Embed Size (px)
Citation preview

Proficiency of Internal Medicine Residents in Outpatient Care of Patients with HIV Infection
PETER SCHULTZ, MD, MPH, ANDREW B. BINDMAN. MD, MOLLY COOKE, MD
To determine internal medicine residents' knowledge of HIV care, the authors conducted a survey of residents from four internal medicine programs in the San Francisco Bay area. On a knowledge test, the mean score was 42.4/55, 77% correct. The residents performed relatively worse on questions regarding didanosine and zalcitabine, tuberculosis prophylaxis, and risk of cervical neoplasia in HIV-infccted women. Predictors of greater knowledge were specific residency program, higher postgraduate year, primary care residency track, and more extensive HIV experience. Primary care internal medicine residencies and programs with more exposure to HIV patients are most effective in producing knowledgeable residents. K ~ words: human immuno- deficiency virus; internship and residency; internal medicine; ambu- latory care, knowledge, attitudes, practice; primary care.
J GEN INTERN MED 1994;9:459-461.
APPROPRIATE MANAGEMENT o f H I V - i n f e c t e d i nd iv idua l s s l o w s
the progression to AIDS and has the potential to prevent immunodeficiency-related morbidity and mortality. 1 Es- tablished recommendations for the care of HIV-infected persons at the time of this study included CD4 + T-lym- phocyte testing, 2 screening and prophylaxis for tuber- culosis (TB) 3 and hepatitis B, 4, s screening for syphilis, 6 pneumococcal 7 and influenza 8 vaccinations, counseling about minimizing the risk of infecting others with HIV, 9
zidovudine for those with CD4 + cell counts <500 cells/ mm3, t°' ~ and Pneumocys t i s carini i pneumonia (PCP) prophylaxis for those with CD4 + cell counts <200 cells/ mm~. 2 HIV-infected women may benefit from frequent cervical cytologic screening. 12 Alternative antiretroviral agents are under study, and two of these, didanosine and zalcitabine, have now been approved by the U.S. Food and Drug Administration for use in selected HIV-infected patients. ~ -~
For HIV-infected patients to have access to high- quality medical care, their physicians must be knowl- edgeable about early interventions for HIV infection. As
Received from the Division of General Internal Medicine, San Francisco General Hospital (PS, ABB), the Institute for Health Policy Studies (ABB), and the Division of General Internal Medicine, Department of Medicine, and the Center for AIDS Prevention Studies (MC), University of California San Francisco, San Francisco, California.
Supported by the AIDS Clinical Research Center, University of California San Francisco, VA Medical (;enter (141A), 4150 Clement Street, San Francisco, CA 94121; and National Institute of Mental Health (;rant: MH44045 (Dr. Cooke). Dr. Bindman is a Robert Wood Johnson Generalist Physician Faculty Scholar.
This research was conducted, in part, while Dr. Schultz was a fellow in general internal medicine and clinical epidemiology in the Division of General Internal Medicine, San Francisco General Hospital, San Francisco, California.
Address correspondence and reprint requests to Dr. Bindman: Division of General Internal Medicine, Room 5H22, San Francisco General Hospital, 1001 Potrero Avenue, San Francisco, California 94l 10.
the epidemic grows, it is increasingly important that internal medicine residents become competent in HIV care. This study describes the level of knowledge about appropriate interventions in HIV-infected outpatients among a group of internal medicine residents.
METHODS
We performed a cross-sectional study of knowledge regarding outpatient HIV care by mailing self-adminis- tered questionnaires* in March 1992 to 293 residents in four internal medicine residency programs in the San Francisco Bay area. Program A is in a public hospital, program B is in a health maintenance organization, and programs C and D are university-based. The question- naire contained closed-ended items on demographics, residency program characteristics, HIV experience, and knowledge about preventive care. Questions about pre- ventive care were developed from the published liter- ature and pretested with 23 senior physicians who had expertise in HIV care. The questions for which the "cor- rect" response could be supported in the literature and validated by concurrence of 80% or more of the experts were used for analysis. The directions accompanying the questionnaire asked the respondents to complete the survey at a single sitting and not to consult outside sources or to guess at answers. We analyzed the respondents' overall knowledge, differences between the most and least knowledgeable quintiles, and individual and pro- gram characteristics associated with HIV knowledge.
