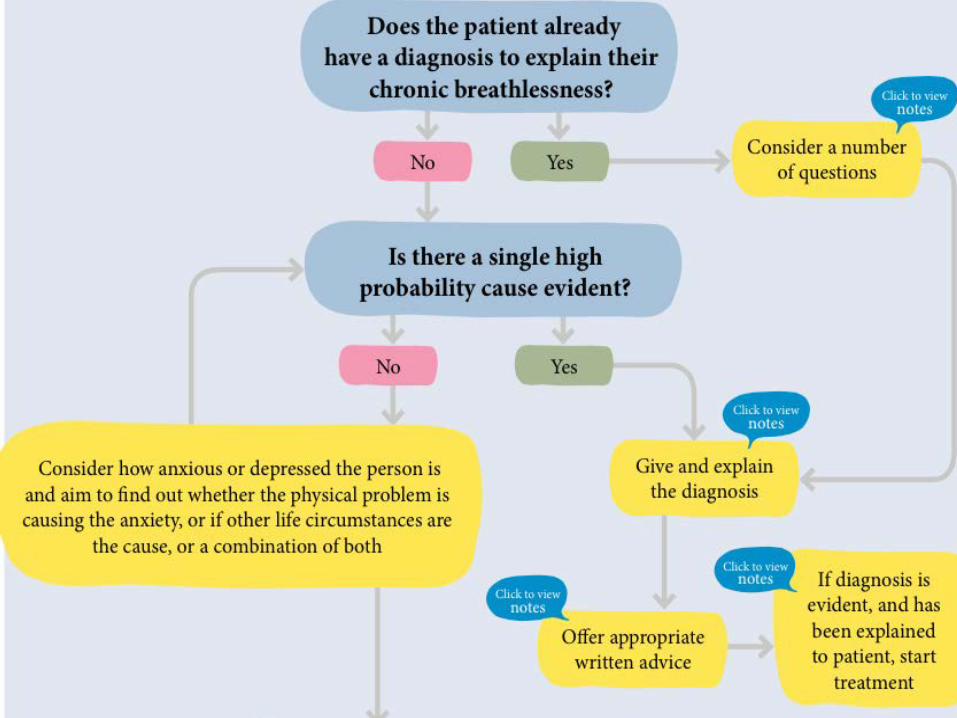
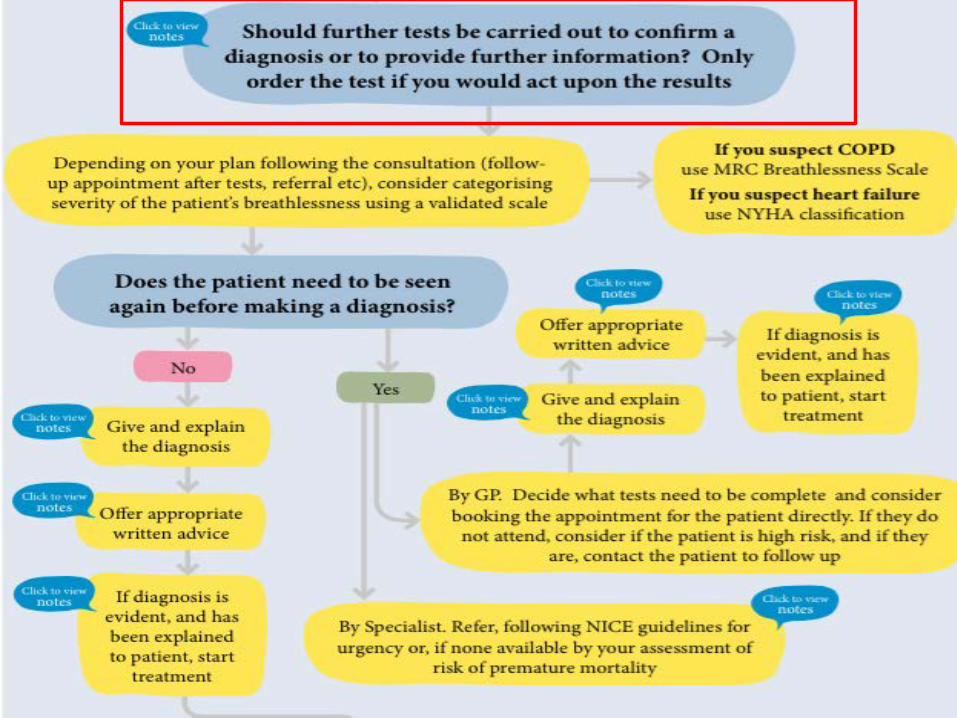
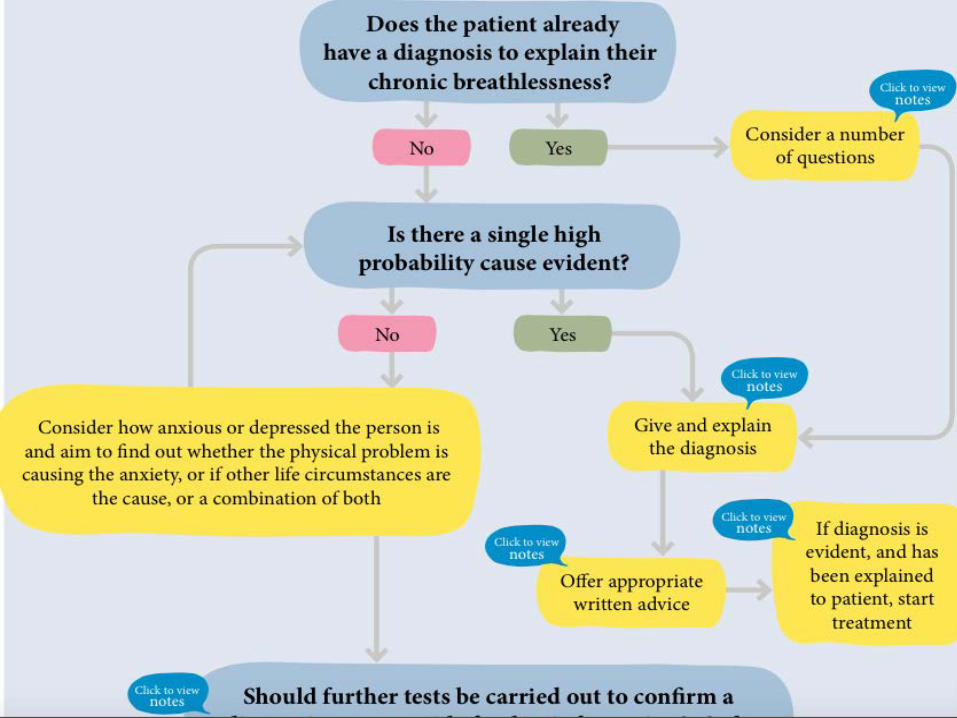
Search online for the Impress Breathlessness Algorithm
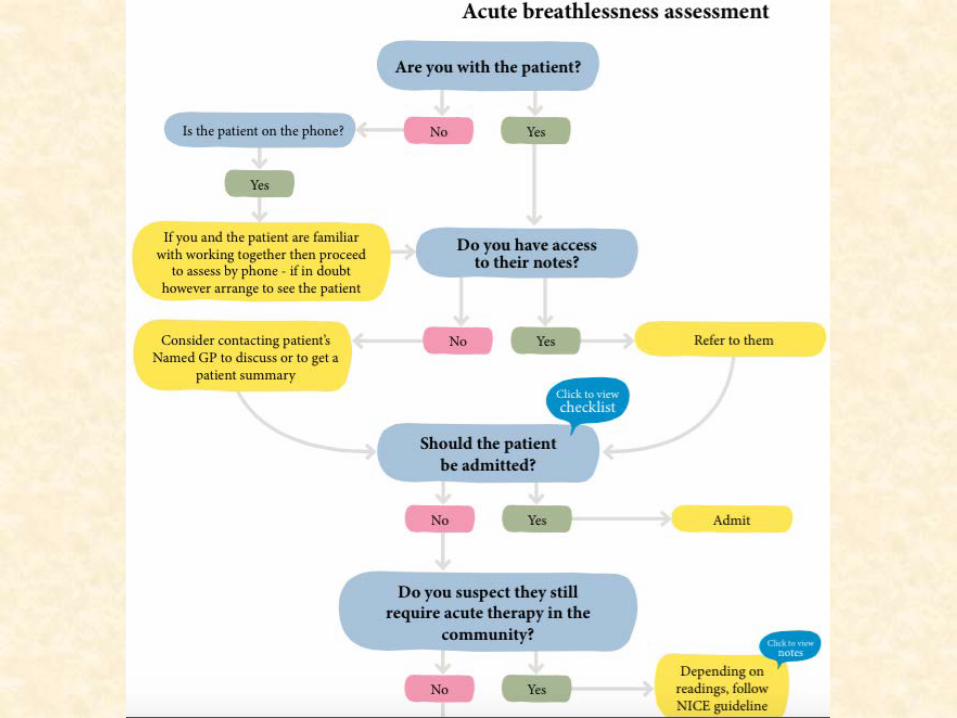
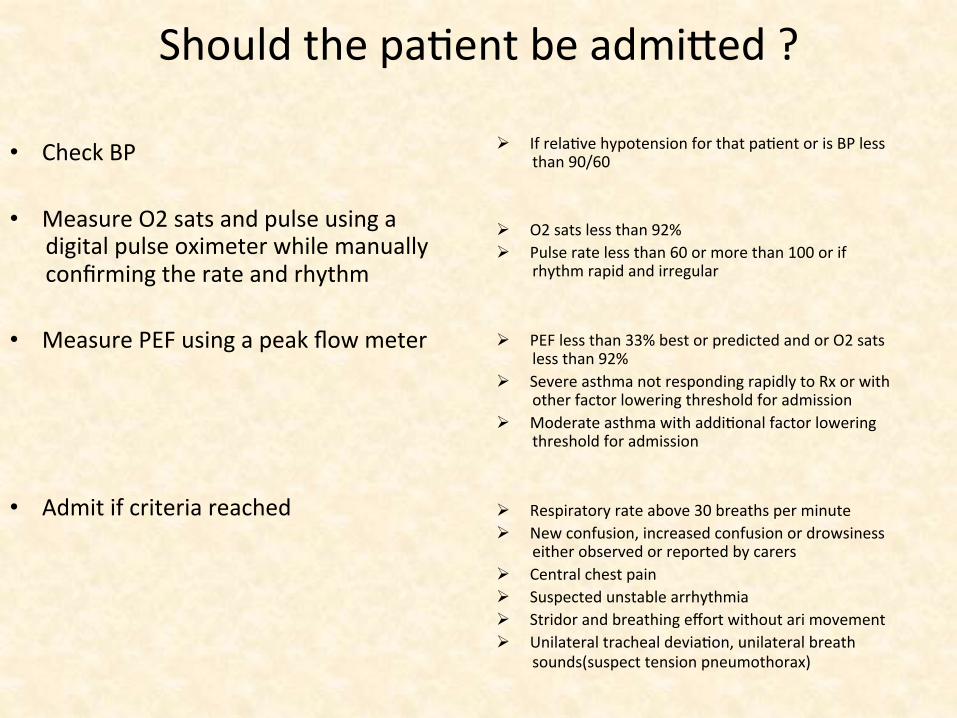
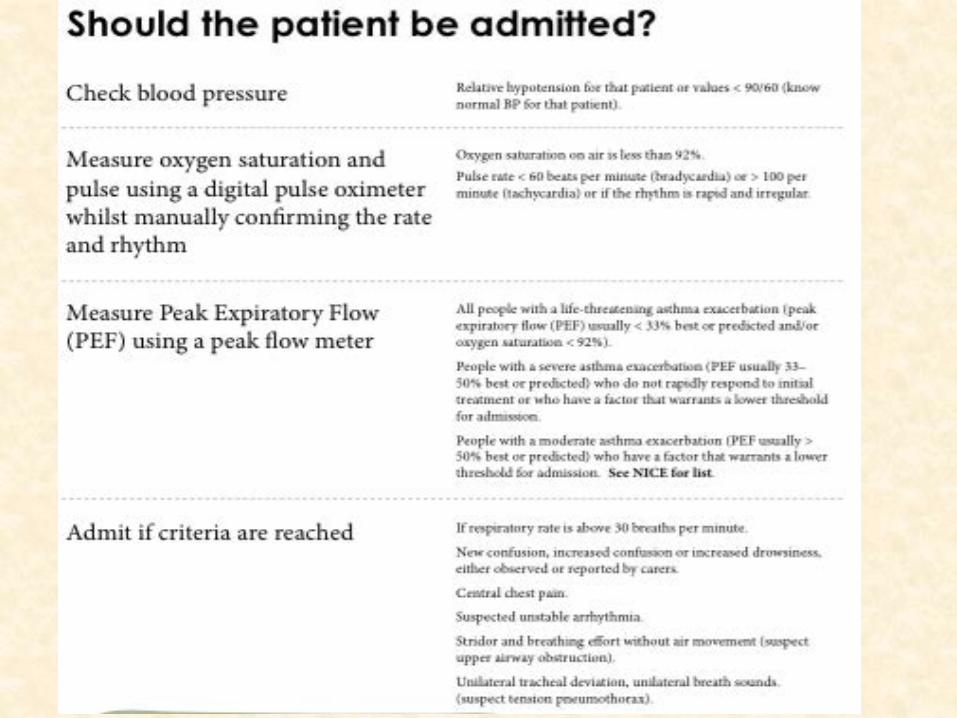
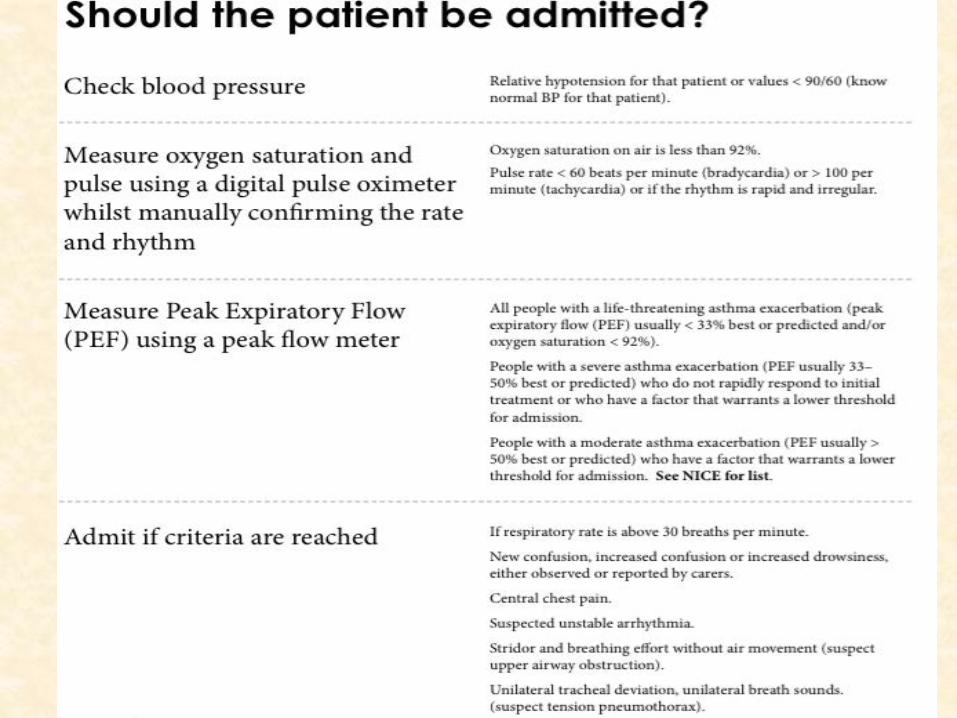
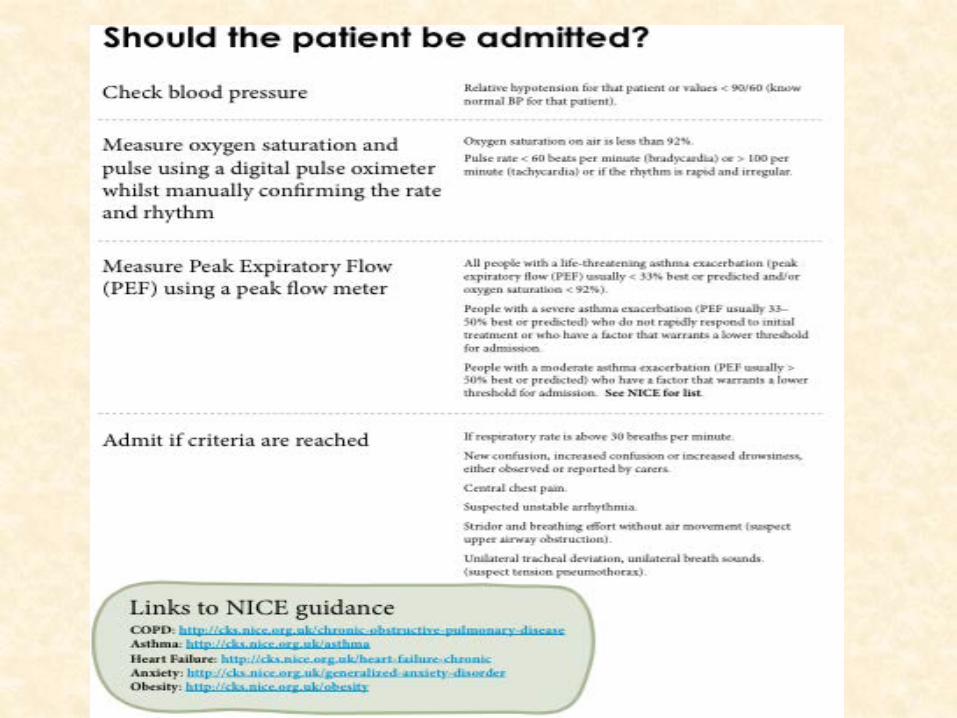
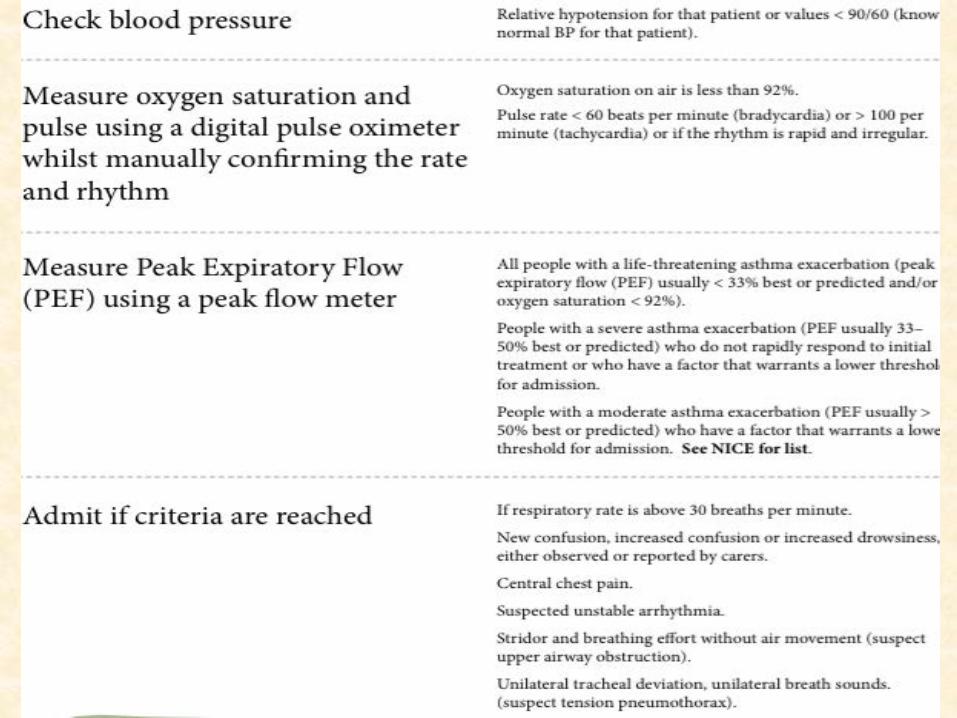
Should the paFent be admijed ? • Check BP
• Measure O2 sats and pulse using a digital pulse oximeter while manually confirming the rate and rhythm
• Measure PEF using a peak flow meter
• Admit if criteria reached
! If relaFve hypotension for that paFent or is BP less than 90/60
! O2 sats less than 92% ! Pulse rate less than 60 or more than 100 or if
rhythm rapid and irregular
! PEF less than 33% best or predicted and or O2 sats less than 92%
! Severe asthma not responding rapidly to Rx or with other factor lowering threshold for admission
! Moderate asthma with addiFonal factor lowering threshold for admission
! Respiratory rate above 30 breaths per minute ! New confusion, increased confusion or drowsiness
