-
UNIVERSITY OF ZAMBIAINSTITUTE FOR HEALTH METRICS AND
EVALUATIONUNIVERSITY OF WASHINGTON
Assessing Impact, Improving HealthProgress in Child Health
Across Districts in ZambiaA REPORT OF THE MCPA PROJECT
-
This report was prepared by the Institute for Health Metrics and
Evaluation (IHME) and the Department of Economics at the University
of Zambia (UNZA). This work is intended to provide in-formation on
levels and trends in under-5 mortality and coverage of key child
health interventions across districts in Zambia. The estimates may
change following peer review. The contents of this publication may
not be reproduced in whole or in part without permission from
IHME.
Institute for Health Metrics and Evaluation2301 Fifth Ave.,
Suite 600Seattle, WA 98121USA
Telephone: +1-206-897-2800Fax: +1-206-897-2899Email:
comms@healthmetricsandevaluation.orgwww.healthmetricsandevaluation.org
Printed in the United States 2014 Institute for Health Metrics
and Evaluation
-
1TABLE OF CONTENTS3 Acronyms
4 Termsanddefinitions
5 Executivesummary
6 Introduction
8 Mainfindings
12 Conclusionsandpolicyimplications
13 References
14 Annex1.OverviewoftheMCPAanalyticalapproachandmethods
15 Districtprofiles
17 Centralprovince
31 Copperbeltprovince
53 Easternprovince
71 Luapulaprovince
87 Lusakaprovince
97 Northernprovince
123 North-westernprovince
139 Southernprovince
163 Westernprovince
AssessingImpact,ImprovingHealthProgress in Child Health Across
Districts in ZambiaA REPORT OF THE MCPA PROJECT
-
2ABOUT IHME
ACKNOWLEDGMENTS
ABOUT THIS REPORT
The Institute for HealthMetrics and Evaluation (IHME) is
anindependentglobalhealth researchcenterat
theUniversityofWashington thatprovides
rigorousandcomparablemea-surementoftheworldsmostimportanthealthproblemsandevaluates
thestrategiesused toaddress them.
IHMEmakesthisinformationfreelyavailablesothatpolicymakershavetheevidencetheyneedtomakeinformeddecisionsabouthowtoallocateresourcestobestimprovepopulationhealth.
To express interest in collaborating or request
furtherinformationontheMalariaControlPolicyAssessment(MCPA)projectinZambia,pleasecontactIHMEat:
InstituteforHealthMetricsandEvaluation2301FifthAve.,Suite600Seattle,WA98121USA
Telephone:+1-206-897-2800Fax:+1-206-897-2899E-mail:comms@healthmetricsandevaluation.orgwww.healthmetricsandevaluation.org
Assessing Impact, Improving Health: Progress in Child Health
Across Districts in Zambia provides the most up-to-date
re-sultsfromtheMCPAprojectinZambia,includingdistrict-leveltrendsforarangeofindicatorsandtheimpactofmalariacon-trolandotherchildhealthinterventionsonunder-5mortality.Thisreportexpandsuponthe2011reportproducedbyIHMEand
the University of Zambia (UNZA), Maternal and Child Health
Intervention Coverage in Zambia: the Heterogeneous Picture.
TheMCPAprojectwasledbyEmmanuelaGakidouatIHMEandFelixMasiye
atUNZA.Data collationwasprimarily con-
ductedbyPeterHangomaandPeterMulenga,researchersattheDepartmentofEconomicsatUNZA,andFrankKukungaattheCentralStatisticalOffice(CSO).Trendsinunder-5mortalitywereproducedbyLauraDwyer-Lindgrenat
IHME,withcon-tributionsfromCaseyOlivesoftheUniversityofWashington.AtIHME,interventioncoverageanalyseswereconductedbyK.EllicottColson,withcontributions
fromLauraDwyer-Lind-gren, Tom Achoki, Nancy Fullman, and Matthew
Schneider(nowatUSAID).ThecausalattributionanalysiswasperformedbyMarieNgandK.EllicottColson.ThisreportwaswrittenbyNancyFullman,withcontributionsfromWilliamHeisel.
TheMCPAproject inZambia isacollaborationbetween
theDepartmentofEconomicsatUNZAand IHMEat
theUniver-sityofWashington.ThisprojecthasbenefitedgreatlyfromkeyinputsandsupportfromtheMinistryofHealth(MOH),theNa-tionalMalariaControlCentre(NMCC),CSO,andtheChurchesHealthAssociationofZambia(CHAZ),inZambia.Wearemostgratefultotheseorganizations,especiallyfortheirwillingnessto
facilitate data access and provide crucial content knowl-edge.
We thank the MCPA Advisory Group, which consists
ofinternationalandlocalstakeholderswhocontributedtowardrefining the
projects research concept and
framework.WealsothanktheMalariaControlandEvaluationPartnership
in
Africa(MACEPA)teaminZambiaforfacilitatingdataaccess.AtIHME,wewishtothankHeatherBonander,AnnieHaakenstad,andKelseyPierce
formanaging theproject; PatriciaKiyonoformanaging theproductionof
this report; BrianChildress, Adrienne Chew, and KateMuller for
editorial support; andRyanDiazandAnnKumasaka forgraphicdesign.We
thankSepoKusiyoatUNZA foradministrativesupportof
theZam-bianMCPAteam.
Funding for this research came from the Bill
&MelindaGatesFoundation.
-
3Acronyms AIDS AcquiredimmunodeficiencysyndromeANC4
Antenatalcare,aminimumoffourvisitsBCG
BacillusCalmette-GurinvaccineCSO CentralStatisticalOfficeDPT3
Diphtheria-pertussis-tetanusvaccine(threedoses)GPR
GaussianProcessRegressionHIV HumanimmunodeficiencyvirusIHME
InstituteforHealthMetricsandEvaluationIPTp2
Intermittentpreventivetherapyinpregnancy,aminimumoftwodosesIRS
IndoorresidualsprayingITN Insecticide-treatednetJICA
JapanInternationalCooperationAgencyMCPA
MalariaControlPolicyAssessmentMOH MinistryofHealthMSL
MedicalStoresLimitedNMCC NationalMalariaControlCentrePCA
PrincipalcomponentanalysisPMTCT
Preventionofmother-to-childtransmissionofHIVSBA
SkilledbirthattendanceUNZA UniversityofZambia
-
4Terms and definitionsAll-cause under-5 mortality:
theprobability (expressed as the rateper 1,000
livebirths)thatchildrenbornalivewilldiebeforereachingtheageof5years
Antenatal care (ANC4) coverage:
theproportionofwomen15to49yearsoldwhohadfourormoreantenatalvisitsatahealthfacilityduringpregnancy
BCG immunization coverage:
theproportionofchildrenunder5yearsoldwhohavebeenvaccinatedagainsttuberculosis
Childhood underweight: the proportion of children under 5 years
old who aretwo or more standard deviations below the
internationalanthropometric reference population median of weight
forage
DPT3 coverage: the proportion of children 12 to 59 months old
who havereceived three doses of the
diphtheria-pertussis-tetanus(DPT)vaccine
Exclusive breastfeeding coverage: the proportion of children who
were exclusively breastfedduringtheirfirstsixmonthsafterbirth
Indoor residual spraying coverage: the proportion of households
that were sprayed with
aninsecticide-basedsolutioninthelast12months
Insecticide-treated net (ITN): anet treatedwithan
insecticide-basedsolutionthat
isusedforprotectionagainstmosquitosthatcancarrymalaria
Intermittent preventive therapy in pregnancy, two doses (IPTp2):
theproportionofpregnantwomenwhoreceivedatleasttwotreatmentdosesof
Fansidar (sulfadoxine/pyrimethamine)
atantenatalcarevisitsduringpregnancy
Intervention coverage:
theproportionofindividualsorhouseholdswhoreceivedaninterventionthattheyneeded
ITN ownership: theproportionofhouseholdsthatownatleastoneITN
ITN use by children under 5:
theproportionofchildrenunder5yearsoldwhosleptunderanITNthepreviousnight,asreportedbyhouseholdheads
Measles immunization coverage: the proportion of children 12 to
59 months old who havereceivedmeaslesvaccination
Pentavalent immunization coverage: the proportion of children 12
to 59 months old who havereceivedthepentavalentvaccine,which
includesprotectionagainst diphtheria-pertussis-tetanus (DPT),
hepatitis B, andHaemophilus influenzae typeb
Polio immunization coverage: the proportion of children 12 to 59
months old who havereceivedthreedosesoftheoralpoliovaccine
Prevention of mother-to-child transmission of HIV (PMTCT):the
receipt of antiretroviral drugs as prophylaxis to reducethe risk of
mother-to-child transmission of HIV among
HIV-positivepregnantwomen
Skilled birth attendance coverage:
theproportionofpregnantwomen15 to49yearsoldwhodelivered with a
skilled birth attendant (a doctor,
nurse,midwife,orclinicalofficer)
-
5Executive summaryZambiahasseenremarkable improvement
inchildhoodsur-vivaloverthepasttwodecades.Whilethescale-upofmalariacontrol
interventionshasbeenproposedasoneof
thebig-gestdriversbehindthatimprovement,littleresearchhasbeendoneonhowmuchof
the reduction in
childhoodmortalitymaybeattributedtomalariacontrolandhowmuchisthere-sult
of improvements inother childhealth
interventions.Toaddressthisknowledgegap,theUniversityofZambia(UNZA)and
the Institute for Health Metrics and Evaluation (IHME)worked
together on theMalaria Control Policy Assessment(MCPA) project. The
goal ofMCPAwas to harness
existingdatainZambiaanduserigorousstatisticalmethodstoquan-tify the
impact of malaria control and other child
healthinterventionsonunder-5mortalitytrendsacrossdistricts.
Wefoundthatbetween1990and2010,acombinationofrapidlyscaledupchildhealthinterventionscontributedtoanadditional11%ofdeclinesinunder-5mortalityacrossZambia.We
lookedat thecombinedeffectof these interventionsbe-cause the
scale-up in ownership of insecticide-treated
nets(ITNs)anduseofindoorresidualspraying(IRS)coincidedwiththescale-upinthreeotherkeychildhealthinterventions:thepentavalentvaccine,exclusivebreastfeeding,andservicestohelppreventmother-to-child
transmissionofHIV
(PMTCT)athealthfacilities.Isolatingthespecificimpactofeachinterven-tion
isnotpossible.Nevertheless, jointly, these
interventionscontributedsignificantlytothereductionofunder-5mortalitythroughoutthecountry.
