Embed Size (px)
Citation preview

Which of the following statements is true of glucagon?
Produced in response to hyperglycaemia
Released by beta cells
Inhibits gluconeogenesis
Produced in response to an increase of amino acids
Composed of 2 alpha polypeptide chains linked by hydrogen bonds
Glucagon is a protein comprised of a single polypeptide chain. Produced by alpha cells of pancreatic islets of Langerhans in response to hypoglycaemia and amino acids. It increases plasma glucose and ketones. Please rate this question:
Discuss and give feedback
Next question
Glucagon
Glucagon, the hormonal antagonist to insulin, is released from the alpha cells of the Islets of Langerhans in the pancreas. It will result in an increased plasma glucose level.
Stimulation Inhibition
Decreased plasma glucose Somatostatin
Increased catecholamines Insulin
Increased plasma amino acids
Increased free fatty acids and keto acids

Sympathetic nervous system Increased urea
Acetylcholine
Cholecystokinin
Next question

A 28 year old man undergoes a completion right hemicolectomy for treatment of a 5cm appendiceal
carcinoid. As part of his follow up he is due to undergo 24 hour urine collection for 5-HIAA. Which of
the following causes an elevated 5-HIAA in a 24-hour urine collection?
Naproxen
Oranges
Flucloxacillin
Amiodarone
Beef
It is important to be aware of what can falsely elevate 5-HIAA to avoid diagnosing carcinoid
syndrome incorrectly. These include:
Food: spinach, cheese, wine, caffeine, tomatoes
Drugs: Naproxen, Monoamine oxidase inhibitors
Recent surgery
Please rate this question:
Discuss and give feedback
Next question
Carcinoid syndrome
Carcinoid tumours secrete serotonin Originate in neuroendocrine cells mainly in the intestine (midgut-distal ileum/appendix)
Can occur in the rectum, bronchi Hormonal symptoms mainly occur when disease spreads outside the bowel

Clinical features
Onset: insidious over many years Flushing face Palpitations Pulmonary valve stenosis and tricuspid regurgitation causing dyspnoea
Asthma Severe diarrhoea (secretory, persists despite fasting)
Investigation
5-HIAA in a 24-hour urine collection Somatostatin receptor scintigraphy CT scan
Blood testing for chromogranin A
Treatment
Octreotide Surgical removal
Next question

A 52 year old man develops septic shock following a Hartmans procedure for perforated diverticular disease. He is started on an adrenaline infusion. Which of the following is least likely to occur?
Peripheral vasoconstriction
Coronary artery vasospasm
Gluconeogenesis
Lipolysis
Tachycardia
It's cardiac effects are mediated via β 1 receptors. The coronary arteries which have β 2 receptors are unaffected. Please rate this question:
Discuss and give feedback
Next question
Adrenaline
Fight or Flight response
- Catecholamine (phenylalanine and tyrosine) - Neurotransmitter and hormone - Released by the adrenal glands - Effects on α 1 and 2, β 1 and 2 receptors - Effect on β 2 receptors in skeletal muscle vessels-causing vasodilation - Increase cardiac output and total peripheral resistance - Vasoconstriction in the skin and kidneys causing a narrow pulse pressure Actions
α adrenergic receptors:
Inhibits insulin secretion by the pancreas
Stimulates glycogenolysis in the liver and muscle Stimulates glycolysis in muscle

β adrenergic receptors:
Stimulates glucagon secretion in the pancreas Stimulates ACTH
Stimulates lipolysis by adipose tissue
Next question

Intra cranial pressure is governed by the principles of the Monroe-Kellie doctrine. To which of the following does this concept not apply?
A 2 month old child
A 2 year old child
A 5 year old child
A 10 year old child
An adult
The Monroe-Kelly Doctrine assumes that the cranial cavity is a rigid box. In children with non fused fontanells this is not the case. Please rate this question:
Discuss and give feedback
Next question
Applied neurophysiology
Pressure within the cranium is governed by the Monroe-Kelly doctrine. This considers the skull as a closed box. Increases in mass can be accommodated by loss of CSF. Once a critical point is reached (usually 100- 120ml of CSF lost) there can be no further compensation and ICP rises sharply. The next step is that pressure will begin to equate with MAP and neuronal death will occur. Herniation will also accompany this process.
The CNS can autoregulate its own blood supply. Vaso constriction and dilatation of the cerebral blood vessels is the primary method by which this occurs. Extremes of blood pressure can exceed this capacity resulting in risk of stroke. Other metabolic factors such as hypercapnia will also cause vasodilation, which is of importance in ventilating head injured patients.
The brain can only metabolise glucose, when glucose levels fall, consciousness will be impaired.
Next question

Which of the following is not caused by cortisol in the stress response?
Anti-inflammatory effects
Hypoglycaemia
Skeletal muscle protein breakdown
Stimulation of lipolysis
Mineralocorticoid effects
An 'anti insulin' effect occurs leading to hyperglycaemia. Please rate this question:
Discuss and give feedback
Next question
Stress response: Endocrine and metabolic changes
Surgery precipitates hormonal and metabolic changes causing the stress response. Stress response is associated with: substrate mobilization, muscle protein loss, sodium and
water retention, suppression of anabolic hormone secretion, activation of the sympathetic nervous system, immunological and haematological changes.
The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and there is a failure of the normal feedback mechanisms of control of hormone secretion.
A summary of the hormonal changes associated with the stress response:
Increased Decreased No Change
Growth hormone Insulin Thyroid stimulating hormone
Cortisol Testosterone Luteinizing hormone

Increased Decreased No Change
Renin Oestrogen Follicle stimulating hormone
Adrenocorticotrophic hormone (ACTH)
Aldosterone
Prolactin
Antidiuretic hormone
Glucagon
Sympathetic nervous system
Stimulates catecholamine release
Causes tachycardia and hypertension
Pituitary gland
ACTH and growth hormone (GH) is stimulated by hypothalamic releasing factors, corticotrophin releasing factor (CRF) and somatotrophin (or growth hormone releasing factor)
Perioperative increased prolactin secretion occurs by release of inhibitory control Secretion of thyroid stimulating hormone (TSH), luteinizing hormone (LH) and follicle
stimulating hormone (FSH) does not change significantly
ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH is produced than needed to produce a maximum adrenocortical response.
Cortisol
Significant increases within 4-6 hours of surgery (>1000 nmol litre-1).

The usual negative feedback mechanism fails and concentrations of ACTH and cortisol remain persistently increased.
The magnitude and duration of the increase correlate with the severity of stress and the response is not abolished by the administration of corticosteroids.
The metabolic effects of cortisol are enhanced:
Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein synthesis in the liver Stimulation of lipolysis 'Anti-insulin effect' Mineralocorticoid effects Anti-inflammatory effects Growth hormone
Increased secretion after surgery has a minor role Most important for preventing muscle protein breakdown and promote tissue repair by insulin
growth factors
Alpha Endorphin
Increased
Antidiuretic hormone
An important vasopressor and enhances haemostasis Renin is released causing the conversion of angiotensinogen to angiotensin I Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone
from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule
Insulin
Release inhibited by stress
Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory effects of catecholamines
Insulin resistance by target cells occurs later The perioperative period is characterized by a state of functional insulin deficiency
Thyroxine (T4) and tri-iodothyronine (T3)

Circulating concentrations are inversely correlated with sympathetic activity and after surgery there is a reduction in thyroid hormone production, which normalises over a few days.
Metabolic effect of endocrine response Carbohydrate metabolism
Hyperglycaemia is a main feature of the metabolic response to surgery
Due to increase in glucose production and a reduction in glucose utilization Catecholamines and cortisol promote glycogenolysis and gluconeogenesis Initial failure of insulin secretion followed by insulin resistance affects the normal responses The proportion of the hyperglycaemic response reflects the severity of surgery Hyperglycaemia impairs wound healing and increase infection rates
Protein metabolism
Initially there is inhibition of protein anabolism, followed later, if the stress response is severe, by enhanced catabolism
The amount of protein degradation is influenced by the type of surgery and also by the nutritional status of the patient
Mainly skeletal muscle protein is affected The amino acids released form acute phase proteins (fibrinogen, C reactive protein,
complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for gluconeogenesis
Nutritional support has little effect on preventing catabolism
Lipid metabolism Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis and ketone body production. Salt and water metabolism
ADH causes water retention, concentrated urine, and potassium loss and may continue for 3 to 5 days after surgery
Renin causes sodium and water retention
Cytokines
Glycoproteins Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor
Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to tissue injury from surgery or trauma

IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by the degree of tissue damage Other effects of cytokines include fever, granulocytosis, haemostasis, tissue damage limitation and promotion of healing.
Modifying the response
Opioids suppress hypothalamic and pituitary hormone secretion
At high doses the hormonal response to pelvic and abdominal surgery is abolished. However, such doses prolong recovery and increase the need for postoperative ventilatory support
Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes, although cytokine responses are unaltered
Cytokine release is reduced in less invasive surgery Nutrition prevents the adverse effects of the stress response. Enteral feeding improves
recovery
Growth hormone and anabolic steroids may improve outcome Normothermia decreases the metabolic response
References Deborah Burton, Grainne Nicholson, and George Hall Endocrine and metabolic response to surgery . Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040
Next question

Which of the following features does not put a patient at risk of refeeding syndrome?
BMI < 16 kg/m2
Alcohol abuse
Thyrotoxicosis
Chemotherapy
Diuretics
Diuretics increase the risk of re-feeding syndrome through a process of increasing the risk of depletion of key electrolytes. Please rate this question:
Discuss and give feedback
Next question
Nutrition - Refeeding syndrome
Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person following a period of starvation. The metabolic consequences include:
Hypophosphataemia Hypokalaemia
Hypomagnesaemia Abnormal fluid balance
These abnormalities can lead to organ failure. Re-feeding problems If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels High risk for re-feeding problems If one or more of the following:
BMI < 16 kg/m2 Unintentional weight loss >15% over 3-6 months Little nutritional intake > 10 days

Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high)
If two or more of the following:
BMI < 18.5 kg/m2
Unintentional weight loss > 10% over 3-6 months Little nutritional intake > 5 days History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and
antacids
Prescription
Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days
Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co strong 1 tds and supplements
Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4 mmol/kg/day)
Next question

Which of the following statements relating to the regulation of renal blood flow is untrue?
In a healthy 70Kg male, the glomerular filtration rate will be the same at a systolic blood
pressure of 120mmHg as a systolic blood pressure of 95 mmHg
Over 90% of the blood supply to the kidney is distributed to the cortex
The kidney receives approximately 25% of the total cardiac output at rest
A decrease in renal perfusion pressure will cause the juxtaglomerular cells to secrete renin
Systolic blood pressures of less than 65mmHg will cause the mesangial cells to secrete
aldosterone
The kidney autoregulates its blood supply over a range of systolic blood pressures. Drop in arterial pressure is sensed by the juxtaglomerular cells and renin is released leading to the activation of the renin-angiontensin system. Mesangial cells are contractile cells that are located in the tubule and have no direct endocrine function. Please rate this question:
Discuss and give feedback
Next question
Renal Physiology
Overview
Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular capillary bed.
Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary vasa recta.
The kidney receives up to 25% of resting cardiac output.
Control of blood flow
The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg so there is little variation in renal blood flow.
This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal signals (e.g. renin) are responsible.

Glomerular structure and function
Blood inside the glomerulus has considerable hydrostatic pressure. The basement membrane has pores that will allow free diffusion of smaller solutes, larger
negatively charged molecules such as albumin are unable to cross. The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,
times the volume of urine produced per minute, divided by the plasma concentration (assuming that the solute is freely diffused e.g. inulin).
In clinical practice creatinine is used because it is subjected to very little proximal tubular secretion.
Although subject to variability, the typical GFR is 125ml per minute. Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and
entering the bowman's capsule
Renal clearance = volume plasma from which a substance is removed per minute by the kidneys
Substances used to measure GFR have the following features: 1. Inert 2. Free filtration from the plasma at the glomerulus (not protein bound) 3. Not absorbed or secreted at the tubules 4. Plasma concentration constant during urine collection Examples: inulin, creatinine GFR = urine concentration (mmol/l) x urine volume (ml/min) -------------------------------------------------------------------------- plasma concentration (mmol/l)
The clearance of a substance is dependent not only on its diffusivity across the basement membrane but also subsequent tubular secretion and / or reabsorption.
So glucose which is freely filtered across the basement membrane is usually reabsorbed from tubules giving a clearance of zero.
Tubular function
Reabsorption and secretion of substances occurs in the tubules.
In the proximal tubule substrates such as glucose, amino acids and phosphate are co-transported with sodium across the semi permeable membrane.
Up to two thirds of filtered water is reabsorbed in the proximal tubules.
This will lead to increase in urea concentration in the distal tubule allowing for its increased diffusion.
Substances to be secreted into the tubules are taken up from the peritubular blood by tubular cells.

Solutes such as paraaminohippuric acid are cleared with a single passage through the kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and phosphate will have a tubular reabsorption that is influenced by plasma PTH levels.
Potassium may be both secreted and re-absorbed and is co-exchanged with sodium.
Loop of Henle
Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of the loop of Henle in 24 hours.
Loops from the juxtamedullary nephrons run deep into the medulla. The osmolarity of fluid changes and is greatest at the tip of the papilla. The thin ascending limb is impermeable to water, but highly permeable to sodium and
chloride ions.
This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic compared with adjacent interstitial fluid.
In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both facilitated and passive diffusion pathways.
The loops of Henle are co-located with vasa recta, these will have similar solute compositions to the surrounding extracellular fluid so preventing the diffusion and subsequent removal of this hypertonic fluid.
The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps to maintain this osmotic gradient.
Next question

A 39 year old lady undergoes a laparoscopic cholecystectomy as a daycase. The operation is more difficult than anticipated and the surgeon places a drain to the liver bed. In recovery 1.5 litres of blood is seen to enter the drain. Which of the following substances is the first to be released in this situation?
Angiotensinogen
Renin
Angiotensin I
Angiotensin II
Aldosterone
The decrease in blood pressure will be sensed by the juxtaglomerular cells in the kidney. This will cause renin secretion. Please rate this question:
Discuss and give feedback
Next question
Shock
Shock occurs when there is insufficient tissue perfusion. The pathophysiology of shock is an important surgical topic and may be divided into the
following aetiological groups:
Septic Haemorrhagic Neurogenic Cardiogenic Anaphylactic
Septic shock Septic shock is a major problem and those patients with severe sepsis have a mortality rate in excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ failure to 65% in those with 4 organ failure. Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response
Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90 beats/min, respiratory rate >20/min, WBC count >12,000/mm3 or < 4,000/mm3, altered mental state

or hyperglycaemia (in absence of diabetes). Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis. Those with organ failure have severe sepsis and those with refractory hypotension -septic shock. During the septic process there is marked activation of the immune system with extensive cytokine
release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those ofexcessive inflammation, coagulation and fibrinolytic suppression.
The surviving sepsis campaign (2012) highlights the following key areas for attention:
Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous search for the source of infection.
Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg.
Modulation of the septic response. This includes manoeuvres to counteract the changes and includes measures such as tight glycaemic control. The routine use of steroids is not advised.
In surgical patients, the main groups with septic shock include those with anastomotic leaks, abscesses and extensive superficial infections such as necrotising fasciitis. When performing surgery the aim should be to undertake the minimum necessary to restore physiology. These patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken when physiology is restored and clotting in particular has been normalised. Haemorrhagic shock The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly. The table below outlines the 4 major classes of haemorrhagic shock and their associated physiological sequelae:
Parameter Class I Class II Class III Class IV
Blood loss ml <750ml 750-1500ml 1500-2000ml >2000ml
Blood loss % <15% 15-30% 30-40% >40%
Pulse rate <100 >100 >120 >140
Blood pressure Normal Normal Decreased Decreased

Parameter Class I Class II Class III Class IV
Respiratory rate 14-20 20-30 30-40 >35
Urine output >30ml 20-30ml 5-15ml <5ml
Symptoms Normal Anxious Confused Lethargic
Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is
haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A, although you should understand the principle. In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the following may also be the cause or occur concomitantly:
Tension pneumothorax
Spinal cord injury Myocardial contusion Cardiac tamponade
When assessing trauma patients it is worth remembering that in order to generate a palpable femoral pulse an arterial pressure of >65mmHg is required. Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have such risk factors. Neurogenic shock This occurs most often following a spinal cord transection, usually at a high level. There is resultant interruption of the autonomic nervous system. The result is either decreased sympathetic
tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular resistance mediated by marked vasodilation. This results in decreased preload and thus decreased cardiac output (Starlings law). There is decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types of shock peripheral vasoconstrictors are used to return vascular tone to normal. Cardiogenic shock In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct
myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal

fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but they are less useful in delineating the extent of myocardial trauma than following MI. When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the heart is the most likely site of injury with chamber and or valve rupture. These patients require surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may require intra aortic balloon pump as a bridge to surgery. Anaphylactic shock Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic hypersensitivity reaction. Anaphylaxis is one of the few times when you would not have time to look up the dose of a medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated. Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as follows:
Adrenaline Hydrocortisone Chlorpheniramine
< 6 months 150 mcg (0.15ml 1 in 1,000) 25 mg 250 mcg/kg
6 months - 6 years 150 mcg (0.15ml 1 in 1,000) 50 mg 2.5 mg
6-12 years 300 mcg (0.3ml 1 in 1,000) 100 mg 5 mg
Adult and child 12 years 500 mcg (0.5ml 1 in 1,000) 200 mg 10 mg
Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the anterolateral aspect of the middle third of the thigh. Common identified causes of anaphylaxis
food (e.g. Nuts) - the most common cause in children drugs venom (e.g. Wasp sting)
Next question


Which of the following drugs causes hyperkalaemia?
Heparin
Ciprofloxacin
Salbutamol
Levothyroxine
Codeine phosphate
Both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to be caused by inhibition of aldosterone secretion. Salbutamol is a recognised treatment for hyperkalaemia. Please rate this question:
Discuss and give feedback
Next question
Hyperkalaemia
Plasma potassium levels are regulated by a number of factors including aldosterone, acid-base balance and insulin levels.
Metabolic acidosis is associated with hyperkalaemia as hydrogen and potassium ions compete with each other for exchange with sodium ions across cell membranes and in the distal tubule.
ECG changes seen in hyperkalaemia include tall-tented T waves, small P waves, widened QRS leading to a sinusoidal pattern and asystole
Causes of hyperkalaemia
Acute renal failure
Drugs*: potassium sparing diuretics, ACE inhibitors, angiotensin 2 receptor blockers, spironolactone, ciclosporin, heparin**
Metabolic acidosis Addison's
Tissue necrosis/rhabdomylosis: burns, trauma Massive blood transfusion

Foods that are high in potassium
Salt substitutes (i.e. Contain potassium rather than sodium) Bananas, oranges, kiwi fruit, avocado, spinach, tomatoes
*beta-blockers interfere with potassium transport into cells and can potentially cause hyperkalaemia in renal failure patients - remember beta-agonists, e.g. Salbutamol, are sometimes used as emergency treatment **both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to be caused by inhibition of aldosterone secretion
Next question

A 25-year-old man who has been morbidly obese for the past five years is reviewed in the surgical bariatric clinic. In this patient, release of which of the following hormones would increase appetite?
Leptin
Thyroxine
Adiponectin
Ghrelin
Serotonin
Obesity hormones
leptin decreases appetite
ghrelin increases appetite
Whilst thyroxine can increase appetite it does not fit with the clinical picture being described. Please rate this question:
Discuss and give feedback
Next question
Obesity: physiology
Leptin Leptin is thought to play a key role in the regulation of body weight. It is produced by adipose tissue and acts on satiety centres in the hypothalamus and decreases appetite. More adipose tissue (e.g. in obesity) results in high leptin levels. Leptin stimulates the release of melanocyte-stimulating hormone (MSH) and corticotrophin-releasing hormone (CRH). Low levels of leptin stimulates the release of neuropeptide Y (NPY) Ghrelin Where as leptin induces satiety, ghrelin stimulates hunger. It is produced mainly by the fundus of the stomach and the pancreas. Ghrelin levels increase before meals and decrease after meals
Next question

Which of the following is not linked to excess glucocorticoids?
Osteonecrosis
Osteoporosis
Hypokalaemia
Hyponatraemia
Growth retardation in children
There are many adverse effects associated with excess glucocorticoids. Thinning of the skin, osteonecrosis and osteoporosis are all common. Steroids are associated with retention of sodium and water. Potassium loss may occur and hypokalaemic alkalosis has been reported. Please rate this question:
Discuss and give feedback
Next question
Cortisol
Glucocorticoid
Released by zona fasiculata of the adrenal gland 90% protein bound; 10% active Circadian rhythm: High in the mornings Negative feedback via ACTH
Actions
Glycogenolysis
Gluconeogenesis Protein catabolism Lipolysis Stress response
Anti-inflammatory Decrease protein in bones Increase gastric acid Increases neutrophils/platelets/red blood cells Inhibits fibroblastic activity

A 54-year-old woman is admitted to the Surgical Admissions Unit with abdominal pain. Blood tests taken on admission show the following:
Magnesium 0.40 mmol/l (normal value 0.7-1.0 mmol/l)
Which one of the following factors is most likely to be responsible for this result?
Excessive resuscitation with intravenous saline
Digoxin therapy
Diarrhoea
Hypothermia
Rhabdomyolysis
Please rate this question:
Discuss and give feedback
Next question
Hypomagnasaemia
Cause of low magnesium
Diuretics Total parenteral nutrition Diarrhoea
Alcohol Hypokalaemia, hypocalcaemia
Features
Paraesthesia
Tetany Seizures Arrhythmias

Decreased PTH secretion → hypocalcaemia ECG features similar to those of hypokalaemia Exacerbates digoxin toxicity
Next question

A 43 year old man has a nasogastric tube inserted. The nurse takes a small aspirate of the fluid from the stomach and tests the pH of the aspirate. What is the normal intragastric pH?
0.5
2
4
5
6
Theme from January 2012 Exam The intragastric pH is usually 2. Administration of proton pump inhibitors can result in almost complete abolition of acidity Please rate this question:
Discuss and give feedback
Next question
Gastric secretions
A working knowledge of gastric secretions is important for surgery because peptic ulcers are common, surgeons frequently prescribe anti secretory drugs and because there are still patients around who will have undergone acid lowering procedures (Vagotomy) in the past. Gastric acid
Is produced by the parietal cells in the stomach pH of gastric acid is around 2 with acidity being maintained by the H+/K+ ATP ase pump. As
part of the process bicarbonate ions will be secreted into the surrounding vessels. Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus.
This sets up a negative potential across the membrane and as a result sodium and potassium ions diffuse across into the canaliculus.
Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and are secreted into the lumen of the oxyntic gland.

