Embed Size (px)
DESCRIPTION
In 2000, the Institute of Medicine reported that as many as 98,000 Americans die each year as the result of medical error. This special report on patient safety seeks to foster clearer and better informed discussion of the ethical concerns that are integral to the development and implementation of effective policies that would address the problem of medical error.
Citation preview

A SPEC IAL SUPPLEMENT TO T H E HAST INGS CENTER REPORT
PromotingPATIENT SAFETY
VIRGINIA A. SHARPET H E. . . . . . . . . . . . . . .
HASTINGS. . . . . . . . . . . . . . .
C E N T E R
AN ETHICAL BASIS FOR POLICY DELIBERATION

This is the final report of a two-year Hastings Center research
project that was launched in responseto the landmark 1999 report from theInstitute of Medicine, To Err IsHuman, and the extraordinary atten-tion that policymakers at the federal,state, regulatory, and institutional lev-els are devoting to patient safety. Itseeks to foster clearer and better dis-cussion of the ethical concerns thatare integral to the development andimplementation of sound and effec-tive policies to address the problem ofmedical error. It is intended for poli-cymakers, patient safety advocates,health care administrators, clinicians,lawyers, ethicists, educators, and oth-ers involved in designing and main-taining safety policies and practiceswithin health care institutions.
Among the topics discussed in thereport:
n the values, principles, and per-ceived obligations underlying pa-tient safety efforts;
n the historical and continuingtensions between “individual” and“system” accountability, betweenerror “reporting” to oversight agen-cies and error “disclosure” to pa-tients and families, and betweenaggregate safety improvement andthe rights and welfare of individualpatients;
n the practical implications forpatient safety of defining “respon-sibility” retrospectively, as praise orblame for past events, or prospec-tively, as it relates to professionalobligations and goals for the fu-ture;
n the shortcomings of tort liabili-ty as a means of building institu-tional cultures of safety, learningfrom error, supporting truth tellingas a professional obligation, or ad-
equately compensating patientsand families, contrasted with alter-native models of dispute resolu-tion, including mediation and no-fault liability;
n the needs of patients, families,and clinicians affected by harmfulerrors and how these needs may beaddressed within systems ap-proaches to patient safety; and
n the potential conflicts betweenthe protection of patient privacyrequired by the Health InsurancePortability and Accountability Actand efforts to use patient data forthe purposes of safety improve-ment, and how these conflicts maybe resolved.
Although this report is the work ofthe project’s principal investigator,not a statement of consensus, it drawsfrom the insights of the interdiscipli-nary group of experts convened byThe Hastings Center to make sense ofthe complex phenomenon of patientsafety reform. Working group mem-bers brought their experience as peo-ple who had suffered from devastat-ing medical harms and as institution-al leaders galvanized to reform bytragic events in their own health careinstitutions. They brought expertiseas clinicians, chaplains, and risk man-agers working to deliver health care,confront its problems, and make itsafer for patients. They brought fa-miliarity with the systems thinkingdeployed in air traffic control and inthe military. And they brought criticalinsight from medical history and soci-ology, economics, health care pur-chasing, health policy, law, philoso-phy, and religious studies.
The research project was madepossible through a major grant fromthe Patrick and Catherine WeldonDonaghue Medical Research Founda-tion.
S2 July-August 2003 / HASTINGS CENTER REPORT
AN OVERVIEW OF THE PROJECT
On the cover: Hospital, by Frank Moore,1992. Oil on wood with frame and attach-ments. 49” x 58” overall. Private Collection,Italy. Courtesy Sperone Westwater, NewYork.

The Institute of Medicine report is a publicpolicy document. That is, it proposes theneed for government intervention to address
a problem of serious concern to public health andhealth care financing. Although there was an imme-diate flurry of resistance to the report’s statistics on
the number of deaths associated with preventablemedical error—a key premise in the argument es-tablishing the scope and significance of the prob-lem—these challenges have been effectively silencedby the preponderance of evidence that the rate ofharmful medical error, with its enormous humanand financial consequences in death, disability, lostincome, lost household production, and health carecosts, is unacceptable.
S3SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
by Virginia A. Sharpe
PROMOTING PATIENT SAFETY
Virginia A. Sharpe, “Promoting Patient Safety: An Ethical Basis forPolicy Deliberation,” Hastings Center Report Special Supplement 33,No. 5 (2003), S1-S20.
Over the last three years, patient safety and
the reduction of medical error have come
to the fore as significant and pressing mat-
ters for policy reform in U.S. health care. In 2000,
the Institute of Medicine’s report, To Err Is Human:
Building a Safer Health System presented the most
comprehensive set of public policy recommendations
on medical error and patient safety ever to have been
proposed in the United States.1 Prompted by three
large insurance industry-sponsored studies on the
frequency and severity of preventable adverse events,
as well as by a host of media reports on harmful med-
ical errors, the report offered an array of proposals to
address at the policy level what is being identified as a
new “vital statistic,” namely that as many as 98,000
Americans die each year as a result of medical
error—a figure higher than deaths due to motor ve-
hicle accidents, breast cancer, or AIDS. And this fig-
ure does not include those medical harms that are se-
rious but non-fatal.
The IOM recommendations resulted in a surge of
media attention on the issue of medical error and
swift bipartisan action by President Clinton and the
106th and then the 107th Congress. Shortly after the
report was issued, President Clinton lent his full sup-
port to efforts aimed at reducing medical error by 50
percent over five years. In Congress, the report
prompted hearings and the introduction of a host of
bills including the SAFE (Stop All Frequent Errors)
Act of 2000 (S. 2378), the “Medication Errors Re-
duction Act of 2001” (S. 824 and H.R. 3292), and,
recently, the “Patient Safety and Quality Improve-
ment Act of 2002” (S. 2590) and the “Patient Safety
Improvement Act of 2002” (H.R. 4889). Although
none of these bills has made it into law, each repre-
sents ongoing debate about the recommendations in
the IOM report.
Since the IOM recommendations have been ei-
ther a catalyst or a touchstone for all subsequent pa-
tient safety reform proposals—whether by regulation
or by institutions hoping to escape regulatory man-
dates—they must be part of the context of any poli-
cy-relevant discussion of the ethical basis of patient
safety.
The Institute of Medicine Report

