Embed Size (px)
Citation preview

H E C FORUM © 2002 Kluwer Academic Publishers. 2002; 14(2):132-147. Printed in The Netherlands.
132
PROBLEMS IN CARING FOR CRITICALLY AND TERMINALLY ILL PATIENTS: PERSPECTIVES OF PHYSICIANS AND NURSES
ALLAN S. BRETT, M.D.
Introduction
In recent years, numerous developments have focused attention on medical decisionmaking for critically and terminally ill patients. Traditionally, such decisionmaking was confined largely to the relationship between the patient and physician. While nurses and other non-physician healthcare providers have long been indispensable in providing medical care near the end of life, they were considered to play roles subordinate to that of the physician. Moreover, while the medical care of critically and terminally ill patients usually occurs in hospitals and nursing homes, those institutions traditionally had little direct input into end-of-life decision making.
The passage of the Patient Self-Determination Act in 1990 was perhaps the first organized challenge to the idea that institutions should not meddle in planning care at the end of life. Among other things, this federal statute mandated that hospitals and other healthcare institutions would make information about advance directives available to patients at the time of admission (1). Although this act has been responsible for only modest changes in end-of-life care at most healthcare institutions (2)(3), its appearance did suggest that physicians, acting alone, were not attending adequately to certain aspects of medical decision-making for critically and terminally ill patients.
Several years later, a widely publicized multicenter study (the Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments, or SUPPORT) documented major problems in the provision of medical care at the end of life (4). The study included several interventions – organized in part at the institutional level – designed to overcome those problems. For example, quantitative information on patients’ prognoses was made available to attending physicians at regular intervals; research nurses interviewed patients and family members about their treatment preferences and communicated those preferences to physicians; and the same nurses served as resources to enhance understanding and to facilitate communication and planning. According to a series of study endpoints chosen by the investigators, the SUPPORT interventions were deemed largely ineffective. However, the failure of the SUPPORT study did not

Problems in Caring for Critically and Terminally Ill Patients 133
dampen enthusiasm for the idea that effective end-of-life care should be an institutional enterprise, extending beyond the traditional patient-physician model of decision-making.
The transition from a traditional patient-physician model to a broader institutional model implies, among other things, more explicit attention to the interplay between the various healthcare professions. The underlying assumption is that healthcare workers representing different professions will not necessarily focus attention on the same problem, or will perceive the same problem in a somewhat different light. It follows that we will not understand institutional behavior fully without understanding the similarities and differences in the perspectives of key healthcare professionals that constitute the institution. In the case of end-of-life care in the hospital setting, it is particularly important to compare and contrast the perspectives of physicians and nurses, the professionals most intimately involved in caring for critically and terminally ill patients.
The objective of this study was to determine the most important ethical and psychosocial problems that hospital-based nurses, attending physicians, and resident physicians perceive in caring for critically and terminally ill patients, and to determine whether the concerns of nurses and physicians differ systematically. The data for this analysis were derived from a survey conducted as a part of the “Decisions Near the End of Life” project. Methods
The “Decisions Near the End of Life” project was a national initiative to enhance understanding of the ethical issues surrounding decision making for terminally or critically ill patients in hospitals and nursing homes. In an early phase of the project, conducted in 1989-1990, clinical care providers at four urban acute care teaching hospitals in the United States (a municipal hospital and three private hospitals) were exposed to a curriculum consisting of lectures and small group discussions. Before the educational program began, a questionnaire was circulated to clinically active nurses, physicians, and other caregivers at these institutions. One part of the questionnaire consisted of 65 “closed-ended” questions (e.g., using yes-no and Likert scale formats) to collect demographic data and to assess attitudes, knowledge, and perceptions about the ethical and legal aspects of caring for critically ill patients. For example, many questions explored participants’ views on withdrawing and withholding life-sustaining interventions, institutional policies regarding such matters, and communication and

134 A.S. Brett
disagreements among caregivers. The findings from that part of the questionnaire have been published elsewhere (5).
