Embed Size (px)
Citation preview

103
Promising Practices to Improve Immigrants’ Health and Well-Being
Health is a cornerstone of immigrant integration as much as educationand learning English. If a family has health insurance for their
children, then those children are in school learning and not home sick.Their parents don’t have to miss work as often and can stabilize their family financially. Medical bills are the number-one cause for bankruptcy,so this is also about protecting the family against the financial difficultythat comes along with being uninsured.”
—Laura Hogan, Program Director, Access to Health Services The California Endowment
INTRODUCTION 105
BARRIERS TO HEALTH AND WELL-BEING 106
STATE-FUNDED INSURANCE PROGRAMS 107Securing State-Funded ServicesRestoring Health Insurance for Low-Income ImmigrantsPromoting Coverage for All Children
OUTREACH AND EDUCATION PROGRAMS 113Elements of Promising PracticesMultimedia Health Outreach CampaignIncreasing Enrollment in Public Health Insurance ProgramsIncreasing Access to Reproductive Health CareProviding Accurate Health Information
LANGUAGE ACCESS AND CULTURAL COMPETENCE 118Elements of Promising PracticesHealth Interpretation Services in Rural AreasEffective Health Interpretation SystemsIncreasing Workforce DiversityResponding to Demographic Change, Driven by Community Need
EVALUATION 124
“
104
105
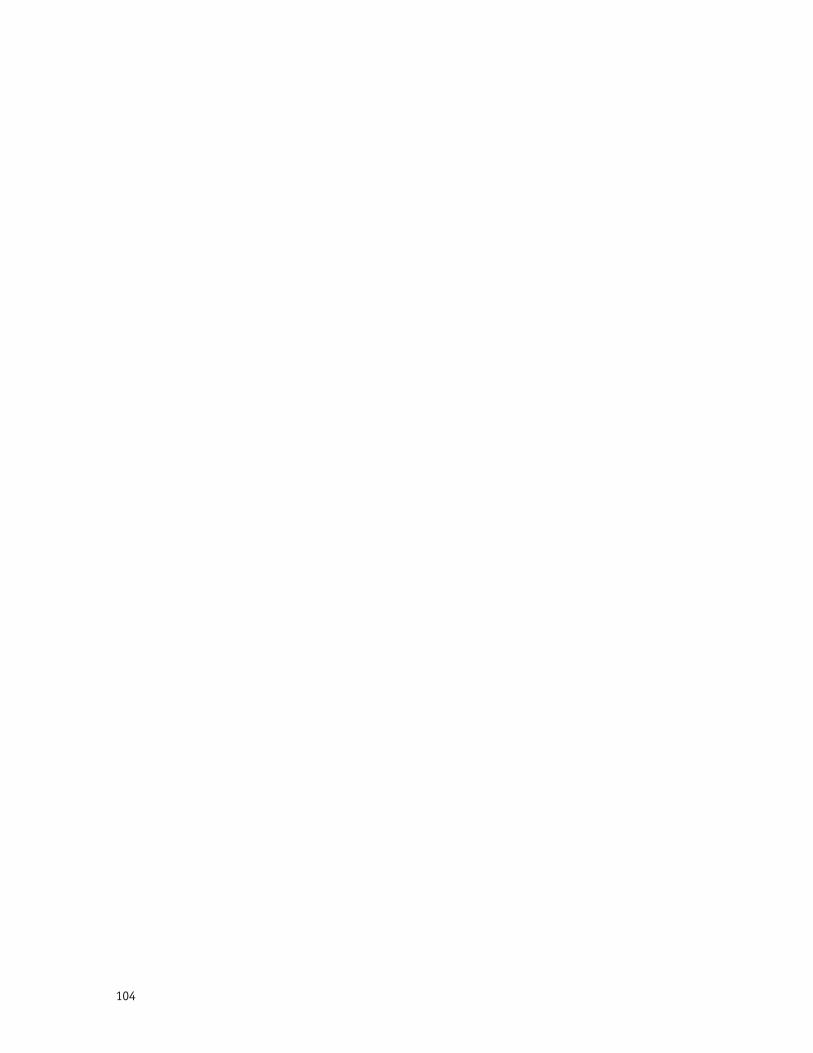
When immigrants arrive in the UnitedStates, they are generally healthier
than native-born residents. However, overtime, their healthconditions convergewith those of thegeneral population.Acculturation toAmerican lifestylesand dietary habitsmay account for part of this change, butimmigrants also face a number of barriersto maintaining good health. As a group,they are much less likely than citizens tohave health insurance, resulting in lessaccess to preventive services, fewer regu-lar check-ups, and ultimately poorerhealth outcomes.1 Even when newcomersare eligible for health insurance, they
often face a variety of language, cultural,and immigration-related barriers thatlimit their access to quality care.
Foundations can support programs thatexpand both eligibility and access, as wellas reduce barriers to health care for new-comers, including:
• Policy and advocacy projects toexpand health insurance coverage forimmigrants and their children.
• Outreach and informational cam-paigns to educate immigrants about theU.S. health care system, their eligibilityfor health care services, and healthybehaviors.
• Efforts to deliver health services toimmigrants in a linguistically and cultur-ally competent manner.
By supporting these strategies, founda-tions will promote good health for immi-grant families and enable newcomers tocontribute to the overall well-being of thebroader community.
INTRODUCTION
© T
ony
Arm
our
Phot
ogra
phy
, In
c.
1. Grantmakers In Health. 2005. For the Benefit of All: Ensuring Immigrant Health and Well-Being.Washington, D.C.: Grantmakers In Health. Availableat www.gih.org.
Maintaining good health is a critical elementof immigrant integration. It is fundamental tonewcomers’ ability to find and keep jobs, learnEnglish, and contribute to the vitality of theirnew communities.

106
This section provides a brief overviewof the health care barriers faced bymany newcomers, as well as promisingpractices to overcome these challenges.
LOWER RATES OF HEALTH INSURANCE
Immigrant families are much less likelythan citizens to have health insurancefor a number of reasons:
• Less coverage from employers.While over 80 percent of immigrantshave families that include at least onefull-time worker, a disproportionatenumber is employed by small firms orlow-wage sectors which are less likelyto offer health benefits.
• Ineligibility for federal healthinsurance programs. The 1996 federalwelfare and immigration laws bar mostlegal immigrants from Medicaid andthe State Children’s Health InsuranceProgram (SCHIP) in their first five yearsin the United States. (The few excep-tions to this bar include refugees andpolitical asylees). After five years, mostremain ineligible due to “sponsordeeming,” which adds the income ofthe person who sponsored the immi-grant to that of the immigrant in determining eligibility.
• Very limited access to publichealth insurance for undocumentedimmigrants. Although some stateshave begun to offer prenatal care andchildren’s coverage to this population,federal and state laws generally barundocumented residents fromMedicaid and other programs exceptfor emergency care.2
• Unfamiliarity with public healthinsurance programs. This unfamiliarityresults in low rates of participation evenamong those eligible, particularly thecitizen or legal-resident children ofimmigrants.3
For immigrants, this low rate of cover-age means that they are less likely tohave a usual source of care, have vis-ited a doctor during the previous year,or receive immunizations and other
preventive services.4 Although few studieshave examined the long-term effects ofbeing uninsured among immigrant popu-lations, research on Latinos participatingin SCHIP and Medicaid consistently findsthat enrollment, even for short periods oftime, leads to better health outcomes.5
ACCESS BARRIERS TO HEALTH SERVICES
While providing health insurance is thefirst step to improving immigrants’ health,the availability of insurance coverage, by itself, does not automatically lead togreater utilization of health services.Newcomers also face access barriers relatedspecifically to their status as immigrantsor their limited English proficiency. These include:
• Confusion about program eligibilityand how to use the U.S. health caresystem. Health systems in immigrants'home countries often differ significantlyfrom the U.S system. Different eligibilityrequirements for various federal and statehealth programs add to the confusion,particularly in mixed-status families, inwhich some members may be eligible forcoverage and others may not, dependingon their immigration or citizenship status.
• Fears about consequences forimmigration status. Many immigrantsare reluctant to use any publicly fundedhealth programs because they are afraidof adverse immigration consequenceseven though most of their concerns areunfounded. Common fears include:
• Being labeled a “public charge,”which can result in difficulties obtain-ing permanent residency (“green card”),re-entering the country, or sponsoringa relative. This concern deters manyfrom seeking care, despite the fact thatreceipt of non-cash benefits, such asMedicaid and other publicly fundedhealth programs, are not a factor inpublic charge.6
• Making an immigrant’s sponsorfinancially liable for the immigrant’s useof public health programs. No state hasprioritized seeking reimbursement fromsponsors in these situations.7
• Providing sensitive informationabout family members that could leadto deportation or other negative immi-gration consequences. The verificationand reporting requirements in somestates’ application processes raiseconcerns that confidential informa-tion will be shared with immigrationenforcement officials.
• Language and cultural barriers.Approximately half of all foreign-bornadults in the United States speakEnglish with some limitations,8 andmany come from cultures that havevery different attitudes toward illnessesand medicine. These differences cancreate barriers to applying for healthcoverage and communicating withhealth care providers.9
BARRIERS TO HEALTH AND WELL-BEING
2. For details on health programs for whichundocumented immigrants qualify, see NationalImmigration Law Center. 2004. Guide toImmigrant Eligibility for Federal Programs. LosAngeles, CA: National Immigration Law Center.Available at www.nilc.org.3. Staudt, Kathleen and Randy Capps. 2004.“Con la ayuda de Dios? El Pasoans at theBorder.” In Philip Kretsedemas and Ana Aparicio,eds. Immigrants, Welfare Reform, and the Povertyof Policy. Westport, CT: Praeger.4. Fremstad, Shawn and Laura Cox. 2004.Covering New Americans: A Review of Federaland State Policies Related to Immigrants’Eligibility and Access to Publicly Funded HealthInsurance. Washington, D.C.: Henry J. KaiserFamily Foundation.5. Shone, Laura, Andrew Dick, Jonathan Klein,Jack Zwanziger, and Peter Szilagyi. 2005.“Reduction in Racial and Ethnic Disparities AfterEnrollment in the State’s Children’s HealthInsurance Program.” Pediatrics 115(6): 697-705;Ku, Leighton. 2005. Medicaid: Improving Health,Saving Lives. Washington, D.C.: Center onBudget and Policy Priorities.6. Fremstad and Cox, 2004.7. National Immigration Law Center. 2005.Overview of Immigrant Eligibility for FederalPrograms. Los Angeles, CA: National ImmigrationLaw Center. Available at www.nilc.org.8. Capps, Randolph, Michael Fix, Jeffrey Passel,Jason Ost, and Dan Perez-Lopez. 2003. A Profileof the Low-Wage Immigrant Workforce.Washington, D.C.: Urban Institute.9. A more detailed overview of the impact ofthese barriers, related language access legalrequirements, and strategies for overcomingthese barriers can be found in the “PromisingPractices in Language Access” section.
