Embed Size (px)
Citation preview

José L. Pomar,MD, PhD
Professor of Surgery
The Thorax Clinic Institute
University of Barcelona
Barcelona, Spain
Professional Societies: Fostering and
monitoring innovation in CVS

Tissue Heart Valves
Homografts: From calves to cryopreservation (UK)
Heterografts: Early studies to nowadays (France)
Porcine versus Perciardial (France and UK)
Stented vs stentless (Toronto)
Tissue engineering (Boston)
TAVI (France)
Sutureless tissue valves (Italy)

Gordon Murray, 1956
Charles Hufnagel (first prosthetic valve 1952)

Homografts in 1962…from Oxford to London & Australia
Carlos M.G. Durán Brian Barratt-Boyes Donald N. Ross
From the lab to straight human implantation
Lariboisière and Broussais Hospitals
François Broussais 1772-1838 Alain Carpentier
Charles Dubost

First commercially available THV
Hancock porcine
Warren Hancock
Warren Hancock

Other times….
Bill Clinton and John F. Kennedy Sarkozy

Alain Cribier and the TAVI

The Transcatheter Heart Valve Implants

Still durability of TAVI remains unknown
Stent design
Tissue handling
Native valve
Residual AR
AV block
TE

Quick evolution of designs
CENTERA Transcatheter Heart Valve
Modifying
stresses, stent
shape, device
profile, skirt,

Also in the mitral position …

Why Irreversible Electroporation (IRE) for tissue ablation?
Irreversible electroporation does not involve thermal heating
1-tissue scaffold is preserved, 2- heat sink effect is irrelevant
Normal rat artery
Rat artery one week after
IRE treatment
Vascular smooth muscle cells in
the Tunica Media are destroyed
but the extracellular matrix is
still functional
(Maor et al. PLoS ONE 4:3 e4757 2009)

Regulatory bodies
CE mark
FDA approval

Somethings are unregulable
Repaired Congenital Heart Diseases in the Adult
The heart physiology
The body adaptation after years
The imaging of the unknown
The new coming symptoms
Their adequate treatment
The best surgical approach for residual complications

Support of Professional Societies
Improve treatment of CV patients through
Continuous education of professionals: Excellence
Incentivize research to achieve
Evidence of the benefits of the diverse therapeutical
options
Safe innovations
“Education of the community through classic and new
communication tools”

Types of CTS Scientific Associations
National
International

Types of Scientific Associations
National: Inclusive
International: Inclusive
Exclusive

Most relevant Scientific Associations
AATS
STS EACTS
CTSNet
ASCVS, ESCVS, ESTS, SHVD …

Scientific Associations: An exclusive
Number of members: For some years 400
US and International members
Membership committee
About 50% acceptance rate
Requisites are for rather high academic level
Great offer of courses and opportunities. Reputation.
Membership
Founded in 1917 by the earliest pioneers in the field of thoracic surgery, the
American Association for Thoracic Surgery (AATS) is now an international
organization of over 1,200 of the world’s foremost cardiothoracic surgeons
representing 35 countries.
Members of the AATS are surgeons with a proven record of distinction within the
international cardiothoracic surgical field and have made meritorious
contributions to the extant knowledge base about cardiothoracic disease and its
surgical treatment.

Scientific Associations: An exclusive
Annual Meeting
Aortic at the Big Apple
Mitral Conclave
Slow Asian and Middle East expansion
Scientific Associations: An exclusive
EXCELLENCE IN RESEARCH AS A MAIN GOAL

Scientific Associations: An inclusive
Purpose
Founded in 1964, The Society of Thoracic Surgeons is a not-for-
profit organization representing over 6,600 surgeons,
researchers and allied health care professionals worldwide
who are dedicated to ensuring the best possible outcomes for
surgeries of the heart, lung, and esophagus, as well as other
surgical procedures within the chest.

