Embed Size (px)
Citation preview

Prognostic Factors in Hairy Cell Leukemia
(Leukemic Reticuloendotheliosis)
DAVID J. STEWART, MD,' TERRY L. SMITH, BSc,t MICHAEL J. KEATING, MBBS,' KENNETH B. McCREDIE, MBBCH,' EVAN M. HERSH, MD,' JORGE QUESADA, MD,'
AND EMlL J. FREIREICH, MD'
Prognostic factors were examined in 31 patients with hairy cell leukemia seen at M. D. Anderson Hospital. Long survival from presentation was significantly associated with ease of aspiration of iliac crest bone marrow, absence of major infection, hemoglobin >10 g/dl, and absence of a prior history of pneumonia. Long survival from splenectomy was associated most closely with absence of a prediagnosis history of pneumonia, suggesting that a long-standing host defense abnormality may exist that is not corrected by splenectomy. Generally, patients with sustained improvement in hematologic parameters postsplenectomy lived longest from splenectomy, although the results were not statistically significant.
Cuneer 53:1198-1201, 1984.
AIRY CELL LEUKEMIA is a disease characterized by H a variable course. While one third of patients may have a relatively good prognosis with survival for 2 3 years, the majority of patients have a less favorable course with bone marrow failure that results in death from in- fection within 1 month to 2 years after diagnosis.' Sple- nectomy remains the initial treatment of choice and will not uncommonly result in improvement in hemoglobin, and platelet count, and to a lesser extent, granulocyte count.2 Controversy exists as to the preferred treatment of hairy cell leukemia once bone marrow failure develops in the postsplenectomy ~ e r i b d . ' . ~ , ~ . ~ In addition, it is very difficult to decide at what point treatment should begin. Intensive chemotherapy may result in prolonged remis- s i o n ~ , ~ . ~ . ~ but the patients are at high risk of life-threatening infection in the immediate posttreatment period,' and, alternatively, some patients will survive for a prolonged period of time without treatment despite the onset of bone marrow failure.
In an attempt to facilitate the decision of which patients with hairy cell leukemia should undergo early intensive
From the Departments of Developmental Therapeutics* and Bio- mathematics,t University of Texas System Cancer Center, M. D. An- derson Hospital and Tumor Institute, Houston, Texas.
Supported by grant CA-10376 from the National Cancer Institute, National Institutes of Health. Bethesda, Maryland.
Address for reprints: David J. Stewart, MD, Ontario Cancer Foun- dation Clinic, Ottawa General Hospital, 501 Srnyth Road, Ottawa, On- tario, Canada, KIG 8L6.
Accepted for publication December 26, 1982.
chemotherapy and which should just be observed, we attempted to define prognostic factors in this disease.
Materials and Methods
A review was conducted of charts of all 31 patients with hairy cell leukemia admitted to M. D. Anderson Hospital between July 1972 and November 1979. All patients were men. Data recorded included dates of onset of symptoms, diagnosis, admission to M. D. Anderson, splenectomy, first major infection, and bone marrow fail- ure; patient's age, occupation, initial signs and symptoms, family history of leukemia and lymphomas, past medical history, history of radiation exposure, and spleen weight. Hepatic and renal function at the time of admission to M. D. Anderson Hospital was also noted. Hematologic parameters including hemoglobin, reticulocyte count, platelet count, leukocyte count, and differential were re- corded for time of onset of symptoms, time of presentation at M. D. Anderson Hospital, time of splenectomy, and at I month and 6 months postsplenectomy. Bone marrow characteristics including aspiratability, cellularity, and dif- ferential were recorded for the same time periods.
The Gehan modification of the Wilcoxon test' was used to compare survival distributions according to patient characteristics, and median survival times were estimated by linear interpolation from survival curves calculated by the method of Kaplan and Meier. Two patients who received chemotherapy that proved highly effective against this disease3 were censored at the time of administration
I198
No. 5 PROGNOSTIC FACTORS IN HAIRY CELL LEUKEMIA - Sfrwurf ef ul. 1199
of the chemotherapy. This was done because it was felt their inclusion after the point of treatment could sub- stantially bias our results. Both patients had bone marrow failure at the point of treatment. and almost normal mar- row function after treatment. Correlation coefficients were calculated to detect association between patient charac- teristics.