This is illustrated diagrammatically below:
Image sourced from Wikipedia
Phases of gastric acid secretion There are 3 phases of gastric secretion: 1. Cephalic phase (smell / taste of food)
30% acid produced
Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells
2. Gastric phase (distension of stomach )
60% acid produced
Stomach distension/low H+/peptides causes Gastrin release

3. Intestinal phase (food in duodenum)
10% acid produced High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion
via enterogastrones (CCK, secretin) and neural reflexes.
Regulation of gastric acid production Factors increasing production include:
Vagal nerve stimulation
Gastrin release Histamine release (indirectly following gastrin release) from enterchromaffin like cells
Factors decreasing production include:
Somatostatin (inhibits histamine release) Cholecystokinin Secretin
The diagram below illustrates some of the factors involved in regulating gastric acid secretion and the relevant associated pharmacology
Image sourced from Wikipedia
Below is a brief summary of the major hormones involved in food digestion:

Source Stimulus Actions
Gastrin G cells in
antrum of the stomach
Distension of
stomach, extrinsic
nerves
Inhibited by: low
antral pH,
somatostatin
Increase HCL, pepsinogen and IF secretion,
increases gastric motility, trophic effect on gastric mucosa
CCK I cells in
upper small
intestine
Partially digested
proteins and
triglycerides
Increases secretion of enzyme-rich fluid
from pancreas, contraction of gallbladder
and relaxation of sphincter of Oddi,
decreases gastric emptying, trophic effect on
pancreatic acinar cells, induces satiety
Secretin S cells in
upper small
intestine
Acidic chyme, fatty acids
Increases secretion of bicarbonate-rich fluid
from pancreas and hepatic duct cells,
decreases gastric acid secretion, trophic effect on pancreatic acinar cells
VIP Small
intestine,
pancreas
Neural Stimulates secretion by pancreas and
intestines, inhibits acid and pepsinogen
secretion
Somatostatin D cells in the
pancreas and
stomach
Fat, bile salts and
glucose in the
intestinal lumen
Decreases acid and pepsin secretion,
decreases gastrin secretion, decreases
pancreatic enzyme secretion, decreases
insulin and glucagon secretion
inhibits trophic effects of gastrin, stimulates gastric mucous production
Next question

Which of the following is the equivalent of cardiac preload?
End diastolic volume
Stroke volume
Systemic vascular resistance
Mean arterial pressure
Peak systolic arterial pressure
Preload is the same as end diastolic volume. When it is increased slightly there is an associated increase in cardiac output (Frank Starling principle). When it is markedly increased e.g. over 250ml then cardiac output falls. Please rate this question:
Discuss and give feedback
Next question
Cardiac physiology
The heart has four chambers ejecting blood into both low pressure and high pressure systems.
The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on the left.
At rest diastole comprises 2/3 of the cardiac cycle. The product of the frequency of heart rate and stroke volume combine to give the cardiac
output which is typically 5-6L per minute.
Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B exam. Electrical properties
Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is capable of contraction.
In the normal situation the cardiac impulse is generated in the sino atrial node in the right atrium and conveyed to the ventricles via the atrioventricular node.

The sino atrial node is also capable of spontaneous discharge and in the absence of background vagal tone will typically discharge around 100x per minute. Hence the higher resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from -70mV to around -50mV at which point an action potential is generated.
Differences in the depolarisation slopes between SA and AV nodes help to explain why the SA node will depolarise first. The cells have a refractory period during which they cannot be re-stimulated and this period allows for adequate ventricular filling. In pathological tachycardic states this time period is overridden and inadequate ventricular filling may then occur, cardiac output falls and syncope may ensue.
Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla. Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential depolarisation. Cardiac cycle
Image sourced from Wikipedia
Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut. Aortic pressure is high.
Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic
volume 130-160ml.

Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceeded- blood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial pressure (x-descent).
Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular pressure drops the aortic pressure remains constant owing to peripheral vascular resistance and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke volume is 70ml (i.e. Volume ejected).
Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure wave associated with closure of the aortic valve increases aortic pressure. The pressure dip before this rise can be seen on arterial waveforms and is called the incisura. During systole the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial pressure exceed ventricular pressure and AV valves open - atria empty passively into ventricles and atrial pressure falls (y -descent )
The negative atrial pressures are of clinical importance as they can allow air embolization to occur if the neck veins are exposed to air. This patient positioning is important in head and neck surgery to avoid this occurrence if veins are inadvertently cut, or during CVP line insertion. Mechanical properties
Preload = end diastolic volume
Afterload = aortic pressure
It is important to understand the principles of Laplace's law in surgery.
It states that for hollow organs with a circular cross section, the total circumferential wall tension depends upon the circumference of the wall, multiplied by the thickness of the wall and on the wall tension.
The total luminal pressure depends upon the cross sectional area of the lumen and the transmural pressure. Transmural pressure is the internal pressure minus external pressure and at equilibrium the total pressure must counterbalance each other.
In terms of cardiac physiology the law explains that the rise in ventricular pressure that occurs during the ejection phase is due to physical change in heart size. It also explains why a dilated diseased heart will have impaired systolic function.

Starlings law
Increase in end diastolic volume will produce larger stroke volume. This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke
volume will fall once more. It is important for the regulation of cardiac output in cardiac transplant patients who need to increase their cardiac output.
Baroreceptor reflexes
Baroreceptors located in aortic arch and carotid sinus.
Aortic baroreceptor impulses travel via the vagus and from the carotid via the glossopharyngeal nerve.
They are stimulated by arterial stretch.
Even at normal blood pressures they are tonically active. Increase in baroreceptor discharge causes:
*Increased parasympathetic discharge to the SA node. *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in stroke volume. *Decreased sympathetic discharge to venous system causing increased compliance. *Decreased peripheral arterial vascular resistance Atrial stretch receptors
Located in atria at junction between pulmonary veins and vena cava.
Stimulated by atrial stretch and are thus low pressure sensors. Increased blood volume will cause increased parasympathetic activity. Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:
theBainbridge reflex.
Decreases in receptor stimulation results in increased sympathetic activity this will decrease renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by juxtaglomerular apparatus-Increase in angiotensin II.
Increased atrial stretch will also result in increased release of atrial natriuretic peptide.
Next question

A 48 year old man undergoes a right hemicolectomy for a large caecal polyp. In the immediate post operative period which of the physiological processes described below is least likely to occur?
Glycogenolysis
Increased production of acute phase proteins
Increased cortisol production
Bronchoconstriction
Release of nitric oxide by vessels
Please rate this question:
Discuss and give feedback
Next question
Response to surgery
Sympathetic nervous system
Noradrenaline from sympathetic nerves and adrenaline from adrenal medulla
Blood diverted from skin and visceral organs; bronchodilatation, reduced intestinal motility, increased glucagon and glycogenolysis, insulin reduced
Heart rate and myocardial contractility are increased
Acute phase response
TNF-α, IL-1, IL-2, IL-6, interferon and prostaglandins are released Excess cytokines may cause SIRS Cytokines increase the release of acute phase proteins
Endocrine response
Hypothalamus, pituitary, adrenal axis

Increases ACTH and cortisol production:
increases protein breakdown increases blood glucose levels
Aldosterone increases sodium re-absorption
Vasopressin increases water re-absorption and causes vasoconstriction
Vascular endothelium
Nitric oxide produces vasodilatation
Platelet activating factor enhances the cytokine response Prostaglandins produce vasodilatation and induce platelet aggregation
Next question

A 73 year old female is referred to the surgical clinic with an iron deficiency anaemia. As part
of the diagnostic work up the doctor requests a serum ferritin level. Which of the conditions
listed is most likely to lead to a falsely elevated result?
Locally perforated sigmoid colonic adenocarcinoma
Colonic angiodysplasia
Dieulafoy lesion of the stomach
Transitional cell carcinoma of the bladder
Endometrial adenocarcinoma
A locally perforated colonic tumour will typically cause an intense inflammatory response and
if peritonitis is not present clinically then at the very least a localised abscess. This
inflammatory process is the most likely (from the list) to falsely raise the serum ferritin level.
Angiodysplasia and dieulafoy lesions are mucosal arteriovenous malformations and unlikely
to result in considerable inflammatory activity.
Please rate this question:
Discuss and give feedback
Next question
Ferritin
Ferritin is an intracellular protein that binds iron and stores it to be released in a controlled
fashion at sites where iron is required. Because iron and ferritin are bound the total body
ferritin levels may be decreased in cases of iron deficiency anaemia. Measurement of serum
ferritin levels can be useful in determining whether an apparently low haemoglobin and
microcytosis is truly caused by an iron deficiency state.
Ferritin is an acute phase protein and may be synthesised in increased quantities in
situations where inflammatory activity is ongoing. Falsely elevated results may therefore be
encountered clinically and need to be taken in context of the clinical picture and full blood
count results.

Which of the following is least likely to cause a prolonged prothrombin time?
Cholestatic jaundice
Disseminated intravascular coagulation
Prolonged antibiotic treatment
Liver disease
Acquired factor 12 deficiency
Vitamin K deficiency results from cholestatic jaundice and prolonged antibiotic therapy.
Acquired factor 12 deficiency causes prolonged APTT.
Please rate this question:
Discuss and give feedback
Next question
Abnormal coagulation
Cause Factors affected
Heparin Prevents activation factors 2,9,10,11
Warfarin Affects synthesis of factors 2,7,9,10
DIC Factors 1,2,5,8,11

Cause Factors affected
Liver disease Factors 1,2,5,7,9,10,11
Interpretation blood clotting test results
Disorder APTT PT Bleeding time
Haemophilia Increased Normal Normal
von Willebrand's disease Increased Normal Increased
Vitamin K deficiency Increased Increased Normal
Next question

Which statement about peristalsis is true?
Longitudinal smooth muscle propels the food bolus through the oesophagus
Secondary peristalsis occurs when there is no food bolus in the oesophagus
Food transfer from the oesophagus to the stomach is 4 seconds
Circular smooth muscle is not involved in peristalsis
Peristalsis only occurs in the oesophagus
Please rate this question:
Discuss and give feedback
Next question
Peristalsis
Circular smooth muscle contracts behind the food bolus and longitudinal smooth muscle propels the food through the oesophagus
Primary peristalsis spontaneously moves the food from the oesophagus into the stomach (9 seconds)
Secondary peristalsis occurs when food, which doesn't enter the stomach, stimulates stretch receptors to cause peristalsis
In the small intestine each peristalsis waves slows to a few seconds and causes mixture of chyme
In the colon three main types of peristaltic activity are recognised (see below)
Colonic peristalsis
Segmentation contractions Localised contractions in which the bolus is subjected to local forces to maximise mucosal absorption
Antiperistaltic contractions
towards ileum
Localised reverse peristaltic waves to slow entry into colon and
maximise absorption

Mass movements Waves migratory peristaltic waves along the entire colon to
empty the organ prior to the next ingestion of food bolus
Next question

A 24 year old man is injured in a road traffic accident. He becomes oliguric and his renal function
deteriorates. Which of the options below would favor acute tubular necrosis over pre renal uraemia?
No response to intravenous fluids
Urinary sodium < 20mmol/L
Bland coloured urinary sediment
Increased urine specific gravity
None of the above
In acute tubular necrosis there is no response to intravenous fluids because the damage occurs from
within the renal system rather than as a result of volume depletion.
Please rate this question:
Discuss and give feedback
Next question
Acute renal failure: Pre renal failure vs. acute tubular necrosis
Prerenal uraemia - kidneys retain sodium to preserve volume
Pre-renal uraemia Acute tubular necrosis
Urine sodium < 20 mmol/L > 30 mmol/L

Pre-renal uraemia Acute tubular necrosis
Fractional sodium excretion* < 1% > 1%
Fractional urea excretion** < 35% >35%
Urine:plasma osmolality > 1.5 < 1.1
Urine:plasma urea > 10:1 < 8:1
Specific gravity > 1020 < 1010
Urine 'bland' sediment brown granular casts
Response to fluid challenge Yes No
*fractional sodium excretion = (urine sodium/plasma sodium) / (urine creatinine/plasma creatinine) x
100
**fractional urea excretion = (urine urea /blood urea ) / (urine creatinine/plasma creatinine) x 100
Next question

Which of the following is not an effect of cholecystokinin?
It causes gallbladder contraction
It increases the rate of gastric emptying
It relaxes the sphincter of oddi
It stimulates pancreatic acinar cells
It has a trophic effect on pancreatic acinar cells
It decreases the rate of gastric emptying. Please rate this question:
Discuss and give feedback
Next question
Gastric secretions
A working knowledge of gastric secretions is important for surgery because peptic ulcers are common, surgeons frequently prescribe anti secretory drugs and because there are still patients around who will have undergone acid lowering procedures (Vagotomy) in the past. Gastric acid
Is produced by the parietal cells in the stomach pH of gastric acid is around 2 with acidity being maintained by the H+/K+ ATP ase pump. As
part of the process bicarbonate ions will be secreted into the surrounding vessels.
Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus. This sets up a negative potential across the membrane and as a result sodium and potassium ions diffuse across into the canaliculus.
Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and are secreted into the lumen of the oxyntic gland.
This is illustrated diagrammatically below:

Image sourced from Wikipedia
Phases of gastric acid secretion There are 3 phases of gastric secretion: 1. Cephalic phase (smell / taste of food)
30% acid produced
Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells
2. Gastric phase (distension of stomach )
60% acid produced
Stomach distension/low H+/peptides causes Gastrin release
3. Intestinal phase (food in duodenum)

10% acid produced High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion
via enterogastrones (CCK, secretin) and neural reflexes.
Regulation of gastric acid production
Factors increasing production include:
Vagal nerve stimulation
Gastrin release Histamine release (indirectly following gastrin release) from enterchromaffin like cells
Factors decreasing production include:
Somatostatin (inhibits histamine release)
Cholecystokinin Secretin
The diagram below illustrates some of the factors involved in regulating gastric acid secretion and the relevant associated pharmacology
Image sourced from Wikipedia
Below is a brief summary of the major hormones involved in food digestion:
Source Stimulus Actions

Gastrin G cells in
antrum of the stomach
Distension of
stomach, extrinsic
nerves
Inhibited by: low
antral pH,
somatostatin
Increase HCL, pepsinogen and IF secretion,
increases gastric motility, trophic effect on gastric mucosa
CCK I cells in
upper small
intestine
Partially digested
proteins and
triglycerides
Increases secretion of enzyme-rich fluid
from pancreas, contraction of gallbladder
and relaxation of sphincter of Oddi,
decreases gastric emptying, trophic effect on
pancreatic acinar cells, induces satiety
Secretin S cells in
upper small
intestine
Acidic chyme, fatty acids
Increases secretion of bicarbonate-rich fluid
from pancreas and hepatic duct cells,
decreases gastric acid secretion, trophic effect on pancreatic acinar cells
VIP Small
intestine, pancreas
Neural Stimulates secretion by pancreas and
intestines, inhibits acid and pepsinogen secretion
Somatostatin D cells in the
pancreas and
stomach
Fat, bile salts and
glucose in the
intestinal lumen
Decreases acid and pepsin secretion,
decreases gastrin secretion, decreases
pancreatic enzyme secretion, decreases
insulin and glucagon secretion
inhibits trophic effects of gastrin, stimulates gastric mucous production
Next question

Which part of the jugular venous waveform is associated with the closure of the tricuspid valve?
a wave
c wave
x descent
y descent
v wave
JVP: C wave - closure of the tricuspid valve
The c wave of the jugular venous waveform is associated with the closure of the tricuspid valve. Please rate this question:
Discuss and give feedback
Next question
Jugular venous pressure
As well as providing information on right atrial pressure, the jugular vein waveform may provide clues to underlying valvular disease. A non-pulsatile JVP is seen in superior vena caval obstruction. Kussmaul's sign describes a paradoxical rise in JVP during inspiration seen in constrictive pericarditis 'a' wave = atrial contraction
large if atrial pressure e.g. tricuspid stenosis, pulmonary stenosis, pulmonary hypertension absent if in atrial fibrillation
Cannon 'a' waves
caused by atrial contractions against a closed tricuspid valve are seen in complete heart block, ventricular tachycardia/ectopics, nodal rhythm, single
chamber ventricular pacing

'c' wave
closure of tricuspid valve not normally visible
'v' wave
due to passive filling of blood into the atrium against a closed tricuspid valve giant v waves in tricuspid regurgitation
'x' descent = fall in atrial pressure during ventricular systole 'y' descent = opening of tricuspid valve
Image sourced from Wikipedia
Next question

Which one of the following serum proteins is most likely to increase in a patient with severe sepsis?
Transferrin
Transthyretin
Ferritin
Albumin
Cortisol binding protein
Ferritin can be markedly increased during acute illness. The other parameters tend to decrease during an acute phase response. Please rate this question:
Discuss and give feedback
Next question
Acute phase proteins
Acute phase proteins
CRP procalcitonin ferritin fibrinogen
alpha-1 antitrypsin caeruloplasmin serum amyloid A haptoglobin complement
During the acute phase response the liver decreases the production of other proteins (sometimes referred to as negative acute phase proteins). Examples include:
albumin
transthyretin (formerly known as prealbumin) transferrin

retinol binding protein cortisol binding protein
Levels of CRP are commonly measured in acutely unwell patients. CRP is a protein synthesised in the liver and binds to phosphocholine in bacterial cells and on those cells undergoing apoptosis. In binding to these cells it is then able to activate the complement system. CRP levels are known to rise in patients following surgery. However, levels of greater than 150 at 48 hours post operatively are suggestive of evolving complications.
Next question

Theme: Critical care
A. Hypovolaemia
B. Normal
C. Cardiogenic shock
D. Septic shock
For each of the scenarios outlined in the tables below, please select the most likely diagnosis from
the list. Each option may be used once, more than once or not at all.
72. A 45 year old man is admitted to the intensive care unit following a laparotomy. He has a central
line, pulmonary artery catheter and arterial lines inserted. The following results are obtained:
Pulmonary artery occlusion
pressure Cardiac output
Systemic vascular
resistance
Low Low High
Hypovolaemia
Theme from April 2012 Exam
Cardiac output is lowered in hypovolaemia due to decreased preload.
73. A 75 year old man is admitted to the intensive care unit following a laparotomy. He has a central
line, pulmonary artery catheter and arterial lines inserted. The following results are obtained:
Pulmonary artery occlusion
pressure Cardiac output
Systemic vascular
resistance
High Low High

