Embed Size (px)
Citation preview

International Journal of Cardiology, 33 (1991) 83-88 0 1991 Elsevier Science Publishers B.V. All rights reserved 0167-5273/91/$03.50 ADONIS 016752739100213C
83
CARD10 01325
Profile of right-sided endocarditis: an Indian experience
Anil Grover, Inder S. Anand, Jagmohan Varma, Rajib Choudhury, Hari N. Khattri, Rajendra P. Sapru, Padmakar S. Bidwai and Purshotam L. Wahi
Department of Cardiolo~, Postgraduate fnsrita#e of ~edicai ~ducafion & research, Chandigarh, India
(Received 9 January 1991; revision accepted 8 April 1991)
Grover A, Anand IS, Varma J, Choudhury R, Khattri HN, Sapru RP, Bidwai PS, Wahi PL. Profile of right-sided endocarditis: on Indian experience. Int J Cardiol 1991;33:83-88.
The clinical profile of right-sided infective endoca~itis in India was studied from a review of records of patients with infective endocarditis admitted to this hospital. Prom November I982 to November 1989, 109 patients with infective endocarditis showed vegetations on cross-sectional echocardiography confirm- ing the diagnosis of infective endocarditis. In 19 (17.4%) patients, only the right side of the heart was involved: specifically the tricuspid valve alone in 10; tricuspid and pulmonary valves in 4; tricuspid valve and right ventricular outflow tract in 1; tricuspid valve and right ventricular free wall in 1; pulmonary valve alone in 2, and bifurcation of pulmonary trunk in 1. Eleven patients (57.9%) had underlying congenital heart disease whereas the ~maining 8 patients f42.190) did not have any underwing heart disease. The latter group, therefore, had isolated right-sided infective endocarditis. Previous illnesses leading to isolated right-sided infective endocarditis were: puerperal sepsis in 4; septic abortion in 1; staphylococcal pneumonia in 2; and epididymoorchitis in one. Eight out of 11 patients with congenital heart disease did not report any previous illness. In the remaining 3, right-sided endocarditis followed cardiac surgery in one; dental extraction without prophylaxis in one; and pulmonary balloon valvoplasty in one. All patients with isolated right-sided infective endoearditis had features of septicaemia, but a mu~ur of tricuspid lotion was audible in only 4 Ml%) of them. We conclude that, unlike western reports, the pattern of ~~t-sid~ infective end~~itis in India is different. No drug addict with right-sided infective endocarditis was seen; puerperal sepsis and septic abortion were the commonest causes of isolated right-sided infective endocarditis. Despite the fact that rheumatic heart disease is very common in India, none of the cases had rheumatic heart disease.
Key words: Infective endocarditis; Isolated right sided endocarditis; Puerperal sepsis
Introduction Correspondence to: Dr. I.S. Anand, FRCP, D Phil (Oxon.),
Dept. of Cardiology, VA Medical Centre lllC, 1, Veterans Drive, Minneapolis, MN 55417, U.S.A.
Intravenous drug abuse is believed to be the major predisposing factor for right-sided infective

84
endocarditis in the developed countries and ac- counts for the increasing incidence of the disease in these areas [1,2]. In India, the problem of drug addiction is small and the number of intravenous drug abusers are even smaller; the pattern of right-sided infective endocarditis seen is different [3]. We have, therefore, reviewed the clinical records of all patients of right-sided endocarditis in whom vegetations were found at cross-sec- tional echocardiography to help in the diagnosis of infective endocarditis. In this report, we review our experience of the clinical profile of the cases diagnosed as having infective endocarditis.