S4 September-October 2003 / HASTINGS CENTER REPORT
The report observes that health care has lagged behindother industries in safety and error prevention in part be-cause, unlike aviation or occupational safety, medicine hasno designated agency to set and communicate priorities orto reward performance for safety. As a result, the IOM’skeystone recommendation is the establishment of a centerfor patient safety to be housed at the Agency for HealthCare Quality and Research under the auspices of the De-partment of Health and Human Services. The center’scharge is to set and oversee national goals for patient safe-ty. In order to track national and institutional perfor-mance, and to hold institutions accountable for harm, theIOM also proposes mandatory, public, standardized re-porting of serious adverse events. In addition to mandato-ry reporting, the IOM advocates efforts to encourage vol-untary reporting. To motivate participation in a voluntaryreporting system, the IOM recommends legislation to ex-tend peer review protections, that is, confidentiality, todata collected in health care quality improvement andsafety efforts.
To complement the national initiative, the IOM rec-ommends that patient safety be included as a performancemeasure for individual and institutional health careproviders and that institutions and professional societiescommit themselves to sustained, formal attention to con-tinuous improvement on patient safety. Finally, regardingmedication safety, the IOM recommends that the FDAand health care organizations pay more attention to iden-tifying and addressing latent errors in the production, dis-tribution, and use of drugs and devices.
A unifying theme in the report is the role that systemsplay in the occurrence of medical mistakes. Over the lastfew decades, research conducted on error in medicine andother high-risk, high-variability industries has revealedthat most quality failures in these industries result notfrom poor, incompetent, or purposefully harmful individ-ual performance but from the very complexity of systems.In the hospital setting, systems of drug dissemination orinfection control, for example, can be designed either toprevent or to facilitate error by individual providers. Rec-ognizing the system dimensions of the problem, the IOMrecommendations promote human factors research—which examines the interface between humans and ma-chines in complex work environments—to get at the rootcauses of error and adverse events. The report encouragesnon-punitive, voluntary reporting as an essential ingredi-ent in understanding lesser injuries and “near misses”—that is, those errors that have the potential to cause harm,but have not yet caused harm.
Although the IOM acknowledges the role that profes-sional ethics and norms play in motivating health carequality, it bases its recommendations on the premise that
internal motivations are insufficient to assure quality andpatient safety consistently throughout the health care sys-tem. Thus, the IOM’s aim is to create external regulatoryand economic structures that will create both a level play-ing field and “sufficient pressure to make errors so cost-ly…that [health care] organizations must take action.”2
Given its aims as a comprehensive policy document, itis understandable that the IOM places only minimal em-phasis on professional norms or the moral motivation ofhealth care providers as the principal catalyst for change.The scope of the change proposed requires a uniform setof incentives and accountabilities. Further, if systemsrather than individuals are the most appropriate targets forimprovement, then appeals to individual virtue wouldseem to be the wrong focus. We will come back to the re-lationship between individuals and systems, but, for themoment, it is enough to point out that the role of ethicsin public policy goes well beyond the question of moralmotivation. Ethics also plays an essential role in the justifi-cation of public policy and the critique of policies alreadyin place.
Underlying all public policy deliberations are specificsocial values and assumptions about how these valuesshould be weighed and balanced or prioritized. In order tounderstand and assess the legitimacy of proposed policiesin a democratic society, therefore, those underlying valuesand assumptions can be made explicit and subject to crit-ical appraisal.
This report takes up this large task. It begins by eluci-dating the ethical values and concepts underlying theIOM recommendations. The central sections of the reportare devoted to a careful unpackaging of the notion of ac-countability. The report argues that accountability re-quires a sophisticated understanding of the causal expla-nation for errors—an account of errors not merely ascauses of harm but as themselves caused by complex sys-tems. The notion of accountability itself can also be expli-cated in different ways; this report argues that account-ability should be understood not merely in a retrospectiveand fundamentally retributive way, but also in a foreword-looking or prospective sense oriented to the deliberativeand practical processes involved in setting and meetinggoals—such as improved patient safety. Both senses of ac-countability must be borne in mind in assessing the prosand cons of the different possible ways of compensatingpatients for adverse events. The demands of justice andsafety improvement, which sometimes conflict and mustbe balanced against each other, argue for compensationschemes based on no-fault liability or mediation. Tradi-tional tort liability is the worst way of achieving these twogoals.

S5SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
Ethical Values and Issues at Stake in Proposed Patient Safety Reforms
Patient Safety
Do No Harm.” The guiding value of patient safety canbe understood to derive from two longstanding prin-
ciples of health care ethics: beneficence, the positive oblig-ation to prevent and remove harm, and nonmaleficence,the negative obligation to refrain from inflicting harm. Asfar as medical error is concerned, the principle of benefi-cence establishes a moral argument against errors of omis-sion such as a misdiagnosis or failure to provide requiredtreatments. The principle of nonmaleficence establishes anargument against errors of commission, such as surgicalslips, drug administration to the wrong patient, or thetransmission of nosocomial infection. Together, these twoprinciples constitute the obligation to “do no harm.”3
Traditionally, the relationship between the clinicianand the patient has been regarded as a fiduciary relation-ship. That is, the power disparity between doctor and pa-tient, the patient’s vulnerability, and the doctor’s offer tohelp are understood to place special obligations on healthcare providers, as professionals, to promote a patient’shealth interests, to respect the patient’s autonomy, and tohold his or her good “in trust.”4
Medical error and injury happens to an identifiable in-dividual. From the point of view of fiduciary ethics, thatis, professionalism, the individual patient is the focus ofthe obligation to do no harm.5 This patient-centered focusis acknowledged by the IOM in its definition of safety as“freedom from accidental injury.” This definition, says thereport, “recognizes that this is the primary safety goal fromthe patient’s perspective.”6
The principle of utility. The goal of patient safety can alsobe justified by the principle of utility, understood in thesimplest terms as the achievement of the greatest good forthe greatest number or the net aggregate benefit across apopulation. For example, policy recommendations areaimed at patient safety as a public health problem—aproblem requiring strategies to improve overall safety inthe health care system. As such, they are based on theprinciple of utility. From the point of view of publichealth ethics, the patient population in the aggregate is thenormative focus, and safety improvements are measuredin terms of population-based or epidemiologic statisticssuch as the IOM’s target goal of a “fifty percent reductionin errors over five years.”7
The value of patient safety is also understood to derivefrom its economic utility. As the IOM report states on thesecond page of its executive summary, the total nationalcost of preventable medical error is between seventeen andtwenty-nine billion dollars a year. The assumption behindthe report’s recommendations is that efforts to reduce
error by the target of 50 percent over five years will be jus-tified by the reduction of associated costs.
Utilitarian and fiduciary justifications for patient safetycan come into tension. For example, although it is possi-ble that the incentive to reduce the extra costs associatedwith preventable error will coincide with the imperative toprotect patients from harmful outcomes, such a coinci-dence is by no means assured. One can easily imagine acost-conscious hospital deciding against certain strategiesto improve safety because the up-front costs are prohibi-tive. Likewise, without a clear prioritization of the fiducia-ry justification for safety—which gives priority to patientwelfare as a policy objective—it is easy to imagine safetyproposals being reduced to their economic value. Undersuch circumstances, policy makers might suppose thateconomic considerations alone will justify certain safetytrade-offs.8
One of the biggest ethical challenges for patient safetyreform will be in confronting the fact that strategies to im-prove overall patient safety have the potential to compro-mise obligations to individual patients. For example, theIOM recommends mandatory reporting of serious adverseevents and voluntary reporting of lesser harms and nearmisses. To the extent that institutions direct their resourcesto meeting the standards for mandatory reporting, theymay de-emphasize voluntary reporting and the follow-upnecessitated by it. This could have the paradoxical effect ofmaking safety improvement activities contingent on a pa-tient having been seriously harmed.
Accountability
To appreciate fully what is at stake here, we need tograpple with the complex issue of accountability. Ac-
countability for harmful medical error is expressed in theIOM’s call for a nationwide mandatory system for report-ing serious adverse events and in its call for performancestandards on patient safety and quality improvement forhealth care organizations.9 Accountability is grounded, inthe report, in the public’s right to know about and be pro-tected from hazards. It also derives from the principle offairness.
From a regulatory perspective, hazards in the healthcare setting are matters of public safety. The IOM’s rec-ommendations regarding mandatory reporting are de-signed to generate standardized information that can beused to understand and track known hazards and to takepreventive action. As the report states: “The public has theright to expect health care organizations to respond to ev-idence of safety hazards by taking whatever steps are nec-essary to make it difficult or impossible for a similar event