You answered Hypovolaemia
The correct answer is Cardiogenic shock
In cardiogenic shock pulmonary pressures are often high. This is the basis for the use of
venodilators in the treatment of pulmonary oedema.
74. A 22 year old lady is admitted to the intensive care unit following a laparotomy. She has a central
line, pulmonary artery catheter and arterial lines inserted. The following results are obtained:
Pulmonary artery occlusion
pressure Cardiac output
Systemic vascular
resistance
Low High Low
You answered Hypovolaemia
The correct answer is Septic shock
Decreased SVR is a major feature of sepsis. A hyperdynamic circulation is often present. This is the
reason for the use of vasoconstrictors.
Please rate this question:
Discuss and give feedback
Next question
Pulmonary artery occlusion pressure monitoring
The pulmonary artery occlusion pressure is an indirect measure of left atrial pressure, and thus filling
pressure of the left heart. The low resistance within the pulmonary venous system allows this useful

measurement to be made. The most accurate trace is made by inflating the balloon at the catheter
tip and "floating" it so that it occludes the vessel. If it is not possible to occlude the vessel in this way
then the measurement gained will be the pulmonary artery end diastolic pressure.
Interpretation of PAOP
PAOP mmHg Scenario
Normal 8-12
Low <5 Hypovolaemia
Low with pulmonary oedema <5 ARDS
High >18 Overload
When combined with measurements of systemic vascular resistance and cardiac output it is possible
to accurately classify patients.
Systemic vascular resistance
Derived from aortic pressure, right atrial pressure and cardiac output.
SVR=80(mean aortic pressure-mean right atrial pressure)/cardiac output
Next question

A 23 year old man has a routine ECG performed. Which part of the tracing obtained represents atrial repolarisation?
P wave
T wave
Q-T Interval
P-R interval
None of the above
The process of atrial repolarisation is generally not visible on the ECG strip. It occurs during the QRS complex. Please rate this question:
Discuss and give feedback
Next question
The normal ECG

Image sourced from Wikipedia
P wave
Represents the wave of depolarization that spreads from the SA node throughout the atria
Lasts 0.08 to 0.1 seconds (80-100 ms) The isoelectric period after the P wave represents the time in which the impulse is traveling
within the AV node
P-R interval
Time from the onset of the P wave to the beginning of the QRS complex Ranges from 0.12 to 0.20 seconds in duration Represents the time between the onset of atrial depolarization and the onset of ventricular
depolarization
QRS complex
Represents ventricular depolarization Duration of the QRS complex is normally 0.06 to 0.1 seconds

ST segment
Isoelectric period following the QRS Represents period which the entire ventricle is depolarized and roughly corresponds to the
plateau phase of the ventricular action potential
T wave
Represents ventricular repolarization and is longer in duration than depolarization
A small positive U wave may follow the T wave which represents the last remnants of ventricular repolarization.
Q-T interval
Represents the time for both ventricular depolarization and repolarization to occur, and therefore roughly estimates the duration of an average ventricular action potential.
Interval ranges from 0.2 to 0.4 seconds depending upon heart rate. At high heart rates, ventricular action potentials shorten in duration, which decreases the Q-T
interval. Therefore the Q-T interval is expressed as a "corrected Q-T (QTc)" by taking the Q-T interval and dividing it by the square root of the R-R interval (interval between ventricular depolarizations). This allows an assessment of the Q-T interval that is independent of heart rate.
Normal corrected Q-Tc interval is less than 0.44 seconds.
Next question

A 72-year-old woman is admitted to the acute surgical unit with profuse vomiting. Admission bloods show the following:
Na+ 131 mmol/l
K+ 2.2 mmol/l
Urea 3.1 mmol/l
Creatinine 56 µmol/l
Glucose 4.3 mmol/l
Which one of the following ECG features is most likely to be seen?
Short PR interval
Short QT interval
Flattened P waves
J waves
U waves
Hypokalaemia - U waves on ECG
J waves are seen in hypothermia whilst delta waves are associated with Wolff Parkinson White syndrome. Please rate this question:
Discuss and give feedback
Next question
ECG features in hypokalemia
U waves Small or absent T waves (occasionally inversion)
Prolonged PR interval ST depression Long QT interval

One registered user suggests the following rhyme!
In Hypokalaemia, U have no Pot and no T, but a long PR and a long QT!
Next question

The oxygen-haemoglobin dissociation curve is shifted to the left in:
With decreased 2,3-DPG in transfused red cells
Respiratory acidosis
High altitude
Pyrexia
Haemolytic anaemia
S shaped curve
The curve is shifted to the left when there is a decreased oxygen requirement by the tissue. This includes: 1. Hypothermia 2. Alkalosis 3. Reduced levels of DPG:
DPG is found in erythrocytes and is reduced in non exercising muscles, i.e. when there is reduced glycolysis.
4. Polycythaemia Please rate this question:
Discuss and give feedback
Next question
Oxygen Transport
Oxygen transport Almost all oxygen is transported within erythrocytes. It has limited solubility and only 1% is carried as solution. Therefore the amount of oxygen transported will depend upon haemoglobin concentration and its degree of saturation. Haemoglobin
Globular protein composed of 4 subunits. Haem consists of a protoporphyrin ring surrounding an iron atom in its ferrous state. The iron can form two additional bonds; one with oxygen and the other with a polypeptide chain. There are two alpha and two beta subunits to this polypeptide chain in an adult and together these form globin. Globin cannot bind oxygen but is able to bind to carbon dioxide

and hydrogen ions, the beta chains are able to bind to 2,3 diphosphoglycerate. The oxygenation of haemoglobin is a reversible reaction. The molecular shape of haemoglobin is such that binding of one oxygen molecule facilitates the binding of subsequent molecules. Oxygen dissociation curve
The oxygen dissociation curve describes the relationship between the percentage of saturated haemoglobin and partial pressure of oxygen in the blood. It is not affected by haemoglobin concentration.
Chronic anaemia causes 2, 3 DPG levels to increase, hence shifting the curve to the right
Haldane effect
Shifts to left = for given oxygen tension there is increased saturation of Hb with oxygen i.e. Decreased oxygen delivery to tissues
Bohr effect
Shifts to right = for given oxygen tension there is reduced saturation of Hb with oxygen i.e. Enhanced oxygen delivery to tissues

Image sourced from Wikipedia
Shifts to Left = Lower oxygen delivery
HbF, methaemoglobin, carboxyhaemoglobin
low [H+] (alkali)
low pCO2
low 2,3-DPG
low temperature
Shifts to Right = Raised oxygen
delivery
raised [H+] (acidic)
raised pCO2
raised 2,3-DPG*
raised temperature
*2,3-diphosphoglycerate
Next question

A homeless 42 year old male had an emergency inguinal hernia repair 24 hours previously. He has a BMI of 15. He has been put on a feeding regime of 35 kcal/kg/day with no additional medications. The nursing staff contact you as he has become confused and unsteady. On examination the patient is disorientated to place, has diplopia and nystagmus. What is the most likely diagnosis?
Cerebellar stroke
Acute dystonic reaction
Cerebrovascular accident
Parkinsonism
Wernickes encephalopathy
Triad of Wernicke encephalopathy:
Acute confusion Ataxia
Opthalmoplegia
This patient has received a carbohydrate rich diet without any thiamine or vitamin B co strong replacement. This has led to Wernickes encephalopathy, which classically presents with confusion, ataxia and opthalmoplegia. Characteristically it is associated with chronic alcoholism, however it is also known to occur post bariatric surgery. Please rate this question:
Discuss and give feedback
Next question
Nutrition - Refeeding syndrome
Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person following a period of starvation. The metabolic consequences include:
Hypophosphataemia
Hypokalaemia Hypomagnesaemia Abnormal fluid balance

These abnormalities can lead to organ failure. Re-feeding problems If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels High risk for re-feeding problems If one or more of the following:
BMI < 16 kg/m2
Unintentional weight loss >15% over 3-6 months Little nutritional intake > 10 days Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high)
If two or more of the following:
BMI < 18.5 kg/m2 Unintentional weight loss > 10% over 3-6 months Little nutritional intake > 5 days
History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and antacids
Prescription
Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co
strong 1 tds and supplements
Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4 mmol/kg/day)
Next question

A 22 year old lady receives intravenous morphine for acute abdominal pain. Which of the following best accounts for its analgesic properties?
Binding to δ opioid receptors in the brainstem
Binding to δ opioid receptors at peripheral nerve sites
Binding to β opioid receptors within the CNS
Binding to α opioid receptors within the CNS
Binding to µ opioid receptors within the CNS
4 Types of opioid receptor:
δ (located in CNS)- Accounts for analgesic and antidepressant effects
k (mainly CNS)- analgesic and dissociative effects µ (central and peripheral) - causes analgesia, miosis, decreased gut motility Nociceptin receptor (CNS)- Affect of appetite and tolerance to µ agonists.
Theme from April 2012 Exam Please rate this question:
Discuss and give feedback
Next question
Morphine
Strong opiate analgesic. It is a pro- type narcotic drug and its effects mediated via the 4 types of opioid receptor. Its clinical effects stem from binding to these receptor sites within the CNS and gastrointestinal tract. Unwanted side effects include nausea, constipation, respiratory depression and, if used long term, addiction . It may be administered orally or intravenously. It can be reversed with naloxone.
Next question

Which one of the following reduces the secretion of renin?
Erect posture
Adrenaline
Hyponatraemia
Hypotension
Beta-blockers
Please rate this question:
Discuss and give feedback
Next question
Renin
Renin is secreted by juxtaglomerular cells and hydrolyses angiotensinogen to produce angiotensin I Factors stimulating renin secretion
Hypotension causing reduced renal perfusion Hyponatraemia Sympathetic nerve stimulation Catecholamines
Erect posture
Factors reducing renin secretion
Drugs: beta-blockers, NSAIDs
Next question

Which of the following stimulates prolactin release?
Leutinising hormone
Dopamine
Thyrotropin releasing hormone
Oestrogen
Follicle stimulating hormone
TRH stimulates prolactin release. Dopamine suppresses the release of prolactin.
Please rate this question:
Discuss and give feedback
Next question
Prolactin
Prolactin is a peptide hormone released from the anterior pituitary. It is under tonic dopamine
inhibition, thyrotropin releasing hormone has a stimulatory effect on release. Prolactin release
stimulates milk production but also reduces gonadal activity. It decreases GnRH pulsatility at the
hypothalamic level and to a lesser extent, blocks the action of LH on the ovary or testis.
Next question

Theme: Vitamin deficiency
A. Vitamin A
B. Vitamin B1
C. Vitamin B12
D. Vitamin B3
E. Vitamin C
F. Vitamin K
G. Vitamin D
Please select the vitamin deficiency most closely associated with the situation described. Each
option may be used once, more than once or not at all.
82. A 3 year old child presents with Rickets
You answered Vitamin A
The correct answer is Vitamin D
Vitamin D is needed to help mineralise bone. When this is deficient, mineralisation is inadequate
and deformities mayt result.
83. A 44 year old lady presents with jaundice. Following a minor ward based surgical procedure she
develops troublesome and persistent bleeding.
You answered Vitamin A
The correct answer is Vitamin K
Patients who are jaundiced usually have impaired absorption of vitamin K. This can result in loss
of the vitamin K dependent clotting factors and troublesome bleeding.

84. A 69 year old man who has been living in sheltered accommodation for many months, with
inadequate nutrition notices that his night vision is becoming impaired.
Vitamin A
Loss of vitamin A will result in impair rhodopsin synthesis and poor night vision.
Please rate this question:
Discuss and give feedback
Next question
Vitamin deficiency
Vitamin Effect of deficiency
A Night blindness
Epithelial atrophy
Infections
B1 Beriberi
B2 Dematitis and photosensitivity
B3 Pellagra
B12 Pernicious anaemia

C Poor wound healing
Impaired collagen synthesis
D Rickets (Children)
Osteomalacia (Adults)
K Clotting disorders
Next question

A 55 year old man undergoes a laparotomy and repair of incisional hernia. Which of the following hormones is least likely to be released in increased quantities following the procedure?
Insulin
ACTH
Glucocorticoids
Aldosterone
Growth hormone
Insulin and thyroxine are often have reduced levels of secretion in the post operative period. This, coupled with increased glucocorticoid release may cause difficulty in management of diabetes in individuals with insulin resistance. Please rate this question:
Discuss and give feedback
Next question
Stress response: Endocrine and metabolic changes
Surgery precipitates hormonal and metabolic changes causing the stress response. Stress response is associated with: substrate mobilization, muscle protein loss, sodium and
water retention, suppression of anabolic hormone secretion, activation of the sympathetic nervous system, immunological and haematological changes.
The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and there is a failure of the normal feedback mechanisms of control of hormone secretion.
A summary of the hormonal changes associated with the stress response:
Increased Decreased No Change
Growth hormone Insulin Thyroid stimulating hormone

Increased Decreased No Change
Cortisol Testosterone Luteinizing hormone
Renin Oestrogen Follicle stimulating hormone
Adrenocorticotrophic hormone (ACTH)
Aldosterone
Prolactin
Antidiuretic hormone
Glucagon
Sympathetic nervous system
Stimulates catecholamine release
Causes tachycardia and hypertension
Pituitary gland
ACTH and growth hormone (GH) is stimulated by hypothalamic releasing factors, corticotrophin releasing factor (CRF) and somatotrophin (or growth hormone releasing factor)
Perioperative increased prolactin secretion occurs by release of inhibitory control Secretion of thyroid stimulating hormone (TSH), luteinizing hormone (LH) and follicle
stimulating hormone (FSH) does not change significantly ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH
is produced than needed to produce a maximum adrenocortical response.

Cortisol
Significant increases within 4-6 hours of surgery (>1000 nmol litre-1). The usual negative feedback mechanism fails and concentrations of ACTH and cortisol
remain persistently increased. The magnitude and duration of the increase correlate with the severity of stress and the
response is not abolished by the administration of corticosteroids. The metabolic effects of cortisol are enhanced:
Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein synthesis in the liver Stimulation of lipolysis 'Anti-insulin effect' Mineralocorticoid effects Anti-inflammatory effects Growth hormone
Increased secretion after surgery has a minor role
Most important for preventing muscle protein breakdown and promote tissue repair by insulin growth factors
Alpha Endorphin
Increased
Antidiuretic hormone
An important vasopressor and enhances haemostasis
Renin is released causing the conversion of angiotensinogen to angiotensin I Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone
from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule
Insulin
Release inhibited by stress Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory
effects of catecholamines
Insulin resistance by target cells occurs later The perioperative period is characterized by a state of functional insulin deficiency

Thyroxine (T4) and tri-iodothyronine (T3)
Circulating concentrations are inversely correlated with sympathetic activity and after surgery there is a reduction in thyroid hormone production, which normalises over a few days.
Metabolic effect of endocrine response
Carbohydrate metabolism
Hyperglycaemia is a main feature of the metabolic response to surgery Due to increase in glucose production and a reduction in glucose utilization Catecholamines and cortisol promote glycogenolysis and gluconeogenesis Initial failure of insulin secretion followed by insulin resistance affects the normal responses
The proportion of the hyperglycaemic response reflects the severity of surgery Hyperglycaemia impairs wound healing and increase infection rates
Protein metabolism
Initially there is inhibition of protein anabolism, followed later, if the stress response is severe, by enhanced catabolism
The amount of protein degradation is influenced by the type of surgery and also by the nutritional status of the patient
Mainly skeletal muscle protein is affected
The amino acids released form acute phase proteins (fibrinogen, C reactive protein, complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for gluconeogenesis
Nutritional support has little effect on preventing catabolism
Lipid metabolism Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis and ketone body production. Salt and water metabolism
ADH causes water retention, concentrated urine, and potassium loss and may continue for 3 to 5 days after surgery
Renin causes sodium and water retention
Cytokines
Glycoproteins

Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to
tissue injury from surgery or trauma
IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by the degree of tissue damage Other effects of cytokines include fever, granulocytosis, haemostasis, tissue damage limitation and promotion of healing.
Modifying the response
Opioids suppress hypothalamic and pituitary hormone secretion At high doses the hormonal response to pelvic and abdominal surgery is abolished.
However, such doses prolong recovery and increase the need for postoperative ventilatory support
Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes, although cytokine responses are unaltered
Cytokine release is reduced in less invasive surgery Nutrition prevents the adverse effects of the stress response. Enteral feeding improves
recovery Growth hormone and anabolic steroids may improve outcome
Normothermia decreases the metabolic response
References
Deborah Burton, Grainne Nicholson, and George Hall Endocrine and metabolic response to surgery . Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040
Next question

Which of the following is not a major function of the spleen in adults?
Iron reutilisation
Storage of platelets
Storage of monocytes
Haematopoeisis in haematological disorders
Storage red blood cells
The reservoir function of the spleen is less marked in humans than other animals (e.g. pigs) and in normal individuals it can sequester between 5 and 10% of the red cell mass. The other stated processes are major splenic functions and this accounts for the answer provided. Please rate this question:
Discuss and give feedback
Next question
Spleen
The spleen is located in the left upper quadrant of the abdomen and its size can vary depending upon the amount of blood it contains. The typical adult spleen is 12.5cm long and 7.5cm wide. The usual weight of the adult spleen is 150g. The exact position of the spleen can vary with respiratory activity, posture and the state of surrounding viscera. It usually lies obliquely with its long axis aligned to the 9th, 10th and 11th ribs. It is separated from these ribs by both diaphragm and pleural cavity. The normal spleen is not palpable. The shape of the spleen is influenced by the state of the colon and stomach. Gastric distension will cause the spleen to resemble the shape of an orange segment. Colonic distension will cause it to become more tetrahedral. The spleen is almost entirely covered by peritoneum, which adheres firmly to its capsule. Recesses of the greater sac separate it from the stomach and kidney. It develops from the upper dorsal mesogastrium, remaining connected to the posterior abdominal wall and stomach by two folds of peritoneum; the lienorenal ligament and gastrosplenic ligament. The lienorenal ligament is derived from peritoneum where the wall of the general peritoneum meets the omental bursa between the left kidney and spleen; the splenic vessels lie in its layers. The gastrosplenic ligament also has two layers, formed by the meeting of the walls of the greater sac and omental bursa between spleen and stomach, the short gastric and left gastroepiploic branches of the splenic artery pass in its layers.