either observed or reported by carers ! Central chest pain ! Suspected unstable arrhythmia ! Stridor and breathing effort without ari movement ! Unilateral tracheal deviaFon, unilateral breath
sounds(suspect tension pneumothorax)
Case study -‐Primary care
• 2 weeks later…… • Just returned from a holiday in Jersey • Present to triage mildly breathless with some chest “restricFon” • Talking easily in sentences • No pleuriFc pain • Slight unproducFve cough • He felt bloated • Noisy breathing intermijently with a lijle catarrh • On examinaFon 96/min regular, 112/62, normal HS (but
sounded unusual) but no murmurs, RR normal , O2 sats 95%, chest clear-‐ PF 480. No fever
• A lijle pimng oedema of both ankles/calfs so]
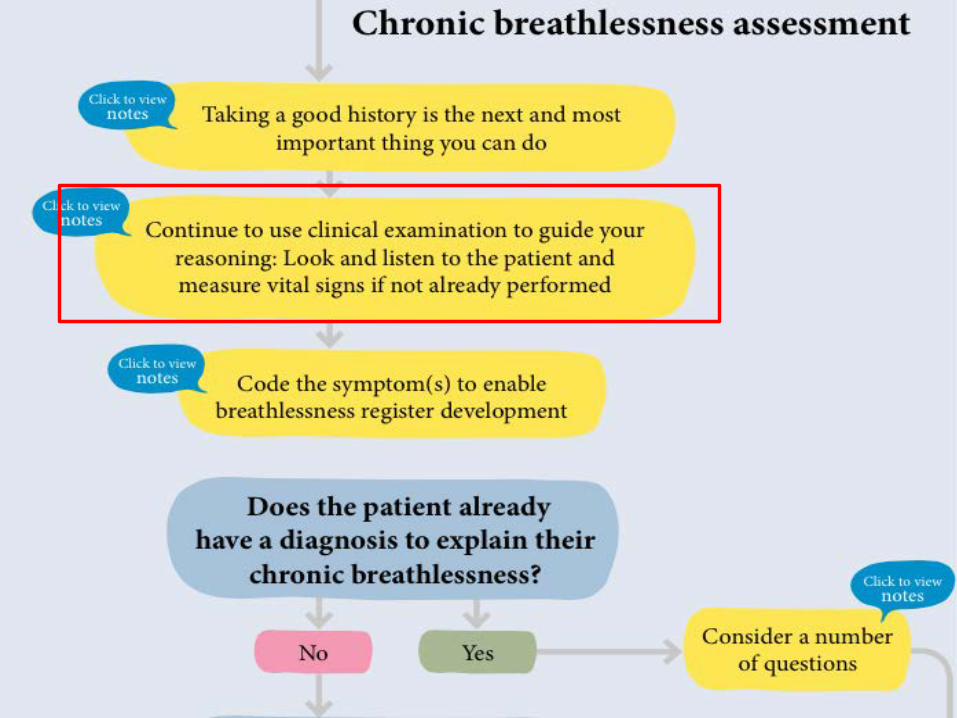
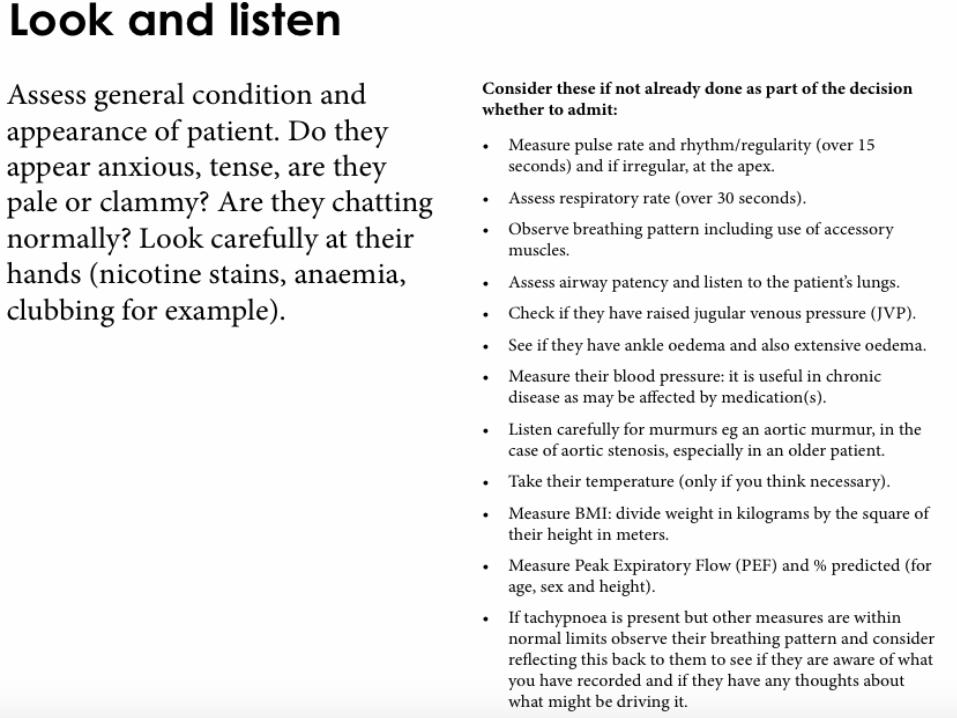
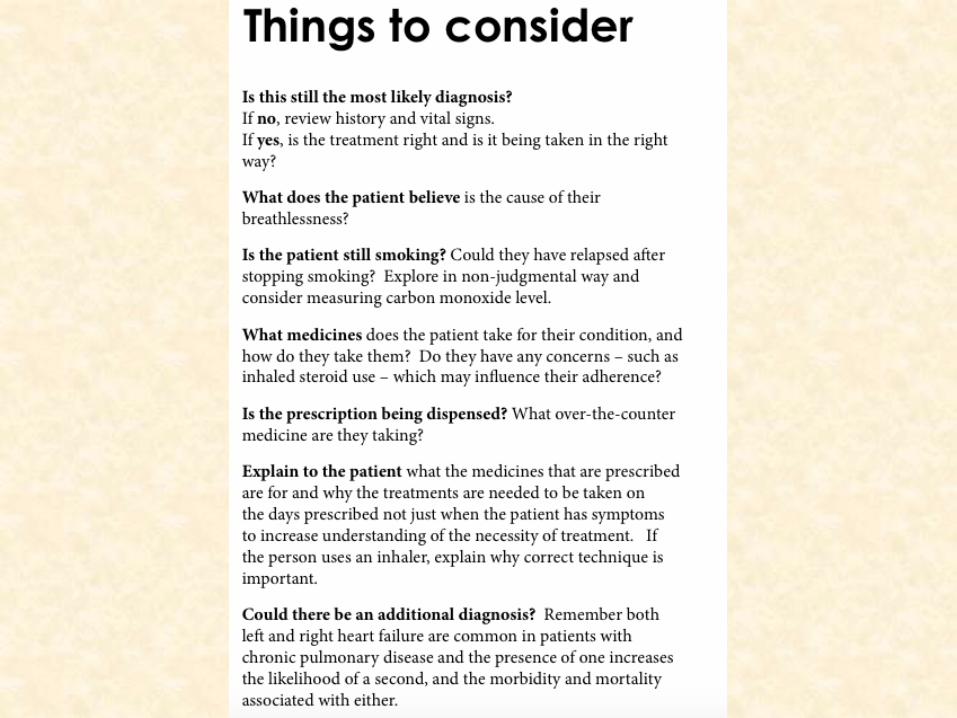
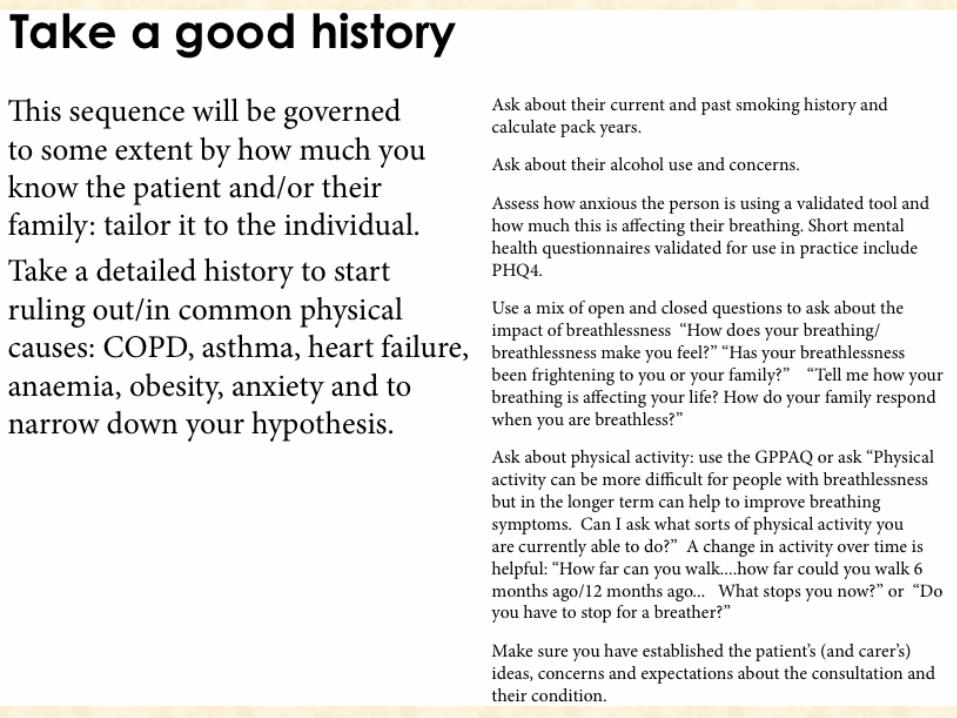
Take a good history
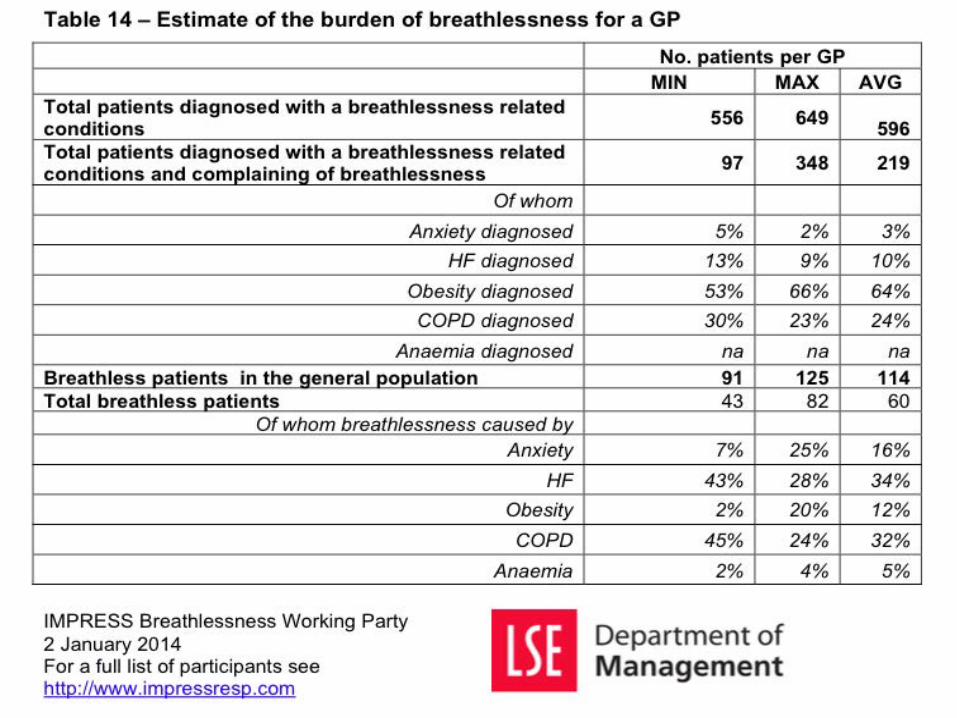