In contrast to the closed-ended questions, the following open-ended question was posed at the end of the questionnaire: “What are the three most pressing issues or problems you currently face involving the care of the critically and terminally ill?” Respondents wrote narrative answers to this question in a blank space subdivided into three areas, to accommodate up to three responses. The themes of the previous portion of the questionnaire prompted respondents to interpret this open-ended question as referring to ethical and psychosocial (and not strictly biomedical) concerns.
Given the ineffectiveness of the SUPPORT intervention (implemented jointly by nurses and physicians), the recent surge of interest in organizational ethics (with its interprofessional emphasis) (6), and a recently voiced perception of a “troubled partnership” between physicians and nurses (7), it seemed appropriate to revisit the “Decisions Near the End of Life” database and analyze this open-ended portion of this survey, in order to determine whether there are systematic differences in the perspectives of nurses and physicians. In the current study, I performed a content analysis of the narrative responses to the open-ended question by nurses and physicians at the four hospitals.
The primary analysis was a categorization of each narrative response. To develop a sense of the principal themes and concerns expressed by respondents, a research assistant and I each read several hundred questionnaires chosen randomly from the four hospitals, and devised a list of 17 thematic categories to capture all responses. Using these thematic categories to code a random sample of 50 responses simultaneously, we achieved perfect agreement for 82% of the sample. The two investigators then coded all responses (each coded half the questionnaires). Finally, to determine the stability of agreement over time, we simultaneously coded 50 responses near the end of the formal coding exercise, with 90% inter-rater agreement.
We next aggregated the 17 categories into the following six conceptually coherent broader categories – problems with communication, lack of respect for the patient as person, unrealistic expectations, uncertainty, inappropriate care, and external factors (Table 1).

Problems in Caring for Critically and Terminally Ill Patients 135
Table 1. Primary and aggregated conditions
Primary Categories
Aggregated Categories
1. Communication among providers 2. Communication between providers and
patients/families 3. Communication within families 4. Decision-making authority
Communication
5. Respect for patient Respect for patient 6. Unrealistic expectations among providers 7. Unrealistic expectations among
patient/families Expectations
8. Uncertainty (general) 9. Uncertainty (about patient wishes) Uncertainty
10. Inappropriate care (overtreatment) 11. Inappropriate care (undertreatment) Inappropriate care
12. Economic factors 13. Legal factors 14. Work environment 15. Need for guidelines and policy 16. Morale
External factors
17. Other In a second analysis, we tabulated the frequency with which respondents noted the following specific interventions to be problematic: cardiopulmonary resuscitation (CPR), including orders not to resuscitate (DNR orders); intubation or mechanical ventilation; nutrition or hydration; and pain control.
Descriptive statistics included the proportion of subjects responding in each category, and a breakdown of responses by profession (nurse, staff physician, resident). Differences in responses by profession were assessed using chi-square analysis with a two-tailed p level of 0.05 or less indicating significance. All analyses were performed using the PC version of SPSS.

