Embed Size (px)
Citation preview

Hematology Education: the education program for the annual congress of the European Hematology Association | 2014; 8(1) | 69 |
J.G. Gribben
Barts Cancer Institute,Queen Mary, University of London,UK
Correspondence: John G. GribbenE-mail: [email protected]
Hematology Education:the education program for the annual congress of the EuropeanHematology Association
2014;8:69-74
Prognostic and predictive factors in chronic lymphocyticleukemia
Introduction
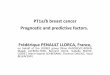
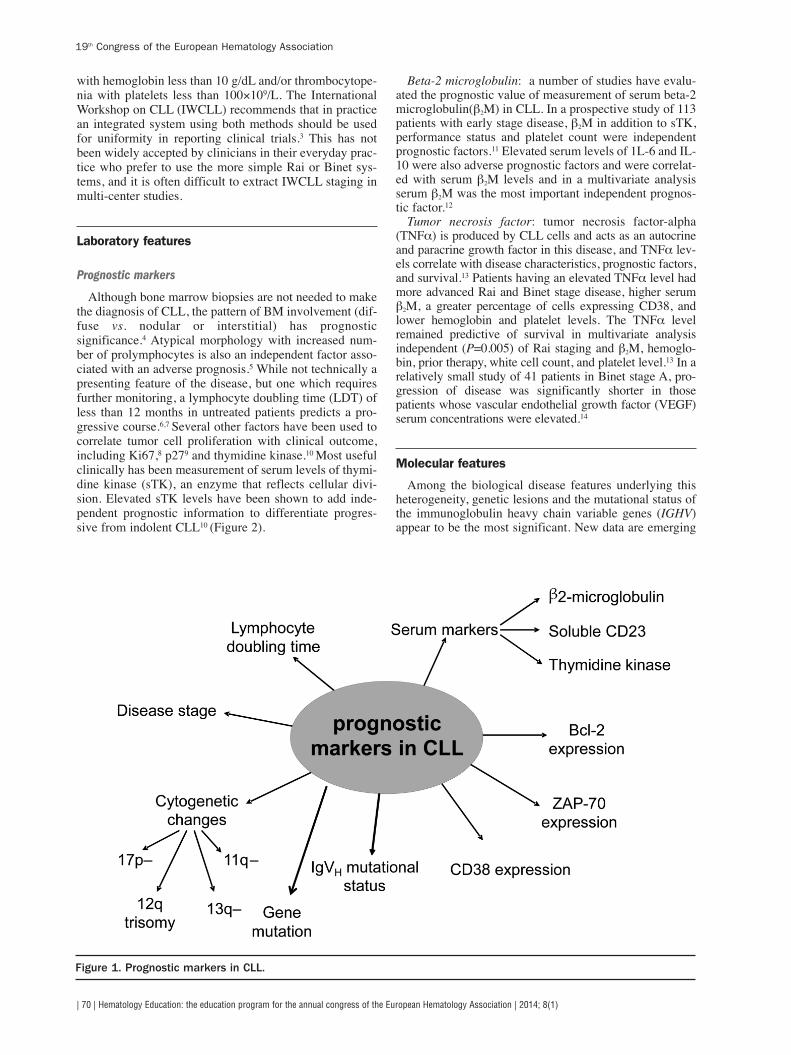
Chronic lymphocytic leukemia (CLL) ischaracterized by a highly variable clinicalcourse. Increasingly patients are being diag-nosed in early stage disease and many of thesepatients will follow a watch and wait approachand never require therapy. Others present witha rapidly progressive clinical course, with ashort time to time to first therapy (TFT), shortprogression free survival (PFS) and overallsurvival (OS). There is, therefore, a need toidentify factors that are predictive of the likelyclinical course. Once patients have progressedto require treatment, subsequent clinical out-comes typically reflect disease aggressiveness,response to first-line therapy, first PFS,response to treatment for relapsed disease andsubsequent remission duration, and these fea-tures all impact OS. A large number of prog-nostic factors, including clinical and laborato-ry features (Figure 1), have been correlatedwith clinical outcomes.
