Embed Size (px)
Citation preview
Amniotic fluid embolism “ Anaphylactoid Syndrome of Pregnancy “
Prof. Dr. Bahaa EwissProfessor of Ansthesia & Intensive Care Unit
Ain Shams university

Introduction Amniotic fluid embolism is pure
unpreventable, unpredictable & incompletely
understood syndrome with potentially lethal
complication ( mortality rate up to 85%).
So since it is rapid , progressive & with lethal
complication, so the diagnosis is very difficult
& by exclusion.

It was 1st described by Brazilian medical journal in
1926 , then diagnosed in 1941 by finding fetal debris
in maternal lungs & Finally, in 1966, fetal debris were
found in maternal lungs, kidneys, spleen.
The pulmonary artery contains layers of pink
strips of squames,
derived from the amniotic
fluid.
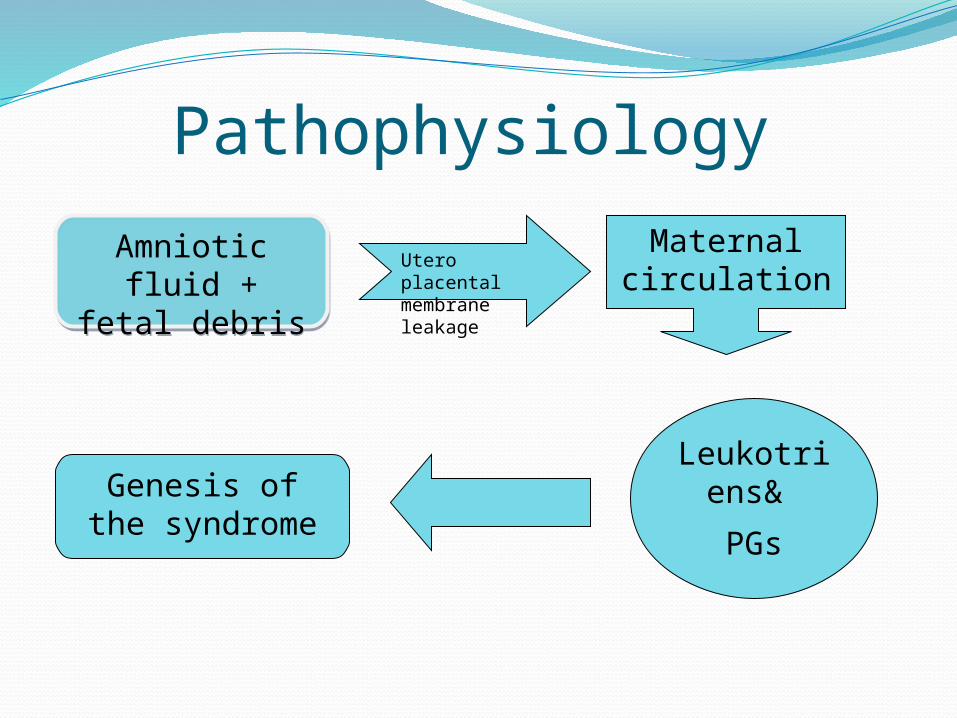
Pathophysiology
Amniotic fluid + fetal debris
Amniotic fluid + fetal debris
Utero placental membrane leakage
Maternal circulation
Leukotriens&
PGs
Genesis of the syndrome

Predisposing factorsAge: > 35 years oldAmniocentesisArtificial rupture of
membraneCervical ulcerationC.S.EclampsiaFetal macrosomiaFetal distress
Medical induction of labor
InstrumentationMultiparicictyPlacenta previaPolyhydramniosUterine rupture
Presentation
In case of vaginal delivery or C.S. under
spinal anesthesia:
Acute unexplained hypotension
Desaturation , hypoxia , bronchospasm, ….
In case of C.S. under G.A. :
Unexplained hypotension, hypoxia ,
coagulopathy

