Embed Size (px)
Citation preview

Project Inform © 2005 1
Immune Pathogenesis
of HIV
Pathogenesis:The way that something causes disease.Immune pathogenesis is how the virus (HIV) interacts with the immune system, what happens to the immune system and how.
205 13th Street #2001San Francisco, CA 94103Website: http://www.projectinform.orgHotline: 415-558-9051 or 800-822-7422
Information, Inspiration and Advocacy for People Living with HIV/AIDS.
Project Inform

© Project Inform 2005 2
HIV Disease
Caused by Human Immunodeficiency Virus (HIV) Disables the immune system in many complex
ways HIV infects CD4+ (T4) and other immune cells CD4+ cells are important immune cells
Key ‘mediator’ of immune responses’ Communicating through chemicals (called ‘cytokines’)
CD4+ cells mediate humoral (antibody) and cellular immune responses

© Project Inform 2005 3
CD4+ Cells:Mediators of Immune Responses
BB B
B
B
B
T
T
T
T
T
ThymusT-cells (e.g. CD4+ and CD8+)
Bone MarrowB-cells CD4
Th0
CD4Th1
CD4Th2
IL-2IL-12INF-gamma
IL-4IL-6
IL-10
Humoral• B-Cells• Antibodies• Attacks “critters” outside of Cell
(e.g. free virus in blood)
Cellular• CD8+ cells, NK
cells• Cell to Cell killing• Attacks “critters”
inside of cells(e.g. HIV infected cells)

© Project Inform 2005 4
Infected CD4+ cells may die or become dysfunctional
HIV also infects other immune cells (e.g. antigen presenting cells)
Virus reproduces, infecting cells throughout the body Immune system is gradually weakened Body loses the ability to fight off infections
HIV Disease (continued)
IL-4IL-6IL-10
IL-2IL-12INF-g
Humoral Cellular
Antigen Presenting CellAntigen Presenting Cell(e.g. dendritic cell, macrophage)CD4+ T-CellCD4+ T-Cell

© Project Inform 2005 5
HIV Disease (continued)
Co-factors may further weaken the immune system Other sexually transmitted diseases and active infections
Active infection can increase HIV replication (HIV RNA increases 100 fold+)
StressChemicals released destroys (involutes) thymus and weaken cell walls
Poor nutritionEarly signs of nutritional deficienciesDeficiencies have similar symptoms as early signs of HIV disease
Lifestyle Factors (e.g. substance use, poor sleeping habits, etc.)
Acquired Immune Deficiency Syndrome (AIDS) is the advanced stage of HIV disease

© Project Inform 2005 6
CD4+ Cell Ranges
1500 and up
500
200100 50 0
NormalNormal RangeRange
PredictPredictiveive
RangeRange
LowestLowest RangeRange
Normal Range (500-1500+) Predictive Range (below 500)
Changes in CD4+ counts become ‘meaningful’ Data supports intervention (200 to 350)
Gray Zone For Therapy (350+) Guidelines suggest either Tx or no Tx
depending on HIV RNA & preference Limited data on use of Tx in this range
Lowest Range (below 200) Increased Risk for opportunistic infections
*Note: Trends are most important*Note: Number does not equal function

© Project Inform 2005 7
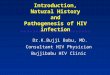
Immunopathogenesisof HIV Infection
Early
Intermediate
High Burst ofHigh Burst ofViral ActivityViral Activity
Development of Antibodies (seroconversion))
EarlyIntermediate
CD4+ > 500
CD4+ 200-500
AdvancedCD4+ <200
Onset of SymptomsOnset of SymptomsInfection with HIVInfection with HIV TIME
Viral ActivityCD4+ Count
Acute SyndromeAcute Syndrome

© Project Inform 2005 8
Immune Pathogenesis
Population-based information provides insights into disease, but each person experiences HIV disease uniquely

© Project Inform 2005 9
Early Infection/Acute Syndrome
Burst of viral replication Wide distribution of virus “Seeding” of virus in lymph tissue
Some believe that this early stage is very important and may determine the course of disease in each individual
Control of virus is probably not only due to immune response (cellular and humoral) but also to ‘sequestration’ of virus in lymph tissue
Early
High Burst ofHigh Burst ofViral ActivityViral Activity
Infection with HIVInfection with HIV
Development of Antibodies(seroconversion))

