Embed Size (px)
DESCRIPTION
PROGRESS & MAIN CHALLENGES IN TB DRUG R&D. Expert consultation Geneva 11 Apr 2008. Martina Casenghi, PhD Biologist. An improved landscape for TB drug R&D. Establishment of TB Alliance in 2000-Associated approximately with half of projects in the pipeline. - PowerPoint PPT Presentation
Citation preview

PROGRESS & MAIN CHALLENGES IN TB DRUG R&D
Martina Casenghi, PhD
Biologist
Expert consultation
Geneva 11 Apr 2008
An improved landscape for TB drug R&D An improved landscape for TB drug R&D
Few multinational Pharma companies (Novartis, GSK, AstraZeneca, Eli-Lilly, Sanofi Aventis, J&J, Pfizer) engaged in R&D for anti-TB drug on a “no-profit-no-loss” basis
Establishment of TB Alliance in 2000-Associated approximately with half of projects in the pipeline
Several other small-middle size Pharma companies -i.e. Otsuka, Lupin, Chiron, FasGen, Sequella etc.- engaged in R&D for anti-TB drug
TB Alliance strategy for identification of novel compounds
-shortening of treatment
-active against MDR-TB
-no interactions with ARVs
b-SulfonylcrboxamidesJohns Hopkins Univ, NIH
Cell Wall Biosynthesis InhibitorsSeveral Institutions
Mycobacterial Siderophore Biosynthesis Inhibitors-CDD Univ Minnesota, NIAID, NIH
Dihydrolipoamide Acyltransferase InhibitorsCornell Univ, NIAID
Diphenyl ether based inhibitors of FabI (InhA) Stony Brook, NIH,NIAID, CSU, NJRMC, Univ Wuzburg
Nitroimidazole analogsTB Alliance, Univ Auckland
Ftsz InhibitorsStony Brook, Colorado State Univ, SRI
Indole DerivativesColorado State Univ, NIH, INEOS Moscow
Novartis portfolioNovartis
Myocobacterial Sulfation Pathway Inhibitors-Univ California Berkley, NIH
Malate Synthase InhibitorsGSK, Rockefeller Univ, Texas A&M, TB Alliance
PleuromutilinesGSK, TB Alliance
Natural Products ExplorationSeveral institutions
Mycobacterial Gyrase InhibitorsGSK, TB Alliance
Promazine AnalogsSalisbury University
NitrofuranylamidesNIH, NIAID, Univ Tennessee, Colorado State Univ
Peptide Deformylase InhibitorsGSK, TB Alliance
QuinolonesKRICT, Yonsey Univ, TB Alliance
OxazolidinononesPfizer
Proteasome InhibitorsCornell Univ, NIAID
Small molecules Inhibitors of validated target-Seattle Biomed research Inst., BMGF
Phenotypic Whole cell Screening(1) Univ Illinois Chicago,TB Alliance (2) NIH, NIAID, TAACF (3) Astra zeneca
Sanofi Aventis PortfolioSanofi-Aventis
NM4TBAstraZeneca, European Commission
Protease InhibitorsIDRI
Type II NADH-menaquinone oxireductase InhibitorsUniv Pennsylvania, Univ Illinois Chicago, NIH
Multi-Functional MoleculesCumbre, TB Alliance, Colorado State Univ
RiminophenazinesInst. of Materia Medica, BTTRI, TB Alliance
Energy MetabolismGSK, TB Alliance
InhA InhibitorsGSK, TB Alliance
Target Based ScreeningAstraZeneca
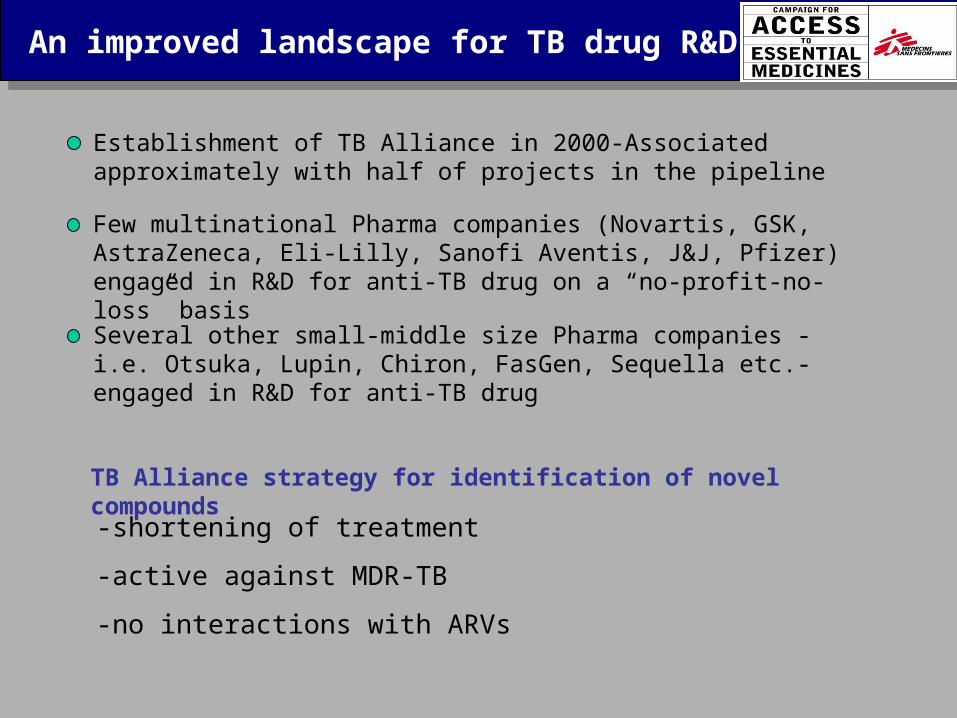
DISCOVERY
(STOP TB WG on new Drugs Annual Meeting, Cape Town Nov 2007)

