Embed Size (px)
Citation preview
![Page 1: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/1.jpg)
CHA
L.C. Weaver and C. Polosa (Eds.)
Progress in Brain Research, Vol. 152
ISSN 0079-6123
Copyright r 2006 Elsevier B.V. All rights reserved
PTER 16
Autonomic dysreflexia after spinal cord injury:central mechanisms and strategies for prevention
Lynne C. Weaver1,�, Daniel R. Marsh2, Denis Gris1, Arthur Brown1 and Gregory
A. Dekaban1
1Spinal Cord Injury Team, BioTherapeutics Research Group, Robarts Research Institute, 100 Perth Drive, P.O. Box 5015,London, ON N6A 5K8, Canada
2Department of Anatomy and Cell Biology, Dalhousie University, Halifax, NS, Canada
Abstract: Spinal reflexes dominate cardiovascular control after spinal cord injury (SCI). These reflexes areno longer restrained by descending control and they can be impacted by degenerative and plastic changeswithin the injured cord. Autonomic dysreflexia is a condition of episodic hypertension that stems fromspinal reflexes initiated by sensory input entering the spinal cord caudal to the site of injury. This hy-pertension greatly detracts from the quality of life for people with cord injury and can be life-threatening.Changes in the spinal cord contribute substantially to the development of this condition. Rodent modelsare ideal for investigating these changes. Within the spinal cord, injury-induced plasticity leads to nervegrowth factor (NGF)-dependent enlargement of the central arbor of a sub-population of sensory neurons.This enlarged arbor can provide increased afferent input to the spinal reflex, intensifying autonomicdysreflexia. Treatments such as antibodies against NGF can limit this afferent sprouting, and diminish themagnitude of dysreflexia. To assess treatments, a compression model of SCI that leads to progressivesecondary damage, and also to some white matter sparing, is very useful. The types of spinal reflexes thatlikely mediate autonomic dysreflexia are highly susceptible to inhibitory influences of bulbospinal pathwaystraversing the white matter. Compression models of cord injury reveal that treatments that spare whitematter axons also markedly reduce autonomic dysreflexia. One such treatment is an antibody to theintegrin CD11d expressed by inflammatory leukocytes that enter the cord acutely after injury and causesignificant secondary damage. This antibody blocks integrin-mediated leukocyte entry, resulting in greatlyreduced white-matter damage and decreased autonomic dysreflexia after cord injury. Understanding themechanisms for autonomic dysreflexia will provide us with strategies for treatments that, if given early aftercord injury, can prevent this serious disorder from developing.
Introduction to autonomic dysreflexia
In 2001, my co-authors and I published a chapterreviewing the central mechanisms for autonomicdysreflexia in a volume of Progress in Brain Re-search that focused on spinal cord injury (SCI)(Weaver et al., 2001a). The present volume,
�Corresponding author. Tel.: +519 663 3776;
Fax: +519 663 3789; E-mail: [email protected]
DOI: 10.1016/S0079-6123(05)52016-8 245
entirely devoted to autonomic dysfunction aftercord injury, contains many chapters written byinvestigators quoted in that 2001 review. As thework of others is presented elsewhere in this book,this chapter will focus on the 10 years of investi-gations of autonomic dysreflexia from our labo-ratory that began in 1995.
After SCI, large increases in arterial pressure(AP) can develop in response to sensory input en-tering the spinal cord below the level of the lesion
![Page 2: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/2.jpg)
246
(Mathias and Frankel, 1992a, b; Lee et al., 1994;Krassioukov and Weaver, 1995; Maiorov et al.,1998). This hypertension, part of a conditiontermed autonomic dysreflexia, occurs in 50–90%of people with tetraplegia or high paraplegia(Corbett et al., 1975; Erickson, 1980; Lindan etal., 1980; Mathias and Frankel, 1992a; Lee et al.,1994; Giannantoni et al., 1998; Vaidyanathanet al., 1998; Karlsson, 1999; Krassioukov et al.,2003). The hypertension can result in debilitatingheadaches, seizures, strokes and even death. Asblood pressure control normally depends uponsupraspinal regulation of sympathetic neurons(Calaresu and Yardley, 1988), SCI leads to a con-dition in which central nervous system (CNS)regulation of AP is dominated by excitatory spinalreflexes. This excitation is prominent, in part,because cord injury blocks descending bulbospinalinhibition of spinal sympathetic reflexes (Sato andSchmidt, 1973; Dembowsky et al., 1978, 1980); theunchecked activity of these reflexes leads toautonomic dysreflexia.
Dysreflexia occurs after injury at or rostral tothe 6th thoracic spinal segment, because injury atthese levels leaves the sympathetic control of theextensive abdominal circulation amenable to un-restrained spinal reflexes (Mathias and Frankel,1992a). These reflexes can be caused by innocuousor noxious stimulation of the skin, pressure sores,distension or inflammation of the urinary bladderor gastrointestinal tract and also by muscle spasmsthat often develop after SCI (Guttman andWhitteridge, 1947; Corbett et al., 1975; Mathiasand Frankel, 1992a; Blackmer, 2003). They can beinitiated by routine daily procedures such as blad-der catheterization and bowel evacuation. Dysre-flexia is not always severe and may include onlysweating, flushed skin above the segment of injury,piloerection and small increases in AP. However,this condition can become uncontrolled, leading tolife-threatening hypertension (Shea et al., 1973;Naftchi, 1990; Mathias and Frankel, 1992c; Leeet al., 1994; Naftchi and Richardson, 1997;Giannantoni et al., 1998; Blackmer, 2003). Mech-anisms for autonomic dysreflexia may involve af-ferent, interneuronal and efferent components ofthe spinal sympathetic reflex and the vasculature,as also discussed in other chapters of this book.
This chapter will review studies in rats thatdemonstrated some of the changes within thespinal cord that can contribute to the developmentof autonomic dysreflexia, and experiments thatshow the potential for treatments to prevent thedevelopment of dysreflexia.
Rodent models of autonomic dysreflexia
Rats and mice readily develop autonomic dysre-flexia after SCI (Osborn et al., 1990; Maiorovet al., 1997a, b, 1998, 2001; Landrum et al., 1998;Jacob et al., 2001, 2003). In response to distensionof the urinary bladder or colon, exaggerated in-creases in AP are apparent within a day of a cordtransection at the upper thoracic (T) segments(T2–4) and these responses augment with time af-ter injury. This progression after cord transectionin rats was followed for up to 5 weeks in ourlaboratory. A conscious, unrestrained rat with anintact CNS has a transient, 5–15mmHg increase inmean arterial pressure (MAP) upon colon disten-sion, accompanied by an increase in heart rate(HR) (Krassioukov and Weaver, 1995; Maiorovet al., 1997b). In this chapter, changes in bloodpressure will be expressed as changes in MAP,unless otherwise indicated. The first day aftercord transection, the increase in AP, in responseto visceral stimulation, can be as great as4172mmHg, but within the next few days, theseresponses become smaller, perhaps associated withdegenerative changes in the spinal sympatheticpreganglionic neurons caudal to the injury (see thefollowing sections) (Krassioukov and Weaver,1995; Maiorov et al., 1997a, b). Then, in the en-suing weeks, the increases in AP during dysreflexiabecome larger, reaching values as high as5274mmHg by 5 weeks after SCI. The large re-sponse on the first day likely reflects the full ca-pacity of the spinal reflex, without descendinginhibitory restraint (Dembowsky et al., 1980), andbefore the secondary effects of cord injury haveimpacted greatly. After this time, the magnitude ofthe hypertension appears to become a function ofmany changes ongoing in the spinal cord andvasculature, some degenerative and others, plasticresponses to the injury. These intraspinal changes,
![Page 3: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/3.jpg)
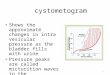
Fig. 1. The MAP, pulsatile AP and HR in two rats, 2 weeks
after clip-compression SCI: after intrathecal treatment with
control immunoglobulin G (IgG) (A) and after intrathecal
treatment with trkA-IgG (B). Colon distension for 60 s (onset
and duration marked with a thick line) stimulated a large in-
crease in AP and MAP and a decrease in HR in the control
IgG-treated rat. In contrast, colon distension caused only a
modest decrease in AP and MAP after treatment with trkA-
IgG. Reprinted with permission from Marsh et al. (2002).
247
and their relationship to this time course of auto-nomic dysreflexia will be discussed later in thischapter.
