Embed Size (px)
Citation preview

PROPHYLAXISdialogueJournal for Oral Prevention in Practice
The Microbial Ecology of the Mouth and Its Significancein Oral and General Health
Quality of Life Related to Dental Health (MLQ)in Children and Adolescents
Electron-optical Investigations of Formationof CaF2 Fluoride Reservoirs on the Tooth Surface
PROPHYLAXISdialogue
Key issue
The human body is composed of approximately1014 cells, of which only 10% are mammalian. Themajority are micro-organisms that comprise the resi-dent microflora of the host and which are found on allenvironmentally exposed surfaces of the body. The res-ident microflora is natural and contributes to the nor-mal development of the physiology and antimicrobialdefences of the host. The pre dominant organisms varyat distinct habitats (e.g. skin, mouth, gastro-intestinaltract) due to the biological and physical properties ofeach site, demonstrating a direct relationship betweenthe environment and the composition of the micro-flora. An appreciation of this relationship is critical tounderstanding the role of the oral microflora in healthand disease.
The mouth as a microbial habitat
The mouth is an attractive habitat for micro-organ-isms. Oral surfaces are bathed in saliva, which keepsthe pH buffered around neutrality, and saliva providesproteins and glycoproteins that are used as nutrientsby the resident microflora. Conditions can also be hos-tile to micro-organisms. Saliva contains an array ofantimicrobial molecules (e.g. lysozyme, lactoferrin,host defence peptides, sialoperoxidase, etc), and onlya fraction of the microbes that gain access to themouth are able to colonise. Desquamation ensures thatthe microbial load on mucosal surfaces is low, althoughteeth provide a unique hard, non-shedding surface forcolonisation enabling large numbers of bacteria andtheir products to accumulate, especially at stagnantsites that provide refuge from the host.
The resident oral microflora
Microbial colonisation starts from birth, and distinctspecies of bacteria (mainly streptococci) are recoveredfrom the mouth of infants only a few hours old. Thecomplexity of the developing microflora increases overtime, particularly following tooth eruption. Once estab-lished, the resident microflora has a diverse composi-tion, consisting of a wide range of Gram positive andGram negative bacterial species, as well as yeasts andother types of micro-organism. The most diverse col-lections of micro-organisms are found in the biofilmson teeth (dental plaque) (Aas et al. 2005).
These biofilms develop in a particular pattern.Molecules (adhesins) on early colonisers bind to spe-cific receptors on saliva-coated tooth surfaces; morefastidious bacteria bind to these early colonisers andtheir metabolism modifies the local environment (e.g.make it more anaerobic) and produce extracellularpolymers (plaque matrix) that consolidates attachmentof the biofilm. These biofilms are spatially- and func-tionally-organised, and the conditions within thebiofilm induce novel patterns of bacterial gene expres-sion, an important consequence of which is a reducedsensitivity to antimicrobial agents which can affecttreatment outcomes (Marsh 2005). The diverse collec-tions of micro-organism in these biofilms function asconsortia, and engage in numerous interactions:
W nutritional interactions – food-chains; metabolicco-operation to catabolism complex host macro-molecules,
W cell-cell signalling – co-ordinates gene expression,
W gene transfer – transfer of antibiotic resistance, and
W antagonism – production of inhibitory moleculeswhich may increase competitiveness and/or ex-clude undesirable microbes.
The Microbial Ecology of the Mouthand Its Significance in Oral and General HealthPD Marsh, HPA CEPR, Salisbury and Leeds Dental Institute, UK
Scanning electronmicrograph of adental plaque bio-film. The morpho-logical diversity ofthe micro-organismsfound in dentalplaque can be seen.

Distinct environments exist on mucosal surfaces(e.g. cheek, palate, tongue) which differ from those onteeth (e.g. fissures, gingival crevice). The biologicalproperties of each site determine which organisms areable to colonise, be competitive and predominate orbe excluded or persist as only a minor component (Aaset al. 2005). Relatively few bacterial species are found infissures; the predominant bacteria are streptococci andthere are few Gram negative or anaerobic organisms.In contract, the gingival crevice has a more diversemicroflora, including many Gram negative anaerobicand proteolytic species.
Conventionally, the oral microflora was characte-rised by traditional culture techniques. Recently, mole-cular approaches have been used, and this has revo-lutionised our concept of the diversity of the oralmicroflora; >700 distinct bacterial types have now beenrecognised, with about 50% unculturable in the labora-tory at present (Aas et al. 2005).
Stability of the oral microflora
Once established at a site, the resident microfloraremains relatively stable over time, unless there aremarked changes to the habitat. For example, certainbacteria only appear in the mouth once teeth erupt,and bacterial diversity can be reduced if patients aretaking broad spectrum antibiotics. This stability, termedmicrobial homeostasis, stems not from any metabolicindifference by the oral microflora, but reflects a highlydynamic state in which the relative proportions of indi-vidual species are in balance due to numerous inter-actions, both synergistic and antagonistic. The residentoral microflora brings numerous benefits to the host bypromoting the:
W normal development of host cell structure and func-tion,
W normal development of the immune system, anddamping down deleterious immune responses, and
W exclusion of exogenous (and often pathogenic)micro-organisms. This process (colonisation resis-tance) is due to the resident microflora being morecompetitive in terms of nutrient acquisition andattachment to oral receptors, and by producinginhibitory molecules.
The oral microflora in disease
On occasions, microbial homeostasis breaks downand disease can result. Breakdown can be due to avariety of factors but is generally a response to a sub-stantial change in a key ecological determinant, such asan increase in the frequency of dietary sugar intake or adecrease in either saliva flow or the immune response(see graphic on page 6).
Dental caries
Caries is a result of acid production from the micro-bial fermentation of dietary sugars. Extensive studiesover several decades of a range of age groups, on dif-ferent diets have shown an increase in the proportionsof acid-producing (acidogenic) and acid-tolerating(aciduric) bacteria in plaque biofilms at sites with caries.The most common bacteria with these properties aremutans streptococci (Streptococcus mutans, S. sobri-nus) and lactobacilli, but the relationship betweenthese organisms and caries is neither absolute nor diag-nostic (Marsh & Nyvad 2007).
These bacteria are not detected from all carioussites, implicating other bacteria with similar propertiesin disease, while they can also be found at sites withoutevidence of demineralisation.
Periodontal diseases
Periodontal diseases are a collection of conditionsin which the supporting tissues of the teeth areattacked. Plaque accumulates at the gingival marginbeyond levels that are compatible with health, andthere is an increase in numbers of obligately anaero-bic, proteolytic and often Gram negative bacteria(Socransky & Haffajee 2005). The host mounts aninflammatory response to this microbial insult, and theflow of gingival crevicular fluid (GCF) is increased todeliver antibodies, complement and phagocytic cells.
If the microbial challenge is not controlled, the sub-gingival microbial consortia can subvert the hostresponse by producing cytotoxins, inflammatory media-tors, and proteases that degrade host regulatory pro-teins (Curtis et al. 2005). This leads to an inappropriateand damaging inflammatory response resulting in by-stander damage to host tissues.
Key issue
PROPHYLAXISdialogue
Recently, an ecological hypothesis was proposed toexplain the relationship between plaque compositionand caries and periodontal disease (Marsh 2003).Briefly, a major change in local environmental condi-tions can alter the competitiveness of plaque bacteria,leading to the enrichment of organisms most suited tothe altered environment.
In caries, an increased frequency of sugar intake, ora reduction in saliva flow, results in plaque biofilmsspending more time at low pH. This selects for acido-genic and aciduric species (most commonly mutansstreptococci, but not exclusively so) at the expense ofhealth associated bacteria that prefer pH values aroundneutrality. Increases in the acidogenic populationsleads to even greater production of acid and furtherraises the risk of demineralisation. In periodontal dis-ease, the inflammatory response to plaque accumula-tion results in an increased flow of GCF which, in addi-tion to introducing components of the host defences,also delivers host molecules (haemoglobin, transferrin)that can be catabolised by anaerobic and proteolyticbacteria. This metabolism makes the site more anaero-bic and the local pH increases, and this selects for thecomplex consortia detected at inflamed sites.
Key issue
PROPHYLAXISdialogue
A key principle of this hypothesis is that disease canbe treated not only by improving oral hygiene or tar-geting the putative pathogens directly, but also byinterfering with the environmental pressures that selectfor the pathogenic micro-organisms. In caries, thiscould be by reducing the low pH challenge by recom-mending snack foods containing non-fermentable
sweeteners, using fluoride pro-ducts to reduce acid produc-tion and encourage reminerali-sation, or boosting saliva flowwith sugar-free gums, while theuse of oxidising agents to makesites less anaerobic or anti-inflammatory compounds toreduce GCF flow would restrictthe growth of periodontalpathogens (Marsh 2003).
Periodontal health and generalhealth
Evidence linking oral and general health is accumu-lating, particularly with respect to cardiovascular andrespiratory diseases, diabetes mellitus and a risk of pre-term labour and low birth weight infants. The theorybehind this association is that:
W many oral bacteria can act as opportuniticpathogens if they gain access to sites not normallyaccessible to them, or if host defences are compro-mised, and
W subgingival biofilms in periodontal disease containnumerous Gram negative species which (a) possessinflammatory cell surface components (e.g. lipo-polysaccharide), and (b) shed toxic metaboliteswhich induce prostaglandins and pro-inflammatorycytokines. The vascular nature of the periodontiummeans that these inflammatory mediators couldaffect distant sites in the body.
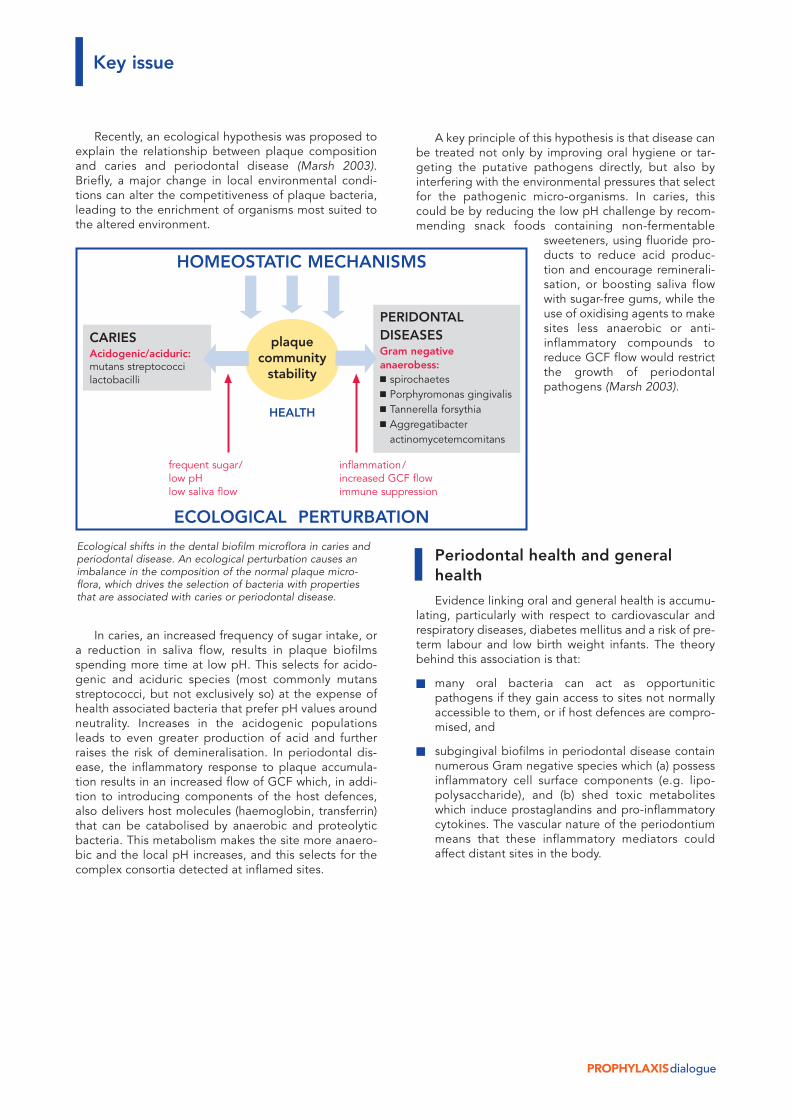
Ecological shifts in the dental biofilm microflora in caries andperiodontal disease. An ecological perturbation causes animbalance in the composition of the normal plaque micro-flora, which drives the selection of bacteria with propertiesthat are associated with caries or periodontal disease.