TheMCPAprojectinZambiaproduceddistrict-leveltrendsforkeychildhealthoutcomesandinterventionsfrom1990to2010.This
is thefirst time thatannualestimates
forunder-5mortalityandinterventioncoveragehavebeengeneratedatthedistrict
level. In this report,districtprofilesdetail trendsin child health
over time and benchmark the districts per-formance across
indicators.With this information, local
andnationalpolicymakersandhealthofficials can identify
areasofsuccessfulhealthservicedeliveryanddetectearlysignsofdeclininginterventioncoverageorstalledprogress.
This report shows that Zambia is succeeding on
severalfrontsinchildhealth.First,countrywidereductionsinunder-5mortalitywerealsoaccompaniedbyimprovementsinequity
acrossdistricts,assomeofthedistrictswiththehighestmor-talityratesin1990recordedsomeofthegreatestdeclinesby2010.Second,coverageofkeymalariacontrolinterventions,such
as ITN ownership, increased dramatically inmany
dis-tricts.Third,themajorityofdistrictsweresuccessfulinquicklyincreasing
coverage of the pentavalent vaccine after its in-troduction in
2005. Finally, rates of exclusive breastfeedingmarkedly rose in
most districts, reflecting the countrys in-vestments in improving
child nutrition and breastfeedingpractices(WBTi2008).
ThesesuccesseswereaccompaniedbyconcerningtrendsforthreekeychildhealthinterventionsinZambia.First,mostdistrictssawadeclineinthe2000sinantenatalcare(ANC4),which
is theproportionofpregnantwomen15 to49 yearsold who had four or
more visits to a health facility duringpregnancy. This finding is
particularlyworrisomegiven
thatdistrictsgenerallyincreasedlevelsofANC4duringthe1990s.Second,
coverage of polio immunization dropped in someof thedistricts that
are consideredathigh risk forpolio
im-portationfromneighboringcountries.Third,insomeareasofZambia,
skilledbirthattendancedeclined tovery low levels.Targeting these
areas for improvement shouldbe
aprioritytoensurethatthecountrysachievementsinchildhealthcon-tinueintothepresentdecade.
Withafocusondistricts,findingsfromtheMCPAprojectin Zambia
provide side-by-side comparisons of health per-formanceover time,
geography, and intervention type.Thechild health landscape is
remarkably heterogeneous
acrossdistricts,highlightingtheneedforcontinuousandtimelyas-sessmentofdistrict-leveltrends.Withregularlycollectedandanalyzed
district health information, policymakers can
havetheevidencebasetomaketargeted,data-drivendecisionsforachievinggreaterandmoreequitablehealthgainsinZambia.
-
6IntroductionOver the past decade, Zambias child health and
develop-ment landscape has been substantially reshaped by
newprograms, interventions, and priorities, including
extensivemalariacontrolprograms. Inorder to
fullyunderstandwhathascontributedtoZambiasprogress
inunder-5mortality,
itisimportanttocomprehensivelyaccountforalleffortstoim-provechildhealth.
TheMCPAprojectinZambiahadtwomainobjectives:
1) Determine what proportion of the decline in all-causeunder-5
mortality in Zambia was attributable to
thescale-upofmalariacontrolinterventions,whileaccountingfor a range
of other key child health interventions andnon-healthfactors.
2) Assessthisimpactatthedistrictlevelbetween1990and2010.
Inordertoachievetheseobjectives,annualestimatesofdistrict-level
trends from 1990 to 2010 were systematicallygenerated foreachof
the72districts inZambiaandacrossa range of key child health
outcomes and
interventions.Detaileddescriptionsofthefindingsforeachdistrictarepre-sented
in this report.District-leveldatacanbedownloadedfrom IHMEs Global
Health Data Exchange:
http://ghdx.healthmetricsandevaluation.org/.
TheMCPAprojectsoughttouseallavailabledatasources,whicharepresentedinTable1.Theseanalysesaimedtomakefull
useof thebest availabledata in Zambia. Provincial esti-matesof
under-5mortality and intervention
coveragewerepreviouslyavailable,butforthefirsttimedistrict-leveltrendswerederivedfromthesedatasourcesusingrobuststatisticalmethods.Annex1providesanoverviewoftheanalyticalap-proachusedtogeneratetheestimatesinthisreport.
BOX 1MAIN FINDINGS FROM THE MCPA PROJECT IN ZAMBIA
Under-5mortalitysubstantiallydeclinedthroughoutZambiafrom1990to2010.Someofthegreatestprogresswasrecordedindistrictswiththehighestlevelsofunder-5mortalityin1990.
Coverage of malaria control interventions rapidly increased,
especially between 2005 and
2010.ThesegainsincoveragewereobservedthroughoutZambia.
Atthesametimemalariainterventionswerescaledup,Zambiaalsosuccessfullyincreasedlevelsofcoverageforthreenon-malariachildhealthinterventions:thepentavalentvaccine,exclusivebreast-
feeding,andtheavailabilityofPMTCTservicesathealthfacilities.
Together,theserapidlyscaledupinterventionswereresponsibleforan11%reductionintheunder-5mortalityratefrom2000to2010.Sustaininghighcoverageoftheseinterventionsiscriticalforchild
healthinZambia.
Amidstthecountryshealthsuccesses,someworrisometrendsemergedthatwarrantattention.Mostdistrictssawsharpdeclinesinantenatalcarevisitsduringthe2000s,andskilledbirthattendancefell
toverylowlevelsinseveralplaces.Othersexperiencedaminimalscale-upofthepentavalentvaccine,
andsomeofthehigh-riskdistrictsforpolioimportationrecordeddropsinpolioimmunizationcov-
erage.Addressingthesegapsinhealthserviceprovisioniscrucialtomaintainingthecountrysgains
inchildhealth.
-
7Table 1. Data sources used in the MCPA project
Anearlierversionofthisreportwaspublishedin2011,Ma-ternal and
Child Health Intervention Coverage in Zambia: the Heterogeneous
Picture,andfocusedoninterventioncoveragetrendsbetween1990and2010.Thepresentreportprovidesabroaderrangeofupdatedresults,includingunder-5mortality
and coverageof thepentavalent vaccine, anddrills deeperinto
Zambias trends in child health at the district level.
Fur-ther,thepresentreportquantifiesthecontributionofmalariacontrolandotherkeychildhealth
interventions toZambiasreductionsinunder-5mortality.
DATA SOURCE YEARS REPRESENTED
SURVEYS
DemographicandHealthSurvey(DHS)
1992,1996-1997,2001-2002,2007
MalariaIndicatorSurvey(MIS) 2006,2008,2010,2012
MultipleIndicatorClusterSurvey(MICS) 1999
LivingConditionsMonitoringSurvey(LCMS)
1996,1998,2002-2003,2004-2005,2006,2010
HealthFacilityCensus
JapanInternationalCooperationAgency(JICA)(2005-2006)
SexualBehaviorSurvey(SBS) 2005,2009
HouseholdHealthCoverageSurvey 2008
NetmarkSurveyreports 2000,2004
POPULATION CENSUSES
Nationalcensus 1990,2000,2010
ADMINISTRATIVE SOURCES
HealthManagementInformationSystem(HMIS) 2000-2008;2009
Malariainterventiondatabases
NationalMalariaControlCentre(NMCC)(2005-2010)
Facility-levelPMTCTservices
NationalAIDSCouncilquarterlystatusreport(2005-2009)
HIV/AIDSprojections CentralStatisticalOffice(CSO)(2005)
Drugsupplyanddeliveryrecords
MedicalStoresLimited(MSL)(2007-2010)
Precipitationdata
GlobalPrecipitationClimatologyCentre(1986-2012)
Malariaendemicity(PfPR2-10) MalariaAtlasProject(2007,2010)
-
8Main findings
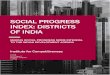
Under-5 mortality declines observed across districts,
accompanied by reductions in inequities Zambia made substantial
progress in improving child
sur-vivalbetween1990and2010.Atthenationallevel,all-causeunder-5
mortality decreased by 37%, from 174 deaths per1,000 livebirths
in1990 (95%CI: 168, 181) to109
in2010(95%CI:104,116).Alldistrictssawreductionsintheirlevelsofunder-5mortalityduringthistime.Moreover,manyofthedistrictswith
thehighest levelsofunder-5mortality
in1990showedthegreatestdeclinesby2010.Figure1depictshowthe range in
under-5mortality across districts has becomenarrower.
In 1990, levels of under-5 mortality spanned from 125deaths per
1,000 live births (95%CI: 97, 161) to 276
(95%CI:220,338)indifferentdistricts.Twentyyearslater,thisgapsubstantiallytightened,witharangeof83deathsper1,000livebirths(95%CI:60,113)to150(95%CI:109,203).Thedif-ferencebetweenthedistrictwiththehighestlevelofunder-5mortalityandthelowestwasmorethanhalvedfrom1990to2010
(dropping fromadifferenceof 151 to 67),
illustratinghowZambiasprogressinreducingunder-5mortalitywasalsoassociatedwithdecreasedhealthinequitiesacrossdistricts.
Despitetheseimprovements,itisworthnotingthatsomedistricts and
regionsdocumented lessprogress.Districts
inNorthernprovincehadveryhigh levelsofunder-5mortalityin 1990, and
though many recorded large declines,
theirratesstillremainedamongthehighestinthecountryin2010(greater
than 120 deaths per 1,000 live births). Additionalefforts
toreduceunder-5mortalityneedtobeprioritized inthesedistricts.
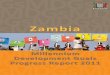
Malaria interventions are rapidly scaled up in Zambia, but most
districts fall short of national
targetsCoverageofmalariainterventionsgreatlyincreasedthrough-
outZambiaafter2000,withmostofthegainsoccurringsince2005.
Nationally, the proportion of households that
eitherownedatleastoneITNorreceivedIRSincreasedfrom8%in2000to37%in2005andthenrapidlyclimbedto71%in2010.Coverage
of intermittent preventive therapy in
pregnancy(IPTp2)quicklyrosefrom16%in2002toaround70%in2008.
In theearly2000s, coverageofmalaria control
interven-tionswasverylowthroughoutZambia,withonlyafewdistrictsbenefitingfromITNpilotprogramsandearlyimplementationofIRS.By2010,however,alldistrictshadcoveragelevelsex-ceeding55%forhavingeitherITNsorIRS.Figure2showstheriseincoverageofmalariacontrolfrom2000to2010.