Clinical features with prognostic signifi-cance
Clinical staging of CLL patients is a simpleand effective tool for assessing the prognosisof CLL patients. This system allows patients tobe separated into low-, intermediate- and high-risk groups, with clear differences in estimatedsurvival among the three groups. The twowidely used staging systems that are now inplace are based upon their prognostic implica-tions for survival.1,2 The Rai staging system isbased upon the premise that there is a progres-sive accumulation of neoplastic cells manifest-ed by increasing lymphocytosis, progressivelymphadenopathy, splenomegaly andhepatomegaly, followed by bone marrowreplacement with development of anemia andthrombocytopenia.1 The Binet system takesinto consideration five potential sites ofinvolvement: cervical, axillary and inguinallymph nodes (either unilateral or bilateralcounts as one site), spleen and liver.2 Patientsare staged according to the number ofinvolved sites plus the presence of anemia
Chronic lymphocytic leukemia
Patients with chronic lymphocytic leukemia (CLL) have a very variable clinical course, with somepatients having an extremely indolent course and never requiring therapy, while others have rapidlyprogressive disease, with short time to need for treatment and short survival. The Rai and Binet clinicalstaging systems were the first to classify CLL patients into prognostic categories. Newer prognosticmarkers that correlate with shorter time to progression and treatment include elevated serum beta-2microglobulin (β2M), TK, unmutated IgVH and increased expression of ZAP-70 or CD38, as well as poorrisk cytogenetic changes in CLL cells. In clinical practice, stage and cytogenetics are the most impor-tant prognostic factors as they impact upon when and how to treat patients. The presence of del17p,as well as mutations of TP53, are associated with an aggressive clinical course and short overall sur-vival (OS), and identify a group of patients who need different treatment approaches. Patients withdel17p should be evaluated for novel agents and/or allogeneic stem cell transplantation in first remis-sion. Nearly one-fifth of patients have del11q and these patients benefit from treatment with an alky-lating agent in addition to nucleoside analogs and rituximab. Patients with trisomy 12 and del6q iden-tify intermediate-risk cytogenetic findings, and patients with trisomy 12 may express higher levels ofCD20, thereby making the malignant cells more susceptible to biological agents targeting CD20.Despite advances in stratifying patients and improved treatment regimens, there is little evidence yet,with the exception of patients with del 17p, that different subgroups of patients merit different treat-ment approaches. As we enter the era of personalized medicine, additional research into biomarkersis needed to optimize treatment outcomes for our CLL patients.
Learning goals
At the conclusion of this activity, participants should:- understand the molecular basis of the heterogeneous clinical course in CLL;- understand the clinical use of prognostic factors to help predict the clinical course of CLL;- begin to understand how these prognostic factors might be used to optimize treatment choices in CLL.
A B S T R A C T
with hemoglobin less than 10 g/dL and/or thrombocytope-nia with platelets less than 100¥109/L. The InternationalWorkshop on CLL (IWCLL) recommends that in practicean integrated system using both methods should be usedfor uniformity in reporting clinical trials.3 This has notbeen widely accepted by clinicians in their everyday prac-tice who prefer to use the more simple Rai or Binet sys-tems, and it is often difficult to extract IWCLL staging inmulti-center studies.
Laboratory features
Prognostic markers
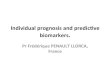
Although bone marrow biopsies are not needed to makethe diagnosis of CLL, the pattern of BM involvement (dif-fuse vs. nodular or interstitial) has prognosticsignificance.4 Atypical morphology with increased num-ber of prolymphocytes is also an independent factor asso-ciated with an adverse prognosis.5 While not technically apresenting feature of the disease, but one which requiresfurther monitoring, a lymphocyte doubling time (LDT) ofless than 12 months in untreated patients predicts a pro-gressive course.6,7 Several other factors have been used tocorrelate tumor cell proliferation with clinical outcome,including Ki67,8 p279 and thymidine kinase.10 Most usefulclinically has been measurement of serum levels of thymi-dine kinase (sTK), an enzyme that reflects cellular divi-sion. Elevated sTK levels have been shown to add inde-pendent prognostic information to differentiate progres-sive from indolent CLL10 (Figure 2).