to occur in the future. The public also has a right to be in-formed about unsafe conditions.”10
The principle of fairness operates on two levels in themandatory reporting proposal. First, mandatory reportingis intended to level the playing field for health care insti-tutions so that none is exempt from data collection onsafety, or from penalties or civil liability in the case of se-rious patient harms. Second, mandatory reporting tooversight bodies is intended to provide an avenue forharmed patients to gain access to information regardingthe circumstances surrounding an injury and use it to seekjustice for negligent harm associated with care.11
Although a number of states currently mandate exter-nal reporting of serious adverse events—usually to thestate health department—in most cases the informationcollected is intended to be protected by law from poten-tial claimants.12 Many state programs fail to provide pub-lic access to the information and most require subpoenaor court order for release of information. By contrast, theIOM proposes meaningful public access to informationabout serious harms; it states that “requests by providersfor confidentiality and protection from liability seem in-appropriate in this context.”13
A conceptual distinction between reporting and disclo-sure is important. Reporting refers to the provision of in-formation to oversight bodies such as state agencies, or theproposed Center for Patient Safety. Disclosure, by con-trast, refers to the provision of information to patients andtheir families. It is important to point out that the IOM’semphasis on accountability and the public’s right to knowin the context of mandatory reporting have nothing to dowith active disclosure of information by health care insti-tutions to harmed parties. Although the mandatory re-porting of serious or fatal adverse events would, in princi-ple, trigger meaningful investigation and administrativeaction, it does not automatically direct that informationto the patients who have been harmed. The “right toknow” invoked by the IOM, is thus not an endorsementof the individual’s right to know or of the obligation of re-spect for the autonomy of individuals. In this way, theIOM’s understanding of accountability is extremely nar-row and points up one of the ways in which a publichealth or safety approach overlooks obligations to specificindividuals.
Although it is not a feature of the IOM’s recommen-dations, the need for disclosure, understood as a primafacie obligation of professionalism,14 is being addressed onother fronts in the patient safety movement. For example,in 2001, the JCAHO put into effect a disclosure standardthat requires hospitals and physicians to inform patients(and families) about “unanticipated outcomes” associatedwith their care.15 This requirement is included in theJCAHO’s Patient Right’s and Organizational Ethics stan-dards. Likewise, a number of forward-looking health careinstitutions, such as the Veterans Affairs (VA) MedicalCenter in Lexington, Kentucky,16 have embraced disclo-
sure as an institutional obligation that has the added ad-vantage, from a consequentialist point of view, of not re-sulting in a negative financial impact on the hospital. AsSteve Kraman of the Lexington VA hospital says, “Wedidn’t start doing this to try to limit payments; we did itbecause we decided we weren’t going to sit on or hide ev-idence that we had harmed a patient just because the pa-tient didn’t know it. . . .We started doing it because it wasthe right thing to do, and after a decade of doing it decid-ed to look back to see what the experience had been. Theindication that it’s costing us less money was really unex-pected.”17 Implicit in Kraman’s remark is an endorsementof disclosure as an obligation of professionalism, as “theright thing to do.”
The IOM also calls for accountability of health care in-stitutions to performance standards regarding continuousimprovement in safety and quality. The emphasis here ison pressure that will be applied by regulators, accreditors,and purchasers to evaluate and compare hospitals accord-ing to their demonstrated commitment to safety. Givenits public policy focus, the IOM report focuses on ac-countability of organizations, not of individuals. If we lookat the history of medicine, however, we see that it is indi-viduals—specifically physicians—who have historicallybeen regarded as the locus of health care quality and whohave been held responsible for it.18
These assumptions have shaped medical culture to theextent that a rethinking of accountability must be centralto the “culture change” that is the rallying cry of reform.If, as safety experts both within and outside medicinemaintain,19 it is flaws in a system, rather than in individ-ual character or performance, that produce the vast ma-jority of preventable errors—a premise this essay ac-cepts—then the dominant strategy of blaming individualswill continue to be ineffectual and counterproductive inimproving safety. This point was made early by leaders ofthe patient safety movement: “A new understanding of ac-countability that moves beyond blaming individualswhen they make mistakes must be established if progressis to be made.”20 The dynamic between institutional andindividual accountability is one of the most importantand complex issues at the heart of patient safety reform.We analyze this concept and its practical implications laterin this essay.
Confidentiality
In addition to its recommendations regarding a nation-wide mandatory reporting system, the IOM also rec-
ommends that voluntary, confidential reporting systemsbe implemented within health care institutions and en-couraged through accrediting bodies. In this context, con-fidentiality refers specifically to the restriction of publicaccess to information on the quality and safety of healthcare delivery—also known as “peer review protection.”Ordinarily, when we speak of “confidentiality” in health
S6 September-October 2003 / HASTINGS CENTER REPORT

S7SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
care we are referring to the confidentiality of patient in-formation and restricted access to that information exceptby patient consent.21 Such systems, many of which are al-ready in place in health care and other high-risk indus-tries, are essential to safety improvement efforts, insofar asthey can encourage providers to supply information need-ed to identify and take action to address hazardous condi-tions. As many observers of high-risk industries havenoted, it is the information about near misses that pro-vides the richest resource for safety improvement efforts.22
In its distinction between thresholds for mandatory andvoluntary reporting, the IOM combines, under the vol-untary reporting system, near misses and errors that havecaused minor or moderate injuries.
In order for voluntary reporting to be workable, theIOM states, providers need to be assured that the infor-mation they report will not be used against them in thecontext of malpractice litigation. As such, the IOM rec-ommends that “Congress pass legislation to extend peerreview protections to data related to patient safety andquality improvement that are. . . collected or shared withothers solely for purposes of improving safety and quali-ty.” Although the guarantee of secrecy has a political pur-pose (to gain participation from clinicians who wouldotherwise fear exposure to liability), from an ethical pointof view, the guarantee of peer protection is justified by theprinciple of utility. A reduction in harmful errors acrossthe patient population can be achieved only if front-linehealth care professionals are willing to supply informationregarding specific health care delivery problems. The freeflow of this information to create an epidemiology oferror can occur only if secrecy regarding the informationis assured.
As recommended, this proposal has been introducedinto legislation under the “Patient Safety and Quality Im-provement Act,” introduced into the Senate 5 June 2002,and the Patient Safety Improvement Act of 2002, intro-duced into the House 6 June 2002. According to the bills,all information collected for the purpose of patient safetyand quality improvement will be confidential and pro-
tected from subpoena, legal discovery, Freedom of Infor-mation Act requests, and other potential disclosures.23
There are a number of ethical problems with this ap-proach. First, the proposed legislation allows informationabout adverse medical events (which it calls “lesser in-juries”) to be concealed from harmed parties. It is notclear how the legislation squares with accreditation re-quirements for disclosure that are mandated by theJCAHO or that may be part of a hospital’s institutionalpolicy. Second, peer review protections formalize and re-inforce the conflict between the provider’s interest in self-protection and patients’ legitimate interest in informationabout their care. In so doing, the restriction of access toinformation about adverse events undercuts fiduciaryobligations and patients’ right to know about informationpertinent to their care. Third, the enhancement of peerreview protection is premised on the assumption of thestatus quo with regard to the current malpractice system.Peer review protection is made to do all of the heavy lift-ing to circumvent what Troyen Brennan has called the“the dead weight of the litigation system.”24 Brennan iscritical of the IOM recommendations and other reformproposals that fail to address the ways in which the cur-rent malpractice system is ethically and practically coun-terproductive as a response to medical harms. The struc-tures and incentives of the tort system are inconsistentwith accountability for truth telling, and safety improve-ment (a point taken up again below).25
As we have pointed out, the notion of accountability iscentral to patient safety reform. It guides our expectationsand judgments regarding the performance of health careproviders. More challenging, the causal story now beingtold about medical errors from the systems perspectivefundamentally challenges those conventional expectationsand judgments; that is, the assumption of individual ac-countability that forms the fabric of medicine and law.So, in order to hold health care providers accountableunder a systems approach, we have to reinvent not onlyour understanding of accountability, but also the struc-tures of accountability institutionalized in our legal andcultural approaches to medical error.