CARIESAcidogenic/aciduric:mutans streptococcilactobacilli
PERIDONTALDISEASESGram negativeanaerobess:W spirochaetesW Porphyromonas gingivalisW Tannerella forsythiaW AggregatibacterW actinomycetemcomitans
HOMEOSTATIC MECHANISMS
ECOLOGICAL PERTURBATION
plaquecommunity
stability
HEALTH
frequent sugar/low pHlow saliva flow
inflammation/increased GCF flowimmune suppression
PROPHYLAXISdialogue
Oral micro-organisms can enter the blood streamduring transient bacteraemias and play a role in sys-temic disease. The link between oral bacteria (especial-ly streptococci) and infective endocarditis is irrefutable,but research also suggests that periodontal bacteriamay be an added risk factor for cardiovascular disease(Demmer & Desvarieux 2006). Molecular techniqueshave also detected DNA from oral Gram negative bac-teria in atheromatous plaques.
Periodontal diseases can represent a small risk fac-tor for pre-term or low birth weight babies, either as adirect consequence of pre-term labour or due to pre-mature rupture of membranes (Vergnes & Sixou 2007).Elevated levels of prostaglandins have been found inthe GCF of mothers with pre-term, low birth weightbabies.
Micro-organisms associated with periodontal dis-eases may also give rise to aspiration pneumonia in sus-ceptible patients as anaerobic bacteria from periodon-tal pockets have been isolated from infected lungs(Mojon 2002).
In this important clinical area, there is a need formore large, well-controlled investigations in diverse buthomogeneous population groups, in which the statisti-cal analyses are adequately adjusted for other life-styleconfounding risk factors (smoking, alcohol consump-tion, maternal education, etc). Longitudinal, prospec-tive studies are also needed to determine whether peri-odontal disease is causal for these medical conditions.
The outcome of intervention studies, in which theimpact of periodontal treatment on the subsequentdevelopment of systemic disease is monitored, willbe crucial in confirming the impact of oral disease ongeneral health.
PD MarshHPA CEPR, Salisbury and Leeds Dental Institute, UK
Study of Health inPomerania (SHIP) –A Health Study in EasternGermanyRisk factors for periodontitisand periodontitis as a risk factorfor cardiovascular diseases
Daniela Gätke, Prof. Dr. Thomas Kocher,University of Greifswald, Germany
Epidemiology deals with the causes and conse-quences, as well as spread of health-related conditionsand events in the populations. Factors are studied thatcontribute to health and disease. Many epidemiologi-cal studies focus on selected diseases and risk factors:cardiovascular diseases in general medicine and crowncaries in dentistry in particular have been the subject ofmany studies. The health of a person, however, is rarelydetermined by a disease and very few illnesses canbe attributed to one cause. Several factors at a mini-mum have a complex impact on many illnesses. Epi-demiology attempts to identify new risk and protectivefactors to then use them as prognostic factors in a riskscore or as a new point of attack for therapeutic inter-ventions.
The ”Study of Health in Pomerania” (SHIP) is apopulation-based study in the Pomerania region. Arepresentative selection of subjects was taken from theregistration office and invited to participate in thestudy. 4310 men and women in ages between 20 and79 years were studied (participation rate of 68.8%). Thebaseline data was collected from 1997 to 2001 (SHIP-0).A 5-year follow-up was carried out from 2002 to 2006(SHIP-1). We were able to follow up with 3300 subjects.A 10-year follow-up is scheduled for 2008 (SHIP-2). Thedata from SHIP 0 in the form of a cross-sectional studyare to be viewed as a ”snap shot” in time and thecausal relationships generated from the data betweenrisk factors and disease are weak and are used to gene-rate hypotheses. Causal risk factors can be verified onlyafter analysis of the longitudinal data set.
The goal of SHIP is to study health and illness in itscomplexity. It involves the prevalence and incidence ofcommon and population-relevant diseases and theirrisk factors (Hensel et al. 2003). In order to develop riskmodels, comprehensive data are collected on familyand work environment, on social relationships andchronic diseases, on nutrition, on tobacco and alcoholabuse and on the use of medical services.
Key issue

PROPHYLAXISdialogue
The dental examination includes assessment of theteeth, prosthetics, periodontium, oral mucosa and dys-function of the craniomandibular systems. As part ofthe medical examination, blood pressure was mea-sured, an electrocardiogram and echocardiogramtaken, as well as the carotid artery, thyroid and liverexamined with ultrasound. In addition, a neurologicalscreening was performed and DNA, serum and urinesamples taken.
Risk factors for periodontitis
Periodontal diseases are diseases with ”continuous”and not ”categorial” expression. Their symptoms canrange from subclinical changes (bleeding when prob-ing) to tooth loss. This defines the problem whether aperiodontal diseased area is enough to view a subjectas having periodontal disease and what threshold hasto be exceeded. If a person is regarded as having aperiodontal diseased area, this observation leads to anoverestimation of the prevalence. There is currently noaccepted definition of prevalence. Therefore, preva-lence data on periodontal disease should be viewedwith a question mark and prevalence in various studiesare only conditionally comparable.
The observation that prevalence of periodontal dis-eases can be very different throughout the populationprompted the search for risk factors (Kocher et al.2005). For their evaluation, the Odds Ratio (OR) is oftennamed as a measured value. The Odds Ratio indicateshow much greater the risk of occurrence is for peoplewith than for people without the risk factor. We exam-ined the following as risk factors for periodontitis:sociodemographic factors (age, gender, income, edu-cation), medical factors (systemic diseases, medica-tions), behavioral factors (regular check-ups at thedentist, smoking) and oral factors (presence ofsupragingival tartar and plaque).
The following risk factors were determined to besignificant: male, low level of education (OR 2.3), thepresence of supragingival tartar (OR 2.8) and plaque(OR 2.3). Smoking was the risk factor with the greatestimpact, i.e. the more one smokes, the greater the riskfor attachment loss (> = 20 cigarettes, OR 6.8). Formersmokers are still of increased risk of getting periodonti-tis than non-smokers. The combination of the inter-leukin genotype and smoking also increases the proba-bility of getting periodontal disease (OR 4.0) (Meisel etal. 2004). Data yet unpublished suggest that over-weight people are at greater risk of getting periodonti-tis than those who are not overweight. Subjects withsevere periodontal disease have an approx. 50% lowerrisk of getting allergies (Friedrich et al. 2006).
From the prospective results of the coming year, wewant to develop a forecast model for periodontal dis-eases and tooth loss that also takes genetic back-ground into account. Unfortunately, no microbiologicalswabbings were taken in SHIP 0.
Periodontitis as a risk factor forcardiovascular diseases
Periodontitis is one of the most common bacterialinfectious diseases worldwide. It involves close contactof bacteria with the microcirculation of the periodontalpocket and thereby, bacteremia with various systemiceffects.
Ultrasound can be used to show subclinical arte-riosclerotic processes. The wall thickness of the artery isused as a measurement for subclinical arteriosclerosis.The intima-media thickness of the carotid artery corre-lates with future cardio- or cerebrovascular events.Because tooth loss is closely correlated with periodon-tal diseases in our population, we also examined toothloss as an end point for periodontitis. In SHIP, we wereable to show that subjects with increasing severity ofperiodontitis or tooth loss exhibit thicker intima-mediaor an increased prevalence of arterial plaque. For sub-jects with 0–9 missing teeth, 46% exhibited arterialplaque in the carotid artery and 60% for those with 10or more missing teeth. Surprisingly, these relationshipswere only found in men between 45 and 60 years ofage (Desvarieux 2004). This observation are consistentwith the results of other workgroups.
An analysis in which we examined the relationshipbetween tooth loss and high blood pressure revealedthe observation that periodontal diseases have in-creased systemic effects in men than in women. Theaverage systolic blood pressure in men with 0–6 teethwas 149.6 mmHg compared to 142.6 mmHg for menwith 27–28 teeth. Subjects with fewer teeth were morelikely hypertensive and more likely to take antihyper-tensives. In women, however, no relationship wasapparent (Volzke et al. 2006).
These findings help explain the relationshipbetween tooth loss and mortality. If this observation isconfirmed in both our longitudinal and in other datasets, the patient group could be narrowed further for afuture therapeutic study and their risk of arteriosclerosispossibly reduced through periodontal treatment.
Prof. Dr. Thomas KocherErnst-Moritz-Arndt-Universität GreifswaldZentrum ZMK · Abt. ParodontologieRotgerberstrasse 8 · 17487 Greifswald · Germany
Key issue
PROPHYLAXISdialogue
The MLQ concept
Nearly every discussion between a dentist or doctorand a patient regardless of age is directly or indirectlybased on the question ”How are you today (in terms ofthe teeth and mouth)?”. It is anticipated everyday in thepractice what the dental research today tries to opera-tionalize, i.e. to understand the physical and psycho-social aspects of oral diseases from the perspective ofthose affected. Why is this perspective important?
In their daily work, dentists normally establish thestatus of oral diseases as a basis for treatment planingand therapy. The caries index (01 finding) describes thescope of teeth treated as a result of caries and teeth yetto be treated, pocket depth measurements are used toestimate the severity of a periodontal disease, plaqueindices or bleeding measurements of the gingiva arethe basis for individual prophylaxis. All these indicatorsdescribe the objectifiable status of an individual findingin the masticatory system, but they have disadvantagethat they say little about the function of the masticatorysystem or the patient as a whole and do not identify thesubjective status of the well-being perceived by thepatient. Missing teeth or their carious or traumaticdestruction has multiple consequences according tothe health care model by Locker (1988) (see figure).
For example, limitations in terms of food selection(avoidance of hard foods) may result from structuralloss, or the person affected avoids laughing or eatingtogether with other people.
A disadvantage compared with the environment isanother consequence if one impaired at work or schoolby unclear speech or an unattractive appearance.Similar problems can also involve dysgnathias ormalformations (Hatch, Rugh et al. 1998, O’Brien et al.1998).
Overall, oral diseases in our culture have a verydirect impact on the life of those affected. With anindex for quality of life based on dental health, theimpact can be described based on a bio-psycho-socialunderstanding of disease.
Introduction of MLQ instrumentsfor children and adolescents in theGerman-speaking area
For children and adolescents where oral preventionmeasures are viewed as particularly useful and promis-ing, psychosocial health indicators are yet to be intro-duced in Germany. That may be surprising because oralproblems in childhood and adolescence are multi-faceted and in no way limited to caries damage, whichincidentally still occurs in approx. half of 12 year olds(Micheelis & Schiffner 2006):
Individual prophylaxis
Quality of Life Related to Dental Health (MLQ)in Children and AdolescentsPractice-relevant aspects of dental research
Prof. Dr. Christian Hirsch, University of Leipzig, Germany
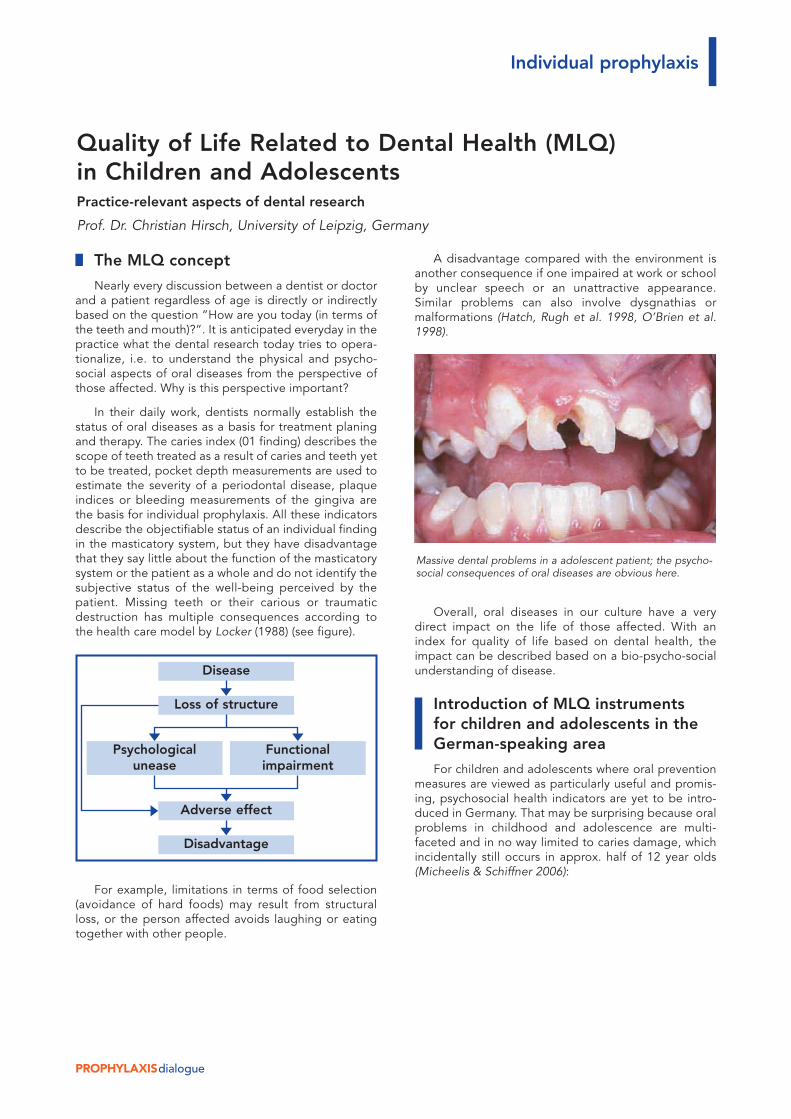
Massive dental problems in a adolescent patient; the psycho-social consequences of oral diseases are obvious here.