136 A.S. Brett
Results
Questionnaires were circulated to 2,169 physicians and nurses at the four institutions, and 1,323 were returned, for a response rate of 61%. Of the 1,323 questionnaires that were returned, the open-ended question was answered in 981 (74%). Demographic characteristics of the respondents are given in Table 2. Compared with subjects who left the open-ended question unanswered, those who completed it were younger, worked as health professionals for fewer years, and cared for a higher percentage of critically and terminally ill patients. Nurses and residents were more likely to respond to this question than staff physicians. Table 2. Characteristics of Participants
Respondents (n=981)
Non-Respondents
(n=342)
P value Number (%), by profession
Nurses 576 (58.7) 168 (49.1) .0005 staff M.D. 297 (30.3) 143 (41.8) resident M.D. 108 (11.0) 31 (9.1) Total 981 (100) 342 (100)
Age in years * 37.7 ± 11.1 40.5 ± 12.0 .000 Years in profession * 12.8 ± 10.3 15.0 ± 11.2 .001 Years at institution * 8.5 ± 8.6 9.6 ± 8.8 .050 % patients critically ill 28.0 ± 26.8 16.6 ± 22.9 .000 & patients who die * 11.2 ± 13.3 6.2 ± 10.6 .000 * Mean, ± SD
Problems in Caring for Critically and Terminally Ill Patients 137
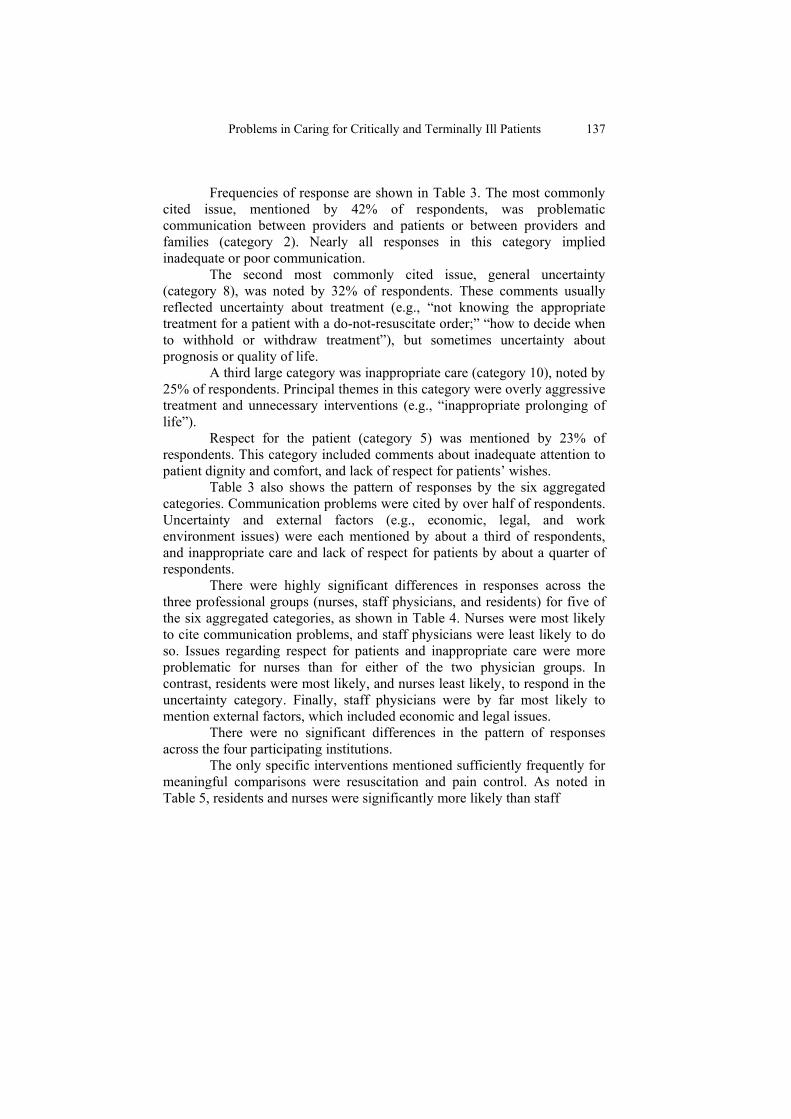
Frequencies of response are shown in Table 3. The most commonly
cited issue, mentioned by 42% of respondents, was problematic communication between providers and patients or between providers and families (category 2). Nearly all responses in this category implied inadequate or poor communication.
The second most commonly cited issue, general uncertainty (category 8), was noted by 32% of respondents. These comments usually reflected uncertainty about treatment (e.g., “not knowing the appropriate treatment for a patient with a do-not-resuscitate order;” “how to decide when to withhold or withdraw treatment”), but sometimes uncertainty about prognosis or quality of life.
A third large category was inappropriate care (category 10), noted by 25% of respondents. Principal themes in this category were overly aggressive treatment and unnecessary interventions (e.g., “inappropriate prolonging of life”).