S8 September-October 2003 / HASTINGS CENTER REPORT
Rethinking Accountability
Getting clear on the notion of accountability re-quires that we sort out and appraise two differentcausal explanations for medical error. Further, in
examining one of these explanations—the story of com-plex causation in a systems approach to error—we willneed to dstinguish between two different senses of ac-countability—a backward-looking sense and a forward-looking sense—and consider the implications of each forboth how we compensate those who have been harmedand for safety improvement.
Two Causal Stories
With the emergence of the systems approach to pa-tient safety, a paradigm shift has occurred in the
causal story of why errors occur and how they can be pre-vented. According to the conventional story, medicalerror, and specifically harmful medical error, is the resultof individual actors and their individual actions—the slipof a scalpel, a wrong diagnosis, a failure to wash one’shands, the failure to check a hematocrit. As far as respon-sibility for such errors is concerned, the earliest moderncodes of medical ethics by Thomas Percival in 1803 andby the AMA in 1847, state that the doctor’s conscience isthe “only tribunal” and his responsibility is to learn fromhis mistake and to make sure it does not recur.26 As Ken-neth De Ville has observed, after the late 1800s, whenmedical malpractice emerged as a new public “tribunal,”this causal story became the basis for negligence claimsagainst physicians.27 Tort law remains the dominant nar-rative of responsibility in the arena of medical error, and itoperates on the basis of a notion of simple causation. Pooror unsafe care is attributable to the actions or inactions ofindividual health care providers who are cast as “bad ap-ples.”28 The shadow of liability reflects and reinforces a“shame and blame culture” within which people hide theirmistakes.
Starting about four decades ago, W. Edwards Demingand J.M. Juran’s work in human factors research and in-dustrial engineering, Charles Perrow’s book Normal Acci-dents, and James Reason’s Human Error, all offered a newcausal story about quality and quality failure. That story,which has been told in the medical context by DonaldBerwick, Lucien Leape, and the National Patient SafetyFoundation,29 among others, is that human error shouldnot be regarded narrowly as the cause of harm; it shouldbe regarded as the effect of complex causation. Why? Be-cause the majority of errors do not produce harm, butthey have the potential to reveal latent errors or potential-ly harmful failures within a complex system. Unless welook in greater detail at the causal web, we will be ignorant
of the weaknesses in the system and powerless to preventtheir causing future harm.
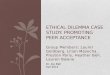
The lesson of human factors research and cognitivepsychology is that to understand error causation it is notenough to examine one’s own actions or to look for the“smoking gun” or proximate cause of the active error; wemust also examine the interrelationships between humans,technology, and the environment in which we work.30 Ap-plying this research to accidents involving the leaking ofradioactive material at Three Mile Island and the explo-sion of the space shuttle Challenger, psychologist JamesReason determined that most accidents were caused bymismatches between the design of complex systems andthe ways humans process information. In the medicalcontext, a system failure in drug administration, for exam-ple, might involve look-alike packaging or sound-alikedrug names—situations that are literally “accidents wait-ing to happen.”
According to safety experts in aerospace, atomic energy,and other complex, technology-based industries, the mostconstructive approach to error reduction is the creation ofa blame-free environment that sees every error as “a trea-sure.”31 There are at least two justifications for this coun-terintuitive approach to responsibility or accountability(which for the purposes of this report are interchangeableterms). The first is, again, that error-prevention dependson information that will be forthcoming only if individu-als feel free enough from liability concerns to provide it.The second is based on the principle of justice. As Merryand McCall Smith point out in their book Errors, Medi-cine, and the Law, errors are by definition exculpatory be-cause they are involuntary.32 So, holding individuals re-sponsible for errors is wrong on two counts. First, a trueaccident, whether it is an act or an omission, is not blame-worthy because it is not intentional, and its result was ei-ther unforeseeable or could not have reasonably been pre-vented. Second, most errors cannot be causally attributedsolely to an individual actor.
“Don’t Blame Me, It Was a System Problem”
This new causal story has understandably given rise toa number of concerns about accountability for harm-
ful mistakes.The first worry is that a systems explanation gives peo-
ple permission to pass the buck by saying that their ownactions were so controlled by “the system” that they sim-ply were not free to do otherwise. In this sense, appeals tothe “system” provide a convenient pretext for moral shirk-ers. In its most extreme form, this is the problem of freewill and determinism in a new context. Appealing to the“system” in the broadest metaphysical sense, one’s actions

are seen to be determined by forces outside of all humanagency. Responsibility is located outside the individualactor. But this sort of defense against responsibility is notreally plausible in the case of health care practitioners,whose self-understanding includes the ability to influencethe course of illness. As long as freedom of the will pro-vides one of the guiding justifications of their work, theycannot also reject it whenever they make a mistake. Thatsaid, however, the literature on the history and sociologyof medical law indicates that a fatalistic belief in divineprovidence was one of the key exculpating factors in med-ical harm until the early nineteenth century and that itcontinues to be an important, if sometimes disingenuousone today.33 In her book Wrongful Death, Sandra Gilbert,whose husband died as the result of a medical error, re-counts a story about the benefactor of a Catholic hospitalwhose wife’s doctors repeatedly assured him that it was“God’s will” that she was comatose and later died afterroutine surgery. Her husband sued to find out what every-one had “known all along,” namely, that the patient’scoma was the result of an identifiable error.34
A related worry about a systems approach is the “Dil-bert problem.” Unlike the metaphysical problem of deter-minism that implicates the human condition, the “Dil-bert problem” implicates the conditions under which hu-mans work and is implicit in the problem of learned help-lessness.35 The worry is that the systems approach so min-
imizes the role of individualagency that it will choke off themotivation to sustain high-quality performance, encouragepoor performance, and lead toan erosion of the trustworthi-ness of health professionals.36
This worry is based on theassumption that individual ac-tors are morally and practicallydisempowered within such asystem, or that individuals can
step “outside” a system and claim moral immunity. As weshall see, however, the kind of responsibility envisionedwithin the systems approach is based on the empower-ment of individuals to contribute to system improvement.
Another, more practical concern about the systems ap-proach to medical error is that it will make assigning re-sponsibility for preventable adverse events difficult if notimpossible. This worry about the loss of an identifiabletarget of blame is fostered, in part, by the very human de-sire for vengeance.37 The invocation of a “system” rendersfaceless and anonymous the perpetrator of harm, and vic-tims are left powerless. Also at play here is the assumptionthat justice to harmed parties requires being able to pointto a wrongdoer. This is an assumption fostered by the ev-identiary requirements of malpractice, which link com-pensable negligence to an identifiable lapse in the stan-dard of care. If a wrongdoer is able to take refuge in the“system,” then harmed parties may be denied access tocompensation.
This concern is directly linked to a worry that thepractical demands of the systems approach—that is, theneed to collect information about errors and adverseevents—will be possible only at the expense of the pa-tient’s right to know. If protections against subpoena andlegal discovery are extended to information regardingharmful quality failures, then accountability to individu-
S9SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
Local triggers, intimate defects,atypical conditions
Defense-in-depth
Latentfailures atthe manageriallevels
Trajectory ofaccident opportunity
Source: James Reason, Human Error (Cambridge University Press, 1990), p. 208. Reprinted with permission.
n The Dynamics of Accident Causation n