Disease
Loss of structure
Adverse effect
Disadvantage
Psychologicalunease
Functionalimpairment
PROPHYLAXISdialogue
W About one third of this age group also show mal-positions of the teeth and jaw (Micheelis & Bauch1991).
W Also in about a third of children and adolescents,non-carious tooth damage as a result of parafunc-tional activities in the masticatory system (bruxism)are also observed (Hirsch, John et al. 2004).
W Accidental tooth damage occurs in about every 3rdor 4th child; approx. 10% of those lose the injuredteeth completely (Andreasen & Daugaard-Jensen1991).
W Chronic pain in the are of the jaw and face is report-ed by up to 15% (monthly prevalence) of childrenand adolescents (Hirsch & John 2003).
W Congenital abnormalities of the jaw (e.g. cheilog-nathouranoschisis) have an incidence of 2 in 1000live births, the most common malformation overall(Zieglowski & Hemprich 1999).
W General diseases that occur in childhood and ado-lescence also have their manifestations or effects inthe orofacial system (e.g. acid erosion from eatingdisorders) (Bartlett 1998).
The importance of the mouth and facial area forpsychological and social development in childhood andadolescence is undisputed (Jokovic, Locker et al. 2005).However, the impact of the oral diseases enumeratedhere on the child or adolescent, i.e. how the adolescentperceives his or her dental health, which daily activities(e.g. play, school) are limited and how the family is alsoaffected by these diseases (e.g. non-productive time ofthe parents) has to date has hardly been examined.There are only a few concrete studies nationally andinternationally.
The WHO estimates thatapprox. 50 million school hoursannually are lost due to dentalproblems worldwide (Chen,Andersen et al. 1997). Othersurveys have shown that chil-dren and adolescents with oraldiseases exhibit respiratory andspeech disorders, are teasedand miss school more often(Locker, Jokovic et al. 2005).
In a current representativestudy in Saxony-Anhalt, 11% of12-year-olds asked said theyhave not smiled due to theappearance of their teeth, 9%missed school because oftoothaches and 5% were
teased by their classmates because of their teeth(Brauner 2005). It was also shown that the family isaffected by oral diseases of the children (Locker,Jokovic et al. 2002).
In order to understand the complex effects of oraldiseases on children and adolescents, an MLQ instru-ment adapted from English (CPQ – Child PerceptionQuestionnaire; Jokovic, Locker et al. 2002) for childrenand adolescents is being tested in a research project inthe Pedodontics Department of the Leipzig DentalClinic – first for the age group of 10 to 15 years. Clinicalparameters for a variety of patients must be correlatedwith MLQ to demonstrate the validity of the instrument.In its complete form, the instrument has 50 questions.For some questioning, there will also be a short instru-ment in the future with approx. 10 questions. Data isbeing collected in parallel from the general populationto have standard values available for MLQ in this agegroup.
The use of MLQ instruments withchildren and adolescents
Are there even significant differences in perceptionfrom MLQ in the different age groups that justifythe considerable expense of developing age-specificinstruments?
Based on initial data, the table shows that the 10problems most commonly reported differ significantlybetween 10 to 15 year olds and adults (from John,LeResche et al. 2003).
Individual prophylaxis
Frequency of oral problems in adolescents and adults (according to John et al. 2003)
Adolescents Adults*
Rank Problem % Problem %
1 Had breathed through the mouth 21 Food residue gets stuck 39to the teeth
2 Difficulty with warm/cold 14 Sensitive teeth 33food and drinks
3 Food residue gets stuck 14 Bad breath 33to the teeth
5 Difficulty chewing solid food 7 Sore gums 276 Pain in the mouth area 7 Difficulty chewing solid food 26
4 Bleeding of the gums 10 Toothaches 29
8 Was irritable/ frustrated/ 4 Dry mouth 24disagreeable
7 Bad breath 5 Stressed 25
9 Could not be with other children 4 General health was worsened 24
10 Could not got to family events 4 Sores in the mouth 23
PROPHYLAXISdialogue
In addition to consistently reported problems (e.g.pain, bad breath), the group of 10 to 15 year olds alsoreported acceptance by the environment (“couldn't bewith others”, “couldn't go to family events”) as animportant aspect. Not surprisingly, problems emerge inthe questionnaire for the adolescents that are notreported by adults (e.g. “fear of speaking in front of theclass” or ”fear of being ignored by other children”).Conversely, adults have problems that naturally do notoccur in adolescence, e.g. with their dental prosthesis.Therefore, the consequences of oral diseases in adoles-cents and adults cannot be represented with identicalquality of life questionnaires.
What do we do now with the MLQ information forchildren and adolescents? First, we as dentists can con-firm our feelings to really help the patient throughunpleasant dental treatments with concrete data, i.e.with substantial improvements in MLQ. At the sametime, statements about the relatively “severity” oral dis-eases, i.e. caries defects can be compared with mis-aligned teeth or diseases of the oral mucosa in terms oftheir consequences for the patients using a “measuredvalue” on the MLQ scale. A concrete example of a15-year-old boy missing a total of 17 permanent teeth(oligodontia) was used show that the patient belongs tothe 10% of his peer group who fair most poorly withregard to dental health (Hirsch et al. 2005).
Moreover, the use of prevention measures, whichhelp prevent oral diseases or dental treatments, can beverified beyond the purely commercial level. Until now,prevention and treatment services are providedbecause experts believe they are beneficial for thepatients (and the society). In many cases, e.g. for painintervention, that will also add up. When regulating themalposition of teeth however (keyword KIG – orthodon-tic indication groups), it is easily conceivable thatexpert opinion is quite different than the patient's per-spective. The sole purpose of quality of life research inmedicine (i.e. dentistry) is to discover which preventa-tive and therapeutic measures offer the greatestincrease in quality of life to patients from their point ofview.
Another important advantage of using MLQ instru-ments is that dental health can also be described with-out dental indices that can be very difficult for the den-tal layman to understand, which may make establishingrelevant social groups and decision makers (health carepolicy makers, cost bearers) for dental interests easier.
The introduction of MLQ instruments for childrenand adolescents in the German-speaking area alsomakes comprehensive country and cultural com-parisons of entire health care systems possible for thefirst time. Is dental care for children and adolescentsbetter or worse in Scandinavia or Great Britain than inGermany? In the face of scarce resources in health caresystems, such questions are highly relevant. It is alsoclear that comparing one parameter such as the cariesindex (which incidentally is handled) cannot sufficientlyanswer this question.
Outlook
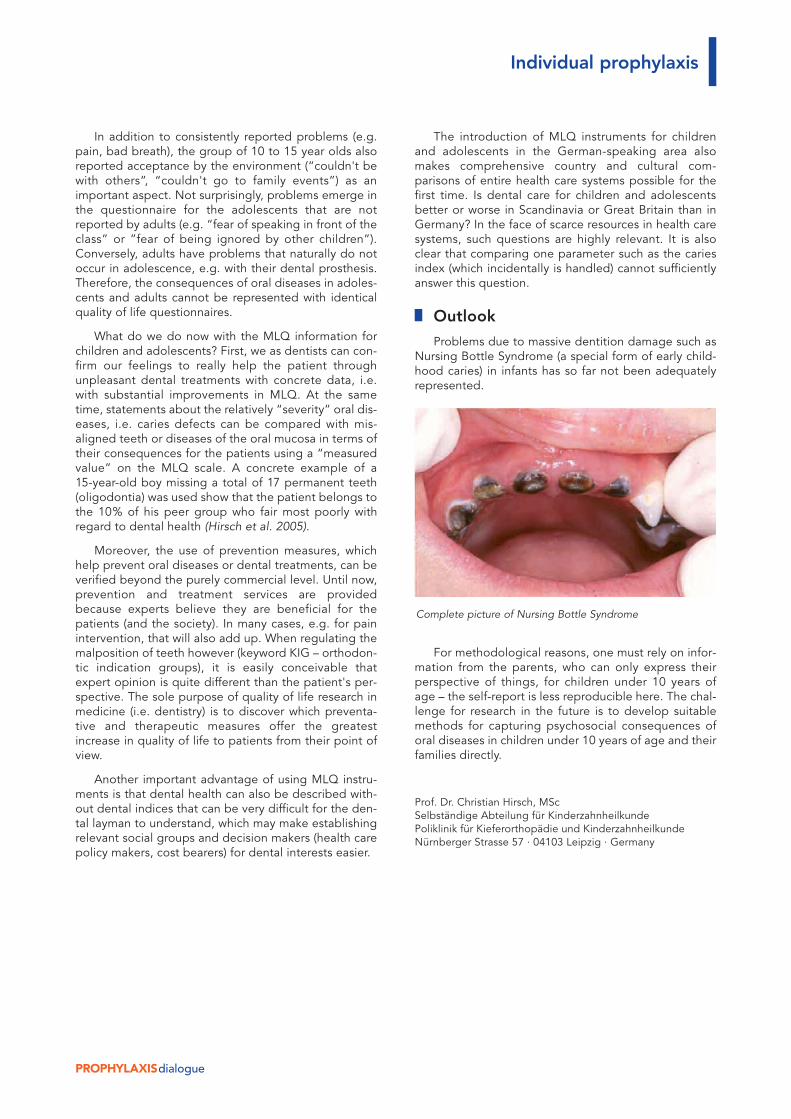
Problems due to massive dentition damage such asNursing Bottle Syndrome (a special form of early child-hood caries) in infants has so far not been adequatelyrepresented.
For methodological reasons, one must rely on infor-mation from the parents, who can only express theirperspective of things, for children under 10 years ofage – the self-report is less reproducible here. The chal-lenge for research in the future is to develop suitablemethods for capturing psychosocial consequences oforal diseases in children under 10 years of age and theirfamilies directly.
Prof. Dr. Christian Hirsch, MScSelbständige Abteilung für KinderzahnheilkundePoliklinik für Kieferorthopädie und KinderzahnheilkundeNürnberger Strasse 57 · 04103 Leipzig · Germany
Individual prophylaxis
Complete picture of Nursing Bottle Syndrome
PROPHYLAXISdialogue
Introduction
Due to levels of efficacy confirmed by numerousstudies, fluorides have become irreplaceable in cariesprevention. Results of extensive clinical and chemicalstudies have demonstrated that fluorides reduce thesusceptibility of the tooth material to demineralizationin an acidic milieu, at the same time facilitating reminer-alization by way of reintegration of calcium and phos-phates (see for example the summaries in Hellwig et al.2006, Fejerskov et al. 1996 for an overview). For sometime now, direct application of fluorides to the toothsurface, e.g. by using toothpastes and oral rinses con-taining fluoride, has been considered more effectivethan systemic fluoridation.
A mechanism of action that must be taken intoaccount in this connection is the formation of calciumfluoride (CaF2)-like material (designated hereinafter asCaF2) either directly on the tooth surface or in theadjoining plaque formations. A broad consensus in cur-rent literature confirms that such CaF2 reaction pro-ducts can assume the role of temporary fluoride reser-voirs, the gradual dissolution of which maintains a con-tinuous low-level fluoride concentration in the oralcavity, even during periods between applications oftooth care products. Assuming this, the capacity oftooth care products to form such reservoirs gains aconsiderable practical significance. An attempt followsto demonstrate the formation of CaF2 fluoride reser-voirs on the tooth surface with the help of electronmicroscopic analyses, which formation results from useof active agents and tooth care products containingamine fluorides.