Districts sawawide varietyof trends in IPTp2
coverageduringthe2000s. IPTp2levelsroserapidly
inmanydistrictsthroughout the 2000s.Others saw an increase in
coverageandthenalevelingoffby2010.Athirdgroupofdistrictsex-perienced
substantial declines in coverage during the
late2000s.Last,asubsetofdistrictsrecordedverysmallchangesinIPTp2coverageduringthisperiod.
ZambiasNational Malaria Strategic Plan, 2006-2010
setseveralmalaria intervention coverage targets to achieveby2010,
including (1)80%ofhouseholdswithat least threeITNs;
(2)85%ofeligiblehouseholds in15
targetdistrictshavingreceivedIRS;(3)80%ofpregnantwomenreceiving2dosesofFansidar/SP(IPTp2);and(4)80%ofchildrenunder5yearsoldsleepingunderanITNorresidinginahousewithIRS(MOH2006).Thesetargetswereveryambitious,anddespitemarkedprogresssince2000,nodistrictachievedallfourtargetsin2010.Onlyfivedistrictsreachedtwoofthefourtargets.Table2displaysthe28districtsthatmetoneormoreofthesetargetsin2010.Thetargetthatwasmostfrequentlymetwas
the third target,with16districts achievingat
least80%IPTp2coveragein2010.
Figure 1. District-level estimates of all-cause under-5
mortality for 1990, 2000, and 2010
1990 2000 2010
80
120
160
200
240
280
-
92000 2005 2010
0
20
40
60
80
100
Figure 2. Percentage of households covered by an ITN, IRS, or
both interventions, in 2000, 2005, and 2010
GEOGRAPHY MALARIA INTERVENTION TARGETS
OWNERSHIP IRS UNDER-5 ITN PROVINCE DISTRICT OF 1 ITN* COVERAGE**
IPTP, 2 DOSES USE OR IRS
Central Kabwe 81%
Mkushi 92%
Copperbelt Chingola 93%
Kalulushi 83%
Kitwe 87% 81%
Lufwanyama 91%
Masaiti 89%
Mpongwe 89%
Mufulira 80% 85%
Ndola 94%
Eastern Chadiza 81% 81%
Chama 90%
Katete 85% 81%
Mambwe 90% 89%
Petauke 80%
Luapula Chiengi 80%
Milenge 80%
Lusaka Chongwe 87%
Kafue 90%
Luangwa 89%
North-western Mufumbwe 82%
Northern Mpulungu 87%
Mungwi 84%
Nakonde 81%
Southern Livingstone 90%
Western Lukulu 96%
Mongu 89%
Senanga 88%
Table 2. District attainment of 2010 malaria intervention
targets
Notes:*TheNMCCgoalwasownershipofatleastthreeITNsby2010.
**TheNMCCgoalwas85%coverageofeligiblehouseholdsby2010.BasedonMCPAanalyses,nodistrictreached85%IRScoverage;
however,householdeligibilitycouldnotbeascertained.
-
1 0
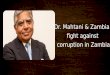
Scale-up of the pentavalent vaccine varies, polio immunization
falls in some
areasJustlookingatthenationallevel,trendsinimmunizationcov-eragegenerallypointtoprogress.Butatthedistrictlevel,wesee
a wide range of trends, with progress, stagnation,
andtroublingdeclinesincoverage.
ThepentavalentvaccinewasformallyintroducedinZambiain2005,andthecountryachieved67%coveragein2010.Atthedistrictlevel,coverageofthepentavalentvaccinerangedfromaslowas22%(95%CI:8%,44%)toashighas90%(95%CI:
81%, 96%) in 2010, with some districts showing
strongprogresssince2005andothersshowingminimalgainsincov-erage.Figure3depicts
this range
forpentavalentcoveragein2010.ManyofthelargestgainswereobservedinEasternprovince,
while several districts in North-western provincecontinued tohave
someof the lowest
levelsofpentavalentcoveragein2010.Identifyinghowtoimprovethedeliveryoruptakeofthepentavalentvaccineforthesedistrictsoughttobeapriority.
In 2010, polio immunization coverage reached 81% atthe national
level. However, coverage varied greatly
acrossdistricts,rangingfrom24%(95%CI:10%,42%)to99%(95%CI:98%,100%).Zambiaspolio-freecertificationwasacceptedin2005,but
severaldistricts thatborder theDemocraticRe-public of Congo (DRC)
andAngola are considered at highrisk forpolio importation from
thesecountries
(WHO2011).Someofthesehigh-riskdistrictsrecordeddecliningcoverageofpolioimmunizationduringthe2000sandhadsomeofthelowest
levelsofcoverage inZambia in2010. IfZambia is
tooptimallyprotectitselffromimportedpolio,deliberateeffortsare
needed to ensure that levels of polio immunization
aresustainedathighlevelsinhigh-riskareas.
Figure 3. The proportion of children who received the
pentavalent vaccine in 2010
Coverage of antenatal care substantial declined while skilled
birth attendance gradually
increasedAftermaintainingmoderatelyhighlevelsofANC4throughthe1990s,coverageinZambiadeclinedduringthe2000s,drop-pingto37%in2010.Atthesametime,skilledbirthattendance(SBA)coveragegraduallyincreased,risingto55%in2010.
For most districts, ANC4 coverage reached its
highestlevelsbetween1990and2000,afterwhichcoveragemarkedlyfell.Figure4showsANC4coverageinmostdistrictsdroppingfrom
higher levels (green) to much lower ones (shades oforange to
red).Understandingwhysomanydistrictsexperi-encedsuchsharpdeclinesinantenatalcareshouldbeahighpriority
inZambia. It is important tonote thata
fewdistrictsdidincreaseANC4coverageduringthistime.It is
likelythatmuchcouldbelearnedfromthesedistrictsaboutapproachestoANC4provisionandsupportofhealth-seekingbehaviors.
Trends
inSBAcoveragewidelyvariedacrossdistricts,asdidtherangeinlevelsofcoveragethroughoutthecountry.In2010,SBAcoveragerangedfromlessthan1%to98%(95%CI:91%,100%).AboutfivedistrictshadverylowlevelsofSBA
0
20
40
60
80
100
Figure 4. Coverage of four or more antenatal care visits (ANC4)
in 2000, 2005, and 2010
2000 2005 2010
0
20
40
60
80
100
-
1 1
during the 1990s but then brought coverage to above
thenationalaveragein2010.Approximately10recordedsteadygainsinSBAduringthe1990sbeforesharplyfallingtolevelsbelow20%.Anumberofdistrictshadconsistentlylowlevelsoverthetwodecades,whileafewmaintainedhighcoverage.Zambiawouldlikelybenefitfromfurtherinvestigationintothedistrictsdifferences
in skilledbirthattendance
trends,espe-ciallytodeterminewaystoimprovecoverageinplaceswhereSBAappearstobeminimal.
Breastfeeding increased to high
levelsRatesofexclusivebreastfeedingrosesteadilythroughoutthe1990sand2000sbeforereaching80%nationallyin2010.Mostdistrictsfollowedthistrend,butthereweresomenotableex-ceptions.
Some districts experienced an earlier scale-up
ofexclusivebreastfeeding,recordingtheirhighestlevelsintheearly2000s,butsawcoveragequicklydeclineby2010.Afewdistricts,mostly
in Eastern province, consistently trailed
thenationalscale-upofexclusivebreastfeeding,barelyreaching60%in2010.
Rapid scale-up of key child health interventions contributes to
declines in under-5 mortalityToassess the
impactofmalariacontrolonunder-5mortalityin Zambia, theMCPA research
team conducted a causal at-tribution analysis that included a full
range of child healthinterventions and non-health factors. More
details on
themethodsandstatisticalmodelsusedcanbefoundinAnnex1.
The teamfoundthatZambiahadscaledupseveral inter-ventionsat
thesametime.Figure5showshowgains in ITNand IRS coverage coincided
with rising levels of the
pen-tavalentvaccine,exclusivebreastfeeding,andtheavailabilityof
PMTCT in health facilities. It was statistically impossibleto
teaseout the individual effects of these
interventionsonunder-5mortality. Instead, researchers created a
compositeindicatorofrapidlyscaledupinterventions.
Figure 5. The scale-up of malaria control interventions and a
subset of key child health interventions
After accounting for other factors (including socioeco- nomic
indicators), rapidly scaled up interventions were sig- nificantly
associated with Zambias reductions in all-causeunder-5mortality.
Ifthecoverageoftheseinterventionshadremainedatlevelsobservedin2000,under-5mortalitywouldhave
been 11% higher in 2010 (124 deaths per 1,000
livebirths(95%CI:118,129))thanwhatwasactuallyobservedforthatyear(109deathsper1,000livebirths(95%CI:104,116))(Figure6).
Figure 6. Trends in under-5 mortality as observed and predicted
in the absence of rapidly scaled up interventions, 1990-2010
Thisfindingsuggeststhattherapidscale-upofthesefivematernalandchildhealthinterventionshastenedthedeclineofunder-5mortalityby1%peryear.Itisimportanttonotethatunder-5mortality
rateswould have continued to decline
inZambiabetween2000and2010,evenwithoutthescale-upoftheseinterventions.Infact,under-5mortalitydecreased14%between1990and2000,droppingfrom174deathsper1,000livebirths(95%CI:168,181)to149in2000(95%CI:144,156).GiventhedeclinesthatZambiaexperiencedinunder-5mor-tality
from1990 to 2000,wewouldhavepredicted an18%decrease in under-5
mortality between 2000 and 2010.
In-stead,withthescale-upofthesefiveinterventions,thecountryrecordeda26%declineduringthistime.Inotherwords,thesimultaneous
scale-upof ITNs, IRS, thepentavalent
vaccine,exclusivebreastfeeding,andPMTCTservicesacceleratedthedeclinesinunder-5mortalitybyanadditional1%peryear.