Materials and Methods
Patients
The clinical records of all patients with infec- tive endocarditis treated at this institute between November 1982 and November 1989 were re- viewed. All patients were subjected to cross-sec- tional echocardiography which permitted localisa- tion of the site of the vegetations. Only patients satisfying the following criterions were included for analysis: Demonstration of an echo-dense, freely mobile mass attached to any cardiac struc- ture on the right side of heart [tricuspid valve, pulmonary valve, pulmonary arteries, right ven- tricular endocardium or right side of interventric- ular septum]. In addition, any two of the follow- ing: (i) fever > 38 o C for at least 3 days in the hospital; (ii) two or more positive blood cultures growing the same organism; (iii) evidence of sep- tic pulmonary emboli.
Echocardiography
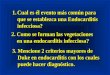
Simultaneous M-mode and cross-sectional echocardiographic examination was performed with a 3.5 or 5 MHz transducer using a Diasonics V 3400 (Diasonics USA) or Ultramark 8 (Ad- vanced Technological Laboratories, Bothell) equipment. Standard cross-sectional images of the heart were obtained and recorded on videotapes for subsequent analysis. Any underlying cardiac anomaly was carefully looked for and established. The diagnosis of a vegetation (Figs. 1 and 2) was
Fig. 1. Cross-sectional echocardiograph in parasternal short axis view. Arrows showing vegetations on tricuspid valve (case 2, isolated right sided endocarditis). RVOF = right ventricular
outflow tract; AOV = aortic valve.
made according to the established criterions [4,5]. For the present study, only unequivocal evidence of a vegetation (verified by two independent ob- servers) was accepted as positive. Technically in- adequate studies were excluded from analysis.
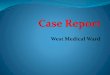
Fig. 2. Cross-sectional echocardiograph in a modified para- sternal short axis view to profile a vegetation attached to pulmonary valve (case 9, group II). PV = pulmonary valve;
RVOF = right ventricular outflow tract; A0 = aorta.

85
The cases were divided into two groups. The first group comprised patients who did not have any underlying congenital or valvular lesion and were designated as isolated right-sided infective endocarditis. The second group comprised pa- tients with right-sided infective endocarditis with underlying heart disease.
Results
TABLE 1
Site of vegetations in patients with right-sided endocarditis.
Tricuspid valve alone 10 Tricuspid valve and pulmonary valve 4 Tricupid valve and RV free wall 1 Tricuspid valve and RV outflow tract 1 Pulmonary valve alone 2 Bifurcation of pulmonary trunk 1
Total 19
A review of the case records showed that 109 patients had infective endocarditis. Of these, 19 (17.4%) had vegetations on the right side of the heart and also fulfilled at least two of the three criterions of right-sided endocarditis. The site of vegetations in these 19 patients, is shown in Table 1. All patients had fever lasting more than 3 days in the hospital but only 13 patients had a positive blood culture. The six patients with negative blood cultures had underlying heart disease, features of septicaemia, chest pain, breathlessness, tachyp- noea and expectoration: symptoms suggestive of
RV = right ventricular.
septic pulmonary embolism. One of the patients also had haemoptysis.
Eight of the 19 (42.1%) patients had isolated right-sided endocarditis and 11 (57.8%) had un- derlying heart disease. In the group with isolated lesions, there were 2 male and 6 female patients (mean age 21.6 years, range 2-29 years). Details of these patients are given in Table 2. All these patients presented with severe septicaemia. Sep- sis, either during puerperium after home delivery
TABLE 2
Patients with right-sided endocarditis without underlying heart disease.
Case
1
Sex
M
Age (years)
29
Predisposing condition
Epididymoorchitis
Vegetation site
Tricuspid
Blood culture
Organism
Streptococcus
Outcome
Improved valve kidans
2 F 29 Puerperal sepsis Tricuspid Staphylococcus valve aureu.5
3 F 25 Septic abortion
4 F 31 Puerperal sepsis
5 F 28 Puerperal sepsis
Tricuspid Escherichia valve coli
Tricuspid Staphylococcus valve aureus
Tricuspid Staphylococcus valve aureus
6 M 2 Bronchopneu- Tricuspid Staphylococcus
Died Pulmonary embolism
Improved
Improved
Died Uncontrolled septicemia
Died monia and PV aureus Uncontrolled
septicemia F 7 Bronchopneu- Tricuspid Staphylococcus Died
monia valve aureus Uncontrolled CHF
F 28 Puerperal sepsis Tricuspid Staphylococcus Improved valve aureus
PV = pulmonary valve; CHF = congestive heart failure.