Respect for the patient (category 5) was mentioned by 23% of respondents. This category included comments about inadequate attention to patient dignity and comfort, and lack of respect for patients’ wishes.
Table 3 also shows the pattern of responses by the six aggregated categories. Communication problems were cited by over half of respondents. Uncertainty and external factors (e.g., economic, legal, and work environment issues) were each mentioned by about a third of respondents, and inappropriate care and lack of respect for patients by about a quarter of respondents.
There were highly significant differences in responses across the three professional groups (nurses, staff physicians, and residents) for five of the six aggregated categories, as shown in Table 4. Nurses were most likely to cite communication problems, and staff physicians were least likely to do so. Issues regarding respect for patients and inappropriate care were more problematic for nurses than for either of the two physician groups. In contrast, residents were most likely, and nurses least likely, to respond in the uncertainty category. Finally, staff physicians were by far most likely to mention external factors, which included economic and legal issues.
There were no significant differences in the pattern of responses across the four participating institutions.
The only specific interventions mentioned sufficiently frequently for meaningful comparisons were resuscitation and pain control. As noted in Table 5, residents and nurses were significantly more likely than staff

138 A.S. Brett
Table 3. Classification and frequency of responses Primary Category
Percentage of
respondents
Aggregated
category
Percentage of
respondents 1. Communication among
providers 9
2. Communication between providers and patients/families
42
3. Communication within families 2
4. Decision-making authority 8
Communication 52
5. Respect for patient 23 Respect for patient 23
6. Unrealistic expectations among providers 4
7. Unrealistic expectations among patient/families 5
Expectations 9
8. Uncertainty (general) 32 9. Uncertainty (about patient
wishes) 4 Uncertainty 34
10. Inappropriate care (overtreatment) 25
11. Inappropriate care (undertreatment) 2
Inappropriate care 26
12. Economic factors 14 13. Legal factors 10 14. Work environment 11 15. Need for guidelines and
policy 4
16. Morale 3
External factors 37
17. Other 23 Other 23 * Sum of percentages exceeds 100% because respondents were permitted up to three responses. A given percentage for an aggregated category may be less than 100% of sum of percentages for component primary categories because some respondents gave two responses within an aggregated category.
Problems in Caring for Critically and Terminally Ill Patients 139
Table 4. Responses (by profession) for aggregated categories (%)* Category Nurses Staff M.D.s Residents P Value Communication
57
44
51
.0015
Respect for Patients 30 14 18 .0000 Expectations 8 10 7 .5928 Uncertainty 28 40 52 .0000 Inappropriate care 31 18 19 .0000 External factors 33 48 25 .0000 * Sum of percentages for each profession exceeds 100% because respondents were permitted up to 3 responses. Table 5. Interventions mentioned (%) (by profession) Intervention Nurses Staff M.D.s Residents P Value Resuscitation
34
22
38
.0002
Pain control 17 8 7 .0000 physicians to mention problems surrounding cardiopulmonary resuscitation (e.g., “having to ‘code’ patients with no DNR orders and little hope”). Pain control was viewed as problematic by nurses significantly more often than by the two physician groups. Discussion
In this study, I used the open-ended responses of physicians and nurses to identify their perceptions of problems in caring for critically ill patients. These responses could be assigned reliably to 17 primary categories, which could be further aggregated into six broader, conceptually coherent categories. The results – with nurses more likely to cite problems with communication and respect for patients, and physicians more likely to highlight uncertainty and external factors – tend to support traditionally held distinctions between the professional roles of nurses and physicians. That is, the nursing role emphasizes care and advocacy (8)(9), processes which

140 A.S. Brett
depend heavily on personal relationships with patients, while the physician role emphasizes cure and rationality, with greater attention to scientific than relational processes. However, these distinctions should not be overstated. Although the large sample size made it possible to find highly statistically significant differences in responses across the professions, the differences between staff physicians and nurses did not exceed 16 percentage points for any category.