Scientific Associations: An inclusive
Staff Core Values
With a staff of approximately 50 employees, The Society of
Thoracic Surgeons is headquartered in Chicago and has an
additional office near Capitol Hill in Washington, DC. A team of
dedicated professionals, the STS staff strives for excellence as it
upholds the staff core values of respect, teamwork, innovation,
quality service, and ownership.

Scientific Associations: An inclusive
STS National Database
The STS National Database was established in 1989 as an initiative for quality
improvement and patient safety among cardiothoracic surgeons. There are three
components to the STS National Database, each focusing on a different area of
cardiothoracic surgery—Adult Cardiac, General Thoracic, and Congenital Heart
Surgery, with the availability of Anesthesiology participation within the Congenital
Heart Surgery Database. The Database has grown exponentially over the years, both
in terms of participation and stature.

Scientific Associations: EACTS
Francis Fontan Keyvan Mogishi Marko Turina
27 years ago…. From ESCVS to EACTS
Scientific Associations: EACTS
OBJECTS
The Charity's objects are specifically restricted to the following:
1. To advance education in the field of cardiac, thoracic and vascular interventions
2. To promote for the public benefit research into
cardiovascular and thoracic physiology, pathology and therapy and to correlate and disseminate the useful results thereof.

Scientific Associations: EACTS
The Bergamo School for CT Surgery
The Windsor Headquarters. Staff
The Freiburg Editorial office after Lausanne and Zurich
An outstanding Multi Media Manual
The first approximation to EuroPCR
Joint ventures with ESC
The Syntax, the Excel, and others…
The HEART TEAM model

Scientific Associations: EACTS

Scientific Associations: EACTS
OFFICE NAME TERM OF OFFICE
Chair Philippe H. Kolh 2012 - 2013
Member Joel Dunning 2008 - 2012
Ex-officio A. Pieter Kappetein 2011 - 2014
Member Ulf Lockowandt 2008 - 2012
Member Jose Luis Pomar 2012 - 2013
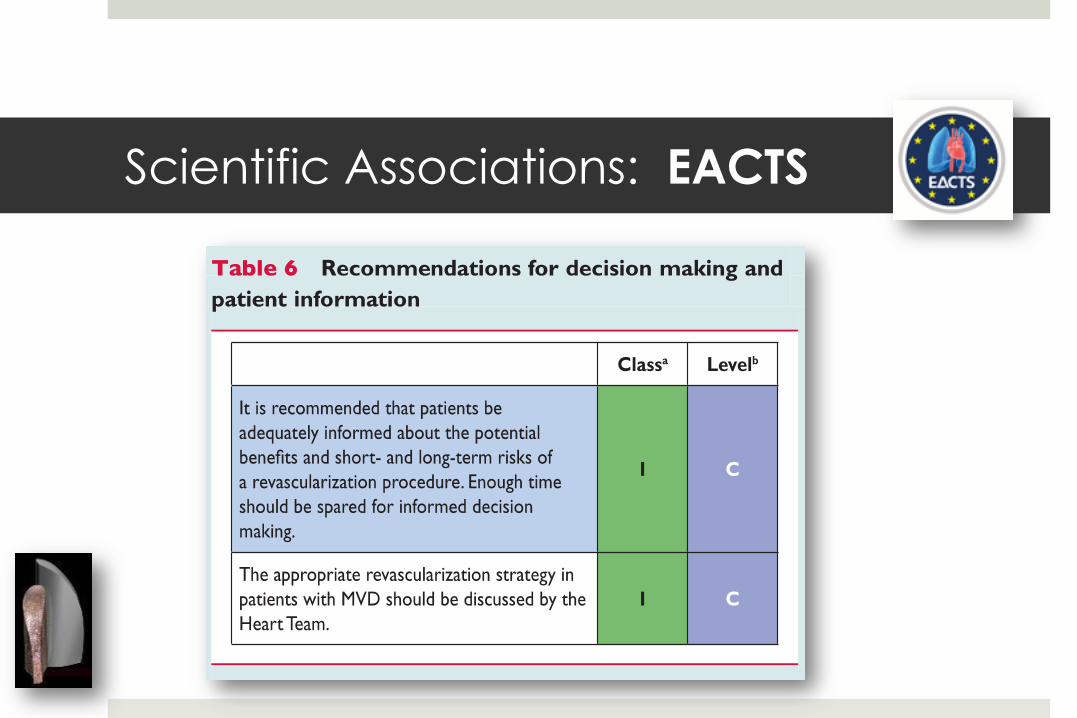
The Guidelines Committee