Formation and stability ofcalcium fluoride-like materialon the tooth surface
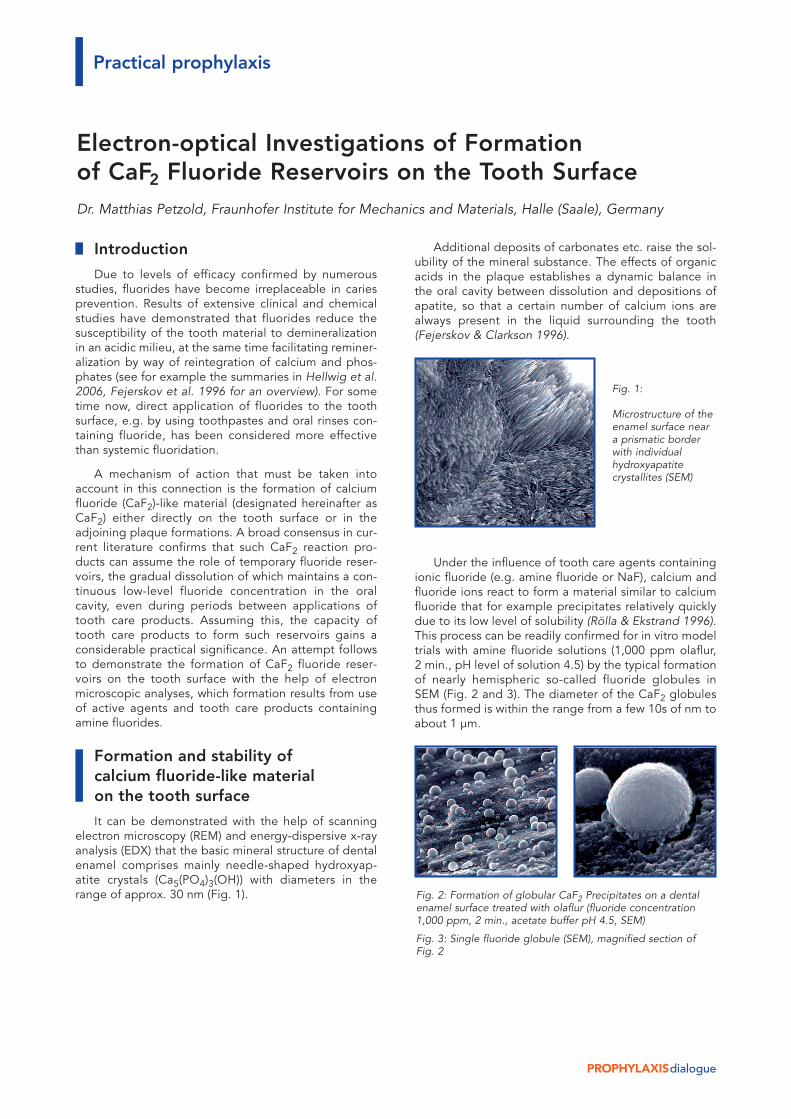
It can be demonstrated with the help of scanningelectron microscopy (REM) and energy-dispersive x-rayanalysis (EDX) that the basic mineral structure of dentalenamel comprises mainly needle-shaped hydroxyap-atite crystals (Ca5(PO4)3(OH)) with diameters in therange of approx. 30 nm (Fig. 1).
Additional deposits of carbonates etc. raise the sol-ubility of the mineral substance. The effects of organicacids in the plaque establishes a dynamic balance inthe oral cavity between dissolution and depositions ofapatite, so that a certain number of calcium ions arealways present in the liquid surrounding the tooth(Fejerskov & Clarkson 1996).
Under the influence of tooth care agents containingionic fluoride (e.g. amine fluoride or NaF), calcium andfluoride ions react to form a material similar to calciumfluoride that for example precipitates relatively quicklydue to its low level of solubility (Rölla & Ekstrand 1996).This process can be readily confirmed for in vitro modeltrials with amine fluoride solutions (1,000 ppm olaflur,2 min., pH level of solution 4.5) by the typical formationof nearly hemispheric so-called fluoride globules inSEM (Fig. 2 and 3). The diameter of the CaF2 globulesthus formed is within the range from a few 10s of nm toabout 1 µm.
Practical prophylaxis
Electron-optical Investigations of Formationof CaF2 Fluoride Reservoirs on the Tooth SurfaceDr. Matthias Petzold, Fraunhofer Institute for Mechanics and Materials, Halle (Saale), Germany
Fig. 1:
Microstructure of theenamel surface neara prismatic borderwith individualhydroxyapatitecrystallites (SEM)
Fig. 2: Formation of globular CaF2 Precipitates on a dentalenamel surface treated with olaflur (fluoride concentration1,000 ppm, 2 min., acetate buffer pH 4.5, SEM)
Fig. 3: Single fluoride globule (SEM), magnified section ofFig. 2
PROPHYLAXISdialogue
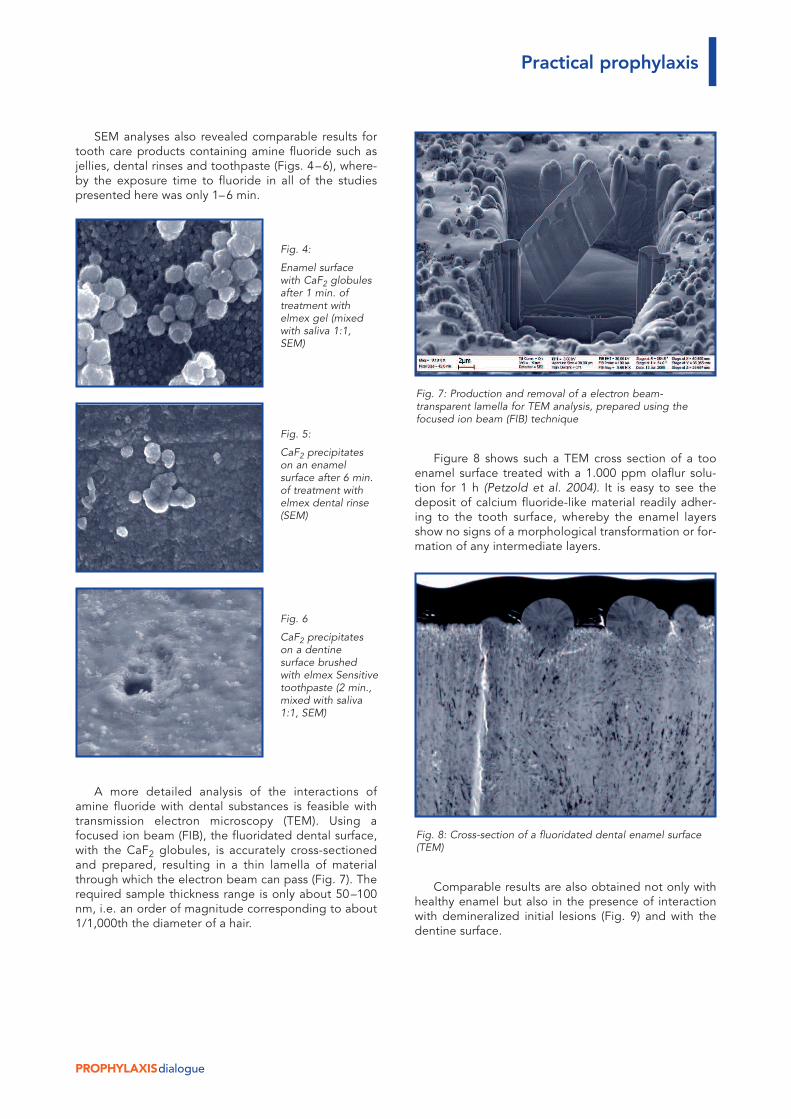
SEM analyses also revealed comparable results fortooth care products containing amine fluoride such asjellies, dental rinses and toothpaste (Figs. 4–6), where-by the exposure time to fluoride in all of the studiespresented here was only 1–6 min.
A more detailed analysis of the interactions ofamine fluoride with dental substances is feasible withtransmission electron microscopy (TEM). Using afocused ion beam (FIB), the fluoridated dental surface,with the CaF2 globules, is accurately cross-sectionedand prepared, resulting in a thin lamella of materialthrough which the electron beam can pass (Fig. 7). Therequired sample thickness range is only about 50–100nm, i.e. an order of magnitude corresponding to about1/1,000th the diameter of a hair.
Figure 8 shows such a TEM cross section of a tooenamel surface treated with a 1.000 ppm olaflur solu-tion for 1 h (Petzold et al. 2004). It is easy to see thedeposit of calcium fluoride-like material readily adher-ing to the tooth surface, whereby the enamel layersshow no signs of a morphological transformation or for-mation of any intermediate layers.
Comparable results are also obtained not only withhealthy enamel but also in the presence of interactionwith demineralized initial lesions (Fig. 9) and with thedentine surface.
Practical prophylaxis
Fig. 4:
Enamel surfacewith CaF2 globulesafter 1 min. oftreatment withelmex gel (mixedwith saliva 1:1,SEM)
Fig. 5:
CaF2 precipitateson an enamelsurface after 6 min.of treatment withelmex dental rinse(SEM)
Fig. 6
CaF2 precipitateson a dentinesurface brushedwith elmex Sensitivetoothpaste (2 min.,mixed with saliva1:1, SEM)
Fig. 8: Cross-section of a fluoridated dental enamel surface(TEM)
Fig. 7: Production and removal of a electron beam-transparent lamella for TEM analysis, prepared using thefocused ion beam (FIB) technique
PROPHYLAXISdialogue
The nanospot EDX analysis of the atomic-levelchemical structure of the fluoride globules that can alsobe performed in TEM typically shows values of about50 atomic % fluoride plus integration of, for instance,phosphates (Petzold et al. 2004, Petzold 2001).Compared to this, either no fluoride accumulation atall, or amounts within the measurement uncertaintyrange only, are found in the immediately adjacentenamel (less than approx. 1%). Direct conversion of thedental enamel into fluoroapatite as a result of a singleexposure to fluoridation can therefore be consideredunlikely.
To assume the role of a fluoride reservoir, the fluo-ride globules that have formed on the dental surfacemust not only show a high fluoride concentration, theymust also demonstrate sufficiently stable retentionproperties under mechanical and chemical stress loads.To investigate the stability of CaF2 precipitates on thetooth surface, enamel samples were first fluoridated ina test tube, then placed in orthodontic apparatuses insitu in the oral cavity.
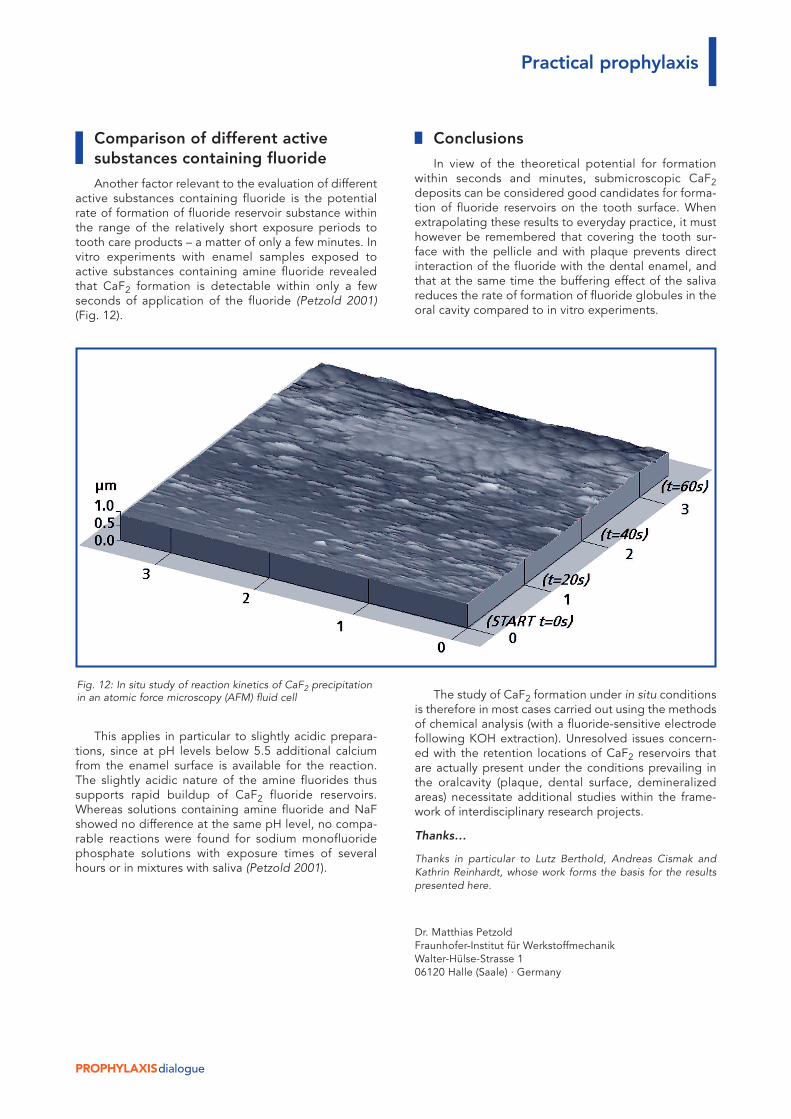
The SEM analysis (Fig. 10) shows the condition ofsuch a sample thus “worn” for 10 days. The lossof some CaF2 is recognizable, but the presence offluoride precipitates is still demonstrable (Petzold et al.2004).