107
Recognizing that a growing uninsuredpopulation undermines public health,
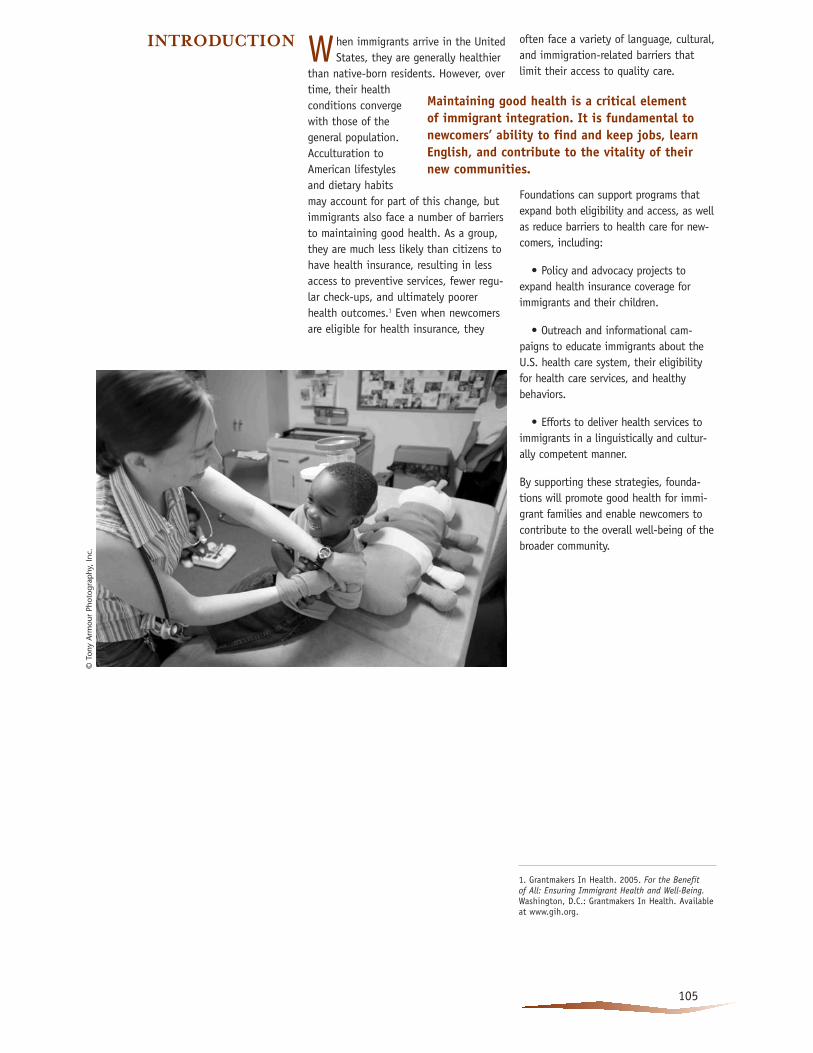
stretches already scarce emergency roomservices, and increases health care costsfor everyone, a number of states areusing their own funds to offer healthinsurance to low-income immigrantswho are ineligible for Medicaid or SCHIP.As of 2004, 22 states and the District ofColumbia were using state funds to pro-vide health coverage to some or all ofthese immigrants (See Figure 1). Almostall of these state programs provide coverage to immigrants with legal status, including low-income immigrantchildren and pregnant women, andabout two-thirds cover seniors, peoplewith disabilities, and the parents ofimmigrant children. Seven states usefederal SCHIP funds to cover prenatalcare for all women, regardless of immigration status.
Foundation-supported policy advocacyhas been critical to the developmentand preservation of these programs,especially in the states where the pro-grams have come under attack fromanti-immigrant forces or from state law-makers facing a budgetary crisis.10 Whileall of the traditional immigrant gatewaystates have enacted various state-funded health programs for immigrants,relatively few states in the South andMidwest have done so, creating oppor-tunities for foundations to support pol-icy advocacy efforts in these new gate-way states.
Supported by both foundation and gov-ernment funding, universal health insur-ance programs for children have greatlyexpanded over the past five years. As ofearly 2006, New York, Washington, D.C.,Massachusetts, Rhode Island, WashingtonState, Illinois, and a growing number ofcounties in California offer programsthat cover children without regard tocitizenship or immigration status.
STATE-FUNDED INSURANCEPROGRAMS
Figure 1: State-Funded Health Coverage for Immigrants Ineligible for Medicaid or SCHIP, May 2004
SOURCE:
Fremstad, Shawn and Laura Cox. 2004. Covering New Americans: A Review of Federal and State PoliciesRelated to Immigrants’ Eligibility and Access to Publicly Funded Health Insurance. Washington, D.C.: Henry J. Kaiser Family Foundation.
� 22 states providestate-funded coverage
� 28 states do not provide state-fundedcoverage
© Ju
pite
r Im
ages
108
SECURING STATE-FUNDEDSERVICES
California Immigrant WelfareCollaborative Los Angeles, Californiawww.caimmigrant.org
The work of the California ImmigrantWelfare Collaborative (CIWC), a partner-ship among four organizations, hasmade California a model for providinghealth and social service programs forlow-income immigrants. The 1996 fed-eral welfare and immigration lawsrestricting newcomers’ access to publichealth and social service programs had aparticularly harsh impact on California.While an estimated 40 percent of theimmigrants affected by the new restric-tions resided in the state, no singleorganization had the capacity to developa statewide response. Funding from TheCalifornia Endowment, The CaliforniaWellness Foundation, the Ford Foundation,and the David and Lucille Packard
Foundation made it possible for a coregroup of legal and community-basedorganizations (Asian Pacific AmericanLegal Center, Coalition for HumaneImmigrant Rights of Los Angeles (CHIRLA),National Immigration Law Center, and Northern California Coalition forImmigrant Rights) to form CIWC.11 In itsfirst years, CIWC documented the harm-ful effects of these federal restrictionsand developed into a statewide networkthat successfully advocated for the con-tinued provision of public health careand social services to immigrants.
Over the course of several years, CIWCplayed a pivotal role in securing whatthe Urban Institute has described asone of the most “generous” and “com-prehensive” state-funded safety nets forimmigrants who lost eligibility for fed-eral programs.12 With state funding,California’s Medicaid and SCHIP pro-grams have remained available to allimmigrants who would have been eligi-ble prior to 1996. In addition, the state
created new food and cash assistanceprograms for immigrants who lost eligi-bility for federal Food Stamps andSupplemental Security Income (SSI), aswell as a state-only cash assistance pro-gram for legal immigrants who becameineligible for federal TemporaryAssistance for Needy Families (TANF).CIWC also helped preserve prenatal carefor low-income women regardless ofimmigration status.
CIWC’s success is especially striking inthat it came shortly after the passage ofthe anti-immigrant state ballot measureProposition 187,13 which proposed torestrict immigrants’ access to educationand public benefit programs. However,rather than allowing Proposition 187and federal welfare laws to paralyzeimmigrant communities, CIWC and otheradvocates used these harsh measures tobuild and mobilize support for newcom-ers. A key strategy was to increase thevisibility and involvement of affectedcommunities in policymaking. Severalfactors contributed to CIWC’s success:
• Rapid response and multi-yearsupport by funders. Early recognitionby funders of the developing crisis cre-ated by the 1996 laws made it possiblefor CIWC to launch a rapid, large-scaleresponse. And multi-year foundationsupport gave CIWC the opportunity toadvocate for incremental expansions ofreplacement programs that, over time,came to cover most immigrants who wereno longer eligible for federal programs.
• Combining policy analysis withcommunity-based advocacy. CIWC hasbeen effective because its membershave diverse and complementary skills,include broad-based immigrant rights
Tena
nts
and
Wor
kers
Uni
ted,
© R
ick
Rein
hard
11. The current organizational members of CIWChave changed slightly with Services ImmigrantRights and Education Network (SIREN) joining inthe early 2000s after the Northern CaliforniaCoalition for Immigrant Rights discontinued opera-tions.12. Zimmerman, Wendy and Karen Tumlin. 1999.Patchwork Policies: State Assistance for Immigrantsunder Welfare Reform. Washington, D.C.: UrbanInstitute. 13. Proposition 187 was an initiative approved byCalifornia voters in 1994 that, among other things,prohibited undocumented immigrants from attend-ing public schools and limited their access to pub-lic benefits programs. Proposition 187 never tookeffect; it was immediately enjoined by a federalcourt, which eventually ruled that the measure violated the U.S. Constitution.
109
© D
avid
Bac
on
coalitions in Northern and SouthernCalifornia, and have access to a widerange of institutions and communitiesthat can mobilize public support.
• Extensive outreach to affectedpopulations. In its first three years,CIWC project staff traveled throughoutthe state and provided training on leg-islative changes to over 1,000 commu-nity organizations, ranging from largeservice providers to small, emergingimmigrant groups. Staff also conductedworkshops and presentations to morethan 10,000 immigrants, where they botheducated community members and broughtthem into the policymaking process.
• Empowering community groupsand immigrant leaders to participatein policymaking. This began in 1997with an annual “Immigrant Day” thatbrought up to 1,000 people to the statecapital to share their concerns directlywith policymakers. “The large size ofthese initial events,” recalls Susan Drake,then executive director of the NationalImmigration Law Center, “made a deepimpression on policymakers, as manywere only beginning to recognize thatnewcomers were a growing part of theirconstituencies.”
