Embed Size (px)
DESCRIPTION
SAS Journal - December 2010 (Vol. 4, Issue 4, Pages 122-128, DOI: 10.1016/j.esas.2010.09.001) Results at 24 months from the prospective, randomized, multicenter Investigational Device Exemption trial of ProDisc-C versus anterior cervical discectomy and fusion with 4-year follow-up and continued access patients. Rick B. Delamarter, Daniel Murrey, Michael E. Janssen, Jeffrey A. Goldstein, Jack Zigler, Bobby K.-B. Tay, Bruce Darden
Citation preview

A
BwToM6ipRfPaCm6CAl©
K
pm
S9
Available online at www.sciencedirect.com
SAS Journal 4 (2010) 122–128
1d
Cervical arthroplasty
Results at 24 months from the prospective, randomized, multicenterInvestigational Device Exemption trial of ProDisc-C versus
anterior cervical discectomy and fusion with 4-year follow-upand continued access patients
Rick B. Delamarter, MD a,*, Daniel Murrey, MD b, Michael E. Janssen, DO c,Jeffrey A. Goldstein, MD d, Jack Zigler, MD e, Bobby K-B Tay, MD f,
Bruce Darden II, MD b
a The Spine Center at Cedars-Sinai Medical Center, Los Angeles, CAb OrthoCarolina, PA, OrthoCarolina Spine Center, Charlotte, NC
c Center for Spinal Disorders, Thornton, COd New York University/Hospital for Joint Diseases, New York, NY
e Texas Back Institute, Plano, TXf Department of Orthopaedic Surgery, University of California San Francisco, San Francisco, CA
bstract
ackground: Cervical total disk replacement (TDR) is intended to address pain and preserve motion between vertebral bodies in patientsith symptomatic cervical disk disease. Two-year follow-up for the ProDisc-C (Synthes USA Products, LLC, West Chester, Pennsylvania)DR clinical trial showed non-inferiority versus anterior cervical discectomy and fusion (ACDF), showing superiority in many clinicalutcomes. We present the 4-year interim follow-up results.ethods: Patients were randomized (1:1) to ProDisc-C (PDC-R) or ACDF. Patients were assessed preoperatively, and postoperatively atweeks and 3, 6, 12, 18, 24, 36, and 48 months. After the randomized portion, continued access (CA) patients also underwent ProDisc-C
mplantation, with follow-up visits up to 24 months. Evaluations included Neck Disability Index (NDI), Visual Analog Scale (VAS) forain/satisfaction, and radiographic and physical/neurologic examinations.esults: Randomized patients (103 PDC-R and 106 ACDF) and 136 CA patients were treated at 13 sites. VAS pain and NDI score improvements
rom baseline were significant for all patients (P � .0001) but did not differ among groups. VAS satisfaction was higher at all time points forDC-R versus ACDF patients (P � .0499 at 48 months). The percentage of patients who responded yes to surgery again was 85.6% at 24 monthsnd 88.9% at 48 months in the PDC-R group, 80.9% at 24 months and 81.0% at 48 months in the ACDF group, and 86.3% at 24 months in theA group. Five PDC-R patients (48 months) and no CA patients (24 months) had index-level bridging bone. By 48 months, approximately 4-foldore ACDF patients required secondary surgery (3 of 103 PDC-R patients [2.9%] vs 12 of 106 ACDF patients [11.3%], P � .0292). Of these,ACDF patients (5.6%) required procedures at adjacent levels. Three CA patients required secondary procedures (24 months).onclusions: Our 4-year data support that ProDisc-C TDR and ACDF are viable surgical options for symptomatic cervical disk disease.lthough ACDF patients may be at higher risk for additional surgical intervention, patients in both groups show good clinical results at
onger-term follow-up.2010 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
eywords: Cervical arthroplasty; Symptomatic cervical disc disease; Total disc replacement
www.sasjournal.com
pw2spTt
Since 2007, 3 cervical total disk replacement (TDR)rostheses have been approved by the Food and Drug Ad-inistration (FDA) for marketing in the United States. As
* Corresponding author: Rick B. Delamarter, MD, The Spine Institute ataint John’s Health Center, 1301 20th St, Ste 400, Santa Monica, CA0404; Tel.: 310-828-7757; Fax: 310-828-6847.
mE-mail address: [email protected]
935-9810 © 2010 SAS - The International Society for the Advancement of Spinoi:10.1016/j.esas.2010.09.001
art of their application to the FDA, these devices under-ent an Investigational Device Exemption clinical trial and-year follow-up results were presented.1–3 All 3 studieshowed non-inferiority of the investigational device com-ared with anterior cervical discectomy and fusion (ACDF).he ProDisc-C (Synthes USA Products, LLC, West Ches-
er, Pennsylvania) TDR was also able to prove superiority in
any clinical outcomes in comparison to ACDF.1 However,e Surgery. Published by Elsevier Inc. All rights reserved.