by unqualified persons or following induced sep- tic abortion, was the commonest cause (5 out of 6 female patients). Three patients had clinical fea- tures of congestive heart failure and tricuspid regurgitation. One (case 6) had tricuspid and pulmonary regurgitation. One patient (case 3) had haemoptysis. Two patients (case 6 and 7) had pneumatoceles in the chest X-ray. Although all 8 patients had involvement of tricuspid valve, mur- mur of tricuspid regurgitation was not audible in four. All patients received antibiotics depending upon the sensitivity report. Cloxacillin and gen- tamicin were given to most patients. Two patients also received rifampicin. Three patients (cases 5, 6 and 7) did not respond to treatment and died within one week of admission because of uncon- trolled septicaemia and worsening cardiac haemodynamics. Five patients showed clinical im- provement, one of them (case 2) later developed
TABLE 3
Patients with right-sided endocarditis and underlying heart disease.
massive pulmonary embolism and died. The other four survived and were discharged from the hos- pital after six weeks of therapy. No surgical inter- vention was undertaken in any of the patients. On follow-up (8 to 24 months later) the 4 sur- vivors have remained asymptomatic, although 3 patients were found to have an audible murmer of tricuspid regurgitation.
There were eleven patients (57.8%) with right-sided infective endocarditis and underlying heart disease. All of them had underlying congen- ital heart disease and none of them had rheumatic valvular involvement (Table 3). There were 8 males and 3 females (mean age 16.6 years, range 7-38 years). In eight patients no predisposing factors could be found. In one case (case 9, infective endocarditis followed surgery for total correction of tetralogy of Fallot. In another, a 32-year-old woman (case 81, it followed balloon
Case Age (years)
Sex Lesion Site of
vegetation
Blood culture
Organism Outcome
1 22
2 7
3 38
M
M
F
VSD + AR
PS+TR
PAD
4 14 M VSD
5 15 M Operated
TOF
6 9
7 19
8 32
M
F
F
9
10
11
13 M
M
M
VSD
Eisenmenger
WSD) PS after
balloon
valvuloplasty
PAD
6 VSD
8 VSD
TV
TV
Bifurcation
of PA
TV, PV
TV, RVOF
TV, RV free wall
TV
PV
PV
TV, PV
TV, PV
Sterile
Sterile
Strepfo- cocclls viridans
Strepto- COCCUS
Lliridans Staphylo-
coccus aureus
Sterile
Sterile
Sterile
Sterile
Staphylo- coccus aweus
Staphylo- coccus aurew
Died
Myocardial abscess
Improved
Improved
Duct closure
VSD closure
after therapy
Died
Uncontrolled
septicemia
Improved
Died
Brain abscess
Improved *
Improved
Duct closure
Died
Septicaemia Improved
TV = tricuspid valve; PV = pulmonary valve; RVOF = right ventricle outflow tract; VSD = ventricular septal defect; AR = aortic
regurgitation; PS = pulmonary stenosis; PAD = patent arterial duct; TOF = tetralogy of Fallot. * Kalra et al. [6].

