Embed Size (px)
Citation preview

ICARO 2009 Round Table Discussion
Cost & Economic Analyses in Radiation Oncology
Prof. Rajiv
Sarin, MD, FRCR
Director
Advanced Centre for Treatment, Research & Education in Cancer (ACTREC)
TATA MEMORIAL CENTRE
MUMBAI
INDIA

Criteria for deciding cost effectiveness for expensive new anti‐cancer agents
Sarin
R (Editorial), Jr. Cancer Res. Ther. 4(1) 2008.
•
New Radiation Technologies should be subjected to same analyses and same cut offs as for other health interventions including the
new molecular targeted therapies
•
WHO recommends using per capita GDP (adjusted for Purchase Power Parity) of a country for deciding the cut off for cost
effectiveness of health interventions
IF additional cost incurred to gain 1 quality adjusted life year
is< 1 times the GDP:
COST EFFECTIVE INTERVENTION
1 – 3 times the GDP:
PROBABLY COST EFFECTIVE INTERVENTION
> 3 times the GDP:
NOT COST EFFECTIVE INTERVENTION
INDIA: Per capita GDP adjusted for Purchase Power Parity: 3800 US$

Radiotherapy is one of the most cost effective modality for cancer management
Cost effectiveness analyses for radiotherapy is complicated by major global differences in
•
Type and stages of cancers to be treated
•
Throughput ‘required’
per unit & handicaps in expertise
•
Work practices (Monday – Friday: 9am – 5pm or weekends also)
•
Initial Capital Cost of Equipment
•
Interest rates
•
Cost of maintenance
•
Downtime of the machine
•
Replacement cycle or life of machine
UNIVERSAL PROBLEMIntegration of New
Technology in ‘Routine Care’without proper analysis of
‘Clinical Benefit’ complicates Cost effectiveness analyses

How New Technology is being Integrated in How New Technology is being Integrated in Radiation Oncology in Radiation Oncology in ‘‘most partsmost parts’’ of the worldof the world
We start with & often get lost in discussing the technical capabilities, finesse, &
precision of new technology & how good it would be for our patients.
Soon we say that patients want this new technology & it becomes ‘standard of care’

Evidence Based Assessment & Integration of Evidence Based Assessment & Integration of Technology in Radiation OncologyTechnology in Radiation Oncology
Societal Costs
Technical Capabilities &
Precision
Clinical Benefit
Research (Clinical and Health Economic Evaluation) in Emerging Technology becomes a necessity in Emerging economies to provide a solid foundation
Could be the starting point
BUT not the Centre point

How should we integrate New Technology in How should we integrate New Technology in ‘‘Routine Clinical PracticeRoutine Clinical Practice’’
•
Overwhelming superiority in the clinical
outcome with new technology OR
•
Modest but definite benefit
•
Results are generally reproducible
•
Possible to integrate the new technology in a
particular health care system

Emerging Technology PromisesEmerging Technology Promises
•
Lower toxicity
•
Improved Patient and Personnel Safety
•
Better documentation and validation
<< Improved cure rates >>
May be Higher Throughput & Cost effectiveness in certain clinical contexts

Emerging Technology Generally EntailsEmerging Technology Generally Entails
•
Higher initial and maintenance Cost
•
Uncertainty of clinical benefits
•
Uncertainty of sturdy performance
•
Human resource implications
•
Skepticism of the critics & health economists
May prove to be expensive experimental tool, especially in emerging economies

Cost –
effectiveness of RT can be improved by
•
Optimal utilization of the conventional technologies and better work practices
–
Indications and prioritization
–
Fractionation
–
Audits, QA and QC programme
•
New Technologies–
For better case selection (e.g. PET imaging)
–
Hypo‐fractionation in select indications
•
Indigenous Technology –
May have lower initial / maintenance cost
–
Better suited for local conditions

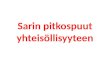
α/β ratio of tumour
(7-10Gy) much higher than late responding
normal tissues (2-4Gy); e.g. Squamous Ca
H&N, Lung, Cervix
α/β ratio of Tumour
(1.5 - 2Gy) < late
responding normal tissue (2-4Gy);
e.g. Prostate Cancer
HYPERRACTIONATED / ACCELERATED RT
HYPERRACTIONATED / ACCELERATED RT
Improve tumour control without increasing late
toxicity (possibly more acute toxicity)HYPOFRACTIONATED RT
HYPOFRACTIONATED RT
Better utilisation of health resources
Tumour control &late toxicity comparableα/β ratio of Tumour (3 – 5Gy) similar
or slightly higher than late
responding normal tissue (2-4Gy);
e.g. Breast Cancer
HYPOFRACTIONATED RT
HYPOFRACTIONATED RT
Improve tumour control
with similar or reduced
late & acute toxicity
Evidence Based Clinico-Radiobiological Fractionation Pyramid
New Technology generally permits greater normal tissue sparing, thereby facilitating hypo-fractionation in ‘certain clinical contexts’ with similar / better Therapeutic Ratio
SarinSarin R, Lancet R, Lancet OncolOncol. 2006 (7); 445. 2006 (7); 445--47 47
Higher initial cost of new technology may be
partly offset if it provides clinical benefit to sufficient number of patients with suitable
tumours types
Use of fewer fractions, if safe would be to
great advantage for patients and
‘professionals’ alike

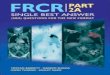
BHABHATRON BHABHATRON --
TELECOBALTTELECOBALTDeveloped by BARC, Dept.
of Atomic Energy in 2004Technology Transferred to
Panacea Tech. Ltd. BangaloreDosimetric & Clinical
evaluation of Prototype unit at ACTREC in 2005 - 06
Refined version Bhabhatron-II in use at ACTREC and in almost dozen Indian centres
Integrated in Indian National Cancer Control Programme in the 11th Five Year Plan in 2008
VISIONVISIONDept. of Atomic Energy of India set up a special Apex committee in 2003 to develop
high quality & cost effective indigenous equipment with initial emphasis on Telecobalt
Indian Indigenous Cancer Technology Development Programme

MISSION MODE Academia – Industry
partnership can facilitate development of high quality
and cost effective indigenous technology in developing countries with some pre-
existent technological base.
Indian Indigenous Cancer Technology Development Programme
The Dept. of Atomic Energy & Tata Memorial Centre are continuing with coordinated efforts to develop and validate Indigenous Equipment for Cancer (LINAC, PACS, SIMULATOR etc.)
Bhabhatron II

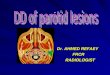
India is donating India is donating BhabhatronBhabhatron
TelecobaltTelecobalt
to Vietnam under the to Vietnam under the IAEA IAEA ‐‐
PACT (Programme Action for Cancer Therapy)PACT (Programme Action for Cancer Therapy)
Building SustainableBuilding Sustainable Cancer Control Capacity and InfrastructureCancer Control Capacity and Infrastructure
in Developing Countries in Developing Countries
Chairman, Atomic Energy Commission of India handing over a model of Bhabhatron to IAEA Director General, Dr El-Baradei at ACTREC, Mumbai (2007)

Emerging economies have TWIN REALITIES which pose Special Challenges of Optimizing limited resources through Indigenous R&D;
Evaluation of new technology & Cost effectiveness studies
Two localities in Mumbai few miles apart Two bunkers in ACTREC sharing a wall
Indigenous Indigenous TelecobaltTelecobalt
TomotherapyTomotherapy