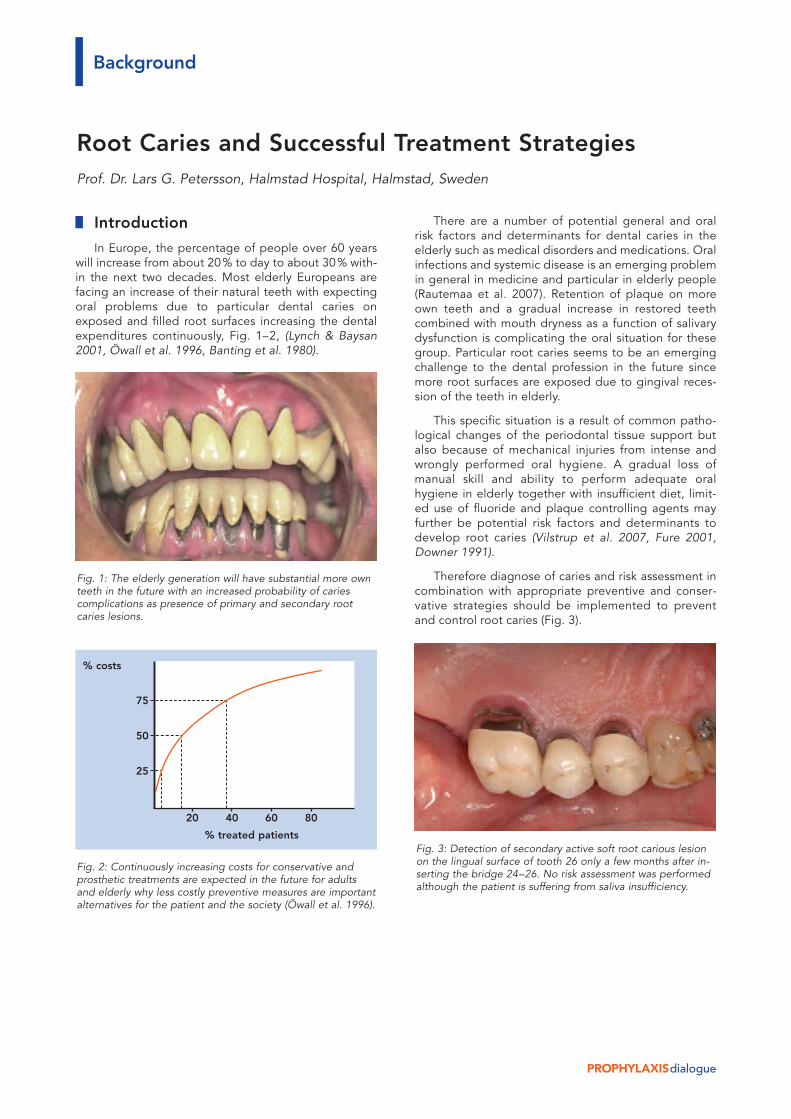
A high level of stability was also determined undermechanical stress with a toothbrush (Fig. 11).
A number of questions concerned with the solubilityand reactivity of precipitates containing fluoride remainto be resolved in view of potential interactions with theoral environment, resulting for example in adsorption ofproteins and/or phosphates on the surface (Rölla &Ekstrand 1996).
Practical prophylaxis
Fig. 10: In vitro fluoridated dental enamel sample, residualCaF2 precipitates after exposure for 10 days in an in situexperiment
Fig. 11 SEM image of a fluoridated enamel surface withCaF2 precipitates following frictional contact with a tooth-brush filament (bottom right)
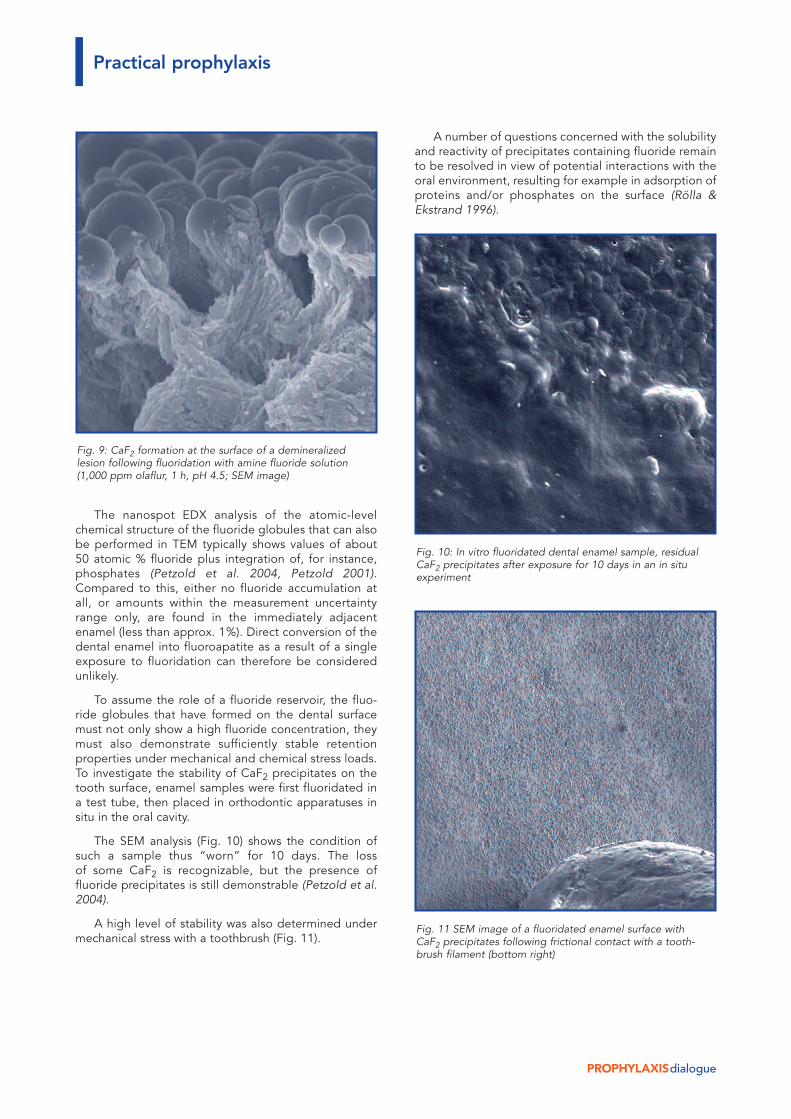
Fig. 9: CaF2 formation at the surface of a demineralizedlesion following fluoridation with amine fluoride solution(1,000 ppm olaflur, 1 h, pH 4.5; SEM image)
PROPHYLAXISdialogue
Comparison of different activesubstances containing fluoride
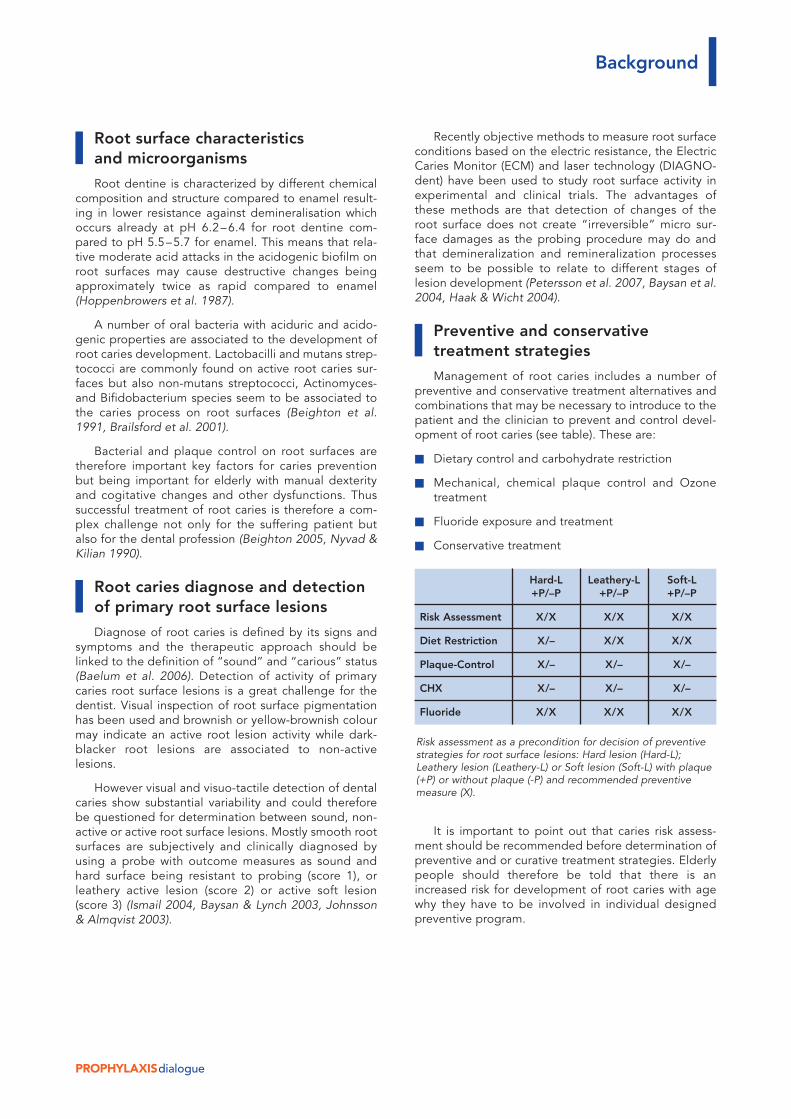
Another factor relevant to the evaluation of differentactive substances containing fluoride is the potentialrate of formation of fluoride reservoir substance withinthe range of the relatively short exposure periods totooth care products – a matter of only a few minutes. Invitro experiments with enamel samples exposed toactive substances containing amine fluoride revealedthat CaF2 formation is detectable within only a fewseconds of application of the fluoride (Petzold 2001)(Fig. 12).
This applies in particular to slightly acidic prepara-tions, since at pH levels below 5.5 additional calciumfrom the enamel surface is available for the reaction.The slightly acidic nature of the amine fluorides thussupports rapid buildup of CaF2 fluoride reservoirs.Whereas solutions containing amine fluoride and NaFshowed no difference at the same pH level, no compa-rable reactions were found for sodium monofluoridephosphate solutions with exposure times of severalhours or in mixtures with saliva (Petzold 2001).
Conclusions
In view of the theoretical potential for formationwithin seconds and minutes, submicroscopic CaF2deposits can be considered good candidates for forma-tion of fluoride reservoirs on the tooth surface. Whenextrapolating these results to everyday practice, it musthowever be remembered that covering the tooth sur-face with the pellicle and with plaque prevents directinteraction of the fluoride with the dental enamel, andthat at the same time the buffering effect of the salivareduces the rate of formation of fluoride globules in theoral cavity compared to in vitro experiments.
The study of CaF2 formation under in situ conditionsis therefore in most cases carried out using the methodsof chemical analysis (with a fluoride-sensitive electrodefollowing KOH extraction). Unresolved issues concern-ed with the retention locations of CaF2 reservoirs thatare actually present under the conditions prevailing inthe oralcavity (plaque, dental surface, demineralizedareas) necessitate additional studies within the frame-work of interdisciplinary research projects.
Thanks…
Thanks in particular to Lutz Berthold, Andreas Cismak andKathrin Reinhardt, whose work forms the basis for the resultspresented here.
Dr. Matthias PetzoldFraunhofer-Institut für WerkstoffmechanikWalter-Hülse-Strasse 106120 Halle (Saale) · Germany
Practical prophylaxis
Fig. 12: In situ study of reaction kinetics of CaF2 precipitationin an atomic force microscopy (AFM) fluid cell
Introduction
In Europe, the percentage of people over 60 yearswill increase from about 20% to day to about 30% with-in the next two decades. Most elderly Europeans arefacing an increase of their natural teeth with expectingoral problems due to particular dental caries onexposed and filled root surfaces increasing the dentalexpenditures continuously, Fig. 1–2, (Lynch & Baysan2001, Öwall et al. 1996, Banting et al. 1980).
PROPHYLAXISdialogue
There are a number of potential general and oralrisk factors and determinants for dental caries in theelderly such as medical disorders and medications. Oralinfections and systemic disease is an emerging problemin general in medicine and particular in elderly people(Rautemaa et al. 2007). Retention of plaque on moreown teeth and a gradual increase in restored teethcombined with mouth dryness as a function of salivarydysfunction is complicating the oral situation for thesegroup. Particular root caries seems to be an emergingchallenge to the dental profession in the future sincemore root surfaces are exposed due to gingival reces-sion of the teeth in elderly.
This specific situation is a result of common patho-logical changes of the periodontal tissue support butalso because of mechanical injuries from intense andwrongly performed oral hygiene. A gradual loss ofmanual skill and ability to perform adequate oralhygiene in elderly together with insufficient diet, limit-ed use of fluoride and plaque controlling agents mayfurther be potential risk factors and determinants todevelop root caries (Vilstrup et al. 2007, Fure 2001,Downer 1991).
Therefore diagnose of caries and risk assessment incombination with appropriate preventive and conser-vative strategies should be implemented to preventand control root caries (Fig. 3).
Background
Root Caries and Successful Treatment StrategiesProf. Dr. Lars G. Petersson, Halmstad Hospital, Halmstad, Sweden
Fig. 1: The elderly generation will have substantial more ownteeth in the future with an increased probability of cariescomplications as presence of primary and secondary rootcaries lesions.