Beta-2 microglobulin: a number of studies have evalu-ated the prognostic value of measurement of serum beta-2microglobulin(β2M) in CLL. In a prospective study of 113patients with early stage disease, β2M in addition to sTK,performance status and platelet count were independentprognostic factors.11 Elevated serum levels of 1L-6 and IL-10 were also adverse prognostic factors and were correlat-ed with serum β2M levels and in a multivariate analysisserum β2M was the most important independent prognos-tic factor.12
Tumor necrosis factor: tumor necrosis factor-alpha(TNFa) is produced by CLL cells and acts as an autocrineand paracrine growth factor in this disease, and TNFa lev-els correlate with disease characteristics, prognostic factors,and survival.13 Patients having an elevated TNFa level hadmore advanced Rai and Binet stage disease, higher serumβ2M, a greater percentage of cells expressing CD38, andlower hemoglobin and platelet levels. The TNFa levelremained predictive of survival in multivariate analysisindependent (P=0.005) of Rai staging and β2M, hemoglo-bin, prior therapy, white cell count, and platelet level.13 In arelatively small study of 41 patients in Binet stage A, pro-gression of disease was significantly shorter in thosepatients whose vascular endothelial growth factor (VEGF)serum concentrations were elevated.14
Molecular features
Among the biological disease features underlying thisheterogeneity, genetic lesions and the mutational status ofthe immunoglobulin heavy chain variable genes (IGHV)appear to be the most significant. New data are emerging
| 70 | Hematology Education: the education program for the annual congress of the European Hematology Association | 2014; 8(1)
19th Congress of the European Hematology Association
Figure 1. Prognostic markers in CLL.

from next generation sequencing (NGS) studies, regardingthe prognostic significance of novel mutations recentlyidentified in this disease.
CLL can be divided into two subgroups based upon thepresence or absence of somatic hypermutation of theIGHV genes,15 and this finding has prognostic signifi-cance.16,17 Unmutated IGHV is associated with high�riskcharacteristics and shorter survival. This initially led to thehypothesis that there are two subsets of B-cell CLL, basedupon different cells of origin. However, gene expressionprofiling studies from 2 independent analyses has demon-strated that both subtypes of CLL display a common anddistinct gene expression profile, suggesting that bothgroups share a common mechanism of transformation.18,19
These findings are not in keeping with two distinct diseaseentities arising from different cells of origin and CLLappears most likely derived from pre and post germinalCD5+ B cells.20 It is technically challenging for routinelaboratories to characterize IGHV mutational status andtherefore attempts have been made to identify surrogatemarkers for this.
Gene profiling studies identified a restricted number ofgenes that are capable of distinguishing IgVH mutatedversus unmutated cases.18,19 Most attention has focused onexpression of ZAP70, which is expressed at higher levelsin unmutated than in mutated cases.21 Higher levels ofZAP70 expression were associated with more rapid clini-cal progression.22,23 There is a high, but incomplete overlapbetween ZAP70 expression and IGHV mutational status.In addition, ZAP70 expression in CLL cells is not simplya case of presence or absence but of variable expressionamong patients, and therefore an arbitrary cut-off pointmust be made to define cases as positive or negative. ZAP-
70 testing is based on flow cytometric identification ofCD19+/CD5+ positive cells that also express ZAP-70, andthis has led to significant inter-laboratory variation.Despite technical challenges, results from a number ofstudies lead to the conclusion that cases of ZAP-70 posi-tive CLL (usually >20% of CD19+/CD5+cells positive forZAP-70) progress substantially faster than ZAP-70 nega-tive cases. High ZAP-70 expression appears to be astronger predictor of initial CLL disease progression thaneither IgVH unmutated CLL23 or CD38+ CLL.24 If reliableZAP-70 testing can be guaranteed by a commercial labo-ratory, then ZAP-70 testing is one of the best tests toobtain at disease presentation. The value of ZAP-70 test-ing in relapsed patients or previously untreated patientsthat are years out from diagnosis and that have not pro-gressed remains undefined.
Higher levels of expression of CD38 are associated withunmutated IgVH genes.16 In multivariate analysis, highlevels of expression of CD38 on CLL cells were associat-ed with more rapid progression of disease and poorresponse to therapy.25,26 However, there can be discor-dance between IgVH status and CD38 expression, whichmay be partly explained by the finding that the level ofexpression of CD38 may vary over time.27
A multivariate analysis examined the prognostic signif-icance of genetic abnormalities (detected at or shortlyafter presentation), clinical stage, lymphocyte morpholo-gy, CD38 expression, and IGVH gene status in 205patients with CLL.28 Deletion of chromosome 11q23,absence of a deletion of chromosome 13q14, atypicallymphocyte morphology, and more than 30% CD38expression were significantly associated with the pres-ence of unmutated IgV genes. Advanced stage, male sex,
Hematology Education: the education program for the annual congress of the European Hematology Association | 2014; 8(1) | 71 |
Milan, Italy, June 12-15, 2014
Figure 2. Prognostic markers at time of first treatment.