This sequence is governed to some extent by how much you know the paFent and /or their family Take a detailed history to start ruling out /in common physical causes :COPD, asthma, heart failure, anaemia ,obesity , anxiety to narrow down your hypothesis
• Smoking history /pack years • Alcohol use and concerns • Anxiety -‐use MH quesFonnaire PHQ4 • Impact of breathlessness -‐how does it make you feel -‐is it frightening you/your your family -‐how does it affect your life -‐how do your family respond • Physical acFvity -‐what sorts of physical acFvity -‐has this changed over Fme -‐what stops you Establish pa8ent/family ideas, concerns and expecta8ons
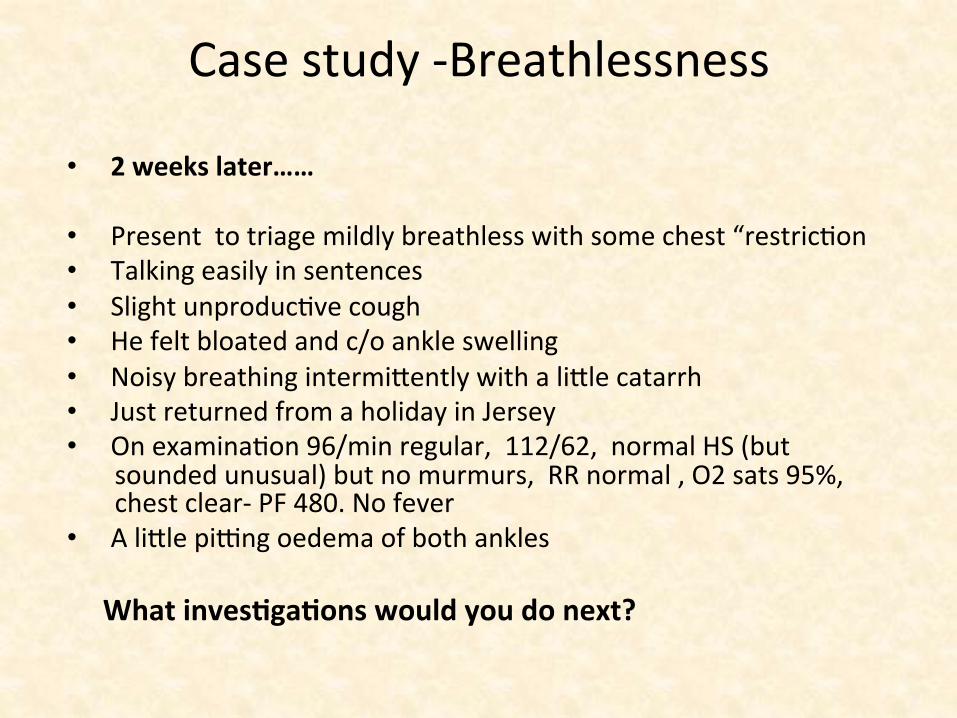
Case study -‐Breathlessness
• 2 weeks later…… • Present to triage mildly breathless with some chest “restricFon • Talking easily in sentences • Slight unproducFve cough • He felt bloated and c/o ankle swelling • Noisy breathing intermijently with a lijle catarrh • Just returned from a holiday in Jersey • On examinaFon 96/min regular, 112/62, normal HS (but
sounded unusual) but no murmurs, RR normal , O2 sats 95%, chest clear-‐ PF 480. No fever
• A lijle pimng oedema of both ankles
What inves8ga8ons would you do next?