Laterally, the spleen is in contact with the phrenicocolic ligament. Relations
Superiorly Diaphragm
Anteriorly Gastric impression
Posteriorly Kidney
Inferiorly Colon
Hilum Tail of pancreas and splenic vessels (splenic artery divides here, branches pass to the
white pulp transporting plasma)
Contents
White
pulp
Immune function. Contains central trabecular artery. The germinal centres are supplied
by arterioles called penicilliary radicles.
Red pulp Filters abnormal red blood cells.
Function
Filtration of abnormal blood cells and foreign bodies such as bacteria. Immunity: IgM. Production of properdin, and tuftsin which help target fungi and bacteria for
phagocytosis.
Haematopoiesis: up to 5th month gestation or in haematological disorders. Pooling: storage of 40% platelets. Iron reutilisation Storage monocytes
Disorders of the spleen Massive splenomegaly
Myelofibrosis Chronic myeloid leukaemia Visceral leishmaniasis (kala-azar)
Malaria Gaucher's syndrome
Other causes (as above plus)
Portal hypertension e.g. secondary to cirrhosis
Lymphoproliferative disease e.g. CLL, Hodgkin's Haemolytic anaemia

Infection: hepatitis, glandular fever Infective endocarditis Sickle-cell*, thalassaemia Rheumatoid arthritis (Felty's syndrome)
*the majority of adult patients with sickle-cell will have an atrophied spleen due to repeated infarction
Next question

Which one of the following is associated with increased lung compliance?
Kyphosis
Pulmonary oedema
Emphysema
Pulmonary fibrosis
Pneumonectomy
Please rate this question:
Discuss and give feedback
Next question
Respiratory physiology: lung compliance
Lung compliance is defined as change in lung volume per unit change in airway pressure Causes of increased compliance
age emphysema - this is due to loss alveolar walls and associated elastic tissue
Causes of decreased compliance
pulmonary oedema pulmonary fibrosis pneumonectomy kyphosis
Next question

Which of the following areas is predominantly concerned with thermoregulation?
Hypothalamus
Anterior pituitary
Cerebellum
Brain stem
Temporal lobe
Theme from 2012 Exam The hypothalamus is primarily concerned with thermoregulation. It may relay to the cerebral cortex to induce behavioural adaptation to facilitate the thermoregulatory process. Please rate this question:
Discuss and give feedback
Next question
Thermoregulation
The hypothalamus is the main centre for thermoregulation. Peripheral and central thermoreceptors relay to this region.
Central thermoreceptors play the main role in maintenance of core temperature. Hypothalamus may initiate involuntary motor responses to raise body temperature
(e.g.shivering). It will also stimulate the sympathetic nervous system to produce peripheral vasoconstriction and release of adrenaline from the adrenal medulla.
Heat loss is governed by behavioural responses and by autonomic responses including peripheral vasodilation.
Heat loss can be maintained within the thermoneutral zone (25 to 30 degrees) although the absolute value depends upon atmospheric humidity.
Sepsis results in the release of cytokines that reset the thermoregulatory centre resulting in fever.
Next question

Theme: Acid - base disorders
A. pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20
B. pH 7.25 pO2 8.9 pCO2 3.2 HCO3 10
C. pH 7.20 pO2 6.2 pCO2 8.2 HCO3 27
D. pH 7.60 pO2 8.2 pCO2 5.8 HCO3 40
E. pH 7.45 pO2 7.2 pCO2 2.5 HCO3 24 Please match the diagnosis with the arterial blood gas result. Each option may be used once, more than once or not at all.
89. Pulmonary embolus
You answered pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20
The correct answer is pH 7.45 pO2 7.2 pCO2 2.5 HCO3 24
A combination of hypoxia and respiratory alkalosis should suggest a pulmonary embolus.
The respiratory alkalosis is due to hyperventilation associated with the pulmonary
embolism.
90. High output ureterosigmoidostomy
You answered pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20
The correct answer is pH 7.25 pO2 8.9 pCO2 3.2 HCO3 10
There is acidosis. To compensate the patient will attempt to raise the pH level in the blood
by hyperventilating, hence the low CO2 level .
91. Widespread mesenteric infarction
You answered pH 7.64 pO2 10.0 kPa pCO2 2.8 kPa HCO3 20
The correct answer is pH 7.25 pO2 8.9 pCO2 3.2 HCO3 10
This is usually associated with acidosis, hyperventillation and reduction in bicarbonate.
Please rate this question:
Discuss and give feedback
Next question

Disorders of acid - base balance
Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ sections. The acid-base normogram below shows how the various disorders may be categorised
Image sourced from Wikipedia
Metabolic acidosis
This is the most common surgical acid - base disorder.
Reduction in plasma bicarbonate levels. Two mechanisms:
1. Gain of strong acid (e.g. diabetic ketoacidosis) 2. Loss of base (e.g. from bowel in diarrhoea) - Classified according to the anion gap, this can be calculated by: (Na+ + K+) - (Cl- + HCO3
-). - If a question supplies the chloride level then this is often a clue that the anion gap should be calculated. The normal range = 10-18 mmol/L Normal anion gap ( = hyperchloraemic metabolic acidosis)
Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula

Renal tubular acidosis Drugs: e.g. acetazolamide Ammonium chloride injection Addison's disease
Raised anion gap
Lactate: shock, hypoxia Ketones: diabetic ketoacidosis, alcohol
Urate: renal failure Acid poisoning: salicylates, methanol
Metabolic acidosis secondary to high lactate levels may be subdivided into two types:
Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns)
Lactic acidosis type B: (Metabolic e.g. metformin toxicity)
Metabolic alkalosis
Usually caused by a rise in plasma bicarbonate levels.
Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess bicarbonate.
Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of the kidney or gastrointestinal tract
Causes
Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction)
Diuretics Liquorice, carbenoxolone Hypokalaemia Primary hyperaldosteronism
Cushing's syndrome Bartter's syndrome Congenital adrenal hyperplasia
Mechanism of metabolic alkalosis

Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised
aldosterone levels
In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H+ into cells to maintain neutrality
Respiratory acidosis
Rise in carbon dioxide levels usually as a result of alveolar hypoventilation Renal compensation may occur leading to Compensated respiratory acidosis
Causes
COPD
Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary oedema
Sedative drugs: benzodiazepines, opiate overdose
Respiratory alkalosis
Hyperventilation resulting in excess loss of carbon dioxide This will result in increasing pH
Causes
Psychogenic: anxiety leading to hyperventilation Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude Early salicylate poisoning*
CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis Pregnancy
*Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of salicylates (combined with acute renal failure) may lead to an acidosis
Next question

A 45 year old male is diagnosed with carcinoma of the head of the pancreas. He reports that his stool sticks to the commode and will not flush away. Loss of which of the following enzymes is most likely to be responsible for this problem?
Lipase
Amylase
Trypsin
Elastase
None of the above
Theme from April 2014 Exam Loss of lipase is one of the key features in the development of steatorrhoea which typically consists of pale and offensive stools that are difficult to flush away. Please rate this question:
Discuss and give feedback
Next question
Pancreatic cancer
Adenocarcinoma Risk factors: Smoking, diabetes, adenoma, familial adenomatous polyposis Mainly occur in the head of the pancreas (70%) Spread locally and metastasizes to the liver
Carcinoma of the pancreas should be differentiated from other periampullary tumours with better prognosis
Clinical features
Weight loss
Painless jaundice Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a late feature) Pancreatitis Trousseau's sign: migratory superficial thrombophlebitis

Investigations
USS: May miss small lesions CT Scanning (pancreatic protocol). If unresectable on CT then no further staging needed
PET/CT for those with operable disease on CT alone ERCP/ MRI for bile duct assessment Staging laparoscopy to exclude peritoneal disease
Management
Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer techniques include pylorus preservation and SMA/ SMV resection
Carcinoma body and tail: poor prognosis, distal pancreatectomy, if operable Usually adjuvent chemotherapy for resectable disease ERCP and stent for jaundice and palliation
Surgical bypass may be needed for duodenal obstruction
Next question

Which of the following drugs does not interfere with the laboratory analysis of serum cortisol levels?
Dexamethasone
Prednisolone
Hydrocortisone IV
Hydrocortisone PO
Hydrocortisone IM
Prednisolone and it's metabolites can chemically mimic cortisol in radio-immunoassay techniques of laboratory analysis.
Dexamethasone can be given as glucorticoid replacement during testing for addisons or adrenal insufficiency as it does not interfere with cortisol levels. For example, if you have a patient with polymyalgia rheumatica and they are on long term prednisolone, you can replace the prednisolone with dexamethasone to undertake a short synacthen test. Please rate this question:
Discuss and give feedback
Next question
Cortisol
Glucocorticoid Released by zona fasiculata of the adrenal gland 90% protein bound; 10% active Circadian rhythm: High in the mornings
Negative feedback via ACTH
Actions
Glycogenolysis
Gluconeogenesis Protein catabolism Lipolysis Stress response Anti-inflammatory

Decrease protein in bones Increase gastric acid Increases neutrophils/platelets/red blood cells Inhibits fibroblastic activity
Next question

An elderly lady who presented with weight loss and malabsorption was found to have amyloid of the
small bowel. On presentation she was found to have osteomalacia and was hypocalcaemic. Over
the past seven days she has received total parenteral nutrition with adequate calcium replacement.
Despite this she remained hypocalcaemic. Deficiency of which of the following electrolytes is most
likely to account for this process?
Magnesium
Potassium
Sodium
Phosphate
None of the above
Theme from September 2015 Exam
Patients with malabsorption may develop magnesium deficiency, although her TPN feeds may have
contained magnesium it may not have been sufficient to correct her losses. Sodium, phosphate and
potassium would not have this effect on serum calcium.
Please rate this question:
Discuss and give feedback
Next question
Combined deficiency of magnesium and calcium
Magnesium is required for both PTH secretion and its action on target tissues. Hypomagnesaemia
may both cause hypocalcaemia and render patients unresponsive to treatment with calcium and
vitamin D supplementation.
Magnesium is the fourth most abundant cation in the body. The body contains 1000mmol, with half
contained in bone and the remainder in muscle, soft tissues and extracellular fluid. There is no one

specific hormonal control of magnesium and various hormones including PTH and aldosterone affect
the renal handling of magnesium.
Magnesium and calcium interact at a cellular level also and as a result decreased magnesium will
tend to affect the permeability of cellular membranes to calcium, resulting in hyperexcitability.
Next question

A 19 year old man is attacked outside a club and beaten with a baseball bat. He sustains a blow to the right side of his head. He is brought to the emergency department and a policy of observation is adopted. His glasgow coma score deteriorates and he becomes comatose. Which of the following haemodynamic parameters is most likely to be present?
Hypertension and bradycardia
Hypotension and tachycardia
Hypotension and bradycardia
Hypertension and tachycardia
Normotension and bradycardia
Theme from April 2013 Exam Hypertension and bradycardia are seen prior to coning. The brain autoregulates its blood supply by controlling systemic blood pressure. Please rate this question:
Discuss and give feedback
Next question
Head injury
Patients who suffer head injuries should be managed according to ATLS principles and extra cranial injuries should be managed alongside cranial trauma. Inadequate cardiac output will compromise CNS perfusion irrespective of the nature of the cranial injury. Types of traumatic brain injury
Extradural
haematoma
Bleeding into the space between the dura mater and the skull. Often results from
acceleration-deceleration trauma or a blow to the side of the head. The majority
of extradural haematomas occur in the temporal region where skull fractures
cause a rupture of the middle meningeal artery.
Features
Raised intracranial pressure
Some patients may exhibit a lucid interval

Subdural
haematoma
Bleeding into the outermost meningeal layer. Most commonly occur around the
frontal and parietal lobes. May be either acute or chronic.
Risk factors include old age and alcoholism.
Slower onset of symptoms than a extradural haematoma.
Subarachnoid
haemorrhage
Usually occurs spontaneously in the context of a ruptured cerebral aneurysm, but
may be seen in association with other injuries when a patient has sustained a
traumatic brain injury.
Pathophysiology
Primary brain injury may be focal (contusion/ haematoma) or diffuse (diffuse axonal injury)
Diffuse axonal injury occurs as a result of mechanical shearing following deceleration, causing disruption and tearing of axons
Intra-cranial haematomas can be extradural, subdural or intracerebral, while contusions may occur adjacent to (coup) or contralateral (contre-coup) to the side of impact
Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory processes are disrupted following trauma rendering the brain more susceptible to blood flow changes and hypoxia
The Cushings reflex (hypertension and bradycardia) often occurs late and is usually a pre terminal event
Management
Where there is life threatening rising ICP such as in extra dural haematoma and whilst theatre is prepared or transfer arranged use of IV mannitol/ frusemide may be required.
Diffuse cerebral oedema may require decompressive craniotomy
Exploratory Burr Holes have little management in modern practice except where scanning may be unavailable and to thus facilitate creation of formal craniotomy flap
Depressed skull fractures that are open require formal surgical reduction and debridement, closed injuries may be managed non operatively if there is minimal displacement.
ICP monitoring is appropriate in those who have GCS 3-8 and normal CT scan.
ICP monitoring is mandatory in those who have GCS 3-8 and abnormal CT scan. Hyponatraemia is most likely to be due to syndrome of inappropriate ADH secretion. Minimum of cerebral perfusion pressure of 70mmHg in adults. Minimum cerebral perfusion pressure of between 40 and 70 mmHg in children.
Interpretation of pupillary findings in head injuries
Pupil size Light response Interpretation

Pupil size Light response Interpretation
Unilaterally dilated Sluggish or fixed 3rd nerve compression secondary to tentorial
herniation
Bilaterally dilated Sluggish or fixed Poor CNS perfusion
Bilateral 3rd nerve palsy
Unilaterally dilated or
equal
Cross reactive (Marcus -
Gunn)
Optic nerve injury
Bilaterally constricted May be difficult to
assess
Opiates
Pontine lesions
Metabolic encephalopathy
Unilaterally
constricted
Preserved Sympathetic pathway disruption
Next question

Which of the following drugs does not cause pseudohaematuria?
Rifampicin
Quinine
Noradrenaline
Levodopa
Phenytoin
Rifampicin, phenytoin, levodopa, methyldopa, and quinine all cause pseudohaematuria. Please rate this question:
Discuss and give feedback
Next question
Haematuria
Causes of haematuria
Trauma Injury to renal tract
Renal trauma commonly due to blunt injury (others penetrating
injuries)
Ureter trauma rare: iatrogenic
Bladder trauma: due to RTA or pelvic fractures
Infection Remember TB
Malignancy Renal cell carcinoma (remember paraneoplastic syndromes):
painful or painless
Urothelial malignancies: 90% are transitional cell carcinoma, can
occur anywhere along the urinary tract. Painless haematuria.
Squamous cell carcinoma and adenocarcinoma: rare bladder
tumours
Prostate cancer

Penile cancers: SCC
Renal disease Glomerulonephritis
Stones Microscopic haematuria common
Structural
abnormalities
Benign prostatic hyperplasia (BPH) causes haematuria due to
hypervascularity of the prostate gland
Cystic renal lesions e.g. polycystic kidney disease
Vascular malformations
Renal vein thrombosis due to renal cell carcinoma
Coagulopathy Causes bleeding of underlying lesions
Drugs Cause tubular necrosis or interstitial nephritis: aminoglycosides,
chemotherapy
Interstitial nephritis: penicillin, sulphonamides, and NSAIDs
Anticoagulants
Benign Exercise
Gynaecological Endometriosis: flank pain, dysuria, and haematuria that is cyclical
Iatrogenic Catheterisation
Radiotherapy; cystitis, severe haemorrhage, bladder necrosis
Pseudohaematuria For example following consumption of beetroot
References Http://bestpractice.bmj.com/best-practice/monograph/316/overview/aetiology.html
Next question

A 74-year-old woman with thyroid cancer is admitted due to shortness of breath. What is the best
investigation to assess for possible compression of the upper airways?
Arterial blood gases
Forced vital capacity
Transfer factor
Peak expiratory flow rate
Flow volume loop
Flow volume loop is the investigation of choice for upper airway compression.
Please rate this question:
Discuss and give feedback
Next question
Flow volume loop
A normal flow volume loop is often described as a 'triangle on top of a semi circle'
Flow volume loops are the most suitable way of assessing compression of the upper airway
Next question

Which of the following statements relating to cerebrospinal fluid is untrue?
The choroid plexus is only present in the lateral ventricles
Total CSF volume is 100-150ml
CSF pressure is usually 10-15mmHg
The cerebral aqueduct connects the third and fourth ventricles
The foramen of Luschka are paired and lie laterally in the fourth ventricle
The choroid plexus lies in all ventricles. Please rate this question:
Discuss and give feedback
Next question
Cerebrospinal fluid
The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain). The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the arachnoid granulations which project into the venous sinuses. Circulation
1. Lateral ventricles (via foramen of Munro) 2. 3rd ventricle 3. Cerebral aqueduct (aqueduct of Sylvius) 4. 4th ventricle (via foramina of Magendie and Luschka) 5. Subarachnoid space 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus Composition
Glucose: 50-80mg/dl
Protein: 15-40 mg/dl Red blood cells: Nil White blood cells: 0-3 cells/ mm3
Next question

Which substance can be used to achieve the most accurate measurement of the glomerular filtration rate?
Glucose
Protein
Inulin
Creatinine
Para-amino hippuric acid
Theme from April 2016 exam Creatinine declines with age due to decline in renal function and muscle mass. Glucose, protein (amino acids) and PAH are reabsorbed by the kidney. Please rate this question:
Discuss and give feedback
Next question
Renal Physiology
Overview
Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular capillary bed.
Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary vasa recta.
The kidney receives up to 25% of resting cardiac output.
Control of blood flow
The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg so there is little variation in renal blood flow.
This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal signals (e.g. renin) are responsible.

Glomerular structure and function
Blood inside the glomerulus has considerable hydrostatic pressure. The basement membrane has pores that will allow free diffusion of smaller solutes, larger
negatively charged molecules such as albumin are unable to cross. The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,
times the volume of urine produced per minute, divided by the plasma concentration (assuming that the solute is freely diffused e.g. inulin).
In clinical practice creatinine is used because it is subjected to very little proximal tubular secretion.
Although subject to variability, the typical GFR is 125ml per minute. Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and
entering the bowman's capsule
Renal clearance = volume plasma from which a substance is removed per minute by the kidneys
Substances used to measure GFR have the following features: 1. Inert 2. Free filtration from the plasma at the glomerulus (not protein bound) 3. Not absorbed or secreted at the tubules 4. Plasma concentration constant during urine collection Examples: inulin, creatinine GFR = urine concentration (mmol/l) x urine volume (ml/min) -------------------------------------------------------------------------- plasma concentration (mmol/l)
The clearance of a substance is dependent not only on its diffusivity across the basement membrane but also subsequent tubular secretion and / or reabsorption.
So glucose which is freely filtered across the basement membrane is usually reabsorbed from tubules giving a clearance of zero.
Tubular function
Reabsorption and secretion of substances occurs in the tubules.
In the proximal tubule substrates such as glucose, amino acids and phosphate are co-transported with sodium across the semi permeable membrane.
Up to two thirds of filtered water is reabsorbed in the proximal tubules.
This will lead to increase in urea concentration in the distal tubule allowing for its increased diffusion.
Substances to be secreted into the tubules are taken up from the peritubular blood by tubular cells.

Solutes such as paraaminohippuric acid are cleared with a single passage through the kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and phosphate will have a tubular reabsorption that is influenced by plasma PTH levels.
Potassium may be both secreted and re-absorbed and is co-exchanged with sodium.
Loop of Henle
Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of the loop of Henle in 24 hours.
Loops from the juxtamedullary nephrons run deep into the medulla. The osmolarity of fluid changes and is greatest at the tip of the papilla. The thin ascending limb is impermeable to water, but highly permeable to sodium and
chloride ions.
This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic compared with adjacent interstitial fluid.
In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both facilitated and passive diffusion pathways.
The loops of Henle are co-located with vasa recta, these will have similar solute compositions to the surrounding extracellular fluid so preventing the diffusion and subsequent removal of this hypertonic fluid.
The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps to maintain this osmotic gradient.
Next question

A 45 year old man sustains a closed head injury. He is initially alert, however, his level of consciousness deteriorates on arrival at hospital. An intra cranial pressure monitor is inserted. What is the normal intracranial pressure?
35 - 45mm Hg
45 - 55mm Hg
<15mm Hg
25 - 35mm Hg
25 - 30 mm Hg
The normal intracranial pressure is between 7 and 15 mm Hg. The brain can accommodate increases up to 24 mm Hg, thereafter clinical features will become evident. Please rate this question:
Discuss and give feedback
Next question
Applied neurophysiology
Pressure within the cranium is governed by the Monroe-Kelly doctrine. This considers the skull as a closed box. Increases in mass can be accommodated by loss of CSF. Once a critical point is reached (usually 100- 120ml of CSF lost) there can be no further compensation and ICP rises sharply. The next step is that pressure will begin to equate with MAP and neuronal death will occur. Herniation will also accompany this process.
The CNS can autoregulate its own blood supply. Vaso constriction and dilatation of the cerebral blood vessels is the primary method by which this occurs. Extremes of blood pressure can exceed this capacity resulting in risk of stroke. Other metabolic factors such as hypercapnia will also cause vasodilation, which is of importance in ventilating head injured patients.
The brain can only metabolise glucose, when glucose levels fall, consciousness will be impaired.
Next question

A 55-year-old man with a history of type 2 diabetes mellitus, bipolar disorder and chronic obstructive pulmonary disease has bloods taken during a pre operative assessment of an inguinal hernia repair:
Na+ 125 mmol/l
K+ 3.8 mmol/l
Bicarbonate 24 mmol/l
Urea 3.7 mmol/l
Creatinine 92 µmol/l
Due to his smoking history a chest x-ray is ordered which is reported as normal. The Consultant asks you what is the most likely cause for the hyponatraemia?
Metformin
Lithium
Carbamazepine
Sodium valproate
Pioglitazone
SIADH - drug causes: carbamazepine, sulfonylureas, SSRIs, tricyclics
Lithium can cause diabetes insipidus but this is generally associated with a high sodium. Lithium only tends to cause raised antidiuretic hormone levels following a severe overdosage. Please rate this question:
Discuss and give feedback
Next question
syndrome of inappropriate antidiuretic hormone (SIADH): causes
Malignancy
especially small cell lung cancer

also: pancreas, prostate
Neurological
stroke
subarachnoid haemorrhage subdural haemorrhage meningitis/encephalitis/abscess
Infections
tuberculosis pneumonia
Drugs
sulfonylureas SSRIs, tricyclics carbamazepine vincristine
cyclophosphamide
Other causes
positive end-expiratory pressure (PEEP) porphyrias
Next question