atypical morphology, more than 30% CD38 expression,trisomy 12, deletion of chromosome 11q23, loss or muta-tion of the p53 gene, and unmutated IgVH genes were allpoor prognostic factors in the univariate analysis in thisstudy. However, IgVH gene mutational status, loss ormutation of the p53 gene, and clinical stage retainedprognostic significance in a multivariate analysis.28 Asubsequent study assessed the relative strength of desig-nating a case as positive for IGVH mutation, CD38 orZAP-70 in a test cohort of 307 patients and used thesedata-defined criteria to stratify patients in an independentcohort of 705 patients.24 Multivariable analysis revealedthat ZAP-70 was the strongest risk factor and knowledgeof the IGVH mutation status or CD38 did not improve ourability to predict the time to first treatment except forZAP-70-negative cases, which could be segregated into 2groups of intermediate-risk or low-risk disease based onwhether they expressed unmutated or mutated IGHV.ZAP-70 maintained its high relative prognostic value forthe subset of patients with early stage, asymptomatic dis-ease, including patients evaluated within one year ofdiagnosis. Although it remains premature to recommendtherapy based on these risk factors, it was suggested thatpatients with ZAP-70-positive CLL cells should be mon-itored closely for disease progression as they have amedian time from diagnosis to requiring initial therapy bystandard criteria of only approximately three years.
Cytogenetics and fluorescence in situ hybridization
While conventional cytogenetic analyses detected chro-mosome aberrations in only 40% of cases, the use of fluo-rescence in situ hybridization (FISH) has greatly enhancedour ability to detect chromosomal abnormalities in CLL.In the definitive study of the utility of FISH in CLL, chro-mosomal abnormalities were detected in 268 of 325 (82%)CLL patients studied.29 Dohner and colleagues convinc-ingly demonstrated that genomic aberrations in CLL arelikely the most important independent predictors of dis-ease progression and survival. The most frequent changesobserved were deletion in 13q(del13q), with deletions at13q14 occurring in more than 50% of cases. The next mostcommon abnormality of deletion is 11q (del11q), withdeletions at 11q22-23 occurring in up to 20% of CLLcases. These deletions are associated with patients with adistinct clinical presentation including younger age, malegender, extensive adenopathy and poor prognosis.30
Trisomy 12 (+12) occurs in up to 20% of cases of CLL butthe molecular mechanism by which this genetic abnormal-ity contributes to leukemogenesis is unknown. Deletion in17p(del17p) occurs in only approximately 5-10% ofpatients who have progressed to require treatment, but isassociated with rapid progression of disease, poorresponse to therapy and short survival.29,31 The FISH find-ings led to establishment of a hierarchical model of theirprognostic impact29 that defines 5 subgroups with increas-ingly poor prognosis: del 13q as the sole abnormality(median survival 133 months), +12 (median survival 114months), normal karyotype (median survival 111 months),del 11q (median survival 79 months) and del 17p (mediansurvival 32 months). Patients in the 17p- and 11q-deletiongroups had more advanced disease than those in the other3 groups. Patients with 17p deletions had the shortest
median treatment-free interval (9 months), and those with13q deletions had the longest (92 months). The poor out-come of CLL with del 17p is due to inactivation of thetumor suppressor TP53, and sole mutation of TP53(TP53mut) has also been associated with inferiorsurvival.32 Ongoing studies are assessing the impact ofspecific cytogenetic abnormalities on response to particu-lar therapeutic approaches. However, the presence of 17pdeletion predicts for treatment failure with alkylatingagents and fludarabine and short survival times. In multi-variate analysis, 11q and 17p deletions provided independ-ent adverse prognostic information and these findingshave implications for the design of risk-adapted treatmentstrategies.33 Importantly, early stage patients with del17pshould be observed and can sometimes have a more indo-lent course.
