Embed Size (px)
Citation preview

PROGRESSIVE CHANGES I N T H E SMALL-INTESTINAL VILLOUS PATTERN WITH INCREASING LENGTH OF GESTATION
ANNE FERGUSON, J. D. MAXWELL AND KATHARINE E. CARR* University of Glasgow Department of Medicine, Glasgow Royal Infirmary, and the
*Bioengineering Unit, University of Strathclyde
PLATE XXXVIII
IN the newborn human infant, the small intestine is said to be lined with long, finger-like villi (Baker et al., 1962; Stanfield, Hutt and Tunnicliffe, 1965). In older children there is a mixture of finger-, tongue- and leaf-villi and short ridges (Walker-Smith, 1967). The original purpose of this study was to determine the factors causing changes in the intestinal villi after birth. When the results were assembled it became obvious that the original premise (that the villous pattern at birth is of sheets of finger-villi) was incorrect. We therefore report in this paper the results of observations on the intestinal villous pattern in these human infants.
MATERIAL AND METHODS
At routine necropsies in the Royal Hospital for Sick Children, Glasgow, and the Glasgow Royal Maternity Hospital, the small intestine was sampled at four levels. Two to four centimetre segments were removed from the duodenum (second part), jejunum, and the proximal and distal ileum, placed in normal saline and allowed to autolyse for 4-5 days. The pieces of gut were then cut longitudinally and washed, and the mucosal surface was examined with the dissecting microscope with either transmitted or incident light. After examination the tissues were stored in formalin.
All specimens were examined without knowledge of the clinical or autopsy findings. They were classified as: type F--finger-villi only; type FT-mixture of finger- and tongue- (deltoid) villi; and type FTL-mixture of finger-, tongue- and leaf-villi.
Some specimens were examined subsequently by scanning electron microscopy (Carr and Toner, 1968; Swift and Marsh, 1968; Toner and Carr, 1969).
Tissues were washed in Sorensen’s phosphate buffer to remove formalin and were post- fixed in 1 per cent. aqueous osmium tetroxide. Specimens were pinned out on cork, air-dried, mounted on metal stubs and vacuum-coated with approximately 50 nm of gold palladium, and then examined with the Cambridge Mark IIA stereoscan scanning electron microscope, operated at an accelerating voltage of from 10 to 30 kV. The results were recorded on IIford FP4 120 film, with a Zenza S Bronica camera with a 2+ in. (55 mm) frame. The villous architecture displayed by the scanning electron microscope agreed with the classification assigned to these specimens by dissecting microscopy.
After 40 groups of tissues had been examined, the necropsy and clinical records were con- sulted. Details were obtained of maternal history, gestation, labour, progress of baby after birth, feeding, therapy, and the cause of death.
Of the 40 infants, 11 were stillborn and 29 survived after birth for periods ranging from 10 min. to 4 days. Details of gestation and causes of death are contained in the table. There
Received 30 Apr. 1969; accepted 22 May 1969. J. PATH.-VOL. 99 (1969) 87

88 ANNE FERGUSON, J . D. MAXWELL AND KATHARlNE E. CARR
was serious maternal disease in only one case, a woman with severe multiple sclerosis who was delivered of a full-term stillborn anencephalic baby. Only two of the babies had been given milk. Therapeutic measures included resuscitation at birth, antibiotics if indicated, and correction of acidosis with intravenous fluids.
TABLE Details of length of gestation and causes of death in the 40 infants
1 Number of infants dying from this cause
c. 34 wk ~ _ _ _
0 6 0 0 2 0 3
~-
11
Cause of death i at length of gestation
term ~
0 0 2 6 0 4 0
- _ _
12
I 1 c. 26 wk c. 30 wk
Prematurity Respiratory distress syndrome Congenital heart disease Other congenital malformations Rhesus incompatibility Abnormality in labour Unknown
Total I 9 l 8
Total
7 15 2 7 2 4 3
40
RESULTS In these partly autolysed tissues the general contours of the mucosal surface
are retained (Loehry and Creamer, 1966). These authors described, in the adult
F MIL
FTL Mnii 0 0
S.B. , I
Length of life (hr) 0 20 40 60 80 100
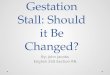
FIG. 3.--Jejunal villous pattern related to duration of extra-uterine life in the 40 infants.
small intestine, different types of villi, crypt mouths, intervillous ridges and Peyer’s patches. All these features were easily seen in the infant mucosa. Scanning electron microscopy confirmed these findings in several cases and allowed clear visualisation of villous shape. Fig. 1 is a low-power scanning

