-
7/28/2019 Prolapse Lumbar Disc
1/40
1
-
7/28/2019 Prolapse Lumbar Disc
2/40
2
-
7/28/2019 Prolapse Lumbar Disc
3/40
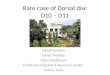
PROLAPSE LUMBAR DISC
- also known as slipped disc, spinal disc herniation,
orprolapsus disci intervertebralis
- a tear in the outer, fibrous ring of an intervertebral
disc allows the soft, central portion to bulge out
-
7/28/2019 Prolapse Lumbar Disc
4/40
-
7/28/2019 Prolapse Lumbar Disc
5/40
PATHOPHYSIOLOGY
Risk Factors:
1. Men
2. Increasing Age
3. Obesity
4. Degenerative Disorders
5. Trauma
6. Congenital Predisposition
Rupture ofAnnulus Pulposus(discs outer ring)
-
7/28/2019 Prolapse Lumbar Disc
6/40
PATHOPHYSIOLOGY
Protrusion of a portion of theNucleus pulposus
(soft, gelatinous inner part)
Pressure on spinal nerve roots
Signs and Symptoms
-
7/28/2019 Prolapse Lumbar Disc
7/40
SIGNS AND SYMPTOMS
Varies with the location and degree of herniation
and the course of its progression
Some are asymptomatic
-
7/28/2019 Prolapse Lumbar Disc
8/40
SIGNS AND SYMPTOMS
Back pain
- In lumbar herniation, often radiating down the
posterior thigh and leg, exacerbated by coughing,
sneezing, and straining
Motor and Sensory Impairment
- Muscle weakness, diminished deep tendon
reflexes in the lower extremitiespin and needle prick
sensation
-
7/28/2019 Prolapse Lumbar Disc
9/40
SIGNS AND SYMPTOMS
Nerve Root Pain (Sciatica)
- In lumbar disc herniation, pressure on the sciatic
nerve produces severe, sometimes debilitating
pain
- Pain may also be felt on the lower extremities
since the Sciatic nerve extends to the gluteal area,
going down the posterior leg.
-
7/28/2019 Prolapse Lumbar Disc
10/40
SIGNS AND SYMPTOMS
Cauda equina syndrome
- Rare but a medical emergency where the nerves
at the very bottom of the spinal cord are pressed
on
- Causes low back pain and disturbances in bowel
and bladder function
-
7/28/2019 Prolapse Lumbar Disc
11/40
DIAGNOSTIC STUDIES
Straight-leg raising test or the LeSegue test result
is positive.
CT, MRI, or Myelography may reveal the locationof
herniation.
-
7/28/2019 Prolapse Lumbar Disc
12/40
NURSING MANAGEMENT
Administer prescribed medications.
- May include muscle relaxants, narcotic or non-
narcotic analgesics
Provide on-going assessment.
- Assess the site, nature, course, and progress of
back pain
- Monitor motor and sensory status
-
7/28/2019 Prolapse Lumbar Disc
13/40
NURSING MANAGEMENT
Provide conservative management, if indicated.
- Encourage bed rest
- Position the patient with the head of bed
elevated at 30 degrees and knees slightly flexed- Apply heat
- Instruct in appropriate exercises to increase
muscle strength around the spinal cord (e.g. Pelvic
tilts, straight-leg raises)
-
7/28/2019 Prolapse Lumbar Disc
14/40
NURSING MANAGEMENT
- Keep the patient in proper body alignment when in
bed (provide firm mattress) and when turning
(use log-rolling technique)
- Teach proper body mechanics
-
7/28/2019 Prolapse Lumbar Disc
15/40
NURSING MANAGEMENT
Maximize functional abilities.