0
.5
1
1. 5
2
2. 5
3
No.
of f
acilit
ies
with
PM
TCT
per c
apita
*
0
20
40
60
80
100
Perc
ent (%
)
1990 1995 2000 2005 2010
ITN ownership and/or IRS Pentavalent vaccineExclusive
breastfeeding Facilities offering PMTCT per capita*
* Children under 1 year old
100
110
120
130
140
150
160
170
180
All
caus
e un
der
5 m
orta
lity
1990 1995 2000 2005 2010
Observed under5 mortality
Predicted under5 mortality without scaleup Under5 deaths averted
due to scaleup
-
1 2
Between 1990 and 2010, the health landscape in
Zambiamarkedlychanged,and for themostpart, thesechangesre-flect
progress and service delivery success throughout
thecountry.Under-5mortalitysubstantiallydecreasedat
thena-tionallevel,andthegapbetweendistrictswiththehighestandlowest
under-5 mortality substantially decreased. These
de-clinesinunder-5mortalitycanbetiedtoZambiassuccessfulefforts in
expanding coverage for a subset of child
healthinterventions:ITNownership,IRS,thepentavalentvaccine,ex-clusivebreastfeeding,andtheavailabilityofPMTCTservices.These
five interventions were rapidly scaled up during
the2000sandjointlycontributedtoanadditional11%reductioninall-causeunder-5mortalityinZambiabeyondwhatwouldhavebeenexpectedbasedonthecountrystrendsinunder-5mortality
during the 1990s. The scale-up ofmalaria controlhas been a key part
of Zambias improved health serviceenvironment, and sustaining high
levels of malaria controlinterventions, alongsideother life-saving
interventions, is ofcriticalimportance.
Amidstthesesuccesses,IHMEandUNZAidentifiedsometroublingtrendsthatwarrantfurtherpolicyattention.Overall,theproportionofpregnantwomenwhosoughtat
least
fourantenatalcarevisitsdrasticallydecreasedbetween2000and2010.SeveraldistrictsrecordedlevelsofANC4below20%in2010,whichsuggeststhatavastmajorityofwomenintheseplaces
do not receive optimal antenatal care during
preg-nancy.Knowingthatantenatalcareservicesarecloselylinkedto
bettermaternal and child health outcomes (WHO
2003),ZambiashouldaddressthesedecliningtrendsinANC4.
Immunizationratesremainedat leastmoderatelyhighatthenational
level,butsomedistrictsshowedconcerningde-clinesforcertainvaccines,namelypolio,andfellbehindinthescale-upofthepentavalentvaccine.AnumberofdistrictsthatareconsideredatriskforpolioimportationfromtheDRCandAngola
recorded recent declines in immunization coverage.Several districts
showed minimal gains in coverage of the
pentavalentvaccine, fallingwellbelow
thenationalaveragein2010.Prioritizingtheaccelerationofpentavalentcoverageindistricts
laggingbehindthenationaltrendshouldbecon-sidered.
Zambiasnewmalariastrategicplanmapsoutanambitiousgoal towarda
malaria-freeZambia (MOH2011), forwhichuniversal coverageof ITNsor
IRS and increasing IPTp
fromtwotothreedoses(IPTp2toIPTp3)arenewinterventiontar-getsfor2015.GiventhatfewerthanhalfofZambiasdistrictsachievedatleastoneofthemalariainterventioncoveragetar-getsfor2010,thecountrymayneedtoconsiderstrategiestofurtherexpandandsustainhigher
levelsofmalaria interven-tioncoverageinordertomeetits2015goals.
As demonstrated through the MCPA project in
Zambia,nationaltrendscanmasksignificantdifferencesatthedistrictlevel.Thedistrictprofiles
included in this reportprovidea
data-drivenfoundationforbenchmarkingdistrictperformanceandtargetingareasfor
improvement. It is importantforgov-ernments
toprioritizemonitoringanddatagatheringat
thedistrictleveltomakefutureanalysesmorerobustandtopro-videcriticalinputsfordecision-makingandpriority-settingbydistricthealthoffices.
TomaintainandfurtheracceleratethehealthgainsZambiahas made in
child survival, continued efforts dedicated todeliveringa
rangeofhealth interventions,
includingmalariacontrol,areneeded.Theregularandtimelycollectionofdis-trict
health datawill be crucial for guiding policy
decisionsandresourceallocation.Thecountrys investments
innation-widesurveysservedasthecornerstonefortheanalysesinthisreport,and
theyare likely to remainavital
sourceofhealthdataalongsideZambiashealthinformationsystems.Byusingitsdistrict-leveldataandfocusingonhealthgapsexperiencedby
its districts, Zambia is in the position to further
accel-erateprogress
inchildhoodsurvivalandtopromotegreaterequalityinhealthattainmentthroughoutthecountry.
Conclusions and policy implications
-
1 3
ReferencesTheWorldBreastfeedingTrendsInitiative(WBTi).Zambia
Country Assessment Report 2008.NationalFoodand
NutritionCommission/IBFANAfrica,2008.Availableat:http://www.worldbreastfeedingtrends.org/report/WBTi-Zambian-2008.pdf[AccessedFebruary2014].
WorldHealthOrganization(WHO).Antenatal Care in Developing
Countries: Promises, Achievements, and Missed Opportunities: an
Analysis of Trends, Levels, and Differentials,
1990-2001.Geneva,Switzerland:WHO,2003.
WorldHealthOrganization(WHO).Annual Report of the WHO Country
Office Zambia, 2011.Lusaka,Zambia:WHO,2011.
ZambiaMinistryofHealth(MOH).National Malaria Strategic Plan
20062011: A Road Map for RBM Impact in Zambia.
Lusaka,Zambia:MOH,2006.
ZambiaMinistryofHealth(MOH).National Malaria Strategic Plan
20112015: Consolidating Malaria Gains for Impact.
Lusaka,Zambia:MOH,2011.
-
1 4
Inordertocomprehensivelyassesstheimpactofmalariacon-trolonunder-5mortalityinadata-driven,systematicway,theMCPAresearchteamsmethodologicalframeworktookplaceinthreemainsteps:
(1) Collating data and generating source-specific esti-mates.
TheMCPA research teambrought togetherabroadrange of data sources,
including surveys, population
cen-suses,andadministrativesources,togeneratesource-specificestimatesforall
indicatorsof interest.
Intotal,20householdsurveys,onehealthfacilitycensus,threepopulationcensuses,and
two administrative sources (National Malaria
ControlCentreindoorresidualsprayingdatabaseandfacilityPMTCTservicesfromtheNationalAIDSCouncil)wereincludedinthefinalanalysis.
(2) Estimating trends for 72 districts from 1990 to 2010.
GiventherangeofdatatypesassembledfortheMCPAproject,statisticalmodelingapproacheshad
tobeused inorder
tosynthesizetheestimatesfromthesedifferentdatasourcesintoaunifiedtrend.Demographicmethodsforanalyzingbirthhis-torydatawerecombinedwithsmallareaestimationmodelingtogeneratedistrict-leveltrendsforall-causeunder-5mortality.Atwo-stepmethodinvolvingspatio-temporalsmoothingandGaussianProcessRegression(GPR)wasusedtoproducedis-trict-level
trends for intervention coverage and non-healthindicators.
(3) Conducting causal attribution analyses. Many models and
combinations of covariates were rigorously tested inorder to
identify the most robust and valid model for as-sessing the
relationship between declines in mortality andindividual health
interventions and non-health
indicators.Thetypesofmodelsthatwereexploredincludedsingle-andmultistage
linearmodels, lasso, functionaldataanalysis,firstdifferences,
differences-in-differences, structural
equationsmodeling,andfactoranalysis.Themodelthatwasultimatelyselectedisalinearmodelwithbootstrapping,asitbetterac-countsforautocorrelationoveryearsanddistricts.Thelistofcovariatesthatwereexploredincludedrainfalllevels,fertility,birthspacing,maternaleducation,schoolattendanceamongteenagers,femaleheadshipofhouseholds,meanhouseholdsize,
household sanitation, prevalence of improved
sourcesofcookingfuel,prevalenceof improvedwall type
inhomes,electricity, immunization coverage, and
coverageofmalariaandmaternalandchildhealthinterventionsdescribedinthe
main text of this report. Covariates that were not
includedbecauseof lackofdata availability include
coverageofma-lariatreatmentforchildrenwithfever,coverageofantibiotictreatment
for childrenwithpneumonia, coverageof oral re-hydration treatment
for children with diarrhea, coverage ofpediatricHIV
treatment,qualityofdistrict healthofficeman-agement, district
health expenditures and health
personnel,accesstohealthfacilities,malariatransmission
intensityovertimeandbydistrict,andnutritionalinterventions.
The MCPA research team found that it was statisticallyimpossible
to tease out the impact of malaria control in-terventions from
other interventions that also experiencedlargegains
incoverageduring the2000s.
Instead,principalcomponentanalysis(PCA)wasusedtobundletheserapidlyscaled-up
interventionsmalaria control, exclusive
breast-feeding,facilitiesofferingPMTCTperpopulationunder1yearold,
and coverage of the pentavalent vaccineinto a
com-positeindicator.Thefinalmodelestimatesthejointeffectoftheseinterventionsonunder-5mortality:
ln(q) = 0 + 1Scaled + 2SES + 3Und + 4SES * Scaled + 5SES * Und +
6ANC1 + 7DPT3 + 8Meas + 9Year + k[ ] +
The final model was a linear model with
bootstrapping,whereforeachdistrict ,provincek,andyear i, ln(q)
isthenatural logarithm of the under-5mortality rate, 0 is the
in-tercept, Scaled is the composite indicator for rapidly scaledup
interventions,andSES is thecompositemeasure fornon-health factors.
Und is the proportion of children who areunderweight,SES * Scaled
isan interactionbetween
thenon-healthfactorcompositemeasureandthecompositeindicatorforrapidlyscaledupinterventions,SES
* Undisaninteractionbetween the non-health factor compositemeasure
and theproportion of children who are underweight, ANC1 is
cov-erageofoneantenatal care visit,DPT3 is coverageof
threedosesofDPT,Meas iscoverageofonedoseof
themeaslesvaccine,Yearisthecorrespondingyear,k[
j]isarandomeffectonprovincektowhichj belongs,and
istheerrorterm.
Annex 1. Overview of the MCPA analytical approach and
methods
-
1 5
District profiles
Trackingtrendsinchildhealthoutcomesandinterventioncoverageatthedistrictlevelprovidestimely,useful,andactionableinformationtonationalandlocalpolicymakersinZambia.
Thedistrictprofilesareorderedalphabeticallywithineachprovince.Eachprofileprovidesachildhealthbarometerfor2010,whichcomparesagivendistrictsperformanceonkeychildhealthoutcomesandinterventionstothenationalaverageandtherangeobservedacrossdistricts.Further,eachprofiledetailstrendsobservedforeachgroupofinterventions:malariainterventions,immunizations,andothermaternalandchildhealthinterventions.