A large percentage of each professional group described problems with communication. Most of these responses indicated inadequate communication between healthcare providers and patients or families, but not among the providers themselves. The higher frequency among nurses than physicians may result from nurses’ more sustained contact with hospitalized patients and families. Alternatively, nurses might be dissatisfied with their degree of participation in discussions between physicians and patients. Finally, nurses might have a different threshold than physicians for perceiving certain types of communication as problematic, as a result of differences in training or role perceptions.
Similarly, respect for patients was more problematic for nurses than for physicians. In most hospital settings, nurses bear the immediate responsibility for attending to the comfort of patients, and nurses usually witness the suffering of critically ill patients more intimately and continuously than physicians. While nurses’ responses might in part reflect a sense that their physician counterparts are not appropriately sensitive to the patient's experience of illness, both physicians’ and nurses’ responses in this category might represent an acknowledgement of their own dehumanizing or insensitive behaviors.
A third category cited more frequently by nurses than by physicians was inappropriate care. Most of these responses reflected a value judgment that patients were “overtreated” near the end of life; for example, results from the closed-ended part of this survey indicated that 55% of providers were concerned about overtreatment, but only 12% about undertreatment (5). The predominance of nurses in this category may be an extension of their concern with respect for patients. That is, they may view the inappropriate use of life-sustaining interventions as eroding the dignity of patients. Moreover, nurses may believe that their care-giving role is frustrated by having to implement physician-initiated interventions that appear futile or even inhumane (10). In contrast, physicians were significantly more likely than nurses to consider medical uncertainty as problematic. Within the category of general medical uncertainty (category 8), we did not formally

Problems in Caring for Critically and Terminally Ill Patients 141
distinguish between uncertainty about the probability of medical outcomes and uncertainty about what is considered ethically or legally permissible, but single responses in this category could conceivably incorporate more than one kind of uncertainty. For example, the comment “difficulty in deciding whether to discontinue mechanical ventilation” might encompass uncertainties about the probability of recovery, quality of life of intubated patients, and the ethical aspects of terminating life-support. Notably, only 4% of respondents cited uncertainty about patient wishes as problematic (category 9).
The predominance of physician respondents in the uncertainty category may reflect physicians’ self-perception as problem solvers for whom the elimination of uncertainty is a central role-defining task. Moreover, physicians generally bear ultimate responsibility for clinical decisions and their consequences. Within the physician group, residents responded more frequently in the uncertainty category than staff physicians. Residents may feel less secure in decision making under conditions of uncertainty because of their earlier professional stage. In addition, because residents provide more immediate “hands-on” care than staff physicians at most teaching hospitals, they may experience the anxiety of uncertainty in decision making more acutely than staff physicians.
Outside constraints on the patient-provider relationship are captured by the category of “external factors.” Not surprisingly, staff physicians cited external factors much more frequently than the other two groups, largely because of their greater concern with medicolegal and economic issues. In contrast, the working environment (e.g., inadequate nurse-to-patient staffing ratios) was a prominent theme for nurses responding in this category.
Clinicians in inpatient settings frequently perceive that patients and families “expect miracles” or make unreasonable demands. Thus, it is surprising that relatively few responses were in the category of “unrealistic expectations.” There are at least three possible reasons for this finding. First, providers may be vocal about specific “problem patients” and families, but nevertheless believe that such cases are infrequent exceptions and not the rule. Second, some providers may view unrealistic patient expectations not as a primary problem area, but rather as a secondary effect of more fundamental problems such as poor communication of prognostic information from physician to patient. And finally, since unrealistic expectations might lead to the provision of inappropriate care, some respondents who commented in the category of “inappropriate care” might have assumed that an additional comment about expectations would be redundant.