Fig. 2: Continuously increasing costs for conservative andprosthetic treatments are expected in the future for adultsand elderly why less costly preventive measures are importantalternatives for the patient and the society (Öwall et al. 1996).
Fig. 3: Detection of secondary active soft root carious lesionon the lingual surface of tooth 26 only a few months after in-serting the bridge 24–26. No risk assessment was performedalthough the patient is suffering from saliva insufficiency.
75
50
25
20 40 60 80
% treated patients
% costs
PROPHYLAXISdialogue
Root surface characteristicsand microorganisms
Root dentine is characterized by different chemicalcomposition and structure compared to enamel result-ing in lower resistance against demineralisation whichoccurs already at pH 6.2–6.4 for root dentine com-pared to pH 5.5–5.7 for enamel. This means that rela-tive moderate acid attacks in the acidogenic biofilm onroot surfaces may cause destructive changes beingapproximately twice as rapid compared to enamel(Hoppenbrowers et al. 1987).
A number of oral bacteria with aciduric and acido-genic properties are associated to the development ofroot caries development. Lactobacilli and mutans strep-tococci are commonly found on active root caries sur-faces but also non-mutans streptococci, Actinomyces-and Bifidobacterium species seem to be associated tothe caries process on root surfaces (Beighton et al.1991, Brailsford et al. 2001).
Bacterial and plaque control on root surfaces aretherefore important key factors for caries preventionbut being important for elderly with manual dexterityand cogitative changes and other dysfunctions. Thussuccessful treatment of root caries is therefore a com-plex challenge not only for the suffering patient butalso for the dental profession (Beighton 2005, Nyvad &Kilian 1990).
Root caries diagnose and detectionof primary root surface lesions
Diagnose of root caries is defined by its signs andsymptoms and the therapeutic approach should belinked to the definition of “sound” and “carious” status(Baelum et al. 2006). Detection of activity of primarycaries root surface lesions is a great challenge for thedentist. Visual inspection of root surface pigmentationhas been used and brownish or yellow-brownish colourmay indicate an active root lesion activity while dark-blacker root lesions are associated to non-activelesions.
However visual and visuo-tactile detection of dentalcaries show substantial variability and could thereforebe questioned for determination between sound, non-active or active root surface lesions. Mostly smooth rootsurfaces are subjectively and clinically diagnosed byusing a probe with outcome measures as sound andhard surface being resistant to probing (score 1), orleathery active lesion (score 2) or active soft lesion(score 3) (Ismail 2004, Baysan & Lynch 2003, Johnsson& Almqvist 2003).
Recently objective methods to measure root surfaceconditions based on the electric resistance, the ElectricCaries Monitor (ECM) and laser technology (DIAGNO-dent) have been used to study root surface activity inexperimental and clinical trials. The advantages ofthese methods are that detection of changes of theroot surface does not create “irreversible” micro sur-face damages as the probing procedure may do andthat demineralization and remineralization processesseem to be possible to relate to different stages oflesion development (Petersson et al. 2007, Baysan et al.2004, Haak & Wicht 2004).
Preventive and conservativetreatment strategies
Management of root caries includes a number ofpreventive and conservative treatment alternatives andcombinations that may be necessary to introduce to thepatient and the clinician to prevent and control devel-opment of root caries (see table). These are:
W Dietary control and carbohydrate restriction
W Mechanical, chemical plaque control and Ozonetreatment
W Fluoride exposure and treatment
W Conservative treatment
It is important to point out that caries risk assess-ment should be recommended before determination ofpreventive and or curative treatment strategies. Elderlypeople should therefore be told that there is anincreased risk for development of root caries with agewhy they have to be involved in individual designedpreventive program.
Background
Risk assessment as a precondition for decision of preventivestrategies for root surface lesions: Hard lesion (Hard-L);Leathery lesion (Leathery-L) or Soft lesion (Soft-L) with plaque(+P) or without plaque (-P) and recommended preventivemeasure (X).
Hard-L Leathery-L Soft-L+P/–P +P/–P +P/–P
Risk Assessment X/X X/X X/X
Diet Restriction X/– X/X X/X
Plaque-Control X/– X/– X/–
CHX X/– X/– X/–
Fluoride X/X X/X X/X

PROPHYLAXISdialogue
Dietary control and carbohydratesrestriction
The role of dietary control of caries promoting foodand drinks is essential to limit the number of cariesassociated bacteria in the dental plaque. Since root sur-faces are more sensitive to acid demineralization com-pare to enamel surfaces, intake of food or drinks witheven moderate content of carbohydrates should berestricted in order to avoid development caries in thesetooth sites. Many elderly are also depending on intakeof medical drugs, which often interfere with salivarysecretion and saliva buffer capacity creating salivaryinsufficiency, which slow down salivary glucose clear-ance and promote the development of caries associat-ed bacteria in the dental plaque (Beighton 2005,Lundgren 1997).
Replacing sugar rich “sweeteners” with non-caloric“sweeteners” e.g. Cyclamate can be recommendedsince these intense “sweeteners” do not contribute toacid production in the dental plaque. Bulk caloric“sweeteners” as Xylitol is recommended in productsinstead of sugar, since it shows almost total inhibition ofacid production from oral bacteria associated to dentalcaries. Sorbitol, another caloric sugar alcohol may, incontrast to Xylitol, be contributing to acid production inthe dental plaque in patients with salivary insufficiency,why daily intake of food and sweets containing Sorbitolshould be avoided in these patients (Moynihan et al.2003, Kalfas et al. 1990).
Mechanical plaque control
Oral hygiene resulting in adequate personal/profes-sional regular plaque control is a cornerstone to controlgingivitis/periodontitis and dental caries. Plaque con-trol can be effectuated either mechanically with manualor electric tooth brushing or chemically using differentantibacterial agents. Recent studies and reviews favourthe use of electric tooth brushing for plaque control;however the use of electric tooth brushing needsadequate oral use instructions by professionals in orderto show effectiveness and minimize side effects such asretraction of protecting gingival soft tissues (Sbu 2007,Axelsson et al. 2004, Heanie et al. 2003, Sicilia et al.2002). Regular professional tooth cleaning with oralhygiene instructions at 3 months interval combinedwith good home bound care seem to be effective tocontrol cariogenic microbiota of exposed root surfaces.In this context, the use of chlorhexidine or fluoride didnot show additional benefit to these regimens (Bizhanget al. 2007).
Chemical plaque control(Chlorhexidine) and Ozone treatment
Chemical plaque control is a further preventivemeasure that can be used to control root caries devel-opment. Different chemical agents can reduce bacteriaand plaque levels through either inhibition of microbialcolonization, microbial growth and metabolism but alsomodify the ecology and biochemistry of the biofim onthe teeth. Anti-plaque agents may be administrated indifferent vehicles, i.e. dentifrice, mouth rinse, varnishes,gel, spay, chewing gum and permanent sustained ve-hicles (Scheie 2003). In general cationic agents (chlor-hexidine/CHX) are more potent than anionic agentsand other antimicrobial agents. Suppression of rootcaries associated bacteria has been shown after treat-ment with CHX-varnishes with varying composition andconcentrations (Matthijs & Adriaens 2002).
Studies by Huizinga et al. (1990), Lynch & Beighton(1993) and Ekenback et al. (2000) show that CHX-varnish treatment of root surfaces are effective butshould be repeated at regular intervals. Twetman(2004), in a review article, points out that CHX-rinses incombination with fluoride varnish showed weak effecton root caries development in elderly.
There is a diminished effect of CHX on dentalplaque that reinforces the necessity of disruption ofstructured biofilm before treatment with CHX (Zanattaet al, 2007). Such an effect may favour “surfactants”with low molecular weight e.g. Delmopinol, that pri-marily is interfering with adhesion of the biofilm to thetooth surface (Addy et al. 2007, Scheie 2003).
Alternative pharmaceuticals approach includingphenol compounds, metal ions quaternary ammonium,plant extracts, essential oils, peroxide enzymes andpolymers have been suggested) but their long termeffect on root caries is uncertain and limited studied(Lynch & Baysan 2003).
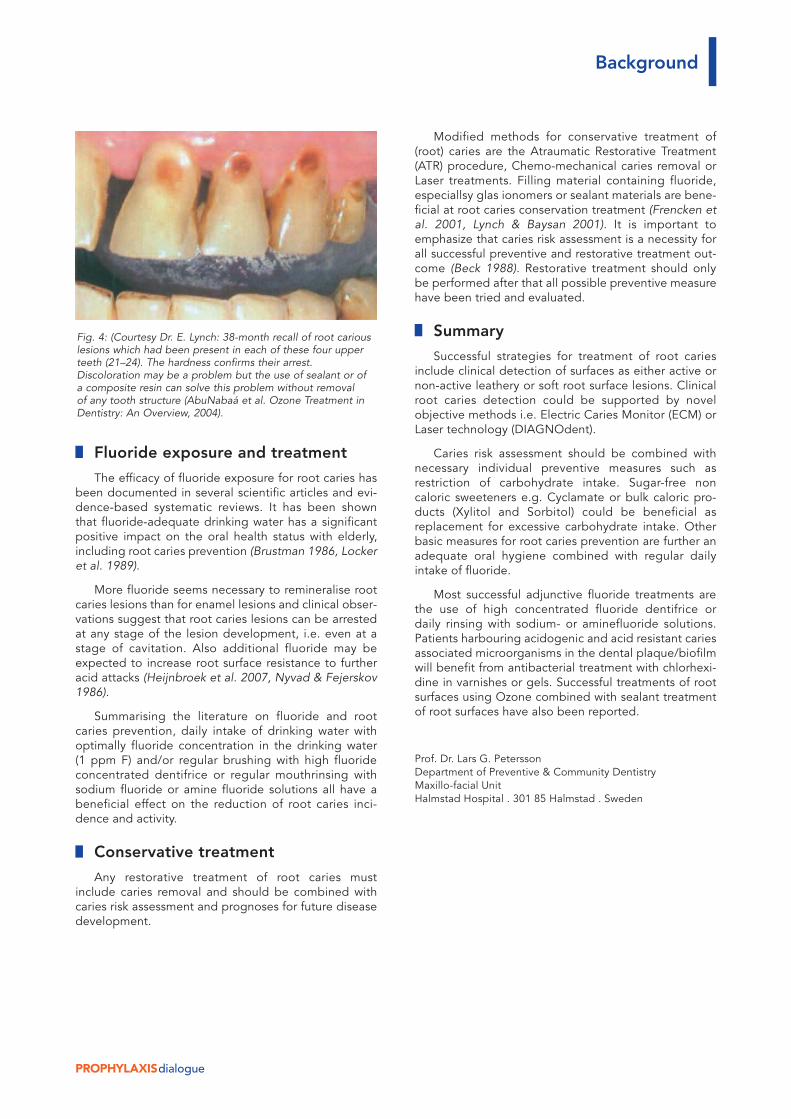
Ozone treatment in dentistry has gained anincreased interest in recent years and studies haveshown that Ozone application can reverse primary rootcaries lesions significantly (Baysan & Lynch 2007,AbuNabaá et al. 2004, Holms 2003, Baysan et al. 2001)(Fig. 4).
Use of sealants over Ozone remineralized rootcaries has been studied with success and may be a fur-ther strategy to improve treatment of root caries(Baysan & Lynch 2004).
Background
PROPHYLAXISdialogue
Fluoride exposure and treatment
The efficacy of fluoride exposure for root caries hasbeen documented in several scientific articles and evi-dence-based systematic reviews. It has been shownthat fluoride-adequate drinking water has a significantpositive impact on the oral health status with elderly,including root caries prevention (Brustman 1986, Lockeret al. 1989).
More fluoride seems necessary to remineralise rootcaries lesions than for enamel lesions and clinical obser-vations suggest that root caries lesions can be arrestedat any stage of the lesion development, i.e. even at astage of cavitation. Also additional fluoride may beexpected to increase root surface resistance to furtheracid attacks (Heijnbroek et al. 2007, Nyvad & Fejerskov1986).
Summarising the literature on fluoride and rootcaries prevention, daily intake of drinking water withoptimally fluoride concentration in the drinking water(1 ppm F) and/or regular brushing with high fluorideconcentrated dentifrice or regular mouthrinsing withsodium fluoride or amine fluoride solutions all have abeneficial effect on the reduction of root caries inci-dence and activity.
Conservative treatment
Any restorative treatment of root caries mustinclude caries removal and should be combined withcaries risk assessment and prognoses for future diseasedevelopment.
Modified methods for conservative treatment of(root) caries are the Atraumatic Restorative Treatment(ATR) procedure, Chemo-mechanical caries removal orLaser treatments. Filling material containing fluoride,especiallsy glas ionomers or sealant materials are bene-ficial at root caries conservation treatment (Frencken etal. 2001, Lynch & Baysan 2001). It is important toemphasize that caries risk assessment is a necessity forall successful preventive and restorative treatment out-come (Beck 1988). Restorative treatment should onlybe performed after that all possible preventive measurehave been tried and evaluated.