tnww
pSciaphiatcisd
l
M
cMdma1becttw
tCpiFvPrgssp
mstgv
wgp
R
pitrCtftAOtA1u6A.Po
N
psngBnaAtw
N
g5sf(sf16AP
123R.B. Delamarter et al. / SAS Journal 4 (2010) 122–128
here was still a significant concern in the medical commu-ity regarding performance over the longer term andhether these areas of superiority compared with ACDFould bear out over time.Widely accepted as one of the most successful spine
rocedures performed today, ACDF was first described bymith and Robinson4 in 1958 and remained largely un-hanged until the 1990s, when anterior cervical plates werentroduced. However, there has been increased reporting ofdjacent segment degeneration ranging from 2.9% to 6.9%er year as a consequence of ACDF5–10 despite reports ofigh fusion rates.5,11–13 It has been shown in biomechanicaln vitro studies that fusion causes increased stress or motiont the adjacent levels,14–16 and it has been hypothesized thathis may contribute to adjacent segment breakdown byhanging segmental motion and increasing strains in thentervertebral disk adjacent to fusion.16 Long-term data willhow whether substituting arthroplasty for fusion will re-uce the incidence of adjacent segment degeneration.
The purpose of this report is to present the 4-year fol-ow-up results of the ProDisc-C TDR clinical trial.
aterials and methods
Complete methodology of this prospective, randomized,ontrolled, multicenter trial was previously described byurrey et al.1 In brief, patients with symptomatic cervical
isk disease who were unresponsive to nonoperative treat-ents for at least 6 weeks, met the inclusion/exclusion criteria,
nd had signed informed consent forms were randomized in a:1 ratio to ProDisc-C (PDC-R) or ACDF. Patients remainedlinded to randomization until immediately after surgery. Afternrollment of the randomized portion of the clinical trial wasompleted, the FDA allowed the study investigators to con-inue to implant the investigational device in patients who methe original study criteria until study approval. These patientsere termed continued access (CA).Patients were evaluated preoperatively and postopera-
ively at 6 weeks and 3, 6, 12, 18, 24, 36, and 48 months.A patients had only reached the 24-month follow-up timeoint at the time of this report. Patient self-assessmentsncluded Neck Disability Index (NDI) questionnaire, Shortorm 36 (SF-36), neck and arm pain intensity on a 100-mmisual analog scale (VAS), and VAS for patient satisfaction.hysical and neurologic examinations included root tension,eflexes, muscle strength, and sensory deficits. Radio-raphic evaluation consisted of anteroposterior and lateraltanding, flexion, and extension films. Radiographic analy-is of range of motion (ROM) was measured by an inde-endent third party (Medical Metrics Inc., Houston, Texas).
For between–treatment group comparisons of continuouseasurements such as NDI, VAS for pain, and SF-36
cores, the Wilcoxon rank sum test was used. To comparehe mean improvement from baseline within the treatmentroups for the patient self-assessment data at each follow-up
isit, paired t tests were performed. The Fisher’s exact test aas used to compare success rates between treatmentroups such as neurologic success and the percentage ofatients indicating that they would have the surgery again.
esults
From August 2003 to October 2004, 209 randomizedatients (103 PDC-R and 106 ACDF) had surgery at 13nvestigational sites across the United States and are con-inuing to be followed up for 7 years. After closure ofandomized enrollment in 2004, an additional series of 136A patients had ProDisc-C TDR surgery from March 2005
o January 2008. Follow-up rates at 24 months were 98.0%or PDC-R, 94.8% for ACDF, and 77.4% for CA. At theime of this publication, the follow-up rates for PDC-R andCDF were 63.0% and 46.2%, respectively, at 48 months.verall patient demographics showed no difference be-
ween randomized and CA cohorts of ProDisc-C–treated orCDF-treated patients (Table 1). Operative time (PDC-R,07.4 minutes; ACDF, 98.7 minutes; and CA, 108.8 min-tes) and estimated blood loss (PDC-R, 83.5 mL; ACDF,3.5 mL; and CA, 84.2 mL) were statistically lower forCDF compared with PDC-R patients (P � .0063 and P �
0094, respectively). There was no difference betweenDC-R or ACDF patients and CA patients in operative timer blood loss.