Novel gene mutations
Novel gene mutations have been identified in CLL bynext generation sequencing (NGS). Recent studies havedemonstrated substantial differences in genomic alterationsbetween mutated and unmutated IGHV subgroups, andamong distinct cytogenetic subgroups. This likely reflectsdistinct molecular pathways and mutagenic mechanisms inCLL pathogenesis. NGS has demonstrated that this is char-acterized by a relatively low number of somatic mutationsper case, with relatively few recurrent novel mutationsobserved at moderate frequency (5-15%) but with a largernumber of recurrent low frequency somatic mutations.Mutations of NOTCH1 and SF3B1 are among the most fre-quent and are detected in 5-20% of patients.34-37 Mutationsof NOTCH1 have been found associated with trisomy 12and unmutated IGHV. Mutations in SF3B1 affect the splic-ing machinery, representing a novel pathogenic mechanismin CLL. These mutations are correlated with 11q- as wellas unmutated IGHV. In initial studies, both mutations havebeen associated with advanced disease and poorprognosis.34-39 NGS technology allows us to detect novelmutations and this has expanded our knowledge of thegenomic alterations in CLL. But this technique also pro-vides a new tool for analyzing leukemic clonal architectureand to examine clonal heterogeneity, which is striking inCLL. NGS studies of CLL are expanding our fundamentalknowledge on the molecular mechanisms involved in thepathogenesis of the disease and will offer new perspectivesfor the clinical management of the patients, particularlywhen used in combination with novel agents as we movetowards an era of personalized medicine.
Biomarkers in clinical use
Although there is a wealth of clinical and laboratoryparameters identifying subgroups of patients with CLLwith different clinical course, none of these markers iden-tify when we should treat and few of these markers direct-ly influence therapy. Indeed, only the detection of del17por TP53 mutations have entered routine clinical practice toalter treatment decisions.40 There is also a paucity of dataon whether specific parameters fulfill strict criteria forbiomarkers that influence treatment decision-makingprocesses. It is also unclear to what extent addition ofmolecular biomarkers adds to clinical data. Complex
| 72 | Hematology Education: the education program for the annual congress of the European Hematology Association | 2014; 8(1)
19th Congress of the European Hematology Association

nomograms have been developed that can help to deter-mine time to first treatment in CLL patients.41,42 To date,these algorithms have been assessed only in single centerpopulations and have not been evaluated in any prospec-tive studies. Ongoing studies are assessing the impact of alarge number of biomarkers on outcome after first andsubsequent treatments, and will require large numbers ofpatient to assess their impact on multivariate analyses
Conclusions
Recommendations for obtaining biomarkers in CLL in 2014
Prognostic factors useful at diagnosis are shown inTable 1. The aim is to provide prognostic information andestimate time to need for first treatment. This mightimpact upon proposed frequency of monitoring in the clin-ic. The factors assessed are clinical factors and biochemi-cal markers (most commonly β2M and TK). Flow cytome-try is required for diagnosis and this usually includesCD38. ZAP70 may be available in some centers, butresults should be used with caution unless the assay hasbeen well validated. FISH provides valuable informationand is vital in research studies and for studies of clonalevolution of disease. In my experience, patients requestthe test hoping that they have isolated del13q. The findingof poor prognosis markers may increase anxiety, yet notimpact on therapy. If cost is a factor, then FISH is morevaluable at time for next treatment and is not vital at diag-nosis. NGS remains a research tool only.
Factors useful at time of first treatment are shown inTable 2. Clinical stage and biochemical markers are usefulprognostic markers. FISH must be repeated as this is not astable marker over time and there can be clonal evolutionfrom time of diagnosis to time of need for treatment. FISHand TP53 mutation analysis are important to identify thosepatients who should not be offered conventionalchemotherapy and to identify patients who will be candi-dates for novel agents, and/or stem cell transplantation.Patients with del 11q are candidates for fludarabine+
cyclophosphamide+rituximab (FCR) therapy and appearto benefit most from the addition of alkylating agent andanti-CD20 monoclonal to purine analog based therapy.Other markers that are predictive of time to first treatmentare not yet informative with regards to guiding treatmentdecisions. Detection of patients with NOTCH1 mutationsmay identify a subset of patients who have no clear benefitof chemoimmunotherapy and this might be recommendedin the near future, but this remains a research study only. Novel treatments
Novel treatment approaches such as ibrutinib and idelal-isib may be able to overcome many of the poor prognosticfactors such as IgVH mutational status, del 17p and del11q, although the follow up on clinical studies remainsshort and there is a suggestion that relapses are occurringmore quickly in patients with del 17p.