Pre-clinical
Dipiperidine SQ-609
Sequella Inc.
Gyrase Inhibitor
Pharma
Compounds with in vivo activity against M.tb in animal models-NIH, NIAID, Colorado Univ
Nitroimidazole Backup compound
Otsuka Pharm.
Non-fluorinated Quinolone
TaiGen
Oxazolidinones
Pfizer
Synthase Inhibitor FAS20013
Fasgen Inc
Translocase I Inhibitors
Sequella Inc., Sankyo
(STOP TB WG on new Drugs Annual Meeting, Cape Town Nov 2007)
HIV drug preclinical pipeline: ~ 100 compounds!
(TAG report http://www.aidsinfonyc.org/tag/tx/pipeline2006a.html)

Clinical Development
Moxifloxacin
(1) Bayer, TB Alliance, CDC TBTC, JHU, TB Alliance (2) DMID/NIAID/NIH, TBRU
Diamine SQ-109
Sequella
Vitamin D
Christian Medical College Vellore, Dalhousie Univ
Gatifloxacin
OFLOTUB Consortium
Pyrrole LL-3858
Lupin Limited
Linezolid
(1)DMID/NIAID/NIH, TBRU;
(2) CDCTBTC
Diarylquinoline TMC 207
Tibotec Pharm. Ltd
Levofloxacin
DMID/NIAID/NIH, TBRU
Rifapentine
Sanofi-Aventis, TBTC
Nitrodihydro-imidazooxazole OPC- 67683
Otsuka pharm
Capreomycin for Inhalation
MEND, NIAID, BMGF
Metronidazole for Latent Infection
Imperial College London, BMGF, Wellcome Trust
Nitroimidazole PA-824
TB Alliance
High dose Rifampicin
Univ. of Nijmegen, EDCTP
(STOP TB WG on new Drugs Annual Meeting, Cape Town Nov 2007)
HIV drug clinical pipeline: ~ 30 compounds!
(TAG report http://www.aidsinfonyc.org/tag/tx/pipeline2006b.html)