© Project Inform 2005 10
Early Intermediate (CD4+ >500)Clinical Latency?
EarlyIntermediate
CD4+ > 500
Virus is ‘trapped’ in follicular dendritic cells (FDC)
Dendritic cells act as a filter and central clearing house for ‘antigen presentation’ Unfortunately, HIV collects in large number
and use FDC as a ‘central’ infection center CD4+ cells, macrophages and monocytes
become infected when traveling through the lymph nodes
Virus levels in lymph tissue are generally much higher than what is seen in the blood/plasma

© Project Inform 2005 11
Follicular Dendritic Cells The “string mops” of the immune system, sweeping up ‘dirt’
that needs to be dealt with
“Critters” moving through lymph nodes and are ‘caught’ in FDC network
CD4+ and other cells also move through lymph nodes to see what kind of “critters” need to be dealt with

© Project Inform 2005 12
Intermediate (CD4+ 200-500)
IntermediateCD4+ 200-500
Structure and function of lymph nodes begin to degrade due to high level of viral activity
Beginning to lose follicular dendritic cells Are “strings” falling off the mop? Do FDCs become infected by HIV? Do FDCs die for unknown reasons?
Clinically: Minor problems begin to worsen (e.g. herpes, genital warts, thrush), blood tests begin to show abnormalities.

© Project Inform 2005 13
Lymph Node “Architecture”
Healthy lymph node:Healthy lymph node: Arranged like an egg FDC form the yolk in an intricate ‘network’ Network is like a cotton ball
Deteriorated lymph node:Deteriorated lymph node: FDC are scattered throughout Cotton ball network is ripped apart Decrease number of FDCs

© Project Inform 2005 14
Advanced DiseaseOnset of Severe Symptoms
AdvancedCD4+ <200
Onset of SymptomsOnset of Symptoms
Complete ‘burn out’ of lymph node centers? Some studies say no, even in advanced
disease. Much that is not wholly understood Loss or dysfunction of many cell types
CD4+ and CD8+ cells, FDC, B cells, macrophages, others
Virus levels similar in lymph node and blood/plasma
Possible changes in virus (M-tropic to T-tropic, syncitia inducing)
Immune system more resilient than we thought

© Project Inform 2005 15
Diversity of Immune Cells
Active vs. Resting cells HIV is a retrovirus, and can only reproduce from
activated (e.g. actively replicating) cells
T-cell receptor diversity V-beta repertoire (Variable region of the beta chain
of the T-cell receptor, immunologic alphabet)
Naïve vs. Memory Co-receptor expression (e.g. CKR5, CXCR4)

© Project Inform 2005 16
V-Beta RepertoireNaïve and Memory CellsP
A
W
C
P
B
W
C
H
M
Specificity of cell is dependent on the composition of the T-cell Receptor (TCR)
The greater the ‘repertoire’ of TCRs, larger the diversity of cells and function
“Naïve” cells are “rookies” in the immune system army
“Memory” cells are “veterans”, which respond more quickly and potently
P C M F H B P C M F H B

© Project Inform 2005 17
Co-receptors
CD4 receptorCKR5CXCR4Others...
Rantes, MIP1a, MIP1bSDF1, MDC
2 ‘receptors’ are necessary ‘doorways’ for HIV to infect a cell (CD4+ plus chemokine receptors)
Chemokines (chemicals produced by immune cells) block the doorways
Genetic alterations in receptors may inhibit HIV from using them to infect cells (CCR5 32bp-delta)
NSI virus uses R5; SI virus uses X4

© Project Inform 2005 18
Plasma HIV RNACD4+ T cell count
CD4+ cells in GALTViral Divergence from “founder strain”
Viral Diversity
CXCR4 or “X4” virus
Dual tropic – X4/R5 virus
Immune activation (esp CD8+ cell activation)
EmergingEmerging Information Information