Summary
There are a plethora of prognostic markers available,many of which have been shown to have prognostic sig-nificance often only in univariate analyses, although somecombinations have been assessed also in multivariateanalyses. Performing all potential biomarkers at diagnosiscan lead to conflicting results and clinical stage is the fac-tor that changes time to treatment. Once treatment is indi-cated, the most important factor currently is identificationof patients with dysfunctional TP53, and patients withdel17p and TP53 mutations should be offered alternativetherapy and considered for stem cell transplantation, ifsuitable, in first remission. The frequency of detection ofdel 17p and TP53 mutation increases with subsequentrelapse and analysis is vital at time of each subsequenttreatment. The treatment algorithm is CLL will likelychange in the near future with the availability of a numberof novel agents, which may alter the impact of many of theknown prognostic markers. Novel mutations that havebeen identified by NGS are still under investigation andthis technology remains a research tool only.
Hematology Education: the education program for the annual congress of the European Hematology Association | 2014; 8(1) | 73 |
Milan, Italy, June 12-15, 2014
Table 1. Prognostic factors useful at diagnosis.
Factor At diagnosis Available with Research interest and follow up only useful when available
Clinical stage Treat patients with advanced stage disease.
FISH Does not impact when to treat. Argument could be made to reserve this until time to need for treatment.
Biochemical markers β2M, TK prognostic, but do not impact when to treat.
CD38 Likely included in CLL diagnostic panel by flow.
IgVH Research tool only. Available in selected centers, but useful where available.
ZAP70 May be available in some centers. Use with caution if assay not well validated.
Lymphocyte doubling time May be used as an indication when to treat.
Next generation sequencing Research tool only.
References1. Rai KR, Sawitsky A, Cronkite EP, Chanana AD, Levy RN,
Pasternack BS. Clinical staging of chronic lymphocyticleukemia. Blood. 1975;46:219-34.
2. Binet JL, Auquier A, Dighiero G, Chastang C, Piguet H,Goasguen J, et al. A new prognostic classification of chroniclymphocytic leukemia derived from a multivariate survivalanalysis. Cancer. 1981;48:198-206.
3. Chronic lymphocytic leukaemia: proposals for a revised prog-nostic staging system. Report from the International Workshopon CLL. Br J Haematol. 1981;48:365-7.
4. Rozman C, Montserrat E, Rodriguez-Fernandez JM, Ayats R,Vallespi T, Parody R, et al. Bone marrow histologic pattern—the best single prognostic parameter in chronic lymphocyticleukemia: a multivariate survival analysis of 329 cases. Blood.1984;64:642-8.
5. Oscier DG, Matutes E, Copplestone A, Pickering RM,Chapman R, Gillingham R, et al. Atypical lymphocyte mor-phology: an adverse prognostic factor for disease progressionin stage A CLL independent of trisomy 12. Br J Haematol.1997;98(4):934-9.
6. Montserrat E, Sanchez-Bisono J, Vinolas N, Rozman C.Lymphocyte doubling time in chronic lymphocytic leukaemia:analysis of its prognostic significance. Br J Haematol.1986;62:567-75.
7. Molica S, Alberti A. Prognostic value of the lymphocyte dou-bling time in chronic lymphocytic leukemia. Cancer.1987;60:2712-7.
8. Cordone I, Matutes E, Catovsky D. Monoclonal antibody Ki-67 identifies B and T cells in cycle in chronic lymphocyticleukemia: correlation with disease activity. Leukemia.1992;6(9):902-6.
9. Vrhovac R, Delmer A, Tang R, Marie JP, Zittoun R,Ajchenbaum-Cymbalista F. Prognostic significance of the cellcycle inhibitor p27Kip1 in chronic B-cell lymphocyticleukemia. Blood. 1998;91(12):4694-700.
10. Hallek M, Langenmayer I, Nerl C, Knauf W, Dietzfelbinger H,Adorf D, et al. Elevated serum thymidine kinase levels identi-fy a subgroup at high risk of disease progression in early, non-smoldering chronic lymphocytic leukemia. Blood.1999;93(5):1732-7.