Thesedistrictprofilesaimtoprovideafoundationfromwhich
localhealthofficialscanassesstheirdistrictschildhealthstatusandthentargethigh-priorityareasforimprovement.IndividualprofilescanbedownloadedfromIHMEsGlobalHealthDataExchange:http://ghdx.healthmetricsandevaluation.org/.
-
1 7
Central province
-
1 8
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From1990to2010,Chibomborecordedasignificantreduc-tion in
all-cause under-5mortality, dropping 37% from
149deathsper1,000livebirthsin1990(95%CI:116,190)to94in2010(95%CI:69,126).In2010,thedistrictsunder-5mortalitywasmuchlowerthanthenationalaverageof109deathsper1,000livebirths(95%CI:104,116)andwasamongthelowestinZambiaforthatyear.
Theproportionofchildrenwhowereunderweightsteadilyincreasedfrom11%in1990(95%CI:6%,19%)to19%intheearly2000s.Levelsofunderweightremainedat19%through2003,afterwhichprevalencedeclinedto14%in2010(95%CI:10%,18%),equalingthenationalaverageforthatyear.
CHILD HEALTH OUTCOMES
SUMMARYChibombosubstantially
reducedall-causeunder-5mortalitybetween1990and2010,bringingitsmortalitylevelsamongthe
lowest in Zambia. Childhood underweight, however,
in-creasedduringthe1990sbeforedeclining.Prioritizingwaysto further
accelerate gains for child health outcomes,
espe-ciallyunderweight,shouldbeconsidered.
Several interventions, including IPTp2, the pentavalentvaccine,
and exclusive breastfeeding, were scaled up toor above the national
averageby 2010.After slight dips
incoverage,BCGandmeaslesimmunizationroseabovethena-tionalaveragesin2010.
However, amidst these gains, some worrisome trendswere
identified and warrant further attention. Chibombosscale-up of ITNs
and IRS laggedbehind the national
trend,andpoliocoveragedeclinedinrecentyears.Skilledbirthat-tendance
stayedquite low, and
alarmingly,ANC4droppedsharplyfromhighlevelsofcoverageintheearly1990s.
In2010,Chibombogenerallymetorexceedednationallevelsforimmunizations,andequaledorfellbelowformalariainterventions.Formaternalandchildhealthinterventions,thedistricthadamoremixedperformance.
Incomparisonwiththenationalaverage,Chibomboshowedmuchlowerlevelsofmortalityandsimilarlevelsofunderweight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Chibombo Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Chibombo
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes
(orange)andhigherlevelsofinterventioncoverage(green).
Chibombo
-
1 9
ITNownership
remainedbelow10%until2004,afterwhichcoverageincreasedto56%in2009(95%CI:51%,60%)andremainedat56%through2010.This
levelof ITNownershipwaslowerthanthenationalaverageof62%for2010.
ITNusebychildrenunder5yearsoldroseto44%in2010(95%CI: 38%, 50%),
which was lower than the national
av-erageof51%.ThedifferencebetweenITNownershipanduse(12percentagepoints)inChibombowascomparabletowhatwasobservedatthenationallevelfor2010.
Chibombo formally implemented IRS activities in
2010,andreached16%ofhouseholdsthatyear(95%CI:11%,22%).ThiswasamongthelowestlevelsofIRScoverageacrossthe54districtsthathadIRSby2010.
Theproportionofpregnantwomenwho received
IPTp2remainedbelow10%until 2001, afterwhich coverage
roseto70%in2008(95%CI:60%,80%).IPTp2coverageslippedto68%in2010(95%CI:56%,78%),equalingthenationalav-erageforthatyear.
BCGcoveragedeclinedfrom99%intheearly1990sto94%intheearly2000s,butincreasedto97%in2009(95%CI:94%,98%)andremainedat97%through2010.This
levelofBCGcoverage was higher than the national average of 95%
for2010.
Measles immunization decreased from 98% in the
early1990sto91%inthelate1990s,afterwhichcoverageclimbedto 99% in
2007 (95% CI: 98%, 99%) and remained at 99%through 2010. This level
of measles coverage was
slightlyhigherthanthenationalaverageof98%for2010.
Coverage of polio immunization dropped from 95%
in1990(95%CI:91%,98%)to70%in1997(95%CI:65%,75%),but then rose to
90% in themid-2000s. Polio coverage de-clinedsoonafter,decreasing
to79% in2010
(95%CI:62%,91%),slightlybelowthenationalaverageof81%.
Afterthepentavalentvaccinewasformally
introducedinChibomboin2005,coverageincreasedto51%in2006(95%CI:44%,57%)and69%in2010(95%CI:55%,82%),slightlyexceedingthenationalaverageof67%.
ANC4coveragesteadily fell from84%in1990(95%CI:74%,92%) to38%
in2010
(95%CI:11%,74%),whichwascompa-rabletothenationalaverageof37%thatyear.ThefindingthatChibombos
levelsofcoveragefellmorethan45percentagepointsduringthistimeiscauseforconcern.
Skilled birth attendance decreased from 40% in
1990(95%CI:26%,55%)to21%intheearly2000s,afterwhichcov-erageslowlyroseto30%in2010(95%CI:7%,66%).ThislevelofSBAcoveragewasbelowthenationalaverageof55%for
2010,andChibombogenerallyhadlowerSBAcoveragethanthenationalaveragefrom1990to2010.
Theproportionofchildrenwhowereexclusivelybreastfedremained below
20% until 1998, after which coverageclimbed to 67% in 2004 (95%CI:
60%, 73%).Gains in
cov-eragestalleduntil2008,afterwhichexclusivebreastfeedingincreasedto91%in2010(95%CI:83%,96%),farexceedingthenationalaverageof80%.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
Indoor residual spraying
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 2005 2010
Skilled birth attendance
0
20
40
60
80
100
1990 1995 2000 2005 2010
Exclusive breastfeeding
0
20
40
60
80
100
1990 1995 2000 2005 2010
-
2 0
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From1990to2010,Kabwerecordedareductioninall-causeunder-5mortality,dropping33%from143deathsper1,000livebirthsin1990(95%CI:111,184)to96in2010(95%CI:69,132);however,thisdeclinewasnotstatisticallysignificant.In2010,thedistrictsunder-5mortalitywaslowerthanthena-tionalaverageof109deathsper1,000livebirths(95%CI:10,116).
The proportion of children who were underweight
in-creasedfrom11%intheearly1990sto14%intheearly2000s,after which
underweight slightly declined to 13% in
2003(95%CI:11%,16%)andremainedatthislevelthrough2010.Althoughchildhoodunderweightwascomparabletothena-tionalaverageof14%for2010,thedistrictsminimalprogressiscauseforconcern.
CHILD HEALTH OUTCOMES
SUMMARYBetween1990and2010,Kabwereduceditsall-causeunder-5mortality,buttherelativemagnitudeofthedistrictsprogresswasfairlylow.Whilechildhoodunderweightwascomparableto
the national average, Kabwe made minimal progress inreducing
prevalence. Prioritizing ways to further
accelerategainsforchildhealthoutcomesshouldbeconsidered.
Kabwe increased IPTp2 coverage to well above the na-tional
average in 2010, and IRS coverage was among thehighest
inZambiathatyear.Thedistrictmadenotableprog-ress in
increasingcoverageof thepentavalent
vaccine,andhighlevelsofBCGandmeaslesimmunizationweresustainedduring
the 2000s. Exclusive breastfeeding rebounded
fromdeclinesincoverageduringtheearly2000s.Skilledbirthat-
tendancesteadilyincreasedovertime,reachingsomeofthehighestlevelsofcoverageinthecountry.
However, amidst these gains, some troubling
trendswereidentifiedandwarrantfurtherattention.Poliocoveragedeclinedinrecentyears,andalarmingly,ANC4coveragede-creasedsharplyfromveryhighlevelsduringthe1990s.
In 2010, Kabwe generally met or exceeded
nationallevelsacrossinterventions,withthestarkexceptionofANC4coverage.
In comparison with the national average, Kabweshowedlower
levelsofmortalityandsimilar levelsofunder-weight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Kabwe Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Kabwe
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes(orange)andhigherlevelsofinterventioncoverage(green).
Kabwe
-
2 1
ITNownership
remainedbelow10%until2001,afterwhichcoverageincreasedto59%in2008(95%CI:55%,64%)butslippedto56%in2010(95%CI:50%,61%).ThislevelofITNownership
was lower than the national average of 62% in2010.
ITNusebychildrenunder5yearsoldclimbedto48%in2010(95%CI:42%,55%),butremainedslightlylowerthanthenationalaverageof51%forthatyear.ThedifferencebetweenITN
ownership and use (8 percentage points) was
slightlylowerinKabwethanwhatwasobservedatthenationallevel(11percentagepoints)for2010.
Kabwe formally implemented IRS activities in 2003,
andwasoneofthefirst15districts inZambiatorolloutIRS.
IRScoveragepeakedat67% in2008 (95%CI:63%,71%),
afterwhichcoveragedroppedto58%in2010(95%CI:52%,64%).Nonetheless,Kabwehadoneof
thehighest levelsof IRS inZambiain2010.
Theproportionofpregnantwomenwho received
IPTp2remainedbelow10%until2001,afterwhichcoveragerapidlyroseto2009at81%(95%CI:72%,88%)andwasmaintainedthrough2010.ThislevelofIPTp2coveragewasmuchhigherthanthenationalaverageof68%for2010.
BCGcoveragedeclinedfrom97%in1990(95%CI:94%,99%)to95%intheearlytomid-1990s,butincreasedto99%inthemid-2000s.Coverageslippedto96%in2010(95%CI:93%,98%),butremainedslightlyhigherthanthenationalaverageof95%.
Measlesimmunizationincreasedfrom82%in1990(95%CI:69%,91%)to98%in2003(95%CI:97%,99%),afterwhichcoveragewassustainedat98%through2010,equaling
thenationalaverage.
Coverage of polio immunization sharply declined
from93%in1990(95%CI:87%,96%)to76%in1997(95%CI:72%,80%). Polio
coverage hovered just above 80% from 2000
to2008,afterwhichimmunizationratesdroppedto72%in2010(95%CI:57%,83%),fallingbelowthenationalaverageof81%.
Afterthepentavalentvaccinewasformally
introducedinKabwein2005,coverageincreasedto53%in2006(95%CI:46%,60%)and68%in2010(95%CI:57%,79%),whichwascomparabletothenationalaverageof67%.