What inves8ga8ons would you do next ?
• Chest x-‐ray (again?) • ECG • NatriureFc pepFde tesFng (if available) • D Dimer • Troponin T • All of those above • All except D dimer & Trop T • None of the above opFons
….inves8ga8ons undertaken…
• Chest x-‐ray • ECG • NatriureFc pepFde tesFng (if available)
• D Dimer • Troponin • All of these • All of these except D dimer and Troponin T • None of the other opFons
Results of invesFgaFons
• D Dimer raised at 1.1 ugFEU/ml (>0.35 =posiFve ) • Trop T raised 35ng/L (>30 raised) • Chest x-‐ray reported as showing some increased bronchovascular markings with borderline cardiomegaly but no pleural effusion
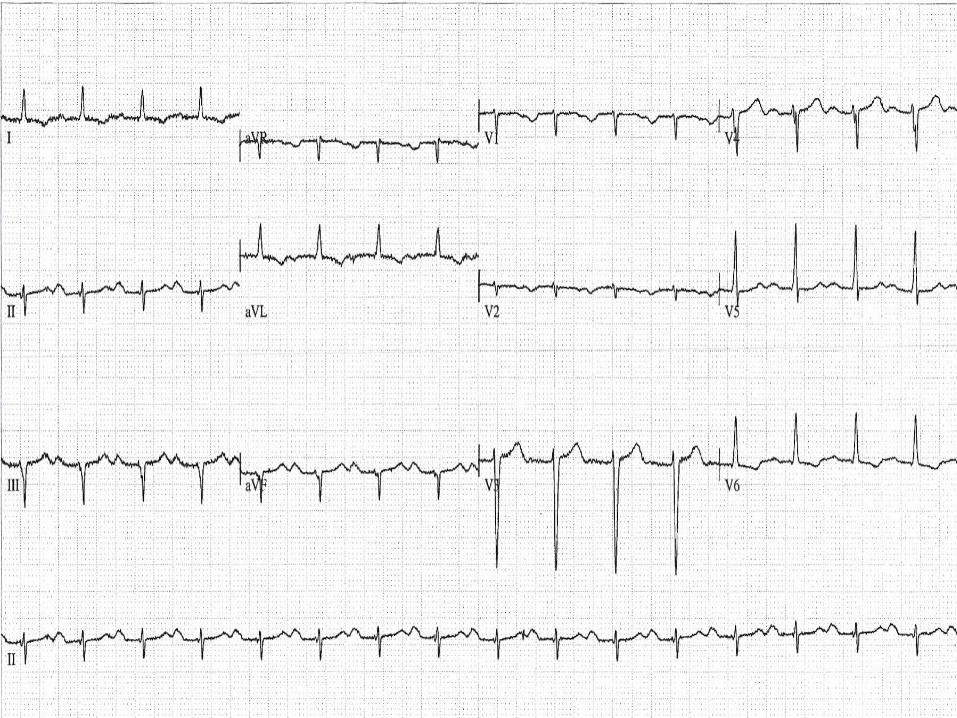
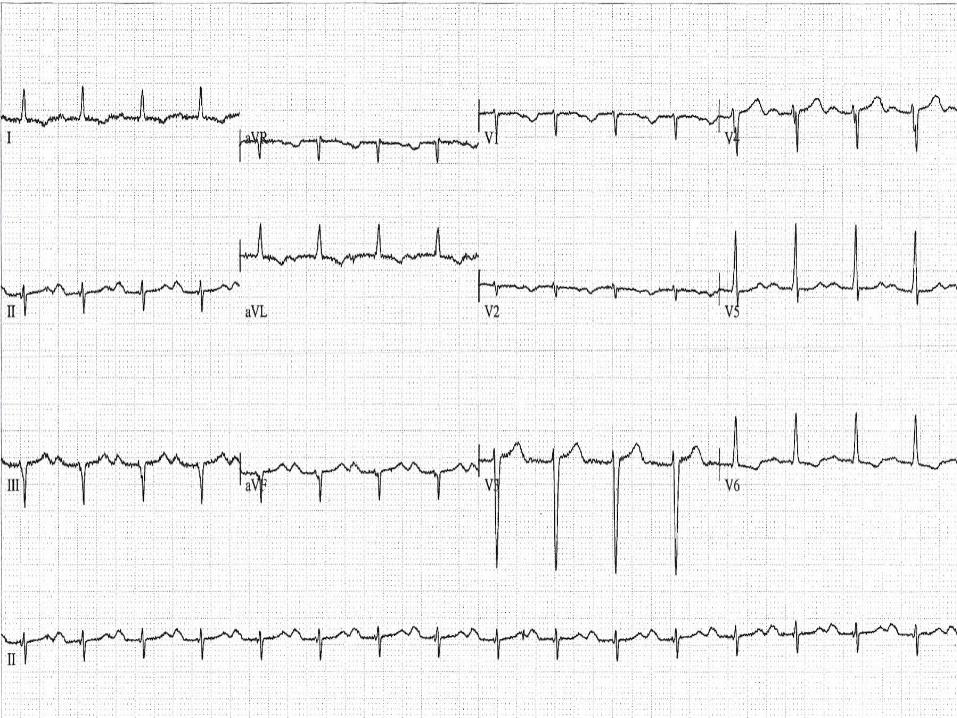
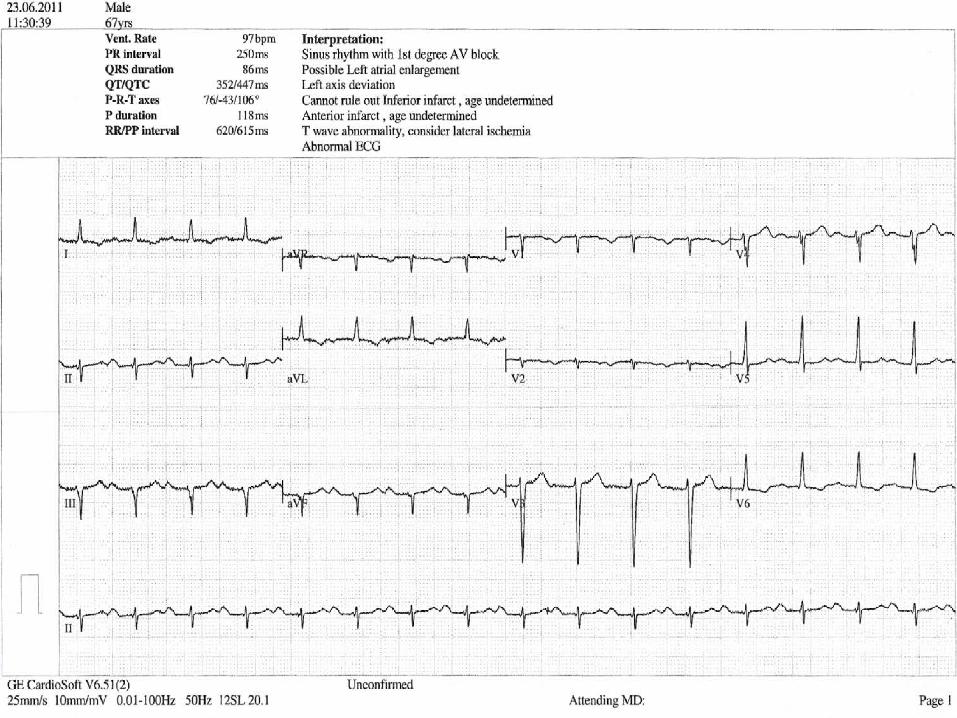
• eGFR40 • ECG …as follows
…and guess who is on call that aOernoon!!!!!!

What did I do next?
What did I do next • Leave for colleague to follow up in the morning as the results
were reassuring. • Given the results admit the paFent to hospital as an
emergency ( I have a rehearsal for a concert at 7.30pm) • Phoned the paFent to discuss results and then decide on
further management • Reviewed the paFent in surgery later that evening • Asked the Dr who had seen the paFent what I should do now
What I did next
• Reviewed the paFent in surgery that evening • Asked the Dr who had seen the paFent what I should do now …..well almost !
Case study -‐Primary care • 2 weeks later……Summary • Just returned from a holiday in Jersey (by air) • Present to triage mildly breathless with some chest “restricFon” • Talking easily in sentences • No pleuriFc pain • Slight unproducFve cough • He felt bloated • Noisy breathing intermijently with a lijle catarrh • On examinaFon 96/min regular, 112/62, normal HS (but
sounded unusual) but no murmurs, RR normal , O2 sats 95%, chest clear-‐ PF 480. No fever
• A lijle pimng oedema of both ankles/calfs so] • Raised troponin and D Dimer • CXR -‐bronchovascular markings and borderline CT raFo • ECG -‐SR -‐no acute changes ,non specific abnormaliFes
Salient points
• Not acutely unwell • Several episodes of SOB associated with travel • 45 min flight recently though several long haul flights in
the past 8 weeks with a raised D DImer • No persistent morning cough nor past history of recurrent
chest problems nor pleurisy • No exerFonal chest pain or Fghtness • Raised Trop T • CXR -‐bronchovascular markings& borderline cardiomegaly • ECG -‐SR -‐no diagnosFc changes but abnormal
Examina8on similar to colleague except ……

What are you listening to ?
• Normal splimng of the first heart sound in inspiraFon
• Widely split first heart sound • Widely split second heart sound • Normal heart sounds with mid systolic click • 3rd heart sound • 4th heart sound • 11.30 train from Cheltenham just arriving at Paddington
What are you listening to ?
• Normal splimng of the first heart sound in inspiraFon
• Widely split first heart sound • Widely split second heart sound • Normal heart sounds with mid systolic click • 3rd heart sound • 4th heart sound • 11.30 from Cheltenham just arriving at Paddington
What would you do next ?
• Admit the paFent ?CTPA • Urgent referral to RACPC • Refer for Echocardiogram(?urgently) • Refer Cardiology • Refer
What would you do next ?
• Admit the paFent ?CTPA • Urgent referral to RACPC • Refer for Echocardiogram(?urgently) • Refer cardiology • Ultrasound venography of lower limbs
Fourth heart sound
• VibraFon in the LV wall in late diastole related to forcible le] atrial contracFon into a sFff ,non compliant le] ventricle.