RESULTS
Respondents
One hundred seventy-three of the 293 residents returned the surveys (response rate of 59% ). Response rates from specific residency programs varied: program A, 28/50 (56%); program B, 12/32 (37.5%); program C, 38/75 (51%); and program D, 95/136 (70%) (chi square, p = 0.03).
Knowledge
The mean performance of all the respondents and the scores of the most and least knowledgeable quintiles on the 55-item knowledge test and in specific knowledge
*The study questionnaire and additional information about the study methodology and data analysis are available from the authors upun request.
459
460 Schultz et 31. RESIDENTS" PROFICIENCY IN HIV CARE
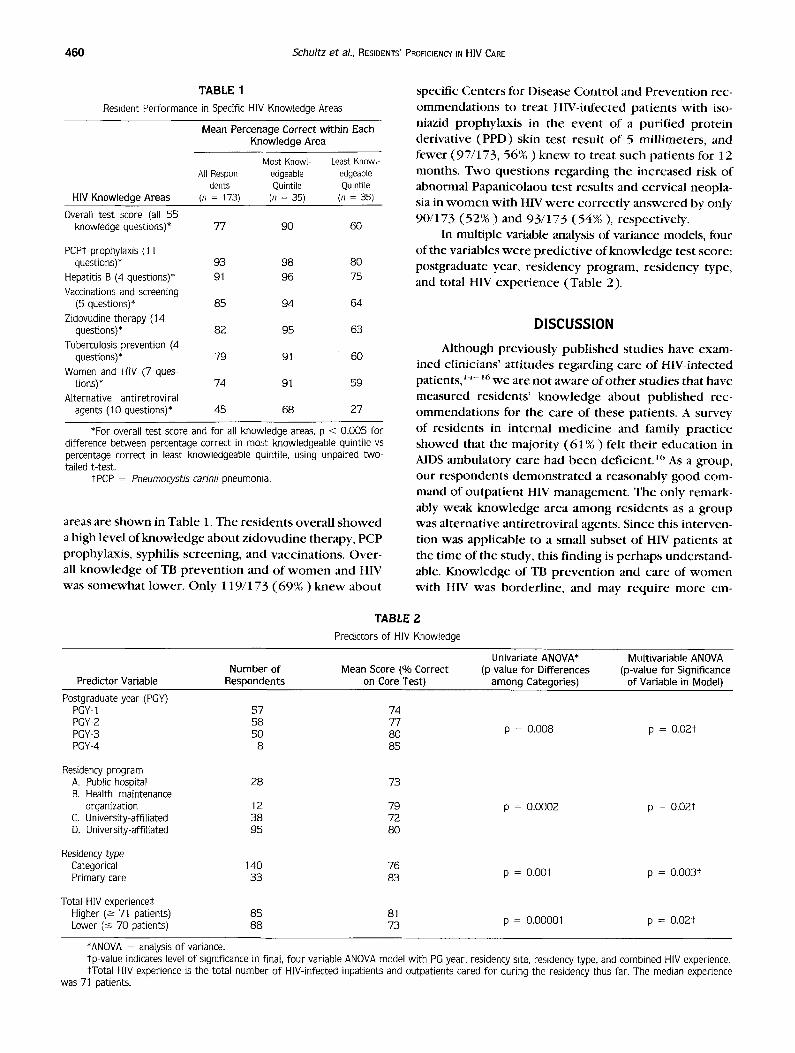
TABLE 1 Resident Performance in Specific HIV Knowledge Areas
HIV Knowledge Areas
Mean Percenage Correct within Each Knowledge Area
Most Knowl Least Knowl- All Respon- edgeable edgeable
dents Quintile Quintile (n = 173) (n : 35) (n = 35)
Overall test score (all 55 knowledge questions)* 77 90 60
PCPt prophylaxis (11 questions)* 93 98 80
Hepatitis B (4 questions)* 91 96 75 Vaccinations and screening
(5 questions)* 85 94 64 Zidovudine therapy (14
questions)* 82 95 63 Tuberculosis prevention (4
questions)* 79 91 60
Women and HIV (7 ques- tions)* 74 91 59
Alternative antiretroviral agents (10 questions)* 45 68 27
*For overall test score and for all knowledge areas, p < 0.005 for difference between percentage correct in most knowledgeable quintile vs percentage correct in least knowledgeable quintile, using unpaired two- tailed t-test,
tPCP = Pneumocystis cariniJ pneumonia.