A 24 year old man is involved in a road traffic accident. His right leg is trapped for 6 hours whilst he is moved. On examination his foot is insensate and a dorsalis pedis pulse is only weakly felt. Which of the biochemical abnormalities listed below is most likely to be present?
Alkalosis
Hypercalcaemia
Hypocalcaemia
Hyperkalaemia
Hyponatraemia
In this scenario the patient will have a compartment syndrome, delayed diagnosis and muscle death. The effect of muscle death will result in the release of potassium. It is also highly likely that there will be a degree of renal impairment, the result of which is that the serum potassium is likely to be high. Please rate this question:
Discuss and give feedback
Next question
Hyperkalaemia
Plasma potassium levels are regulated by a number of factors including aldosterone, acid-base balance and insulin levels.
Metabolic acidosis is associated with hyperkalaemia as hydrogen and potassium ions compete with each other for exchange with sodium ions across cell membranes and in the distal tubule.
ECG changes seen in hyperkalaemia include tall-tented T waves, small P waves, widened QRS leading to a sinusoidal pattern and asystole
Causes of hyperkalaemia
Acute renal failure Drugs*: potassium sparing diuretics, ACE inhibitors, angiotensin 2 receptor blockers,
spironolactone, ciclosporin, heparin** Metabolic acidosis Addison's Tissue necrosis/rhabdomylosis: burns, trauma

Massive blood transfusion
Foods that are high in potassium
Salt substitutes (i.e. Contain potassium rather than sodium)
Bananas, oranges, kiwi fruit, avocado, spinach, tomatoes
*beta-blockers interfere with potassium transport into cells and can potentially cause hyperkalaemia in renal failure patients - remember beta-agonists, e.g. Salbutamol, are sometimes used as emergency treatment **both unfractionated and low-molecular weight heparin can cause hyperkalaemia. This is thought to be caused by inhibition of aldosterone secretion
Next question

A 39 year old lady has recurrent attacks of biliary colic. What is the approximate volume of bile to
enter the duodenum per 24 hours?
500 mL
50 mL
100 mL
2000 mL
150 mL
Between 500 mL and 1.5 L of bile enters the small bowel daily. Most bile salts are recycled by the
enterohepatic circulation. When the gallbladder contracts the lumenal pressure is approximately
25cm water, which is why biliary colic may be so painful.
Please rate this question:
Discuss and give feedback
Next question
Bile
Bile is produced at a rate of between 500ml and 1500mL per day. Bile is composed of bile salts,
bicarbonate, cholesterol, steroids and water. There are three main factors regulating bile flow;
hepatic secretion, gall bladder contraction and sphincter of oddi resistance. Bile salts are absorbed
in the terminal ileum (and recycled to the liver). Over 90% of all bile salts are recycled in this way,
such that the total pool of bile salts is recycled up to six times a day.
Primary bile salts
Cholate and chenodeoxycholate.
Secondary bile salts

Formed by bacterial action on primary bile salts. These are deoxycholate and lithocholate. Of these
deoxycholate is reabsorbed, whilst lithocholate is insoluble and excreted.
Pathophysiology of gallstones
Bile salts have a detergent action. They aggregate to form micelles and these have a lipid centre in
which fats may be transported. Excessive quantities of cholesterol cannot be transported in this way
and will tend to precipitate, resulting in the formation of cholesterol rich gallstones.
Next question

At which of the following sites is the most water absorbed?
Right colon
Left colon
Stomach
Jejunum
Duodenum
Water absorption in the gastrointestinal tract predominantly occurs in the small bowel (jejunum and
ileum). The colon is an important site of water absorption, however, its overall contribution is
relatively small. The importance of the colonic component to water absorption may increase
following extensive small bowel resections.
Please rate this question:
Discuss and give feedback
Next question
Water absorption
During a 24 hours period the average person will ingest up to 2000ml of liquid orally. In addition a
further 8000ml of fluid will enter the small bowel as gastrointestinal secretions. Intestinal water
absorption is a passive process and is related to solute load. In the jejunum the active absorption of
glucose and amino acids will create a concentration gradient that water will flow across. In the ileum
most water is absorbed by a process of facilitated diffusion (with sodium).
Approximately 150ml of water enters the colon daily, most is absorbed, the colon can adapt to, and
increase this amount following resection.
Next question

Which of the following is not a characteristic of the proximal convoluted tubule in the kidney?
Up to 95% of filtered amino acids will be reabsorbed at this site
It is a risk of damage in a patient with compartment syndrome due to a tibial fracture
It is responsible for absorbing more than 50% of filtered water
Its secretory function is most effective at low systolic blood pressures (typically less than
100mmHg)
Glucose is reabsorbed by a process of facilitated diffusion
The proximal convoluted tubule may undergo necrosis in situations such as compartment syndrome. It is responsible for reabsorbing up to two thirds of filtered water. Low systolic blood pressures (below the renal autoregulatory range) are a risk factor for acute tubular necrosis. Within the autoregulatory range the absolute value of systolic BP has little effect. Please rate this question:
Discuss and give feedback
Next question
Renal Physiology
Overview
Each nephron is supplied with blood from an afferent arteriole that opens onto the glomerular capillary bed.
Blood then flows to an efferent arteriole, supplying the peritubular capillaries and medullary vasa recta.
The kidney receives up to 25% of resting cardiac output.
Control of blood flow
The kidney is able to autoregulate its blood flow between systolic pressures of 80- 180mmHg so there is little variation in renal blood flow.
This is achieved by myogenic control of arteriolar tone, both sympathetic input and hormonal signals (e.g. renin) are responsible.

Glomerular structure and function
Blood inside the glomerulus has considerable hydrostatic pressure. The basement membrane has pores that will allow free diffusion of smaller solutes, larger
negatively charged molecules such as albumin are unable to cross. The glomerular filtration rate (GFR) is equal to the concentration of a solute in the urine,
times the volume of urine produced per minute, divided by the plasma concentration (assuming that the solute is freely diffused e.g. inulin).
In clinical practice creatinine is used because it is subjected to very little proximal tubular secretion.
Although subject to variability, the typical GFR is 125ml per minute. Glomerular filtration rate = Total volume of plasma per unit time leaving the capillaries and
entering the bowman's capsule
Renal clearance = volume plasma from which a substance is removed per minute by the kidneys
Substances used to measure GFR have the following features: 1. Inert 2. Free filtration from the plasma at the glomerulus (not protein bound) 3. Not absorbed or secreted at the tubules 4. Plasma concentration constant during urine collection Examples: inulin, creatinine GFR = urine concentration (mmol/l) x urine volume (ml/min) -------------------------------------------------------------------------- plasma concentration (mmol/l)
The clearance of a substance is dependent not only on its diffusivity across the basement membrane but also subsequent tubular secretion and / or reabsorption.
So glucose which is freely filtered across the basement membrane is usually reabsorbed from tubules giving a clearance of zero.
Tubular function
Reabsorption and secretion of substances occurs in the tubules.
In the proximal tubule substrates such as glucose, amino acids and phosphate are co-transported with sodium across the semi permeable membrane.
Up to two thirds of filtered water is reabsorbed in the proximal tubules.
This will lead to increase in urea concentration in the distal tubule allowing for its increased diffusion.
Substances to be secreted into the tubules are taken up from the peritubular blood by tubular cells.

Solutes such as paraaminohippuric acid are cleared with a single passage through the kidneys and this is why it is used to measure renal plasma flow. Ions such as calcium and phosphate will have a tubular reabsorption that is influenced by plasma PTH levels.
Potassium may be both secreted and re-absorbed and is co-exchanged with sodium.
Loop of Henle
Approximately 60 litres of water containing 9000mmol sodium enters the descending limb of the loop of Henle in 24 hours.
Loops from the juxtamedullary nephrons run deep into the medulla. The osmolarity of fluid changes and is greatest at the tip of the papilla. The thin ascending limb is impermeable to water, but highly permeable to sodium and
chloride ions.
This loss means that at the beginning of the thick ascending limb the fluid is hypo osmotic compared with adjacent interstitial fluid.
In the thick ascending limb the reabsorption of sodium and chloride ions occurs by both facilitated and passive diffusion pathways.
The loops of Henle are co-located with vasa recta, these will have similar solute compositions to the surrounding extracellular fluid so preventing the diffusion and subsequent removal of this hypertonic fluid.
The energy dependent reabsorption of sodium and chloride in the thick ascending limb helps to maintain this osmotic gradient.
Next question

An arterial blood gas sample is taken and the following results obtained;
PaO2 8kPa
PaCO2 4kPa
pH 7.4
With which of the following are these values most consistent?
Compensated metabolic alkalosis
Pulmonary atelectasis
Alveolar hypoventilation
Residing at 4500M for 48 hours
LAD occlusion
The patient has low oxygen tension and low carbon dioxide. The pH is normal so there is
compensation for a long standing condition in which oxygenation is reduced. There is neither
alkalosis, nor hypoventilation as the carbon dioxide is low. At very high altitude, the low oxygen
tension can exceed the anaerobic threshold and carbon dioxide levels increase.
Please rate this question:
Discuss and give feedback
Next question
Arterial blood gas interpretation

In advanced life support training, a 5 step approach to arterial blood gas interpretation is advocated.
1. How is the patient?
2. Is the patient hypoxaemic?
The Pa02 on air should be 10.0-13.0 kPa
3. Is the patient acidaemic (pH <7.35) or alkalaemic (pH >7.45)
4. What has happened to the PaCO2?
If there is acidaemia, an elevated PaCO2 will account for this
5. What is the bicarbonate level or base excess?
A metabolic acidosis will have a low bicarbonate level and a low base excess (< -2 mmol)
A metabolic alkalosis will have a high bicarbonate and a high base excess (> +2 mmol)
Next question

Which of the following does not cause a normal anion gap acidosis?
Pancreatic fistula
Acetazolamide
Uraemia
Ureteric diversion
Renal tubular acidosis
Normal Gap Acidosis: HARDUP H - Hyperalimentation/hyperventilation A - Acetazolamide R - Renal tubular acidosis D - Diarrhoea U - Ureteral diversion P - Pancreatic fistula/parenteral saline
Uraemia will typically cause a high anion gap acidosis. It is one of the unmeasured anions. Please rate this question:
Discuss and give feedback
Next question
Disorders of acid - base balance
Disorders of acid- base balance are often covered in the MRCS part A, both in the SBA and EMQ sections. The acid-base normogram below shows how the various disorders may be categorised

Image sourced from Wikipedia
Metabolic acidosis
This is the most common surgical acid - base disorder.
Reduction in plasma bicarbonate levels. Two mechanisms:
1. Gain of strong acid (e.g. diabetic ketoacidosis) 2. Loss of base (e.g. from bowel in diarrhoea) - Classified according to the anion gap, this can be calculated by: (Na+ + K+) - (Cl- + HCO3
-). - If a question supplies the chloride level then this is often a clue that the anion gap should be calculated. The normal range = 10-18 mmol/L Normal anion gap ( = hyperchloraemic metabolic acidosis)
Gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula
Renal tubular acidosis Drugs: e.g. acetazolamide Ammonium chloride injection Addison's disease
Raised anion gap

Lactate: shock, hypoxia Ketones: diabetic ketoacidosis, alcohol Urate: renal failure Acid poisoning: salicylates, methanol
Metabolic acidosis secondary to high lactate levels may be subdivided into two types:
Lactic acidosis type A: (Perfusion disorders e.g.shock, hypoxia, burns) Lactic acidosis type B: (Metabolic e.g. metformin toxicity)
Metabolic alkalosis
Usually caused by a rise in plasma bicarbonate levels.
Rise of bicarbonate above 24 mmol/L will typically result in renal excretion of excess bicarbonate.
Caused by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to problems of the kidney or gastrointestinal tract
Causes
Vomiting / aspiration (e.g. Peptic ulcer leading to pyloric stenosis, nasogastric suction)
Diuretics Liquorice, carbenoxolone Hypokalaemia Primary hyperaldosteronism Cushing's syndrome Bartter's syndrome
Congenital adrenal hyperplasia
Mechanism of metabolic alkalosis
Activation of renin-angiotensin II-aldosterone (RAA) system is a key factor
Aldosterone causes reabsorption of Na+ in exchange for H+ in the distal convoluted tubule ECF depletion (vomiting, diuretics) → Na+ and Cl- loss → activation of RAA system → raised
aldosterone levels In hypokalaemia, K+ shift from cells → ECF, alkalosis is caused by shift of H+ into cells to
maintain neutrality

Respiratory acidosis
Rise in carbon dioxide levels usually as a result of alveolar hypoventilation Renal compensation may occur leading to Compensated respiratory acidosis
Causes
COPD Decompensation in other respiratory conditions e.g. Life-threatening asthma / pulmonary
oedema
Sedative drugs: benzodiazepines, opiate overdose
Respiratory alkalosis
Hyperventilation resulting in excess loss of carbon dioxide
This will result in increasing pH
Causes
Psychogenic: anxiety leading to hyperventilation
Hypoxia causing a subsequent hyperventilation: pulmonary embolism, high altitude Early salicylate poisoning* CNS stimulation: stroke, subarachnoid haemorrhage, encephalitis Pregnancy
*Salicylate overdose leads to a mixed respiratory alkalosis and metabolic acidosis. Early stimulation of the respiratory centre leads to a respiratory alkalosis whilst later the direct acid effects of salicylates (combined with acute renal failure) may lead to an acidosis
Next question

Which one of the following would cause a rise in the carbon monoxide transfer factor (TLCO)?
Emphysema
Pulmonary embolism
Pulmonary haemorrhage
Pneumonia
Pulmonary fibrosis
Transfer factor
raised: asthma, haemorrhage, left-to-right shunts, polycythaemia low: everything else
Where alveolar haemorrhage occurs the TLCO tends to increase due to the enhanced uptake of carbon monoxide by intra-alveolar haemoglobin. Please rate this question:
Discuss and give feedback
Next question
Transfer factor
The transfer factor describes the rate at which a gas will diffuse from alveoli into blood. Carbon monoxide is used to test the rate of diffusion. Results may be given as the total gas transfer (TLCO) or that corrected for lung volume (transfer coefficient, KCO)
Causes of a raised TLCO
asthma
pulmonary haemorrhage (Wegener's, Goodpasture's)
left-to-right cardiac shunts
polycythaemia
hyperkinetic states
Causes of a lower TLCO
pulmonary fibrosis
pneumonia
pulmonary emboli
pulmonary oedema
emphysema

male gender, exercise anaemia
low cardiac output
KCO also tends to increase with age. Some conditions may cause an increased KCO with a normal or reduced TLCO
pneumonectomy/lobectomy scoliosis/kyphosis neuromuscular weakness
ankylosis of costovertebral joints e.g. ankylosing spondylitis
Next question

Which of the following is least likely to be associated with hypercalcaemia?
Thiazides
Antacids
Coeliac disease
Sarcoidosis
Zolinger-Ellison syndrome
Mnemonic for the causes of hypercalcaemia: CHIMPANZEES C alcium supplementation H yperparathyroidism I atrogentic (Drugs: Thiazides) M ilk Alkali syndrome P aget disease of the bone A cromegaly and Addison's Disease N eoplasia Z olinger-Ellison Syndrome (MEN Type I) E xcessive Vitamin D E xcessive Vitamin A S arcoidosis
Patients with coeliac disease tend to develop hypocalcaemia due to malabsorption of calcium by the bowel. Please rate this question:
Discuss and give feedback
Next question
Hypercalcaemia
Main causes
Malignancy (most common cause in hospital in-patients) Primary hyperparathyroidism (commonest cause in non hospitalised patients)

Less common
Sarcoidosis (extrarenal synthesis of calcitriol ) Thiazides, lithium
Immobilisation Pagets disease Vitamin A/D toxicity Thyrotoxicosis MEN Milk alkali syndrome
Clinical features
Stones, bones, abdominal groans, and psychic moans High serum calcium levels result in decreased neuronal excitability. Therefore sluggish reflexes, muscle weakness and constipation may occur.
Next question

Release of somatostatin from the pancreas will result in which of the following?
Decrease in pancreatic exocrine secretions
Contraction of the gallbladder
Increase in the rate of gastric emptying
Increased synthesis of growth hormone
Increased insulin release
Octreotide reduces exocrine pancreatic secretions so is used to treat high output pancreatic fistulae
(though parenteral feeding is most effective). Other uses include variceal bleeding and treatment of
acromegaly.
Inhibits growth hormone and insulin release (when released from pancreas).
Somatostatin is also released by the hypothalamus causing a negative feedback response on
growth hormone.
Please rate this question:
Discuss and give feedback
Next question
Somatostatin
Somatostatin is produced in the D cells of the pancreatic islets. It is also produced in the gut
(enterochromaffin cells) and is found in brain tissue. Those substances that stimulate insulin release
will also induce somatostatin secretion. It is an inhibitor of growth hormone, it also delays gastric
emptying and reduces gastrin secretion.
It reduces pancreatic exocrine secretions and may be used therapeutically to treat pancreatic
fistulae.

Somatostatinomas are rare pancreatic endocrine tumours and will result in the clinical
manifestations of diabetes mellitus, gallstones and steatorrhoea.
Next question

A 34 year old lady develops septic shock and features of the systemic inflammatory response syndrome as a complication of cholangitis. Which of the following is not a typical feature of this condition?
Body temperature less than 36oC or greater than 38oC
Respiratory rate >20
Lactate <4 mmol/L
High levels of tumour necrosis factor α
WCC >12,000 mm3
Septic shock will typically result in end organ hypoperfusion and as a result lactate levels will often be high. In the surviving sepsis campaign it is suggested that elevated lactate levels are an independent indicator for vasopressor support in patient with sepsis. The WCC may be paradoxically low in severe sepsis, although it is most often elevated. Please rate this question:
Discuss and give feedback
Next question
Shock
Shock occurs when there is insufficient tissue perfusion. The pathophysiology of shock is an important surgical topic and may be divided into the
following aetiological groups: Septic Haemorrhagic Neurogenic Cardiogenic
Anaphylactic
Septic shock
Septic shock is a major problem and those patients with severe sepsis have a mortality rate in excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ failure to 65% in those with 4 organ failure. Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response
Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90

beats/min, respiratory rate >20/min, WBC count >12,000/mm3 or < 4,000/mm3, altered mental state or hyperglycaemia (in absence of diabetes). Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis. Those with organ failure have severe sepsis and those with refractory hypotension -septic shock. During the septic process there is marked activation of the immune system with extensive cytokine
release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those ofexcessive inflammation, coagulation and fibrinolytic suppression. The surviving sepsis campaign (2012) highlights the following key areas for attention:
Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous search for the source of infection.
Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg.
Modulation of the septic response. This includes manoeuvres to counteract the changes and includes measures such as tight glycaemic control. The routine use of steroids is not advised.
In surgical patients, the main groups with septic shock include those with anastomotic leaks, abscesses and extensive superficial infections such as necrotising fasciitis. When performing surgery the aim should be to undertake the minimum necessary to restore physiology. These patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken when physiology is restored and clotting in particular has been normalised. Haemorrhagic shock The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly. The table below outlines the 4 major classes of haemorrhagic shock and their associated physiological sequelae:
Parameter Class I Class II Class III Class IV
Blood loss ml <750ml 750-1500ml 1500-2000ml >2000ml
Blood loss % <15% 15-30% 30-40% >40%
Pulse rate <100 >100 >120 >140

Parameter Class I Class II Class III Class IV
Blood pressure Normal Normal Decreased Decreased
Respiratory rate 14-20 20-30 30-40 >35
Urine output >30ml 20-30ml 5-15ml <5ml
Symptoms Normal Anxious Confused Lethargic
Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A, although you should understand the principle. In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the following may also be the cause or occur concomitantly:
Tension pneumothorax
Spinal cord injury Myocardial contusion Cardiac tamponade
When assessing trauma patients it is worth remembering that in order to generate a palpable femoral pulse an arterial pressure of >65mmHg is required. Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have such risk factors. Neurogenic shock This occurs most often following a spinal cord transection, usually at a high level. There is resultant interruption of the autonomic nervous system. The result is either decreased sympathetic
tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular resistance mediated by marked vasodilation. This results in decreased preload and thus decreased cardiac output (Starlings law). There is decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types of shock peripheral vasoconstrictors are used to return vascular tone to normal.