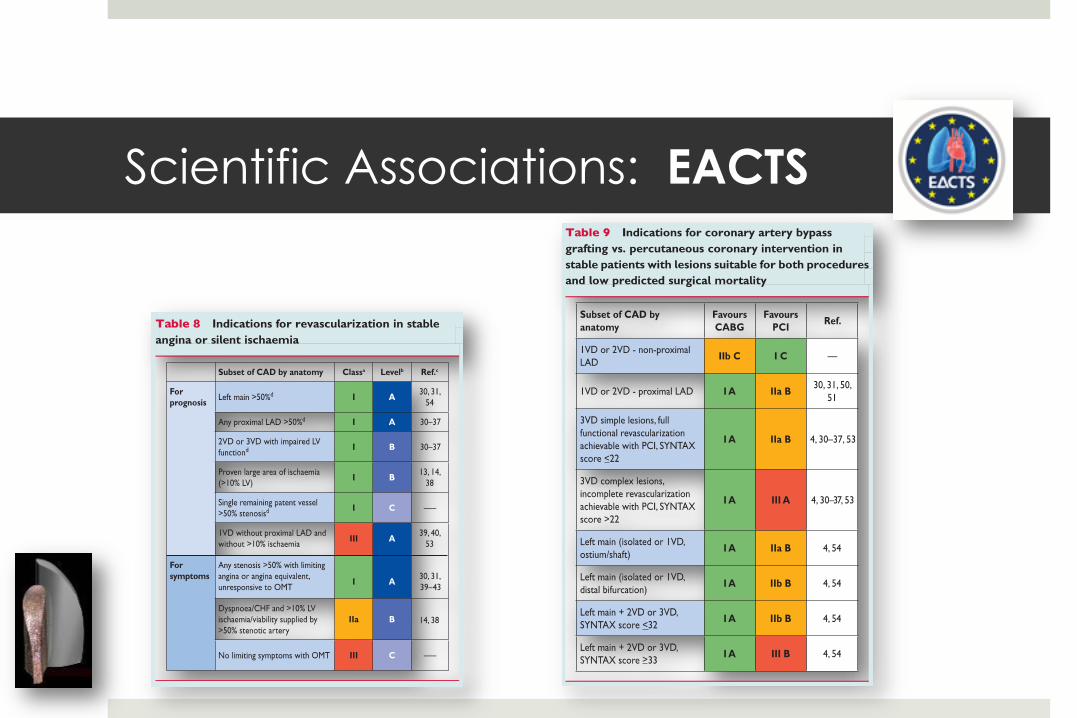
Scientific Associations: EACTS ESC/EACTS GUIDELINES
Guidelines on myocardial revascularizat ion
The Task Force on Myocardial Revascular izat ion of the European
Society of Cardiology (ESC) and the European Associat ion for
Cardio-Thoracic Surgery (EACTS)
Developed with the special cont r ibut ion of the European Associat ion
for Percutaneous Cardiovascular Intervent ions (EAPCI)‡
Authors/Task Force Members: W illiam W ijns (Chairperson) (Belgium)*, Philippe Kolh
(Chairperson) (Belgium)*, NicolasDanchin (France), Car lo Di Mar io (UK),
Volkmar Falk (Switzer land), Thierry Folliguet (France), Scot Garg (The Nether lands),
Kur t Huber (Austr ia), Stefan James (Sweden), Juhani Knuut i (Finland), Jose
Lopez-Sendon (Spain), Jean Marco (France), Lorenzo Menicant i (Italy)
Miodrag Ostojic (Serbia), Massimo F. Piepoli (Italy), Char lesPir let (Belgium),
Jose L. Pomar (Spain), N icolausReifar t (Germany), Flavio L. Ribichini (Italy),
Mar t in J. Schalij (The Nether lands), Paul Sergeant (Belgium), Patr ick W . Serruys
(The Nether lands), Sigmund Silber (Germany), Miguel Sousa Uva (Por tugal),
David Taggart (UK)
ESC Commit tee for Pract ice Guidel ines: Alec Vahanian (Chairperson) (France), Angelo Aur icchio (Switzer land),
Jeroen Bax (The Nether lands), Claudio Ceconi (Italy), Veronica Dean (France), Gerasimos Filippatos (Greece),
Chr ist ian Funck-Brentano (France), Richard Hobbs (UK), Peter Kearney (Ireland), Theresa McDonagh (UK),
Bogdan A. Popescu (Romania), Zeljko Reiner (Croat ia), Udo Sechtem (Germany), Per Anton Sirnes (Norway),
Michal Tendera (Poland), Panos E. Vardas (Greece), Pet r W idimsky (Czech Republic)
EACTS Clinical Guidelines Commit tee: Philippe Kolh (Chair person) (Belgium), Ot tavio Alfier i (Italy), Joel Dunning
(UK), Stefano Elia (Italy), Pieter Kappet ein (The Nether lands), Ulf Lockowandt (Sweden), George Sarr is (Greece),
Pascal Vouhe (France)
Document Reviewers: Peter Kear ney (ESC CPG Review Coordinator) (Ireland), Ludwig von Segesser (EACTS
Review Coordinat or) (Switzer land), Stefan Agewall (Norway), Alexander Aladashvi li (Georgia),
Dimit r ios Alexopoulos (Greece), Manuel J. Antunes (Portugal ), Enver Atalar (Turkey), Aar t Brutel de la Riviere