Autonomic dysreflexia is readily apparent inrats when SCI is caused by a method that repro-duces the typical clinical injury. This method en-tails brief (60 s) extradural compression of the cordwith a calibrated, modified aneurysm clip. Theclip-compression model mimics the key patho-physiological features of human SCI. This modelproduces mechanical injury (primary injury) andsecondary damage by a variety of well-character-ized mechanisms including microvasculature dis-ruption, hemorrhage, ischemia, increases inintracellular calcium, calpain activation, progres-sive axonal injury and glutamate toxicity (Wallaceand Tator, 1986; Wallace et al., 1986; Fehlingset al., 1989; Koyanagi et al., 1993a, b; Agrawaland Fehlings, 1996, 1997a, b; Agrawal et al., 1998;Schumacher et al., 1999). Marked autonomicdysreflexia is readily evoked after severe (50 g)clip-compression cord injury at T2–4 in rats andmice (Maiorov et al., 1998; Mayorov et al., 2001;Weaver et al., 2001b; Jacob et al., 2003) (Fig. 1A).Distension of the colon with a small balloon-tipped catheter or cutaeous stimulation in con-scious rats at two weeks after injury causes pressorresponses that continue to increase in magnitudeuntil 6 weeks after cord injury, when they appearto plateau (Gris et al., 2004; Marsh and Weaver,2004). Dysreflexia after clip-compression injurycan be evoked by visceral or cutaneous stimuli thatare noxious or non-noxious. Gently stroking theskin of the back caudal to the segment of injurycauses pressor responses of 2375mmHg, whereaspinching the skin increases pressure by up to3272mmHg. Likewise, distension of the colon toan extent that would be noxious in the intact an-imal increases AP by 4274mmHg, whereas amilder distension, that would not be noxious, stillincreases AP by 2473mmHg. In a conscious ratwith an intact CNS, this non-noxious cutaneous orvisceral stimulation would cause either no changein AP or a transient (5–10 s) increase of5–10mmHg. These findings refute the idea thatautonomic dysreflexia is initiated only by noxiousstimuli. The responses to the non-noxious stimuliare smaller than those to noxious stimuli, but are
abnormal, or dysreflexic responses, as they aremore than twice the magnitude of those in anintact rat.
The large increase in noradrenaline spill-over re-ported during dysreflexia is consistent with intense
![Page 4: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/4.jpg)
248
sympathetic firing relative to baseline values(Karlsson et al., 1998). Direct measurements ofvisceral vasomotor sympathetic firing can be madein animals. The renal nerve has mostly vasomotorsympathetic axons, and renal sympathetic firingrecorded in conscious rats, after cord transectionat T4, increases massively during episodes of au-tonomic dysreflexia (Maiorov et al., 1998). Theincreases are at least sixfold above baseline firingand, during the first week after cord transection,they parallel the increase in amplitude of the bloodpressure responses. Recordings at later times havenot been reported. These spinal reflexes are muchlarger than they would be if the nervous systemwere intact (Coote et al., 1969; Koizumi andBrooks, 1972; Dembowsky et al., 1980) and reflectloss of descending inhibition and, with time, plas-tic changes within the spinal cord.
Basal firing of the renal sympathetic nerve isgreatly reduced by cord transection so that thenerve targets are possibly approaching the state of‘‘denervation’’ postulated by McLachlan andBrock (see this volume and Yeoh et al., 2004).The low firing rate certainly could prompt signif-icant changes in the peripheral sympathetic systemand vascular targets. However, even the low basalsympathetic firing in the first week after T4 tran-section appears to make a contribution to vaso-motor control, as ganglionic blockade decreasesresting AP by 4577mmHg (Maiorov et al.,1997b). This lowered sympathetic activity becomesthe norm after cord injury, and, if this activity isgreatly increased by a spinal reflex, coupled with amore reactive vasculature and changes in periph-eral neurotransmission, large hypertensive re-sponses can occur.
Spinal cord transection or compression also hassignificant initial effects on resting AP, decreasingit by 2374mmHg during the first 24 h after cordinjury (Maiorov et al., 1997b). This decrease istransient and by 1 week after injury AP returns tonormal values (10173mmHg). This range of APis stable for at least 6 weeks (Krassioukov andWeaver, 1995; Maiorov et al., 1997a; Krenz et al.,1999; Weaver et al., 2001b; Marsh et al., 2002; Griset al., 2004; Marsh and Weaver, 2004). In contrast,HR initially is not altered by cord transection orclip-compression at T4, but gradually increases
with time after injury, from �400 to 450 beats/minin intact rats or cord-injured rats up to a weekafter injury, to rates of �500–570 beats/min at 2–6weeks after injury. In one study, we attributed thistachycardia to increased afferent input to upperthoracic preganglionic neurons, resulting fromsprouting of primary afferent fibers in the dorsalhorn (Krenz et al., 1999). This input, if tonicallyactive, could contribute to enhanced sympatheticdrive to the heart. Others have also reported in-creases in HR after cord transection at T4(Rodenbaugh et al., 2003), and have suggestedseveral mechanisms for this tachycardia (seeCollins et al., this volume).
Reorganization of the injured spinal cord
Caudal to the SCI, the loss of supraspinal inputmay make the sympathetic preganglionic neuronmore sensitive to spinal afferent input, not onlybecause of the loss of tonically active inhibitorysupraspinal influences, but also because, in theabsence of descending excitatory synaptic input,the remaining excitatory synapses within spinalreflex circuits have a more dominant influence. Asreviewed by Llewellyn-Smith et al. (this volume),glutamatergic inputs to preganglionic neurons arelargely lost within a few days of cord transection(Llewellyn-Smith and Weaver, 2001), yet, at thesame time, the neurons respond vigorously toreflex inputs, suggesting that a few dominantsynapses can activate the neurons. Reorganizationof the spinal pathways controlling sympatheticpreganglionic neurons after the loss of supraspinalinput is likely to change the makeup of inputs tothese neurons (Krassioukov and Weaver, 1996;Cassam et al., 1997, 1999; Weaver et al., 2001b).We searched for changes in glutamatergic spinalreflex transmission via N-methyl-D-aspartate(NMDA) and a-amino-3-hydroxy-5-methyl-4-isoxazolpropionic acid (AMPA) receptors duringthe first 2 weeks after spinal cord transection(Maiorov et al., 1997a). Using selective receptorantagonists, these two receptors appeared to con-tribute about equally (�35% each) to the reflexexcitation causing autonomic dysreflexia, at 2 and16 days after the injury, demonstrating no change
![Page 5: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/5.jpg)
249
with time in the roles of these receptors during theinitial period after injury.
The enhanced transmission through the spinalreflex circuits suggested by the recording of renalnerve responses (Maiorov et al., 1997b) could bemediated by changes in the afferent, interneuronalor preganglionic neuronal components of the arc.Earlier studies lead to the hypothesis that synapticinput to preganglionic neurons undergoes plasticreorganization after cord injury, resulting inreplacement of inputs from bulbospinal neuronswith those from interneurons (Krassioukov andWeaver, 1996; Weaver et al., 1997). Thoracicpreganglionic neurons undergo a transient degen-erative response, characterized by retraction ofdendrites and shrinkage of the soma, during thefirst week after cord transection (the period ofsynaptic loss), and then re-establish a normaldendritic arbor and soma size within 2–4 weeksafter the injury (Krassioukov and Weaver, 1996;Krenz and Weaver, 1998a; Llewellyn-Smith andWeaver, 2001). This acute degenerative responseof the preganglionic neurons with later morpho-logical recovery was also found in samples of in-jured human spinal cord (Krassioukov et al.,1999). These observations led us to propose amodel in which synapses from supraspinal neuronswere replaced with those from spinal circuits,leading to exaggerated spinal reflex control ofpreganglionic neurons. Immediately after cordinjury, the preganglionics are intact and descend-ing inhibition is lost, leading to robust spinalreflex-mediated pressor responses. Then, pregangl-ionic neurons undergo a degenerative responsethat is maximal at about 1 week, the time whenautonomic dysreflexia is decreased in magnitude.Finally, as the preganglionic neurons recover fromthe atrophy and have a normal soma size anddendritic tree, with potentially new synaptic inputsfrom interneurons, autonomic dysreflexia beginsto increase in magnitude. Although this was anappealing model, an electron microscopic study(Llewellyn-Smith and Weaver, 2001) demonstratedthat the loss of bulbospinal synaptic input tothoracic preganglionic neurons reduces the num-ber of synapses on these neurons by 50–70%, andthis loss is not replaced by intraspinal inputs.Accordingly, the number of synapses from the
interneurons after cord injury does not appear toincrease and, therefore, an increased number ofsynapses from interneurons to preganglionic neu-rons does not mediate the time-dependent increas-es in the spinal sympathetic reflexes and pressorresponses. The interneurons may still contribute ifthey are more excited by an afferent input to thespinal cord, and provide increased preganglionicexcitation through temporal rather than spatialsummation. Consistent with this view, an electro-physiological study of responses of sympathetical-ly correlated spinal interneurons to cutaneousinputs, after spinal cord transection, showed thatthe receptive fields of individual interneurons tothis input enlarge with time after spinal cordtransection, increasing their capacity to provideexcitatory input to the preganglionic neurons(Krassioukov et al., 2002) (see also Schramm, thisvolume). Moreover, the gray matter containingthoracic preganglionic neurons, and interneuronsproviding input to them, develops a network offibers immunoreactive to growth-associatedprotein-43 that increases in density between 2and 4 weeks after cord transection (Weaver et al.,1997). This protein was also present in putativegrowth cones and in cell bodies that likely wereinterneurons. These data suggest that, althoughthe thoracic preganglionic neurons themselves didnot receive new synaptic inputs, growth within thelocal neuropil likely generated new inputs to otherneurons antecedent to the preganglionics.