• Low pitched sound best heard at the apex in the le] decubitus posiFon
• Cadence “tennessee” or bababump • Common in le] ventricular hypertrophy (hypertension), HOCM,IHD
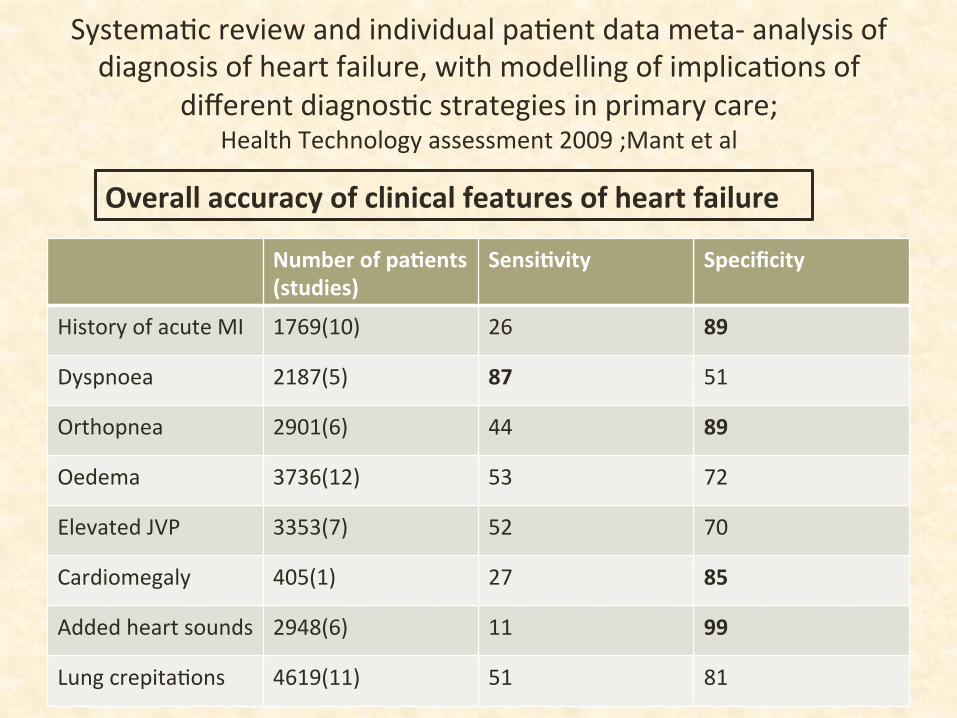
SystemaFc review and individual paFent data meta-‐ analysis of diagnosis of heart failure, with modelling of implicaFons of
different diagnosFc strategies in primary care; Health Technology assessment 2009 ;Mant et al
Number of pa8ents (studies)
Sensi8vity Specificity
History of acute MI 1769(10) 26 89
Dyspnoea 2187(5) 87 51
Orthopnea 2901(6) 44 89
Oedema 3736(12) 53 72
Elevated JVP 3353(7) 52 70
Cardiomegaly 405(1) 27 85
Added heart sounds 2948(6) 11 99
Lung crepitaFons 4619(11) 51 81
Overall accuracy of clinical features of heart failure
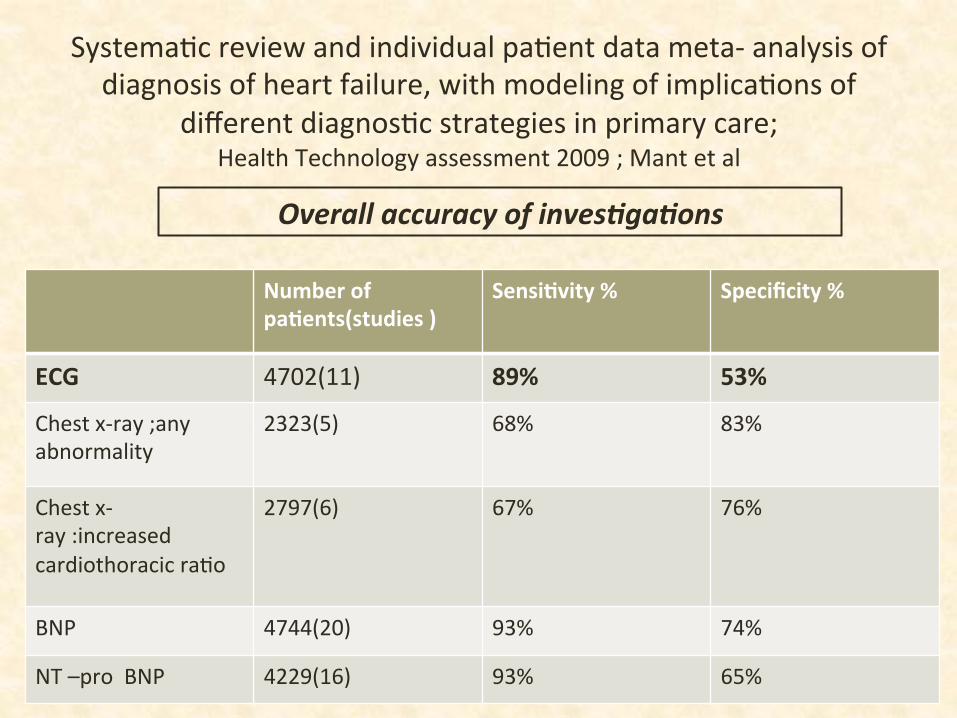
SystemaFc review and individual paFent data meta-‐ analysis of diagnosis of heart failure, with modeling of implicaFons of
different diagnosFc strategies in primary care; Health Technology assessment 2009 ; Mant et al
Number of pa8ents(studies )
Sensi8vity % Specificity %
ECG 4702(11) 89% 53%
Chest x-‐ray ;any abnormality
2323(5) 68% 83%
Chest x-‐ray :increased cardiothoracic raFo
2797(6) 67% 76%
BNP 4744(20) 93% 74%
NT –pro BNP 4229(16) 93% 65%
Overall accuracy of inves0ga0ons
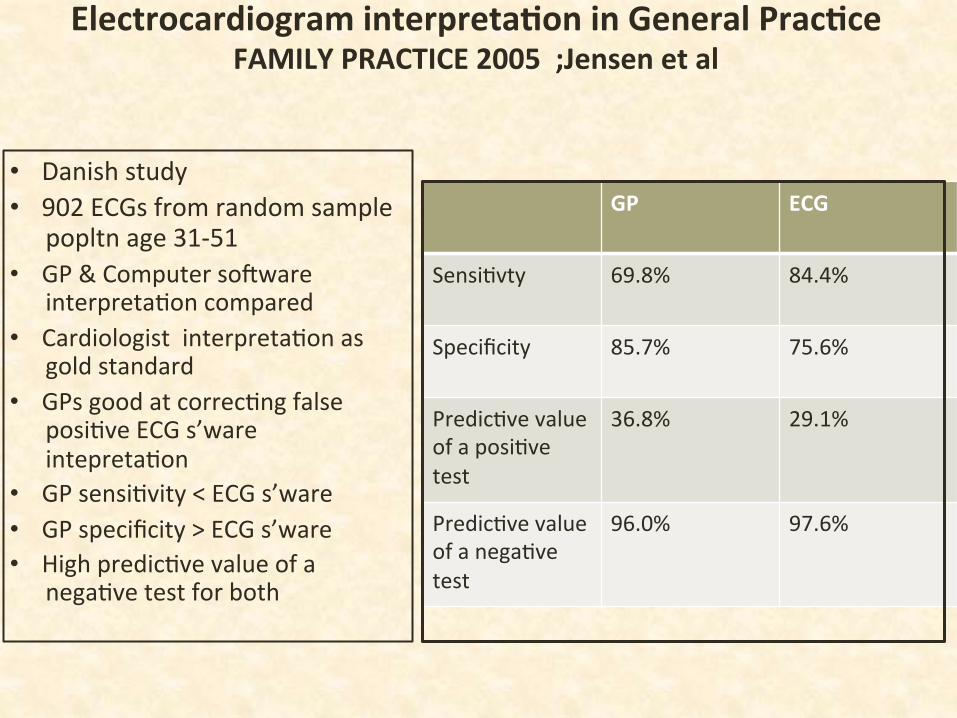
Electrocardiogram interpreta8on in General Prac8ce FAMILY PRACTICE 2005 ;Jensen et al
GP ECG
SensiFvty 69.8% 84.4%
Specificity 85.7% 75.6%
PredicFve value of a posiFve test
36.8% 29.1%
PredicFve value of a negaFve test
96.0% 97.6%
• Danish study • 902 ECGs from random sample
popltn age 31-‐51 • GP & Computer so]ware
interpretaFon compared • Cardiologist interpretaFon as
gold standard • GPs good at correcFng false
posiFve ECG s’ware intepretaFon
• GP sensiFvity < ECG s’ware • GP specificity > ECG s’ware • High predicFve value of a
negaFve test for both
D Dimer
• Raised level indicates fibrin degradaFon due to fibrinolysis of clot or thrombus
• 50% people with DVT not aware they have it • Commoner than MI/Stroke • 2-‐4 Fmes increased risk of symptomaFc DVT for long haul flights of
greater than 4hours duraFon • Ajributable risk up to 8weeks a]er flight • 12% of posiFve D Dimers have VTE • Raised in infecFon, heart failure ,trauma • Good rule out test • Incidence highest in the first 2 weeks a]er flight, increased if there
has been several flights and various other risk factors (very tall)
Likely heart failure….unFl proven otherwise
• Need to establish cause. • Stopped thiazide and started furosemide 40mg daily .