© Project Inform 2005 19
Acute Infection/Early Disease (Emerging Information)
Within weeks of initial infection: ~75% depletion of “memory” CD4+ cell in gut Destruction of gut-associated lymphoid tissue
(GALT) “architecture” ~50% loss of total body “memory” CD4+ cells
Initial infection typically with CCR5 or “R5” type of virus
Virus closely resembles “founder strain” Virus population not diverse
Plasma HIV RNACD4+ T cell count
CD4+ cells in GALT Viral Divergence from “founder strain”
Viral DiversityImmune activation (esp CD8+ cell activation)

© Project Inform 2005 20
Early Intermediate and Intermediate(Emerging Information)
Rising levels of immune activation (not viral load) predicts rate of CD4+ cell loss
Continued destruction of GALT Increased divergence from initial
infecting strain Increased viral diversity (believed
to be due to escape from cellular immune responses)
Possible rise of dual tropic virus
Plasma HIV RNA
CD4+ T cell count
CD4+ cells in GALT
Viral Divergence from “founder strain”
Viral Diversity
CXCR4 or “X4” virus
Dual tropic – X4/R5 virusImmune activation (esp CD8+ cell activation)

© Project Inform 2005 21
Advanced Disease(Emerging Information)
High levels of immune activation increasingly believed to be responsible for immune deficiency/AIDS
Rise and disappearance of X4 virus (re-emergence of R5 virus?)
Decrease in viral diversity (possibly due to loss of CTL, no pressure on virus to “escape”)
Plasma HIV RNA
CD4+ T cell count
CD4+ cells in GALT
Viral Divergence from “founder strain”
Viral Diversity
CXCR4 or “X4” virus
Dual tropic – X4/R5 virusImmune activation (esp CD8+ cell activation)

Project Inform © 2005 22
Future Directions in AIDS Research
Project Inform

© Project Inform 2005 23
Immune Restoration: Rationale
AIDS is a disease of PRIMARY IMMUNE DEFICIENCY caused by a virus (HIV)
Anti-HIV Therapies alone do not appear to fully restore the immune system
Strategies that build on advances in anti-HIV therapy and enhance immune recovery and restoration are critical
Treatment for the major defect in HIV/AIDS, the primary immune deficiency/dysfunction

© Project Inform 2005 24
Immune Restoration:Areas of FocusEnvironmentEnvironment NumberNumber ProtectionProtection FunctionFunction
School
Virus
Cell
Bone Marrow
ThymusSpleenLymph tissue

Project Inform © 2005 25
Addendum Materials:Immune Pathogenesis of HIV
Project Inform

© Project Inform 2005 26
The Immune Response
B-cell
CD8+ T-cell
Antigen Presenting cells - Cells of the immune system that bring intruders to CD4+ T cells. (e.g. macrophages and dendritic cells )
CD4+ T-cells (also may be called “T4 helper cells”, “T4 cells”, or less accurately “T-cells”. CD4+ T cells mediate the immune system response.
CD4+T-cell
CD8+ T-cells - Some CD8+ T cells, when ordered by CD4+ cells will specifically seek out and destroy infected cells.
B cells - During an immune response B-cells make antibodies.
Antibodies - Antibodies are made by B-cells, they attach to “critters”, marking them for destruction by the immune system. Antibodies are specific to the “critter” (bacteria, virus, or other harmful toxins).

© Project Inform 2005 27
Immune Deficiency in HIV Disease Decreased number of lymphocytes
Initial decrease then stabilization of CD4+ cell number Increase in activated CD4+ Depletion of CD4+ naïve cells
Initial increase in CD8+ cell number Increase in activated CD8+ cells (CD8+CD38+/DR+) Despite increase CD8+ cell number, poor anti-HIV responses Decrease in CD8+ naïve cell parallels loss in CD4+
Impairment of Cell Function Decreased ability to produce cytokines, respond to antigens, loss
of TCR diversity & APC function, loss of B-cell function Increased risk of opportunistic infection
Impairment of Immune Environment Damage to immune tissues (LN architecture, FDC Network), status
of thymus Evidence of immune activation
Increased CD38+/DR+ expression, increased TNF-alpha