eurologic success
Neurologic success was defined as maintenance or im-rovement in each of the neurologic evaluations includingensory, motor, and reflex functions. At 24 months, theeurologic success rate was not different among the 3roups (PDC-R, 90.9%; ACDF, 88.0%; and CA, 94.3%).oth the PDC-R and ACDF groups were able to maintaineurologic success levels from 24 to 48 months, because 24-nd 48-month follow-up values were not statistically different.t 48 months, the overall neurologic success rate trended
oward significance for PDC-R patients (88.9%) comparedith ACDF patients (74.4%) (P � .0665).
eck Disability Index
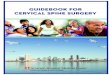
Preoperative NDI scores were not different betweenroups (PDC-R, 53.9 � 15.1; ACDF, 52.2 � 14.5; and CA,2.1 � 12.7). Regardless of treatment, all patients showedtatistically significant improvement in NDI scores at allollow-up periods compared with baseline (P � .0001)Fig. 1). At 24 months, there was no significant differenceeen between groups. The mean NDI score was 21.4 � 20.3or PDC-R patients, 20.6 � 18.4 for ACDF patients, and8.5 � 17.7 for CA patients. These scores represent a 60.3%,0.6%, and 64.5% improvement from baseline, respectively.t 48 months, the mean NDI score was 20.3 � 18.6 forDC-R patients and 21.2 � 14.9 for ACDF patients, a 62.3%
nd 59.5% improvement from baseline, respectively.
V
srm4aspgAVimmrs
S
ab
po8snAigp
P
p2f8sippw
TP
V
P
I
Sgorical v
124 R.B. Delamarter et al. / SAS Journal 4 (2010) 122–128
AS for neck and arm pain
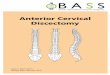
VAS neck and arm pain intensity assessments indicatedtatistically significant improvement from preoperative scoresegardless of treatment (P � .0001) (Figs. 2 and 3). At 24onths, mean VAS neck pain intensity scores were reduced by
7.3 mm in the PDC-R group, 41.5 mm in the ACDF group,nd 49.8 mm in the CA group. At 48 months, the ACDF grouphowed only a 38.7 mm reduction in mean VAS score fromreoperative levels compared with 49.3 mm in the PDC-Rroup, although this difference was not statistically significant.t 24 months, a reduction of 43.7 mm was observed in meanAS arm pain intensity scores in the PDC-R group, 43.4 mm
n the ACDF group, and 43.8 mm in the CA group. At 48onths, the PDC-R group maintained a 43.8-mm reduction inean VAS score, whereas ACDF patients showed a 40.2-mm
eduction in mean VAS score compared with preoperativecore.
hort Form 36
Regardless of treatment and at all time points, there wasstatistically significant improvement in SF-36 scores from
able 1atient demographics and intraoperative data.
ariableACDF(n � 106)
Pro(n
atient demographicsGender [n (%)]
Male 57 (53.8%)Female 49 (46.2%)
Age (years)n 106 10Mean (SD) 43.5 (7.2) 4
Race [n (%)]White 88 (85.4%)African American 4 (3.9%)Hispanic 3 (2.9%)Asian 5 (4.9%)Other 3 (2.9%)
Body mass indexn 106 10Mean (SD) (kg/m2) 27.3 (5.5) 2
Smoking statusFormer 20 (22.5%)Current 37 (34.9%)
ntraoperative dataImplant level
C3–C4 1 (0.09%)C4–C5 6 (5.7%)C5–C6 61 (57.5%)C6–C7 38 (35.8%)
Intraoperative timen 106 10Mean (SD) (minutes) 98.7 (47.0) 10
Estimated blood lossn 105 10Mean (SD) (mL) 63.5 (50.4) 8
D � standard deviation.* Continuous variables were analyzed by the Wilcoxon rank sum test; cate
aseline (P � .0016). At 24 months, SF-36 physical com- a
onent scores improved in 83.8% of PDC-R patients, 84.4%f ACDF patients, and 84.6% of CA patients. At 48 months,7.1% of PDC-R patients and 83.3% of ACDF patientshowed improvement. At 24 months, SF-36 mental compo-ent scores improved in 75.8% of PDC-R patients, 80.0% ofCDF patients, and 76.0% of CA patients. At 48 months,
mprovement was seen in 80.6% of patients in the PDC-Rroup whereas only 73.8% of ACDF patients showed im-rovement.