• Referred for echo
Case study
• June 11 On holiday on South Africa Sudden onset of SOB & mild leg oedema 6days a]er arriving Taking Ibuprofen for pseudogout Seen by local GP Blood pressure was raised CXR had showed small amount of fluid at the lung base Δ unclear Started on enalapril and hydrochlothiazide by GP
……fed furosemide 40mg prn by his wife
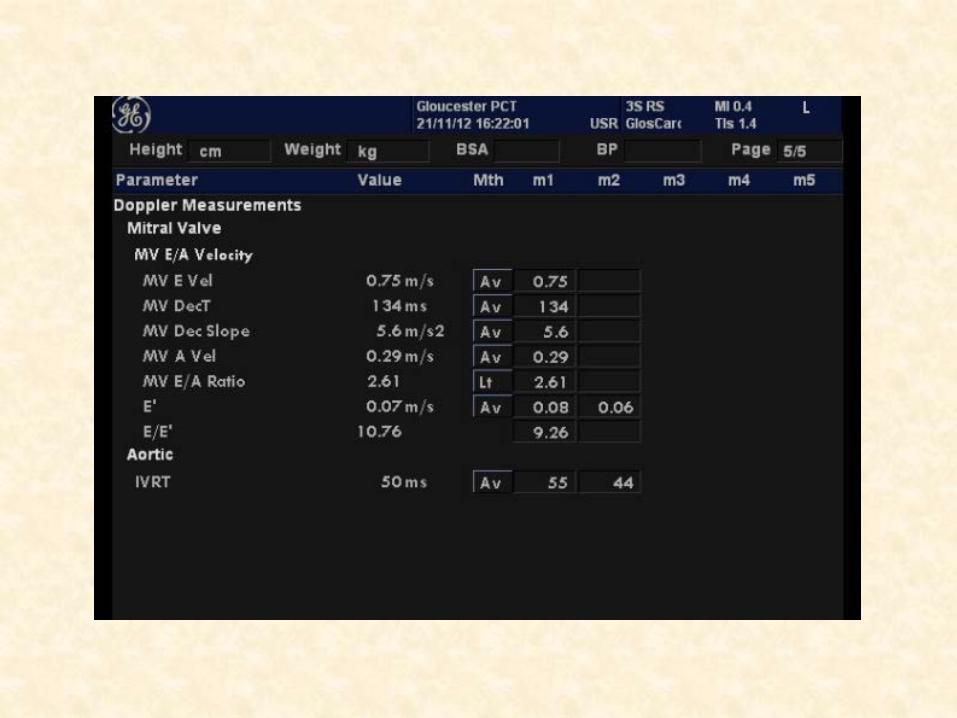
Case Study-‐ Echo summary report
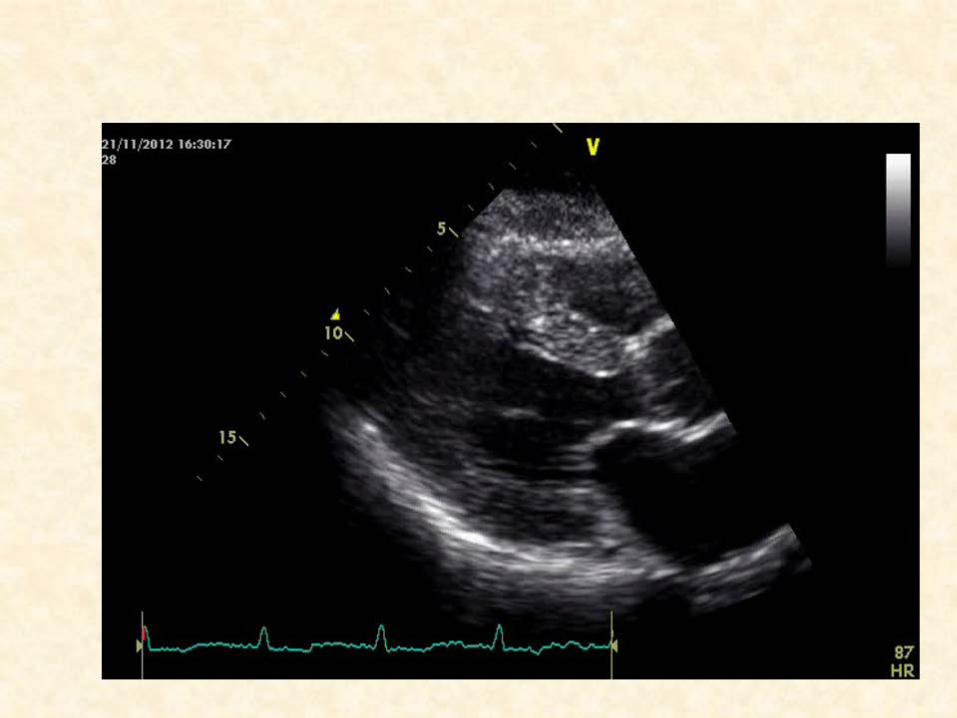
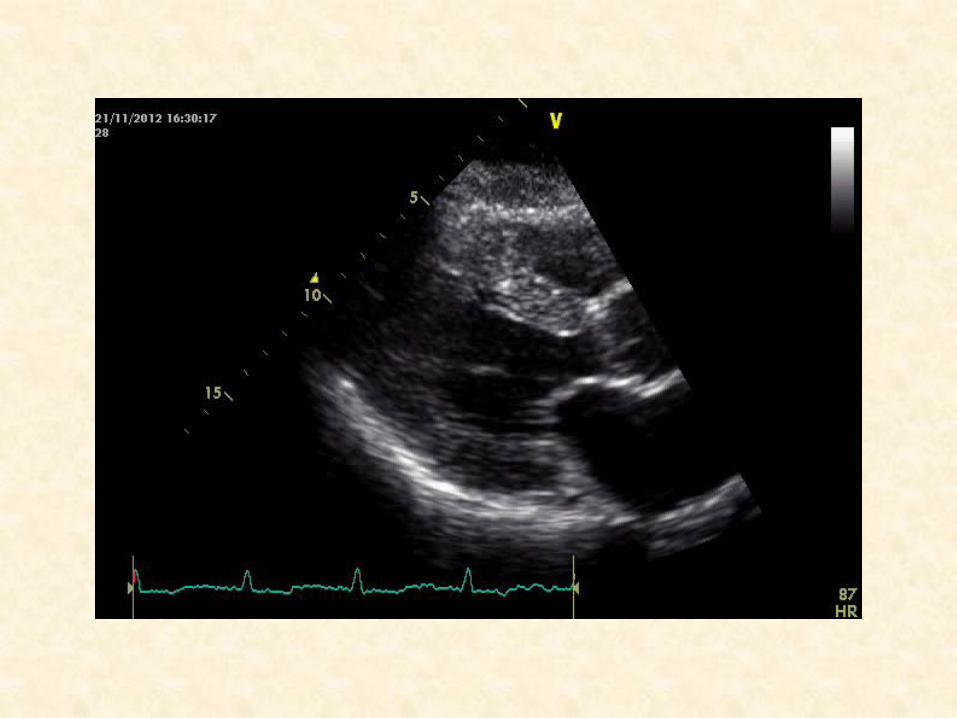
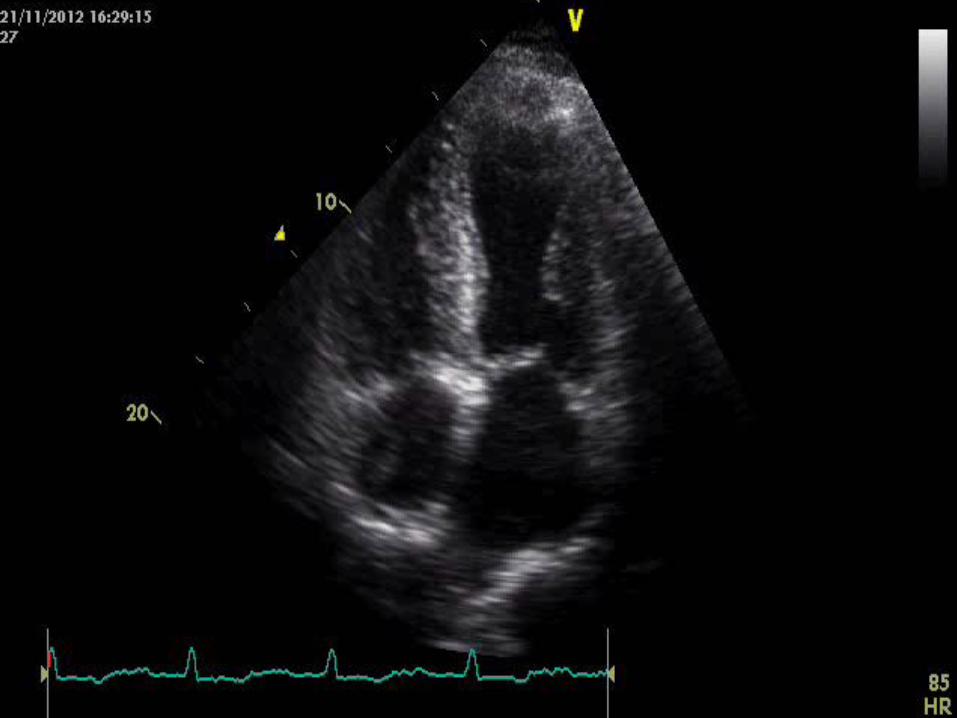
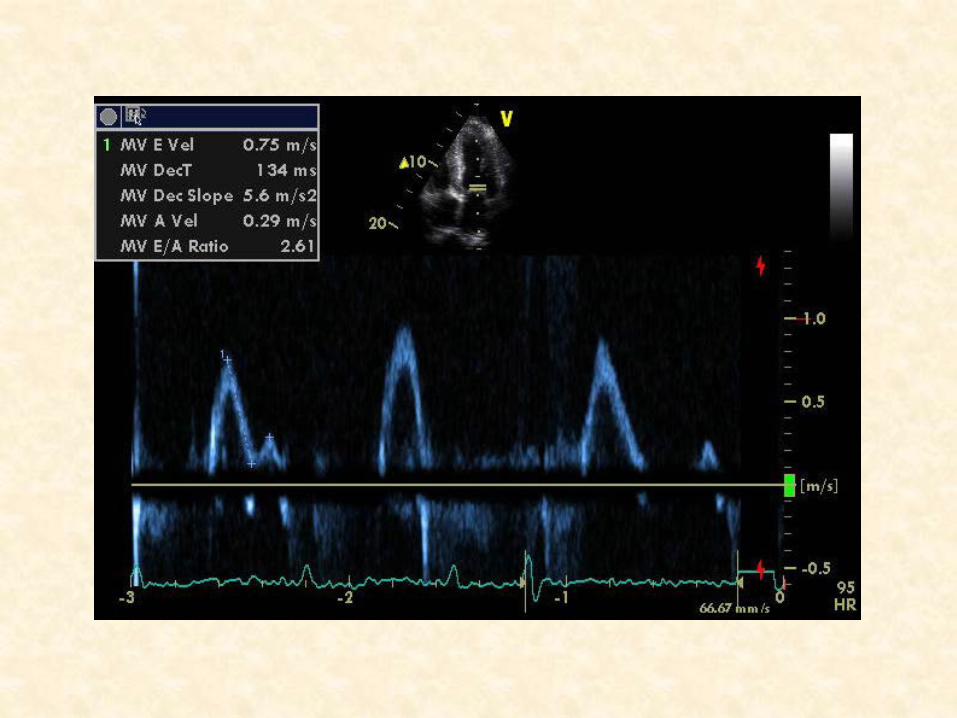
• LV not dilated but mild to moderate LVH Septum shows a “speckled appearance” Systolic funcFon –sFff , moderately impaired ( EF 40-‐45%) No SAM/early AV closure /LVOT obstrucFon Mild thickening AV cusps Impaired diastolic funcFon RVH with impaired systolic funcFon GPSI to review
Case Study 27th July 2011 HFS clinic assessment (GPSI&HFSN) • AsymptomaFc including no SOB • Mild cough • o/e 82/min reg ,128/80, normal heart sounds & 4th HS ,chest clear • No fluid retenFon • Moderate LVSD/impaired diastolic funcFon ?InfiltraFve
cardiomyopathy Management plan • Refer local cardiologist (needs MRI scan ) • Reduce furosemide to 20mg • Stopped enalapril and start ramipril • Stopped Ibuprofen and thiazide • Which drugs in the longer term ? BB/MRA • Follow up HFSN
Case Study 14th September 11 Seen by Cardiologist • AsymptomaFc & no signs of decompensaFon • 4th heart sound confirmed • Warrants further invesFgaFon ?infiltraFve cardiomyopathy -‐coronary angiography -‐MRI scan • No change in management
13th October11 • Coronary angiogram normal • Consider adding procorolan
18th November 11 • MRI scan …………….
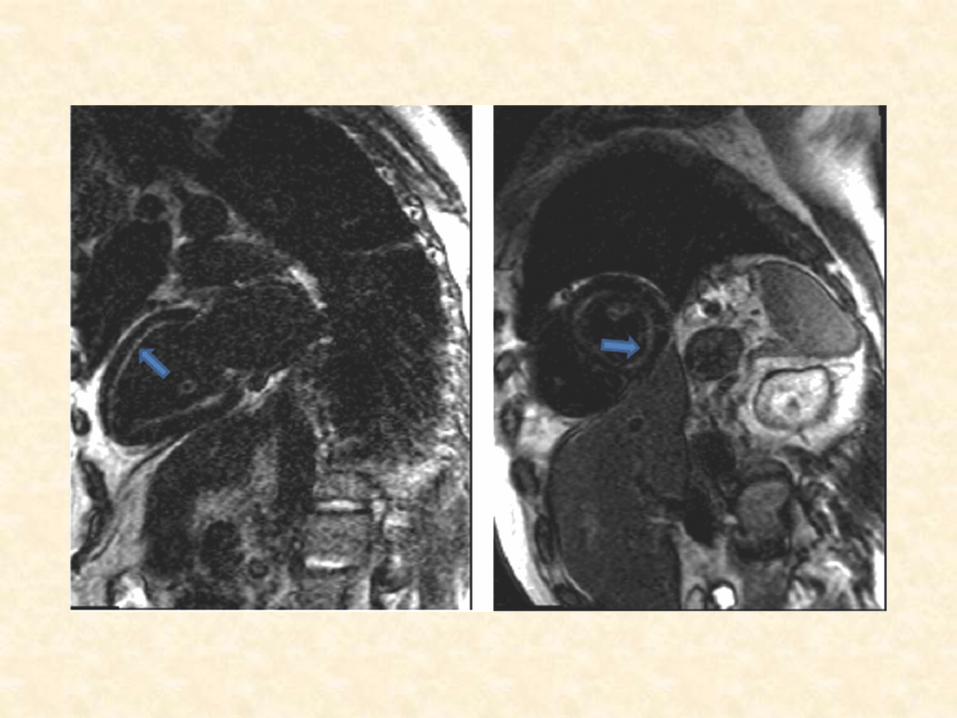
Case study –MRI • Moderate symmetrical LV hypertrophy with elevated LV mass . • Mild systolic dysfuncFon and low-‐normal stroke volume (LVEF51%). • Diffuse ,mostly subendocardial circumferenFal late gadolinium
enhancement in both ventricles and atria. • No SAM/LVOT obstrucFon. • These findings are typical of cardiac amyloidosis
…………..refer Na8onal Amyloidosis Centre
Amyloidosis
• RelaFvely rare mulFsystem disease characterised by the extracellular deposiFon of a normally soluble autologous protein unfolding to become an insoluble β-‐pleated fibrillary sheet deposited in the extracellular Fssues
• 23 differing precursor proteins can cause amyloid • Clinical phenotype varies greatly as does cardiac involvement.