11. Hallek M, Wanders L, Ostwald M, Busch R, Senekowitsch R,Stern S, et al. Serum beta(2)-microglobulin and serum thymi-dine kinase are independent predictors of progression-free sur-vival in chronic lymphocytic leukemia and immunocytoma.Leuk Lymphoma. 1996;22(5-6):439-47.
12. Fayad L, Keating MJ, Reuben JM, O’Brien S, Lee BN, LernerS, et al. Interleukin-6 and interleukin-10 levels in chronic lym-phocytic leukemia: correlation with phenotypic characteristicsand outcome. Blood. 2001;97(1):256-63.
13. Ferrajoli A, Keating MJ, Manshouri T, Giles FJ, Dey A, EstrovZ, et al. The clinical significance of tumor necrosis factor-alpha plasma level in patients having chronic lymphocyticleukemia. Blood. 2002;100 (4):1215-9.
14. Molica S, Vitelli G, Levato D, Gandolfo GM, Liso V.Increased serum levels of vascular endothelial growth factorpredict risk of progression in early B-cell chronic lymphocyticleukaemia. Br J Haematol. 1999;107 (3):605-10.
15. Fais F, Ghiotto F, Hashimoto S, Sellars B, Valetto A, Allen SL,et al. Chronic lymphocytic leukemia B cells express restrictedsets of mutated and unmutated antigen receptors. J Clin Invest.1998;102(8):1515-25.
16. Damle RN, Wasil T, Fais F, Ghiotto F, Valetto A, Allen SL, etal. Ig V gene mutation status and CD38 expression as novelprognostic indicators in chronic lymphocytic leukemia. Blood.1999;94(6):1840-7.
17. Hamblin TJ, Davis Z, Gardiner A, Oscier DG, Stevenson FK.Unmutated Ig V(H) genes are associated with a more aggres-sive form of chronic lymphocytic leukemia. Blood.1999;94(6):1848-54.
18. Klein U, Tu Y, Stolovitzky GA, Mattioli M, Cattoretti G,Husson H, et al. Gene expression profiling of B cell chroniclymphocytic leukemia reveals a homogeneous phenotyperelated to memory B cells. J Exp Med. 2001;194(11):1625-38.
19. Rosenwald A, Alizadeh AA, Widhopf G, Simon R, Davis RE,Yu X, et al. Relation of gene expression phenotype toimmunoglobulin mutation genotype in B cell chronic lympho-cytic leukemia. J Exp Med. 2001;194(11):1639-47.
20. Seifert M, Sellmann L, Bloehdorn J, Wein F, Stilgenbauer S,Durig J, et al. Cellular origin and pathophysiology of chroniclymphocytic leukemia. J Exp Med. 2012;209(12):2183-98.
21. Chen L, Widhopf G, Huynh L, Rassenti L, Rai KR, Weiss A,
et al. Expression of ZAP-70 is associated with increased B-cell receptor signaling in chronic lymphocytic leukemia.Blood. 2002;100(13):4609-14.
22. Orchard JA, Ibbotson RE, Davis Z, Wiestner A, Rosenwald A,Thomas PW, et al. ZAP-70 expression and prognosis in chron-ic lymphocytic leukaemia. Lancet. 2004;363(9403):105-11.
23. Rassenti LZ, Huynh L, Toy TL, Chen L, Keating MJ, GribbenJG, et al. ZAP-70 compared with immunoglobulin heavy-chain gene mutation status as a predictor of disease progres-sion in chronic lymphocytic leukemia. N Engl J Med.2004;351(9):893-901.
24. Rassenti LZ, Jain S, Keating MJ, Wierda WG, Grever MR,Byrd JC, et al. Relative value of ZAP-70, CD38, andimmunoglobulin mutation status in predicting aggressive dis-ease in chronic lymphocytic leukemia. Blood.2008;112(5):1923-30.
25. Del Poeta G, Maurillo L, Venditti A, Buccisano F, EpicenoAM, Capelli G, et al. Clinical significance of CD38 expressionin chronic lymphocytic leukemia. Blood. 2001;98(9):2633-9.
26. Ibrahim S, Keating M, Do KA, O’Brien S, Huh YO, Jilani I,et al. CD38 expression as an important prognostic factor in B-cell chronic lymphocytic leukemia. Blood. 2001;98(1):181-6.