- Prevent complications of immobility
- Coordinate with a physiotherapist, chiropractor,
or osteopath for manipulation and other physicaltreatments
- Promote self-care
-
7/28/2019 Prolapse Lumbar Disc
16/40
NURSING MANAGEMENT
Provide preoperative and postoperative care if
Discectomy is ordered
Pre-operative Nursing Interventions:
a.1. Avoid taking aspirin or aspirin-containing products for 2
weeks prior to
surgery unless approved by physician
a.2. Discontinue nonsteroidal anti-
inflammatory medications 48 to 72 hoursbefore surgery
-
7/28/2019 Prolapse Lumbar Disc
17/40
NURSING MANAGEMENT
Provide preoperative and postoperative care if
Discectomy is ordered
Pre-operative Nursing Interventions:
a.3. Bring a list of current medications beingtaken
a.4. Wear loose clothing that can easily be
removed (e.g., avoid clothing that pulls on
and off over the head)
-
7/28/2019 Prolapse Lumbar Disc
18/40
NURSING MANAGEMENT
Provide preoperative and postoperative care if
Discectomy is ordered
Pre-operative Nursing Interventions:
a.5. Instruct the patient tobathe/shower/shampoo the evening
before
or morning of surgery. Men should be
cleanly shaved.
a.6. Instruct the patient on oral intakerestrictions and
medication schedule
as ordered
-
7/28/2019 Prolapse Lumbar Disc
19/40
NURSING MANAGEMENT
Provide preoperative and postoperative care if
Discectomy is ordered
Pre-operative Nursing Interventions:
a.7. Inform patient that before going to theoperating room he
will have to remove:
dentures, eye glasses, contact lenses,
appliances, prosthesis, make-up, nail polish,
hairpins, and undergarments
-
7/28/2019 Prolapse Lumbar Disc
20/40
NURSING MANAGEMENT
Provide preoperative and postoperative care if
Discectomy is ordered
Post-operative Nursing Interventions:
b.1. Monitor vital signs frequently b.2. Activity/diet
restrictions
b.3. Nursing personnel must assist with
initial ambulation
b.4. Medications available for pain andnausea upon request
-
7/28/2019 Prolapse Lumbar Disc
21/40
SURGICAL MANAGEMENT
The primary focus of surgery is to remove
pressure or reduce mechanical compression on
a neural element: either the spinal cord, or a
nerve root.
-
7/28/2019 Prolapse Lumbar Disc
22/40
SURGICAL MANAGEMENT
Foraminotomy
An incision is made in the back, the muscle peeled
away to reveal the bone underneath, and a small
hole cut into the vertebra itself. Through this hole,
using an arthroscope, the foramen can be
visualized, and the impinging bone or disk
material removed.
-
7/28/2019 Prolapse Lumbar Disc
23/40
SURGICAL MANAGEMENT
Discectomy
This is the surgical removal of herniated disc
material that presses on a nerve root or the spinal
cord.
The procedure involves removing the central
portion of an intervertebral disc, the nucleus
pulposus, which causes pain by stressing the
spinal cord or radiating nerves.
-
7/28/2019 Prolapse Lumbar Disc
24/40
-
7/28/2019 Prolapse Lumbar Disc
25/40
THE CASE
Patients Initials: AAAA
Age: 49 years old
Nationality: Indian
Consultant Surgeon: Dr. Khalid Saeed
Date of Admission: 8/6/2011
Diagnosis: Prolapsed Lumbar Disc L4-5 Right
-
7/28/2019 Prolapse Lumbar Disc
26/40
THE CASE
A 49 years old, Indian male was admitted in the
MDH Surgical Ward with a 3-month history of hip
pain radiating to the feet, occurring alternately
without numbness, paresthesia or motor power
disturbance. He sought conservative treatment in
the past but was unrelieved.
Non smoker, claims no allergies to food and
medications, and with no previously related
medical history.