These activities, combined with growingrepresentation of minority communitiesin the state legislature, created oppor-tunities to build long-lasting support forincreasing immigrants’ access to publichealth and economic security programs.
Ten years after its inception, CIWC continues to protect access and servicesfor immigrants. With its extensive net-work and policy advocacy experience,CIWC emerged as the leading pro-immigrant voice in the state capital.
RESTORING HEALTH INSURANCE FOR LOW-INCOME IMMIGRANTS
Children’s AllianceSeattle, Washingtonwww.childrensalliance.org
In 2002, the Washington State legisla-ture responded to a budgetary crisis bycutting some of its health care programs,including eliminating three insuranceprograms for low-income individualswhose immigration status made themineligible for Medicaid. These cutsaffected over 28,000 people, 90 percentof them children. While individuals wholost coverage were eligible for the state’sBasic Health program, less than halfenrolled because the program requiredmonthly premiums and significant co-pays, offered fewer medical services, andprovided few language access services.14
Although the cuts initially caught healthadvocates by surprise, they quicklydeveloped a campaign to restore cover-age for tens of thousands of children.Recognizing that Washington State hastraditionally been a leader in expandingpublic health insurance coverage and
that the public was generally supportiveof providing children with health services,Children’s Alliance and other advocacygroups developed a multi-year campaignto restore the cuts through the followingstrategies:
• Developing a broad coalition oforganizations and institutions thatsupported restoring health insurance forimmigrants, including local governments,community-based organizations, clinics,hospitals, and private businesses.
• Working with health providers toidentify individual stories that put ahuman face to the cuts. These storiesincluded children who were no longerable to receive preventive care or couldnot afford needed medical procedures.
• Providing legislators and govern-ment officials with analysis of thecuts’ impact. Children’s Alliance beganpublishing policy bulletins immediatelyafter the cuts took effect, showing highnumbers of children losing coverage. Italso worked with researchers on a report(supported by the Henry J. Kaiser FamilyFoundation) that provided detailedanalysis of the cuts’ harmful effects andtrue costs.15 The report showed that the“cuts” actually resulted in substantialcost shifting to county public healthagencies and local clinics.
• Developing public messages thatpromoted coverage for immigrantchildren as part of an overall campaignto increase health care coverage forall children. Children’s Alliance foundthat its message resonated better withpolicymakers and the public as part ofan effort to help all children, includingU.S. citizens, who were losing healthinsurance because of recent budget cuts.
As a result of this campaign, the legis-lature and the governor restored thepreviously cut health insurance cover-age for all children, including programsfor immigrant children, regardless ofimmigration status. Research and advo-cacy played a key role in convincing
14. Gardner, Mark and Janet Varon. 2004. MovingImmigrants from a Medicaid Look-Alike Program toBasic Health Insurance in Washington State: EarlyObservations. Washington, D.C.: Henry J. KaiserFamily Foundation.15. Ibid.

110
policymakers to reverse these cuts. AsLiz Arjun of Children’s Alliance observes,“They may have initially thought theircuts would have minimal effect. Butwhen we showed them that tens ofthousands of children were no longerreceiving regular medical care and thecost savings were minimal, they realizedthat taking health insurance away fromimmigrant children and children in gen-eral was a bad decision.”
PROMOTING COVERAGE FOR ALL CHILDREN
County and Statewide Approaches in Californiawww.insureallkids.org
In 2000, government and communityleaders in California’s Santa ClaraCounty came together to determine thebest way to allocate new monies thatwould be arriving from the TobaccoSettlement Fund. After considering vari-ous options, they identified a key prior-ity: to make fundamental changes inthe fragmented and confusing systemthat prevented many eligible childrenfrom enrolling in publicly funded healthinsurance programs.
The system was especially difficult forimmigrant families, the majority ofwhich have mixed immigration status.Depending on the children’s citizenshipor immigration status, an immigrantfamily could have one child eligible forMedicaid, one child eligible for theState Child Health Insurance Program(SCHIP), and one child eligible for nopublicly funded health coverage at all.
It became clear to these leaders thatthe County needed to create a moreefficient, better coordinated system toincrease both coverage and enrollmentof qualified children. After more than ayear of planning, the Children’s HealthInitiative (CHI) was launched in 2001.CHI has three components: (1) healthcoverage for all children in Santa ClaraCounty whose family income was under300 percent of the federal poverty leveland who were not currently eligible forexisting Medicaid or SCHIP coverage; (2)expanded and coordinated outreach toincrease enrollment; and (3) significantstreamlining of enrollment processesacross multiple public programs.
“What people inside the health systemsaw was that a lot of children who wereeligible for programs were not enrollingbecause the system was so tough tonavigate. They felt they had a responsi-bility to simplify the system and createan enrollment program that would reallywork,” says Laura Hogan, director ofAccess to Health Services at The CaliforniaEndowment. In December 2005, TheCalifornia Endowment awarded $7.5 million in grants to local Children’sHealth Initiatives in counties through-out California as part of its ongoingsupport of such efforts.
The initial idea in Santa Clara Countyoriginated at the grassroots. Two localadvocacy groups—Working PartnershipsUSA, a labor-based research group, and the faith-based People Acting inCommunities Together (PACT)—knew
that the tobacco money would be coming in and quickly drew up a plan to provide health coverage to childrenwhose family income and immigrationstatus left them uninsured.
Although Medicaid and SCHIP coverchildren under 250 percent of the fed-eral poverty level, there was nothing forchildren in families who earned morethan that threshold yet too little toafford private health insurance. Ineligiblefor any publicly funded health coverage,undocumented children also fell throughthe cracks.
To implement the program, WorkingPartnerships USA and PACT partneredwith the County Health Department, the First Five Commission, the SocialServices Agency, the Santa Clara HealthPlan, and officials at both the countyand city levels. From the very begin-ning, the Children’s Health Initiative inSanta Clara has been a partnershipbetween the private and the public sec-tors. While the proportion varies fromcounty to county, all counties with aChildren’s Health Initiative are public-private partnerships, supported by pub-lic funds as well as foundation grantsand other private donations.
“In just about every county, it’s been acooperative and collaborative effort on thepart of a lot of different sectors, andthat’s what makes it so powerful,” notesRebecca Stark, program coordinator at PICOCalifornia, which is working to promotestatewide health coverage for children.©
Juan
Mira
nda
© Ju
pite
r Im
ages
In polling, we’ve discovered that
people understand that health
coverage for all children is both the
right thing to do and the smart thing
to do.”
—Laura Hogan, Program Director,The California Endowment
“
111
Under the CHI guidelines, all children up to the 300 percent of the federalpoverty level are guaranteed health coverage, meaning that in 2006, ahousehold of four can earn up to$60,000 and still qualify. CHI, unlikethe state’s Medicaid and SCHIP pro-grams, also covers undocumented chil-dren. “It’s a program for all kids, soimmigration status doesn’t become anissue,” says Linda Baker, program officerat the David and Lucile PackardFoundation.
The Children’s Health Initiatives thatmany California counties have adoptedalso streamline a daunting applicationprocess. Under such programs, allincome-eligible families, even thosethat include children in mixed-statusfamilies, fill out a single applicationwith the assurance that all of their children will be enrolled in a health care program. Moreover, children in onefamily are able to see the same providersregardless of the program in which theyare enrolled.
“When Santa Clara gave families a simplemessage that they could enroll in oneplace with one application, families didcome in and enroll,” Hogan says.
This strategy eliminated the confusionand intimidation that prevented manyfamilies from applying in the first place,significantly increasing enrollment in allthree public health insurance programs.In its first two years alone, Santa Clara’sChildren’s Health Initiative increasedenrollment in Medicaid and SCHIP in thecounty by 28 percent.
Santa Clara County’s success helped spurthe creation of similar programs in 17other counties, including, significantly,Los Angeles County which started aninitiative in 2003 and already hasenrolled 43,000 children. In all, theseinitiatives have provided coverage tomore than 80,000 children in California
and assisted in enrolling another 80,000in Medicaid and SCHIP. As of 2005, 90percent of all children in California wereinsured, either through public or privateinsurance programs. In pioneering SantaClara County, this statistic reached animpressive 98 percent.
Planning of similar initiatives in a numberof other counties is underway. “Themost important thing for a county to dowhen starting an initiative is to buildthe right coalition of people, and it hasto be a broad coalition that includesbusiness, teachers, health providers, andothers,” advises Hogan. “You have tohave champions who really want toachieve this goal and believe in what’shappening.”
Hogan further explains, “In polling,we’ve discovered that people understandthat health coverage for all children isboth the right thing to do and thesmart thing to do. Issues related toimmigration status do not weigh heavily
in the public’s mind when consideringthe benefit of this policy change. Thefeeling is that they didn’t come here oftheir own choosing, they are in societynow, and they are here to stay.”
In addition to addressing ethical and societal responsibility, having aChildren’s Health Initiative providespractical economic benefits.
“Investing in insurance for children,especially undocumented children, pro-vides them with greatly improved accessto care. And, the fact that CHI bringsinsurance to nearly all children pullsinto the system many children who havebeen eligible for insurance but were notpreviously enrolled. This is smart fiscalpolicy,” Baker says. She also notes thatin 2001 and 2002, the evaluation of theSanta Clara initiative showed that the28 percent increase in enrollment in thestate’s Medicaid and SCHIP programs hasbrought nearly $25 million in federaland state dollars into the county, whichlocal officials appreciate and need.
Although the initiatives vary slightlyfrom county to county, they remainlargely similar for pragmatic and long-term fiscal reasons. But their compre-hensive approach to coverage—and thehigh level of demand for coverage—means that the initiatives cannot besustained in the long term by local dol-lars alone. Funding, especially for smallrural counties, is a major challenge.
© Ju
pite
r Im
ages
When Santa Clara gave families
a simple message that they
could enroll in one place with one
application, families did come in and
enroll.”
—Laura Hogan, Program DirectorThe California Endowment
It’s a program for all kids, so
immigration status doesn’t
become an issue.”
—Linda Baker, Program OfficerDavid and Lucile Packard
Foundation
“
“
112
policy,” Baker says. She also notes thatin 2001 and 2002, the evaluation of theSanta Clara initiative showed that the28 percent increase in enrollment in thestate’s Medicaid and SCHIP programshas brought nearly $25 million in fed-eral and state dollars into the county,which local officials appreciate and need.