S10 September-October 2003 / HASTINGS CENTER REPORT
als will be subordinated to the ostensible aims of safetyimprovement.
Two Notions of Accountability
We may allay both these speculative and practicalconcerns by distinguishing two different ways in
which we think about accountability. Ascribing responsi-bility depends for its sense on the purposes or ends towhich we put it and the information that we take or donot take to be directly relevant. Put differently, when wetalk about responsibility we need to be clear not onlyabout the information that we take to be relevant, or not,but also about what we hope to accomplish in assigningresponsibility. With that in mind, we can make a distinc-tion between two types of responsibility ascription: re-sponsibility in the backward-looking or retrospective sense,and responsibility in the forward-looking or prospectivesense.38
In the backward-looking sense, responsibility is linkedto practices of praising and blaming and is typically cap-tured in expressions such as “she was responsible forharming the patient” or “he made a mistake and heshould be held responsible for it.” When we speak of“holding someone accountable” we tend to be using thisphrase after some action has gone awry.
The forward-looking or prospective sense of responsi-bility is linked to goal-setting and moral deliberation. It isexpressed in phrases such as “as parents, we are responsi-ble for the welfare of our child,” or “democratic citizen-ship involves both rights and responsibilities.” Responsi-bility in this sense is about the particular roles that a per-son may occupy, the obligations they entail, and howthose obligations are best fulfilled. But whereas responsi-bility in the retrospective sense focuses on outcomes,prospective responsibility is oriented to the deliberativeand practical processes involved in setting and meetinggoals.39
Currently, the dominant view of responsibility regard-ing medical error is grounded in tort liability, that is, mal-practice. The aim of responsibility ascription in this con-text is compensation to harmed parties and deterrence offurther malpractice. Through the lens of malpractice,error is germane only as the cause of harm, and informa-tion about errors that do not cause harm is irrelevant. Re-sponsibility ascription in this context is retrospective; itspoint is the assignment of blame.
A systems approach to error emphasizes responsibilityin the prospective sense. It is taken for granted that errorswill occur in complex, high-risk environments, and par-ticipants in that system are responsible for active, com-mitted attention to that fact. Responsibility takes theform of preventive steps to design for safety, to improveon poor system design, to provide information about po-tential problems, to investigate causes, and to create anenvironment where it is safe to discuss and analyze error.
Although there is much disagreement in the medicalethics literature about the source of moral norms in med-icine,40 it is generally accepted that, at minimum, healthcare is guided by the imperative “to help, or at least to dono harm.”41 Traditionally, this role responsibility has beenassociated exclusively with clinicians—those who have adirect relationship with patients. In part, this stems fromthe historical origins of healing, which until the emer-gence of the modern hospital was the domain largely ofsolitary practitioners. It also reflects the ethical standardsestablished to legitimate professional self-regulation.Given the complexity in the dimensions both of the fi-nancing and the delivery of today’s health care system inthe United States, a strong case can be made that this roleresponsibility should also be extended to those who haveindirect but significant control over decisionmaking thataffects patient welfare. This includes health care managersand administrators who have not traditionally been heldaccountable to standards of medical professionalism.
Since prospective responsibility is linked to practicesand roles, it applies to collectives as well as to individuals.To the extent that a group of people contributes to a prac-tice and the goals that define it, they can be said to have“collective responsibility”—in the prospective sense. Inhealth care, helping and avoiding harm is one of the pri-mary bases on which physicians, nurses, and other healthcare providers find solidarity in their work. Collective re-sponsibility in this uncontroversial sense has been largelyoverlooked because, like most discussions of responsibili-ty in the philosophical and legal literature, discussions ofcollective responsibility have focused almost exclusivelyon the retrospective question of blame and whether andhow collectives can properly be held accountable forharmful events.42
An emphasis on prospective responsibility is helpfulbecause it forces us to re-examine, in light of the com-plexities of institutionally delivered health care, the con-tent and scope of responsibility. This is something wehave lost sight of in our narrow reliance on the malprac-tice paradigm as an explanatory framework for medicalerror. We need new structures to account for what wenow know about the occurrence of error in complex sys-tems.
In the context of health care delivery, the aim ofprospective responsibility ascription is to orient everyonewho has an effect on patient care (including clinicians,health care administrators, hospital managers and boards,technicians, computer data specialists) toward safety im-provement. Through the lens of patient safety, error isgermane as an indicator of vulnerabilities in a system andas an opportunity to prevent harm. The point of forward-looking responsibility ascription is to specify the obliga-tions entailed in creating a safer health care environment.Given a systems approach to error, these obligations entaila high degree of transparency about errors, analysis of er-rors to determine their causes, and the implementation of

systemic improvements. To the extent that current struc-tures prevent health care providers from meeting these re-sponsibilities, the structures are inconsistent with theethics of professionalism.
But what is the patient’s own responsibility for safety?If, as Leape and others have argued, a system is “an inter-dependent group of items, people or processes with acommon purpose,”43 and responsibility in the prospectivesense belongs to all who contribute to the healing enter-prise, isn’t it reasonable to include patients in this collec-tive?
For some, the suggestion is offensive because it can veryeasily shade into blaming the victim. If the patient is re-sponsible for assuring safety, and she does not ask about amedication she knows to be unfamiliar, will we say thatshe somehow failed?44 On the other hand, if patients sup-ply information and insights essential to their care—andindeed they must provide information regarding their his-tory—then should they not be considered as members ofthe team?
We can all agree that patients are de facto central totheir care. The sticking point is whether this centrality im-plies that they are morally responsible for the safety orquality of their health care.45 Unlike clinicians and otherswho deliver health care, patients have not committedthemselves to the practice of health care delivery and thegoals that define it. Most people do not freely choose tobecome patients. That said, the rise of the patient advoca-cy movement has been based on the call for patients to be-come more active in their care. Patient safety advocateRoxanne Goeltz, whose brother Mike died as a result of amedical error, has argued forcefully that patients and theirfamilies should take active measures to assure that theircare is delivered safely. This includes having a friend orfamily with the hospitalized patient twenty-four hours aday, seven days a week.46 Bryan Liang has also argued that
patients are responsible at least for supplying health careproviders with personal information that is as completeand accurate as possible.47
An axiom of responsibility ascription is “ought impliescan.” In order to say that someone is responsible, he or shehas to be in a position to act on that obligation. In the caseof patients, taking responsibility for the quality or safety oftheir care will often be out of the question. For those pa-tients who can be actively involved, their positive contri-bution to their health care delivery should be facilitatedand commended, but required only in the provision of in-formation that is as accurate and complete as possible andin following, as much as possible, the treatment regimen.The onus of responsibility for patient involvement is oninstitutional and individual health care providers.48 Re-spect for patient self-determination requires that providersinvolve patients in their care, and the lessons of safety im-provement indicate that including patients (or their fami-lies) as members of the health care team (by asking themto confirm their surgical site, by paying attention to theirreports on themselves) may be one of the most effectiveand commonsensical ways of improving care.
If we find that most preventable harms are caused bycomplex factors involving latent failures at the manageriallevel, system defects, unsafe acts, and psychological pre-cursors, and if we agree that an essential moral responsi-bility of health care providers is “to help or at least to dono harm,” then meeting that responsibility will requireconditions under which these causal factors can bebrought to light, assessed, and improved. Currently, thesystem of liability for medical harms makes meeting thatresponsibility possible only through exceptional acts ofcourage.49 Likewise, it makes respect for patients throughdisclosure almost impossible because it discourages hon-esty and openness on the part of health care professionals.
S11SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation

Prospective accountability means creating safe condi-tions for patient care. Retrospective accountabilitymeans achieving justice for harmed parties. As a pol-
icy matter, both forms of accountability must be under-stood in light of the ethical pros and cons of compensationschemes for adverse patient outcomes: tort liability, no-fault liability, and mediation. No-fault and mediationseem likeliest to meet the demands of justice without in-hibiting safety improvement. Traditional tort liability isthe least ethically viable means of achieving these twogoals, although it is the most deeply entrenched system,politically speaking.
Tort Liability
Tort liability is a fault-based system of compensationfor those who sustain injury as a result of their med-
ical care. To qualify for payment, the injured party mustprove that his or her injury was the result of negligence onthe part of the health care provider. A second goal of tortliability is deterrence. The expectation is that the threat oflegal action will keep providers from straying from stan-dards of due care.
As David Studdert, Edward Dauer, and Bryan Liangeach argue, tort liability not only fails in respect of bothcompensation and deterrence, but also inhibits safety im-provement.50 They point out that malpractice law fallsshort in at least six ways. First, it is a haphazard compen-sation mechanism. According to findings from the Har-vard Medical Practice Study, one of the largest insuranceindustry-sponsored studies of medical error, only one inseven patients who are negligently harmed ever gain accessto the malpractice system, with those who are older andpoorer disproportionately excluded from access.51 Forthose patients who do sue, the severity of the injury ap-pears to be a more powerful predictor of compensationthan the fact of negligence.52 And because of that, physi-cians believe that liability correlates not with the quality ofthe care they provide, but with outcomes over which theyhave little control. As a result, “risk management” has be-come an effort to avoid liability rather than error.
A second problem with malpractice law is that it deliv-ers compensation inefficiently. Administrative costs ac-count for more than 50 percent of total system costs,53 anda successful plaintiff recoups only one dollar of every$2.50 spent in legal and processing costs.54 Third, mal-practice claims offer only a monetary outcome, ignoringthe harmed party’s need for noneconomic remediation,such as a guarantee of corrective action, an apology, or anexpression of regret and concern. Fourth, the negligencestandard, because it is embedded in an adversarial process,is inconsistent with attempts to learn from errors and im-
prove quality. Malpractice claims, including pre-trial dis-covery, are shrouded in secrecy, with legal rules governingdisclosure and protection of information. This means thatinstitutions and individual providers typically forego op-portunities to learn from the problems that lawsuits cansometimes help illuminate.
Fifth, as Dauer points out, the adversarial process isbased on the belief that the presentation of relentless, one-sided arguments to an impartial judge or jury is the bestway to discern the truth. This process necessarily rules outthe prospect of collectively analyzing information to dis-cern what happened. The malpractice system thus “exter-nalizes” responsibility for truth by selectively taking infor-mation out of the hands of involved parties—a processthat is emotionally brutal for patients and families tryingto reconstruct their lives after medical harm.55 Finally, re-garding its deterrence function, evidence indicates thatmalpractice stimulates defensive medicine rather thanhigh quality care,56 and that the stress and isolation thatphysicians experience while subject to malpractice claimscan impair their performance.57
These shortcomings reveal the moral flaws of tort lia-bility. With regard to the claims of justice, tort system failsto deliver compensation in a fair and timely way toharmed parties. Those with lesser claims are kept out of aprohibitively expensive malpractice system; those who arecompensated may spend years obtaining this result; thosewho are old and poor may be excluded from the system al-together. For Sandra Gilbert, who settled under the shad-ow of malpractice, the adversarial process guaranteed thatthe plaintiffs would never know the case’s full details andwould never receive an apology or recognition from thedefendant. The tort system creates incentives against truthtelling on the part of health care providers. Also, with re-gard to justice for clinicians, the tort system overlooks thesystem dimensions of error and thus may unfairly targetindividual providers for acts, omissions, and outcomes forwhich they cannot fairly be held culpable. When it comesto harm prevention, the tort system stifles safety improve-ment, and, by externalizing responsibility for truth, en-genders a defensive rather than a constructive posture to-ward error prevention. Viewed from the perspective ofutility, the tort process is inefficient.
No-Fault Liability
No-fault liability is a compensation scheme that doesnot base the award of damages on proof of provider
fault. As Studdert observes, “to qualify for compensationin these schemes, claimants must still prove that they suf-fered an injury and that it was caused by an accident in aspecific domain, such as the workplace, road, or hospital,
S12 September-October 2003 / HASTINGS CENTER REPORT
Justice

but it is not necessary to demonstrate that the party whocaused the accident acted negligently.”58 No-fault liabilityis consistent with the prospective assignment of responsi-bility. It is predicated on a high risk of hazard in a partic-ular industry and assigns absolute liability in advance re-gardless of contributory fault. In other words, no-fault lia-bility is based on the presumption that harms will occur ina particular setting, and it incorporates provisions forcompensation.
Studdert cites empirical research indicating that no-fault has led to increases in average monetary compensa-tion for injured workers as well as gains in worker safety.Although more evidence will be needed, Studdert andothers are optimistic that similar benefits would be ob-tained by implementing no-fault in health care. No-faulthas a number of potential moral advantages. First, since itsuspends the fault requirement, no-fault could remove in-centives to conceal information, thereby supporting fidu-ciary obligations of disclosure and creating the conditionsfor the collection and analysis of error information. Sec-ond, no-fault could overcome some of the inequities in ac-cess to compensation under malpractice law. Unlike thetort system, which distributes compensation haphazardly,no-fault, as an administrative scheme, could determineremedies in advance and distribute them according to theseverity of injury. One potential problem, however, is inthe calculation of loss. If a person’s loss is determined bythe person’s salary, for example (as it was for victims of theSeptember 11 attacks), then age-based, gender-based, orincome-based inequities could be repeated in a no-faultscheme.
This weakness is also related to the health care financ-ing system that we have in this country. As Haavi Mor-reim points out, countries where no-fault schemes formedical harm have been implemented also offer their citi-zens universal health care coverage and other social welfareprograms, so that ongoing health care and other needs arealready covered and need not be obtained through no-fault compensation.59 Without this and other social wel-fare programs to support the needs of the injured and in-firm, the efficiencies of no-fault will quite likely not be re-alized.
Nonetheless, the potential for no-fault to remove barri-ers to information access both for patients and for safetyimprovement, along with its potential for fairer distribu-tion of compensation, make it a promising context inwhich justice, fiduciary responsibility to patients, and safe-ty improvement can thrive.
Interest-based Mediation
Interest-based mediation is a means of opening directcommunication between parties in a dispute. Its aim is
to address the parties’ actual interests and needs ratherthan the inflated interests and needs evoked by the adver-sarial arrangement of malpractice law. Empirical research
indicates that patients who suffer injury often have non-economic motivations—such as a desire for informationand communication—in bringing a claim.60 Likewise, ithas been argued that what physicians want out of litiga-tion (whether that means winning a malpractice suit or asubsequent defamation claim that they have brought asplaintiff ) is not monetary repair, but repair of reputa-tion.61 Mediation is a means of addressing these interestsin a “restorative” way that is impossible within the contextof traditional tort litigation.
Another potential advantage of mediation is that, al-though it takes place within the existing fault-based sys-tem, its confidentiality is ostensibly assured through statu-tory legal privilege in almost every state.62 Although thedegree to which legal privilege does actually guarantee a“safe harbor” against subsequent litigation has been ques-tioned,63 mediation has the advantage of “internalizing”responsibility for the resolution so that the parties are ableto communicate directly rather than through legal inter-mediaries. As a result, the parties may all benefit from theresolution. Health care providers can avoid a costly law-suit, consequent reporting to the National PractitionerData Bank, and loss of reputation, while patients and fam-ilies can make a human connection following a loss, andpatients can be brought into the peer review process by re-questing follow-up or remedial actions in lieu of or in ad-dition to monetary damages. Although mediation doesnot offer a direct avenue to information collection aboutadverse events and errors, it may create a less adversarialcontext in which safety, rather than money, can be pur-sued as a mutual goal and the patient’s experience can beexplicitly used to improve care.
Mediation can also provide a much-needed contextthat supports truth-telling as an avenue to justice. Patientsare routinely excluded from rituals of forgiveness in themedical context. In Charles Bosk’s description of forgive-ness for the technical and moral errors committed by sur-gical residents,64 analogs of “confession” and “repentance”take place in the “hair shirt” ritual of the morbidity andmortality conference. Here, physicians report to peers andsuperiors on the circumstances surrounding their involve-ment in an adverse event, and forgiveness is conferred bythe superior. A second ritual involves peer support for clin-icians confronting the emotional trauma of harmful er-rors. Absent from all of these contexts is the patient. All ofthese rituals serve important purposes; justice to specificpatients is not one of them.
In her work on religious and cultural perspectives onerror and forgiveness, Nancy Berlinger argues that suchrituals are incomplete.65 In the Jewish and Christian tradi-tions that have helped to shape Western cultural norms,argues Berlinger, the possibility of forgiveness or reconcili-ation in the service of justice to harmed parties—in thiscase, patients—involves repairing one’s relationship withthe patient, not with one’s superordinates or peers. Repair-ing the relationship requires appropriate actions of confes-
S13SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation

sion and repentance. Practices that could be described asconfession in the Jewish and Christian traditions wouldinclude (to list only a few possibilities Berlinger mentions)promptly acknowledging error and disclosing to the pa-tient a cogent and complete narrative of what happened;accepting personal accountability even in cases of systemserror, bearing in mind that some patients may always un-derstand error as an individual rather than a systemic fail-ure; and giving clinicians opportunities to process inci-dents and receive counseling in an environment that isneither punitive nor demoralizing. Practices that could bedescribed as repentance could include (again listing only afew examples) apologizing and expressing remorse to aninjured patient (and allowing oneself to feel remorseful);offering injured patients and family members pastoral careor other counseling services; and covering the cost of treat-ing injuries resulting from error. Berlinger also detailspractices that might promote forgiveness or reconciliation.For example, forgiveness might be promoted by invitingpatients to be part of the hospital’s quality improvementprocess, to allow them, if they wish, to take an active rolein working with clinicians and administrators to create apatient-centered culture of safety by sharing their experi-ences of medical harm and their perspectives on hospitalculture (although injured patients are not to be made tofeel that they ought participate in QI).
Berlinger also notes that forgiveness might be promot-ed by challenging aspects of institutional culture that denythe fallibility, and therefore the humanity, of clinical staff,or that work against truth-telling, accountability, compas-sion, and justice in dealing with medical error and pro-moting patient safety.
It is important to remember that the IOM report in-cludes both errors that cause no harm (near misses) anderrors that cause “lesser injuries” within its recommenda-tion for voluntary reporting.66 The recommendationshould not be regarded as a substitute for the establishedprofessional obligation for disclosure of harmful errors, bethey serious, moderate, or minor. Regardless of the policyrecommendations, the ethical obligation for disclosure ofharmful error stands. The challenge, therefore, will be tocreate a context in which this obligation can be honoreddespite seemingly contradictory policy proposals.
As Berlinger’s recommendations about disclosure makeclear, delivering justice to harmed parties entails the insti-tutionalization of new norms and practices of disclosure.The greater openness potentially afforded by no-fault ormediation and voluntary compensation in the context ofexisting tort liability may provide environments in whichsuch norms and practices can take hold and harmonizewith the long-established fiduciary obligations of disclo-sure.
S14 July-August 2003 / HASTINGS CENTER REPORT

S15SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
The chief premise of a systems approach to error isthat overall safety improvement requires that oldforms of individual interrogation (shame and
blame) be replaced by new forms of “system interroga-tion” (that is, root cause analysis). Another premise of asystems approach is that success depends on the collectionand analysis of information gleaned from real life healthcare delivery. The IOM report recommends that informa-tion about error not associated with serious harm be pro-tected from all uses not connected with safety improve-ment, including uses requiring access to information bysuch methods as subpoena, legal discovery, and the Free-dom of Information Act.
As we have just noted, the recommended protection ofinformation about “lesser harms” is incompatible withprofessional obligations of disclosure. Equally if not moredisturbing, both the IOM recommendations and ensuinglegislation (the “Patient Safety and Quality ImprovementAct” in the Senate, and the “Patient Safety ImprovementAct of 2002” in the House67) make safety improvementcontingent on patients being harmed—even though theharms in question can be of “lesser” severity. The effort toprotect information that is part of a voluntary reportingscheme is a “workaround” in the malpractice status quo. Itpits the value of safety improvement against the values ofnonmaleficence and truthtelling. As Brennan points out,the IOM sought to assure accountability through its pro-posed mandatory reporting of serious, preventable adverseevents. Not surprisingly, however, the dominance of mal-practice has made this recommendation politically unten-able.68 Thus, reconsideration of the malpractice system it-self, in favor of no-fault and mediation, may be necessaryto overcome the antagonism between safety improvementand the values of nonmaleficence and truth-telling, as wellas to achieve accountability in the prospective as well asthe retrospective sense.
The recently finalized Health Insurance Portability andAccountability Act (HIPAA) has also given rise to con-cerns about the extent to which data collection for safetyimprovement will be hampered by HIPAA provisions tosafeguard the privacy of patient records. At issue iswhether patient records—primarily intended to supportthe health care needs of the patient—can also be used for
the secondary purpose of improving safety or quality. AsBryan Liang points out, HIPAA was not designed withsafety improvement research in mind and may presentsome obstacles to the use of patient information in thisarena.69 In the original version of the regulation, before itwas modified in August 2002, patient consent was re-quired for the release of personal, identifiable informationthat could be used for safety improvement. The modifica-tions eliminate the consent requirement for the disclosureof personal information for “health care operations,”which may include quality improvement activities. Underthe rubric of “quality,” data collection for safety withoutpatient consent appears to be allowable in the final rule.But if quality- or safety- improvement rises to the level of“research”—if it involves the production of “generalizableknowledge”—the activities will fall under the require-ments of human subjects protection requiring Institution-al Review Board approval or HIPAA authorization. Themodifications to HIPAA also allow for researchers to haveaccess, without patient consent, to a “limited data set,”that is, to information that has been partially de-identi-fied. It is not clear whether this limited information willbe useful in fine-grained safety improvement work.
The final privacy rule goes some way towards harmo-nizing patient privacy and the promotion of safety-im-provement activities. Still, safety improvement activitiesought not to be conducted on the basis of information towhich harmed patients themselves are denied access, ei-ther because of the structure of peer review protections orbecause providers are reluctant to disclose due to liabilityfears.70 No-fault liability offers one way around this con-flict. Under such a system, existing obstacles to patient ac-cess to information about the delivery of their health carewould be largely removed, and this secondary use ofhealth information would not be contingent on deprivingpatients of their rights to know about problems associatedwith their health care. Although the HIPAA privacy pro-visions have been finalized and compliance is now re-quired, it is likely that definitive answers to questions re-garding privacy and “research” will be obtained only as therule is tested or as advocates seek amendments to it.
Safety Improvement