Changes in the primary afferent arbor contributing
to autonomic dysreflexia
In the dorsal horn, the arbors of small-diameterprimary afferent neurons can enlarge greatly inrats and mice after SCI (Krenz and Weaver,1998b; Krenz et al., 1999; Wong et al., 2000; Jacobet al., 2001, 2003; Weaver et al., 2001b) (Fig. 2)potentially leading to increased reflex excitation ofpreganglionic neurons, via interneuronal path-ways. These afferent neurons that are calcitoningene-related peptide (CGRP)-immunoreactive,and the interneurons in laminae III–VII activatedby these afferent projections, make up the path-way, mediating spinal reflex excitation of
![Page 6: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/6.jpg)
Fig. 2. Digital photomicrographs of CGRP-immunoreactive (left, red) and substance P-immunoreactive (right, green) afferent fibers in
the dorsal horn of sham-injured rats (A and B) and of rats with clip-compression SCI at T4 (C-H). Examples are shown at 2 weeks after
sham or SCI. Tissue sections (30mm) from T12 to L1 were processed for double immunofluorescence for CGRP (red) and substance P
(green) and visualized with a 10� objective (A–D, calibration bar ¼ 100mm), a 20� objective (E–G, calibration bar ¼ 50 mm), or with
confocal microscopy (H, calibration bar ¼ 10mm). Co-localization of CGRP and substance P in afferent fibers is indicated by yellow.
Reprinted with permission from Marsh and Weaver (2004).
250
![Page 7: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/7.jpg)
251
preganglionic neurons (Sato and Schmidt, 1973;Cabot et al., 1994; Joshi et al., 1995; Clarke et al.,1998). After cord transection or compression inrats and some strains of mice, the 2-week timecourse for the increased arbor size correlates withthe gradual increase in the magnitude of auto-nomic dysreflexia (described earlier) and may alsobe a factor contributing to the increase. Aftertransection injury, the size of the increase in theCGRP-immunoreactive afferent arbor correlateswith the magnitude of dysreflexia (Krenz et al.,1999; Jacob et al., 2001, 2003). This afferent arborremains enlarged at 1 month after cord injury, atime when autonomic dysreflexia is well developedin rats (Krassioukov and Weaver, 1995). The‘‘enlarged’’ CGRP-immunoreactive afferent arbormight reflect only increased CGRP expression inthe fibers rather than a sprouting or growthresponse. However, a confocal microscopicanalysis of changes in the afferent arbor after T4cord transection, using retrograde transport ofwheat germ agglutinin, revealed a true increase inthe size of the arbor of small diameter fibers in thelumbar spinal cord (Wong et al., 2000). Likewise,transport of the b subunit of cholera toxin aftercord transection also revealed expansion of thearbor of larger afferent fibers in the lumbar cord(Krenz and Weaver, 1998b). Together, these find-ings demonstrate that the increase in CGRP aftercord injury reflects a growth response, not simply anincrease in gene expression. The changes in thelarger diameter fibers probably underlie the re-sponses to non-noxious cutaneous and visceral stim-ulation described above (Marsh and Weaver, 2004).
The relationship between changes in the afferentarbor and the magnitude of dysreflexia is less ro-bust in the clip-compression cord-injury modelthat spares some descending pathways. Enlarge-ment of the CGRP-immunoreactive primary af-ferent arbor is also characteristic of this model, butchanges are smaller than after cord transection,whereas the magnitude of dysreflexia can also beas great (Krenz and Weaver, 1998b; Krenz et al.,1999; Weaver et al., 2001b). Injury to the cordmust be severe for enlargement of the primary af-ferent arbor and autonomic dysreflexia to occur.At 2 weeks after moderate/mild (20 g) clip-com-pression cord injury at T4, rats have no autonomic
dysreflexia in response to colon distension and nochange in the CGRP-immunoreactive afferentarbor. In contrast, after a more severe (50 g) inju-ry, autonomic dysreflexia develops consistentlyand the CGRP-immunoreactive arbor in the lowerthoracic and lumbar spinal cord enlarges. The dif-ference between the transection and compressioninjury model is the sparing of a limited number ofwhite-matter axons that pass through the lesionsite. If the compression is only moderate, andmany axons are spared, sufficient bulbospinal in-put remains to prevent the development ofdysreflexia and afferent sprouting. However, aftersevere compression injury, the small sparing ofdescending fibers is not adequate to block dysre-flexia and the sprouting response does develop,albeit modestly.
The small diameter C-type sensory neurons inthe dorsal root ganglia contain a population thatexpress CGRP, and a subset of neurons within thispopulation also express substance P (Price, 1985;Ju et al., 1987). In addition to the small-diameterneurons, CGRP is also expressed in some of thelarger sensory neurons (McCarthy and Lawson,1990; Lawson et al., 1993, 1996). The plasticity inthe CGRP-immunoreactive afferent arbor initiat-ed by cord injury appears to target only the pop-ulation that expresses CGRP without substance P(Marsh and Weaver, 2004) (Fig. 2). The absence ofsprouting of substance P-containing afferent fibersin the dorsal horn, in the presence of increaseddensities of CGRP-containing fibers, shows theselectivity of this response, suggesting that thelarger fibers play a greater role in dysreflexia.Finally, as also discussed by Rabchevsky (this vol-ume), increases or decreases in the afferent arborare only relevant to inputs entering the spinal cordat the same segmental region. For example, be-cause of the segmental arrangement of the primaryafferent projections to the spinal cord (Vizzardet al., 2000), changes in the lumbosacral arbor willimpact on responses to colon or bladder distensionbut not on those to cutaneous stimulation of themid-thoracic trunk. Likewise, changes in the mid-thoracic region do not impact on responses to co-lon distension (Cameron et al., 2003; Gris et al.,2005). In our studies, the afferent arbor was par-ticularly increased in the lower lumbar segments
![Page 8: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/8.jpg)
252
after cord transection or compression (Krenz andWeaver, 1998b; Krenz et al., 1999; Jacob et al.,2001, 2003; Weaver et al., 2001b), making afferentplasticity more of an issue to responses initiatedfrom the pelvic organs or hind limbs.
Enlargement of the afferent arbor depends uponactions of nerve growth factor (NGF) in the in-jured rat spinal cord. Intrathecal delivery of ahighly selective neutralizing antibody to NGF for2 weeks after cord transection at T4 completelyblocked the sprouting of the small-diameter affer-ent fibers in the dorsal horn (Krenz et al., 1999).Delivery of the antibody subcutaneously to pe-ripheral targets of the sensory neurons had no ef-fect, demonstrating that the afferent sprouting wasnot caused by a target-derived source of NGF.Blockade of the sprouting response was due to theneutralizing effects of the anti-NGF antibody onthe trkA-expressing central arbors of these sensoryneurons. Autonomic dysreflexia was measured inthe same rats and the increases in AP caused byvisceral stimulation were reduced by 43% in the(intrathecal) antibody-treated rats. This reducedthe dysreflexia to the magnitude of the spinal reflexthat is present in the conscious rat within 48 h ofcord transection, before enlargement of the affer-ent arbor could occur (Maiorov et al., 1997a).Similarly, intrathecal delivery, for 2 weeks afterclip-compression injury at T4, of a trkA-IgG fu-sion protein that sequesters NGF decreaseddysreflexia in rats by 30% (Marsh et al., 2002)(Fig. 1B). These data led to two conclusions. First,afferent sprouting in the spinal cord dorsal horn isclearly associated with the time-dependent increasein hypertensive responses to sensory stimulation,characteristic of autonomic dysreflexia. Second,the sprouting is caused by an intraspinal action ofNGF, presumably at the central arbors of the sen-sory neurons containing CGRP.
These studies suggest that NGF is a culpritin the development of autonomic dysreflexia.Normally, the spinal cord contains very littleNGF but NGF levels within a few segments of acord injury site have been reported to increase to apeak at 1 week post injury, remaining increased for4 weeks (Bakhit et al., 1991). Using a two-siteenzyme-linked immunosorbant assay (ELISA) toanalyze spinal cord homogenates from rats with a
T4 SCI, we have confirmed that NGF levels in theinjured rat spinal cord are significantly greater inand adjacent to the injury (T3–5) than rostral tothe injury (T1 and 2) or in the lumbar cord. NGFat the injury site was approximately twofold great-er than the content in this region in un-injured rats(1.570.8 pg/mg). Immunocytochemistry on spinalcord sections revealed increased NGF-immunore-activity in cells and fibers in the dorsal rootentry zone, and in astrocytes, microglia andleptomeningeal cells of cord-injured rats (Krenzand Weaver, 2000). These were prevalent insegments T3–8.