Although the initiatives vary slightlyfrom county to county, they remainlargely similar for pragmatic and long-term fiscal reasons. But their compre-hensive approach to coverage—and thehigh level of demand for coverage—means that the initiatives cannot besustained in the long term by local dol-lars alone. Funding, especially for smallrural counties, is a major challenge.
“Each county has used a different strat-egy for funding,” Baker explains. “Theyall use First Five, tobacco settlementmoney, county general funds, privatedonations, and foundation dollars, butat this point, the demand for services isso high that waiting lists are forming,and fundraising has become a chal-lenge. It’s not easy.”
The hope, says Baker, is that eventuallyall the programs in each county canbecome one statewide initiative.
A coordinated advocacy effort is under-way to make this hope a reality. Thiseffort is led by PICO California and the100% Campaign, which is a coalition ofthree children’s advocacy organizations:Children Now, The Children’s Partnership,and Children’s Defense Fund.
Two strategies are simultaneously inplay: working through the budget andlegislative process in the CaliforniaGeneral Assembly and passing astatewide tobacco-tax ballot initiative.If either the legislation or the initiativewere to pass, statewide universal healthinsurance for low-income children wouldbecome a reality. California would joinsix other states in the country thatoffer such coverage.
Supporters of universal health coveragefor children in California continue theirefforts to win public support for theballot initiative and the bill under con-sideration in the General Assembly,while also advocating for state fundingfor county-level initiatives. This multi-strategy approach is particularly impor-tant because several counties havestarted to freeze their Children’s HealthInitiative enrollment due to insufficientfunding.
With the number of uninsured and thecost of health care skyrocketing, afford-able health coverage is vital to thewell-being of low-income families.Hogan sums it up this way, “Health is a cornerstone of immigrant integrationas much as education and learningEnglish. If a family has health insurancefor their children, then those childrenare in school learning and not homesick. Their parents don’t have to misswork as often and can stabilize theirfamily financially. Medical bills are thenumber-one cause for bankruptcy, sothis is also about protecting the familyagainst the financial difficulty thatcomes along with being uninsured.”
Watch the DVDCalifornia Healthy Kids
Most of us agree that all children,regardless of their immigration status,deserve to be healthy. Be inspired byan energetic and wide cross-section ofgrassroots and grass-tops stakeholders
as they raise the long-term implications—and the short-term
urgency—of universal healthcare for every child.
© T
ony
Arm
our
Phot
ogra
phy
, In
c.
In 2006, Illinois became the
first state in the nation to
provide universal health coverage
for all children through age 18, with
graduated premiums based on family
income. The All Kids program,
effective July 1, 2006, provides
coverage for preventive care, dental
and vision services, hospital costs,
and prescription medicine.

113
© Ju
pite
r Im
ages
Helping immigrants become more famil-iar with the U.S. health care system andthe services for which they are eligibleis an important first step toward self-sufficiency.
ELEMENTS OF PROMISINGPRACTICES
Successful health outreach and commu-nication campaigns that target newcomersrequire addressing the immigrant-specific barriers discussed above (e.g.,language, culture, and perceived andreal immigration consequences), help-ing them understand how to access andreceive medical services, and communi-cating the information through multiplesources that are trusted by the targetedcommunity. General elements of aneffective health outreach effort target-ing newcomers include:
• Culturally appropriate materialsand messages. Simply translating materials into other languages is notenough; messages and materials need tobe developed specifically for the targetedaudience. Public health campaigns areincreasingly using market research,focus groups, and community discus-sions to identify appropriate messagesand messengers. “
• Targeted campaigns that utilizeethnic or foreign-language print andelectronic media. Many immigrant fam-ilies rely upon media sources in theirnative language for information andnews. Research suggests that healthoutreach efforts conducted through eth-nic media can be less costly and moreeffective in reaching newcomers thanmainstream media campaigns.16
• Community-based strategies.Effective strategies include distributinginformation at neighborhood fairs, mak-ing presentations at community meet-ings or churches, and going door-to-door in immigrant enclaves. Combininga targeted media campaign with com-munity-based outreach is an especiallypromising approach.17
• Provider-based outreach. Trustedand accessible clinics and health centerworkers can be very effective in com-municating information and encourag-ing enrollment in public health pro-grams. In Los Angeles, for instance, 40percent of all applications to the stateSCHIP program come through healthproviders, more than twice the numberfrom any other single source.18
• School-based strategies.Promising practices include programsthat link enrollment of children in pub-lic health programs with the applicationprocess for subsidized school lunches.
Although these general strategies canbe utilized with most immigrant popu-lations, differences in beliefs and back-ground need to be taken into account.For instance, focus groups reveal thatsome ethnic groups are less likely toenroll in health programs because ofimmigration concerns, while the pri-mary barriers for others are languagecapacity or misunderstandings of eligi-bility requirements.19 Outreach needs totake into account these differences andshould incorporate media outlets andcommunity-based groups that aretrusted by each targeted group.
MULTIMEDIA HEALTH OUTREACH CAMPAIGN
North Carolina Division of PublicHealth and North Carolina HealthyStart FoundationRaleigh, North Carolinawww.ncpublichealth.comwww.nchealthystart.org
In 2000, North Carolina officialslaunched an outreach campaign to pro-mote awareness of the state’s publiclyfunded children’s health insurance pro-grams among Latino families. Ratherthan simply translating materials into
16. USC Division of Community Health. 2006.Reaching Out and Reaching In: Understanding Effortsto identify and Enroll Uninsured Children into HealthInsurance Programs. Los Angeles, CA: The CaliforniaEndowment.17. USC Division of Community Health. 2006.Reaching Out and Reaching In: Understanding Effortsto identify and Enroll Uninsured Children into HealthInsurance Programs. Los Angeles, CA: The CaliforniaEndowment.18. Ibid.19. Ibid.
OUTREACH AND EDUCATION PROGRAMS
114
toll-free, bilingual hotline that providesinformation and referral on material andchild health. The campaign includedprint materials, advertisements, andradio programming featuring “Ana Maria,”a trustworthy Mexican woman and her family.
One highlight of the campaign is a col-orful “fotonovela,” or picture book, fea-turing Ana Maria’s family. The bookexplains complicated information in aformat that is familiar to the intendedaudience. Bilingual state andFoundation staff held focus groups tounderstand what information could help“bridge” Latinos from their previoushealth care systems to the one in theUnited States. This research was used todesign and distribute the fotonovelaand other bilingual materials to commu-nities across the state through a net-work of community service providers,clinics, businesses, and outreach work-ers. Nearly 500,000 copies of Spanishoutreach materials were distributed in2005. The materials were reinforcedthrough the placement of news storiesand advertisements in Spanish media.
The popular “Ana Maria” now appears inmaterials on other health topics, suchas obtaining preventive health care forchildren, reducing the risk of SuddenInfant Death Syndrome, the dangers ofsecondhand smoke, and the importance offolic acid for women of childbearing age.
To expand its efforts, the Foundationlaunched a Spanish website(www.nchealthystart.org/enespanol) inearly 2006 with information on childhealth insurance, the state’s health caresystem, infant mortality reduction,women's health, pregnancy, and infantcare. All materials can be easily down-loaded or ordered from the site.
Although the program’s impact is stillbeing assessed, observers note that theLatino community’s contact with publichealth programs has increased signifi-cantly. More than 25 percent of the callsto the state’s health resource hotline in2005 were made by Spanish-speakingindividuals, and 77 percent of thesecallers inquired about the state’schild health insurance program.
Spanish, the state’s Division of PublicHealth entered a unique public-privatepartnership with the North CarolinaHealthy Start Foundation to developappropriate messages and strategies tar-geting Latinos through a broad mediaand community outreach campaign.
The success of this on-going campaignis due in large measure to the partners’collective vision, cooperation, and will-ingness to build on each partner’sstrengths and expertise. The projectbegan by convening an advisory panelof Latino advocates, holding consumerfocus groups, and hiring one of thestate’s first Latino public relationsfirms. The result was a multi-facetedcampaign to promote a state-run,

115
INCREASING ENROLLMENT IN PUBLIC HEALTH INSURANCE PROGRAMS
GEM: Get Enrollment MovingA project of Citrus Valley Health PartnersCovina, Californiawww.cvhp.org/gem
Another approach to increasing immigrants’ enrollment in public healthprograms is face-to-face outreach.Although this type of outreach can belabor intensive, it can help alleviatefears, build trust, and provide accurateinformation to families who otherwisewould be hard to reach.
Over the last five years, Citrus ValleyHealth Partner’s Get Enrollment Moving(GEM) project has successfully utilizedthis approach to enroll nearly 30,000people into California’s Medicaid, SCHIP,and public health programs for childrenand pregnant women. GEM estimatesthat approximately 85 percent of theenrollees are Latino, three-quarters havelimited English skills, and nearly 35 per-cent live in a family headed by at leastone undocumented adult.
GEM started in 2001 in response to thegrowing number of immigrant families inthe San Gabriel Valley that lacked healthinsurance. GEM recognized that a successful outreach program requirednot only educating immigrants abouttheir health insurance options but alsoaddressing deep-rooted fears and mis-perceptions about the immigration con-sequences of using public programs.
The result was the creation of a programof volunteer health educators, “promo-toras de salud,” who go door-to-door inlow-income neighborhoods to personallyurge eligible families to enroll in publichealth programs. The volunteers, trainedand supervised by GEM staff, visit fami-lies, provide health care information,and identify individuals who are eligiblefor coverage. At GEM’s central office,multilingual staff members provideapplication assistance. As of early 2006,GEM had over 300 volunteers in the pro-motora program covering 27 zip codes
east of Los Angeles. The promotorasalso work with GEM staff to provideinformation and enrollment opportuni-ties at churches, schools, health clinics,community centers, nonprofits, andbusinesses. GEM estimates that its out-reach program makes contact withapproximately 18,000 families each year.