Limitations of current pipelineLimitations of current pipeline
Approximately 40 compounds in the pipeline-That’s not enough
• In average in a drug discovery program for anti-infectives only 1 compound in 20 makes it (Payne et al., 2007)
• Glickman et al. (Glickman et al., Science 2006):
-likelihood of introducing at least one successful anti-TB drug by 2010 is < 5%
- likelihood to introduce a novel regimen with at least 2 new drugs by 2015 is < 1%
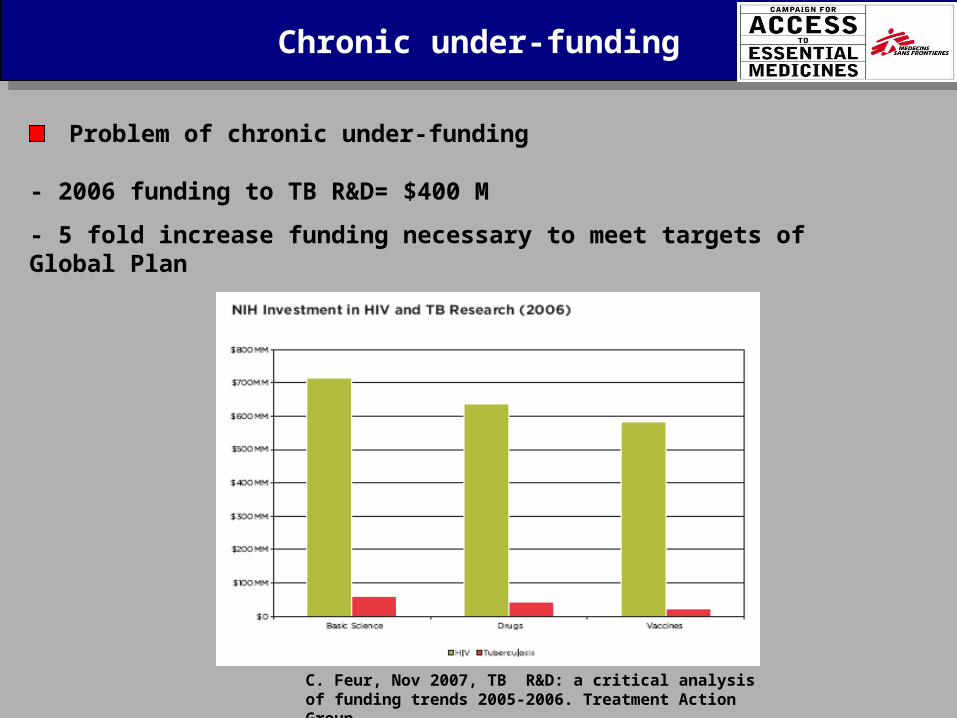
Chronic under-fundingChronic under-funding
Problem of chronic under-funding
- 2006 funding to TB R&D= $400 M
- 5 fold increase funding necessary to meet targets of Global Plan
C. Feur, Nov 2007, TB R&D: a critical analysis of funding trends 2005-2006. Treatment Action Group

Critical bottlenecks in TB drug R&D Critical bottlenecks in TB drug R&D
RESEARCH:• Drug Discovery
DEVELOPMENT:• Clinical Trial Capacity
• Accelerate TB drug development-Test new drugs in MDR-TB patients-need for reliable biomarkers that correlates with clinical cure
Gaps in the TB drug R&D pipeline:
-MSF/Weill Cornell Medical college supported symposium to discuss roadblocks and possible solutions (Jan 2007)
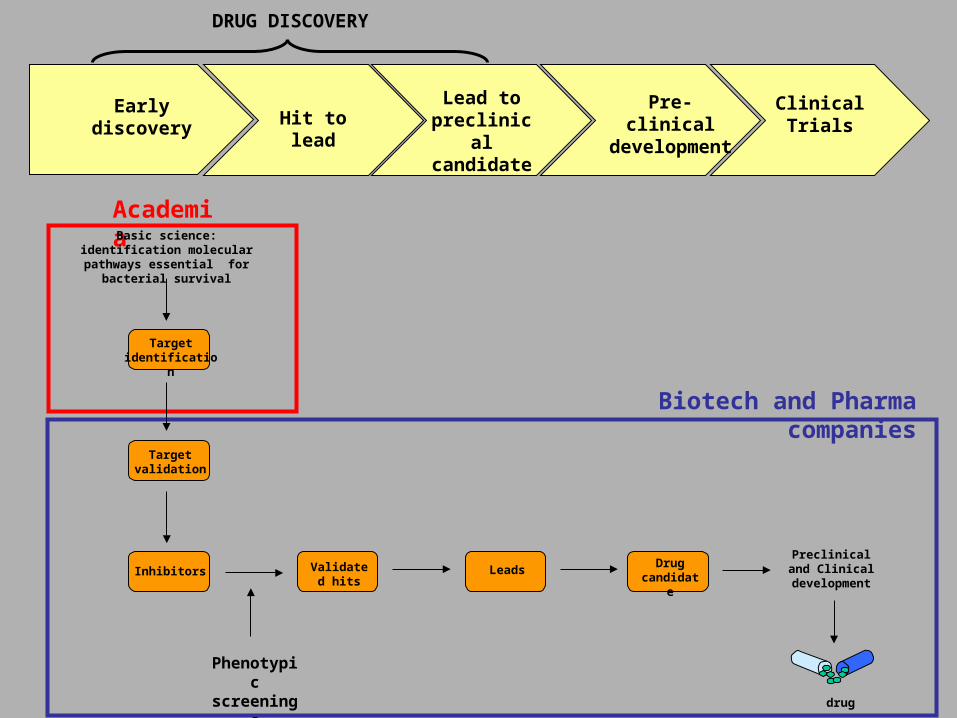
Early discovery Hit to lead
Lead to preclinical candidate
Pre-clinical developme
nt
Clinical Trials
DRUG DISCOVERY
Biotech and Pharma companies
Academia
Validated hits
Target validation
Inhibitors
Target identification
LeadsDrug
candidate
Preclinical and Clinical
development
drug
Basic science: identification molecular pathways
essential for bacterial survival
Phenotypic
screenings

