Embed Size (px)
Citation preview

Prof. L. DamjanovichInstitute of Surgery
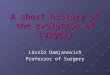
A group of diseases with diverse etiology The common feature is obstruction of the
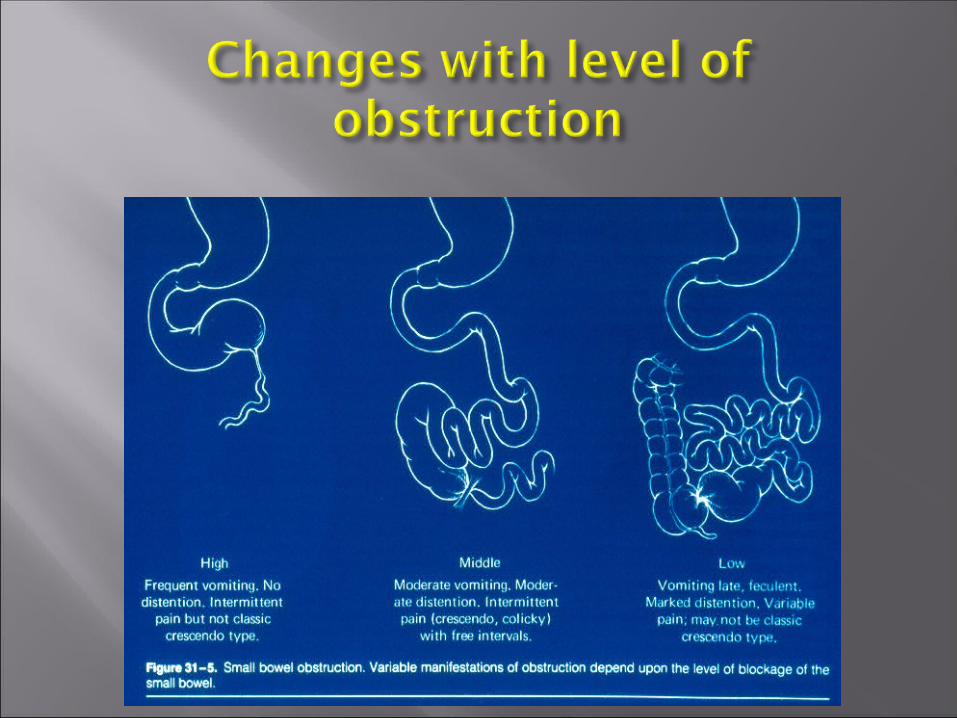
bowel Similar set of symptoms, which may vary
according to site and cause of obstruction Therapy is according to etiology, aiming at
relief from obstruction, and treatment of primary disease
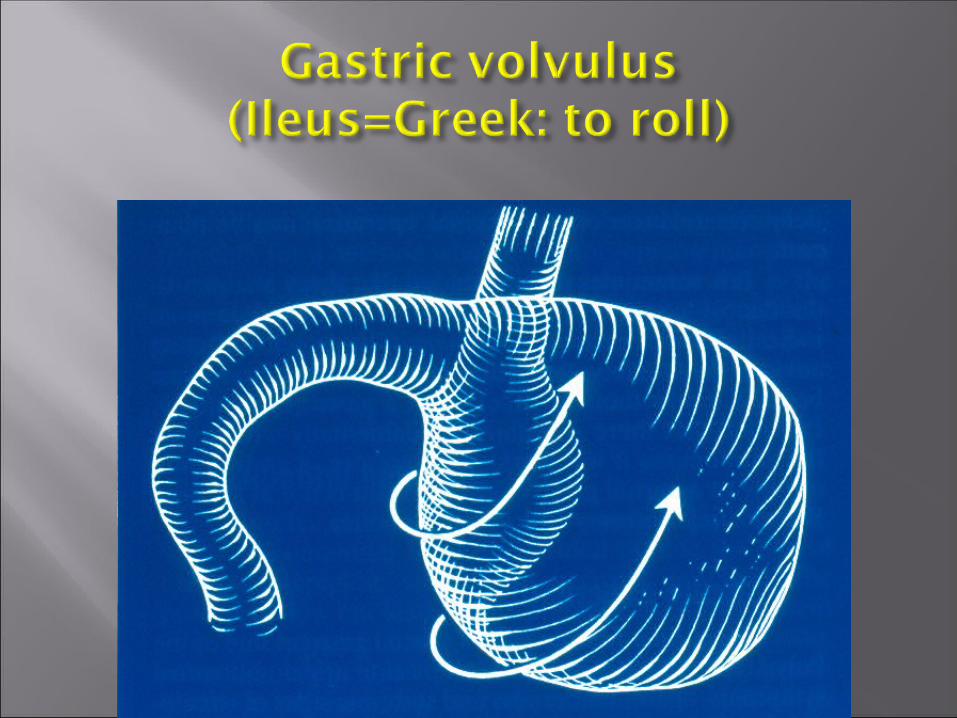
May be mechanical or paralytic (US: ileus)