Several factors have contributed to thesuccess of GEM’s promotora program:
• Recruiting volunteers from thecommunity. Volunteers share the cul-ture and language of community mem-bers and face some of the same chal-lenges (e.g., limited English skills,poverty, and undocumented immigrationstatus). Volunteers can build trust withresidents and help them overcome fearsof enrolling in public health programs.
• Making volunteers partners inprogram development. GEM looks tothe promotoras for leadership in devel-oping outreach strategies. The coordina-tor of the promotora program describesher approach as “helping to lead theprogram from beside.” The GEM staffmeets with the volunteers weekly togather and incorporate feedback, ideas,and concerns. GEM also holds an annualretreat with volunteer leaders to discusschallenges facing the program, as wellas to offer an opportunity for respite,education, and camaraderie.
• Providing volunteers with anappropriate level of training andencouraging collaboration with healthworkers. GEM provides all volunteers training on the U.S. healthcare system and eligibility requirements
for public health insurance programs.According to Silvia Rodriguez, executivedirector of GEM, “The promotoras play acritical role in outreaching and identifyingpeople who are eligible. Our staff has acomplementary role in answering thetechnical questions and helping identi-fied individuals enroll in a health plan.”
• Providing personal support andprofessional development opportuni-ties for promotoras. The promotoraprogram helps volunteers develop healthcare knowledge and communicationskills, build self-esteem, gain workexperience, and access professionaltraining courses. In fact, several currentGEM staff originally started as promo-toras. Rodriguez notes that being sup-portive of volunteers encourages long-term participation and strengthens theprogram. “These women are becomingempowered and are taking it as theirmission to start addressing other issuesin their community,” she says. “Theiractivities will not only make a huge dif-ference in their own lives but ultimately,it will benefit their communities.”
The GEM’s promotora program is beingevaluated by researchers at the USCDivision of Community Health. GEMreceives funding from The CaliforniaEndowment, Kaiser Permanente, First 5LA, and L.A. County Department ofHealth Services.
© Ju
pite
r Im
ages

116
relationships with specific communities,provide services and advocacy in neigh-borhood centers, and have the languageand cultural expertise to communicateeffectively. All eight community organi-zations receive training and technicalassistance from the policy and legalorganizations, and each employs atleast one part-time bicultural, bilingualhealth advocate. The Collaborative’sactivities include:
• Conducting community educationand outreach to raise the awarenessand confidence of immigrants andrefugees interacting with the healthcare system. Community workshops,public education materials, and outreachthrough the ethnic media inform immi-grants of their rights to health care,their eligibility for insurance and afford-able payment options, and any potentialimmigration consequences.
• Providing direct assistance toimmigrants and refugees who havebeen unable to access or pay forhealth care. With technical assistanceprovided by the policy and legal organi-zations, the community health advo-cates help address problems involvinglack of access to services, health cover-age, hospital payments, or discrimina-tion. The initial four community groupsin the Collaborative assisted over 1,100clients annually. The numbers haveincreased with the addition of four newcommunity groups in 2005.
• Using knowledge gained frominteraction with individual immi-grants to develop recommendationsfor policy reform. With the informationprovided by the community partners,the Collaborative has been able to pro-vide feedback to hospitals and otherpublic agencies on improving their serv-ices (as well as file civil rights complaintswhen agencies have been unresponsive).The Collaborative is also bringing immi-grant voices to health policy debates atthe state and national levels.
• Developing the skills of immi-grant-serving organizations throughongoing capacity-building partner-ships. This project has developed thecapacity of relatively small immigrant-based organizations to provide accurateand timely health information to com-munity members. The community part-ners, in turn, are able to implementbroad public education in multiple lan-guages and can mobilize their communi-ties to support public policy reforms.
The Collaborative has an annual budgetof approximately $250,000, with fund-ing from Elebash Fund, United HospitalFund, Alman Foundation, New YorkCommunity Trust, Long Island CommunityFoundation, and Westchester CommunityFoundation. “All of the organizations inthe Collaborative are responding to theircommunities’ need for accurate healthinformation and advocacy, and theydevote considerably more resources tohealth care work than what they receivethrough these grants,” Gurvitch pointsout. “But what the grants have done isallow them to go deeper on these issues,work together, learn from each other, anddevelop a coalition that has addressedshared challenges far beyond what anysingle group could do by itself.”
© Ju
pite
r Im
ages
21. The eight community organizations are HaitianAmericans United for Progress, Korean CommunityServices of Metropolitan New York, Latin AmericanIntegration Center, Shorefront YW-YMHA ofManhattan-Brighton Beach, Council of PeoplesOrganization, Filipino American Human Services,Make the Road by Walking, and Reconciliation andCulture Cooperative.22. Bernstein, Nina. 2006. “Recourse Grows Slim forImmigrants Who Fall Ill,” The New York Times, March 3.
PROVIDING ACCURATE HEALTH INFORMATION
Immigrant Health Access andAdvocacy CollaborativeA project of the New YorkImmigration CoalitionNew York, New Yorkwww.thenyic.org
Addressing barriers to low-income immigrants’ access to health care in NewYork City is the mission of theImmigrant Health Access and AdvocacyCollaborative. Begun in 2000, theCollaborative involves the New YorkImmigration Coalition, New York Lawyersfor the Public Interest, and eight com-munity organizations that serve new-comers. Together, these orgainizationsprovide outreach, training, individualassistance, and systemic advocacy onpublic health care.21
According to Project Director AdamGurvitch, nearly two-thirds of uninsuredadults in New York City are immigrants,and the rate of uninsured immigrantchildren is five times higher than thecity average, even though all childrenare eligible for the state’s SCHIP pro-gram. These disparities are due in largepart to conflicting messages aboutimmigrants’ rights to public health careand the risks of using such services.Since September 11, 2001, newcomershave only become more fearful of theimmigration consequences of using pub-lic health resources. As The New YorkTimes observed, “More and more immi-grants are delaying care or retreatinginto a parallel universe of bootleg reme-dies and unlicensed practitioners.”22
The Collaborative has been successful in addressing these misunderstandingsbecause the partners are trusted com-munity groups that have longstanding
© Ju
pite
r Im
ages

117
INCREASING ACCESS TO REPRODUCTIVE HEALTH CARE
La Promesa and Adult Role ModelsPlanned Parenthood Southeastern Floridawww.plannedparenthood.org
Responding to the fast-growing Latinoand immigrant communities in south-eastern Florida, Planned Parenthood ofGreater Miami, Palm Beach, and TreasureCoast Area (Planned Parenthood)23
established two programs, La Promesaand Adult Role Models, to increase thesecommunities’ awareness and access toreproductive health.
La Promesa’s goal is to “break down bar-riers to reproductive health care for theHispanic population,” says Maria Kulp,vice president of education of the localPlanned Parenthood. The program usesbilingual community health workers,known as “promotoras de salud,” toconduct outreach and communicate withSpanish-speaking individuals, primarilywomen, served by its health centers.Reflecting the area’s ethnic diversity,the promotoras include women from theCaribbean, Mexico, and Central America.
In addition to increasing the access ofLatina immigrants to Planned Parenthoodservices, La Promesa works to heightentheir awareness of reproductive andfamily health issues, promote earlydetection of and reduce the mortalityrate for breast and cervical cancer, andassist families in communicating effec-tively about sexual and reproductivehealth.
La Promesa promotoras typically connectwith their Spanish-speaking clients atoutreach events, including health fairs,after-school programs, and presentationsat faith-based organizations. They alsogo door-to-door to homes, markets, andbusinesses in Latino communities.
To encourage Latina women to seekhealth services, La Promesa offers freePap smears and linguistically and cultur-ally appropriate services. “We startedthis knowing that Latina women proba-bly are one of the worst groups at seek-ing care for themselves. We wanted todo outreach to promote the health cen-ter, let them know that this was afford-able. The program just took off andbecame a lot larger than anyone hadanticipated,” Kulp says.
When women call to make an appoint-ment at a Planned Parenthood healthcenter, they are asked for their languagepreference. If their response is Spanish,a La Promesa staff person will usuallygreet the person on arrival to the office,help with the completion of forms, andfollow-up with the individual after themedical appointment as needed. Kulpestimates that about 3,000 women areserved through La Promesa each year,and the program has increased requestsfor contraception at Planned Parenthoodoffices in southeastern Florida by 129 percent.
Planned Parenthood also operates AdultRole Models (ARM), a unique trilingualprogram that utilizes parent volunteersto educate youth and the broader com-munity about sexual health and teenpregnancy. It works with three agencies
that primarily serve Latinos, Haitians,and African-Americans to recruit parentsfrom those communities to participatein the program and organize trainings inEnglish, Spanish, and Creole. ARM alsoprovides 75 hours of training to parentvolunteers on information about sexual-ity. Topics include contraception,puberty, sexual orientation, prenatalcare, HIV/AIDS, and more.
“The curriculum is designed to providethe Adult Role Models with current,accurate information on these topics.There is a pre- and post-test completedat each session to let us know if theyhave increased their knowledge…Additionally, at the end of the trainingsessions, the [role models] have todesign and present a workshop to thegroup that is taped to be able to givethem feedback,” Kulp explains.
After their training, these parents returnto their communities and train otherparents on how they can talk to theirchildren about sex. These sessions canbe either formal or informal in nature,depending on the experience of the par-ents who have finished their ARMstraining. While some, particularly thosewho were professionals in their nativecountries, teach at churches and com-munity groups, others prefer to teach in their homes. In 2005, the projecttrained over 70 parents, who in turnhave reached another 5,000 parents.
Although the ARM program, which has astaff of three, is funded solely by theChildren Services Council of Palm BeachCounty, La Promesa has received founda-tion support, including grants from theQuantum Foundation and the PicowerFoundation. The success of these pro-grams has led funders to urge thatPlanned Parenthood expand them tonearby counties. Planned Parenthoodchapters in St. Lucy County and MartinCounty have both adopted La Promesaprograms. St. Lucy County also has anARM program, and Martin County is considering launching one as well.
© Ju
pite
r Im
ages
23. Planned Parenthood of Greater Miami, PalmBeach, and Treasure Coast Area operates eighthealth centers in six counties. In 2005, the eightcenters served more than 30,000 individuals,approximately 17 percent of whom were Latino.