Filling the TB drug pipelineFilling the TB drug pipeline
THE PROBLEM:A) TB drug R&D too risky from a commercial perspective
limited engagement from private sector
- Small number of compounds in the pipeline is reflected by low number of Pharma companies involved in TB R&D
(MSF TB drug pipeline report, Oct 2006)
Drugs Pharma companies
DALYs

Filling the TB drug pipelineFilling the TB drug pipeline
THE PROBLEM:B) Academic scientists carry out drug discovery projects but in sub-optimal conditions because of:
1) ACCESS TO TOOLS & EXPERTISE BARRIERLack of access to:-appropriate compound libraries-screening facilities-medicinal chemistry and pharmacology expertise
2) FUNDING BARRIER: limited access to funding streamlines to run applied research projects
C) TB Alliance had limited capacity to impact early stage drug discovery

?
TB Alliance
Validated hits
Target validation
Inhibitors
Target identification
LeadsDrug
candidate
Preclinical and Clinical
development
drug
Basic science: identification molecular pathways essential
for bacterial survival
Academia
Biotech and Pharma companies

Filling the TB drug pipelineFilling the TB drug pipeline
PROBLEM PERSIST DESPITE THE CONTRIBUTION OF RECENT INITIATIVES:
- NIH/NIAID funded facilities for compound screenings (TACCF) and comprehensive target validation (TARGET)
- Gates foundation funded projectsa) Grand Challenges for Global Health # 11 “Drugs for treatment of latent TB infection” : grant awarded in 2005, $20Mb) TB drug Accelerator: launched beginning of 2006, $40M over 2 years
- EU funded New Medicines for TB (NM4TB) project (about 10 M euro over 5 years)
- TB drug R&D facilities established by few multinational companies (often represent private partner of grant funded consortia)

Filling the TB drug pipelineFilling the TB drug pipeline
MAJOR CHALLENGE THAT THESE RECENT INITIATIVES HAVE TO FACE:- Run drug discovery projects on a VIRTUAL basis- Big consortia, collaborators spread all over the world-
coordination is a challenge
Certainly helpful contributions but NOT able to trigger the substantial boost in TB drug R&D that is necessary

Filling the TB drug pipelineFilling the TB drug pipeline
(Nathan, Nat. Med 2007)
PROPOSAL EMERGED at the MSF TB drug symposium (Jan 2007):
RESEARCH:• Drug Discovery
DEVELOPMENT:• Clinical Trial Capacity
Critical bottlenecks in TB drug R&D Critical bottlenecks in TB drug R&D
Clinical Trial capacity gapClinical Trial capacity gap
THE PROBLEM:
-Clinical Trials need to be performed in high burden countries
- High-burden countries have poor capacity to run clinical trials conforming to international guidelines (ICH/GCP and GLP)
CLINICAL TRIAL CAPACITY:
-Infrastructures (lab and health facilities adequate to run research projects conforming to international standards)
-Trained personnel
-Functioning Institutional review boards/ethics committees
-Regulatory guidance at national level