Summary
Successful strategies for treatment of root cariesinclude clinical detection of surfaces as either active ornon-active leathery or soft root surface lesions. Clinicalroot caries detection could be supported by novelobjective methods i.e. Electric Caries Monitor (ECM) orLaser technology (DIAGNOdent).
Caries risk assessment should be combined withnecessary individual preventive measures such asrestriction of carbohydrate intake. Sugar-free noncaloric sweeteners e.g. Cyclamate or bulk caloric pro-ducts (Xylitol and Sorbitol) could be beneficial asreplacement for excessive carbohydrate intake. Otherbasic measures for root caries prevention are further anadequate oral hygiene combined with regular dailyintake of fluoride.
Most successful adjunctive fluoride treatments arethe use of high concentrated fluoride dentifrice ordaily rinsing with sodium- or aminefluoride solutions.Patients harbouring acidogenic and acid resistant cariesassociated microorganisms in the dental plaque/biofilmwill benefit from antibacterial treatment with chlorhexi-dine in varnishes or gels. Successful treatments of rootsurfaces using Ozone combined with sealant treatmentof root surfaces have also been reported.
Prof. Dr. Lars G. PeterssonDepartment of Preventive & Community DentistryMaxillo-facial UnitHalmstad Hospital . 301 85 Halmstad . Sweden
Background
Fig. 4: (Courtesy Dr. E. Lynch: 38-month recall of root cariouslesions which had been present in each of these four upperteeth (21–24). The hardness confirms their arrest.Discoloration may be a problem but the use of sealant or ofa composite resin can solve this problem without removalof any tooth structure (AbuNabaá et al. Ozone Treatment inDentistry: An Overview, 2004).
PROPHYLAXISdialogue
Aim
To assess the effect of daily use of a dental rinsecontaining amine fluoride (AmF), in addition to AmF-containing toothpaste, on primary root carious lesionsin adults with an increased caries risk.
Trial conditions
Products under investigation
Group 1: elmex SENSITIVE toothpaste(1400 ppm F– from AmF)+ elmex SENSITIVE dental rinse(250 ppm F– from AmF/KF)
Group 2: elmex SENSITIVE toothpaste(1400 ppm F– from AmF)+ Placebo dental rinse (no fluoride)
Participants
70 subjects (male and female, aged 55 to 81 years)with at least two primary root caries lesions wereenrolled in this double-blind, parallel-group study.
Method
The Electrical Caries Monitor (ECM) was used tomeasure the remineralisation based on the differ-ences of electrical conductivity between hard andcarious soft or leathery primary root caries lesions.Differences between the groups were assessedusing Mann-Whitney- and signed-rank tests.
Trial
Subjects were randomly allocated to two groups(each n = 35). At baseline, the primary root carieslesions were classifed as hard (non active), leathery orsoft (both active) on clinical examination. Subjects inGroup 1 brushed their teeth twice daily with elmexSENSITIVES toothpaste and rinsed twice daily withelmex SENSITIVE dental rinse for 12 months. Subjectsin Group 2 used the same toothpaste but rinsed with aplacebo solution without fluoride. Electrical resistanceof selected lesions showing the altering of the porositesin the carious process was measured at baseline andafter 3, 6, 9 and 12 months, using an electronic cariesmonitor (ECM).
Results
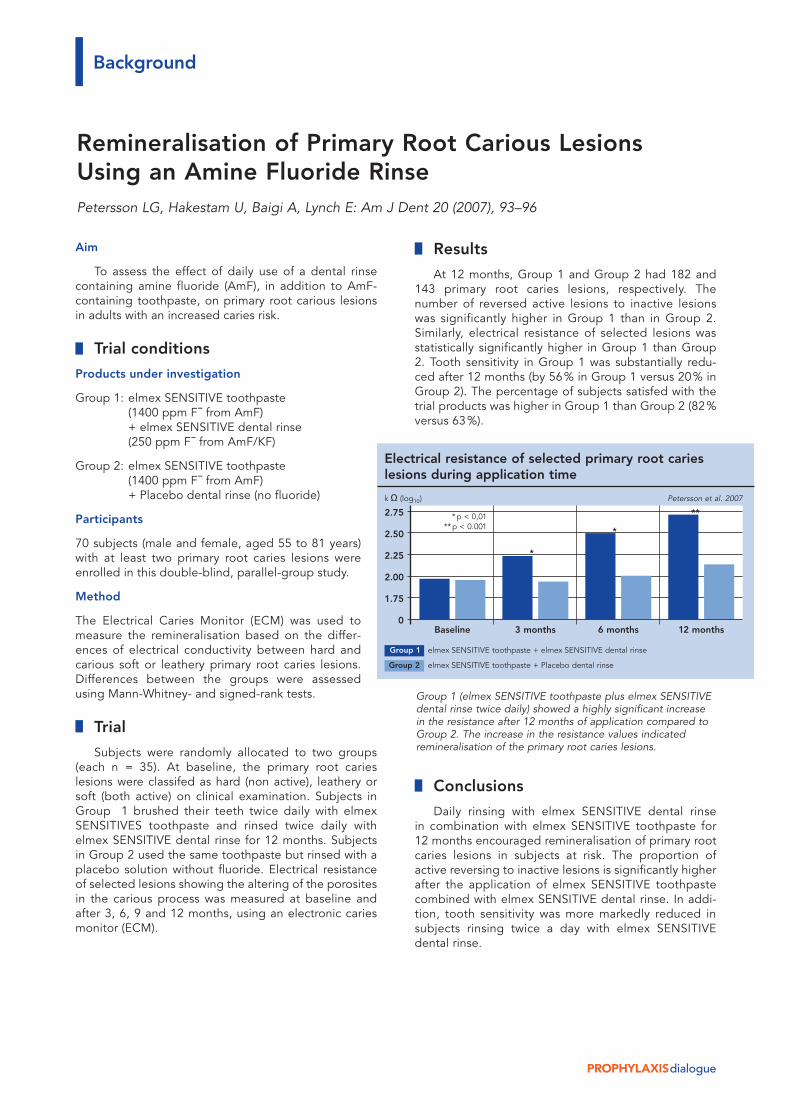
At 12 months, Group 1 and Group 2 had 182 and143 primary root caries lesions, respectively. Thenumber of reversed active lesions to inactive lesionswas significantly higher in Group 1 than in Group 2.Similarly, electrical resistance of selected lesions wasstatistically significantly higher in Group 1 than Group2. Tooth sensitivity in Group 1 was substantially redu-ced after 12 months (by 56% in Group 1 versus 20% inGroup 2). The percentage of subjects satisfed with thetrial products was higher in Group 1 than Group 2 (82%versus 63%).
Conclusions
Daily rinsing with elmex SENSITIVE dental rinsein combination with elmex SENSITIVE toothpaste for12 months encouraged remineralisation of primary rootcaries lesions in subjects at risk. The proportion ofactive reversing to inactive lesions is significantly higherafter the application of elmex SENSITIVE toothpastecombined with elmex SENSITIVE dental rinse. In addi-tion, tooth sensitivity was more markedly reduced insubjects rinsing twice a day with elmex SENSITIVEdental rinse.
Background
Remineralisation of Primary Root Carious LesionsUsing an Amine Fluoride RinsePetersson LG, Hakestam U, Baigi A, Lynch E: Am J Dent 20 (2007), 93–96
Group 1 (elmex SENSITIVE toothpaste plus elmex SENSITIVEdental rinse twice daily) showed a highly significant increasein the resistance after 12 months of application compared toGroup 2. The increase in the resistance values indicatedremineralisation of the primary root caries lesions.
Electrical resistance of selected primary root carieslesions during application time
Group 1 elmex SENSITIVE toothpaste + elmex SENSITIVE dental rinse
Group 2 elmex SENSITIVE toothpaste + Placebo dental rinse
k Ω (log10) Petersson et al. 2007
2.75
2.50
2.25
2.00
1.75
0Baseline 3 months 6 months 12 months
*
*
***p < 0,01**p < 0.001
Relative Dentin Abrasion(RDA) of ToothpastesProf. Dr. Thomas Imfeld, University of Zurich,Suisse
Effect and side effects of oralhygiene
The population's growing awareness of health, oralhygiene education in schools, intense television com-mercials from cosmetic manufacturers and countlessarticles in periodicals and journals about the correlationbetween oral hygiene and the health of teeth and gumshave been fruitful. The prevalence of caries hasdropped by about 90% in the last 40 years. At the sametime, the aesthetic demands on teeth have alsochanged. A brilliant white, natural bite and healthygums have become desirable goals.
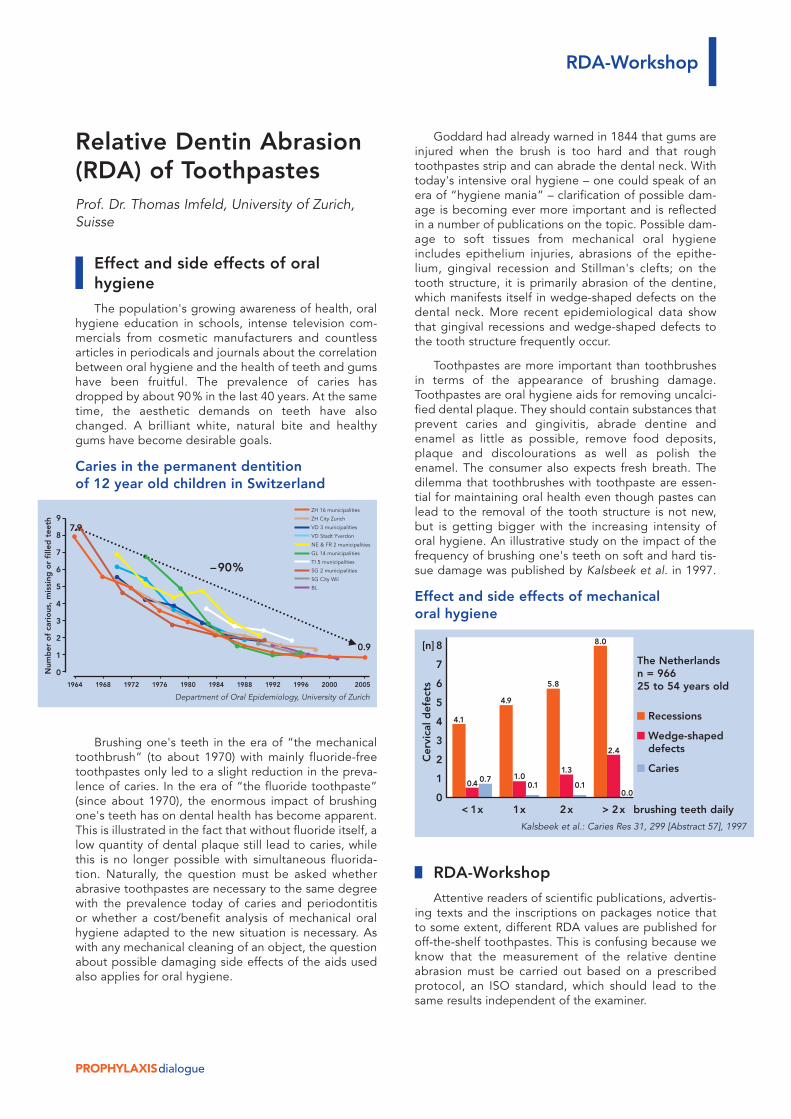
Caries in the permanent dentitionof 12 year old children in Switzerland
Brushing one's teeth in the era of “the mechanicaltoothbrush” (to about 1970) with mainly fluoride-freetoothpastes only led to a slight reduction in the preva-lence of caries. In the era of “the fluoride toothpaste”(since about 1970), the enormous impact of brushingone's teeth has on dental health has become apparent.This is illustrated in the fact that without fluoride itself, alow quantity of dental plaque still lead to caries, whilethis is no longer possible with simultaneous fluorida-tion. Naturally, the question must be asked whetherabrasive toothpastes are necessary to the same degreewith the prevalence today of caries and periodontitisor whether a cost/benefit analysis of mechanical oralhygiene adapted to the new situation is necessary. Aswith any mechanical cleaning of an object, the questionabout possible damaging side effects of the aids usedalso applies for oral hygiene.
Goddard had already warned in 1844 that gums areinjured when the brush is too hard and that roughtoothpastes strip and can abrade the dental neck. Withtoday's intensive oral hygiene – one could speak of anera of “hygiene mania” – clarification of possible dam-age is becoming ever more important and is reflectedin a number of publications on the topic. Possible dam-age to soft tissues from mechanical oral hygieneincludes epithelium injuries, abrasions of the epithe-lium, gingival recession and Stillman's clefts; on thetooth structure, it is primarily abrasion of the dentine,which manifests itself in wedge-shaped defects on thedental neck. More recent epidemiological data showthat gingival recessions and wedge-shaped defects tothe tooth structure frequently occur.