118
While new immigrants frequently experi-ence communication problems in theirdaily lives, language and cultural barri-ers can be much more harmful whenimmigrants are seeking medical services.Miscommunications between medicalpersonnel and patients can have costlyand tragic consequences for both indi-vidual immigrants and the broader com-munity. A report by Grantmakers in Healthidentifies some of the harmful effects oflanguage barriers in health care:27
• Reduced access to health insurance,preventive care, and specialty services.
• Compromised patient understandingof diagnosis and treatment plans.
• Lower patient satisfaction.
• Lower quality of care, which canlead to serious complications andadverse clinical outcomes.
• Higher costs to the health care sys-tem through unnecessary testing as wellmedical complications resulting from thelack of treatment or misdiagnoses.
Conversely, there are a number of stud-ies showing the positive health effectsof providing LEP patients with languageservices. A review of these studies foundthat:
…[P]atients with limited English proficiency who are provided with...interpreters make more outpatient visits,receive and fill more prescriptions, donot differ from English proficientpatients in test costs or receipt ofintravenous hydration, have outcomesamong those with diabetes that are
24. Capps, Fix, Passel, et al., 2003. 25. Moran and Petsod. 2004. Newcomers in theAmerican Workplace: Improving EmploymentOutcomes for Low-Wage Immigrants and Refugees.Sebastopol, CA: Grantmakers Concerned withImmigrants and Refugees and NeighborhoodFunders Group.26. For a detailed analysis of relevant federal lawsrequiring language access, see: Perkins, Jane, MaraYoudelman, and Doreena Wong. 2003. EnsuringLinguistic Access in Health Care Settings: LegalRights and Responsibilities, 2nd Edition. LosAngeles, CA: National Health Law Program.27. Grantmakers In Health. 2003. In the RightWords: Addressing Language and Culture in ProvidingHealth Care. Washington, D.C.: Grantmakers InHealth.28. Ku, Leighton and Glenn Flores. 2005. “Pay NowOr Pay Later: Providing Interpreter Services InHealth Care.” Health Affairs 24: 435-444.
This federal law requires states, counties,and private health providers receivingfederal funds to make reasonableefforts to provide language assistanceto limited English proficient individuals.This longstanding requirement gainedsignificant public attention afterPresident Clinton issued ExecutiveOrder 13166 in 1999, requiring federalagencies to develop procedures for
TITLE VI OF THE 1964 CIVIL RIGHTS ACT
improving language access to their programs, as well as issuing specificguidance on how recipients of federalfunding should implement Title VI’s language access requirements. Thisorder has been affirmed by the Bushadministration, which has set up a web-site to provide guidance, best practices,and resources at www.lep.org.
© Ju
pite
r Im
ages
Providing newcomers with access tohigh-quality health care requires
that service providers and insuranceprograms be able to communicate withthem effectively. Because nearly half ofall immigrant adults speak English withsome limitations24 and 40 percent haveresided in the United States for lessthan 10 years,25 reducing language andcultural barriers is critical to increasingaccess to good health care.
The “Improving Language Access inGovernment Services” section of thistoolkit provides a general overview ofthe language barriers faced by newimmigrants, describes the legal obliga-tions of federal contractors and grantees(including public health agencies andmedical service providers) to providelinguistically accessible services, andhighlights promising practices. The general elements of a successful lan-guage access policy for assessment, plandevelopment, bilingual staffing, transla-tion of written materials, training ofstaff, evaluation, and outreach apply inthe health care setting as well. Healthcare organizations that receive federalfunds are required to make reasonableefforts to offer free language assistanceservices to limited English proficient(LEP) individuals.26
In addition to language, culture playsan important role in determining thequality of an individual’s interactionwith the health care system. Recentimmigrants often bring traditions andpractices unfamiliar to U.S. health careprofessionals, and they often have lim-ited experience with Western medicine.
LANGUAGE ACCESSAND CULTURAL
COMPETENCE
119
superior or equivalent to those ofEnglish-proficient patients, and havehigh satisfaction with care. LEPpatients with bilingual providers askmore questions, have better overallinformation recall, and are more com-fortable discussing sensitive or embar-rassing issues; those with hypertensionor diabetes have less pain and betterphysical functioning, psychologicalwell-being, and health perceptions andhave high patient satisfaction…28
ELEMENTS OF PROMISING PRACTICES
The health care sector has been a leaderin developing promising practices toreduce language and cultural barriers.There is federal funding available tosupport language assistance in healthprograms serving low-income families.In addition, several foundations havefunded projects that provide advocacy,technical assistance, and research sup-port to help states seek federal match-ing funds and develop long-term fund-ing streams for this purpose.29 Thehealth care sector has also been wellahead of other fields in developingstandards for providing linguistically and culturally competent services.
Improving communications betweenhealth care providers and recent immi-grants in the service delivery settinghas been the focus of most efforts toincrease access. Because of the diversityof health care providers (ranging fromsmall clinics to large public hospitals),varying demographics of local communi-ties, and differences in culture and lan-guage among immigrant communities, awide range of practices have been devel-oped over the years. They include:
• Assessing community needs anddeveloping administrative infrastruc-ture for providing language services.Each agency begins with an assessmentof the language needs of its servicepopulation and its capacity to servethese individuals. This is followed bythe development of a plan for communi-cating both verbal and written informa-tion. Providing funding for these initialsteps can encourage health care institu-tions to make the changes needed toserve LEP individuals.
• Increasing the number of bilingual/bicultural medical staffmembers. Research suggests that thebest way to provide medical services tonewcomers is through bilingual medicalproviders who are familiar with the culture of their patients. Foundation-supported projects in this area include(1) language and cultural training toexisting medical staff; (2) resources torecruit bilingual health workers, nurses,and physicians; and (3) programs totrain immigrants to become healthworkers.30
• Increasing interpretationresources. In recent years, a number ofthird-party interpretation models haveemerged, including (1) dedicated staffinterpreters at a specific hospital orclinic; (2) private or non-profit in-person contract interpreters; and (3)remote, third-party interpretation.Support for research in using innovativenew technologies has helped makeremote interpretation services—tele-phonic, videoconferencing,31 and remotesimultaneous medical interpreting usingwireless technology32—increasinglyviable. Initial research suggests thatthese approaches can enhance access tomedical interpretation because there isno wait for interpreters to be physicallypresent, and they may be more cost-efficient than in-person interpretation.
• Supporting translation of writtendocuments. Written materials are criti-cal to communicating health-relatedinformation. Patient care instructions,consent forms, medical history forms,and health education materials are allvital documents that should be language-accessible. Health care organizationsneed to identify and prioritize the mostimportant documents for translationinto languages commonly spoken by
patient populations. Ideally, translatedwritten materials should reflect the cul-tural nuances of the target populationand be at the appropriate educationaland literacy levels.
• Promoting advocacy and policyreform. As with efforts to expand immi-grant eligibility for state public healthprograms, advocacy is important indeveloping policies that lessen languageand cultural barriers to health care.Foundation-funded advocacy effortshave included projects to urge federalagencies to enforce existing languageaccess laws, advocate that states seekfederal reimbursement for languageservice costs, educate policymakers onthe importance of language access, andnegotiate with state or local healthagencies to develop effective accessplans. In some communities, founda-tions can also play a convening role inbringing various stakeholders together toaddress language and cultural barriers.
© Ju
pite
r Im
ages
29. See examples discussed in Grantmakers InHealth, 2003.30. See profiles of the International Institute ofMinnesota’s Medical Careers Project in the“Promising Practices in English Acquisition” sectionand the Welcome Back Initiative in the “PromisingPractices in Economic Mobility” section.31. Health Access. 2002. Videoconferencing MedicalInterpretation: The Result of Clinical Trials. Oakland,CA: Health Access.32. Youdelman, Mara and Jane Perkins. 2002.Providing Language Interpretation Services in theHealth Care Settings: Examples from the Field. LosAngeles, CA: National Health Law Program.
Watch the DVDHold Your Breath:The Doctor’s Office
Health care is a challenge for manyAmericans, and particularly problematic for
immigrants who may lack English skills, accessto care, and familiarity with Western medicine.
Hear from both “sides,” as an immigrant family faces confusing, possibly devastating
information, about their cancer-strickenfather, and as their American-born physician struggles with his own
cultural limitations.

120
telephonic interpretation for doctors,dentists, nurses, and other medicalstaff. In 2004-05, its staff providedinterpretation for approximately 5,150medical appointments.
By all accounts, El Puente provides acritical service to both the local Latinocommunity and health agencies.Although providers have increased hir-ing of bilingual personnel and use ofcontract interpreters, El Puente contin-ues to play a major role in makinghealth services accessible. “The interpre-tation services provided by El Puente forour non-English speaking patients areextremely important for safe and effec-tive patient care,” explains BeckyKimmel, executive director of St. JohnMedical Center. “Both patients andthe medical community benefit from
increased understanding, which enablesus to deliver efficient and compassion-ate care.”
El Puente’s success suggests that itcould serve as a model for other immi-grant communities located in regionswhere bilingual medical resources arescarce and health care providers havelittle experience serving newcomers. Theproject has also played a role in easingpotential tensions between native-bornresidents and the growing Latino com-munity. According to El Puente execu-tive director Vida Day, the rapid growthin the Latino population had causedsome residents to perceive new immi-grants as a “drain” on the local healthcare system. “The nonprofit modelallows us to demonstrate the Latinocommunity’s commitment to finding asolution to this challenge, while alsodrawing resources from local foundationsand individuals.” As of 2005, El Puentereceived about half its revenues fromover 10 local foundations, with the remaining coming from individualdonors. “Funders should understand thattheir support is absolutely critical inrural communities,” says Day, “whereresources are scarce and their contribu-tions can make a tremendous differencein improving the health of immigrants.”
EFFECTIVE HEALTH INTERPRETATION SYSTEMS
Cambridge Health AllianceCambridge, Massachusettswww.challiance.org
Providing language access in large hospital settings requires more thanqualified interpreters. Well-designed systems are needed to enable providersand patients to utilize interpretersquickly and effectively. Research indi-cates that patient and provider satisfac-tion with language services depends inpart on how easily interpreters areavailable. When requests for interpreta-tion lead to delays, providers and LEPpatients often try to communicatewithout assistance, and over the long-term may be discouraged from request-ing interpreters altogether.