ClassificationClassification DivisionDivision
EtiologyEtiology IntraluminalIntraluminal
IntramuralIntramural
ExtrinsicExtrinsic
Location within the Location within the
gastrointestinal tractgastrointestinal tractSmall bowelSmall bowel
Large bowelLarge bowel
Speed of onsetSpeed of onset AcuteAcute
SubacuteSubacute
ChronicChronic
DegreeDegree Partial or completePartial or complete
ProgressionProgression Open versus closed loopOpen versus closed loop
Simple versus strangulatedSimple versus strangulated

Site of obstructionSite of obstruction CauseCauseLuminalLuminal Intussusception, Meconium,Intussusception, Meconium,
Polypoid tumor, Gallstone,Polypoid tumor, Gallstone,
Bezoar, Parasites,Bezoar, Parasites,
FecesFeces
MuralMural StrictureStricture (Crohn’s disease, (Crohn’s disease, radiation)radiation)
Small bowel tumorSmall bowel tumor
Congenital atresia, stenosis, Congenital atresia, stenosis, duplicationduplication
ExtrinsicExtrinsic AdhesionAdhesion
HerniaHernia
Malignant or inflammatory Malignant or inflammatory massmass Volvulus Volvulus
Pain Nausea and vomiting Abdominal distension Decreased passage of flatus and stool Possible causes of obstruction:
previous operations, presence of hernias,previous irradiation, previous malignancy

Obstruction-incresased luminal pressure-increased secretion, decreased absorption
Increased peristalsis-stasis-bacterial overgrowth-translocation-septic complications
Sequestration of fluid-third spacing-hypovolemia
Impared perfusion-ischemia-necrosis
Degree of distress Severity of dehydration Evidence of sepsis (if any) Inspection: scars, hernia orifices, distension Auscultation: tinkling, splashing, quiet
abdomen Palpation: location of tenderness, rigidity,
garding Rectal exam

Degree of dehydration Electrolyte imbalance Exclusion of possible other diseases (eg.:
pancreatitis) Imaging: plain abdominal films,
ultrasound CT in special cases (tu. recurrence,
radiation enteritis, Crohn’s disease)

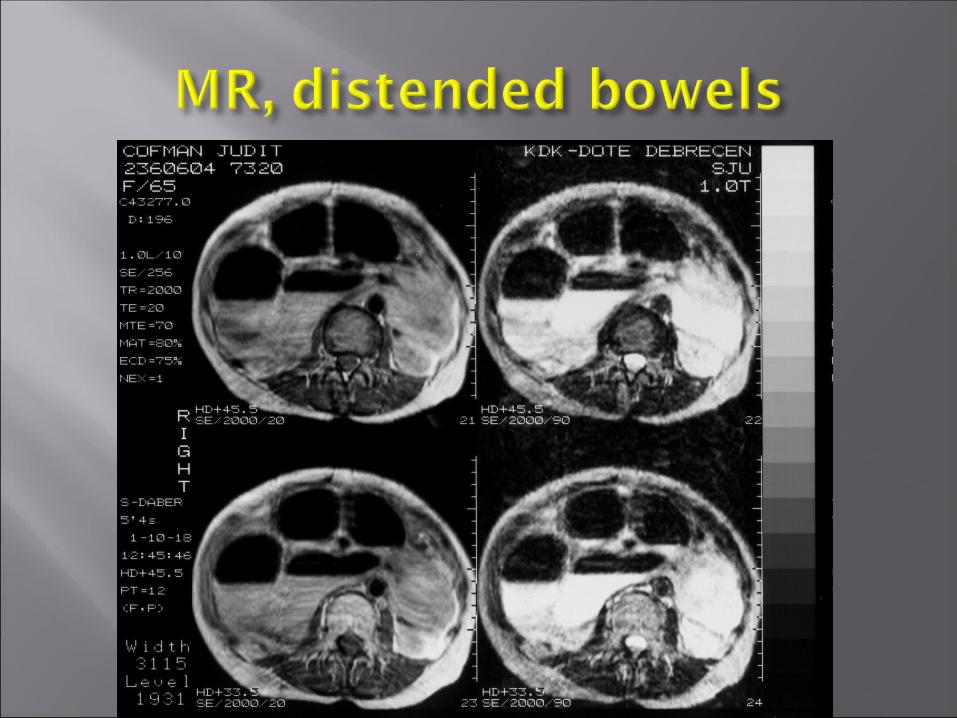
Schematic drawing of X-ray findings in small bowel distension














