Embed Size (px)
Citation preview

5/24/2013
1
Ahmed El-Massry M.D.
Professor of Ophthalmology
Alexandria University
Egypt
No Financial interest ESOIRS 2013
ASCRS 2013
Acknowledgement
Dr. Mones Abdalla

5/24/2013
2
History
The concept of adding tissue in the periphery
of the cornea to reshape its curvature was
introduced earlier by Barraquer in 1949.
In 1986, Ferrara, initiated the use of ICRs to
moderate and high myopia.
In 1995, a phase II clinical trial (FDA) began using
intrastromal corneal ring segments by Keravision
Inc.
In 1999, Approved by the FDA for myopia of -1.00
to -3.00 diopters (D) and thus received the name
Intacs. by Addition Technology Inc.,.

5/24/2013
3
MECHANISM OF ACTION
When material is
removed from the
central area of the
cornea or added to
the periphery:
a central flattening
effect is achieved
Mechanism of Action
Shorten the corneal cord length → flattening of the
entire cornea maintaining its +ve asphericity.
El-Massry
Mechanism of action (cont)

5/24/2013
4
Mechanism of Action (cont):
For correction of astigmatism, the base of each
segment can produce a traction force on the
surface, leading to a further flattening on its axis of
reference.
This causes:
1- Corneal apex displacement towards the
center.
2- Preservation of corneal Asphericity .
3- reduced surface irregularity.

5/24/2013
5
Indications:
The main indications for the use of ICRs had
steadily increased aiming for :
Correcting Irregular Corneas :
1- Keratoconus.
2- Pellucid marginal degeneration.
3- Post lasik ectasia..
4- Irregular astigmatism after penetrating
keratoplasty,
5- Irregular astigmatism after radial
keratotomy.
6- After corneal trauma on uneven surfaces.
Inclusion criteria for ICRS in KC:
- Clear central cornea.
- Best corrected visual acuity (BCVA)of ≥0.05
- Contact lens intolerant.
- Corneal thickness not less than 400 μ m in the
area of insertion.
.

5/24/2013
6
Inclusion criteria for ICRS (cont):
- - Maximum keratometric readings <64 D
- Spherical equivalent >-3 D
-Base of the cone, by posterior float using
pentacam, was within 5mm optical zone.
Contraindications
• Severe atopic disease.
• Presence of active infection.
• Autoimmune disease systemic or localized.
• Recurrent corneal erosion syndrome.
• Corneal scarring & Hydrops.
• Extensive corneal dystrophies.

5/24/2013
7
TYPES:
INTACs (Addition Technology, Inc, Fremont,CA)
KERA ring (Mediphacos, Belo Horizonte, Brazil) .
150° ring segments
PMMA
Hexagonal CS
6.8 mm
8.1 mm
Sizes (mm) 0.250, 0.300, 0.350, 0400, 0.450
Original Intacs
El-Massry

5/24/2013
8
ICR : Mode of Action
Safest Optical Zones
6.0mm Optical Zone
7.0mm Optical Zone6

5/24/2013
9
Kera Rings: PMMA :
•A triangular cross section of
600 μ m.
•Thickness ranging from 150 to
350 μ m.
• Has arc length variable (90 ° ,
120 °,150 °, 160 ° , 210 ° and
240 ° ).
•There are two models, the SI5
(optical zone of 5.0 mm) and
SI6 (optical zone of 5.5 mm or
6.0 mm)
Kera rings: It changes the contour of the corneal
surface but not by pushing out on the edge
of the cornea like Intacs.
It simply flattens the cornea . Its apex act like
a pivot for corneal stromal tissue.

5/24/2013
10
The Differences:
• Kera rings correct a high myopia : 4.8mm vs.
> 6.0mm in INTACs.
• Shape – Kera shape is triangular shape.
• Kera have rounded edges vs sharper edges.
• Keratacs have an arc
Of 320º vs Intacs of 300º
Pre-surgical planning:
Step 1 : Corneal topography and manifest refraction.

5/24/2013
11
Step 2:
Incision Placement & Verification : Locate and verify positive cylinder axis for incision
placement:
Posterior Float,
Pachymetry.
Peripheral Flattening
Comatic axis

5/24/2013
12
Step 3 : Select segment using proper Nomogram.

5/24/2013
13
Depth of insertion :
Pachymetry at the site of
insertion is verified by
using U/S pachymetry
and anterior segmant
OCT.
insertion to 66%, 70%, 75% and 80% depth.
Leaving at least 100 µ residual stromal bed.
The difference between the inner & outer
depth was adjusted in laser settings
according to OCT measurements.

5/24/2013
14
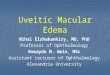
The incision along the topographic axis of positive cylinder (slit lamp).
the centre of the cornea marked geometrically.
75% depth at 7mm OZ using ultrasound pachymetry
Pocketing on either side of the incision
Globe fixation with a vacuum centering guide. Two intrastromal channels were created .
Two 450 microns equal PMMA segments were implanted. 10-0 Nylon sutures.
El-Massry
Intacs with mild corneal
haze few days after CXL

5/24/2013
15

5/24/2013
16
Mechanical Intacs
Mechanical Intacs

5/24/2013
17
Complications of mechanical
Tunnel creation:
Epithelial defects.
Perforation.
Infectious keratitis.
Shallow or asymmetric segment placement.
Corneal stromal edema around the incision.
Extension of the incision toward the central visual
axis or the limbus ,
Unpredictable tunnel depth and persistent incisional
gaping.
Decentration,
Extrusion.
Ring migration.

5/24/2013
18
Complications are minimized as tunnel
creation now can be carried out with the
femtosecond laser.
Implementation in the Femtosecond laser:
Procedure:
1.) Femtosecond laser cut:
a) Tunnel
b) Access
2.) Insertion of the Rings.
Advantages
(all femtosecond-systems):
- Arbitrary diameter.
- Controlled width of the tunnel.
- Selectable/controlled depth.
- Defined access cut.
- different depth inside/outside
(e.g. for back-plane parallel ICR)
- tunnel segments < 360° (90° - 270°)
(e.g. for asymmetric Keratoconus)
- shape of access
- 1 or 2 access ports

5/24/2013
19
Tailor-made incisions
- Inner diameter of ring tunnel.
- Outer diameter of ring tunnel.
- Incision depth of inner ring tunnel.
- Incision depth of outer ring tunnel.
- Anterior width of access incision.
- Posterior width of access incision.
- Number of tunnel access incisions ( 1, 2)
Fig. 1 Front view of the eye with
tunnel and access incisions
Fig. 2 Side view of the section of the
cornea with tunnel incision sections
Fig. 3 Sections of the cornea
in the access incision plane

5/24/2013
20
The procedure.
ASSOCIATION OF ICRs AND CROSS-
LINKING
Few studies combining the two
techniques described so far.(Coskunseven et
al. 2009 , Wollensak et al., Ertan et al. )
Greatest effect with the addition of cross-
linking treatment.
Initially, it can function as a simple additive
effect.

5/24/2013
21

5/24/2013
22

5/24/2013
23
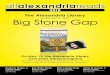
Anterior segment OCT for
femtosecond laser assisted ICRS
CONCLUSIONS:
- Rate of Complications is higher in the
mechanical group.
- Faster rehabilitation period in
Femtosecond laser group
- ICRs using either mechanical or femtosecond
laser; provide similar visual and refractive
outcomes

5/24/2013
24