Cambridge Health Alliance (CHA), whichoperates three large hospitals and 20primary care sites in the area north ofBoston, has developed an innovativesystem of language services. Key elementsinclude (1) development of a centralizeddispatch system; (2) training of medicalstaff on how to best utilize interpreters;(3) outreach to hospitalized LEP patients;and (4) ongoing monitoring and evalua-tion of the program.
In May 2005, almost three decadesafter it first started providing languageassistance to LEP patients, CHA adoptednew “one number calling” for all inter-pretation requests. Providers canrequest face-to-face or telephonic inter-pretation in the three languages pro-vided by CHA staff (Portuguese,Spanish, and Haitian Creole), as well asin over 40 languages that are providedby “per diem” interpreters.34 If staff orper diems are unavailable, the systemrefers providers to the telephonic inter-pretation services of a third party con-tractor. Prior to this system, CHA med-ical staff had to call different numbers
© Ju
pite
r Im
ages
33. All of the demographic information was provided by El Puente.
HEALTH INTERPRETATION SERVICES IN RURAL AREAS
El Puente (The Bridge) Jackson, Wyoming
Like many rural communities, TetonCounty, located on the Wyoming-Idahoborder, is undergoing dramatic demo-graphic changes. The availability ofagricultural and service jobs has drawnnewcomers to the region, and themostly Latino immigrant population hasgrown fourfold since 1995, to 2700 resi-dents. And these newcomers are seekingservices from the local health care sys-tem. In 1990, the primary local hospi-tal—St. John Medical Center—did notdeliver a single Latino baby. By 2005,over 24 percent of the babies born therewere Latino.33 Local health care providershave struggled to make their servicesaccessible to this fast growing population.
El Puente was started in October 2003to help address these challenges by pro-viding interpreter services and healthcare education for immigrants. El Puenteoffers medical interpreting services athospitals and medical offices free ofcharge to both patients and health careproviders. It also works with individualpatients to help them navigate the localhealth care system, enroll in insuranceprograms, and receive care as needed.With an annual budget of only $200,000and a staff of four full-time trainedmedical interpreters and six part-timeinterpreters, El Puente provides almost400 hours per month of in-person and
121
based on their location and the lan-guage needed. The new system, whichutilizes automatic call distributionqueues staffed by Portuguese, Spanish,and Creole interpreters at 10 sites, notonly makes it easier for providers torequest assistance, it also helps CHAutilize its interpreter staff more effi-ciently. Interpreters at the three hospi-tals and seven health centers providetelephone interpreting to all 23 CHAsites, as well as face-to-face interpret-ing at their own sites. The new systemautomatically connects a caller to anavailable interpreter. These changeshave resulted in significantly less wait-ing time for LEP patients and more efficient use of CHA’s resources.
To implement the new system, CHA hasprovided orientation and training to itsmedical personnel. Equally important,CHA’s interpretation unit and the nurs-ing staff have worked to identify situa-tions in which interpretation is under-utilized. For instance, requests for inter-preters are less likely to occur for hospi-talized patients, who may then have dif-ficulty communicating discomfort, symp-toms, or other important information toinpatient care providers.
With support from the Blue Cross BlueShield of Massachusetts Foundation,CHA is installing dual handset speakerphones in its inpatient facilities neareach patient bed. CHA will train nursingstaff to identify situations that requireinterpretation, address the reluctance of some staff to utilize telephonic inter-pretation, and provide orientation topatients on how and when to request aninterpreter. Staff interpreters will alsoconduct daily visits to each inpatient-care facility, speak directly with LEPpatients, and record relevant informa-tion in the individual’s medical records.
According to Director of MultilingualInterpreting Loretta Saint-Louis, thenew system’s centralized nature allowsmanagers to monitor performance andidentify and respond to problems.“Overall,” says Saint-Louis, “the changeshave made the system easier to use andhave maximized our productivity.” Theaverage wait time for interpreter serv-ices in the three most common non-English languages is now less than oneminute. CHA’s interpreting volume grewby 14 percent in the first six months of
the program, while expendituresincreased by less than half that amount.Telephonic interpretation expanded byan astounding 82 percent, suggestingthat providers were becoming more com-fortable with the service. “While we stillhave a lot to learn and evaluate,” Saint-Louis notes, “the bottom line is thatthese changes have made it easier for LEPpatients to obtain accessible health care.”
INCREASING WORKFORCEDIVERSITY
Welcome Back InitiativeSan Francisco, Californiawww.e-welcomback.org
Providing accessible medical services tonewcomers requires hiring providers withrelevant cultural backgrounds and lan-guage skills. An innovative approach isthe Welcome Back Initiative, whichbuilds on the skills of internationallytrained immigrant health professionals.This California-wide project has helpedthousands of immigrant health workersbecome oriented to the U.S. health caresystem, enroll in English classes andhealth care courses, obtain requiredlicenses and credentials, and find jobsin the health field. The project is help-ing immigrants improve their economicsituations, while also making healthservices more accessible to newcomers.The Welcome Back Initiative is describedin detail in the “Promising Practices inEconomic Mobility” section.
© H
arry
Cut
ting
Phot
ogra
phy
, In
c.
34. “Per diem” staff members are on-call employeeswho only come in when there is need for their services.

122
Opened in 1913 in East Los Angeles bythe Seventh Day Adventist Church,White Memorial Medical Center startedas a medical clinic and slowly grew intoa major teaching hospital. Today, it isthe flagship facility for Adventist Health,a nonprofit that operates a number ofhealth facilities on the West Coast.
More importantly, White Memorial hasemerged as a powerful example forhow integrating newcomers into thehealth care system—as patients, healthprofessionals, vendors, leaders, andstakeholders—can reap enormous ben-efits for the receiving community.
White Memorial, says Ignatius Bau, aprogram director at The CaliforniaEndowment, is a story of “how an insti-tution that was increasingly becomingirrelevant in the neighborhood trans-formed itself by reaching out to theimmigrants and refugees that are nowthere. The way indigenous leadershipemerged to broker relationships betweenthe hospital and the community in alldifferent kinds of ways could be appliedto integration strategies beyond thehealth arena.”
Over the course of its history, WhiteMemorial experienced both lean timesand periods of expansion. In the decadesafter World War II, the hospital flour-ished as a pioneer in open-heart surgery
and other specialty procedures. But bythe 1980s, White Memorial, like othersafety-net hospitals that provided a sizableamount of uncompensated care, was facing a financial crisis and the possibilityof closure.
One reason for the hospital’s financialdecline was its slowness to adjust to thearea’s changing demographics. BeforeWorld War II, East Los Angeles was pre-dominantly home to immigrants ofJapanese and European descent. But bythe 1980s, working-poor Latino immi-grants, most of whom spoke Spanish astheir primary language, made up the vastmajority of the area’s population. Largelyuninsured patients began using the hospi-tal primarily for emergency services, leav-ing its specialty service underutilized. Anddespite the increase in Latino patients, thehospital had very few Latino or Spanish-speaking staff who could effectively serveits new patient population.
A STRATEGY FOR SURVIVAL
In the wake of its financial crisis, WhiteMemorial recognized that its future exis-tence depended on its ability to adapt tothis new demographic reality. It devised astrategy to build a closer relationship withthe growing Latino community by becom-ing a community-based hospital focusedon the area’s most critical health need: thesevere shortage of primary care providers,especially for Spanish-speaking patients.
White Memorial eliminated several of its specialized residency programs andshifted its focus to building the capacityto provide culturally competent primarycare to Latino patients. Over time, thehospital recruited a diverse professionalstaff, instituted effective training andretention programs, and learned how toincorporate neighborhood residents intoall aspects of the medical center’s activi-ties—as patients, employees, vendors,board members, and future health profes-sionals. In developing this successful strat-egy, White Memorial transformed itselfinto an invaluable community healthresource whose services and contributionsgo well beyond providing traditionalmedical services.
DIVERSIFYING THE HEALTH CARE WORKFORCE
Developing a diverse workforce, WhiteMemorial recognized, would be criticalto meeting the area’s health care needs.To increase the number of qualifiedhealth professionals, the hospital estab-lished the Family Medicine Residencyprogram to (1) recruit medical residentsfrom East Los Angeles, as well as otherswho plan to practice in underservedareas; (2) provide them with the skillsand understanding to be successful inworking with the health problems theyencounter in underserved areas; and(3) equip them with the knowledgeand networking needed to have a successful practice.
Developing local talent is a top priorityfor the residency program. Four of theseven founding members of the privatefamily practice group, who also serveas faculty for the Family MedicineResidency program, grew up uninsuredin East Los Angeles. With their leader-ship, White Memorial developed amulti-faceted strategy to prepare andrecruit neighborhood residents to workat the hospital. By expanding primarycare services to meet local needs, forexample, the hospital also created anopportunity to hire a number of newphysicians who were local residents orhad the necessary language and cul-tural skills to serve Latino patients.
According to Dr. Hector Flores, co-director of Family Medicine Residency,these changes “immediately increasedthe hospital’s opportunity to connectwith the community. It opened thedoor to the immigrant population.They began to feel that not only was[White Memorial] a good place to go if you needed emergency care, but itwas also a good place to go for all yourmedical needs, for keeping yourselfwell, managing a chronic condition,and so on.”
As part of its long-term strategy, theprivate family practice group also sup-ports pipeline programs to providementoring and increase interest inhigher education, especially the health
RESPONDING TO DEMOGRAPHIC CHANGE, DRIVEN BY COMMUNITY NEEDS
WHITE MEMORIAL MEDICAL CENTER WWW.WHITEMEMORIAL.COM
White Memorial is a story of
how an institution that was
increasingly becoming irrelevant
in the neighborhood transformed
itself by reaching out to the
immigrants and refugees that are
now there. The way indigenous
leadership emerged to broker
relationships between the hospital
and the community in all different
kinds of ways could be applied
to integration strategies beyond
the health arena.”
–Ignatius Bau, Program DirectorThe California Endowment
“

123
professions, among local high schoolstudents. It also developed partnershipswith two science magnet schools thatbring students and residence stafftogether regularly. Cultivating the inter-est of area students serves multiplegoals: It increases the number of physi-cians interested in working in under-served areas; creates career paths andexpands economic opportunity foryoung people in the community; andincreases minority representation andcultural and linguistic competency inthe health field over the long term.