ANC4coverage increased from66% in1990 (95%CI:
53%,78%)to74%inthemid-1990s,butdroppedconsiderablyto23%in2010(95%CI:5%,53%),fallingbelowthenationalav-erageof37%.ThefindingthatKabweslevelsofcoveragefell50percentagepointssincethemid-1990sisworrisome.
Skilled birth attendance steadily increased from 48%
in1990(95%CI:36%,61%)to86%in2007and2008,afterwhichcoverageslippedto83%in2010(95%CI:57%,96%).Despite
thisdecline,KabwesSBAcoveragewasamongthehighestinZambiain2010.
Theproportionofchildrenwhowereexclusivelybreastfedremainedbelow20%until1995,afterwhichcoveragerapidlyclimbedto78%in2002(95%CI:73%,82%).Exclusivebreast-feedingthendeclined,droppingto60%in2006(95%CI:53%,67%).Coveragereboundedto77%in2010(95%CI:66%,85%),butremainedslightlylowerthanthenationalaverageof80%.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
Indoor residual spraying
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 2005 2010
Skilled birth attendance
0
20
40
60
80
100
1990 1995 2000 2005 2010
Exclusive breastfeeding
0
20
40
60
80
100
1990 1995 2000 2005 2010
-
2 2
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From 1990 to 2010, Kapiri-Mposhi recorded a reduction
inall-causeunder-5mortality, dropping26%
from151deathsper1,000livebirthsin1990(95%CI:118,193)to112in2010(95%CI:83,149);however,
thisdeclinewasnotstatisticallysignificant.In2010,thedistrictsunder-5mortalitywasslightlyhigherthanthenationalaverageof109deathsper1,000livebirths(95%CI:104,116).
The proportion of children who were underweight
in-creasedfrom9%in1990(95%CI:4%,18%)toahighof18%in1999(95%CI:15%,21%),butthendeclinedto9%in2009(95%CI:
7%,12%) and remainedat 9% through2010.Thislevel of underweight
wasmuch lower than the national
av-erageof14%in2010andamongthelowestinZambia.
CHILD HEALTH OUTCOMES
SUMMARYKapiri-Mposhi reduced its all-cause under-5 mortality
be-tween 1990 and 2010, but the relative magnitude of
thedistrictsprogresswaslow.Afteraperiodofincreasinglevelsofunderweight,thedistrictreduceditsprevalencetosomeofthelowestlevelsinZambia.Prioritizingwaystofurtheraccel-eratedeclinesinchildhealthoutcomes,especiallyforunder-5mortality,shouldbeconsidered.
The district successfully scaled up several
interventions,rangingfromIPTp2to thepentavalentvaccine,
tocoveragelevels equaling or exceeding the national average in
2010.High levels of measles coverage were maintained after
in-creasesinthe1990s,andpoliocoveragerosetoamongthehighestinZambiain2010.
However,amidstthesesuccesses,sometroublingtrendswereidentifiedandwarrantfurtherattention.BCGcoveragefellbelow
thenationalaverage in2010,and ITNownershipwas among the lowest
levels in Zambia. The district expe-rienced substantial declines in
ANC4 coverage and skilledbirthattendance.
In2010,Kapiri-Mposhigenerallymetorexceedednationallevels for
immunizations, andequaledor
fellbelownationallevelsformaternalandchildhealthinterventions.Formalariainterventions,
thedistricthadamoremixedperformance.
Incomparisonwiththenationalaverage,Kapiri-Mposhishowedslightlyhigherlevelsofmortalityandmuchlowerlevelsofun-derweight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Kapiri-Mposhi Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Kapiri-Mposhi
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes
(orange)andhigherlevelsofinterventioncoverage(green).
Kapiri-Mposhi
-
2 3
ITNownership remainedbelow10%until2003,afterwhichcoverage
increased to 54% in 2010 (95% CI: 49%,
59%),fallingwellbelowthenationalaverageof62%andamongthelowestinZambiathatyear.
ITNusebychildrenunder5yearsoldclimbedto57%in2009(95%CI:52%,62%),butslippedto55%in2010(95%CI:49%,61%).ThislevelofITNusewasslightlyhigherthanthenationalaverageof51%for2010.ITNusewasslightlyhigherthanITNownershipinKapiri-Mposhifor2010,whichsuggeststhatnetusebychildrenunder5maybehighamonghouse-
holdsthathaveITNs.Kapiri-MposhiformallyimplementedIRSactivitiesin2008
andreached19%ofhouseholdsin2010(95%CI:16%,23%).Thisscale-upof
IRSwasamongthelowestamongtheotherdistrictsthatalsobeganIRSin2008.
Theproportionofpregnantwomenwho received
IPTp2remainedbelow10%until2003,afterwhichcoveragerapidlyincreased
to 70% in 2010 (95% CI: 56%, 81%), slightly
ex-ceedingthenationalaverageof68%.
BCGcoveragedeclinedfrom93%in1990(95%CI:86%,97%)to 89% during the
mid- to late 1990s. Coverage
hoveredaround90%inthe2000s,risingto91%in2010(95%CI:85%,95%),whichwaslowerthanthenationalaverageof95%.
Measles immunization remained below 80% until
1998,afterwhichcoveragesteadilyclimbedto98%in2008(95%CI:95%,99%)andremainedatthislevelthrough2010,equalingthenationalaverageforthatyear.
Risingfromalowof64%in1990(95%CI:48%,79%),cov-erage of polio
immunization largely hovered around 70%
until2006,afterwhichpoliocoverageclimbedto94%in2010(95%CI:87%,98%)andemergedasoneofthehighestlevelsinZambia
for
thatyear.Thesegainsareparticularlynotablegiventhatthedistrictspoliocoveragewasconsistentlylowerthanthenationalaverageuntilthemid-2000s.
Afterthepentavalentvaccinewasformally introducedinKapiri-Mposhi
in 2005, coverage increased to 47% in
2006(95%CI:40%,55%)and78%in2010(95%CI:68%,88%),farexceedingthenationalaverageof67%.
ANC4coveragegraduallydeclined from52% in1990
(95%CI:34%,68%)to36%in2010(95%CI:9%,72%).WhilethedistrictsANC4coveragewascomparabletothenationalav-erageof37%in2010,itslevelsofANC4remainedquitelow.
Skilled birth attendance decreased from 48% in
1990(95%CI:31%,64%)toalowof22%in2010(95%CI:5%,55%),fallingbelowthenationalaverageof55%.Thistrendofsteadydeclineiscauseforconcern,directlycontrastingwithgradual
increasesinSBAcoverageobservedatthenationallevel.Theproportionofchildrenwhowereexclusivelybreastfed
remained below 20% until 1998, after which coverage rap-idly
increasedto62%in2004(95%CI:55%,69%).Gains incoveragestalled
through2007,butexclusivebreastfeedingclimbedto80%in2010(95%CI:69%,88%),equalingthena-tionalaverage.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
Indoor residual spraying
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 2005 2010
Skilled birth attendance
0
20
40
60
80
100
1990 1995 2000 2005 2010
Exclusive breastfeeding
0
20
40
60
80
100
1990 1995 2000 2005 2010
-
2 4
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From1990to2010,Mkushirecordedasignificantreductioninall-causeunder-5mortality,dropping34%from169deathsper1,000livebirthsin1990(95%CI:132,213)to111in2010(95%CI:82,149).In2010,thedistrictsunder-5mortalitywascomparabletothenationalaverageof109deathsper1,000livebirths(95%CI:104,116).
The proportion of children who were underweight
in-creasedfrom17%intheearly1990stoahighof21%in1999(95%CI:17%,25%),butthendecreasedto13%in2010(95%CI:10%,18%).Thislevelofunderweightwascomparabletothenationalaverageof14%in2010.
CHILD HEALTH OUTCOMES
SUMMARYMkushisubstantiallyreducedall-causeunder-5mortalityfrom1990to2010.Childhoodunderweight
increasedduringthe1990sbeforedecreasinginrecentyears.Prioritizingwaystofurtheraccelerateratesofprogressinchildhealthoutcomesshouldbeconsidered.
IPTp2 coverage reached some of the highest levels inZambia in
2010, and ITN coverage consistently
exceededthenationalaverage.Pentavalentcoveragewashigher thanthe
national average in 2010, and exclusive
breastfeedingclimbedtosomeofthehighestlevelsinthecountry.BCGandmeaslescoverageremainedhighduringthe2000s,andpoliocoveragewascomparabletothenationalaveragein2010.
However, amidst these gains, some worrisome
trendswereidentifiedandwarrantfurtherattention.ANC4coveragedeclined
after a period of steady gains during the
1990s.Skilledbirthattendancegraduallyincreasedinthe1990s,butsharplydroppedtoverylowlevelsin2010.SBAcoverageinMkushiwasamongthelowestinZambiafor2010.
In2010,Mkushigenerallymetorexceedednationallevelsacrossinterventions,withtheclearexceptionofskilledbirthattendance.Incomparisonwiththenationalaverage,Mkushishowedsimilarlevelsofmortalityandunderweight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Mkushi Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Mkushi
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes
(orange)andhigherlevelsofinterventioncoverage(green).IRScoveragewasnotincludedbecauseMkushistartedIRSafter2010.
Mkushi
-
2 5
ITNownership
remainedbelow10%until2001,afterwhichITNownershiprapidlyincreasedto67%in2008(95%CI:60%,73%).Ownershipslippedto65%in2010(95%CI:57%,71%),remainingslightlyabovethenationalaverageof62%.
ITNusebychildrenunder5yearsoldquicklyroseto64%in2008(95%CI:56%,72%),butdeclinedto58%in2010(95%CI:48%,67%).ThislevelofITNuseremainedhigherthanthenationalaverageof51%for2010.ThedifferencebetweenITNownershipanduse(7percentagepoints)waslowerinMkushi
thanwhatwasobservedatthenationallevel(11percentagepoints)for2010.
IRScoveragetrendsarenotincludedbecauseMkushididnotbeginformalIRSactivitiesuntilafter2010.
Theproportionofpregnantwomenwho received
IPTp2remainedbelow10%until2002,afterwhichcoveragerapidlyclimbed
to92% in2010 (95%CI:85%,96%),
farexceedingthenationalaverageof68%andrisingtoamongthehighestlevelsinZambia.
BCG coverage hovered around 90% until the
mid-2000s,afterwhichcoverageclimbedto99%in2010(95%CI:98%,100%),whichwasamongthehighestlevelsofBCGcoverageinZambiaforthatyear.
Measles immunization steadily increased from 74%
in1990(95%CI:60%,84%)to98%in2008(95%CI:96%,99%).Thislevelofcoveragewasmaintainedthrough2010,equalingthenationalaverage.