‡Other ESC entities having participated in the development of this document :
Associations: Heart Failure Association (HFA), European Association for Cardiovascular Prevention and Rehabilitation (EACPR), European Heart Rhythm Association (EHRA), Euro-
pean Association of Echocardiography (EAE).
Working Groups: Acute Cardiac Care, Cardiovascular Surgery, Thrombosis, Cardiovascular Pharmacology and Drug Therapy.
Councils: Cardiovascular Imaging, Cardiology Practice.
* Corresponding authors (the two chairpersons contributed equally to this document): William Wijns, Cardiovascular Center, OLV Ziekenhuis, Moorselbaan 164, 9300 Aalst,
Belgium. Tel: + 32 53 724 439, Fax: + 32 53 724 185, Email: [email protected]
Disclaimer . The ESC Guidelines represent the views of the ESC and were arrived at after careful consideration of the available evidence at the time they were written. Health
professionals are encouraged to take them fully into account when exercising their clinical judgement. The guidelinesdo not, however, override the individual responsibility of health
professionals to make appropriate decisions in the circumstances of the individual patients, in consultation with that patient, and where appropriate and necessary the patient’s
guardian or carer. It is also the health professional’s responsibility to verify the rules and regulations applicable to drugs and devices at the time of prescription.
& The European Society of Cardiology 2010. All rights reserved. For Permissions please email: journals.permissions@oxfor djournals.org.
Philippe Kolh, Cardiovascular Surgery Department, University Hospital (CHU, ULg) of Liege, Sart Tilman B 35, 4000 Liege, Belgium. Tel: + 32 4 366 7163, Fax: + 32 4 366 7164,
Email: [email protected]
The content of these European Society of Cardiology (ESC) Guidelines has been published for personal and educational use only. No commercial use is authorized. No part of the
ESC Guidelines may be translated or reproduced in any form without written permission from the ESC. Permission can be obtained upon submission of awritten request to Oxford
University Press, the publisher of the European Heart Journal and the party authorized to handle such permissions on behalf of the ESC.
European Heart Journal (2010) 31, 2501–2555
doi:10.1093/eurheartj/ehq277