-
7/28/2019 Prolapse Lumbar Disc
27/40
THE CASE
Vital signs upon admission:
Temp: 36.8C per orem
Pulse: 86 beats/min
RR: 22 breaths/min
SPO2: 100 %
Bp: 110/70 mmHg
General Appearance:
- Appears thin and not in distress, ambulatory
-
7/28/2019 Prolapse Lumbar Disc
28/40
THE CASE
Physical Examination:
Head: No significant findings
Chest: Clear breath sounds
Heart: no murmur noted (S1 + S2 + 0)
Abdomen: soft, non tender
Extremeties: No significant findings
Nervous system: GCS = 15, verbally responsive,
conscious and coherent
-
7/28/2019 Prolapse Lumbar Disc
29/40
THE CASE
Routine and Diagnostic Investigations:
Hgb 14.2
Serum Electrolytes within normal limits
BUN within normal limits
Hepatitis Profile no significant findings
BT within normal limits
RBS within normal limits
Serum Creatinine within normal limits
-
7/28/2019 Prolapse Lumbar Disc
30/40
THE CASE
Routine and Diagnostic Investigations:
Urinalysis within normal limits
PT and INR within normal limits
Chest X-ray no significant findings
ECG no significant findings
MRI Disc dehydration and
minor posterior disc bulge
and annular tear at L5/S1
but no significant foramen
or canal narrowing
-
7/28/2019 Prolapse Lumbar Disc
31/40
THE CASE
Course in the Surgical Ward:
June 8, 2011
Patient was kept on bed rest. Normal diet wasgiven. Vital signs
were taken. All Pre-operative
investigations were done. He was started on
antibiotics and pain relievers and was posted for
Discectomy on 9/6/2011.
-
7/28/2019 Prolapse Lumbar Disc
32/40
THE CASE
Course in the Surgical Ward:
June 9, 2011
Patient was shifted to Operating Theater at0900H. At 1300H,
patient was received from the
recovery room, status post Fenestration and
Discectomy L4-5 with Foraminotomy. He had IVF
of DNS 500 cc to run for 6 hours, with Porto-Vacdrain, and
Foleys catheter connected to urobag.
-
7/28/2019 Prolapse Lumbar Disc
33/40
THE CASE
Course in the Surgical Ward:
June 9, 2011
He was placed on hard mattress, on complete bedrest. Vital
signs, intake and output were
monitored. On antibiotics of Cefizox 1 gm 1 vial IV
BID, and Tavanic 500 mg 1 vial IV OD, with pain
reliever Tramal 50 mg 1 amp IM BID, and Olfen 75mg 1 amp IM BID.
At 2100H, he was placed on
liquid diet as tolerated.
-
7/28/2019 Prolapse Lumbar Disc
34/40
THE CASE
Course in the Surgical Ward:
June 10, 2011 (1st POD)
Dressing was mildly soakedPVAC drained to 30 cc, blood
stained
FC 900 cc clear
Vital Signs are stable, not in distress
-
7/28/2019 Prolapse Lumbar Disc
35/40
THE CASE
Course in the Surgical Ward:
June 11, 2011 (2nd POD)
Started ambulation exercisesSurgical dressing was changed, Wound
appears
clean
FC was removed
PVAC drained to 7 cc, serous
Vital Signs are stable, not in distress
Started with normal diet and oral medicines
-
7/28/2019 Prolapse Lumbar Disc
36/40
THE CASE
Course in the Surgical Ward:
June 12, 2011 (3rd POD)
Ambulation was well-tolerated(+) non productive cough noted
Surgical dressing was changed, Wound appears
dry and clean
PVAC drained to 10 cc, serous
Vital Signs are stable, not in distress
-
7/28/2019 Prolapse Lumbar Disc
37/40
THE CASE
Course in the Surgical Ward:
June 13,2011 (4th POD)
Vital Signs are stable, not in distressPVAC was removed
June 14, 2011 (5th POD)
Vital Signs are stable, not in distress
Defecated
-
7/28/2019 Prolapse Lumbar Disc
38/40
THE CASE
Course in the Surgical Ward:
June 15, 2011 (6th POD)
No pain as verbalizedAmbulated
Wound is clean and dry
For discharge
-
7/28/2019 Prolapse Lumbar Disc
39/40
THE CASE
Discharge Orders:
Celebrex 1 tab BID for 15 days
Sirdalud 2 mg 1 tab BID for 15 daysDorofen cap 1 tab TID for 30
days
Osteocare 1 tab BID for 30 days
Tavanic 500mg 1 tab OD for 5 days
Sickleave for 6 weeks
Follow up after 1 week
-
7/28/2019 Prolapse Lumbar Disc
40/40
40