A second study of NGF in the injured spinalcord extended these observations further bysearching for cells that produced NGF, i.e., con-tained messenger RNA (mRNA) for NGF. In ad-dition, double-labeling immunocytochemistry wasused to identify, with greater certainty, the cellscontaining this protein (Brown et al., 2004). Wealso compared the NGF profiles in spinal cordswith transection or compression injuries. In intactspinal cords, NGF mRNA was in leptomeningealcells and neurons of the intermediate gray matter,whereas NGF protein was only in the leptome-ninges (Fig. 3). At 3–7 days after transection orclip-compression injury NGF mRNA and proteinwere expressed in the lesion and throughout theintermediate gray matter and the white matterrostral and caudal to the injury site. The NGFmRNA and protein in spinal cord sections adja-cent to each other were expressed in ramified mi-croglia, astrocytes, intermediate gray neurons, pialcells, leptomeningeal cells and Schwann cells in thelateral white matter and lesion site (Fig. 4).Rounded macrophages in the lesion containedimmunoreactivity for NGF, but the cells express-ing NGF mRNA were not macrophages, and didnot appear to contain the protein. These findingsdemonstrated that a variety of cells within theinjured spinal cord could produce NGF, but thatmacrophages are not among them. Macrophagesmay have contained NGF because they phagocy-tosed it.
The studies described above show a strongrelationship between NGF and changes in theafferent arbor that can contribute to dysreflexia.The effectiveness of the anti-NGF antibody and
![Page 9: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/9.jpg)
Fig. 3. The NGF mRNA expression in the injured and un-injured (control) spinal cord. Hybridization signals visualized by alkaline
phosphatase are illustrated in longitudinal sections of the 5th thoracic spinal cord segment (T5). The lateral edge of the spinal cord is at
the top of each photomicrograph. In the un-injured control rats, NGF mRNA was intense in leptomeningeal cells at the edge of the un-
injured spinal cord and in gray-matter cells with morphology like neurons (A–C). Processing serial sections to detect either NGF
mRNA (C) or NeuN-immunoreactivity, confirmed that these gray-matter cells were neurons (D). The leptomeningeal cells at the edge
of the un-injured spinal cord had hybridization signal but none was present in white matter cells (B). NGF mRNA expression increased
after T4 transection-SCI (E–G). At one day, little NGF mRNA was present with the exception of patches of signal in the le-
ptomeningeal cells of the pia mater (E). At 3 days, expression of NGF mRNA was robust in white and gray matter and in the
leptomeninges, especially in segments close to the lesion (F). The NGF mRNA signals were still present but less abundant at 7 days
after SCI (G). Panels H–J show cells expressing NGF mRNA 7 days after SCI (at higher magnification). Within the lesion site, cells
were typically round and clustered (H), whereas those in the white matter were long and spindle shaped (I) and gray-matter cells
expressing NGF mRNA were oval and neuron-like in morphology or small and spindle-shaped (J); d, day; wm, white matter; gm, gray
matter; con, control. The scale bars on A and B are 50 mm; the bar on C also refers to D and is 50 mm; the bar for E–G, shown in G is
250mm; the bar for H–J, shown in J is 50mm. Reprinted from Brown et al. (2004) with permission from Elsevier.
253
the trkA-IgG fusion protein in limiting dysreflexiashows that this strategy might be useful clinicallyto prevent the development of dysreflexia. Thestimulus for the increased intraspinal NGF is nowin question. The inflammatory response to trau-matic injury of the spinal cord is likely to promotethe production of NGF. The inflammatory
response to cord injury begins within minutesand evolves for days, spreading throughout thedamaged cord and into adjacent, non-injuredregions (Blight, 1985; Tator and Fehlings, 1991;Young, 1993; Popovich et al., 1997; Taoka andOkajima, 1998). First, pro-inflammatory chemo-kines and cytokines are released into the injured
![Page 10: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/10.jpg)
Fig. 4. Identification of cells immunoreactive for the astrocytes marker glial fibrillary acidic protein (GFAP) and NGF in longitudinal
sections of the T5 spinal cord. Cells in the white matter are shown at 7 days after T4 transection-SCI (transect, A–C) or T4 clip-
compression SCI (clip, D–F). Immunoreactivity in the lesion is shown at 7 days after clip-SCI (G–I). Immunoreactivity for NGF (A, D
and G) and for GFAP (B, E and H) colocalized in the astrocytic glia limitans at the pial border of the white matter (C, arrow), and in
white-matter astrocytes (C, and F arrowheads). As few GFAP-immunoreactive astrocytes are in the lesion center, only small areas of
colocalization were present in the lesion (I, arrowhead). Scale bar in I refers to all panels and is 50 mm. Reprinted from Brown et al.
(2004) with permission from Elsevier.
254
area by astrocytes, microglia and endothelial cells.Next, activation and proliferation of glia (gliosis)occur, and neutrophils and monocyte/macrophagesenter the spinal cord from the circulation (Popovichet al., 1997; Taoka et al., 1997; Leskovar et al.,2000). Details of the inflammation in the injuredspinal cord will be presented below. Inflammation
and NGF expression and/or signaling are clearlyrelated. Interleukin-6 (IL-6) and IL-1b, twocytokines found in the injured cord (Streit et al.,1998; Hayashi et al., 2000), have well-documentedactions to increase the expression of NGF in theCNS (Bandtlow et al., 1990; Spranger et al., 1990;Saporito et al., 1993) and in Schwann cells of
![Page 11: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/11.jpg)
255
peripheral nerves (Heumann et al., 1987a, b;Lindholm et al., 1987). In response to cordinjury, microglial NGF mRNA transcription andNGF protein release (Heese et al., 1998a, b) arestimulated synergistically by IL-1 and tumor ne-crosis factor (TNF)-a. The central processes ofsensory neurons have IL-6 receptors that would beexposed to IL-6 in the injured cord, leading tostimulation of NGF expression.
The NGF also has pro-inflammatory actions(LaSala et al., 2000). The high-affinity trkA re-ceptor is expressed on monocytes, B-lymphocytesand T-lymphocytes. Although the signaling causedby NGF on these receptors is not fully understood,NGF promotes expression of Bcl-2 in monocytesand mast cells, conferring resistance to cell death(Bullock and Johnson, 1996; LaSala et al., 2000;Saragovi and Gehring, 2000). The NGF also canfacilitate inflammation by promoting differentia-tion of myeloid progenitor cells, inducing prolif-eration and maturation of B-lymphocytes andstimulating the release of inflammatory cytokinessuch as TNF-a from basophils and mast cells.In summary, inflammation can promote NGFexpression and NGF can promote the process ofinflammation. Clearly, the relationship betweeninflammation and NGF could contribute to theNGF-dependent increases in primary afferentarbors in the spinal cord and the development ofautonomic dysreflexia.
Inflammation, secondary damage and autonomic
dysreflexia
Whereas blocking inflammation after SCI maylimit the production of NGF, it also has a host ofneuroprotective actions that make this issue a highpriority in devising strategies to prevent the devel-opment of autonomic dysreflexia as well as theother autonomic, sensory and motor dysfunctionsafter cord injury. Secondary damage after an SCIis caused, in part, by ischemia, cellular and tissueedema, amino acid excitotoxicity and oxidativedamage. The extent of this damage directly corre-lates with the magnitude of autonomic dysreflexia(Weaver et al., 2001b). These changes often relate toearly inflammation and lead to myelin degradation
and intensified necrosis and apoptosis of neuronsand glia, events that contribute to increases inlesion size (Taoka and Okajima, 1998; Bethea andDietrich, 2002). Neutrophils and hematogenousmacrophages invade the spinal cord, peaking at12 h and 5–7 days after SCI, respectively(Popovich et al., 1997; Taoka et al., 1997;Leskovar et al., 2000), and releasing pro-inflam-matory cytokines and reactive oxygen and nitro-gen species (Taoka and Okajima, 1998; Popovichet al., 1999). These cytotoxic substances can fur-ther damage the white and gray matter andcontribute to scar formation (Jones et al., 2002).
The progression of secondary damage deterio-rates neurological function, and renders the spinalcord less amenable to repair strategies such as cellreplacement or therapeutic gene transfer. There-fore, preventing this progression is of key impor-tance. No practical way to control the earlyinflammatory response has yet been devised,despite our understanding of its destructive rolein the final outcome of an injury. We postulatedthat a successful anti-inflammatory treatmentmust selectively disrupt the early, destructive,leukocyte-mediated actions in the injured cord,while leaving an opportunity for later regenerativeinterventions and wound-healing responses. AfterSCI, intraspinal leukocyte infiltration first requiresleukocyte tethering, by selectins, to the surface ofendothelial cells (Bevilacqua, 1993). This isfollowed by the interaction of endothelial cell-adhesion molecules with integrins on theleukocyte surface (Neish et al., 1995; Shanleyet al., 1998), facilitating leukocyte extravasationthrough the blood-CNS barrier. To prevent thisinteraction, we used a monoclonal antibody(mAb) to the CD11d subunit of the CD11d/CD18 integrin (Grayson et al., 1999; Van derVieren et al., 1999) (ICOS Corporation, Bothell,WA). This mAb treatment substantially decreasesthe numbers of neutrophils and macrophages atthe lesion at 3 days after SCI (Mabon et al., 2000;Saville et al., 2004). It also markedly reduces oxi-dative damage to the injured spinal cord (Baoet al., 2004a, b). The anti-CD11d mAb was inject-ed intravenously in three consecutive doses at 2, 24and 48 h after clip-compression cord injury at T4,and effects were assessed on autonomic dysreflexia
![Page 12: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/12.jpg)
256
and on the spinal cord lesion at 2 and 6 weeks afterthe injury (Gris et al., 2004) (Figs. 5 and 6).