Scientific Associations: EACTS
Scientific Associations: EACTS
Scientific Associations: EACTS
Scientific Associations: EACTS
TECHNO COLLEGE
Innovation of the last days
No science behind but some evidence of interest
Life vs life in a box demonstrations
Highly attended session during the Annual Meeting

Controversies: Off vs on pump CABG
EACTS News and Recent Publications
Editors: K. M. John Chan FRCS CTh, John R. Pepper FRCS
European Association for Cardio-Thoracic Surgery http://www.eacts.org/
Off- and on-pump CABG have similar early outcomes but
differences in repeat revascularisation and complication rates
29 March 2012
The CORONARY Trial recently reported similar outcomes for off- and on-pump CABG at the American
College of Cardiology Foundation. The results were also published in the NEJM.1 The trial
randomised 4752 patients from 79 centres in 19 countries who were receiving CABG to either an off-
pump or on-pump procedure. Surgeons in the trial who performed off-pump CABG had to have at
least two years’ experience of pe r fo rming the procedure and ha d to ha v e performed at least 100 off-
pump CABGs. The conversion rate from off-pump to on-pump CABG during coronary grafting was
2.6%.
At 30 days, there was no difference between off-pump and on-pump CABG in the primary composite
outcome of death, non-fatal stroke, non-fatal myocardial infarction or new renal failure requiring
dialysis (9.8% vs 10.3%; p=0.59), or in any of its individual components. There were, however,
important differences in revascularisation and complication rates in the two groups with off-pump
CABG having higher revascularisation rates compared to on-pump CABG (0.7% vs 0.2%; p=0.01), but
lower rates of transfusion (50.7% vs 63.3%; p<0.001), re-operation for bleeding (1.4% vs 2.4%;
p=0.02), respiratory complications (5.9% vs 7.5%; p=0.03) and acute kidney injury (28.0% vs 32.1%;
p=0.01) (Table 1). Patients in the off-pump CABG group received less number of grafts (3.0 vs 3.2;
p<0.001) and had a higher rate of incomplete revascularisation as assessed by the surgeon at the
time of surgery (11.8% vs 10.0%; p=0.05).
Off pump
CABG
On pump
CABG
HR 95% CI p
Composite primary outcome (%) 9.8 10.3 0.95 0.79 – 1.14 0.59
Repeat revascularisation (%) 0.7 0.2 4.01 1.34 – 12.0 0.01
Blood product transfusion (%) 50.7 63.3 0.80 0.75 – 0.85 <0.001
Re-operation for bleeding (%) 1.4 2.4 0.61 0.40 – 0.93 0.02
Acute kidney injury (%) 28.0 32.1 0.87 0.80 – 0.96 0.01
Respiratory complications (%) 5.9 7.5 0.79 0.63 – 0.98 0.03
Table 1. 30 day results of the CORONARY Trial.
EACTS News and Recent Publications
Editors: K. M. John Chan FRCS CTh, John R. Pepper FRCS
European Association for Cardio-Thoracic Surgery http://www.eacts.org/
Off- and on-pump CABG have similar early outcomes but
differences in repeat revascularisation and complication rates
29 March 2012
The CORONARY Trial recently reported similar outcomes for off- and on-pump CABG at the American
College of Cardiology Foundation. The results were also published in the NEJM.1 The trial
randomised 4752 patients from 79 centres in 19 countries who were receiving CABG to either an off-
pump or on-pump procedure. Surgeons in the trial who performed off-pump CABG had to have at
least two years’ experience of pe r fo rming the procedure and ha d to ha v e performed at least 100 off-
pump CABGs. The conversion rate from off-pump to on-pump CABG during coronary grafting was
2.6%.
At 30 days, there was no difference between off-pump and on-pump CABG in the primary composite
outcome of death, non-fatal stroke, non-fatal myocardial infarction or new renal failure requiring
dialysis (9.8% vs 10.3%; p=0.59), or in any of its individual components. There were, however,
important differences in revascularisation and complication rates in the two groups with off-pump
CABG having higher revascularisation rates compared to on-pump CABG (0.7% vs 0.2%; p=0.01), but
lower rates of transfusion (50.7% vs 63.3%; p<0.001), re-operation for bleeding (1.4% vs 2.4%;
p=0.02), respiratory complications (5.9% vs 7.5%; p=0.03) and acute kidney injury (28.0% vs 32.1%;
p=0.01) (Table 1). Patients in the off-pump CABG group received less number of grafts (3.0 vs 3.2;
p<0.001) and had a higher rate of incomplete revascularisation as assessed by the surgeon at the
time of surgery (11.8% vs 10.0%; p=0.05).
Off pump
CABG
On pump
CABG
HR 95% CI p
Composite primary outcome (%) 9.8 10.3 0.95 0.79 – 1.14 0.59
Repeat revascularisation (%) 0.7 0.2 4.01 1.34 – 12.0 0.01
Blood product transfusion (%) 50.7 63.3 0.80 0.75 – 0.85 <0.001
Re-operation for bleeding (%) 1.4 2.4 0.61 0.40 – 0.93 0.02
Acute kidney injury (%) 28.0 32.1 0.87 0.80 – 0.96 0.01
Respiratory complications (%) 5.9 7.5 0.79 0.63 – 0.98 0.03
Table 1. 30 day results of the CORONARY Trial.
FOCUS SESSIONS