atient satisfaction and surgery again
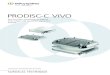
VAS patient satisfaction (Fig. 4) was higher at all timeoints for PDC-R patients compared with the ACDF group. At4 months, the mean satisfaction score was 83.4 � 24.8 mmor PDC-R patients, 80.0 � 28.0 mm for ACDF patients, and7.3 � 20.0 mm for CA patients. At 48 months, there was atatistically significant difference in the mean satisfaction scoren PDC-R patients (85.5 � 23.7 mm) compared with ACDFatients (76.4 � 30.6 mm) (P � .0499). The percentage ofatients considered very to completely satisfied (60–100 mm)as 86.3% in the PDC-R group, 83.0% in the ACDF group,
(PDC-R): ProDisc-C (CA):(n � 136)
P value* forPDC-R vs ACDF
.893%) 58 (42.7%)7%) 78 (57.4%)
.20134
) 43.5 (8.0).10
5%) 125 (92.6%)%) 0 (0%)%) 1 (0.7%)) 5 (3.7%)%) 4 (3.0%)
.09135
) 26.7 (5.1).88
0%) 30 (24.2%)0%) 27 (19.9%)
%) 4 (2.9%) .48%) 14 (10.3%)3%) 82 (60.3%)1%) 36 (26.5%)
.0063135
6) 108.8 (48.6).009
1359) 84.2 (84.6)
ariables were analyzed using Fisher’s exact test.
Disc-C� 103)
57 (55.46 (44.
32.1 (8.4
97 (91.1 (0.95 (4.70 (0%3 (2.8
36.4 (5.3
18 (20.34 (33.
3 (2.910 (9.758 (56.32 (31.
37.4 (35.
33.5 (64.
nd 90.5% in the CA group. At 48 months, the percentage of

psi
spt
ap
R
a
Fc to 24 m
Fa
125R.B. Delamarter et al. / SAS Journal 4 (2010) 122–128
atients considered very to completely satisfied (60–100 mm)tayed consistent for PDC-R patients (85.7%) while droppingn the ACDF group (76.2%).
Patients were asked whether they would have the sameurgical treatment again. At 24 months, 85.6% of PDC-Ratients, 80.9% of ACDF patients, and 86.3% of CA pa-ients responded yes, they would have the same surgery
ig. 1. Mean Neck Disability Index (NDI) scores for anterior cervical diontinued access (CA) patients over time. CA patients were followed out
ig. 2. Mean Visual Analog Scale (VAS) neck pain intensity scores for an
nd ProDisc-C continued access (CA) patients over time. CA patients were follogain. At 48 months, 88.9% of PDC-R and 81.0% of ACDFatients responded yes.
adiography
At 24 months, flexion-extension ROM at the index levelveraged 9.38° � 5.97° for PDC-R patients and 9.50° � 5.15°
y and fusion (ACDF), ProDisc-C randomized (PDC-R), and ProDisc-Conths. Error bars represent standard deviation.
ervical discectomy and fusion (ACDF), ProDisc-C randomized (PDC-R),
scectom
terior c
wed out to 24 months. Error bars represent standard deviation.
fm3tc
c2
RR
Fa re follo
Fa
126 R.B. Delamarter et al. / SAS Journal 4 (2010) 122–128
or CA patients. At 48 months, flexion-extension ROM wasaintained in PDC-R patients (9.12° � 6.06°). By 24 months,cases of bridging bone were identified at the index level in
he PDC-R group. Between 24 and 48 months, an additional 2ases of bridging bone were identified in the PDC-R group. No
ig. 3. Mean Visual Analog Scale (VAS) arm pain intensity scores for annd ProDisc-C continued access (CA) patients over time. CA patients we
ig. 4. Mean Visual Analog Scale (VAS) patient satisfaction scores for an
nd ProDisc-C continued access (CA) patients over time. CA patients were folloases of bridging bone were observed in the CA group at up to4 months.
At 24 months, 91.2% of the ACDF patients had �2°OM; by 48 months, 95.5% of the ACDF group had �2°OM.
ervical discectomy and fusion (ACDF), ProDisc-C randomized (PDC-R),wed out to 24 months. Error bars represent standard deviation.
ervical discectomy and fusion (ACDF), ProDisc-C randomized (PDC-R),
terior c
terior c
wed out to 24 months. Error bars represent standard deviation.