Cardiac presentationBiphasic
Short & rapid Long & slow progressive
Right ventricular failure
Pulmonary hypertension
Pumonary edema
Hypoxia
Mortality 50 %
Left ventricular
failure
Hypotension
Pumonary congestion
Right ventricular
failure
Presentation cont….
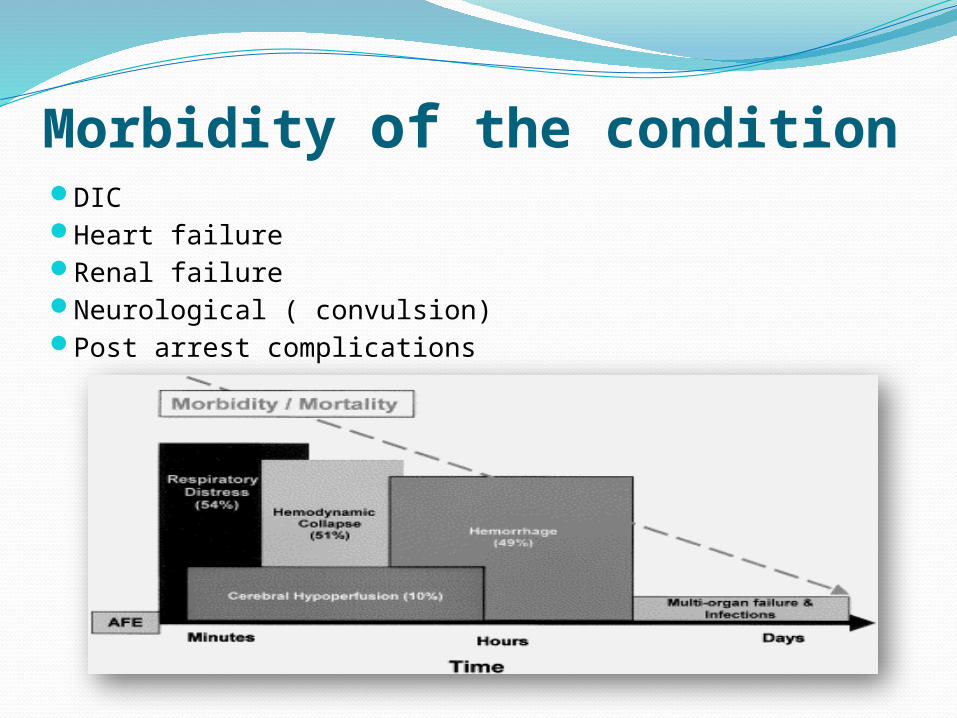
Morbidity of the conditionDICHeart failureRenal failureNeurological ( convulsion)Post arrest complications
MonitoringBasic:
ECGNIBPSO2Capnography
Advanced:T.E.E.Invasive blood pressurePulmonary artery catheterCVP
Investigations “ non specific “
CBC : there is a marked decrease in the platelet levels
Fibrinogen: there is a decrease in the level
FDPs: there is an significant increase in the level
D.dimer : ????
ManagementDelivery may increase the survival of both the
baby & his mother

Management cont…..
According to CPR guideline of pregnant women
Oxygenation
E.T.T
Mechanical ventialtion

Cardio vascular
management
If the patient arrests
CPR must be started
(according to the international guidelines)
Adequate Oxygenation and early intubation
should be considered
Supportive therapy
Vasopressor
Nor adrenaline, dopamine , dobutamine
Management cont…..
Other line of management
Haemofiltration
Plasma exchange
ECMO
Cell salvage
Management of DIC
Ventilator assisted devices
Q1 :What about the role of heparin single dose??
Q2: What about corticosteroid IV??
Frequently asked questions
ConclusionAs it is rapid , progressive with lethal complications so we
should be minded about amniotic fluid embolism & rapid interference.
Good monitoring of the patient during labor , C.S. or in the recovery is mandatory.
Amniotic fluid embolism should be considered in case of rapid progressive hypotension, desaturation & hypoxia.
Rapid delivery of the baby.
CPR as soon as possible.