At 2 weeks after cord injury, colon distensionincreased AP and decreased HR for the durationof stimulus (Fig. 5). The anti-CD11d mAb treat-ment markedly reduced these increases in AP.Mean increases during the 1min stimulation peri-od were reduced significantly from �30mmHg inthe control rats to �20mmHg in the treated rats.As the normal reflex response to this stimulus in anintact rat is an increase of �15mmHg in AP(Maiorov et al., 1997b), this treatment affectedmuch of the reflex increment attributable to cordinjury. The average decreases in HR during the1min colon distension in control rats (�65 beats/min) tended to be greater than in treated rats (�45beats/min), possibly because of the greater arterialbaroreceptor activation by the larger pressor re-sponses. The treatment had little impact on restingAP (�100mmHg) or HR (�500 beats/min). At 6weeks after compression cord injury, the increasesin AP during dysreflexia were greater than at 2weeks and HR responses to colon distension in the
Fig. 5. Anti-CD11d mAb treatment reduces the magnitude of auton
shown during a 2ml balloon distension of the colon in control (A and
weeks (bottom row) after SCI at T4. The large increase in pressure
Average change in MAP was assessed at 2 (C) and 6 (F) weeks after
treated rats (’ C, n ¼ 10; F, n ¼ 7). The dotted lines on the bar graph
by such stimulation in a rat with an intact spinal cord (Maiorov et al.
rats. Reprinted with permission from Gris et al. (2004), copyright 20
control rats more often included arrhythmias(Fig. 5). AP responses of the treated rats remainedsmaller than those of the control rats at this time.Again, the mean changes in AP of the control rats(�40mmHg) were significantly greater than thoseof the treated rats (�28mmHg). At this time, as atthe earlier 2-week analysis, the anti-CD11d treat-ment did not alter resting AP (�110mmHg) orHR (�500 beats/min). Additional experimentswere done to determine the effect of delaying theonset of treatment to 6 h after compression injury.The second and third injections of anti-CD11dantibody were administered at 24 and 48 h, re-spectively. This treatment also decreased dysre-flexia by �50% at 6 weeks after cord injury,demonstrating that a clinically relevant dosingschedule still is highly effective.
The basis for the improved autonomic outcomeafter this selective anti-inflammatory treatmentwas sparing of the tissue surrounding the lesion ar-ea. The spinal cords had increased areas of compactmyelin within 2–3mm of the injury site at 2 and 6weeks after injury (Fig. 6). Neurofilament in the
omic dysreflexia. Changes in pulsatile AP, MAP and HR are
D) and mAb-treated rats (B and E) at 2 weeks (top row) and 6
evoked at 6 weeks was often associated with arrhythmias (D).
cord injury in control rats (& C, n ¼ 14; F, n ¼ 6) and mAb-
s show the approximate change in pressure that would be elicited
, 1997a). bpm, beats per minute; *Po0.05 compared to control
04 by the Society for Neuroscience.
![Page 13: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/13.jpg)
Fig. 6. Anti-CD11d mAb-treatment increases myelin in the injured cord after SCI. Solochrome cyanin-stained sections taken at 6 weeks after T4 SCI are shown at the
lesion epicenter and at 2.0mm caudal to the epicenter in control and mAb-treated rats (a). Arrows on photomicrographs at the epicenter indicate patches of intact dark
blue compact myelin. Note the more intact neuropil at 2mm caudal to the injury site in the rat treated with anti-CD11d mAb, reflected by more abundant compact myelin
and a smaller cavitation than in the control rat. Calibration bar equals 200mm and applies to all photomicrographs. Treatment effects on normalized areas of compact
myelin are illustrated after SCI at T4 (b, 2 weeks; c, 6 weeks). Myelin was stained with luxol fast blue in b and solochrome cyanin in c. & control rats (b, n ¼ 10; c, n ¼ 5).
’ mAb-treated rats (b, n ¼ 8; c, n ¼ 7). *Po0.05 compared to control rats. +shortest distance where area is larger than area at epicenter, Po0.05. Reprinted with
permission from Gris et al. (2004) copyright 2004 by the Society for Neuroscience.
257
![Page 14: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/14.jpg)
Fig. 7. Longitudinal section of rat lumbar (L2) spinal cord illustrating fibers immunoreactive for 5-HT (serotonin, green) streaming
from the spared white matter bundle at the edge of the spinal cord caudal to a clip-compression SCI at the 12th thoracic segment. This
section shows the abundance of these fibers at 4 weeks after cord injury in a rat that had been treated with the anti-CD11d mAb. Fibers
extend to the edge of the gray matter (bottom of illustration) and appear to surround sympathetic preganglionic neurons in the
intermediolateral cell column. The inset shows these lateral horn neurons stained for neurofilament immunoreactivity (red) with fibers
and possible terminals on their somata. This response suggests that axons spared by the anti-CD11d mAb treatment produced
collateral sprouting branches directed toward the preganglionic neurons and possibly innervating them. Calibration bar ¼ 50mm (inset
10 mm).
258
![Page 15: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/15.jpg)
259
gray and white matter was also significantlyincreased, indicative of neuronal sparing. Theimprovement in dysreflexia evoked by colondistension did not relate to effects on the CGRP-immunoreactive primary afferent arbor. No treat-ment effects on this arbor were found in the dorsalhorn of the lumbar spinal cord, the segmentsmediating the afferent input from colon distension(Gris et al., 2005). Remarkably, the afferent arborat T9, caudal to the injury site, actually had agreater area in antibody-treated than control rats.This presumably reflected the tissue sparing in thedorsal horn as the treated rats had almost intactdorsal horns, whereas the controls had significantsecondary tissue damage that extended from T4 toT9. This change would not have impacted ondysreflexia initiated from the colon but might haveaffected dysreflexia evoked from the mid-thoracicregion. This relationship was not assessed in ourstudy, as we did not anticipate the effect near thelesion. However, other than effects due to tissuesparing, the anti-integrin antibody treatmentdid not alter the CGRP-immunoreactive arbor.Instead effects appeared to be caused by retentionof some descending control of spinal neurons.
In a different study of effects of the anti-CD11dantibody treatment (Oatway et al., 2005), wefound that it led to extensive sprouting of de-scending serotonergic axons that passed throughthe margins of the lesion. These axons were par-ticularly attracted to the intermediolateral cell col-umn, forming masses of projections to this area(Fig. 7). The projections provided restored, evenenhanced, bulbospinal serotonergic inputs to thepreganglionic neurons caudal to the injury site. Asthis study concerned only the injury and responsesof the lower thoracic and lumbar cord, it wouldnot have affected autonomic dysreflexia and wecan only speculate that the same phenomenonwould occur after a mid-thoracic injury, leading toenhanced serotonergic input to all preganglionicneurons caudal to the injury site. In summary,blocking inflammation with a selective, transientapproach, which does not impair later woundhealing actions of leukocytes, markedly decreasedthe development of autonomic dysreflexia, bymechanisms that appear to be related to preserva-tion or sprouting of spared descending pathways.
This approach has significant clinical promise as italso has beneficial effects on motor function andthe development of neuropathic pain (Gris et al.,2004; Oatway et al., 2005).
In conclusion, SCI leads to a host of changeswithin the injured cord that promote pathologicalsecondary outcomes such as autonomic dysreflex-ia. Although neurotrophic factors are useful andprobably necessary for the process of regenerationof injured tracts and neurons, NGF does not ap-pear to be a good candidate for this task as itclearly contributes to secondary maladaptive dis-orders. Likewise, inflammation is a necessary partof healing but, in the CNS, inflammation cancause great damage that is not readily reversed.Therefore, the inflammatory response to cordinjury also is an ideal target for manipulation tomaintain its useful functions while limiting itscapacity to cause destructive or maladaptiveresponses. Autonomic dysreflexia is one of manysecondary consequences of cord injury such asbladder and sexual dysfunction, chronic pain,and muscle spasticity. Understanding the mecha-nisms of autonomic dysreflexia and developmentof treatments to prevent its development may im-pact on many of these disabling secondarydisorders.
Acknowledgments
This research was supported by grants from theCanadian Institutes of Health Research, TheHeart and Stroke Foundation of Ontario(T4053) and The Ontario Neurotrauma Founda-tion. The authors wish to acknowledge that part ofthe research reviewed in this chapter was conduct-ed by previous postdoctoral fellows and graduatestudents, Dr. Andrei Krassioukov, Dr. DmitryMayorov, Dr. Natalie Krenz, Dr. Sharon Wong,Mr. Aly Cassam, Ms. Mary-Jo Ricci and Mr.Mark Oatway. We also are indebted to our pastand present excellent technical staff, Mrs. BarbaraAtkinson, Ms. Yuhua Chen, Ms. Eilis Hamilton,Ms. Leyana Saville and Mrs. Carmen Simedreawho have been essential to this research.
![Page 16: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/16.jpg)
260
References
Agrawal, S.K. and Fehlings, M.G. (1996) Mechanisms of
secondary injury to spinal cord axons in vitro role Na+,
Na+–K+–ATPase, the Na+–H+ exchanger, and the
Na+–Ca+ exchanger. J. Neurosci., 16(2): 545–552.