Case study
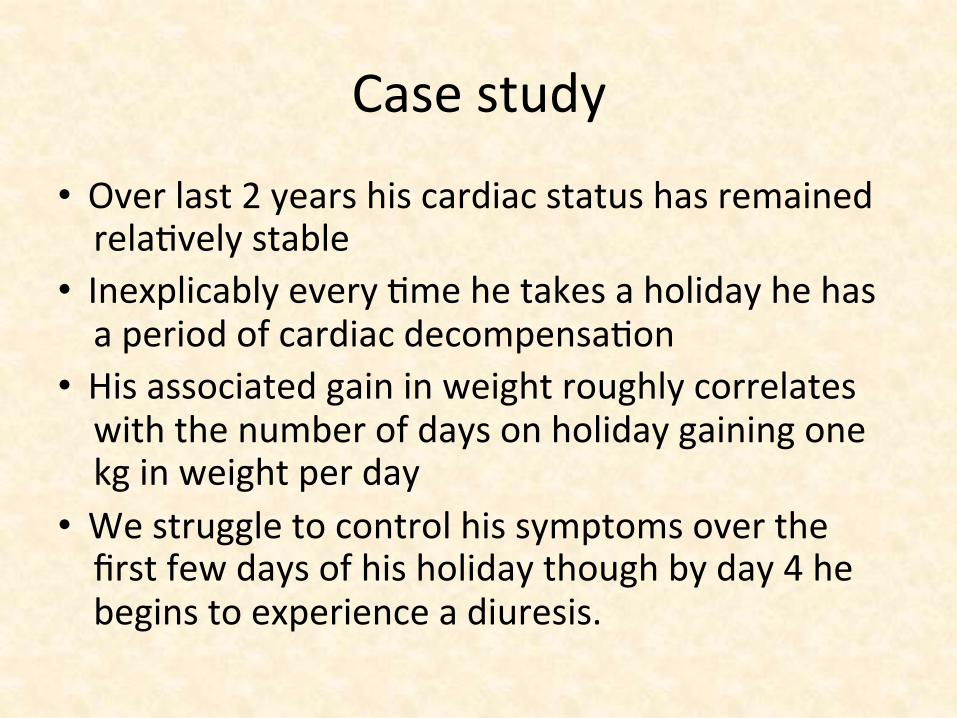
• Over last 2 years his cardiac status has remained relaFvely stable
• Inexplicably every Fme he takes a holiday he has a period of cardiac decompensaFon
• His associated gain in weight roughly correlates with the number of days on holiday gaining one kg in weight per day
• We struggle to control his symptoms over the first few days of his holiday though by day 4 he begins to experience a diuresis.
Learning points
• Good listening skills • Structured and considered approach • Expect the unexpected
Music’s the medicine of the mind John Logan
Thank you ….any quesFons ?
………………….and Bob
Remains asymptomaFc and looking forward to 6 or more years life
THANK YOU
Case Study-‐ Echo summary report
• LV not dilated but mild to moderate LVH Septum shows a “speckled appearance” Systolic funcFon –sFff , moderately impaired( EF 40-‐45%) No SAM/early AV closure /LVOT obstrucFon Mild thickening AV cusps Impaired diastolic funcFon RVH with impaired systolic funcFon GPSI to review RestricFve cardiomyopathy ?amyloid
Case study
26th August 11 HFSN Discussed echo and diagnosis • ^Ramipril 2.5mg bd (no cough) • Furosemide stopped
9th September 11 No decompensaFon Add bisoprolol 1.25mg ……stopped “made him feel awful”

Cardiac Amyloid Main types • Light chain (AL) amyloidosis • Senile systemic amyloidosis (SSA) • Familial amyloidosis (FAP)-‐mutant transthyreFn variants
Others • Secondary amyloid (AA) -‐chronic inflammatory condiFons
including infecFons ) • Hereditary amyloidosis –non transthyreFn variants
(fibrinogen,apolipoprotein and gelsolin) • Isolated Atrial amyloid
Cardiac Amyloidoses Light chain (AL) amyloidosis • Plasma cell dyscrasia • Abnormal paraprotein produced which misfold to cause amyloid • Incidence 6-‐10/million • MulFsystem disease • Macroglossia, perorbital bruising(Panda eyes) • 20% cardiac involvement at the Fme of diagnosis,50% overall • <5%have isolated cardiac involvement • Marked elevaFon of cardiac biomarkers Troponins/NP(if heart
involved = 8mths median survival) • Absence of free light chains make condiFon unlikely • Separate disease enFty from myeloma though may co-‐exist • Bone marrow to confirm and prognosFcate
Senile systemic amyloid (Wild type TransthyreFn)
• Due to a normally soluble protein which is amyloidogenic and leads to fibrillar deposits mainly in the heart though addiFonally found in GI, liver ,spleen and endocrine organs.
• Almost exclusively a disease of men > 65years • Clinical evidence of extra cardiac disease is rare other than carpal
tunnel syndrome which typically preceedes HF by 3-‐5years • Invariably presents with cardiac failure • Autopsy – 20-‐36% over 80,s have evidence of amyloid ?significance • 7% paFents ajending NaFonal Amyloidosis centre • 7 years mean survival from diagnosis • Associated with the H2 haplotype of the Tau gene (Alzheimers) • Consider in the elderly male with LVH & normal ECG voltages • Atrial dysrhythmias & conducFon abnormalites common
Case Study-‐ NaFonal Amyloidosis Centre
25th January 2012 • AsymptomaFc • 83/min reg 102/64 normal HS • No evidence of cardiac decompensaFon • No macroglossia /periorbital bruising • Immunuglobulins normal /no paraproteinaemia • Serum free light chains K/L raFo 1:2 • 24hour protein loss <0.1gm ; no BJP • NT-‐pro BNP 106 pMol/L(raised) • Cardiac hs Troponin T 0.044 mcg/ml(raised) • SAP (serum amyloid P component) scan no visceral organ
uptake( doesn’t show heart ) both quanFtaFve and qualitaFve • Gene sequencing – confirms wild type TTR(excludes familial amyloid
polyneuropathy) • No peripheral neuropathy
Case Study-‐ NaFonal Amyloid centre Summary 1. Very likely cardiac amyloid 2. No detectable plasma cell dyscrasia 3. No extra cardiac amyloid (SAP scan or urinalysis) 4. Wild type TransthyreFn (No FAP) 5. For fat pad biopsy & DPD scan Follow up Fat pad biopsy –negaFve • 99mTc-‐DPD (isotope tracer more specific for cardiac amyloid) –
posiFve at Grade2/3 • Conclusion Almost certainly senile systemic amyloid, No cardiac biopsy indicated unless significant clinical change
Case Study 18th May 12 GP trainee • SOBOE a]er short break in Guernsey • mild ankle oedema ,gained at least 3kg in weight • no orthopnea /PND • 76/min reg ,110/80, normal HS , absent 3rd /4th HS , chest clear ,O2
sats 99% on air • Raised JVP , mild bilateral ankle oedema,so] calfs • eGFR 62,normal electrolytes,LFTS, FBC • Discussed with NAC -‐ restart furosemide 40mg daily started 25th May 12 GPSI • SOB sejled; lost 5kg in weight ; no signs fluid retenFon • Furosemide reduced to 20mg and to conFnue Fll review 17th July 12 GPSI • Post holiday in S Africa • Slightly more SOB;minimal peripheral oedema ;weight ^ 2.5kg to
88.5kg • 76/min 112/76 • ConFnue furosemide 20mg & add spironolactone 25mg
Case study 27th July12 GP(SI) • Feels drained otherwise no significant symptoms • No significant clinical findings;weight 85.5 kg • eGFR 55,normal electrolytes • Stop furosemide 18th September12 NAC • Presumed SSA • Good reponse to diureFcs and presently well compensated • Avoid BB or Procorolan • Echo/ECG unchanged • Rpt DPD scan in 1year • Future decompensaFon –for regular diureFcs • ?novel treaments in future which will require cardiac biopsy –
Tafamidis or anFsense oligonucleoFde therapy
Amyloidosis Treatment –suppor8ve • Standard heart failure treatments –limited benefit / ?
detrimental related to postural hypotension,renal fctn • Maintain filling pressures –judicious use of diureFcs • RAAS drugs/BB have no evidence for use /non use • Heart rate dependent cardiac output =BB may be poorly
tolerated • Avoid Digoxin and CCB as may accumulate in amyloid Fssue
causing toxicity Specific • Amyloid inhibitors-‐ precursor protein stabilisers -‐ diflusinal/
tafamadis in SSA • Chemotherapy -‐Melphalan/bone marrow transplant • Monoclonal anFbody rx –anF SAP anFbody • Cardiac transplantaFon (AL & SSA) • Liver transplantaFon in ATTR
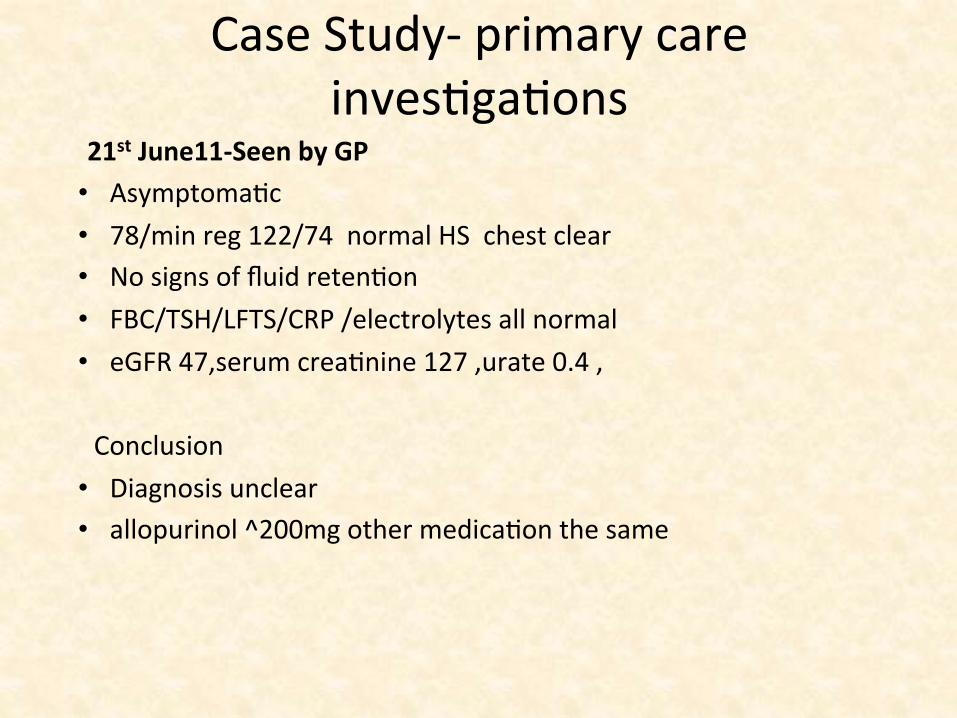
Case Study-‐ primary care invesFgaFons
21st June11-‐Seen by GP • AsymptomaFc • 78/min reg 122/74 normal HS chest clear • No signs of fluid retenFon • FBC/TSH/LFTS/CRP /electrolytes all normal • eGFR 47,serum creaFnine 127 ,urate 0.4 ,
Conclusion • Diagnosis unclear • allopurinol ^200mg other medicaFon the same
Case study
• June 11 On holiday on Mozambique/Zimbabwe border Sudden onset of SOB & orthopnea & leg oedema Taking Ibuprofen for pseudogout Seen by local GP in Zimbabwe CXR had showed large heart and small pleural effusion Δ probable heart failure Started on enalapril and hydrochlothiazide by GP ……fed furosemide 40mg prn by his wife
Case Study-‐ primary care 2 weeks later…… Present to triage mildly breathless with some chest “restricFon” Talking easily in sentences Slight unproducFve cough He felt bloated Noisy breathing intermijently with a lijle catarrh Just returned from a holiday in Jersey On examinaFon96/min regular 112/62, normal HS (sounded unusual) but no murmurs, RR normal , O2 sats 95%, chest clear-‐ PF 450 A lijle pimng oedema of both ankles What happened next ?