S
oitA2tmpa
cTs2tp
glpdw6lp
ptibtaa
D
rsg4ltrsdATgd
ms
tewaptdw
ca4tttcPpgtda
hprmsp
aslvvatgf
A
uPt
R
127R.B. Delamarter et al. / SAS Journal 4 (2010) 122–128
econdary surgical procedures
Secondary surgical procedures were defined as any re-peration, revision, supplemental fixation, or removal of themplant. By 24 months, of the patients originally enrolled inhe study, 2 (1.9%) in the PDC-R group and 9 (8.5%) in theCDF group required a secondary surgical procedure. From4 to 48 months, 1 additional PDC-R patient and 3 addi-ional ACDF patients required secondary surgery. By 48onths, 2.9% of PDC-R patients and 11.3% of ACDF
atients had required a secondary surgical procedure—anpproximately 4-fold difference (P � .0292).
The 3 PDC-R patients reported ongoing pain and wereonverted to fusion. One patient reported worsening pain; theDR was removed and the level converted to a fusion. Theecond case involved removal of the TDR and revision to a-level ACDF because of return of nonspecific neck pain. Thehird patient underwent a posterior decompression with sup-lemental fixation at C6-T1; the TDR was left intact.
Of the 12 secondary surgeries that occurred in the ACDFroup, 6 included an adjacent level in addition to the indexevel. The primary reason for revision at the index level wasseudarthrosis; 1 patient underwent revision because ofysphagia associated with plate liftoff, and 1 patient under-ent posterior decompression for foraminal stenosis. Of thepatients (5.6%) who required procedures at the adjacent
evel, an ACDF was performed at 1 adjacent level in 3atients and at both adjacent levels in 3 patients.
In the CA group, 3 patients required a secondary surgicalrocedure by the 24-month follow-up time point. In 1 casehe implant was repositioned 4 days after surgery. Increas-ng radiculopathy developed in 1 patient due to hypermo-ility at the index level, and this patient underwent revisiono anterior fusion. One patient reported increasing trapezialnd arm pain; the implant was removed, and the index anddjacent levels were converted to anterior fusion.
iscussion
Although a hypothesized benefit of TDR surgery is theeduction of adjacent segment disease alone, this prospectivetudy shows a reduction in the overall rate of secondary sur-ical interventions at both the index and adjacent levels. A-fold increase in reoperation rates at the index and adjacentevels for ACDF-treated patients compared with PDC-R–reated patients was shown in these longer-term results. Theeoperations in the ACDF group were mainly for pseudarthro-is at the index level or the development of symptomaticegeneration at an adjacent level. By 48 months, 5.6% ofCDF patients required further surgery at an adjacent level.his rate was higher than the 1.9% rate observed in the PDC-Rroup. Though preliminary, these results indicate that TDRoes slow the rate of adjacent-level disease.
The rate of reoperation for symptomatic adjacent seg-ent disease after cervical fusion was 1.4% per year in this
tudy, slightly lower than the 1.5% to 4% rate reported in
he literature.7 However, it must be noted that the patientsnrolled in this study were limited to single-level disease,hereas the large patient series reported by Hilibrand et al6
nd Goffin et al17 include a substantial number of multilevelrocedures. Many clinical series have established that pa-ients with multilevel cervical fusions have a higher inci-ence of adjacent-level disease progression when comparedith single-level fusions.In the PDC-R group, radiographic evaluation showed 5
ases of bridging bone. Three of these cases were observedt 12 to 18 months follow-up and two were noted at the8-month follow-up. This radiographic finding was asymp-omatic in these 5 patients. Extensive analysis has shownhat in none of these cases was there any correlation be-ween the development of bridging bone and an effect onlinical outcomes compared with the remainder of theDC-R group. There were no cases of bridging bone re-orted in the CA group. This difference is likely because ofreater attention to soft-tissue handling, endplate prepara-ion, controlling bleeding, and use of bone wax. Nonsteroi-al anti-inflammatory drugs were not required in this study,nd most investigators did not administer them.
With any new technology, there are always the questions ofow steep the learning curve is and how experience affectsatient outcomes. In this study the clinical outcomes of theandomized and CA ProDisc-C patients observed up to 24onths were comparable. Given the relatively straightforward
urgical technique, it appears that a learning curve does notlay a factor and patient outcomes are not affected.