Own Journal original articles

Reviews from other Journals
EACTS News and Recent Publications
Editors: K. M. John Chan FRCS CTh, John R. Pepper FRCS
European Association for Cardio-Thoracic Surgery http://www.eacts.org/
Tricuspid Valve Repair for Tricuspid Annular Dilatation shows benefit
15 April 2012
A randomised trial from Rome recently reported improved cardiac and functional outcomes when
tricuspid valve annnuloplasty was performed in the presence of tricuspid annular dilatation but
without significant functional tricuspid regurgitation.1 The study randomised 44 patients undergoing
mitral valve surgery with less than moderate functional tricuspid regurgitation but a dilated tricuspid
annulus (≥ 40mm) to either mitral valve surgery alone or to mitral valve surgery plus tricuspid valve
annuloplasty. At 12 months, patients who had concomitant tricuspid valve annuloplasty had less TR
(TR absent in 71% versus 19%, p=0.001; moderate-to-severe TR in 0% versus 28%, p=0.02), greater
right ventricular reverse remodelling, and greater improvement in the six minute walk test (+115m
versus +75m, p=0.008).
This study is consistent with an earlier study reporting worsening TR grade and NYHA functional class
if tricuspid annular dilatation is not corrected at the time of mitral valve surgery irrespective of the
grade of TR.2
A previous study from Leiden, Netherlands, also reported that tricuspid valve annuloplasty at the
time of mitral valve surgery in patients with tricuspid annular dilatation but without significant
functional tricuspid regurgitation (TR), improved right ventricular (RV) reverse remodelling and
prevented progression of TR.3 This study compared 80 patients undergoing mitral valve repair in
2002 in whom concomitant tricuspid annuloplasty was only performed if there was grade 3 or 4 TR
(13 patients), against 102 patients operated in 2004 in whom concomitant tricuspid annuloplasty
was performed if there was either grade 3 or 4 TR (21 patients) or tricuspid annular dilatation
greater than 40 mm measured by echocardiography irrespective of the degree of TR (43 patients). At
two years, in the 2002 cohort, where tricuspid annuloplasty was only performed if there was grade 3
or 4 TR, RV reverse remodelling was not demonstrated (RV long axis 69 ± 7 vs 70 ± 8 mm, p=0.30; RV
short axis 29 ± 7 vs 30 ± 7 mm, p=0.08). TR was absent or mild in the 13 patients who had
concomitant tricuspid annuloplasty, but progressed with RV dilatation in the 23 patients with
tricuspid annular dilatation who did not have concomitant tricuspid annuloplasty (p<0.001).
Conversely, in the 2004 cohort, where tricuspid annuloplasty was performed if either tricuspid
annular dilatation or significant TR was present, RV reverse remodelling was observed (RV long axis
71 ± 6 vs 69 ± 9 mm, p=0.01; RV short axis 29 ± 5 vs 27 ± 5 mm; p<0.0001) and TR severity decreased
(1.6 ± 1.0 vs 0.9 ± 0.6; p<0.0001).
ESC guidelines currently recommend tricuspid annuloplasty in patients undergoing left sided valve
surgery with severe TR or moderate TR with tricuspid annular dilatation greater than 40 mm
measured by echocardiography. The ACC/AHA guidelines recommend tricuspid annuloplasty at the
time of mitral valve surgery for severe TR and consideration of tricuspid annuloplasty in less than
severe TR if pulmonary hypertension or tricuspid annular dilatation is present.4,5