Longer anamnesis Gradual increase of dull pain (cramping is
rare) No passage of flatus or stool Blood may be found in feces Vomiting comes late, may be feculent if
ileocecal valve is incompetent Cecum is the most prone to perforation

Cancer Diverticulitis - chr. inflammation –
scarring - stenosis Sigmoid-, cecal volvulus
Ogilvie’s syndrom (colonic pseudo-obsruction-paralysis)
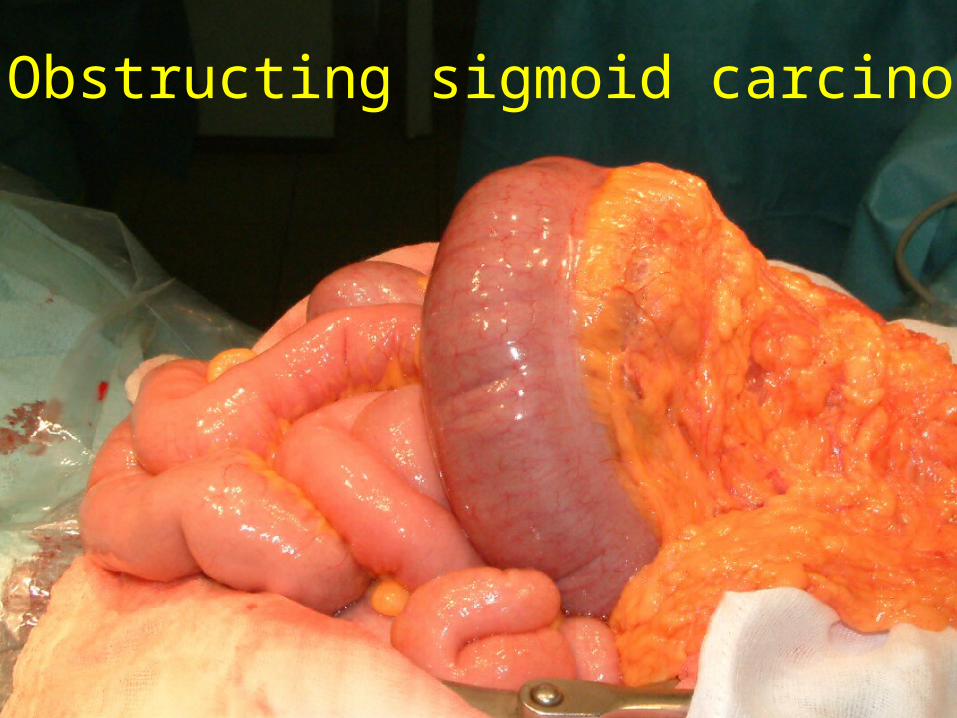
Obstructing sigmoid carcinoma



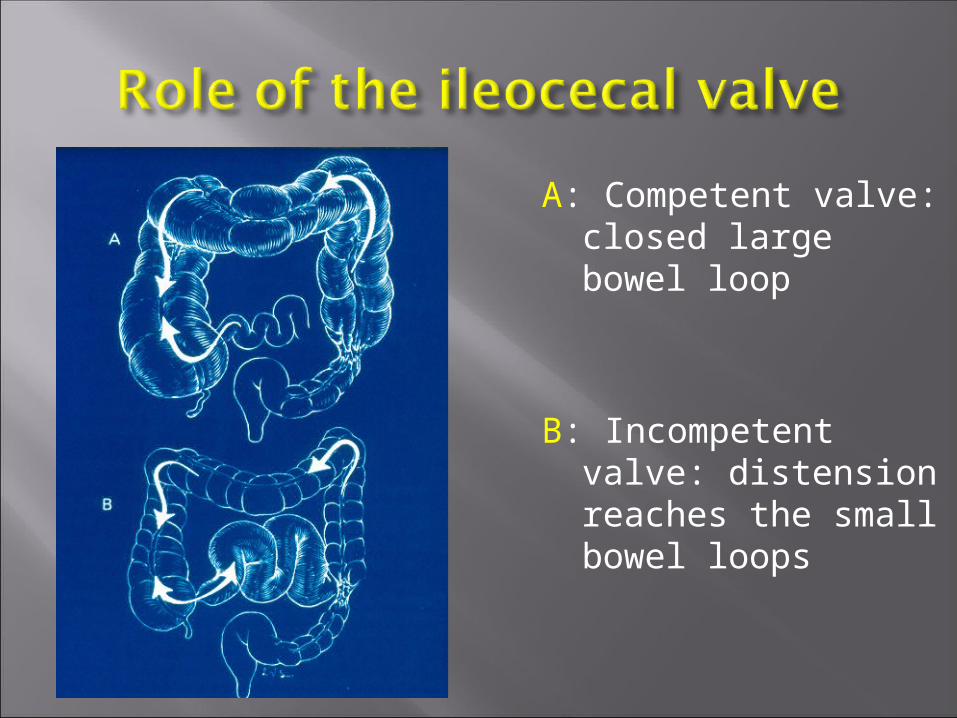
A: Competent valve: closed large bowel loop
B: Incompetent valve: distension reaches the small bowel loops