FORMS OF FOETAL SMALL-INTESTINAL VILLI 89
electron micrograph of the jejunal surface showing the cores of tongue- and finger-villi. The openings of crypts can be seen between the villi. Fig. 2 shows several villi at higher magnification. Although some bending of the villi has occurred the shape of individual villi is satisfactorily demonstrated.
F ivin FT AA
FT L AN-I
a. .a i t
.a
a li tr Prematurity Respiratory Congenital Others
distress malformation syndrome
FIG. 4.-Jejunal villous pattern related to the cause of death in the 40 infants.
F
FT M FTL MA
: e t a 0 .
22 26 30 34 38 42
Length of gestation (weeks from conception)
FIG. 5.-Jejunal villous pattern related to length of gestation (expressed as weeks since conception, assuming conception 2 wk after last menstrual period).
Duodenum. Thirty-six duodenal specimens were available for study. In 29 the pattern was of parallel broad-leaf villi or short ridges, with the long axes of villi running transversely around the gut. The other 7 specimens were of type FT.
Jejunum. Of the 40 specimens of jejunum, 9 were graded as F, 16 as FT and 15 as FTL. In figs. 3-5 we illustrate the relation between jejunal villous pattern and duration of extra-uterine life, cause of death and time since con- ception (assuming conception to have taken place 2 wk after the mother’s last menstrual period).

90 ANNE FERGUSON, J. D. MAXWELL AND KATHARINE E. CARR
The villous pattern was not correlated with length of life. There was some correlation with the cause of death, for types F and FT were found in most babies dying as a result of prematurity or the respiratory distress syndrome. There was a clear relationship between the villous pattern and the length of gestation. Up to 26 wk after conception type F predominated. From 26 to 34 wk type FT was most frequent. After 34 wk the pattern was FTL in all but one case.
Ileum. Examination of specimens from the proximal and distal ileum gave results very similar to those for jejunum, with the same relation to the length of gestation.
DISCUSSION In most newborn mammals the small intestine is lined with tall cylindrical
finger-villi (verzar and McDougall, 1936). However, this pattern is present in only a minority of these 40 human infants, born during the third trimester and dying within 4 days of birth. It is possible that in some cases anoxia or infec- tion, ante- or post-natal, led to the development of abnormal villi. This seems unlikely, for the least '' abnormal " patterns were found in babies dying after periods of severe hypoxia due to the respiratory distress syndrome. Two babies with long leaf-villi in the jejunum were stillborn; in these cases labour had pro- gressed normally until 2 hr and 1 hr before birth. It is unlikely that the villous pattern had radically altered in 2 hr.
The lack of any correlation between villous pattern and the length of time in the extra-uterine environment favours the suggestion that environmental factors have not played a major role in the determination of the villous pattern. Nor can the duodenal leaf-villi and ridges be attributed to damage from food, for these were present in most of the babies who had not ingested food. I t is possible that ingested amniotic fluid or gastric acid secretions had caused slight mucosal damage, but these cannot really be considered as environmental factors. The effects of these physiological, but potentially traumatic, fluids would be established by examination of the small intestine in a baby with duodenal atresia. None of the babies in the present series had this type of congenital abnormality.
It is difficult to explain the finding of finger-villi throughout the intestine of a full-term stillborn Indian infant (Baker et al., 1962). There may be racial differ- ences in villous development; all the babies in the present series were of British Caucasian parentage.
Tongue- and leaf-villi and ridges sometimes are caused by damage to the intestinal mucosa, for example, after gastric surgery (Booth et nl., 1962). Protection of the mucosa from the insult of bacterial contamination leads to the persistence of longer finger-villi in germ-free mice than in conventionally reared mice (Abrams, Bauer and Sprinz, 1963). Protection of the mucosa from mechanical insult, by the creation of a Thiry-Vella intestinal loop, maintains a " less abnormal '' villous pattern in the isolated segment (Chacko, Mathan and Baker, 1968). Such environmental factors may well be important in determining the small-intestinal villous pattern in older children and adults. However, it