142 A.S. Brett
Cardiopulmonary resuscitation (and the related entity of do-not-resuscitate orders) was by far the most frequently mentioned specific problematic intervention. I suggest two major reasons for this finding. First, nurses and residents, who mentioned this intervention significantly more frequently than staff physicians, perform nearly all the CPR in the surveyed hospitals. Previously published data showed that 83% of house officers and 69% of nurses thought that CPR was used inappropriately in these hospitals (5). Many of the open-ended responses suggest that providers often feel forced to perform CPR against their consciences when timely DNR orders have not been written; other authors have made similar observations (11)(12). Second, despite an extensive literature on the subject, there may be ongoing uncertainty about the implications of DNR orders for other life-sustaining treatments (13)(14) and about whether CPR must always be performed in the absence of DNR orders (15).
Several previous studies have examined the differing perceptions of physicians and nurses regarding the care of critically ill patients in the United States. For example, Walker, et al interviewed physicians (primarily residents) and nurses about specific “ethics problems” encountered on the general medical services of a teaching hospital (16). Both physicians and nurses found conflict among staff to be the most common feature of these problems. Youngner, et al examined attitudes of medical staff in a medical intensive care unit using a closed-ended written questionnaire (17). They found that nurses were more likely than residents to perceive disagreement in life-and-death decisions, both among healthcare providers and between providers and patients or families. Moreover, nurses were more likely than residents to view communication among staff as needing improvement. Gramelspacher, et al found that nearly all nurses working in an intensive care unit and an oncology unit perceived conflicts with physicians, but residents and subspecialty fellows rarely perceived conflict with nurses (18). In a study from a nonteaching hospital, Frampton and Mayewski observed that physicians were more likely to favor “aggressive” care than nurses, and that nurses perceived a lack of communication with physicians (19). Baggs and Schmitt noted that nurses and residents agreed about most aspects of decision-making regarding aggressiveness of care in an intensive care unit, but that nurses were less satisfied with the decision-making process (20). Taken together, these previous studies found conflict among staff to be more prominent than our study, but they corroborate our finding that nurses are especially likely to view communication as problematic. Because the previous studies included small numbers of subjects (less than 100 in all but

Problems in Caring for Critically and Terminally Ill Patients 143
one study), single institutions, and usually resident but not staff physicians, their findings may be less generalizable than our findings.
This study has several limitations. First, the open-ended question was answered by only 74% of respondents. However, the results presumably reflect the views of those on the “front lines” of medical care, since the 74% who completed the open-ended question cared for more critically ill and dying patients than non-respondents. Second, open-ended questions allow the respondent considerable latitude, but they may sacrifice the precision achieved by closed-ended questions. Third, because the survey was written, general or vague responses were not clarified through follow-up discussion. Fourth, although two coders achieved a high level of independent agreement in classifying narrative responses, there is an unavoidable element of subjectivity in content analysis. Finally, a decade has passed since these data were collected; it is conceivable that the perspectives of nurses and physicians, or the principal problems in end-of-life care, have changed dramatically during the decade since these data were gathered. However, the steadily increasing stream of literature about problematic medical care near the end of life, and my personal clinical experience, suggest that this is not the case. Indeed a supplement to the February 2001 issue of the journal Critical Care Medicine, entitled “Compassionate End-of-Life Care in the Intensive Care Unit,” includes a series of articles that reinforce many of the themes apparent in our survey. Implications for institutional and organizational ethics
The findings of this study have several implications for institutions. First, when institutional leaders seek to implement more effective strategies in the provision of end-of-life care, they should explicitly acknowledge that nurses and physicians might bring somewhat differing perspectives to the table. To some extent, those perspectives appear to complement each other by emphasizing different facets of the human experience; each can make valuable contributions to institutional policies and procedures.
Second, differences between the physician and nursing perspectives undoubtedly serve as a source of tension in the highly charged environment of critical and terminal illness. Both professions presumably would benefit from more explicit attention to the concerns of the other group, not only informally in the day-to-day work environment, but also formally during institutional planning and in the curricula of medical and nursing schools (7).