87
valvoplasty for pulmonary stenosis [6]. One pa- tient with patency of the arterial duct (case 3) had undergone dental extraction without ade- quate antibiotic cover. Blood cultures yielded Staphylococcus aureus in 3 patients and Strepto- coccus uiridans in 2 patients. Blood cultures were sterile in the remaining 6 patients, all of whom had received some form of antibiotic therapy before reaching our hospital. The 5 patients with positive blood culture received antibiotics to which the organisms found in blood culture were sensitive. Three received cloxacillin and gentam- icin parenterally and two received cephalexin and gentamicin. The six culture negative patients re- ceived empirical therapy with intravenous cloxacillin and gentamicin and meteronidazole in adequate doses. Antibiotics were administered for six weeks in survivors. Four patients who were in congestive heart failure also received diuretics. Seven patients responded to treatment and recov- ered. The remaining four died. Three patients (cases 1, 5 and 10) died because of increasing heart failure and uncontrolled septicaemia. In one case (case 11, autopsy later revealed myocar- dial abscesses. One patient with Eisenmenger syndrome (case 7) developed brain abscess and died despite surgical drainage of abscess. Three of the survivors (two with patency of the arterial duct and one with ventricular septal defect) were operated subsequently for the underlying cardiac lesion (Table 3).
Discussion
The recent increase in the incidence of right- sided endocarditis in the developed countries has been attributed largely to the growing problem of ‘intravenous mainliners’ [1,2,71. Sheikh et al. [71, reported 10 cases of right-sided infective endo- carditis; all of these were drug addicts. Robbins et al. [2] described 21 cases, out of which 18 gave history of drug abuse. Although drug addiction is not as great a problem in third world countries, right-sided infective endocarditis is often seen in these countries [3,8,9]. From Singapore, Chia et al. [8], have reported 8 cases of right-sided infec- tive endocarditis out of a total of 78 cases of infective endocarditis. All 8 had underlying con-
genital heart disease. None were drug addicts. Dental extraction, without antibiotic prophylaxis, was the predisposing factor in 3 cases [8].
Our study highlights some important differ- ences from the western experience. It is believed that, in non-drug addicts, tricuspid valvular endo- carditis occurs usually in the presence of underly- ing heart disease; left-to-right shunts being the commonest [l]. In our series, isolated right-sided infective endocarditis was observed in 8 out of 19 (42.1%). All the eight had tricuspid valvular vege- tations and two had vegetations on the pul- monary valve as well. Puerperal sepsis and septi- caemia following induced abortion by unqualified persons were the commonest underlying causes. None were drug addicts. This is consistent with our earlier report where puerperal sepsis was the underlying cause in 5 out 7 females with isolated right-sided infective endocarditis [31. Lack of asepsis during home delivery and abortion by unqualified persons, a fairly common practice in rural India, may lead to septicaemia [lo]. The absence of clinical signs of tricuspid regurgitation in 4 out of 8 cases of isolated endocarditis is in agreement with our previous experience and em- phasises the importance of high degree of suspi- cion required for the diagnosis of such cases.
Therefore, we recommend that women present- ing with septicaemia following an abortion or a delivery should be screened echocardiographi- tally to exclude tricuspid valvular endocarditis even if there are no cardiac signs. This indication is heightened if pulmonary shadows are seen sug- gesting ‘bronchopneumonia’. As a result of avail- ability of cross-sectional echocardiography, and heightened clinical awareness, more patients can be diagnosed. This report presents the largest clinical series on right-sided endocarditis from India. Since our study was retrospective, it is likely that we might have missed vegetations on the right side of the heart in some of the patients who were found to have left-sided lesions.
Although rheumatic heart disease is one of the commonest causes of hospital admission in India, and the tricuspid valve is involved in about 30% cases [ll], none of our patients with right-sided infective endocarditis had rheumatic heart dis- ease. In an autopsy series, we have reported that

88
involvement of mitral and aortic valves by infec- tive endocarditis, with underlying valvular heart disease, occurred in 19.8% and 8.1% respectively, as compared to only 2.3% of cases involving the tricuspid valve [9]. The reason why the tricuspid valve is spared by infective endocarditis remains unclear.