Toothpastes are more important than toothbrushesin terms of the appearance of brushing damage.Toothpastes are oral hygiene aids for removing uncalci-fied dental plaque. They should contain substances thatprevent caries and gingivitis, abrade dentine andenamel as little as possible, remove food deposits,plaque and discolourations as well as polish theenamel. The consumer also expects fresh breath. Thedilemma that toothbrushes with toothpaste are essen-tial for maintaining oral health even though pastes canlead to the removal of the tooth structure is not new,but is getting bigger with the increasing intensity oforal hygiene. An illustrative study on the impact of thefrequency of brushing one's teeth on soft and hard tis-sue damage was published by Kalsbeek et al. in 1997.
Effect and side effects of mechanicaloral hygiene
RDA-Workshop
Attentive readers of scientific publications, advertis-ing texts and the inscriptions on packages notice thatto some extent, different RDA values are published foroff-the-shelf toothpastes. This is confusing because weknow that the measurement of the relative dentineabrasion must be carried out based on a prescribedprotocol, an ISO standard, which should lead to thesame results independent of the examiner.
PROPHYLAXISdialogue
RDA-Workshop
Cer
vica
l def
ects
[n] 8
7
6
5
4
3
2
1
0
4.1
0.4 0.7
4.9
1.00.1
5.8
1.3
0.1
8.0
2.4
0.0
Kalsbeek et al.: Caries Res 31, 299 [Abstract 57], 1997
The Netherlandsn = 96625 to 54 years old
Recessions
Wedge-shapeddefects
Caries
< 1x 1x 2x > 2x brushing teeth daily
ZH 16 municipalities
ZH City Zurich
VD 3 municipalities
VD Stadt Yverdon
NE & FR 2 municipalities
GL 14 municipalities
TI 5 municipalities
SG 2 municipalities
SG City Wil
BL
Num
ber
of
cari
ous
, m
issi
ng o
r fi
lled
tee
th 9
8
7
6
5
4
3
2
1
0
0.9
–90%
Department of Oral Epidemiology, University of Zurich
1964 1968 1972 1976 1980 1984 1988 1992 1996 2000 2005
7.9

PROPHYLAXISdialogue
GABA International AG therefore thankfully organ-ised an RDA workshop devoted to the problem on 15June 2007 in Frankfurt am Main, Germany. The work-shop was moderated by Dr. Andrea Engl, EuropeanStudy Manager, Scientific Affairs, GABA Internationaland Dr. Christiane Spiegelhalder, Head ScientificAffairs, GABA International. Participants included Prof.Martin Addy, Bristol University, Prof. Christoph Dörfer,University of Kiel, Prof. Roger Ellwood, DirectorColgate-Palmolive Dental Health Unit, Manchester, Dr.Christine Garbers, Head Research and Development,GABA International, Dr. Carlos Gonzalez, DirectorLaboratory Research Facilities, Indiana University, Prof.John Hefferren, University of Kansas, Prof. ThomasImfeld, University of Zurich, Frau Bärbel Kiene, HeadScientific Affairs, GABA Deutschland, Dr. Jim Masters,Associate Director of Technology, Colgate-Palmolive,Piscataway and Dr. Cornelia Scheffel, Head Devel-opment, GABA International.
Particularly enlightening was the comparison of thetesting methods of the three primary RDA laboratoriesIndiana, Missouri and Zurich, which all work in accor-dance with ISO standard 11609: 1995 (E), the actual“recipe” for RDA measurements. However, whetherthree independent cooks, who prepare a meal from thesame cookbook, serve identical dishes primarilydepends on the detail and accuracy of the recipe. Adetailed recipe is required for success. The aforemen-tioned ISO standard for the RDA measurement is notvery precise, which is why different laboratories pro-duce different results.
Here is a brief description of the RDA measurementfor better understanding. The dental roots are irradiat-ed with high energy resulting in the unstable radioac-tive phosphorus isotope 32P and gamma radiation fromthe phosphate of the tooth structure. The dental rootsare then embedded and brushed on a brush machinefor a standardised period of time with standardised hor-izontal movements and standardised application force.Manual toothbrushes with planar bristle fields are usedas test brushes. Brushing media are slurries of thetoothpastes to be tested and a slurry with a standardabrasive.
The brushing passes are performed in the “sand-wich technique”. A pass is made with the standard slur-ry, then with a slurry of the test paste and then anotherpass with the standard slurry. The radiation activity of32P is measured after each brushing pass. A 32P con-centration in the slurry after brushing is the result oftooth substance abrasion. The values of the two stan-dard slurries of each sandwich pass are averaged andthe result set to 100. The relative dentine abrasion ofthe intermediate test paste used is expressed in per-cent of the standard value. This percentage value is theRDA figure.
Many steps of this measuring method are notdescribed in detail in the ISO standard. For example,neither the irradiation type nor duration of the dentinesamples is specifically defined. Only an intensity ofapprox. 1mCurie 32P β-radiation is called for after somehours. The description of test brushes is inexact. Itshould be a nylon brush preferably with a planar bristlefield of approx. 10mm long bristles. Fluctuations in theabrasivity of the standard up to 10% were reported.The number of measurements that may be taken withone dental root is not prescribed. The technique formeasuring the radiation activity is also left to the indi-vidual laboratories.
However, it would be wrong to draw the conclusionfrom the aforementioned that RDA values make nosense. One should be much more aware of the fact thatrelative values (within one and the same study) are atissue. In other words, one should only compare values,which originate from the same laboratory. RDA valuesfrom different laboratories cannot be compared direct-ly. However, the problem for dentists and dentalhygienists is the fact that it is usually not specified withnumerical data of the RDA value from which test labora-tory the values originate.
Measuring the relative dentine abrasion of a tooth-paste in the laboratory captures the “worst case”. Indaily life, the potential for damage of the measuredabrasivity is influenced by several other factors such asthe type of toothbrush used, frequency of brushing,brushing technique, brushing duration and applicationforce, composition of the toothpaste in addition to theabrasive particles, etc. In extreme cases, a very abrasivetoothpaste is not harmful if used very rarely, briefly andwith little force. The caries-protective effect of a fluori-date toothpaste ultimately depends on the frequencyof its use. However, the fact is that today's normal con-sumer cleans and scrubs his or her teeth frequently,with primarily horizontal movements and with too muchforce.
Assessment of the well-organised and very interest-ing workshop is currently under way and a publica-tion should be submitted in December 2007. In themean time, interlaboratory comparisons have beenperformed and clarifications made in the laboratorieslocally. The results of all this work will flow into a a refor-mulation of the ISO standard for measuring the relativedentine abrasion of toothpastes. A new standard abra-sive will be provided, which will be used in the future byall test laboratories. It can be assumed that this will leadto improved comparability and that RDA values fromtoothpastes can be used in the near future withoutuncertainty for the individual care of patients.
RDA-Workshop

PROPHYLAXISdialogue
Fluorides play an important role in the prevention ofmilk tooth caries. Of crucial importance are fluoridatedchildren's toothpastes. Such toothpastes normally havea fluoride concentration of 250–500 ppm. Dentists anddental experts recommend that brushing start uponeruption of the first milk tooth.
Although the scientific discussion in regards to theimportance of fluoride in consideration of all relevantgroups (e.g. various dental and paediatric organisa-tions) has taken place and with the creation and adop-tion of the fluoride guidelines in April 2006, more andmore inaccurate and misleading statements regardingmilk tooth care and fluoridation from children's tooth-paste can be heard – even the recommendation toavoid toothpaste in small children entirely until threeyears of age.
Finally, a medium for paediatricians published suchan article in April 2007. Responding to the previous sci-entific discussion and its results, however, one did notwant to engage oneself with an article from a dentalperspective or even just a letter to the editor. It isregrettable that reckless recommendations, whichcould cause long-term injury to their small patients,may be possible due to misleading information frompaediatricians.
The undeniable fact is that the preventative effect offluoridated children's toothpastes is based on the actu-al mechanical removal of dental plaque in combinationwith the application of fluoride ions on tooth surfacesby the parents after the first milk tooth (Borutta et al.2006, Heyduck et al. 2006, Kneist et al. 2006). The useof fluoridated toothpastes is an important part of theevidence-based fluoride guidelines agreed on in April2006 between all relevant groups (www.zzq-koeln.de >Guideline on fluoridation measures).
Based on the guidelines, a fluoride concentration of500 ppm represents a good compromise betweeneffectiveness and safety: Stookey et al. (2004), forexample, document in a study carried out over twoyears with nearly 1000 subjects a clear reduction incaries due to the use of fluoridated children's tooth-paste (500 ppm), which is similar in effectiveness interms of caries reduction for toothpastes with 1100ppm. Therefore, it is in no way correct that the effec-tiveness of fluoride-reduced children's toothpastes isnot clinically documented.
In contrast, Russel already showed in 1949 that fluo-ride after the tooth eruption must be applied externallyin order to maintain adequate protection against caries.In a clinical study in 1992, Reich et al. showed that thepreventative administration of fluoride tablets beforetooth eruption achieved no reduction in caries. Theeffectiveness of fluoride tablets in the phase, in whichthese tablets – usually in combination with vitamin D forrickets prophylaxis – are most often administered, iscertainly not documented.
In addition, a child's first few months of life repre-sent a critical phase in terms of the development ofdental fluoroses (Hong et al. 2006 a, b). The administra-tion of vitamin D monopreparations (without fluoride)for rickets prophylaxis from birth on and the start oflocal fluoridation measures for caries prophylaxis upontooth eruption thus represent a superior alternativeboth in terms of effectiveness and safety.
Unfounded is also the fear that the use of fluoridat-ed toothpastes could be dangerous for small childrenbecause ingestion tends to occur. In fact, it is true thatthe ingestion of children's toothpastes clearly fallsunder the “foreseeable use” specified in the Food andConsumer Products Code (LFBG): according to § 26 ofthe regulation, “for the manufacture or handling of cos-metics in a means other than suitable for proper orintended use to harm one's health” is prohibited.
In other words, manufacturers are legally required toalign the content and its concentrations with the behav-iour of the target group. Therefore, each ingredient isselected and verified in the safety assessment of chil-dren's toothpastes to ensure it does not lead to healthproblems when brushing (proper use) or when ingested(anticipated use). This rules out any hazard from quanti-ties of toothpaste ingested by children in the context ofbrushing.
There should still be no doubt about the effective-ness of preventing caries by removing plaque by caringfor the teeth of infants and small children. The fact isthat the thorough care of milk teeth from first eruptionis important in preventing damage to the deciduousdentition (Borutta et al. 2003, Kneist et al. 2006).
Current situation
Patient Injuries Through Phantom Discussion:Local fluoridation for small children scientifically substantiated
Dipl.-Biochem. Bärbel Kiene, Dr. Vanêssa de Moura Sieber, GABA GmbH, Lörrach, Germany

PROPHYLAXISdialogue
Because small children are unable to brush them-selves, it is the parent's responsibility to thoroughlycare for the milk teeth, then to monitor and instruct chil-dren in brushing their own teeth and finally, to rebrushtheir children's teeth as required (Ekstrand et al. 2000,Schidlowski et al. 2004, Splieth et al. 2004).
It is a fact that the development of caries is notentirely based on the lack of fluoride, i.e. the cause ofcaries is multifactorial and begins on the surface of theteeth (Hellwig et al. 1999, König 2001, Hellwig et al.2004, Borutta & Kneist 2006, Kneist et al. 2006). Thisapplies to both the erupting milk teeth as well as thepermanent teeth. In other words, the formation ofcaries from the first milk tooth can only be prevented byremoving microbial tooth plaque from the surfaces ofthe teeth mechanically (Borutta et al. 2002, Schidlowskiet al. 2004, Splieth et al. 2004).
In order to remove plaque from erupting milk teethmechanically, one needs a training toothbrush and fluo-ridated children's toothpaste. The fluorides in children'stoothpaste then come into contact with the surfaceof the milk teeth and promote the remineralisationprocesses on the spot (Hellwig et al. 2002). Fluorideions specifically affect the surfaces of the teeth locallyregardless of whether milk teeth or permanent teethare at issue (Hellwig & Lennon 2004, Stösser &Heinrich-Weltzien 2007).
The use of fluoridated toothpastes for caries pro-phylaxis is also viewed as a convenient, inexpensive,culturally accepted and widely used “ideal publichealth method” in international guidelines; fluoride-reduced children's toothpastes are also regarded inter-nationally as the basis of caries prevention (e.g. Oulis etal. 2000).
In conclusion, the use of inappropriate aids such ascotton swabs and water, as well as fluoridated chil-dren's toothpastes or even in general, brushing afterthe eruption of milk teeth has severe consequences onthe child's dentition and permanent teeth (Heyduck etal. 2006, Leroy et al. 2005) and thus have a negativeimpact throughout the child's life.
Current situation





