Results
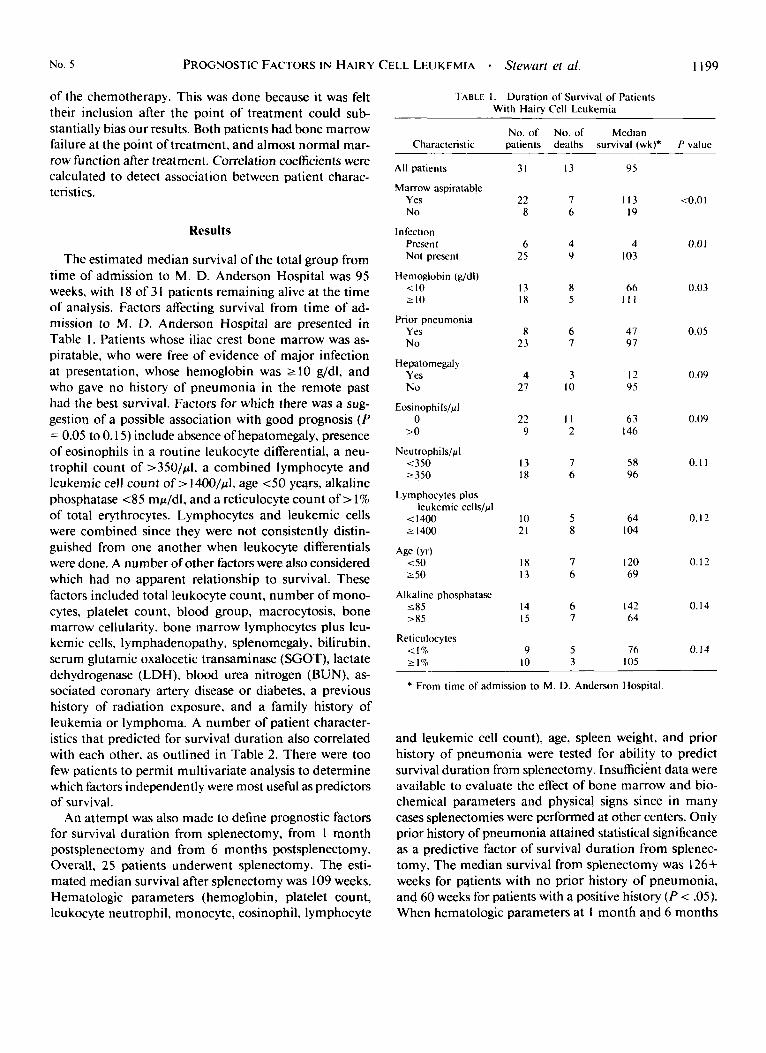
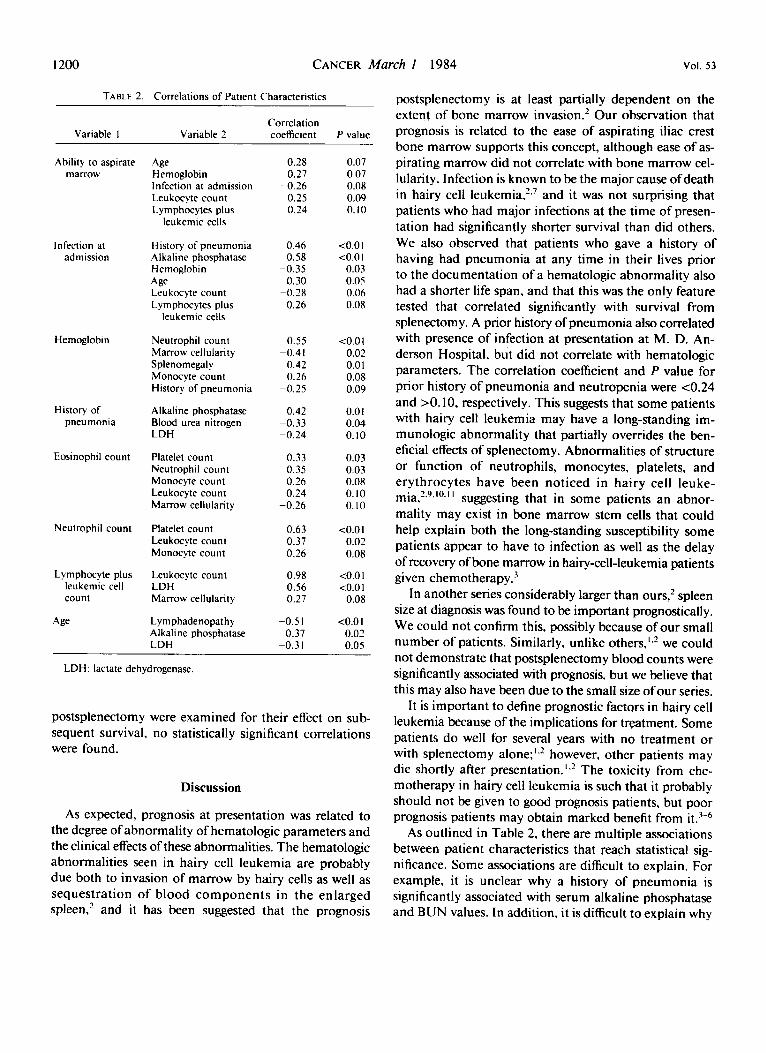
The estimated median survival of the total group from time of admission to M. D. Anderson Hospital was 95 weeks, with 18 of 3 1 patients remaining alive at the time of analysis. Factors affecting survival from time of ad- mission to M. D. Anderson Hospital are presented in Table 1. Patients whose iliac crest bone marrow was as- piratable, who were free of evidence of major infection at presentation, whose hemoglobin was 2 10 g/dl. and who gave no history of pneumonia in the remote past had the best survival. Factors for which there was a sug- gestion of a possible association with good prognosis (P = 0.05 to 0.15) include absence of hepatomegaly, presence of eosinophils in a routine leukocyte differential, a neu- trophil count of >35O/pl, a combined lymphocyte and leukemic cell count of > 14OO/pl, age 4 0 years, alkaline phosphatase 4 5 mp/dl, and a reticulocyte count of > 1% of total erythrocytes. Lymphocytes and leukemic cells were combined since they were not consistently distin- guished from one another when leukocyte differentials were done. A number of other factors were also considered which had no apparent relationship to survival. These factors included total leukocyte count, number of mono- cytes, platelet count, blood group, macrocytosis, bone marrow cellularity, bone marrow lymphocytes plus leu- kemic cells, lymphadenopathy, splenomegaly, bilirubin, serum glutamic oxalocetic transaminase (SGOT), lactate dehydrogenase (LDH), blood urea nitrogen (BUN), as- sociated coronary artery disease or diabetes, a previous history of radiation exposure, and a family history of leukemia or lymphoma. A number of patient character- istics that predicted for survival duration also correlated with each other, as outlined in Table 2. There were too few patients to permit multivariate analysis to determine which factors independently were most useful as predictors of survival.