Cardiogenic shock In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct
myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but they are less useful in delineating the extent of myocardial trauma than following MI. When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the heart is the most likely site of injury with chamber and or valve rupture. These patients require surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may require intra aortic balloon pump as a bridge to surgery. Anaphylactic shock Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic hypersensitivity reaction. Anaphylaxis is one of the few times when you would not have time to look up the dose of a medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated. Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as follows:
Adrenaline Hydrocortisone Chlorpheniramine
< 6 months 150 mcg (0.15ml 1 in 1,000) 25 mg 250 mcg/kg
6 months - 6 years 150 mcg (0.15ml 1 in 1,000) 50 mg 2.5 mg
6-12 years 300 mcg (0.3ml 1 in 1,000) 100 mg 5 mg
Adult and child 12 years 500 mcg (0.5ml 1 in 1,000) 200 mg 10 mg
Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the anterolateral aspect of the middle third of the thigh. Common identified causes of anaphylaxis
food (e.g. Nuts) - the most common cause in children drugs venom (e.g. Wasp sting)
Next question

Which of the following stimulates gastric acid secretion?
Cholecystokinin
Gastric inhibitory peptide
Secretin
Histamine
Somatostatin
Gastrin: From G cells: stimulates gastric acid production
Pepsin: Digestion of protein, secretion occurs simultaneously with gastrin
Secretin: From mucosal cells in the duodenum and jejunum: inhibits gastric acid, stimulates bile and
pancreatic juice production
Gastric inhibitory peptide: (produced in response to fatty acids) inhibits gastrin release and acid
secretion from parietal cells
Cholecystokinin: From mucosal cells in the duodenum and jejunum (produced in response to fatty
acids) inhibits acid secretion from parietal cells, causes gallbladder contraction and relaxation of
sphincter of Oddi
Somatostatin: From D cells
Please rate this question:
Discuss and give feedback
Next question
Hormonal control of gastric acid secretion

Source Stimulus Actions
Gastrin G cells in
antrum of the
stomach
Distension of
stomach, extrinsic
nerves
Inhibited by: low
antral pH,
somatostatin
Increase HCL, pepsinogen and IF secretion,
increases gastric motility, trophic effect on gastric
mucosa
CCK I cells in upper
small intestine
Partially digested
proteins and
triglycerides
Increases secretion of enzyme-rich fluid from
pancreas, contraction of gallbladder and
relaxation of sphincter of Oddi, decreases gastric
emptying, trophic effect on pancreatic acinar
cells, induces satiety
Secretin S cells in
upper small
intestine
Acidic chyme, fatty
acids
Increases secretion of bicarbonate-rich fluid from
pancreas and hepatic duct cells, decreases gastric
acid secretion, trophic effect on pancreatic acinar
cells
VIP Small
intestine,
pancreas
Neural Stimulates secretion by pancreas and intestines,
inhibits acid and pepsinogen secretion
Somatostatin D cells in the
pancreas and
stomach
Fat, bile salts and
glucose in the
intestinal lumen
Decreases acid and pepsin secretion, decreases
gastrin secretion, decreases pancreatic enzyme
secretion, decreases insulin and glucagon
secretion
inhibits trophic effects of gastrin, stimulates
gastric mucous production
Next question

Which of the following statements relating to gastric acid secretions are untrue?
In parietal cells carbonic anhydrase generates hydrogen ions which are then actively
secreted
The cephalic phase is abolished following truncal vagotomy
The intestinal phase accounts for 60% of gastric acid produced
Histamine acts in a paracrine manner on H2 receptors
H2 receptor antagonists will not completely abolish gastric acid production
The intestinal phase of gastric acid secretion accounts for only 10% of gastric acid produced. Please rate this question:
Discuss and give feedback
Next question
Gastric secretions
A working knowledge of gastric secretions is important for surgery because peptic ulcers are common, surgeons frequently prescribe anti secretory drugs and because there are still patients around who will have undergone acid lowering procedures (Vagotomy) in the past. Gastric acid
Is produced by the parietal cells in the stomach pH of gastric acid is around 2 with acidity being maintained by the H+/K+ ATP ase pump. As
part of the process bicarbonate ions will be secreted into the surrounding vessels.
Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus. This sets up a negative potential across the membrane and as a result sodium and potassium ions diffuse across into the canaliculus.
Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and are secreted into the lumen of the oxyntic gland.
This is illustrated diagrammatically below:

Image sourced from Wikipedia
Phases of gastric acid secretion There are 3 phases of gastric secretion: 1. Cephalic phase (smell / taste of food)
30% acid produced Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells
2. Gastric phase (distension of stomach )
60% acid produced Stomach distension/low H+/peptides causes Gastrin release

3. Intestinal phase (food in duodenum)
10% acid produced High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion
via enterogastrones (CCK, secretin) and neural reflexes.
Regulation of gastric acid production Factors increasing production include:
Vagal nerve stimulation
Gastrin release Histamine release (indirectly following gastrin release) from enterchromaffin like cells
Factors decreasing production include:
Somatostatin (inhibits histamine release) Cholecystokinin Secretin
The diagram below illustrates some of the factors involved in regulating gastric acid secretion and the relevant associated pharmacology
Image sourced from Wikipedia
Below is a brief summary of the major hormones involved in food digestion:

Source Stimulus Actions
Gastrin G cells in
antrum of the stomach
Distension of
stomach, extrinsic
nerves
Inhibited by: low
antral pH,
somatostatin
Increase HCL, pepsinogen and IF secretion,
increases gastric motility, trophic effect on gastric mucosa
CCK I cells in
upper small
intestine
Partially digested
proteins and
triglycerides
Increases secretion of enzyme-rich fluid
from pancreas, contraction of gallbladder
and relaxation of sphincter of Oddi,
decreases gastric emptying, trophic effect on
pancreatic acinar cells, induces satiety
Secretin S cells in
upper small
intestine
Acidic chyme, fatty acids
Increases secretion of bicarbonate-rich fluid
from pancreas and hepatic duct cells,
decreases gastric acid secretion, trophic effect on pancreatic acinar cells
VIP Small
intestine,
pancreas
Neural Stimulates secretion by pancreas and
intestines, inhibits acid and pepsinogen
secretion
Somatostatin D cells in the
pancreas and
stomach
Fat, bile salts and
glucose in the
intestinal lumen
Decreases acid and pepsin secretion,
decreases gastrin secretion, decreases
pancreatic enzyme secretion, decreases
insulin and glucagon secretion
inhibits trophic effects of gastrin, stimulates gastric mucous production
Next question

A 22 year old man is undergoing a daycase excision of a sebaceous cyst. He is needle phobic and as the surgeon approaches with the needle the patient begins to hyperventilate. He soon develops circumoral parasthesia and muscular twitching. Which of the following is the most likely explanation for this event?
Temporal lobe epilepsy
Reduction in ionised calcium levels
Increase in ionised calcium levels
Fall in serum PTH levels
Rise in serum PTH levels
50% of plasma calcium is ionised. Hyperventilation will induce a state of alkalosis which will lower ionised plasma calcium levels. Please rate this question:
Discuss and give feedback
Next question
Calcium homeostasis
Calcium ions are linked to a wide range of physiological processes. The largest store of bodily calcium is contained within the skeleton. Calcium levels are primarily controlled by parathyroid hormone, vitamin D and calcitonin. Hormonal regulation of calcium
Hormone Actions
Parathyroid hormone (PTH) Increase calcium levels and decrease phosphate
levels
Increases bone resorption
Immediate action on osteoblasts to increase ca2+ in
extracellular fluid
Osteoblasts produce a protein signaling molecule
that activate osteoclasts which cause bone
resorption

Hormone Actions
Increases renal tubular reabsorption of calcium
Increases synthesis of 1,25(OH)2D (active form
of vitamin D) in the kidney which increases
bowel absorption of Ca2+
Decreases renal phosphate reabsorption
1,25-dihydroxycholecalciferol (the
active form of vitamin D)
Increases plasma calcium and plasma phosphate
Increases renal tubular reabsorption and gut
absorption of calcium
Increases osteoclastic activity
Increases renal phosphate reabsorption
Calcitonin Secreted by C cells of thyroid
Inhibits intestinal calcium absorption
Inhibits osteoclast activity
Inhibits renal tubular absorption of calcium
Both growth hormone and thyroxine also play a small role in calcium metabolism.
Next question

Which of the following inhibits gastric acid secretion?
Histamine
Nausea
Calcium
Parasympathetic vagal stimulation
Gastrin
Nausea inhibits gastric secretion via higher cerebral activity and sympathetic innervation. Please rate this question:
Discuss and give feedback
Next question
Gastric secretions
A working knowledge of gastric secretions is important for surgery because peptic ulcers are common, surgeons frequently prescribe anti secretory drugs and because there are still patients around who will have undergone acid lowering procedures (Vagotomy) in the past. Gastric acid
Is produced by the parietal cells in the stomach pH of gastric acid is around 2 with acidity being maintained by the H+/K+ ATP ase pump. As
part of the process bicarbonate ions will be secreted into the surrounding vessels.
Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus. This sets up a negative potential across the membrane and as a result sodium and potassium ions diffuse across into the canaliculus.
Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and are secreted into the lumen of the oxyntic gland.
This is illustrated diagrammatically below:

Image sourced from Wikipedia
Phases of gastric acid secretion There are 3 phases of gastric secretion: 1. Cephalic phase (smell / taste of food)
30% acid produced
Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells
2. Gastric phase (distension of stomach )
60% acid produced
Stomach distension/low H+/peptides causes Gastrin release
3. Intestinal phase (food in duodenum)

10% acid produced High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion
via enterogastrones (CCK, secretin) and neural reflexes.
Regulation of gastric acid production
Factors increasing production include:
Vagal nerve stimulation
Gastrin release Histamine release (indirectly following gastrin release) from enterchromaffin like cells
Factors decreasing production include:
Somatostatin (inhibits histamine release)
Cholecystokinin Secretin
The diagram below illustrates some of the factors involved in regulating gastric acid secretion and the relevant associated pharmacology
Image sourced from Wikipedia
Below is a brief summary of the major hormones involved in food digestion:
Source Stimulus Actions

Gastrin G cells in
antrum of the stomach
Distension of
stomach, extrinsic
nerves
Inhibited by: low
antral pH,
somatostatin
Increase HCL, pepsinogen and IF secretion,
increases gastric motility, trophic effect on gastric mucosa
CCK I cells in
upper small
intestine
Partially digested
proteins and
triglycerides
Increases secretion of enzyme-rich fluid
from pancreas, contraction of gallbladder
and relaxation of sphincter of Oddi,
decreases gastric emptying, trophic effect on
pancreatic acinar cells, induces satiety
Secretin S cells in
upper small
intestine
Acidic chyme, fatty acids
Increases secretion of bicarbonate-rich fluid
from pancreas and hepatic duct cells,
decreases gastric acid secretion, trophic effect on pancreatic acinar cells
VIP Small
intestine, pancreas
Neural Stimulates secretion by pancreas and
intestines, inhibits acid and pepsinogen secretion
Somatostatin D cells in the
pancreas and
stomach
Fat, bile salts and
glucose in the
intestinal lumen
Decreases acid and pepsin secretion,
decreases gastrin secretion, decreases
pancreatic enzyme secretion, decreases
insulin and glucagon secretion
inhibits trophic effects of gastrin, stimulates gastric mucous production
Next question

A 73 year old lady is diagnosed with hyperaldosteronism. From which of the following structures is
aldosterone released?
Zona fasciculata of the adrenal gland
Juxtaglomerular apparatus of the kidney
Zona reticularis of the adrenal gland
Adrenal medulla
Zona glomerulosa of the adrenal cortex
Aldosterone serves to conserve sodium and water. It is produced in the zona glomerulosa of the
adrenal cortex.
Please rate this question:
Discuss and give feedback
Next question
Aldosterone
Aldosterone is secreted by the zona glomerulosa of the adrenal cortex. It is a mineralocorticoid
hormone. Secretion is regulated by the renin- angiotensin system, and by plasma levels of sodium
and potassium. Aldosterone conserves sodium by stimulating the reabsorption of sodium in the
distal nephron in exchange for potassium. Lack of aldosterone release will result in hyperkalaemia
and hyponatraemia.
Next question

Which of the following hormonal agents will increase secretions of water and electrolytes in
pancreatic juice?
Secretin
Aldosterone
Somatostatin
Cholecystokinin
Adrenaline
Secretin causes secretion of water and electrolytes
Cholecystokinin causes enzyme secretion
While secretin will typically increase electrolyte and water volume of secretions, the enzyme content
in increased by cholecystokinin. Somatostatin will decrease the volume of secretions. Aldosterone
will tend to conserve electrolytes.
Please rate this question:
Discuss and give feedback
Next question
Pancreas exocrine physiology
Composition of pancreatic secretions
Pancreatic secretions are usually 1000-1500ml per 24 hours and have a pH of 8.
Secretion Source Substances secreted
Enzymic Acinar cells Trypsinogen

Procarboxylase
Amylase
Elastase
Aqueous Ductal and
Centroacinar cells
Sodium
Bicarbonate
Water
Potassium
Chloride
NB: Sodium and potassium reflect their plasma levels; chloride
and bicarbonate vary with flow rate
Regulation
The cephalic and gastric phases (neuronal and physical) are less important in regulating the
pancreatic secretions. The effect of digested material in the small bowel stimulates CCK release and
ACh which stimulate acinar and ductal cells. Of these CCK is the most potent stimulus. In the case
of the ductal cells these are potently stimulated by secretin which is released by the S cells of the
duodenum. This results in an increase in bicarbonate.
Enzyme activation
Trypsinogen is converted via enterokinase to active trypsin in the duodenum. Trypsin then activates
the other inactive enzymes
Next question

A 43 year old lady is admitted with cholestasis secondary to a stone impacted at the level of the
ampulla of vater. Which of the following tests is most likely to be predictive of bleeding diathesis at
the time of ERCP in this particular case?
Bleeding time
Prothrombin time
APTT
Platelet count
Factor I levels
PT: Vitamin K dependent factors 2, 7, 9, 10
APTT: Factors 8, 9, 11, 12
Jaundice will impair the production of vitamin K dependent clotting factors. This is most accurately
tested by measuring the prothrombin time. APTT can be affected by vitamin K deficiency (due to
factor 9 deficiency), however this occurs to a lesser extent and is normally associated with severe
liver disease. The bleeding time is a measure of platelet function.
Please rate this question:
Discuss and give feedback
Next question
Abnormal coagulation
Cause Factors affected

Cause Factors affected
Heparin Prevents activation factors 2,9,10,11
Warfarin Affects synthesis of factors 2,7,9,10
DIC Factors 1,2,5,8,11
Liver disease Factors 1,2,5,7,9,10,11
Interpretation blood clotting test results
Disorder APTT PT Bleeding time
Haemophilia Increased Normal Normal
von Willebrand's disease Increased Normal Increased
Vitamin K deficiency Increased Increased Normal
Next question

Which of the following mechanisms best accounts for the release of adrenaline?
Release from the adrenal medulla in response to increased angiotensin 1 levels
Release from the zona fasiculata from the adrenal gland in response to increased
sympathetic discharge
Release from the adrenal medulla in response to increased noradrenaline levels
Release from the adrenal medulla in response to sympathetic stimulation from the
splanchnic nerves
None of the above
The adrenal gland releases adrenaline in response to increased sympathetic discharge from preganglionic sympathetic fibres of the splanchnic nerves. These cause the chromafin cells of the medulla to release adrenaline (which is preformed) by exocytosis. Please rate this question:
Discuss and give feedback
Next question
Adrenaline
Fight or Flight response
- Catecholamine (phenylalanine and tyrosine) - Neurotransmitter and hormone - Released by the adrenal glands - Effects on α 1 and 2, β 1 and 2 receptors - Effect on β 2 receptors in skeletal muscle vessels-causing vasodilation - Increase cardiac output and total peripheral resistance - Vasoconstriction in the skin and kidneys causing a narrow pulse pressure Actions
α adrenergic receptors:
Inhibits insulin secretion by the pancreas
Stimulates glycogenolysis in the liver and muscle Stimulates glycolysis in muscle

β adrenergic receptors:
Stimulates glucagon secretion in the pancreas Stimulates ACTH
Stimulates lipolysis by adipose tissue
Next question

The acute phase response to injury does not include:
Pyrexia
Decreased albumin
Hepatic sequestration of cations
Increased transferrin
Increased serum amyloid A
The acute phase response includes:
Acute phase proteins Reduction of transport proteins (albumin, transferrin) Hepatic sequestration cations Pyrexia
Neutrophil leucocytosis Increased muscle proteolysis Changes in vascular permeability
Please rate this question:
Discuss and give feedback
Next question
Stress response: Endocrine and metabolic changes
Surgery precipitates hormonal and metabolic changes causing the stress response. Stress response is associated with: substrate mobilization, muscle protein loss, sodium and
water retention, suppression of anabolic hormone secretion, activation of the sympathetic nervous system, immunological and haematological changes.
The hypothalamic-pituitary axis and the sympathetic nervous systems are activated and there is a failure of the normal feedback mechanisms of control of hormone secretion.
A summary of the hormonal changes associated with the stress response:

Increased Decreased No Change
Growth hormone Insulin Thyroid stimulating hormone
Cortisol Testosterone Luteinizing hormone
Renin Oestrogen Follicle stimulating hormone
Adrenocorticotrophic hormone (ACTH)
Aldosterone
Prolactin
Antidiuretic hormone
Glucagon
Sympathetic nervous system
Stimulates catecholamine release Causes tachycardia and hypertension
Pituitary gland
ACTH and growth hormone (GH) is stimulated by hypothalamic releasing factors, corticotrophin releasing factor (CRF) and somatotrophin (or growth hormone releasing factor)
Perioperative increased prolactin secretion occurs by release of inhibitory control Secretion of thyroid stimulating hormone (TSH), luteinizing hormone (LH) and follicle
stimulating hormone (FSH) does not change significantly

ACTH stimulates cortisol production within a few minutes of the start of surgery. More ACTH is produced than needed to produce a maximum adrenocortical response.
Cortisol
Significant increases within 4-6 hours of surgery (>1000 nmol litre-1). The usual negative feedback mechanism fails and concentrations of ACTH and cortisol
remain persistently increased.
The magnitude and duration of the increase correlate with the severity of stress and the response is not abolished by the administration of corticosteroids.
The metabolic effects of cortisol are enhanced:
Skeletal muscle protein breakdown to provide gluconeogenic precursors and amino acids for protein synthesis in the liver Stimulation of lipolysis 'Anti-insulin effect' Mineralocorticoid effects Anti-inflammatory effects Growth hormone
Increased secretion after surgery has a minor role
Most important for preventing muscle protein breakdown and promote tissue repair by insulin growth factors
Alpha Endorphin
Increased
Antidiuretic hormone
An important vasopressor and enhances haemostasis
Renin is released causing the conversion of angiotensinogen to angiotensin I Angiotensin II formed by ACE on angiotensin 1, which causes the secretion of aldosterone
from the adrenal cortex. This increases sodium reabsorption at the distal convoluted tubule
Insulin
Release inhibited by stress

Occurs via the inhibition of the beta cells in the pancreas by the α2-adrenergic inhibitory effects of catecholamines
Insulin resistance by target cells occurs later
The perioperative period is characterized by a state of functional insulin deficiency
Thyroxine (T4) and tri-iodothyronine (T3)
Circulating concentrations are inversely correlated with sympathetic activity and after surgery there is a reduction in thyroid hormone production, which normalises over a few days.
Metabolic effect of endocrine response
Carbohydrate metabolism
Hyperglycaemia is a main feature of the metabolic response to surgery Due to increase in glucose production and a reduction in glucose utilization Catecholamines and cortisol promote glycogenolysis and gluconeogenesis
Initial failure of insulin secretion followed by insulin resistance affects the normal responses The proportion of the hyperglycaemic response reflects the severity of surgery Hyperglycaemia impairs wound healing and increase infection rates
Protein metabolism
Initially there is inhibition of protein anabolism, followed later, if the stress response is severe, by enhanced catabolism
The amount of protein degradation is influenced by the type of surgery and also by the nutritional status of the patient
Mainly skeletal muscle protein is affected The amino acids released form acute phase proteins (fibrinogen, C reactive protein,
complement proteins, a2-macroglobulin, amyloid A and ceruloplasmin) and are used for gluconeogenesis
Nutritional support has little effect on preventing catabolism
Lipid metabolism Increased catecholamine, cortisol and glucagon secretion, and insulin deficiency, promotes lipolysis and ketone body production. Salt and water metabolism
ADH causes water retention, concentrated urine, and potassium loss and may continue for 3 to 5 days after surgery
Renin causes sodium and water retention