As of early 2006, the Family MedicineResidency Program had 86 graduates:70 percent are working in underservedareas, and 40 percent have remained inEast Los Angeles.
BUILDING CULTURAL COMPETENCE
Although many young physicians havea personal commitment to serving low-income communities, they may shyaway from the work because they arenot trained in the skills those environ-ments require. With funding from TheCalifornia Endowment, White Memorial’sFamily Practice Residency program cre-ated the Cultural Competence Initiativeto broaden the understanding of cul-tural competence beyond languageand ethnicity. Through the initiative,medical residents learn about cultural,gender, educational, and economicissues that have an influence on patients’health and the challenges the residentsmay face in delivering care to suchpatients. White Memorial’s family medi-cine clinic has served as a “living labo-ratory” for developing this curriculum,drawing on the real-life challenges thathealth professionals experience on adaily basis.
Significantly, all hospital departments arenow easily accessible to Spanish speakersonsite, via telephone, and on the Web. Allhospital staff receive training in cross-cul-tural interaction; many more communityresidents are on staff; and the hospital hasincreased community representation onits governing board.
RESPONDING TO COMMUNITY NEEDS
In the same spirit of responsiveness,White Memorial has looked to communityneeds to drive its service priorities. Forexample, it expanded its maternal andchild health care facilities and services toreflect the needs of the area’s demograph-ics, even though some of these services,like neonatal care, are very expensive. Thehospital also put in place other programsthat provide community members withinformation about how to access healthand related services that may be availableto them. Such programs, delivered inSpanish, demystify an otherwise compli-cated medical system for both immigrantand U.S.-born Latinos.
THE HEALTH INDUSTRY AS AN ECONOMIC ENGINE
The family medicine practitioners at WhiteMemorial understand that the health careindustry can be an engine for neighbor-hood economic growth, and they striveto benefit the community when they hireemployees and contract out services.
For example, local residents account forover half of hospital’s 1500-person work-force—from physicians and health educa-tors to clerks and janitors. Within the fam-ily practice group, which serves 45,000patients annually, about 95 percent of theemployees are women, many of whomare from immigrant backgrounds andabout half of whom are single heads ofhouseholds. For many nonprofessionalemployees, working for the family prac-tice group is their first job, and the groupis deliberate about providing support tohelp them achieve financial stability. Forexample, it provides training in financialliteracy and offers access to interest-freeloans that employees have used to pay offdebt, purchase homes, or send their chil-dren to college. As the practice has grown,it has also offered educational scholar-ships to employees and their family mem-bers who want to improve their careers.
Beyond their work within their practicegroup, family practitioners also haveworked to direct the $100 million thatWhite Memorial contracts with vendorsto businesses in East Los Angeles. Notlong ago, the hospital did no businesswith any East Los Angeles vendors, butas of 2004, between $22 and $25 mil-lion a year of White Memorial contractswas staying in East Los Angeles. This hashad an unexpected positive impact onincreasing health coverage for commu-nity residents. As local businesses thrive,they began to offer employees healthcare benefits, and increasing numbersof local employees are going to WhiteMemorial for their health care needs.
A VALUED COMMUNITY RESOURCE
Nearly 20 years ago, White Memorialchanged with its patient population.The choice has required the disman-tling of barriers, active outreach, andan infusion of ingenuity. Today, WhiteMemorial is thriving in the midst of theimmigrant community it serves. ForIgnatius Bau of The California Endowment,this success was due to “a prettyunique confluence of factors, but thelesson for others is how the organiza-tional transformation happened.”
On April 9, 2006, White Memorial celebrated the opening of a brand-new$200 million state-of-the-art facility. Amongthose celebrating the event were themayor of Los Angeles, a congressionalrepresentative, a city councilmember, theconsul general of Mexico, and a numberof local celebrities. They had gathered tocelebrate not just a hospital but thelifeblood of the community itself.
The beautiful $200-million
state-of-the-art building we
now have makes a statement to
the community that they are
welcome and that they deserve
the best of care, even if they are
poor. It is also a tribute to the
physicians who work here. And
it is all about this community
and its demographics.”
—Dr. Hector Flores, Co-DirectorFamily Medicine Residency
White Memorial Medical Center
© Ju
pite
r Im
ages
“
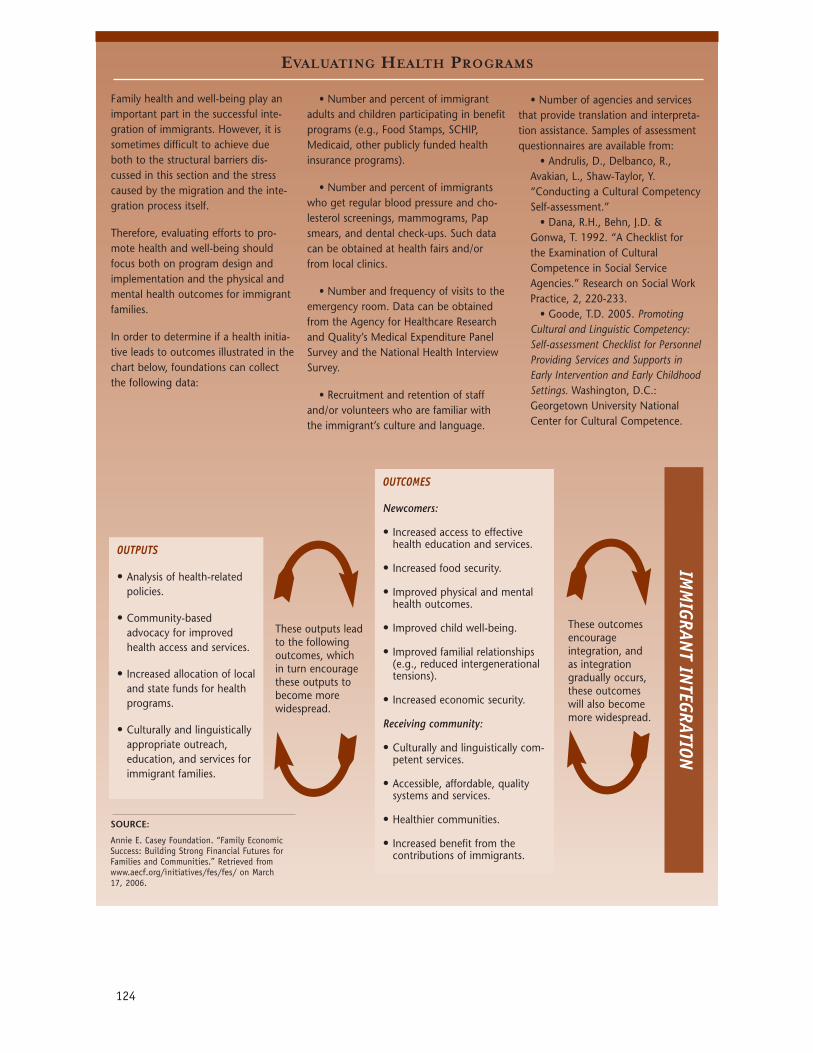
EVALUATING HEALTH PROGRAMS
124
Family health and well-being play animportant part in the successful inte-gration of immigrants. However, it issometimes difficult to achieve dueboth to the structural barriers dis-cussed in this section and the stresscaused by the migration and the inte-gration process itself.
Therefore, evaluating efforts to pro-mote health and well-being shouldfocus both on program design andimplementation and the physical andmental health outcomes for immigrantfamilies.
In order to determine if a health initia-tive leads to outcomes illustrated in thechart below, foundations can collectthe following data:
• Number and percent of immigrantadults and children participating in benefitprograms (e.g., Food Stamps, SCHIP,Medicaid, other publicly funded healthinsurance programs).
• Number and percent of immigrantswho get regular blood pressure and cho-lesterol screenings, mammograms, Papsmears, and dental check-ups. Such datacan be obtained at health fairs and/orfrom local clinics.
• Number and frequency of visits to theemergency room. Data can be obtainedfrom the Agency for Healthcare Researchand Quality’s Medical Expenditure PanelSurvey and the National Health InterviewSurvey.
• Recruitment and retention of staffand/or volunteers who are familiar withthe immigrant’s culture and language.
OUTPUTS
• Analysis of health-relatedpolicies.
• Community-based advocacy for improvedhealth access and services.
• Increased allocation of localand state funds for healthprograms.
• Culturally and linguisticallyappropriate outreach, education, and services forimmigrant families.
OUTCOMES
Newcomers:
• Increased access to effectivehealth education and services.
• Increased food security.
• Improved physical and mentalhealth outcomes.
• Improved child well-being.
• Improved familial relationships(e.g., reduced intergenerationaltensions).
• Increased economic security.
Receiving community:
• Culturally and linguistically com-petent services.
• Accessible, affordable, qualitysystems and services.
• Healthier communities.
• Increased benefit from the contributions of immigrants.
These outputs leadto the followingoutcomes, which in turn encouragethese outputs tobecome morewidespread.
These outcomesencourage integration, and as integration gradually occurs,these outcomeswill also becomemore widespread.
SOURCE:
Annie E. Casey Foundation. “Family EconomicSuccess: Building Strong Financial Futures forFamilies and Communities.” Retrieved from www.aecf.org/initiatives/fes/fes/ on March17, 2006.
• Number of agencies and servicesthat provide translation and interpreta-tion assistance. Samples of assessmentquestionnaires are available from:
• Andrulis, D., Delbanco, R.,Avakian, L., Shaw-Taylor, Y.“Conducting a Cultural CompetencySelf-assessment.”
• Dana, R.H., Behn, J.D. &Gonwa, T. 1992. “A Checklist forthe Examination of CulturalCompetence in Social ServiceAgencies.” Research on Social WorkPractice, 2, 220-233.
• Goode, T.D. 2005. PromotingCultural and Linguistic Competency:Self-assessment Checklist for PersonnelProviding Services and Supports inEarly Intervention and Early ChildhoodSettings. Washington, D.C.:Georgetown University NationalCenter for Cultural Competence.
IMM
IGRANT IN
TEGRATION