Clinical Trial capacity gapClinical Trial capacity gap
BUILDING of CLINICAL TRIALS CAPACITY in HIGH BURDEN COUNTRIES: (Schluger et al., PLoS Med. 2007):
-Currently, specific funding for clinical trials capacity building is tied to individual drugs in the pipeline
-Important to make direct investments in the infrastructure rather than taking a product-by-product approach
-Big funding gap:
2005 worldwide expenditures in clinical trials= US $20-30M
Experts estimation of needed funding= US$ 300-US$500M annually

CONCLUSIONSCONCLUSIONS
• TB DRUG R&D landscape significantly improved in the last 10 years
• Current approaches and initiatives represent useful contribution to revitalize the field BUT they are NOT sufficient to:
- ensure the creation of a sustainable pipeline
- ensure the delivery of new products with timeframes that reflect the urgency of the situation
• Alternative mechanisms and approaches to fund and organize R&D activities are required if we want to trigger a real change that can radically solve the problem


CONCLUSIONSCONCLUSIONS
(Nathan, Nat. Med 2007)
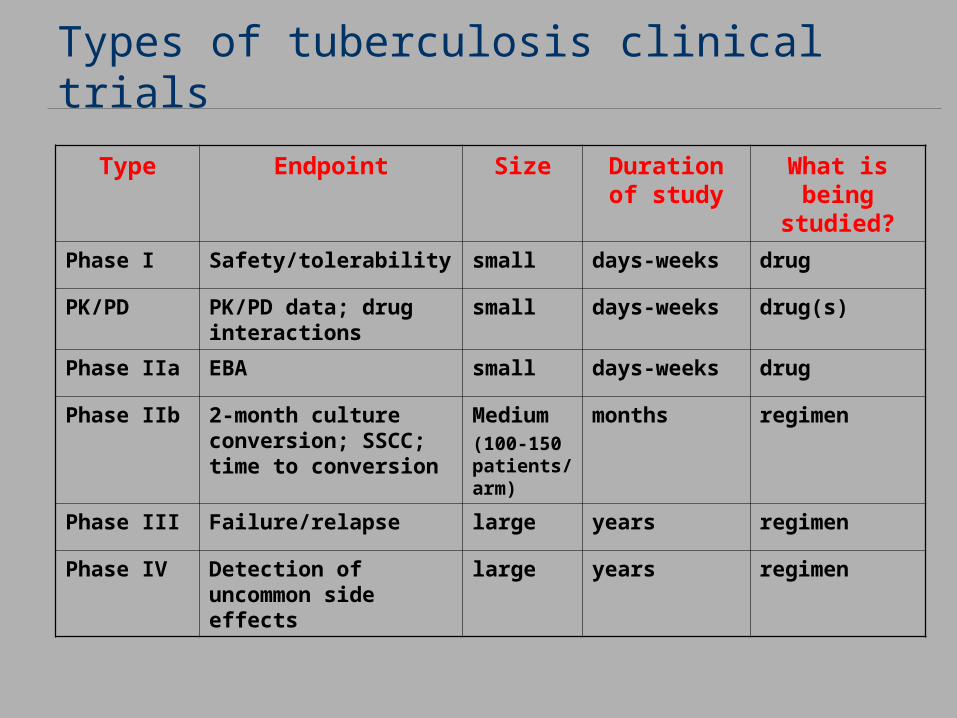
Types of tuberculosis clinical trials
Type Endpoint Size Duration of study
What is being studied?
Phase I Safety/tolerability small days-weeks drug
PK/PD PK/PD data; drug interactions
small days-weeks drug(s)
Phase IIa EBA small days-weeks drug
Phase IIb 2-month culture conversion; SSCC; time to conversion
Medium(100-150 patients/arm)
months regimen
Phase III Failure/relapse large years regimen
Phase IV Detection of uncommon side effects
large years regimen