27. Hamblin TJ, Orchard JA, Gardiner A, Oscier DG, Davis Z,Stevenson FK. Immunoglobulin V genes and CD38 expres-sion in CLL. Blood. 2000;95(7):2455-7.
28. Oscier DG, Gardiner AC, Mould SJ, Glide S, Davis ZA,Ibbotson RE, et al. Multivariate analysis of prognostic factorsin CLL: clinical stage, IGVH gene mutational status, and lossor mutation of the p53 gene are independent prognostic fac-tors. Blood. 2002;100(4): 1177-84.
29. Dohner H, Stilgenbauer S, Benner A, Leupolt E, Krober A,Bullinger L, et al. Genomic aberrations and survival in chroniclymphocytic leukemia. N Engl J Med. 2000;343(26):1910-6.
30. Dohner H, Stilgenbauer S, James MR, Benner A, Weilguni T,Bentz M, et al. 11q deletions identify a new subset of B-cellchronic lymphocytic leukemia characterized by extensivenodal involvement and inferior prognosis. Blood.1997;89(7):2516-22.
31. Dohner H, Fischer K, Bentz M, Hansen K, Benner A, CabotG, et al. p53 gene deletion predicts for poor survival and non-response to therapy with purine analogs in chronic B-cellleukemias. Blood. 1995;85(6):1580-9.
32. Zenz T, Eichhorst B, Busch R, Denzel T, Habe S, Winkler D,et al. TP53 mutation and survival in chronic lymphocyticleukemia. J Clin Oncol. 2010;28(29): 4473-9.
33. Stilgenbauer S, Bullinger L, Lichter P, Dohner H. Genetics ofchronic lymphocytic leukemia: genomic aberrations and V(H)gene mutation status in pathogenesis and clinical course.Leukemia. 2002;16(6): 993-1007.
34. Puente XS, Pinyol M, Quesada V, Conde L, Ordonez GR,Villamor N, et al. Whole-genome sequencing identifies recur-rent mutations in chronic lymphocytic leukaemia. Nature.2011;475(7354):101-5.
35. Fabbri G, Rasi S, Rossi D, Trifonov V, Khiabanian H, Ma J, etal. Analysis of the chronic lymphocytic leukemia codinggenome: role of NOTCH1 mutational activation. J Exp Med.2011;208(7):1389-401.
36. Quesada V, Conde L, Villamor N, Ordonez GR, Jares P,Bassaganyas L, et al. Exome sequencing identifies recurrentmutations of the splicing factor SF3B1 gene in chronic lym-phocytic leukemia. Nat Genet. 2012;44(1):47-52.
37. Wang L, Lawrence MS, Wan Y, Stojanov P, Sougnez C,Stevenson K, et al. SF3B1 and other novel cancer genes inchronic lymphocytic leukemia. N Engl J Med.2011;365(26):2497-506.
38. Rossi D, Bruscaggin A, Spina V, Rasi S, Khiabanian H,Messina M, et al. Mutations of the SF3B1 splicing factor inchronic lymphocytic leukemia: association with progressionand fludarabine-refractoriness. Blood. 2011;118(26):6904-8.
39. Rossi D, Rasi S, Fabbri G, Spina V, Fangazio M, Forconi F, etal. Mutations of NOTCH1 are an independent predictor of sur-vival in chronic lymphocytic leukemia. Blood.2012;119(2):521-9.
40. Zenz T, Mertens D, Kuppers R, Dohner H, Stilgenbauer S.From pathogenesis to treatment of chronic lymphocyticleukaemia. Nat Rev Cancer. 2010;10(1):37-50.
41. Wierda WG, O’Brien S, Wang X, Faderl S, Ferrajoli A, DoKA, et al. Prognostic nomogram and index for overall survivalin previously untreated patients with chronic lymphocyticleukemia. Blood. 2007;109(11): 4679-85.
42. Wierda WG, O’Brien S, Wang XM, Faderl S, Ferrajoli A, DoKA, et al. Multivariable Model for Time to First Treatment inPatients With Chronic Lymphocytic Leukemia. J Clin Oncol.2011;29(31):4088-95.
| 74 | Hematology Education: the education program for the annual congress of the European Hematology Association | 2014; 8(1)
19th Congress of the European Hematology Association