Coverageofpolioimmunizationgraduallyrosefrom69%in 1990 (95%CI:
54%, 81%) to 85% in 2007 (95%CI:
79%,89%),whichwasmaintainedthrough2010.Thislevelofpoliocoveragewasslightlyhigherthanthenationalaverageof81%for
2010.
Afterthepentavalentvaccinewasformally
introducedinMkushiin2005,coverageincreasedto47%in2006(95%CI:39%,55%)and77%in2010(95%CI:63%,87%),risingabovethenationalaverageof67%.
ANC4coveragegraduallyincreasedfrom45%in1990(95%CI:29%,60%) to66%
in theearly2000s,but
thendeclinedto52%in2010(95%CI:14%,86%).WhileANC4coverageinMkushistayedabovethenationalaverageof37%in2010,itslevelsremainedlowerthanoptimal.
Skilled birth attendance slightly increased from 24%
intheearly1990sto30%inthe
late1990s,butthendroppedsharplyto4%in2010(95%CI:0%,16%),
fallingwellbelow
thenationalaverageof55%andamongthelowestinZambiafor 2010.
Mkushis consistently low level of SBA
coverage,pairedwithitsrecentdecline,iscauseforconcern.
Theproportionofchildrenwhowereexclusivelybreastfedremainedbelow20%until1997,afterwhichcoveragerapidlyincreasedto95%in2010(95%CI:91%,98%),risingamongthehighestlevelsinZambiaforthatyear.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 2005 2010
Skilled birth attendance
0
20
40
60
80
100
1990 1995 2000 2005 2010
Exclusive breastfeeding
0
20
40
60
80
100
1990 1995 2000 2005 2010
-
2 6
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From 1990 to 2010, Mumbwa recorded a reduction in
all-causeunder-5mortality,dropping23%from140deathsper1,000
livebirths in1990 (95%CI: 109, 178) to108 in2010(95%CI: 81,144);
however, this declinewas not statisticallysignificant. In2010,
thedistrictsunder-5mortalitywascom-parabletothenationalaverageof109deathsper1,000livebirths
(95%CI:104,116). It is important tonotethatbefore
2000,theunder-5mortalityinMumbwawasgenerallylowerthanthenationaltrend.
Theproportionof
childrenwhowereunderweightgrad-uallydecreasedfrom15%inthe1990sto12%in2005(95%CI:10%,15%).Underweightremainedat12%through2010,whichwasslightlylowerthanthenationalaverageof14%forthatyear.
CHILD HEALTH OUTCOMES
SUMMARYMumbwareducedall-causeunder-5mortalityandchildhoodunderweightfrom1990to2010,buttherelativemagnitudeofthedistrictsprogresswasfairlylow.Prioritizingwaystoaccel-erategainsforchildhealthoutcomesshouldbeconsidered.
Thedistrictrapidlyscaledupcoverageofthepentavalentvaccineandexclusivebreastfeeding,exceedingthenationalaverage
for each in 2010.Mumbwa recorded some of thehighest levels of polio
coverage in the country, and
experi-encedgradualgainsinskilledbirthattendance.
However,amidstthesegains,sometroublingtrendswereidentifiedandwarrant
furtherattention.Mumbwasawsmalldeclinesinmeaslescoverageinthelate2000s.Whilethedis-
trictwasabletoquicklyscaleupcoverageofITNsandIPTp2,coveragelargelyfellbelowthenationalaveragein2010.Fur-ther,
ITNownershipandusedropped toamong the lowestlevels in Zambia in
2010. Like inmany districts, ANC4
cov-eragedecreasedafteraperiodofincreasinglevelsduringthe1990s.
In 2010, Mumbwa generally met or exceeded nationallevels for
immunizations and maternal and child
healthinterventions,butfellbelownationalaveragesformalariainter-
ventions.Incomparisonwiththenationalaverage,Mumbwashowedsimilarlevelsofmortalityandslightlylowerlevelsofunderweight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Mumbwa Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Mumbwa
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes
(orange)andhigherlevelsofinterventioncoverage(green).
Mumbwa
-
2 7
ITNownership remainedbelow10%until2002,afterwhichcoverage
quickly increased to 50% in 2008 (95% CI:
44%,56%).Ownershipslippedto47%in2010(95%CI:41%,53%),fallingwellbelowthenationalaverageof62%andamongthelowestlevelsinZambia.
ITNusebychildrenunder5yearsoldsteadilyroseto35%in2010(95%CI:28%,42%),butthislevelofITNuseremainedwellbelowthenationalaverageof51%andwasamongthelowestinthecountry.ThedifferencebetweenITNownershipanduse(12percentagepoints)inMumbwawascomparable
towhatwasobservedatthenationallevelfor2010.MumbwaformallyimplementedIRSactivitiesin2008,and
reached39%ofhouseholdsin2010(95%CI:34%,45%).Thisscale-upofIRSwasaboutaverageamongtheotherdistrictsthatalsobeganIRSin2008.
Theproportionofpregnantwomenwho received IPTp2remained below 10%
until 2001, after which coverage
rap-idlyroseto65%in2008(95%CI:51%,78%).IPTp2coverageslippedto62%in2010(95%CI:49%,75%),whichwaslowerthanthenationalaverageof68%.
BCGcoveragedecreasedfrom97%intheearly1990sto93%inthelate1990s,butincreasedto98%in2009(95%CI:96%,99%)andremainedat98%through2010.This
levelofBCGimmunizationexceededthenationalaverageof95%for2010.
Measles immunization increased from a low of 79%
in1990(95%CI:65%,89%)to98%in2002(95%CI:96%,98%).Coverageremainedat98%through2003,butdecreasedto96%in2010(95%CI:88%,99%),fallingslightlybelowthena-tionalaverageof98%.
Coverage of polio immunization climbed from 68%
in1990(95%CI:52%,82%)to84%inthemid-1990s.Poliocov-eragehoveredaround80%until2004,afterwhichcoveragesteadilyincreasedto98%in2010(95%CI:95%,100%),risingtoamongthehighestinZambiaforthatyear.
Afterthepentavalentvaccinewasformally
introducedinMumbwain2005,coverage increasedto61%in2006(95%CI: 54%,
69%) and 80% in 2010 (95% CI: 66%, 89%),
ex-ceedingthenationalaverageof67%.
ANC4coveragehoveredaround60%duringtheearlytomid-1990sand then
increased to69% in
theearly2000s.ANC4thendecreasedto56%in2010(95%CI:19%,88%).WhilethislevelofANC4coveragewasstillhigherthanthenationalav-erageof37%for2010,itremainedlowerthanoptimal.
Skilled birth attendance gradually climbed from 33%
in1990(95%CI:20%,47%)to61%in2010(95%CI:25%,90%),
whichwasslightlyhigherthanthenationalaverageof55%forthatyear.
Theproportionofchildrenwhowereexclusivelybreastfedremainedbelow20%until1999,afterwhichcoverageroseto60%in2003(95%CI:53%,67%).Gains
incoveragesloweduntil2007andthenquicklyclimbedto91%in2010(95%CI:82%,95%),farexceedingthenationalaverageof80%.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
Indoor residual spraying
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 2005 2010
Skilled birth attendance
0
20
40
60
80
100
1990 1995 2000 2005 2010
Exclusive breastfeeding
0
20
40
60
80
100
1990 1995 2000 2005 2010
-
2 8
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From1990to2010,Serenjerecordedasignificantreductioninall-causeunder-5mortality,dropping43%from188deathsper1,000livebirthsin1990(95%CI:147,236)to107in2010(95%CI:78,145).In2010,thedistrictsunder-5mortalitywascomparabletothenationalaverageof109deathsper1,000livebirths(95%CI:104,116).
Theproportionofchildrenwhowereunderweightsteadilydeclinedfrom30%in1990(95%CI:20%,43%)to18%in2009(95%
CI: 14%, 23%), which was maintained through
2010.Despitethisprogress,Serenjesprevalenceofchildhoodun-derweightremainedhigherthanthenationalaverageof14%for
2010.
CHILD HEALTH OUTCOMES
SUMMARYSerenjerecordedsubstantialreductionsinall-causeunder-5mortalityandchildhoodunderweightfrom1990to2010,butits
levelsofunderweight remainedhigher than
thenationalaveragein2010.Prioritizingwaystoaccelerategainsforchildhealthoutcomesshouldbeconsidered.
MalariainterventioncoveragequicklyincreasedinSerenjeandwassustainedthrough2010.SerenjeexpandedcoverageofBCGandmeaslesimmunizationafterdeclinesintheearlytomid-2000s,andthedistrictsawsubstantialgainsinskilledbirthattendanceafteryearsofextremelylowcoverage.Exclu-sivebreastfeedingalsowashigherthanthenationalaveragein2010.
At thesame time,Serenjemarginally scaledup thepen-
tavalent vaccine, and polio coverage steeply fell in
recentyears.In2010,thedistrictrecordedsomeofthelowestlevelsof
coverage in Zambia for these two immunizations. ANC4coverage
dramatically decreased to among the
lowestlevelsinthecountry.WithitslowlevelsofANC4inparticular,Serenjewill
likelybenefit from targeting these interventionsforimprovement.
In2010, Serenjegenerally equaledorexceeded
thena-tionallevelsformalariainterventionsandmaternalandchildhealthinterventions(excludingANC4).Serenjesperformanceacross
immunizations wasmore varied. In comparison withthe national
average, Serenje showed similar levels
ofmor-talityandhigherlevelsofunderweight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Serenje Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Serenje
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes
(orange)andhigherlevelsofinterventioncoverage(green).IRScoveragewasnotincludedbecauseSerenjestartedIRSafter2010.
Serenje
-
2 9
ITNownership remainedbelow10%until2003,afterwhichcoverage
rapidly rose to 65% in 2010 (95%CI: 58%,
72%),slightlyexceedingthenationalaverageof62%.
ITNusebychildrenunder5yearsoldquickly
increasedto51%in2010(95%CI:42%,58%),equalingthenationalav-erage for
that year. The difference between ITN
ownershipanduse(14percentagepoints)wasslightlyhigherinSerenjethanwhatwasobservedatthenationallevel(11percentage
points)for2010.IRScoveragetrendsarenotincludedbecauseSerenjedid
notbeginformalIRSactivitiesuntilafter2010.Theproportionofpregnantwomenwho
received IPTp2
remained below 10% until 2003, after which coverage
rap-idlyroseto69%in2009(95%CI:56%,79%).IPTp2coverageslippedto68%in2010(95%CI:54%,79%),equalingthena-tionalaveragefor2010.