An attempt was also made to define prognostic factors for survival duration from splenectomy, from 1 month postsplenectomy and from 6 months postsplenectomy. Overall, 25 patients underwent splenectomy. The esti- mated median survival after splenectomy was 109 weeks. Hematologic parameters (hemoglobin, platelet count, leukocyte neutrophil, monocyte, eosinophil, lymphocyte
TABLE I . Duration of Survival of Patients With Hairy Cell Leukemia
No. of No. of Median Characteristic patients deaths survival (wk)* P value -
All patients
Marrow aspiratahle Yes No
Infection Present Not present
110 2 10
Hemoglohin (g/dl)
Prior pneumonia Yes No
Hepdtomegaly Yes No
Eosinophils/pl 0
>O
Neutrophils/pl <350 2350
Lymphocytes plus leukemic cells/pl i I400 t I400
Age (yr) 4 0 2 50
5 8 5 285
Alkaline phosphatase
Reticulocytes < I 7" 2 17"
31
22 8
6 25
13 18
8 23
4 27
22 9
13 18
I0 21
18 13
14 15
9 10
13
7 6
4 9
8 5
6 7
3 10
I I 2
7 6
5 8
7 6
6 7
5 3
- 95
I I3 19
4 I03
66 I l l
41 91
12 95
63 I46
58 96
64 I04
I20 69
142 64
76 I05
<0.0 I
0.01
0.03
0.05
0.09
0.09
0. I I
0.12
0.12
0.14
0. I4
* From time of admission to M. D. Anderson Hospital
and leukemic cell count), age, spleen weight, and prior history of pneumonia were tested for ability to predict survival duration from splenectomy. Insufficient data were available to evaluate the effect of bone marrow and bio- chemical parameters and physical signs since in many cases splenectomies were performed at other centers. Only prior history of pneumonia attained statistical significance as a predictive factor of survival duration from splenec- tomy. The median survival from splenectomy was 126+ weeks for pqtients with no prior history of pneumonia, and 60 weeks for patients with a positive history ( P < .05). When hematologic parameters at I month and 6 months
1200 CANCER March I 1984 Vol. 53
TABLE 2. Correlations of Patient Characteristics
Correlation Variable I Variable 2 coefficient P value
Ability to aspirate marrow
Infection at admission
Hemoglobin
History of pneumonia
Eosinophil count
Neutrophil count
Lymphocyte plus leukemic cell count
Age
Age Hemoglobin Infection at admission Leukocyte count Lymphocytes plus
leukemic cells
History of pneumonia Alkaline phosphatase Hernoglobin Age Leukocyte count Lymphocytes plus
leukemic cells
Neutrophil count Marrow cellularity Splenomegaly Monocyte count History of pneumonia
Alkaline phosphatase Blood urea nitrogen LDH
Platelet count Neutrophil count Monocyte count Leukocyte count Marrow cellularity
Platelet count Leukocyte count Monocyte count
Leukocyte count LDH Marrow cellularity
Lymphadenopathy Alkaline phosphatase LDH
-0.28 0.27
-0.26 0.25 0.24
0.46 0.58
-0.35 0.30
-0.28 -0.26
0.55 -0.41 -0.42
0.26 -0.25
0.42 -0.33 -0.24
0.33 0.35 0.26 0.24
-0.26
0.63 0.37 0.26
0.98 0.56 0.27
-0.5 I 0.37
-0.3 I
0.07 0.07 0.08 0.09 0.10
<o.o I <o.o I
0.03 0.0s 0.06 0.08
<0.01 0.02 0.0 I 0.08 0.09
0.0 I 0.04 0.10
0.03 0.03 0.08 0.10 0.10
<O.OI 0.02 0.08
<o.o I <o.o I
0.08
<o.o 1 0.02 0.05
LDH: lactate dehydrogenase.
postsplenectomy were examined for their effect on sub- sequent survival, no statistically significant correlations were found.
Discussion
As expected, prognosis at presentation was related to the degree of abnormality of hematologic parameters and the clinical effects of these abnormalities. The hematologic abnormalities seen in hairy cell leukemia are probably due both to invasion of marrow by hairy cells as well as sequestration of blood components in the enlarged spleen,’ and it has been suggested that the prognosis
postsplenectomy is at least partially dependent on the extent of bone marrow invasion.’ Our observation that prognosis is related to the ease of aspirating iliac crest bone marrow supports this concept, although ease of as- pirating marrow did not correlate with bone marrow cel- lularity. Infection is known to be the major cause ofdeath in hairy cell leukemia.’.’ and it was not surprising that patients who had major infections at the time of presen- tation had significantly shorter survival than did others. We also observed that patients who gave a history of having had pneumonia at any time in their lives prior to the documentation of a hematologic abnormality also had a shorter life span, and that this was the only feature tested that correlated significantly with survival from splenectomy. A prior history of pneumonia also correlated with presence of infection at presentation at M. D. An- derson Hospital, but did not correlate with hematologic parameters. The correlation coefficient and P value for prior history of pneumonia and neutropenia were <0.24 and >O. 10, respectively. This suggests that some patients with hairy cell leukemia may have a long-standing im- munologic abnormality that partially ovemdes the ben- eficial effects of splenectomy. Abnormalities of structure or function of neutrophils, monocytes, platelets, and erythrocytes have been noticed in hairy cell leuke- mia,2.9,10.1 I suggesting that in some patients an abnor- mality may exist in bone marrow stem cells that could help explain both the long-standing susceptibility some patients appear to have to infection as well as the delay of recovery of bone marrow in hairy-cell-leukemia patients given chemotherapy.