144 A.S. Brett
Third, physicians and nurses overlap considerably in several areas of concern; those areas should be targets for interventions by both professional groups. Consider, for example, the widely cited problem of inadequate communication between providers and patients. According to interviews with family members of recently deceased patients, patients and families continue to consider inadequate communication to be a major problem (21)(22). In addition, personal observations and accounts in the literature suggest that some physicians are inadequately prepared to conduct skilled discussions with critically ill patients and their families (23)(24); the same is undoubtedly true for some nurses. The challenge is for healthcare institutions to design interventions that enhance providers’ communication skills relevant to end-of-life care, and to remove logistical impediments to timely communication between providers and patients. Ideally, those interventions should involve collaboration between physicians and nurses.
The theme of uncertainty provides another target for intervention. Clinical research can refine probabilities of medical outcomes, educational efforts can reduce uncertainty about ethical and legal standards, and broader use of advance directives may reduce uncertainty about patient preferences. Nevertheless, uncertainty can rarely be eliminated in medical decision making, and none of the aforementioned interventions in themselves address the psychology of coping with uncertainty. Medical and nursing educators should cultivate trainees’ abilities to cope with and accept uncertainty, so that providers will in turn communicate uncertainty to patients and families comfortably and effectively (25).
Finally, problems in medical care at the end of life sometimes reflect organizational aspects of modern medical care rather than the personal inadequacies of physicians or nurses. For example, when members of a large diversified team of multiple physicians and nurses are each caring for several critically ill patients, ensuring a timely flow of information between caregivers, patients, and families becomes difficult. Downsizing of nursing or social work departments in acute-care hospitals may also decrease the availability of psychosocial support for patients and families (26). In addition, the mobility of the American population, the evolving tendency of the American healthcare system to disrupt continuity of care (27), and the frequent transfer of critically ill patients to tertiary care hospitals all tend to undermine the mutual understanding that flows from long-term physician-patient-family relationships. Because of these complexities, systematic improvement in end-of-life care is unlikely to occur merely through the good will of individual clinicians; institutional support is essential. For example, a

Problems in Caring for Critically and Terminally Ill Patients 145
recent study from one institution suggested that proactive ethics consultation enhanced the care of critically ill patients by facilitating communication and education early in the clinical course of high-risk cases (28).
In conclusion, this study suggests that several conceptually coherent categories can capture the major concerns of nurses and physicians caring for critically and terminally ill patients in acute care hospitals. Significant differences between the concerns of nurses and physicians are consistent with traditional distinctions between the nursing role (emphasizing interpersonal relationships) and the physician role (emphasizing rationality and reduction of uncertainty). Nevertheless, there is also considerable overlap between the perspectives of the two professional groups. Recognition of these differences and similarities should inform institutional interventions to enhance end-of-life care.
ACKNOWLEDGEMENT
The Decisions Near the End of Life project was supported by the W. K. Kellogg Foundation. I am indebted to Carl O’Donnell, Sc.D., MPH, for statistical assistance. I also thank Lydia O’Donnell, Ed.D., and Mildred Z. Solomon, Ed.D., investigators in the Decisions project, for allowing me to access the Decisions database.
REFERENCES
1. Wolf SM. Sources of concern about the Patient Self-Determination Act. New England Journal of Medicine. 1991; 325:1666-671.
2. Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the Patient Self-Determination Act and the SUPPORT intervention. Journal of the American Geriatric Society. 1997; 45:500-507.
3. Teno JM, Branco KJ, Mor V, et al. Changes in advance care planning in nursing homes before and after the Patient Self-Determination Act: report of a 10-state survey. Journal of American Geriatric Society. 1997;45:939-44.
4. The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients: The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments (SUPPORT). Journal of the American Medical Association. 1995; 274:1591-598.
146 A.S. Brett
5. Solomon MZ, O’Donnell L, Jennings B, et al. Decisions near the end of life: Professional views on life-sustaining treatment. American Journal of Public Health. 1993; 83:14-23.