Cytokines
Glycoproteins Interleukins (IL) 1 to 17, interferons, and tumour necrosis factor
Synthesized by activated macrophages, fibroblasts, endothelial and glial cells in response to tissue injury from surgery or trauma
IL-6 main cytokine associated with surgery. Peak 12 to 24 h after surgery and increase by the degree of tissue damage Other effects of cytokines include fever, granulocytosis, haemostasis, tissue damage limitation and promotion of healing.
Modifying the response
Opioids suppress hypothalamic and pituitary hormone secretion
At high doses the hormonal response to pelvic and abdominal surgery is abolished. However, such doses prolong recovery and increase the need for postoperative ventilatory support
Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH and epinephrine changes, although cytokine responses are unaltered
Cytokine release is reduced in less invasive surgery Nutrition prevents the adverse effects of the stress response. Enteral feeding improves
recovery
Growth hormone and anabolic steroids may improve outcome Normothermia decreases the metabolic response
References Deborah Burton, Grainne Nicholson, and George Hall Endocrine and metabolic response to surgery . Contin Educ Anaesth Crit Care Pain (2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040
Next question

Which of the following statements relating to blood transfusions in surgical patients is false?
Packed red cells typically have a haematocrit of between 55 and 75%
Clotting factor activity in whole blood decreases in samples stored for longer than 7 days
After 3 weeks of storage blood has a pH of 6.9
Gamma irradiated blood products are not required routinely
Patients should be transfused to achieve a target haemoglobin of 10 g/dl and a haematocrit
of 30%
Patients can generally be managed without transfusion as long as the Hb is 7 or greater. The exact level depends upon patient factors such as co-morbidities. Old blood functions less effectively and should not be used during massive transfusions. Please rate this question:
Discuss and give feedback
Next question
Blood products
Whole blood fractions
Fraction Key points
Packed red cells Used for transfusion in chronic anaemia and cases where infusion of large
volumes of fluid may result in cardiovascular compromise. Product obtained by centrifugation of whole blood.
Platelet rich
plasma
Usually administered to patients who are thrombocytopaenic and are bleeding
or require surgery. It is obtained by low speed centrifugation.
Platelet Prepared by high speed centrifugation and administered to patients with

concentrate thrombocytopaenia.
Fresh frozen
plasma
Prepared from single units of blood.
Contains clotting factors, albumin and immunoglobulin.
Unit is usually 200 to 250ml.
Usually used in correcting clotting deficiencies in patients with hepatic
synthetic failure who are due to undergo surgery.
Usual dose is 12-15ml/Kg-1.
It should not be used as first line therapy for hypovolaemia.
Cryoprecipitate Formed from supernatant of FFP.
Rich source of Factor VIII and fibrinogen.
Allows large concentration of factor VIII to be administered in small
volume.
SAG-Mannitol
Blood
Removal of all plasma from a blood unit and substitution with:
Sodium chloride
Adenine
Anhydrous glucose
Mannitol
Up to 4 units of SAG M Blood may be administered. Thereafter whole blood
is preferred. After 8 units, clotting factors and platelets should be considered.
Cell saver devices These collect patients own blood lost during surgery and then re-infuse it. There are two main types:
Those which wash the blood cells prior to re-infusion. These are more expensive to purchase and more complicated to operate. However, they reduce the risk of re-infusing contaminated blood back into the patient.
Those which do not wash the blood prior to re-infusion.
Their main advantage is that they avoid the use of infusion of blood from donors into patients and this may reduce risk of blood borne infection. It may be acceptable to Jehovah's witnesses. It is contraindicated in malignant disease for risk of facilitating disease dissemination. Blood products used in warfarin reversal
In some surgical patients the use of warfarin can pose specific problems and may require the use of specialised blood products Immediate or urgent surgery in patients taking warfarin(1) (2):

1. Stop warfarin 2. Vitamin K (reversal within 4-24 hours) -IV takes 4-6h to work (at least 5mg) -Oral can take 24 hours to be clinically effective 3. Fresh frozen plasma Used less commonly now as 1st line warfarin reversal -30ml/kg-1 -Need to give at least 1L fluid in 70kg person (therefore not appropriate in fluid overload) -Need blood group -Only use if human prothrombin complex is not available 4. Human Prothrombin Complex (reversal within 1 hour) -Bereplex 50 u/kg -Rapid action but factor 6 short half life, therefore give with vitamin K References
1. Dentali, F., C. Marchesi, et al. (2011). "Safety of prothrombin complex concentrates for rapid anticoagulation reversal of vitamin K antagonists. A meta-analysis." Thromb Haemost 106(3): 429-438. 2. http://www.transfusionguidelines.org/docs/pdfs/bbt-03warfarin-reversal-flowchart-2006.pdf
Next question

Which of the following statements relating the fluid physiology of a physiologically normal 70 Kg
adult male is false?
He will have more water per unit of body weight than a female of similar weight
Plasma will comprise 25% of his body weight
Interstitial fluid will account for up to 24% of body weight
Approximately 65% of total body water is intracellular
60% of his body weight is composed of water
The 60-40-20 rule:
60% total body weight is water
40% of total body weight is intracellular fluids
20% of body weight is extracellular fluids
Plasma typically accounts for 4-6% of body weight in healthy individuals.
Males typically have more water per unit weight than females, as females have a higher fat content.
Please rate this question:
Discuss and give feedback
Next question
Fluid compartment physiology
Body fluid compartments comprise intracellular and extracellular compartments. The latter includes
interstitial fluid, plasma and transcellular fluid.
Typical figures are based on the 70 Kg male.
Body fluid volumes

Compartment Volume in litres Percentage of total volume
Intracellular 28 L 60-65%
Extracellular 14 L 35-40%
Plasma 3 L 5%
Interstitial 10 L 24%
Transcellular 1 L 3%
Figures are approximate
Next question

A 17 year old lady with long standing anorexia nervosa is due to undergo excision of a lipoma. Which of the following nutritional deficiencies is most likely to be implicated in poor collagen formation as the wound heals?
Deficiency of copper
Deficiency of iron
Deficiency of ascorbic acid
Deficiency of phosphate
None of the above
Theme from January 2011 Vitamin C is involved in the cross linkage of collagen and impaired wound healing is well described in cases of vitamin C deficiency. Please rate this question:
Discuss and give feedback
Next question
Collagen
Collagen is one of the most important structural proteins within the extracellular matrix, collagen together with components such as elastin and glycosaminoglycans determine the properties of all tissues.
Composed of 3 polypeptide strands that are woven into a helix, usually a combination of glycine with either proline or hydroxyproline plus another amino acid
Numerous hydrogen bonds exist within molecule to provide additional strength Many sub types but commonest sub type is I (90% of bodily collagen), tissues with increased
levels of flexibility have increased levels of type III collagen Vitamin c is important in establishing cross links Synthesised by fibroblasts
Collagen Diseases Disorders of collagen range from relatively common, acquired defects (typically aging), through to rarer congenital disorders. The latter are exemplified by conditions such as osteogenesis imperfecta

and Ehlers Danlos syndromes. Osteogenesis imperfecta: -8 Subtypes -Defect of type I collagen -In type I the collagen is normal quality but insufficient quantity -Type II- poor quantity and quality -Type III- Collagen poorly formed, normal quantity -Type IV- Sufficient quantity but poor quality Patients have bones which fracture easily, loose joint and multiple other defects depending upon which sub type they suffer from. Ehlers Danlos: -Multiple sub types -Abnormality of types 1 and 3 collagen -Patients have features of hypermobility. -Individuals are prone to joint dislocations and pelvic organ prolapse. In addition to many other diseases related to connective tissue defects.
Next question

A 45 year old man is undergoing a small bowel resection. The anaesthetist decides to administer an
intravenous fluid which is electrolyte rich. Which of the following most closely matches this
requirement?
Dextrose / Saline
Pentastarch
Gelofusine
Hartmans
5% Dextrose with added potassium 20mmol/ L
Theme from April 2012 Exam
Hartmans solution is the most electrolyte rich. However, both pentastarch and gelofusine have more
macromolecules.
Please rate this question:
Discuss and give feedback
Next question
Intra operative fluid management
Composition of commonly used intravenous fluids mmol-1
Na K Cl Bicarbonate Lactate
Plasma 137-147 4-5.5 95-105 22-25 -

0.9% Saline 153 - 153 - -
Dextrose / saline 30.6 - 30.6 - -
Hartmans 130 4 110 - 28
Recommendations for intra operative fluid management
The latest set of NICE guidelines produced in 2013 relating to intravenous fluids did not specifically
address the requirements of intra operative fluid administration. The reason for this is that
administration of fluids in this specific situation does not lend itself to rigid algorithms.
With the introduction of enhanced recovery programmes 10 years ago there was an increasing
emphasis of the concept of fluid restriction. Historically, patients received very large volumes of
saline rich solutions peri-operatively. Clearing the sodium load of a single litre of saline may take up
to 36 hours or more. This can have deleterious effects on the tissues including the development of
oedema. This results in poor perfusion, increased risk of ileus and wound breakdown. A tailored
approach to fluid administration is now practiced and far greater usage is made of cardiac output
monitors in providing goal directed fluid therapy.
References
British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients
GIFTASUP (2009) Revised May 2011.
Frost P. Intravenous fluid therapy in adult inpatients. BMJ 2015 (350): 31-34.
Next question

A 16 year old girl develops pyelonephritis and is admitted in a state of septic shock. Which of the following is not typically seen in this condition?
Increased cardiac output
Increased systemic vascular resistance
Oliguria may occur
Systemic cytokine release
Tachycardia
Cardiogenic Shock: e.g. MI, valve abnormality increased SVR (vasoconstriction in response to low BP) increased HR (sympathetic response) decreased cardiac output decreased blood pressure Hypovolaemic shock: blood volume depletion e.g. haemorrhage, vomiting, diarrhoea, dehydration, third-space losses during major operations increased SVR increased HR decreased cardiac output decreased blood pressure Septic shock: occurs when the peripheral vascular dilatation causes a fall in SVR similar response may occur in anaphylactic shock, neurogenic shock reduced SVR increased HR normal/increased cardiac output decreased blood pressure
Theme from January 2012 Exam The SVR is reduced in sepsis and for this reason a vasopressor such as noradrenaline may be used if hypotension and oliguria remain a concern despite administration of adequate amounts of intravenous fluids. Please rate this question:

Discuss and give feedback
Next question
Shock
Shock occurs when there is insufficient tissue perfusion.
The pathophysiology of shock is an important surgical topic and may be divided into the following aetiological groups:
Septic Haemorrhagic Neurogenic
Cardiogenic Anaphylactic
Septic shock Septic shock is a major problem and those patients with severe sepsis have a mortality rate in excess of 40%. In those who are admitted to intensive care mortality ranges from 6% with no organ failure to 65% in those with 4 organ failure. Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response
Syndrome (SIRS). This is characterised by body temperature outside 36 oC - 38 o C, HR >90
beats/min, respiratory rate >20/min, WBC count >12,000/mm3 or < 4,000/mm3, altered mental state or hyperglycaemia (in absence of diabetes). Patients with infections and two or more elements of SIRS meet the diagnostic criteria for sepsis. Those with organ failure have severe sepsis and those with refractory hypotension -septic shock. During the septic process there is marked activation of the immune system with extensive cytokine
release. This may be coupled with or triggered by systemic circulation of bacterial toxins. These all cause endothelial cell damage and neutrophil adhesion. The overall hallmarks are thus those ofexcessive inflammation, coagulation and fibrinolytic suppression.
The surviving sepsis campaign (2012) highlights the following key areas for attention:
Prompt administration of antibiotics to cover all likely pathogens coupled with a rigorous search for the source of infection.
Haemodynamic stabilisation. Many patients are hypovolaemic and require aggressive fluid administration. Aim for CVP 8-12 cm H2O, MAP >65mmHg.
Modulation of the septic response. This includes manoeuvres to counteract the changes and includes measures such as tight glycaemic control. The routine use of steroids is not advised.
In surgical patients, the main groups with septic shock include those with anastomotic leaks, abscesses and extensive superficial infections such as necrotising fasciitis. When performing surgery the aim should be to undertake the minimum necessary to restore physiology. These patients do not fare well with prolonged surgery. Definitive surgery can be more safely undertaken

when physiology is restored and clotting in particular has been normalised. Haemorrhagic shock The average adult blood volume comprises 7% of body weight. Thus in the 70 Kg adult this will equate to 5 litres. This changes in children (8-9% body weight) and is slightly lower in the elderly. The table below outlines the 4 major classes of haemorrhagic shock and their associated physiological sequelae:
Parameter Class I Class II Class III Class IV
Blood loss ml <750ml 750-1500ml 1500-2000ml >2000ml
Blood loss % <15% 15-30% 30-40% >40%
Pulse rate <100 >100 >120 >140
Blood pressure Normal Normal Decreased Decreased
Respiratory rate 14-20 20-30 30-40 >35
Urine output >30ml 20-30ml 5-15ml <5ml
Symptoms Normal Anxious Confused Lethargic
Decreasing blood pressure during haemorrhagic shock causes organ hypoperfusion and relative myocardial ischaemia. The cardiac index gives a numerical value for tissue oxygen delivery and is given by the equation: Cardiac index= Cardiac output/ body surface area. Where Hb is haemoglobin concentration in blood and SaO2 the saturation and PaO2 the partial pressure of oxygen. Detailed knowledge of this equation is required for the MRCS Viva but not for part A, although you should understand the principle. In patients suffering from trauma the most likely cause of shock is haemorrhage. However, the following may also be the cause or occur concomitantly:
Tension pneumothorax Spinal cord injury

Myocardial contusion Cardiac tamponade
When assessing trauma patients it is worth remembering that in order to generate a palpable femoral pulse an arterial pressure of >65mmHg is required. Once bleeding is controlled and circulating volume normalised the levels of transfusion should be to maintain a Hb of 7-8 in those with no risk factors for tissue hypoxia and Hb 10 for those who have such risk factors. Neurogenic shock This occurs most often following a spinal cord transection, usually at a high level. There is resultant interruption of the autonomic nervous system. The result is either decreased sympathetic
tone or increased parasympathetic tone, the effect of which is a decrease in peripheral vascular resistance mediated by marked vasodilation. This results in decreased preload and thus decreased cardiac output (Starlings law). There is decreased peripheral tissue perfusion and shock is thus produced. In contrast with many other types of shock peripheral vasoconstrictors are used to return vascular tone to normal. Cardiogenic shock In medical patients the main cause is ischaemic heart disease. In the traumatic setting direct myocardial trauma or contusion is more likely. Evidence of ECG changes and overlying sternal fractures or contusions should raise the suspicion of injury. Treatment is largely supportive and transthoracic echocardiography should be used to determine evidence of pericardial fluid or direct myocardial injury. The measurement of troponin levels in trauma patients may be undertaken but they are less useful in delineating the extent of myocardial trauma than following MI. When cardiac injury is of a blunt nature and is associated with cardiogenic shock the right side of the heart is the most likely site of injury with chamber and or valve rupture. These patients require surgery to repair these defects and will require cardiopulmonary bypass to achieve this. Some may require intra aortic balloon pump as a bridge to surgery. Anaphylactic shock
Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic hypersensitivity reaction. Anaphylaxis is one of the few times when you would not have time to look up the dose of a medication. The Resuscitation Council guidelines on anaphylaxis have recently been updated. Adrenaline is by far the most important drug in anaphylaxis and should be given as soon as possible. The recommended doses for adrenaline, hydrocortisone and chlorpheniramine are as follows:
Adrenaline Hydrocortisone Chlorpheniramine
< 6 months 150 mcg (0.15ml 1 in 1,000) 25 mg 250 mcg/kg

6 months - 6 years 150 mcg (0.15ml 1 in 1,000) 50 mg 2.5 mg
6-12 years 300 mcg (0.3ml 1 in 1,000) 100 mg 5 mg
Adult and child 12 years 500 mcg (0.5ml 1 in 1,000) 200 mg 10 mg
Adrenaline can be repeated every 5 minutes if necessary. The best site for IM injection is the anterolateral aspect of the middle third of the thigh. Common identified causes of anaphylaxis
food (e.g. Nuts) - the most common cause in children
drugs venom (e.g. Wasp sting)
Next question

Which of the following statements are not typically true in hypokalaemia?
It may occur as a result of mechanical bowel preparation
Chronic vomiting may increase renal potassium losses
It may be associated with aciduria
It may cause hyponatraemia
It often accompanies acidosis
Potassium depletion occurs either through the gastrointestinal tract or the kidney. Chronic vomiting in itself is less prone to induce potassium loss than diarrhoea as gastric secretions contain less potassium than those in the lower GI tract. If vomiting produces a metabolic alkalosis then renal potassium wasting may occur as potassium is excreted in preference to hydrogen ions. The converse may occur in potassium depletion resulting in acid urine. Hypokalemia is very commonly associated with metabolic alkalosis. This is due to 2 factors: 1) the common causes of metabolic alkalosis (vomiting, diuretics) directly induce H+ and K loss (via aldosterone) and thus also cause hypokalemia and 2) hypokalemia is a very important cause of metabolic alkalosis by three mechanisms. The initial effect is by causing a transcellular shift in which K leaves and H+ enters the cells, thereby raising the extracellular pH. The second effect is by causing a transcellular shift in the cells of the proximal tubules resulting in an intracellular acidosis, which promotes ammonium production and excretion. Thirdly, in the presence of hypokalemia, hydrogen secretion in the proximal and distal tubules increases. This leads to further reabsorption of HCO3-. The net effect is an increase in the net acid excretion. Please rate this question:
Discuss and give feedback
Next question
Hypokalaemia
Potassium and hydrogen can be thought of as competitors. Hyperkalaemia tends to be associated with acidosis because as potassium levels rise fewer hydrogen ions can enter the cells Hypokalaemia with alkalosis
Vomiting Diuretics

Cushing's syndrome Conn's syndrome (primary hyperaldosteronism)
Hypokalaemia with acidosis
Diarrhoea Renal tubular acidosis Acetazolamide Partially treated diabetic ketoacidosis
Next question

A man is admitted after a period of prolonged self, induced starvation. Naso gastric feeding is planned. Which of the following is least likely to occur?
Hypokalaemia
Increased risk of cardiac arrhythmias
His haemoglobin will have decreased affinity for oxygen
Hypophosphataemia
Hypoalbuminaemia
The process of starvation may lower DPG levels, in practice this is unlikely to occur early as it is generated during glycolysis. Altered metabolism in starvation may be more acidotic and this would also tend to impair oxygen carriage. Please rate this question:
Discuss and give feedback
Next question
Nutrition - Refeeding syndrome
Refeeding syndrome describes the metabolic abnormalities which occur on feeding a person following a period of starvation. The metabolic consequences include:
Hypophosphataemia Hypokalaemia Hypomagnesaemia Abnormal fluid balance
These abnormalities can lead to organ failure. Re-feeding problems If patient not eaten for > 5 days, aim to re-feed at < 50% energy and protein levels High risk for re-feeding problems
If one or more of the following:
BMI < 16 kg/m2

Unintentional weight loss >15% over 3-6 months Little nutritional intake > 10 days Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to feeding (unless high)
If two or more of the following:
BMI < 18.5 kg/m2 Unintentional weight loss > 10% over 3-6 months Little nutritional intake > 5 days
History of: alcohol abuse, drug therapy including insulin, chemotherapy, diuretics and antacids
Prescription
Start at up to 10 kcal/kg/day increasing to full needs over 4-7 days Start immediately before and during feeding: oral thiamine 200-300mg/day, vitamin B co
strong 1 tds and supplements
Give K+ (2-4 mmol/kg/day), phosphate (0.3-0.6 mmol/kg/day), magnesium (0.2-0.4 mmol/kg/day)
Next question
v

Where does spironolactone act in the kidney?
Glomerulus
Proximal convoluted tubule
Descending limb of the loop of Henle
Ascending limb of the loop of Henle
Distal convoluted tubule
Please rate this question:
Discuss and give feedback
Next question
Potassium sparing diuretics
Potassium-sparing diuretics may be divided into the epithelial sodium channel blockers (amiloride and triamterene) and aldosterone antagonists (spironolactone and eplerenone). {Amiloride} is a weak diuretic which blocks the epithelial sodium channel in the distal convoluted tubule. Usually given with thiazides or loop diuretics as an alternative to potassium supplementation. {Spironolactone} is an aldosterone antagonist which acts act in the distal convoluted tubule. Indications
ascites: patients with cirrhosis develop a secondary hyperaldosteronism. Relatively large doses such as 100 or 200mg are often used
heart failure nephrotic syndrome Conn's syndrome
Next question