This report is limited by the lower patient accountabilityt 48 months compared with 24 months. This is a continuingtudy, and follow-up is ongoing. Nevertheless, these pre-iminary data at 4 years show that both TDR and ACDF areiable surgical options for patients with symptomatic cer-ical disk disease. Although it appears that ACDF patientsre at higher risk for having an additional surgical interven-ion at the index level or an adjacent level, patients in bothroups continue to show good clinical results at longer-termollow-up.
cknowledgement
The authors thank Johanna Hantel, Synthes USA Prod-cts, LLC, for her editorial collaboration, and Jeff Stein,hD, Synthes USA Products, LLC, for his assistance with
he statistical analysis.
eferences
1. Murrey D, Janssen M, Delamarter R, et al. Results of the prospective,randomized, controlled multicenter Food and Drug Administrationinvestigational device exemption study of the ProDisc-C total discreplacement versus anterior discectomy and fusion for the treatment of1-level symptomatic cervical disc disease. Spine J 2009;9:275–86.
2. Mummaneni PV, Burkus JK, Haid RW, Traynelis VC, Zdeblick TA.
Clinical and radiographic analysis of cervical disc arthroplasty com-
1
1
1
1
1
1
1
1
128 R.B. Delamarter et al. / SAS Journal 4 (2010) 122–128
pared with allograft fusion: a randomized controlled clinical trial.J Neurosurg Spine 2007;6:198–209.
3. Sasso RC, Smucker JD, Hacker RJ, Heller JG. Artificial disc versusfusion: a prospective, randomized study with 2-year follow-up on 99patients. Spine 2007;32:2933–40.
4. Smith GW, Robinson RA. The treatment of certain cervical spinedisorders by anterior removal of the intervertebral disc and interbodyfusion. J Bone Joint Surg Am 1958;40:607–24.
5. Yue WM, Brodner W, Highland TR. Long-term results after anteriorcervical discectomy and fusion with allograft and plating: a 5- to11-year radiologic and clinical follow-up study. Spine 2005;30:2138–44.
6. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH.Radiculopathy and myelopathy at segments adjacent to the site of aprevious anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519–28.
7. Hilibrand AS, Robbins BA. Adjacent segment degeneration and adja-cent segment disease: the consequences of spinal fusion? Spine J2004;4:190–4S.
8. Gore DR, Sepic SB. Anterior cervical fusion for degenerated or pro-truded discs: a review of one hundred forty-six patients. Spine 1984;9:667–71.
9. Robertson JT, Papadopoulos SM, Traynelis VC. Assessment of adja-cent-segment disease in patients treated with cervical fusion or arthro-
plasty: a prospective 2-year study. J Neurosurg Spine 2005;3:417–23.0. Ishihara H, Kanamori M, Kawaguchi Y, Nakamura H, Kimura T.Adjacent segment disease after anterior cervical interbody fusion.Spine J 2004;4:624–8.
1. Bohlman HH, Emery SE, Goodfellow DB, Jones PK. Robinson ante-rior cervical discectomy and arthrodesis for cervical radiculopathy:long-term follow-up of one hundred and twenty-two patients. J BoneJoint Surg Am 1993;75:1298–307.
2. Kaiser MG, Haid RW Jr, Subach BR, Barnes B, Rodts GE Jr. Anteriorcervical plating enhances arthrodesis after discectomy and fusion withcortical allograft. Neurosurgery 2002;50:229–38.
3. Fraser JF, Hartl R. Anterior approaches to fusion of the cervical spine:a metaanalysis of fusion rates. J Neurosurg Spine 2007;6:298–303.
4. Puttlitz CM, Rousseau MA, Xu Z, Hu S, Tay BK, Lotz JC. Interver-tebral disc replacement maintains cervical spine kinetics. Spine 2004;29:2809–14.
5. DiAngelo DJ, Foley KT, Morrow BR, et al. In vitro biomechanics ofcervical disc arthroplasty with the ProDisc-C total disc implant. Neu-rosurg Focus 2004;17:E7.
6. Matsunaga S, Kabayama S, Yamamoto T, Yone K, Sakou T, Nakan-ishi K. Strain on intervertebral discs after anterior cervical decompres-sion and fusion. Spine 1999;24:670–5.
7. Goffin J, Geusens E, Vantomme N, et al. Long-term follow-up afterinterbody fusion of the cervical spine. J Spinal Disord Tech 2004;17:
79–85.