Agrawal, S.K. and Fehlings, M.G. (1997a) Role of NMDA and
non-NMDA ionotropic glutamate receptors in traumatic
spinal cord axonal injury. J. Neurosci., 17(3): 1055–1063.
Agrawal, S.K. and Fehlings, M.G. (1997b) The effect of the
sodium channel blocker QX-314 on recovery after acute
spinal cord injury. J. Neurotrauma, 14: 81–88.
Agrawal, S.K., Theriault, E. and Fehlings, M.G. (1998) Role of
group I metabotropic glutamate receptors in traumatic spinal
cord white matter injury. J. Neurotrauma, 15: 929–941.
Bakhit, C., Armanini, M., Wong, W.L.T., Bennett, G.L. and
Wrathall, J.R. (1991) Increase in nerve growth factor-like
immunoreactivity and decrease in choline acetyltransferase
following contusive spinal cord injury. Brain Res., 554:
264–271.
Bandtlow, C.E., Meyer, M., Lindholm, D., Spranger, M.,
Heumann, R. and Thoenen, H. (1990) Regional and cellular
codistribution of interleukin 1 beta and nerve growth factor
mRNA in the adult rat brain: possible relationship to the
regulation of nerve growth factor synthesis. J. Cell Biol., 111:
1701–1711.
Bao, F., Chen, Y., Dekaban, G.A. and Weaver, L.C. (2004a)
An anti-CD11d integrin antibody reduces cyclooxygenase-2
expression and protein and DNA oxidation after spinal cord
injury in rats. J. Neurochem., 90: 1194–1204.
Bao, F., Chen, Y., Dekaban, G.A. and Weaver, L.C. (2004b)
Early anti-inflammatory treatment reduces lipid peroxidation
and protein nitration after spinal cord injury in rats.
J. Neurochem., 88: 1335–1344.
Bethea, J.R. and Dietrich, W.D. (2002) Targeting the host in-
flammatory response in traumatic spinal cord injury. Curr.
Opin. Neurol., 15(3): 355–360.
Bevilacqua, M.P. (1993) Endothelial-leukocyte adhesion mol-
ecules. Ann. Rev. Immunol., 11: 767–804.
Blackmer, J. (2003) Rehabilitation medicine: 1. Autonomic
dysreflexia. CMAJ, 169: 931–935.
Blight, A.R. (1985) Delayed demyelination and macrophage
invasion: a candidate for ‘‘secondary’’ cell damage in spinal
cord injury. Central Nervous System Trauma, 2: 299–315.
Brown, A., Ricci, M.-J. and Weaver, L.C. (2004) NGF message
and protein distribution in the injured rat spinal cord. Exp.
Neurol., 188: 115–127.
Bullock, E.D. and Johnson, E.M. (1996) Nerve growth factor
induces the expression of certain cytokine genes and bcl-2 in
mast cells. Potential role in survival promotion. J. Biol.
Chem., 271: 27500–27508.
Cabot, J., Alessi, V., Carroll, J. and Ligorio, M. (1994) Spinal
cord lamina V and lamina VII interneuronal projections to
sympathetic preganglionic neurons. J. Comp. Neurol., 347:
515–530.
Calaresu, F.R. and Yardley, C.P. (1988) Medullary basal sym-
pathetic tone. Ann. Rev. Physiol., 50: 511–524.
Cameron, A.A., Smith, G.M., Randall, D.C., Brown, D.R. and
Rabchevsky, A.G. (2003) Effects of nerve growth factor over-
expression on autonomic dysreflexia after spinal cord injury.
J. Neurotrauma, 20: 1086.
Cassam, A.K., Llewellyn-Smith, I.J. and Weaver, L.C. (1997)
Catecholamine enzymes and neuropeptides are expressed in
fibres and somata in the intermediate grey matter in chronic
spinal rats. Neuroscience, 78: 829–841.
Cassam, A.K., Rogers, K.A. and Weaver, L.C. (1999) Co-
localization of substance P and dopamine b-hydroxylase withgrowth associated protein-43 is lost caudal to a spinal cord
transection. Neuroscience, 88: 1275–1288.
Clarke, H.A., Dekaban, G.A. and Weaver, L.C. (1998) Iden-
tification of lamina V and VII interneurons presynaptic to
adrenal sympathetic preganglionic neurons in rats using a
recombinant herpes simplex virus type 1. Neuroscience, 85:
863–872.
Coote, J.H., Downman, C.B.B. and Weber, W.V. (1969) Reflex
discharges into thoracic white rami elicited by somatic and
visceral afferent excitation. J. Physiol., 202: 147–159.
Corbett, J.L., Debarge, O., Frankel, H.L. and Mathias, C.
(1975) Cardiovascular responses in tetraplegic man to muscle
spasm, bladder percussion and head-up tilt. Clin. Exp.
Pharmacol. Physiol., Suppl., 2: 189–193.
Dembowsky, K., Czachurski, J., Amendt, K. and Seller, H.
(1978) Tonic, supraspinal, monoaminergic inhibition on spi-
nal somato-sympathetic reflexes. Pflugers Arch., 373: R76.
Dembowsky, K., Czachurski, J., Amendt, K. and Seller, H.
(1980) Tonic descending inhibition of the spinal somato-
sympathetic reflex from the lower brain stem. J. Auton. Nerv.
Syst., 2: 157–182.
Erickson, R.P. (1980) Autonomic hyperreflexia: pathophysiol-
ogy and medical management. Arch. Phys. Med. Rehabil.,
61: 431–440.
Fehlings, M.G., Tator, C.H. and Linden, R.D. (1989) The ef-
fect of nimodipine and dextran on axonal function and blood
flow following experimental spinal cord injury. J. Neurosurg.,
71: 403–416.
Giannantoni, A., Di, S.S., Scivoletto, G., Mollo, A., Silecchia,
A., Fuoco, U. and Vespasiani, G. (1998) Autonomic
dysreflexia during urodynamics. Spinal Cord, 36: 756–760.
Grayson, M.H., Van der Vieren, M., Sterbinsky, S.A., Gallantin,
W.M., Hoffman, P., Staunton, D. and Bochner, B.S. (1999)
alphadbeta2 integrin is a ligand for vascular cell adhesion
molecule-1. Int. Arch. Allergy Immunol., 118(2–4): 263–264.
Gris, D., Marsh, D.R., Oatway, M.A., Chen, Y., Hamilton,
E.F., Dekaban, G.A. and Weaver, L.C. (2004) Transient
blockade of the CD11d/CD18 integrin reduces secondary
damage after spinal cord injury, improving sensory, auto-
nomic, and motor function. J. Neurosci., 24: 4043–4051.
Gris, D., Marsh, D.R., Dekaban, G.A. and Weaver, L.C.
(2005). Comparison of methylprednisolone and anti-CD11d
antibody treatments on autonomic dysreflexia after spinal
cord injury. Exp. Neurol.
Guttman, F.L. and Whitteridge, D. (1947) Effects of bladder
distention on autonomic mechanisms after spinal cord inju-
ries. Brain, 70: 361–404.
![Page 17: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/17.jpg)
261
Hayashi, M., Ueyama, T., Nemoto, K., Tamaki, T. and
Senba, E. (2000) Sequential mRNA expression for
immediate early genes, cytokines, and neurotrophins in
spinal cord injury. J. Neurotrauma, 17: 203–218.
Heese, K., Fiebich, B.L., Bauer, J. and Otten, U. (1998a)
NF-kappaB modulates lipopolysaccharide-induced micro-
glial nerve growth factor expression. Glia, 22: 401–407.
Heese, K., Hock, C. and Otten, U. (1998b) Inflammatory sig-
nals induce neurotrophin expression in human microglial
cells. J. Neurochem., 70: 699–707.
Heumann, R., Korsching, S., Bandtlow, C. and Thoenen, H.
(1987a) Changes of nerve growth factor synthesis in non-
neuronal cells in response to sciatic nerve transection. J. Cell
Biol., 104: 1623–1631.
Heumann, R., Lindholm, D., Bandtlow, C., Meyer, M.,
Radeke, M.J., Misko, T.P., Shooter, E. and Thoenen, H.
(1987b) Differential regulation of mRNA encoding nerve
growth factor and its receptor in rat sciatic nerve during
development, degeneration, and regeneration: role of
macrophages. Proc. Natl. Acad. Sci. USA, 84: 8735–8739.
Jacob, J.E., Gris, P., Fehlings, M.G., Weaver, L.C. and Brown,
A. (2003) Autonomic dysreflexia after spinal cord transection
and compression in 129Sv, C57BL and wallerian degenera-
tion slow mutant mice. Exp. Neurol., 183: 136–146.
Jacob, J.E., Pniak, A., Weaver, L.C. and Brown, A. (2001)
Autonomic dysreflexia in a mouse model of spinal cord
injury. Neuroscience, 108: 687–693.
Jones, L.L., Yamaguchi, Y., Stallcup, W.B. and Tuszynski,
M.H. (2002) NG2 is a major chondroitin sulfate proteogly-
can produced after spinal cord injury and is expressed by
macrophages and oligodendrocyte progenitors. J. Neurosci.,
22: 2792–2803.