In another series considerably larger than ours,’ spleen size at diagnosis was found to be important prognostically. We could not confirm this, possibly because of our small number of patients. Similarly, unlike others,’.’ we could not demonstrate that postsplenectomy blood counts were significantly associated with prognosis, but we believe that this may also have been due to the small size ofour series.
It is important to define prognostic factors in hairy cell leukemia because of the implications for treatment. Some patients do well for several years with no treatment or with splenectomy alone;’,’ however, other patients may die shortly after presentation.’.’ The toxicity from che- motherapy in hairy cell leukemia is such that it probably should not be given to good prognosis patients, but poor prognosis patients may obtain marked benefit from it.3-6
As outlined in Table 2, there are multiple associations between patient characteristics that reach statistical sig- nificance. Some associations are difficult to explain. For example, it is unclear why a history of pneumonia is significantly associated with serum alkaline phosphatase and BUN values. In addition, it is difficult to explain why

No. 5 PROGNOSTIC FACTORS I N HAIRY CELL LEUKEMIA - Stewart et al. 1201
younger patients were significantly more likely to have lymphadenopathy than were older patients.
Our results must be interpreted cautiously because of the small number of patients analyzed. However, they raise the interesting question of whether some patients with hairy cell leukemia may have a preexisting immu- nologic abnormality that is associated with a relatively poor prognosis. In addition, they suggest that patients who have a bone marrow that is difficult to aspirate, low hemoglobin, or a major infection at initial presentation have a relatively poor prognosis, and should be treated more intensively than other patients.
REFERENCES
I . Catovsky D. Hairy cell leukemia and prolymphocytic leukemia.
2. Jansen J, Hermans J. Splenectomy in hairy cell leukemia: A ret- <?in Lab Huemulo1 1977; 6:245-268.
rospective multicenter analysis. Cancer 198 I : 47:2066-2076.
3. Stewart DJ, Benjamin RS, McCredie KB, Murphy SG. Keating M. The effectiveness of rubidazone in hairy cell leukemia (leukemic reticuloendotheliosis). E h d 1979: 54:298-304.
4. Stewart DJ, Keating MJ, Youness E, Burgess MA. Long-Term chemotherapy induced remission in a probable case of hairy cell leukemia. Cuncer Treul Rep 1981; 65:313-315.
5. Golomb HM, Mintz U. Treatment of hairy cell leukemia (leukemic reticuloendotheliosis): I I . Chlorombucil therapy in postsplenectomy pa- tients with progressive disease. Blood 1979; 54:305-309.
6. Davis TE, Waterbury L, Abeloff M. Leukemic reticuloendotheliosis. Arch lnlern Mid 1976; 136:620-622.
7. Stewart DJ, Bodey GP. Infections in hairy cell leukemia (leukemic reticuloendotheliosis). Cuncer 198 1 : 47:XO 1-805.
8. Gehan E. A generalized Wilcoxon test for comparing arbitrarily singly censored samples. Eiomdriku 1965; 52:203-224.
9. Schnitzer B. Kass L. Hairy cell leukemia: A clinicopathologic and ultrastructural study. Am J C'lin Pulhol 1974; 61:176-187.
10. Hersh EM, Murphy S, Toki H. Immunological deficiency in hairy cell leukemia and its correction by leukocyte transfusion. Proc Am Snc Clin Oncol 1979; 20:382.
I I . Ghadially FN, Skinnider LF. Ultrastructure of hairy cell leukemia. Chncrr 1912; 29:444-452.





