6. Khushf G. Administrative and organizational ethics. HEC Forum. 1997; 9:299-309.
7. Greenfield LJ. Doctors and nurses: a troubled partnership. Annals of Surgery. 1999; 230:279-88.
8. Benner P, Wrubel J. The Primacy of Caring: Stress and Coping in Health and Illness. Menlo Park, CA: Addison Wesley; 1989.
9. Gadow S. Advocacy nursing and new meanings of aging. Nursing Clinics of North America. 1979; 14:81-91.
10. Benjamin M, Curtis J. Ethics in Nursing. (3rd ed.) New York, NY: Oxford University Press; 1992: 97-123.
11. Winkenwerder W. Ethical dilemmas for house staff physicians: The care of critically ill and dying patients. Journal of the American Medical Association. 1985; 254:3454-457.
12. Shreves JG, Moss AH. Residents’ ethical disagreements with attending physicians: An unrecognized problem. Acad Med. 1996; 1103-105.
13. Tomlinson T, Brody H. Ethics and communication in do-not-resuscitate orders. New England Journal of Medicine. 1988; 318:43-46.
14. Uhlman RF, Cassel CK, McDonald WJ. Some treatment-withholding implications of no-code orders in an academic hospital. Critical Care Medicine. 1984; 12:879-81.
15. Blackhall LJ. Must we always use CPR? New England Journal of Medicine. 1987; 317:1281-285.
16. Walker RM, Miles SH, Stocking CB, Siegler M. Physicians’ and nurses’ perceptions of ethics problems on general medical services. Journal of General Internal Medicine. 1991; 6:424-29.
17. Youngner S, Jackson DL, Allen M. Staff attitudes towards the care of the critically ill in the medical intensive care unit. Critical Care Medicine. 1979; 7:35-40.
18. Gramelspacher GP, Howell JD, Young MJ. Perceptions of ethical problems by nurses and doctors. Archives of Internal Medicine. 1986; 146:577-78.
19. Frampton MW, Mayewski RJ. Physicians’ and nurses’ attitudes toward withholding treatment in a community hospital. Journal of General Internal Medicine. 1987; 2:394-99.

Problems in Caring for Critically and Terminally Ill Patients 147
20. Baggs JG, Schmitt MH. Intensive care decisions about level of aggressiveness of care. Research in Nursing and Health. 1995; 18:345-55.
21. Hanson LC, Danis M, Garrett J. What is wrong with end-of-life care? Opinions of bereaved family members. Journal of the American Geriatric Society. 1997; 45:1339-344.
22. Tilden V, Tolle SW, Garland MJ, Nelson CA. Decisions about life-sustaining treatment: Impact of physicians’ behaviors on the family. Archives of Internal Medicine. 1995; 155:633-38.
23. Ventres W, Nichter M, Reed R, Frankel R. Limitation of medical care: An ethnographic analysis. Journal of Clinical Ethics. 1993; 4:134-45.
24. Tulsky JA, Chesney MA, Lo B. ‘See one, do one, teach one’ fails in discussions about resuscitation. Journal of General Internal Medicine. 1994; 9:83.
25. Katz J. Why doctors don't disclose uncertainty. Hastings Center Report. 1984; 14:34-44.
26. Aiken LH, Sochalski J, Anderson GF. Downsizing the hospital nursing workforce. Health Affairs (Millwood). 1996; 15:88-92.
27. Emanuel EJ, Brett AS. Managed competition and the patient-physician relationship. New England Journal of Medicine. 1993;329:879-82.
28. Dowdy MD, Robertson C, Bander JA. A study of proactive ethics consultation for critically and terminally ill patients with extended lengths of stay. Critical Care Medicine. 1998; 26:252-59.




























![Terminally Differentiated SH-SY5Y Cells Provide a Model [887035]](https://img.pdfslide.net/doc/110x75/577c832e1a28abe054b3f104/terminally-differentiated-sh-sy5y-cells-provide-a-model-887035.jpg)