FERGUSON, MAXWELL AND CARR
FORMS OF FOETAL SMALL-INTESTINAL VILLI
PLATE XXXVIII
FIG. 1 .-Low-magnification scanning electron micrograph of jejunal villi from an autolysed specimen showing preservation of the general surface features despite bending of some villi due perhaps to loss of bulk. Crypt mouths are seen between the bases of the villi. x c. 50.
FIG. 2.-Scaming electron micrograph of intestinal villi from an autolysed specimen showing two tongue-shaped villi (T) and two that, although twisted, approximate to finger-villi (F). Crypt mouths are seen between the villi. x c. 200.

FORMS OF FOETAL SMALL-INTESTINAL VILLI 91
would seem that the basic mucosal pattern changes throughout intra-uterine life. For the first 6 mth, finger-villi are present. In the next 2 mth, as the foetus enters the period of rapidly increasing size and weight, there is a gradual broadening of the villi until, at birth, there is a mixture of finger-, tongue- and leaf-villi.
SUMMARY In human infants, the small-intestinal villous pattern has been determined by
dissecting microscope examination of partly autolysed post-mortem material. The villous pattern has been examined in 11 stillborn infants and in 29 infants dying within 4 days of birth. In 29 of 36 duodenal specimens, the pattern was of broad-leaf villi and short ridges. The jejunal villous pattern was not related to the duration of extra-uterine life; there was a clear correlation between villous pattern and gestational age. Up to 26 wk after conception, mainly finger villi were present; from 26 to 34 wk after conception, there was a mixture of finger and tongue villi; at term, the pattern was of mixed finger, tongue and leaf villi.
The authors wish to express their thanks to Dr Scott of the Department of Pathology, Glasgow Royal Maternity Hospital, and Dr MacDonald of the University Department of Pathology, Royal Hospital for Sick Children, Glasgow, who supplied the specimens of small intestine and allowed the publication of clinical and autopsy findings. They are also grateful to Dr D. Murray for his help in interpretation of the dissecting microscope findings.
REFERENCES ABRAMS,G. D.,BAuER, H.,AND SPFUNZ,H. 1963. Lab. Invest., 12, 355. BAKER, S. J., IGNATIOUS, M., MATHAN, 1962. Ciba Fdn Study Grps, 14, 84.
V. I., VAISH, S. K., AND CHACKO, C. C. BOOTH, C. C., STEWART, J. S., HOLMES, R., 1962. Ibid., 14, 2.
CARR, KATHARINE E., AND TONER, P. G. 1968. Lancet, 2, 570. CHACKO, C. J. G., MATHAN, V. I., AND 1968. Br. J. Exp. Path., 49, 40.
LOEHRY, c. A., AND CREAMER, B. . . 1966. Br. Med. J., 1, 827. STANFIELD, J. P., HUTT, M. S. R., AND 1965. Lancet, 2, 519.
SWIFT, J. A., AND MARSH, M. N.. . . 1968. Ibid., 2, 915. TONER, P. G., AND CARR, KATHARINE E. VERZAR, F., AND MCDOUGALL, E. J.. . 1936. In Absorption from the intestine, London,
WALKER-SMITH, J. . . . . . . . 1967. Archs Dis. Childh., 42, 626.
AND BRACKENBURY, w.
BAKER, S. J.
TUNNICLIFFE, R.
1969. J. Puth., 97,611.
p. 53.

![Quantitative Assessment of Endoscopic Images for Degree of ......of villous atrophy classified using the scoring system for villous atrophy developed by Marsh [14] and modified by](https://img.pdfslide.net/doc/110x75/6052605b579c49341e0a18ad/quantitative-assessment-of-endoscopic-images-for-degree-of-of-villous-atrophy.jpg)
![Surgical Approach of Degenerated Giant Rectal Villous ......endoscopic resection of a circumferential lesion: is the occurrence of a stenosis [19]. The huge villous tumor constitutes](https://img.pdfslide.net/doc/110x75/60f7dd8ee931e11a5d1b5077/surgical-approach-of-degenerated-giant-rectal-villous-endoscopic-resection.jpg)