Which receptor does noradrenaline mainly bind to?
α 1 receptors
α 2 receptors
β 1 receptors
β 2 receptors
G receptors
Theme from September 2015 Exam
Noradrenaline is the precursor of adrenaline. It is a powerful α 1 stimulant (although it will increase
myocardial contractility). Infusions will produce vasoconstriction and an increase in total peripheral
resistance. It is the inotrope of choice in septic shock.
Please rate this question:
Discuss and give feedback
Next question
Inotropes and cardiovascular receptors
Inotropes are a class of drugs which work primarily by increasing cardiac output. They should be
distinguished from vasoconstrictor drugs which are used specifically when the primary problem is
peripheral vasodilatation.
Catecholamine type agents are commonly used and work by increasing cAMP levels by adenylate
cyclase stimulation. This in turn intracellular calcium ion mobilisation and thus the force of
contraction. Adrenaline works as a beta adrenergic receptor agonist at lower doses and an alpha
receptor agonist at higher doses. Dopamine causes dopamine receptor mediated renal and
mesenteric vascular dilatation and beta 1 receptor agonism at higher doses. This results in
increased cardiac output. Since both heart rate and blood pressure are raised, there is less overall

myocardial ischaemia. Dobutamine is a predominantly beta 1 receptor agonist with weak beta 2 and
alpha receptor agonist properties. Noradrenaline is a catecholamine type agent and predominantly
acts as an alpha receptor agonist and serves as a peripheral vasoconstrictor.
Phosphodiesterase inhibitors such as milrinone act specifically on the cardiac phosphodiesterase
and increase cardiac output.
Inotrope Cardiovascular receptor action
Adrenaline α-1, α-2, β-1, β-2
Noradrenaline α-1,( α-2), (β-1), (β-2)
Dobutamine β-1, (β 2)
Dopamine (α-1), (α-2), (β-1), D-1,D-2
Minor receptor effects in brackets
Effects of receptor binding
α-1, α-2 vasoconstriction
β-1 increased cardiac contractility and HR
β-2 vasodilatation
D-1 renal and spleen vasodilatation
D-2 inhibits release of noradrenaline
Next question

Adult lung volumes. Which statement is false?
In restrictive lung disease the FEV1/FVC ratio is increased
Residual volume is increased in emphysema
Functional residual capacity is measured by helium dilution test
The tidal volume is approximately 340mls in females
The vital capacity is increased in Guillain Barre syndrome
FEV1/FVC is normal or >80% in restrictive lung disease such as pulmonary fibrosis. The ratio is reduced in obstructive airways disease. The functional residual capacity, residual volume and the total lung capacity cannot be measured with spirometry. They can only be measured by helium dilution. The vital capacity is reduced in: 1. Pulmonary fibrosis/infiltration/oedema/effusions 2. Weak respiratory muscles e.g. MG, GBS, myopathies 3. Skeletal abnormalities e.g. chest wall abnormalities Please rate this question:
Discuss and give feedback
Next question
Lung volumes
The diagram demonstrates lung volumes and capacities

Image sourced from Wikipedia
Definitions
Tidal volume (TV) Is the volume of air inspired and expired during each
ventilatory cycle at rest.
It is normally 500mls in males and 340mls in females.
Inspiratory reserve
volume (IRV)
Is the maximum volume of air that can be forcibly inhaled
following a normal inspiration. 3000mls.
Expiratory reserve
volume (ERV)
Is the maximum volume of air that can be forcibly exhaled
following a normal expiration. 1000mls.
Residual volume (RV) Is that volume of air remaining in the lungs after a maximal
expiration.
RV = FRC - ERV. 1500mls.
Functional residual
capacity (FRC)
Is the volume of air remaining in the lungs at the end of a
normal expiration.
FRC = RV + ERV. 2500mls.
Vital capacity (VC) Is the maximal volume of air that can be forcibly exhaled after
a maximal inspiration.
VC = TV + IRV + ERV. 4500mls in males, 3500mls in
females.

Total lung capacity
(TLC)
Is the volume of air in the lungs at the end of a maximal
inspiration.
TLC = FRC + TV + IRV = VC + RV. 5500-6000mls.
Forced vital capacity
(FVC)
The volume of air that can be maximally forcefully exhaled.
Next question

A 47 year old lady is diagnosed as suffering from a phaeochromocytoma. From which of the
following amino acids are catecholamines primarily derived?
Aspartime
Glutamine
Arginine
Tyrosine
Alanine
Catecholamine hormones are derived from tyrosine, it is modified by a DOPA decarboxylase
enzyme to become dopamine and thereafter via two further enzymic modifications to noradrenaline
and finally adrenaline.
Please rate this question:
Discuss and give feedback
Next question
Adrenal physiology
Adrenal medulla
The chromaffin cells of the adrenal medulla secrete the catecholamines noradrenaline and
adrenaline. The medulla is innervated by the splanchnic nerves; the preganglionic sympathetic fibres
secrete acetylcholine causing the chromaffin cells to secrete their contents by exocytosis.
Phaeochromocytomas are derived from these cells and will secrete both adrenaline and nor
adrenaline.
Adrenal cortex
Three histologically distinct zones are recognised:

Zone Location Hormone Secreted
Zona glomerulosa Outer zone Aldosterone
Zona fasiculata Middle zone Glucocorticoids
Zona reticularis Inner zone Androgens
The glucocorticoids and aldosterone are mostly bound to plasma proteins in the circulation.
Glucocorticoids are inactivated and excreted by the liver.
Next question

Theme: Events in wound healing
A. Platelets
B. Neutrophil polymorphs
C. Endothelial cells
D. Lymphocytes
E. Myofibroblasts
F. Granulomas Please select the dominant cell type present in a wound at the specified timeframe. Each option may be used once, more than once or not at all.
132. 10 weeks following injury
You answered Platelets
The correct answer is Myofibroblasts
These differentiated cell types facilitate wound contraction.
133. 25 seconds following injury
You answered Neutrophil polymorphs
The correct answer is Platelets
Platelet degranulation and haemostasis are some of the earliest events in wound healing.
134. 7 days following injury
You answered Neutrophil polymorphs
The correct answer is Endothelial cells
Angiogenesis which is characterised by endothelial cell proliferation and microvessel
formation is a key step in successful wound healing. It is maximal between 1 and 2 weeks
following injury and wounds may have a reddish appearance during this time.
Please rate this question:
Discuss and give feedback
Next question

Phases of wound healing
Phase Key features Cells Timeframe
Haemostasis Vasospasm in adjacent vessels
Platelet plug formation and
generation of fibrin rich clot
Erythrocytes and
platelets
Seconds/
Minutes
Inflammation Neutrophils migrate into wound
(function impaired in diabetes).
Growth factors released, including
basic fibroblast growth factor and
vascular endothelial growth factor.
Fibroblasts replicate within the
adjacent matrix and migrate into
wound.
Macrophages and fibroblasts
couple matrix regeneration and clot
substitution.
Neutrophils,
fibroblasts and
macrophages
Days
Regeneration Platelet derived growth factor and
transformation growth factors
stimulate fibroblasts and epithelial
cells.
Fibroblasts produce a collagen
network.
Angiogenesis occurs and wound
resembles granulation tissue.
Fibroblasts,
endothelial cells,
macrophages
Weeks
Remodelling Longest phase of the healing
process and may last up to one year
(or longer).
During this phase fibroblasts
become differentiated
(myofibroblasts) and these
facilitate wound contraction.
Collagen fibres are remodelled.
Microvessels regress leaving a pale
scar.
Myofibroblasts 6 weeks to 1
year
Next question

Where are the arterial baroreceptors located?
Carotid sinus and aortic arch
Carotid sinus only
Superior vena cava
External carotid artery
None of the above
Theme from September 2015 Exam They lie in the carotid sinus and aortic arch. Please rate this question:
Discuss and give feedback
Next question
Cardiac physiology
The heart has four chambers ejecting blood into both low pressure and high pressure systems.
The pumps generate pressures of between 0-25mmHg on the right side and 0-120 mmHg on the left.
At rest diastole comprises 2/3 of the cardiac cycle. The product of the frequency of heart rate and stroke volume combine to give the cardiac
output which is typically 5-6L per minute.
Detailed descriptions of the various waveforms are often not a feature of MRCS A (although they are on the syllabus). However, they are a very popular topic for surgical physiology in the MRCS B exam. Electrical properties
Intrinsic myogenic rhythm within cardiac myocytes means that even the denervated heart is capable of contraction.
In the normal situation the cardiac impulse is generated in the sino atrial node in the right atrium and conveyed to the ventricles via the atrioventricular node.

The sino atrial node is also capable of spontaneous discharge and in the absence of background vagal tone will typically discharge around 100x per minute. Hence the higher resting heart rate found in cardiac transplant cases. In the SA and AV nodes the resting membrane potential is lower than in surrounding cardiac cells and will slowly depolarise from -70mV to around -50mV at which point an action potential is generated.
Differences in the depolarisation slopes between SA and AV nodes help to explain why the SA node will depolarise first. The cells have a refractory period during which they cannot be re-stimulated and this period allows for adequate ventricular filling. In pathological tachycardic states this time period is overridden and inadequate ventricular filling may then occur, cardiac output falls and syncope may ensue.
Parasympathetic fibres project to the heart via the vagus and will release acetylcholine. Sympathetic fibres release nor adrenaline and circulating adrenaline comes from the adrenal medulla. Noradrenaline binds to β 1 receptors in the SA node and increases the rate of pacemaker potential depolarisation. Cardiac cycle
Image sourced from Wikipedia
Mid diastole: AV valves open. Ventricles hold 80% of final volume. Outflow valves shut. Aortic pressure is high.
Late diastole: Atria contract. Ventricles receive 20% to complete filling. Typical end diastolic
volume 130-160ml.

Early systole: AV valves shut. Ventricular pressure rises. Isovolumetric ventricular contraction. AV Valves bulge into atria (c-wave). Aortic and pulmonary pressure exceeded- blood is ejected. Shortening of ventricles pulls atria downwards and drops intra atrial pressure (x-descent).
Late systole: Ventricular muscles relax and ventricular pressures drop. Although ventricular pressure drops the aortic pressure remains constant owing to peripheral vascular resistance and elastic property of the aorta. Brief period of retrograde flow that occurs in aortic recoil shuts the aortic valve. Ventricles will contain 60ml end systolic volume. The average stroke volume is 70ml (i.e. Volume ejected).
Early diastole: All valves are closed. Isovolumetric ventricular relaxation occurs. Pressure wave associated with closure of the aortic valve increases aortic pressure. The pressure dip before this rise can be seen on arterial waveforms and is called the incisura. During systole the atrial pressure increases such that it is now above zero (v- wave). Eventually atrial pressure exceed ventricular pressure and AV valves open - atria empty passively into ventricles and atrial pressure falls (y -descent )
The negative atrial pressures are of clinical importance as they can allow air embolization to occur if the neck veins are exposed to air. This patient positioning is important in head and neck surgery to avoid this occurrence if veins are inadvertently cut, or during CVP line insertion. Mechanical properties
Preload = end diastolic volume
Afterload = aortic pressure
It is important to understand the principles of Laplace's law in surgery.
It states that for hollow organs with a circular cross section, the total circumferential wall tension depends upon the circumference of the wall, multiplied by the thickness of the wall and on the wall tension.
The total luminal pressure depends upon the cross sectional area of the lumen and the transmural pressure. Transmural pressure is the internal pressure minus external pressure and at equilibrium the total pressure must counterbalance each other.
In terms of cardiac physiology the law explains that the rise in ventricular pressure that occurs during the ejection phase is due to physical change in heart size. It also explains why a dilated diseased heart will have impaired systolic function.

Starlings law
Increase in end diastolic volume will produce larger stroke volume. This occurs up to a point beyond which cardiac fibres are excessively stretched and stroke
volume will fall once more. It is important for the regulation of cardiac output in cardiac transplant patients who need to increase their cardiac output.
Baroreceptor reflexes
Baroreceptors located in aortic arch and carotid sinus.
Aortic baroreceptor impulses travel via the vagus and from the carotid via the glossopharyngeal nerve.
They are stimulated by arterial stretch.
Even at normal blood pressures they are tonically active. Increase in baroreceptor discharge causes:
*Increased parasympathetic discharge to the SA node. *Decreased sympathetic discharge to ventricular muscle causing decreased contractility and fall in stroke volume. *Decreased sympathetic discharge to venous system causing increased compliance. *Decreased peripheral arterial vascular resistance Atrial stretch receptors
Located in atria at junction between pulmonary veins and vena cava.
Stimulated by atrial stretch and are thus low pressure sensors. Increased blood volume will cause increased parasympathetic activity. Very rapid infusion of blood will result in increase in heart rate mediated via atrial receptors:
theBainbridge reflex.
Decreases in receptor stimulation results in increased sympathetic activity this will decrease renal blood flow-decreases GFR-decreases urinary sodium excretion-renin secretion by juxtaglomerular apparatus-Increase in angiotensin II.
Increased atrial stretch will also result in increased release of atrial natriuretic peptide.
Next question

Which one of the following cells secretes the majority of tumour necrosis factor in humans?
Neutrophils
Macrophages
Natural killer cells
Killer-T cells
Helper-T cells
Please rate this question:
Discuss and give feedback
Next question
Tumour necrosis factor
Tumour necrosis factor (TNF) is a pro-inflammatory cytokine with multiple roles in the immune system TNF is secreted mainly by macrophages and has a number of effects on the immune system, acting mainly in a paracrine fashion:
activates macrophages and neutrophils
acts as costimulator for T cell activation key mediator of bodies response to Gram negative septicaemia similar properties to IL-1 anti-tumour effect (e.g. phospholipase activation)
TNF-alpha binds to both the p55 and p75 receptor. These receptors can induce apoptosis. It also cause activation of NFkB Endothelial effects include increase expression of selectins and increased production of platelet activating factor, IL-1 and prostaglandins TNF promotes the proliferation of fibroblasts and their production of protease and collagenase. It is thought fragments of receptors act as binding points in serum

Systemic effects include pyrexia, increased acute phase proteins and disordered metabolism leading to cachexia TNF is important in the pathogenesis of rheumatoid arthritis - TNF blockers (e.g. infliximab, etanercept) are now licensed for treatment of severe rheumatoid
Next question

Which of the following is responsible for the rapid depolarisation phase of the myocardial action
potential?
Rapid sodium influx
Rapid sodium efflux
Slow efflux of calcium
Efflux of potassium
Rapid calcium influx
Please rate this question:
Discuss and give feedback
Next question
Electrical activity of the heart
Myocardial action potential
Phase Description Mechanism
0 Rapid depolarisation Rapid sodium influx
These channels automatically deactivate after a few ms
1 Early repolarisation Efflux of potassium

Phase Description Mechanism
2 Plateau Slow influx of calcium
3 Final repolarisation Efflux of potassium
4 Restoration of ionic
concentrations
Resting potential is restored by Na+/K+ ATPase
There is slow entry of Na+ into the cell decreasing the potential
difference until the threshold potential is reached, triggering a new
action potential
NB cardiac muscle remains contracted 10-15 times longer than skeletal muscle
Conduction velocity
Atrial conduction Spreads along ordinary atrial myocardial fibres at 1 m/sec
AV node
conduction
0.05 m/sec
Ventricular
conduction
Purkinje fibres are of large diameter and achieve velocities of 2-4 m/sec (this allows a
rapid and coordinated contraction of the ventricles
Next question

Which of the following is not a feature of normal cerebrospinal fluid?
It has a pressure of between 10 and 15 mmHg.
It usually contains a small amount of glucose.
It may normally contain up to 5 red blood cells per mm3.
It may normally contain up to 3 white blood cells per mm3.
None of the above
It should not contain red blood cells. Please rate this question:
Discuss and give feedback
Next question
Cerebrospinal fluid
The CSF fills the space between the arachnoid mater and pia mater (covering surface of the brain). The total volume of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is reabsorbed via the arachnoid granulations which project into the venous sinuses. Circulation
1. Lateral ventricles (via foramen of Munro) 2. 3rd ventricle 3. Cerebral aqueduct (aqueduct of Sylvius) 4. 4th ventricle (via foramina of Magendie and Luschka) 5. Subarachnoid space 6. Reabsorbed into the venous system via arachnoid granulations into superior sagittal sinus Composition
Glucose: 50-80mg/dl
Protein: 15-40 mg/dl Red blood cells: Nil White blood cells: 0-3 cells/ mm3
Next question

Which of the following is not an effect of somatostatin?
It stimulates pancreatic acinar cells to release lipase
It decreases gastric acid secretion
It deceases gastrin release
It decreases pepsin secretion
It decreases glucagon release
It inhibits pancreatic enzyme secretion. Please rate this question:
Discuss and give feedback
Gastric secretions
A working knowledge of gastric secretions is important for surgery because peptic ulcers are common, surgeons frequently prescribe anti secretory drugs and because there are still patients around who will have undergone acid lowering procedures (Vagotomy) in the past. Gastric acid
Is produced by the parietal cells in the stomach
pH of gastric acid is around 2 with acidity being maintained by the H+/K+ ATP ase pump. As part of the process bicarbonate ions will be secreted into the surrounding vessels.
Sodium and chloride ions are actively secreted from the parietal cell into the canaliculus. This sets up a negative potential across the membrane and as a result sodium and potassium ions diffuse across into the canaliculus.
Carbonic anhydrase forms carbonic acid which dissociates and the hydrogen ions formed by dissociation leave the cell via the H+/K+ antiporter pump. At the same time sodium ions are actively absorbed. This leaves hydrogen and chloride ions in the canaliculus these mix and are secreted into the lumen of the oxyntic gland.
This is illustrated diagrammatically below:

Image sourced from Wikipedia
Phases of gastric acid secretion There are 3 phases of gastric secretion: 1. Cephalic phase (smell / taste of food)
30% acid produced
Vagal cholinergic stimulation causing secretion of HCL and gastrin release from G cells
2. Gastric phase (distension of stomach )
60% acid produced
Stomach distension/low H+/peptides causes Gastrin release
3. Intestinal phase (food in duodenum)

10% acid produced High acidity/distension/hypertonic solutions in the duodenum inhibits gastric acid secretion
via enterogastrones (CCK, secretin) and neural reflexes.
Regulation of gastric acid production
Factors increasing production include:
Vagal nerve stimulation
Gastrin release Histamine release (indirectly following gastrin release) from enterchromaffin like cells
Factors decreasing production include:
Somatostatin (inhibits histamine release)
Cholecystokinin Secretin
The diagram below illustrates some of the factors involved in regulating gastric acid secretion and the relevant associated pharmacology
Image sourced from Wikipedia
Below is a brief summary of the major hormones involved in food digestion:
Source Stimulus Actions

Gastrin G cells in
antrum of the stomach
Distension of
stomach, extrinsic
nerves
Inhibited by: low
antral pH,
somatostatin
Increase HCL, pepsinogen and IF secretion,
increases gastric motility, trophic effect on gastric mucosa
CCK I cells in
upper small
intestine
Partially digested
proteins and
triglycerides
Increases secretion of enzyme-rich fluid
from pancreas, contraction of gallbladder
and relaxation of sphincter of Oddi,
decreases gastric emptying, trophic effect on
pancreatic acinar cells, induces satiety
Secretin S cells in
upper small
intestine
Acidic chyme, fatty acids
Increases secretion of bicarbonate-rich fluid
from pancreas and hepatic duct cells,
decreases gastric acid secretion, trophic effect on pancreatic acinar cells
VIP Small
intestine, pancreas
Neural Stimulates secretion by pancreas and
intestines, inhibits acid and pepsinogen secretion
Somatostatin D cells in the
pancreas and
stomach
Fat, bile salts and
glucose in the
intestinal lumen
Decreases acid and pepsin secretion,
decreases gastrin secretion, decreases
pancreatic enzyme secretion, decreases
insulin and glucagon secretion
inhibits trophic effects of gastrin, stimulates gastric mucous production









![Management of hyperglycaemia in type 2 diabetes, 2015: a … · 2017-02-15 · management of hyperglycaemia in patients with type 2 diabetes [1, 2]. This was needed because of an](https://img.pdfslide.net/doc/110x75/5d19738b88c9934e5f8cbe4e/management-of-hyperglycaemia-in-type-2-diabetes-2015-a-2017-02-15-management.jpg)





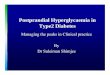

![Management of hyperglycaemia in type 2 diabetes, 2015: a … · 2018. 4. 18. · management of hyperglycaemia in patients with type 2 diabetes [1, 2]. This was needed because of an](https://img.pdfslide.net/doc/110x75/5fda9ab05aea46451967b889/management-of-hyperglycaemia-in-type-2-diabetes-2015-a-2018-4-18-management.jpg)