Unprepared bowel, full of feces, increased bacterial content
Distended, thin walled bowel, compromised circulation
Difficult manipulation because of the distension
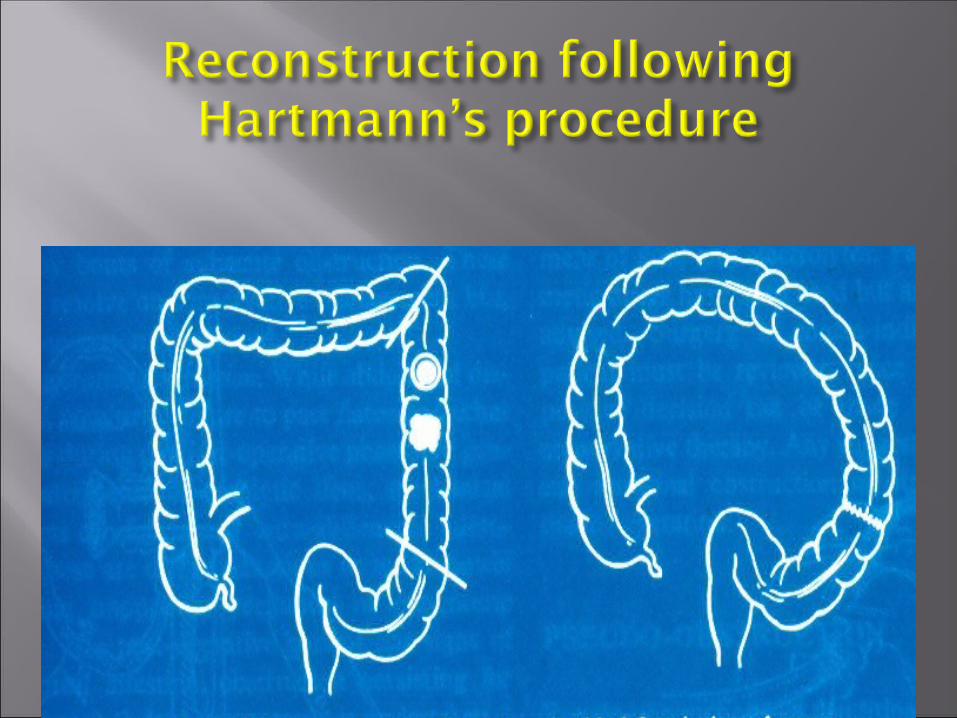
Two stage procedure (Hartmann’s) Extended resection, primary anastomosis Subtotal colectomy On table lavage, primary anastomosis Loop colostomy in inoperable cases Non-operative decompression-
semielective operation
Henrik Kehlet







Causes:DM, hypothyroidism, kidney insuff, opiates, antiparkinson drugscong. heartfailure, MS, lupus, amyloidosis, dermatomyositis, scleroderma, sepsis, trauma (head, spine) operation (abdominal, heart, neurosurgery)
Therapy:Eliminate instigating factors (if possible), Enema, laxativesCholinesterase blocker,Ganglion blockersColonoscopy-may be therapeuticSurgery: perforation, failure of cons. meas.


![Final presentation [Autosaved]...Congenital*Epulis:Unusual*Etiology*of*Airway* Obstruction*and*Feeding*Failure*in*a*Newborn* ShilpaVishwanath,MD,MS 1;H.-James-Williams,-MD2;Aaron-C.-Mason,-MD3](https://img.pdfslide.net/doc/110x75/5f04e2387e708231d410304f/final-presentation-autosaved-congenitalepulisunusualetiologyofairway.jpg)