BCG coverage increased from 69% in 1990 (95% CI:
54%,81%)to95%inthemid-1990s,butfellto90%duringthemid-2000s.Coverage
rebounded to95% in2010 (95%CI:
89%,98%),equalingthenationalaverageforthatyear.
Measlesimmunizationquicklyrosefrom56%in1990(95%CI:40%,73%)to92%duringthemid-tolate1990s.Measlescoverage
dipped below 90% during themid-2000s beforesteadily rising to99%
in2010
(95%CI:96%,100%),slightlyexceedingthenationalaverageof98%forthatyear.
After rising from 67% in 1990 (95% CI: 51%, 80%),
cov-erageofpolioimmunizationhoveredaround77%untilrising
to79%inthelate1990s.Poliocoveragethensteadilydeclined,droppingto46%in2010(95%CI:28%,66%)andfallingwellbelow
the national average of 81%.This level of polio
cov-eragewasamongthelowestinZambiafor2010.
Afterthepentavalentvaccinewasformally
introducedinSerenjein2005,coveragehoveredaround40%through2009,risingslightly
to45%in2010
(95%CI:29%,63%).Serenjeslevelofpentavalentcoveragewaswellbelowthenationalav-erageof67%for2010,andwasamongthelowestinZambia.Thedistrictsminimal
scale-upof thepentavalent vaccine iscause for concern.
ANC4 coverage increased from38% in 1990 (95%CI:
26%,52%)to67%in1998(95%CI:49%,81%),butsteadilydeclinedthereafter,droppingto14%in2010(95%CI:2%,41%)andfallingbelowthenationalaverageof37%.Alarmingly,Seren-jesANC4coveragewasamongthelowestinZambiafor2010.
Skilledbirthattendancedeclinedfrom30%in1990(95%CI:18%,43%)to13%inthe
late1990s,butsteadilyroseto66%in2010(95%CI:28%,92%),whichwashigherthanthenational
averageof55% for that year. Serenjesprogress in
improvingitsSBAcoverageisnotablegiventhatthedistrictconsistently
recorded levelsof coveragewell below
thena-tionalaverageuntilthelate2000s.
Theproportionofchildrenwhowereexclusivelybreastfedremainedbelow20%until1999,afterwhichcoveragerapidlyrose
to 70% in 2003 (95% CI: 63%, 76%). Exclusive
breast-feedingcoverageremainedaround70%until2007,climbingto 86% in
2010 (95%CI: 77%, 93%) and exceeding the na-tionalaverageof80%.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 2005 2010
Skilled birth attendance
0
20
40
60
80
100
1990 1995 2000 2005 2010
Exclusive breastfeeding
0
20
40
60
80
100
1990 1995 2000 2005 2010
-
3 1
Copperbelt province
-
3 2
KEY
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
Allcause under5 mortality
40
120
200
280
360
1990 1995 2000 2005 2010
Childhood underweight
0
20
40
60
80
100
1990 1995 2000 2005 2010
From1990to2010,Chililabombwerecordedasmall reduc-tion in
all-cause under-5 mortality, dropping 7% from
131deathsper1,000livebirthsin1990(95%CI:101,169)to122in 2010
(95%CI: 89, 165). This declinewas not
statisticallysignificant.In2010,thedistrictsunder-5mortalitywasmuchhigherthanthenationalaverageof109deathsper1,000livebirths(95%CI:104,116).Thislackofprogressisworrisome
given that the districts levels of under-5mortality were
farbelowthenationaltrendduringthe1990s.
The proportion of children who were underweight
in-creasedfrom13%intheearly1990sto17%in1998(95%CI:13%,21%),and
remainedat this level
through2002.Under-weightthendeclinedto14%inthelate2000s,equalingthenational
average for 2010.Overall, thedistrict
showedmar-ginalprogressinreducingchildhoodunderweight.
CHILD HEALTH OUTCOMES
SUMMARYChililabombwehadminimalreductionsinitsall-causeunder-5mortalityandchildhoodunderweightfrom1990to2010;fur-ther,thedistrictslevelsofunder-5mortalityremainedhigherthanthenationalaverage
in2010.Prioritizingwaystoaccel-erategainsforchildhealthoutcomesshouldbeconsidered.
Thedistrictgenerallyincreasedandmaintainedcoverageof IRS and
IPTp2, and rapidly scaled up the
pentavalentvaccine.Chililabombwesustainedhighlevelsofmeaslescov-erageovertime,andbroughtupexclusivebreastfeedingafteraperiodofstalledgains.ThedistrictsBCGcoveragein2010wasamongthehighestinZambia.
However,amidstthesesuccesses,sometroublingtrendswere identified
andwarrant further attention. ITN coverage
wasmuchlowerthanthenationalaverage,andpolio immu-nization fell
to oneof the lowest levels in Zambia for
2010.ANC4coveragesteadilydeclinedtovery lowlevels
in2010,andalarmingly,skilledbirthattendancefellfromhighlevelsofcoverageinthe1990s.
In 2010, Chililabombwe generally met or exceeded na-tional
levels for immunizations (with theexceptionofpolio),but fell below
for maternal and child health interventions.The district had a more
mixed performance for malariainterventions. Incomparisonwith
thenationalaverage,Chil-ilabombwe showed higher levels of mortality
and similarlevelsofunderweight.
Dea
thsper1,000
livebirths
Percen
t(%)
Nationaltrend Chililabombwe Uncertaintyinterval
Rangeobserved acrossdistricts
Nationalaverage
Chililabombwe
Deat
hs p
er 1
,000
live
birth
s
60
80
100
120
140
160
CHILD HEALTHOUTCOMES
Childhoodunderweight
Under-5mortality
Malaria Immunizations Maternal & child health
INTERVENTIONS
IPTp(2 doses)
Exclusivebreastfeeding
Antenatalcare
(4 visits)
ITNownership
ITN useunder-5
Indoor residualspraying
BCG PentavalentMeasles Polio Skilledbirth
attendance
0
20
40
60
80
100Pe
rcen
t (%
)
0
20
40
60
80
100
Perc
ent (
%)
Note:Levelsofchildhealthoutcomesandinterventioncoveragearefor2010.Betterperformanceisreflectedbylowerlevelsofchildhealthoutcomes
(orange)andhigherlevelsofinterventioncoverage(green).
Chililabombwe
-
3 3
ITNownership
remainedbelow10%until2003,afterwhichcoverageincreasedto46%in2010(95%CI:36%,56%).ThislevelofITNownershipwaswellbelowthenationalaverageof62%for2010,andwasamongthelowestinZambia.
ITNusebychildrenunder5yearsoldroseto43%in2010(95%CI: 31%, 55%),
which was lower than the national
av-erageof51%.In2010,thedifferencebetweenITNownershipandITNusewasquitelow,whichsuggeststhatnetusebychil-drenunder5maybehighamonghouseholdsthathaveITNs.
ChililabombweformallyimplementedIRSactivitiesin2000,andwasoneofthefirst15districtsinZambiatorolloutIRS.IRScoveragepeakedat58%in2008(95%CI:53%,63%),slightlydecreasingto55%in2010(95%CI:47%,61%).
Theproportionofpregnantwomenwho received IPTp2remained below 10%
until 2002, after which coverage
rap-idlyroseto79%in2008(95%CI:65%,89%).IPTp2coverageslipped to 76%
in 2010 (95%CI: 60%, 88%), but
remainedabovethenationalaverageof68%.
Risingfrom97%intheearly1990s,BCGcoverageremainedat98%through2010,whichexceededthenationalaverageof95%andwasamongthehighestinthecountry.
Measles immunization declined from 98% in the
early1990sto95%duringthelate1990s,butincreasedto99%in2007(95%CI:98%,99%)andremainedat99%through2010.Thislevelofcoveragewasslightlyhigherthanthenationalav-erageof98%for2010.
Coverage of polio immunization dropped from 98%
in1990(95%CI:96%,99%)to81%inthemid-1990s,butclimbed
to94%in2002(95%CI:90%,96%).Poliocoveragethende-clinedsharply,droppingto48%in2010(95%CI:26%,72%),amongthelowestlevelsinZambia.Thisdecreaseiscauseforconcerngiven
that thedistrict consistently
recordedhigherlevelsofcoveragethanthenationaltrendpriorto2006.
Afterthepentavalentvaccinewasformally introducedinChililabombwe
in2005,coverage
increasedto40%in2007(95%CI:33%,47%)and75%in2010(95%CI:60%,87%),ex-ceedingthenationalaverageof67%.
ANC4 coverage dropped considerably from 90% in
1990(95%CI:80%,96%)to15%in2010(95%CI:2%,48%),fallingbelowthenationalaverageof37%for2010.ANC4dramati-callydecreasedthroughoutZambiafrom1990to2010,andthe
finding that Chililabombwes levels of coverage fell
75percentagepointsduringthistimeistroubling.
After rising to 98% in themid-1990s, skilled birth
atten-dancedecreasedto52%in2010(95%CI:12%,88%),whichwasslightlylowerthanthenationalaverageof55%.However,
this decline in SBA coverageduring the 2000s is cause
forconcerngiven that its levelsof coveragehadpreviously
ex-ceededthenationaltrendbyatleast40percentagepoints.
Theproportionofchildrenwhowereexclusivelybreastfedremainedbelow20%until1995,afterwhichcoverageroseto54%
in2001 (95%CI:47%,62%).Gains
incoveragestalleduntil2007,andexclusivebreastfeedingthenclimbedto77%in2010(95%CI:64%,87%).Thislevelofcoveragewasslightlylowerthanthenationalaverageof80%for2010.
MALARIA INTERVENTIONS
IMMUNIZATIONS
MATERNAL AND CHILD HEALTH INTERVENTIONS
ITN ownership
0
20
40
60
80
100
1990 1995 2000 2005 2010
ITN use by children under 5
0
20
40
60
80
100
1990 1995 2000 2005 2010
Indoor residual spraying
0
20
40
60
80
100
1990 1995 2000 2005 2010
IPTp (2 doses)
0
20
40
60
80
100
1990 1995 2000 2005 2010
BCG immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Measles immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Polio immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Pentavalent immunization
0
20
40
60
80
100
1990 1995 2000 2005 2010
Antenatal care (4 visits)
0
20
40
60
80
100
1990 1995 2000 20