Joshi, S., LeVatte, M.A., Dekaban, G.A. andWeaver, L.C. (1995)
Identification of spinal interneurons antecedent to adrenal
sympathetic preganglionic neurons using trans-synaptic trans-
port of herpes simplex virus type 1. Neuroscience, 65: 893–903.
Ju, G., Hokfelt, T., Brodin, E., Fahrenkrug, J., Fischer, J.A.,
Frey, P., Elde, R.P. and Brown, J.C. (1987) Primary sensory
neurons of the rat showing calcitonin gene-related peptide
immunoreactivity and their relation to substance P-,
somatostatin-, galanin-, vasoactive intestinal polypeptide-
and cholecystokinin-immunoreactive ganglion cells. Cell
Tissue Res., 247: 417–431.
Karlsson, A.-K. (1999) Autonomic dysreflexia. Spinal Cord, 37:
383–391.
Karlsson, A.-K., Friden, P.M., Lonnroth, P., Sullivan, L. and
Elam, M. (1998) Regional sympathetic function in high
spinal cord injury during mental stress and autonomic
dysreflexia. Brain, 121: 1711–1719.
Koizumi, K. and Brooks, C.M. (1972) The integration of
autonomic system reactions: a discussion of autonomic
reflexes, their control and their association with somatic
reflexes. In: Adrian R.H., Helmrich E., Holzer H., Jung R.,
Kramer K., Krayer O., Lynen F., Miescher P.A., Rasmussen
H., Renold A.E., Trendelenburg U., Ullrich K., Vogt W. and
Weber A. (Eds.), Reviews of Physiology: Biochemistry and
Experimental Pharmacology. Springer, Berlin, pp. 1–68.
Koyanagi, I., Tator, C.H. and Lea, P.J. (1993a) Three-dimen-
sional analysis of the vascular system in the rat spinal cord
with scanning electron microscopy of vascular corrosion
casts. Part 2: Acute spinal cord injury. Neurosurgery, 33:
285–291.
Koyanagi, I., Tator, C.H. and Theriault, E. (1993b) Silicone
rubber microangiography of acute spinal cord injury in the
rat. Neurosurgery, 32: 260–268.
Krassioukov, A.V., Bunge, M.B., Puckett, W.R. and Bygrave,
M.A. (1999) The changes in human spinal sympathetic
preganglionic neurons after spinal cord injury. Spinal Cord,
37: 6–13.
Krassioukov, A.V., Furlan, J.C. and Fehlings, M.G. (2003)
Autonomic dysreflexia in acute spinal cord injury: an under-
recognized clinical entity. J. Neurotrauma, 20: 707–716.
Krassioukov, A.V., Johns, D.G. and Schramm, L.P. (2002)
Sensitivity of sympathetically correlated spinal interneurons,
renal sympathetic nerve activity, and arterial pressure to so-
matic and visceral stimuli after chronic spinal injury.
J. Neurotrauma, 19: 1521–1529.
Krassioukov, A.V. and Weaver, L.C. (1995) Episodic
hypertension due to autonomic dysreflexia in acute and
chronic spinal cord-injured rats. Am. J. Physiol., 268:
H2077–H2083.
Krassioukov, A.V. and Weaver, L.C. (1996) Morphological
changes in sympathetic preganglionic neurons after spinal
cord injury in rats. Neuroscience, 70: 211–226.
Krenz, N.R., Meakin, S.O., Krassioukov, A.V. and Weaver,
L.C. (1999) Neutralizing intraspinal nerve growth factor
blocks autonomic dysreflexia caused by spinal cord injury.
J. Neurosci., 19(17): 7405–7414.
Krenz, N.R. and Weaver, L.C. (1998a) Changes in the mor-
phology of sympathetic preganglionic neurons parallel the
development of autonomic dysreflexia after spinal cord injury
in rats. Neurosci. Lett., 243: 61–64.
Krenz, N.R. and Weaver, L.C. (1998b) Sprouting of primary
afferent fibers after spinal cord transection in the rat.
Neuroscience, 85: 443–458.
Krenz, N.R. and Weaver, L.C. (2000) Nerve growth factor in
glia and inflammatory cells of the injured rat spinal cord.
J. Neurochem., 74: 730–739.
Landrum, L.M., Thompson, G.M. and Blair, R.W. (1998) Does
postsynaptic a1-adrenergic receptor supersensitivity contrib-
ute to autonomic dysreflexia? Am. J. Physiol., 274:
1090–1098.
LaSala, A., Corinti, S., Federici, M., Saragovi, H.U. and
Girolomoni, G. (2000) Ligand activation of nerve growth
factor receptor TrkA protects monocytes from apoptosis.
J. Leukoc. Biol., 68: 104–110.
Lawson, S.N., McCarthy, P.W. and Prabhakar, E. (1996)
Electrophysiological properties of neurones with CGRP-like
immunoreactivity in rat dorsal root ganglia. J. Comp. Ne-
urol., 365: 355–366.
Lawson, S.N., Perry, M.J., Prabhakar, E. and McCarthy, P.W.
(1993) Primary sensory neurones: neurofilament,
neuropeptides, and conduction velocity. Brain Res. Bull.,
30: 239–243.
![Page 18: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/18.jpg)
262
Lee, B.Y., Karmakar, M.G., Herz, B.L. and Sturgill, R.A.
(1994) Autonomic dysreflexia revisited. J. Spinal Cord Med.,
18: 75–87.
Leskovar, A., Moriarty, L.J., Turek, J.J., Schoenlein, I.A. and
Borgens, R.B. (2000) The macrophage in acute neural injury:
changes in cell numbers over time and levels of cytokine
production in mammalian central and peripheral nervous
systems. J. Exp. Biol., 203(Part 12): 1783–1795.
Lindan, R., Joiner, E., Freehafer, A.A. and Hazel, C. (1980)
Incidence and clinical features of autonomic dysreflexia in
patients with spinal cord injury. Paraplegia, 18: 285–292.
Lindholm, D., Heumann, R., Meyer, M. and Thoenen, H. (1987)
Interleukin-1 regulates synthesis of nerve growth factor in
non-neuronal cells of rat sciatic nerve. Nature, 330: 658–659.
Llewellyn-Smith, I.J. and Weaver, L.C. (2001) Changes in
synaptic inputs to sympathetic preganglionic neurons after
spinal cord injury. J. Comp. Neurol., 435: 226–240.
Mabon, P.J., Weaver, L.C. and Dekaban, G.A. (2000) Inhibi-
tion of monocyte/macrophage migration to a spinal cord in-
jury site by an antibody to the integrin alphaD: a potential
new anti-inflammatory treatment. Exp. Neurol., 166: 52–64.
Maiorov, D.N., Fehlings, M.G. and Krassioukov, A.V. (1998)
Relationship between severity of spinal cord injury and ab-
normalities in neurogenic cardiovascular control in conscious
rats. J. Neurotrauma, 15(5): 365–374.
Maiorov, D.N., Krenz, N.R., Krassioukov, A.V. and Weaver,
L.C. (1997a) Role of spinal NMDA and AMPA receptors in
episodic hypertension in conscious spinal rats. Am. J.
Physiol., 273: H1266–H1274.
Maiorov, D.N., Weaver, L.C. and Krassioukov, A.V. (1997b)
Relationship between sympathetic activity and arterial pres-
sure in conscious spinal rats. Am. J. Physiol., 272:
H625–H631.
Marsh, D.R. and Weaver, L.C. (2004) Autonomic dysreflexia,
induced by noxious or innocuous stimulation, does not de-
pend on changes in dorsal horn substance P. J. Neurotrauma,
21: 817–828.
Marsh, D.R., Wong, S.T., Meakin, S.O., MacDonald, J.I.S.,
Hamilton, E.F. and Weaver, L.C. (2002) Neutralizing intra-
spinal NGF with a trkA-IgG fusion protein blocks develop-
ment of autonomic dysreflexia in a clip-compression model of
spinal cord injury. J. Neurotrauma, 19: 1531–1542.
Mathias, C.J. and Frankel, H.L. (1992a) Autonomic distur-
bances in spinal cord lesions. In: Mathias C.J. and Bannister
R. (Eds.) Autonomic Failure A Textbook of Clinical Disor-
ders of the Autonomic Nervous System, Vol. 4(51). Oxford
University Press, Oxford, pp. 494–513.
Mathias, C.J. and Frankel, H.L. (1992b) Autonomic distur-
bances in spinal cord lesions. In: Bannister R. and Mathias
C.J. (Eds.) Autonomic Failure, a Textbook of Clinical Dis-
orders of the Autonomic Nervous System, Vol. 3(43). Oxford
Medical Publications, Oxford, UK, pp. 839–881.
Mathias, C.J. and Frankel, H.L. (1992c) The cardiovascular
system in tetraplegia and paraplegia. In: Frankel H.L. (Ed.)
Handbook of Clinical Neurology, Vol. 17(25). Elsevier
Science Publishers, B.V., Amsterdam, The Netherlands,
pp. 435–456.