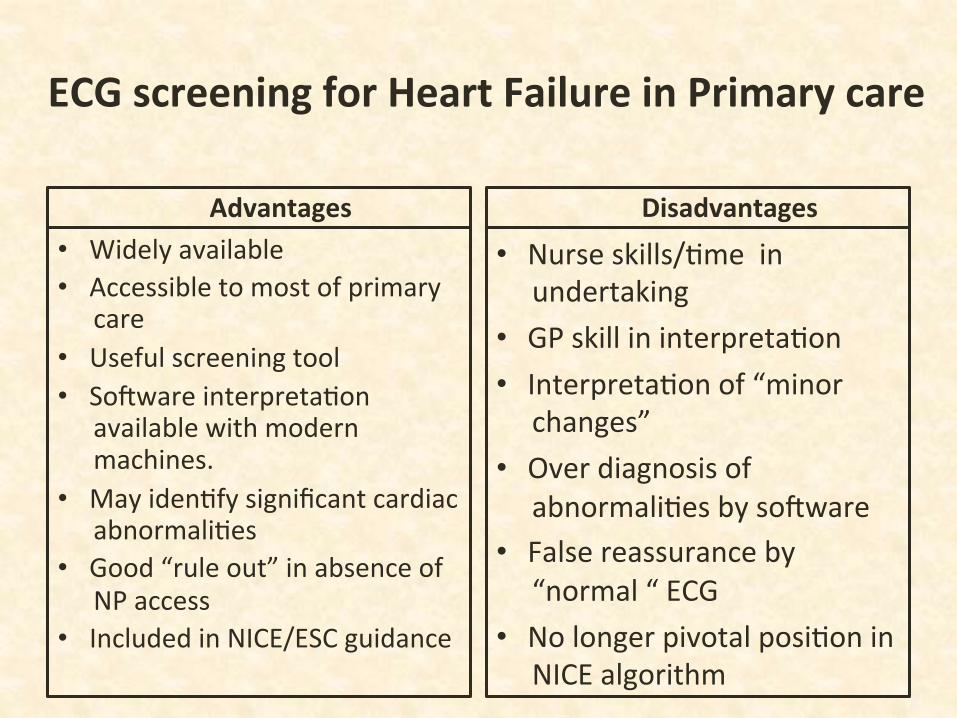
ECG screening for Heart Failure in Primary care
Advantages • Widely available • Accessible to most of primary
care • Useful screening tool • So]ware interpretaFon
available with modern machines.
• May idenFfy significant cardiac abnormaliFes
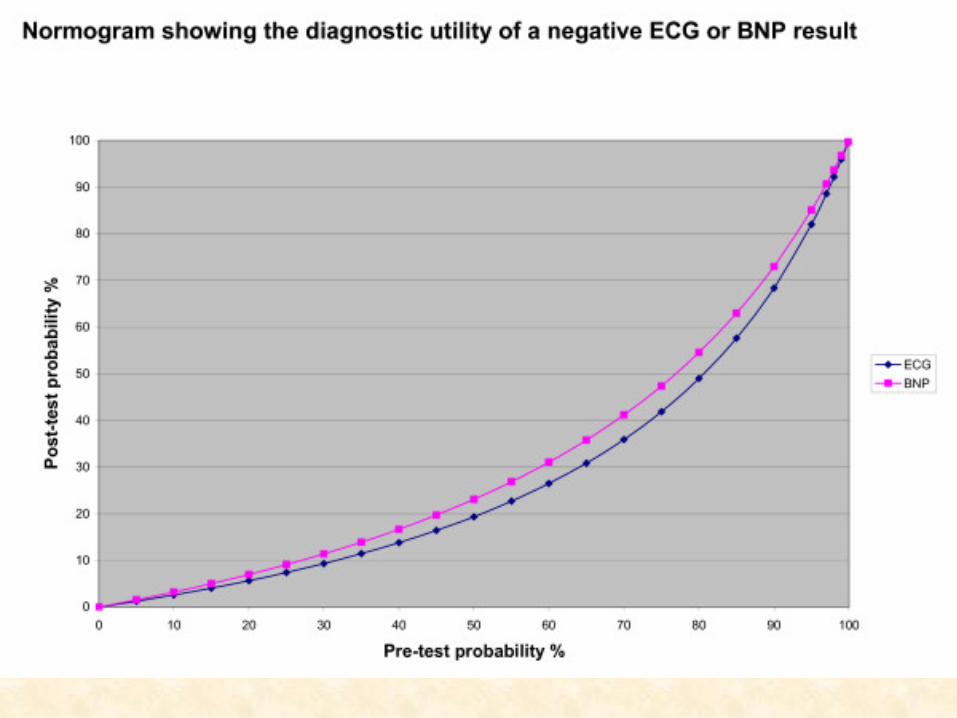
• Good “rule out” in absence of NP access
• Included in NICE/ESC guidance
Disadvantages
• Nurse skills/Fme in undertaking
• GP skill in interpretaFon • InterpretaFon of “minor
changes” • Over diagnosis of
abnormaliFes by so]ware • False reassurance by
“normal “ ECG • No longer pivotal posiFon in
NICE algorithm
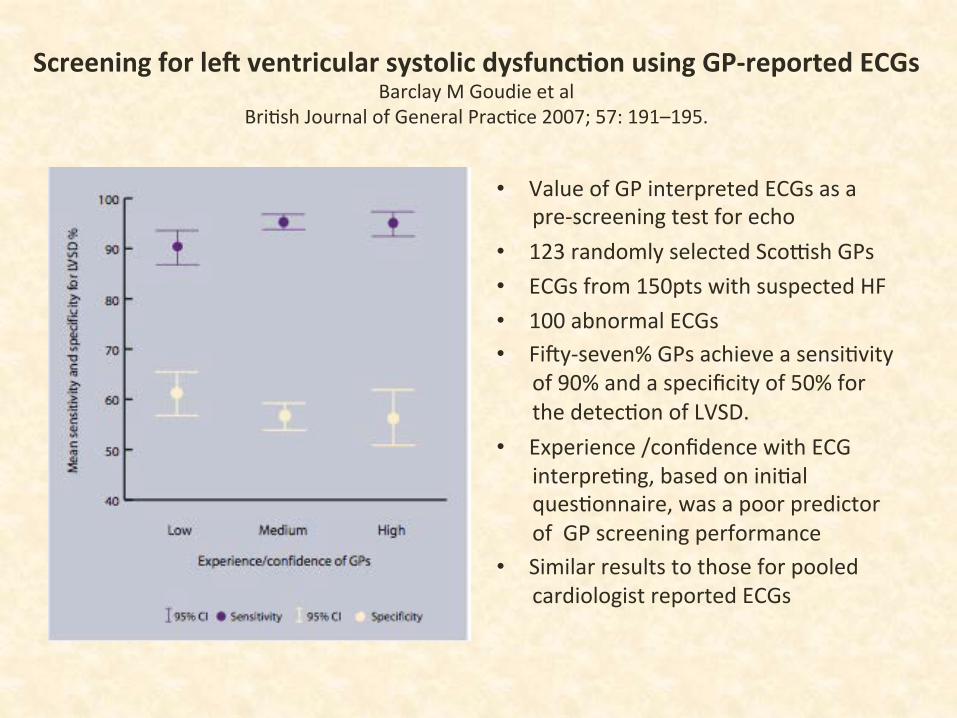
Screening for leO ventricular systolic dysfunc8on using GP-‐reported ECGs Barclay M Goudie et al
BriFsh Journal of General PracFce 2007; 57: 191–195.
• Value of GP interpreted ECGs as a pre-‐screening test for echo
• 123 randomly selected Scomsh GPs • ECGs from 150pts with suspected HF • 100 abnormal ECGs • Fi]y-‐seven% GPs achieve a sensiFvity
of 90% and a specificity of 50% for the detecFon of LVSD.
• Experience /confidence with ECG interpreFng, based on iniFal quesFonnaire, was a poor predictor of GP screening performance
• Similar results to those for pooled cardiologist reported ECGs
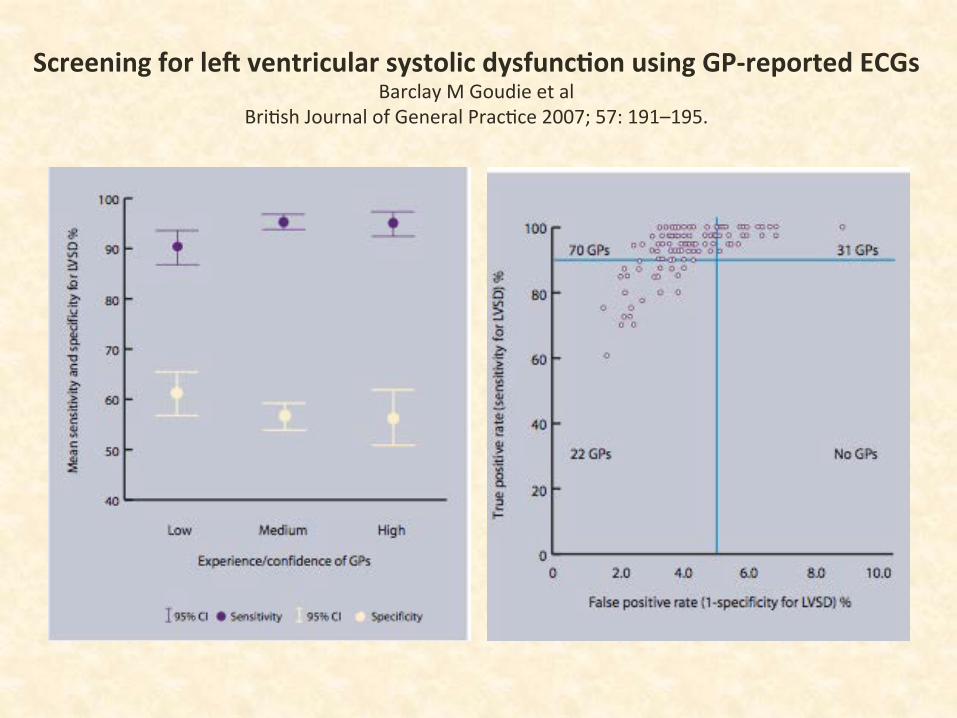
Screening for leO ventricular systolic dysfunc8on using GP-‐reported ECGs Barclay M Goudie et al
BriFsh Journal of General PracFce 2007; 57: 191–195.
Case study
68 year old ReFred mining engineer (precious metals) Lived and worked in South Africa for many years Lives with wife Fit and well unFl …………………..