areas are shown in Table 1. The r e s iden t s overa l l s h o w e d a high level of k n o w l e d g e abou t z i d o v u d i n e therapy, PCP prophylaxis , syphi l is sc reening , and vacc ina t ions . Over- all k n o w l e d g e of TB p r e v e n t i o n and of w o m e n and HIV was s o m e w h a t lower . On ly 119/173 ( 6 9 % ) k n e w abou t
specific Cen te r s for Disease Con t ro l and P reven t ion rec- o m m e n d a t i o n s to t rea t HIV-infected pa t i en t s w i th iso- niazid p rophy lax i s in the even t of a pur i f i ed p ro t e in der ivat ive (PPD) skin tes t resu l t o f 5 mi l l imeters , and fewer (97/173, 56% ) k n e w to t rea t such pa t ien t s for 12 months. Two ques t ions r ega rd ing the i nc reased risk of abnormal Papanico laou tes t resul ts and cerv ica l neopla- sia in w o m e n wi th HIV w e r e c o r r e c t l y a n s w e r e d by on ly 90/173 ( 5 2 % ) and 93 /173 ( 5 4 % ) , respec t ive ly .
In mult iple variable analysis of variance models, four of the var iables w e r e p r e d i c t i v e of k n o w l e d g e test score: pos tg radua te year, r e s i d e n c y p rogram, r e s idency type, and total HIV e x p e r i e n c e (Tab l e 2).
D I S C U S S I O N
Although p rev ious ly p u b l i s h e d s tud ies have exam- ined cl inic ians ' a t t i tudes r ega rd ing ca re o f HIV-infected patients, J~-~6 w e are no t a w a r e of o t h e r s tud ies that have measured res idents ' k n o w l e d g e abou t pub l i shed rec- o m m e n d a t i o n s for the ca re of these pat ients . A survey of res idents in in ternal m e d i c i n e and family p rac t i ce showed that the major i ty ( 6 1 % ) felt t he i r educa t ion in AIDS ambula to ry care had b e e n def ic ient . ~c, As a group, our r e s p o n d e n t s d e m o n s t r a t e d a r ea sonab ly good com- mand of ou tpa t i en t HIV managemen t . The only remark- ably weak k n o w l e d g e area a m o n g r e s iden t s as a g roup was a l ternat ive an t i re t rov i ra l agents. Since this in terven- tion was appl icab le to a small subse t of HIV pa t ien ts at the t ime of the study, this f inding is p e r h a p s unders tand- able. Knowledge of TB p r e v e n t i o n and ca re of w o m e n with HIV was borde r l ine , and may r e q u i r e m o r e em-
TABLE 2 Predictors of HIV Knowledge
Univariate ANOVA* Multivariable ANOVA Number of Mean Score (% Correct (p-value for Differences (p-value for Significance
Predictor Variable Respondents on Core Test) among Categories) of Variable in Model)
Postgradua~ year(PGY) PGY-1 57 74 PGY-2 58 77 PGY-3 50 80 PGY-4 8 85
Residency program A. Public hospital 28 73 B. Health maintenance
organization 12 79 C. University-affiliated 38 72 D. University-affiliated 95 80
Residency type Categorical 140 76 Primary care 33 83
Total HIV experiences Higher (--> 71 patients) 8S 81 Lower (-< 70 patients) 88 73
p = 0.008 p = O,02t
p = 0.0002 p = O.02t
p = 0.001 p = O.O03t
p - 0.00001 p = O.02t
*ANOVA = analysis of variance. tp-value indicates level of significance in final, four variable ANOVA model with PG year, residency site, residency type, and combined HIV experience, *Total HIV experience is the total number of HIV-infected inpatients and outpatients cared for during the residency thus far. The median experience
was 71 patients.

JOURNAL OF GENERAL INTERNAL MEDICINE, Volume 9 (August). 1994 461
phasis in the residency curriculum. There were several areas of possible knowledge deficit among some resi- dents; the least knowledgeable quinti le scored less than 65% in five of seven knowledge areas. These lower scores are of concern because almost half (48 .5%) of this quin- tile was made up of second- and third-year residents, who may be practicing in the clinic with little super- vision.
The superior amounts of knowledge with advancing postgraduate year and with more total H1V experience are not surprising. The finding that training in a primary care internal medicine residency track is associated with higher knowledge of outpat ient HIV care may reflect the
greater commitment to ambulatory care issues in these programs.