EACTS News and Recent Publications
Editors: K. M. John Chan FRCS CTh, John R. Pepper FRCS
European Association for Cardio-Thoracic Surgery http://www.eacts.org/
REFERENCES
1. Benedetto U, Melina G, Angeloni E, Refice S, Roscitano A, Comito C, Sinatra R. Prophylactic
tricuspid annuloplasty in patients with dilated tricuspid annulus undergoing mitral valve surgery.
J Thorac Cardiovasc Surg 2012; 143:632-8
2. Dreyfus GD, Corbi PJ, Chan KMJ, Bahrami T. Secondary tricuspid regurgitation or dilatation:
which should be the criteria for surgical repair? Ann Thorac Surg 2005;79:127-32.
3. Van de Veire NR, Braun J, Delgado V, Versteegh MIM, Dion RA, Klautz RJM, Bax JJ. Tricuspid
annuloplasty prevents right ventricular dilatation and progression of tricuspid regurgitation in
patients with tricuspid annular dilation undergoing mitral valve repair. J Thorac Cardiovasc Surg
2011;141:1431-9.
4. Vahanian A, Baumgartner H, Bax J, Butchart E, et al. Guidelines on the management of valvular
heart disease. Eur Heart J 2007;28:230-268.
5. Nishimura RA, Carabello BA, Faxon DP, Freed MD, Lytle BW, et al. 2008 focused update
incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular
heart disease. Circulation 2008;118:e523-e661
Reviews from other Journals

The literature
Special Boundary Roles in the
Innovation Process
Michael L. Tushman
Administrative Science Quarterly
Vol. 22, No. 4 (Dec., 1977), pp. 587-605

The recommended literature and societies
The International Society for Professional
Innovation Management (ISPIM

Scientific Associations: EACTS
Too few surgeons apply for them….Why?

Scientific Associations: EACTS
EACTS PRIORITIES FOR THE NEXT 3 YEARS
A Pan-European training Program
The quality improvement program (QUIP)
High quality data base
Guidelines reinforcement

Monitoring the good use of innovation

Conclusion
No surgical innovation without evaluation
Peter McCulloch MD a Corresponding AuthorEmail Address, Prof Douglas G Altman DSc b,
Prof W Bruce Campbell FRCS FRCP c, Prof David R Flum MD d, Prof Paul Glasziou PhD e,
Prof John C Marshall MD f, Prof Jon Nicholl DSc g, for the Balliol Collaboration‡
Achievement of improved design, conduct,
and reporting of surgical research will need
concerted action by editors, funders of health
care and research, regulatory bodies, and
professional societies. The Lancet, Volume 374, Issue 9695, Pages 1105 - 1112, 26 September 2009

End of the talk





