Our experience in patients with underlying congenital heart disease is similar to that of Chia et al. [8]. Vegetations on the tricuspid valve, however, were much more common in this series (8 out of 11 cases) as compared to their patients (one out of eight). Pulmonary arterial vegetations, considered to be a rarity [12], were seen in one patient with patency of the arterial duct.
Staphylococcus aureus was the most common organism in the group of patients with isolated endocarditis. Isolation of coagulase positive staphylococci was associated with high mortality in both groups. Nine patients grew coagulase- positive staphylococci and 6 of them died. The high mortality seen in our patients could have been the result of incomplete treatment received elsewhere, late arrival at hospital, and failure to control septicaemia despite administration of ap- propriate antibiotics.
Balloon valvuloplasty is an accepted therapeu- tic measure for pulmonary stenosis. Infective en- docarditis possibly related to its use was encoun- tered by us in one case [61. We are aware of only one other report following aortic balloon valvulo- plasty [ 131.
In conclusion, cross-sectional echocardiogra- phy has enhanced our ability to diagnose right- sided endocarditis during life. Unlike in the west, most patients with right-sided endocarditis in In- dia are found to be infected by staphylococcal endocarditis following puerperal sepsis or septic induced abortion. Drug addiction as a predispos- ing factor is not seen. Clinical signs may be sub- tle, and a high degree of suspicion is essential for
early diagnosis. Mortality in this condition, often associated with fulminant sepsis caused by Staphylococcus aureus, remains high.
References
Panidis IP, Kotler MN, Mintz GS, Segal BL, Ross JJ. Right heart endocarditis: clinical and echocardiographic features. Am Heart J 1984;107:759-764. Robbins M, Frater R, Soeiro R, Frishman W, Strom J. Influence of vegetation size on clinical outcome of right- sided infective endocarditis. Am J Med 1986;80:165-171. Kohli RS, Anand IS, Sivaram SV, Datta BN, Bidwai PS, Wahi PL. Isolated right-sided endocarditis in uon addicts: a review of 10 cases. Ind Heart J 1982;34:17-20. Gilbert BW, Hartley RS, Crawford F et al. Two dimen- sional echocardiographic assessment of vegetative endo- carditis. Circulation 1977;55:346-353. Stewart JA, Silimperi D, Harris P, Kentwise N, Fraker J, Kiss10 JA. Echocardiographic assessment of vegetative le- sions in infective endocarditis. Circulation 1980;61:374- 380. Kalra GS, Wander GS, Anand IS. Right sided endocardi- tis after balloon dilatation of the pulmonary valve. Br Heart J 1990;63:368-369. Sheikh MU, Ah N, Covarrubias E, Fox LM, Morjaria M, Dejo J. Right-sided endocarditis: an echocardiographic study. Am J Med 1979;66:283-287. Chia BL, Yan PC, Ee BK, Choo MH, Lee CN, Tay MB. Right-sided infective endocarditis: a Singapore experience. Am Heart J 1988;116:568-571.
9 Datta BN, Khattri HN, Bidwai PS et al. Infective endo- carditis at autopsy in Northern India. Jpn Heart J 1982;23:329-337.
10 Park JE, Park K. Preventive medicine in obstetrics, pedi- atrics and geriatrics. In: Park JE, Park K, eds. Textbook of social and preventive medicine. 12th ed. Jabalpur, India: Banarasi Das Publishers, 1989;293-323.
11 Datta BN, Nagrani B, Khattri HN et al. Rheumatic heart disease at autopsy. An analysis of 260 cases. Ind Heart J 1978;30:39-43.
12 Vargas-Barron J, Attie F, Buendia-Hernadez A, Keirns C, Esquinel-Avila J. Echocardiographic recognition of pul- monary artery endarteritis in patent ductus arteriosus. Am Heart J 1985;109:368-370.
13 Cujec B, MC Meekin J, Lopez J. Bacterial endocarditis after percutaneous aortic valvuloplasty. Am Heart J 1988;115:178-179.