Validation of our survey was attempted by an ex- tensive literature review during questionnaire devel- opment and by eliminating questions on which HIV ex- perts could not agree, but the weighting of content areas involved the judgment of the researchers. Program D (whose residents performed the best on our survey) had the highest response rate and provided most of the re- spondents, poss ibly leading us to overes t imate the knowledge level of our sample. Our study measured knowledge, which alone does not ensure the provision of appropriate care. On the other hand, the residents were answering questions from memory, and it is pos- sible that they could perform better in clinical settings where they could consult colleagues or written mate- rials. Because of the high prevalence of HIV-infected individuals living in the study area, it is likely that res- ident HIV knowledge is better in this region than in the nation as a whole.
Since we concluded this study, many authorities have changed recommendations regarding antiretro- virals~3. ~7 and other aspects of ambulatory HIV care. Any instrument for measuring HIV knowledge will need to change along with the rapidly changing HIV knowledge base. Other researchers may find our survey a useful starting point for developing their own instruments. Fu- ture research should be aimed at designing and testing interventions to teach about basic HIV care and to en- sure their appropriate implementation.
The authors thank Natasha Berry for help with questionnaire devel- opment, Dennis Keane, Michael Fialkow, and Susan Rtthin for advice on data management, and Alice Pressman for statistical assistance.
REFERENCES
l. Jewett J, Hecht F. Preventive health care for adults with HIV infection. JAMA. 1993;269:1144-53.
2. Centers for Disease Control. Guidelines for prophylaxis against Pneumocystis carinii pneumonia for persons infected with hu- man immunndeficiency virus. MMWR. 1989;28(S-5):1-9.
3. ('enters for Disease Control. Screening for tuberculosis infection in high risk populations, and the use of preventive therapy for tuberculosis infection in the United States: recommendations of the Advisory Committee for the Elimination of Tuberculosis. MMWR. 1990;39(no. RR-8):I- 12.
4. Centers for Disease Control. Protection against viral hepatitis: recommendations of the Immunization Practices Advisory Com- mittee (ACIP). MMWR. 1990;39(no. RR-2):5-22.
5. Hadler S. Hepatitis B prevention and human immunodeficiency virus (HIV) infection. Ann Intern Med. 1988;11)9:92-4.
6. ('enters for Disease Control. Recommendations for diagnosing and treating syphilis in HIV-infected patients. MMWR. 1988;37:600- 2, 607-8.
7. (``enters for Disease Control. Recommendations of the Immuni- zation Practices Advisory Committee: pneumococcal polysac- charide vaccine. MMWR. 1989;38(5):64-76.
8. (',enters for Disease Control. Prevention and control of influenza: recommendations of tbe Immunization Practices Advisory Com- mittee (ACIP). MMWR. 1991;40(no. RR-6):I-13.
9, Coates T, l,o B. Counseling patients seropositive for human im- mure,deficiency virus: an approach for medical practice. West J Med. 1990;153:629-34.
10. National Institute of Allergy and Infectious Diseases. Recommen- dations fnr zidovudine: early infection. JAMA. 1991);263( 12 ): 1606, 1609.
11. Volberding P, Lagakos S, Koch M, et al. Zidovudine in asympto- matic human immunodeficiency virus infection: a controlled trial in persons with fewer than 500 CD4-positive cells per cubic mil- limeter. N Engl J Med. 1990;322:941-9.
12. Schrager L, Friedland G, Maude D, et al. Cervical and vaginal squamous cell abnormalities in women infected with human im- munodeficiency virus. J Acquir Immune Defic Syndr. 1989;2:570- 5.
13. I.ips~, JJ. Zalcitahine and didanosine, l.ancet. 1993;341:31)- 2. 14. Gerbert B, Maguire B, Bleecker T, Coates T, McPhee S. Primary
care physicians and AIDS: attitudinal and structural barriers to care. JAMA. 1991;266:2837-42.
15. Calabrese LH, Kelley DM, Cullen RJ, Locker G. Physicians' atti- tudes, beliefs, and practices regarding AIDS health care promotion. Arch Intern Med. 1991;151:1157-60.
16. Hayward RA, Shapiro MF. A national study of AIDS and residency training: experiences, concerns, and consequences. Ann Intern Med. 1991;114:23-32.
17. Bartlett J. Zidovudine now or later? [editorial]. N Engl J Med. 1993;329:351 - 2.





