Mayorov, D.N., Adams, M.A. and Krassioukov, A.V. (2001)
Telemetric blood pressure monitoring in conscious rats be-
fore and after compression injury of spinal cord. J. Neuro-
trauma, 18: 727–736.
McCarthy, P.W. and Lawson, S.N. (1990) Cell type and con-
duction velocity of rat primary sensory neurons with ca-
lcitonin gene-related peptide-like immunoreactivity.
Neuroscience, 34: 623–632.
Naftchi, N.E. (1990) Mechanism of autonomic dysreflexia;
contributions of cathecholamine and peptide neurotransmit-
ters. Ann. NY Acad. Sci., 579: 133–148.
Naftchi, N.E. and Richardson, J.S. (1997) Autonomic dysreflexia:
pharmacological management of hypertensive crises in spinal
cord injured patients. J. Spinal. Cord. Med., 20: 355–360.
Neish, A.S., Read, M.A., Thanos, D., Pine, R., Maniatis, T.
and Collins, T. (1995) Endothelial interferon regulatory fac-
tor 1 cooperates with NF-kappa B as a transcriptional ac-
tivator of vascular cell adhesion molecule 1. Mol. Cell Biol.,
15(5): 2558–2569.
Oatway, M.A., Chen, Y., Bruce, J.C., Dekaban, G.A. and
Weaver, L.C. (2005) An anti-CD11d integrin antibody treat-
ment restores normal serotonergic projections to the dorsal,
intermediate and ventral horns of the injured spinal cord.
J. Neurosci., 25: 637–647.
Osborn, J.W., Taylor, R.F. and Schramm, L.P. (1990) Chronic
cervical spinal cord injury and autonomic hyperreflexia in
rats. Am. J. Physiol., 258: R169–R174.
Popovich, P.G., Guan, Z., Wei, P., Huitinga, I., van Rooijen,
N. and Stokes, B.T. (1999) Depletion of hematogenous ma-
crophages promotes partial hindlimb recovery and neuroan-
atomical repair after experimental spinal cord injury. Exp.
Neurol., 158: 351–365.
Popovich, P.G., Wei, P. and Stokes, B.T. (1997) Cellular in-
flammatory response after spinal cord injury in Sprague–Da-
wley and Lewis rats. J. Comp. Neurol., 377: 443–464.
Price, J. (1985) An immunohistochemical and quantitative ex-
amination of dorsal root ganglion neuronal subpopulations.
J. Neurosci., 5(8): 2051–2059.
Rodenbaugh, D.W., Collins, H.L. and DiCarlo, S.E. (2003)
Increased susceptibility to ventricular arrhythmias in hyper-
tensive paraplegic rats. Clin. Exp. Hypertens., 25: 349–358.
Saporito, M.S., Wilcox, H.M., Hartpence, K.C., Lewis, M.E.,
Vaught, J.L. and Carswell, S. (1993) Pharmacological induc-
tion of nerve growth factor mRNA in adult rat brain. Exp.
Neurol., 123: 295–302.
Saragovi, H.U. and Gehring, K. (2000) Development of phar-
macological agents for targeting neurotrophins and their re-
ceptors. Trends Pharmacol. Sci., 21: 93–98.
Sato, A. and Schmidt, R.F. (1973) Somatosympathetic reflexes:
afferent fibers, central pathways, discharge characteristics.
Physiol. Rev., 53(4): 916–947.
Saville, L.R., Pospisil, C.H., Mawhinney, L.A., Bao, F.,
Simedria, F.C., Peters, A.A., O’Connell, P.J., Weaver, L.C.
and Dekaban, G.A. (2004) A monoclonal antibody to
CD11d reduces the inflammatory infiltrate into the injured
spinal cord: a potential neuroprotective treatment. J. Ne-
uroimmunol., 156: 42–57.
![Page 19: [Progress in Brain Research] Autonomic Dysfunction After Spinal Cord Injury Volume 152 || Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention](https://reader031.pdfslide.net/reader031/viewer/2022030200/5750a2aa1a28abcf0c9ce472/html5/thumbnails/19.jpg)
263
Schumacher, P.A., Eubanks, J.H. and Fehlings, M.G. (1999)
Increased calpain I-mediated proteolysis and preferential loss
of dephosphorylated NF200, following traumatic spinal cord
injury. Neuroscience, 91: 733–744.
Shanley, T.P., Warner, R.L., Crouch, L.D., Dietsch, G.N.,
Clark, D.L., O’Brien, M.M., Gallatin, W.M. and Ward, P.A.
(1998) Requirements for ad in IgG immune complex-induced
rat lung injury. J. Immunol., 160: 1014–1020.
Shea, J.D., Gioffre, R., Carrion, H. and Small, M.P. (1973)
Autonomic hyperreflexia in spinal cord injury. Southern
Med. J., 66(8): 869–872.
Spranger, M., Lindholm, D., Bandtlow, C., Heumann, R.,
Gnahn, H., Naher-Noe, M. and Thoenen, H. (1990) Regu-
lation of nerve growth factor (NGF) synthesis in the rat
central nervous system: comparison between the effects of
interleukin-1 and various growth factors in astrocyte cultures
and in vivo. Eur. J. Neurosci., 2: 69–76.
Streit, W.J., Semple-Rowland, S.L., Hurley, S.D., Miller, R.C.,
Popovich, P.G. and Stokes, B.T. (1998) Cytokine mRNA
profiles in contused spinal cord and axotomized facial nu-
cleus suggest a beneficial role for inflammation and gliosis.
Exp. Neurol., 152: 74–87.
Taoka, Y. and Okajima, K. (1998) Spinal cord injury in the rat.
Prog. Neurobiol., 56: 341–358.
Taoka, Y., Okajima, K., Uchiba, M., Murakami, K.,
Kushimoto, S., Johno, M., Naruo, M., Okabe, H. and
Takatsuki, K. (1997) Role of neutrophils in spinal cord injury
in the rat. Neuroscience, 79(4): 1177–1182.
Tator, C.H. and Fehlings, M.G. (1991) Review of the secondary
injury theory of acute spinal cord trauma with emphasis on
vascular mechanisms. J. Neurosurg., 75: 15–26.
Vaidyanathan, S., Soni, B.M., Sett, P., Watt, J.W.H., Oo, T.
and Bingley, J. (1998) Pathophysiology of autonomic
dysreflexia: long-term treatment with terazosin in adult and
paediatric spinal cord injury patients manifesting recurrent
dysreflexic epidsodes. Spinal Cord, 36: 761–770.
Van der Vieren, M., Crowe, D.T., Hoekstra, D., Vazeux, R.,
Hoffman, P.A., Grayson, M.H., Bochner, B.S., Gallatin,
W.M. and Staunton, D.E. (1999) The leukocyte integrin
aDb2 binds VCAM-1: evidence for a binding interface be-
tween I domain and VCAM-1. J. Immunol., 163: 1984–1990.
Vizzard, M.A., Brisson, M. and De Groat, W.C. (2000)
Transneuronal labeling of neurons in the adult rat central
nervous system following inoculation of pseudorabies virus
into the colon. Cell Tissue Res., 299(1): 9–26.
Wallace, M.C. and Tator, C.H. (1986) Spinal cord blood flow
measured with microspheres following spinal cord injury in
the rat. Can. J. Neurol. Sci., 13: 91–96.
Wallace, M.C., Tator, C.H. and Frazee, P. (1986) Relationship
between posttraumatic ischemia and hemorrhage in the in-
jured rat spinal cord as shown by colloidal carbon angio-
graphy. Neurosurgery, 18: 433–439.
Weaver, L.C., Cassam, A.K., Krassioukov, A.V. and
Llewellyn-Smith, I.J. (1997) Changes in immunoreactivity
for growth associated protein-43 suggest reorganization of
synapses on spinal sympathetic neurons after cord transec-
tion. Neuroscience, 81: 535–551.
Weaver, L.C., Marsh, D.R., Gris, D., Meakin, S.O. and
Dekaban, G.A. (2001a) Central mechanisms for autonomic
dysreflexia after spinal cord injury. In: McKerracher L.,
Douchet D. and Rossignol S. (Eds.) Progress in Brain Re-
search, Vol. 7. Elsevier Science B.V., Amsterdam, pp. 83–95.
Weaver, L.C., Verghese, P., Bruce, J.C., Fehlings, M.G., Krenz,
N.R. and Marsh, D.R. (2001b) Autonomic dysreflexia and
primary afferent sprouting after clip-compression injury of
the rat spinal cord. J. Neurotrauma, 18: 1107–1119.
Wong, S.T., Atkinson, B.A. and Weaver, L.C. (2000) Confocal
microscopic analysis of sprouting small-diameter primary af-
ferent fibres after spinal cord injury. Neurosci. Lett., 296:
65–68.
Yeoh, M., McLachlan, E.M. and Brock, J.A. (2004) Chronic
decentralization potentiates neurovascular transmission in
the isolated rat tail artery, mimicking the effects of spinal
transection. J. Physiol., 561: 583–596.
Young, W. (1993) Secondary injury mechanisms in acute spinal
cord injury. J. Emerg. Med., 11: 13–22.