S16 September-October 2003 / HASTINGS CENTER REPORT
The chief goal of this report has been explore andclarify both the ethical considerations that enterinto patient safety reform and the ethical implica-
tions of various reform proposals at federal state and insti-tutional levels. Elucidating the ethical basis of policy de-liberation leads to several important recommendations:
n Federal officials, privacy advocates and advocates ofsafety improvement should work together to clarify theimplications of the HIPAA privacy rule for the collectionof safety data.
n Policymakers should look for alternatives to the tortsystem to serve the purposes of compensation and safetyimprovement.
n Institutional change depends on understanding how acultural context shapes perceptions about why errors hap-pen and how actors within a culture learn to think aboutand deal with them. Institutional leaders in health carewill need more self-consciously to examine the “hiddencurriculum” in medical and nursing education; that is, thepractices that are taught and rewarded through example,rather than through what is conveyed in the official cur-riculum.
n Errors cannot be eliminated. We can, however, reducethem, learn from them, improve the way we handle them,and deal more justly with all those (including clinicians)touched by them.
Recommendations

S17SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
References
1. L.T. Kohn, J.M. Corrigan, M.S. Don-aldson, eds, To Err is Human: Building aSafer Health System (Washington, DC: Na-tional Academy Press, 2000).
2. Ibid., p. 18.3. V.A. Sharpe and A.I. Faden, Medical
Harm: Historical, Conceptual and EthicalDimensions of Iatrogenic Illness (New York:Cambridge U. Press, 1998); T.L.Beauchamp and J.F. Childress, Principles ofBiomedical Ethics 4th ed. (New York: Ox-ford University Press, 1994).
4. E.D. Pellegrino, “Toward a Recon-struction of Medical Morality: The Primacyof the Act of Profession and the Fact of Ill-ness,” Journal of Medicine and Philosophy 4(1979):32-55; E.D. Pellegrino ED, D.C.Thomasma, For the Patient’s Good: TheRestoration of Beneficence in Health Care(New York: Oxford, 1988).
5. E.D. Pellegrino, “Prevention of Med-ical Error: Where Professional and Organi-zational Ethics Meet,” in Promoting PatientSafety: An Ethical Basis for Policy Reform, ed.V.A. Sharpe (Washington, DC: George-town University Press, in press).
6. Kohn, et al.,. To Err is Human, p. 4.7. Kohn, et al.,. To Err is Human, p. 4.8. See T. Brennan, “The Institute of
Medicine Report on Medical Errors—Could it do Harm?” New England Journalof Medicine 342 (2000):1123-1125.
9. Kohn, et al., To Err is Human, p. 87-88; 133.
10. Kohn, et al., To Err is Human, p.102.
11. It is well known that the threat ofmedical malpractice has created a culture ofsilence in medicine, discouraging healthcare providers from telling patients aboutproblems associated with their care. Evenclaimants who settle a lawsuit may neverknow the events surrounding an injury. See,S. Gilbert, Wrongful Death (New York,Norton & Norton, 1997)
12. Liang has indicated the multipleways in which such confidentiality can, infact, be breached, by legal maneuvers. SeeBryan Liang, “Error Disclosure for QualityImprovement: Authenticating a Team ofPatients and Providers to Promote PatientSafety,” in Promoting Patient Safety: An Eth-ical Basis for Policy Reform, ed. V.A. Sharpe(Washington, DC: Georgetown UniversityPress, in press).
13. Kohn, et al., To Err is Human, p.102.
14. F. Rosner, J.T. Berger, P. Kark, J.Potash, A.J. Bennett, “Disclosure and Pre-vention of Medical Error,” Archives of Inter-nal Medicine 160 (2000):2089-2092;American Medical Association, Council onEthical and Judicial Affairs. Code of Medical
Ethics: Current Opinions with Annotations.Chicago: AMA, 1997, sec. 8.12:125.
15. Joint Commission on Accreditationof Health Care Organizations: 2002 Com-prehensive Accreditation Manual for Hospi-tals: The Official Handbook (Oakbrook Ter-race, IL, JCAHO, 2001). See standardRI.1.2.2: “Patients and, when appropriate,their families are informed about the out-comes of care, including unanticipated out-comes.”
16. S.S. Kraman and G. Hamm, “RiskManagement: Extreme Honesty May Bethe Best Policy,” Ann Intern Med 131(1999):963-967.
17. N. Osterweil, “Truth or Conse-quences: Does Disclosure Reduce Risk Ex-posure?: Admitting Errors Makes ProcessLess Adversarial, MDs, Lawyers Agree,”WebMD Medical News, 20 December 1999.http://my.webmd.com/content/arti -cle/1728.53548.
18. L.L. Leape, “Error in Medicine,”Journal of the American Medical Association272 (1994):1851-7.
19. D. Maurino, J. Reason, R. Lee. Be-yond Aviation Human Factors. (AldershotUK: Avery Press, 1995); James Reason,Human Error (New York: Cambridge Uni-versity Press, 1990); James Reason,.“Human Error: Models and Management,”British Medical Journal 320 (2000):768-70; James Reason. Managing the Risks of Or-ganizational Accidents (Aldershot, UK: Ash-gate, 1998).
20. L.L. Leape, D.D. Woods, M.J.Hatlie, K.W. Kizer, S.A. Schroeder, G.D.Lundberg, “Promoting Patient Safety byPreventing Medical Error,” Journal of theAmerican Medical Association 280(1998):1444-1447.
21. Thanks to Janlori Goldman forpointing out this important ambiguity.
22. W.E. Deming, Out of the Crisis,(Cambridge, Mass.: MIT Center for Ap-plied Engineering Studies, 1986); D.M.Berwick, “Continuous Improvement as anIdeal in Health Care,” New England Journalof Medicine 320 (1989):53-56; J. Reason J.Human Error.
23. See the text of the bills, S. 2590, andH.R. 4889 on Thomas, the federal govern-ment’s legislative information site on the In-ternet, http://thomas.loc.gov/
24. T. Brennan, “The Institute of Medi-cine Report on Medical Errors—Could itdo Harm?” New England Journal of Medi-cine 342 (2000):1123-1125.
25. E.A. Dauer, “Ethical Misfits: Media-tion and Medical Malpractice Litigation,”in Promoting Patient Safety: An Ethical Basisfor Policy Reform, ed. V.A. Sharpe (Washing-ton, D.C.: Georgetown University Press, inpress).
26. T. Percival, Medical Ethics or A Codeof Institutes and Precepts adapted to the Pro-fessional Conduct of Physicians and Surgeons(Manchester: S. Russell, 1803).
27. K.A. De Ville, “God, Science, andHistory: The Cultural Origins of MedicalError,” in Promoting Patient Safety: An Ethi-cal Basis for Policy Reform, ed. V.A. Sharpe(Washington, DC: Georgetown UniversityPress, in press); K.A. De Ville, Medical Mal-practice in Nineteenth-Century America: Ori-gins and Legacy (New York: NYU Press,1990).
28. D.M. Berwick, “Continuous Im-provement as an Ideal in Health Care”; J.Reason Human Error.
29. R.I. Cook, D.D. Woods, C. Miller.“A Tale of Two Stories: Contrasting Viewsof Patient Safety. Report from a Workshopon Assembling the Scientific Basis forProgress on Patient Safety.” (Chicago: Na-tional Patient Safety Foundation, 1998)http://www.npsf.org/exec/front.html.
30. J. Reason. Managing the Risks of Or-ganizational Accidents (Aldershot, UK: Ash-gate, 1998).p. 208.
31. D. Blumenthal, “Making MedicalErrors into “Medical Treasures.’’ Journal ofthe American Medical Association 272(1994):1867-68. Karl E. Weick, KathleenM. Sutcliffe, Managing the Unexpected : As-suring High Performance in an Age Of Com-plexity (San Francisco: Jossey-Bass, 2001).
32. A. Merry, A.M. Smith, Errors, Med-icine and the Law. (Cambridge, UK: Cam-bridge University Press. 2001). It is alsoworth noting that in his NicomacheanEthics, Aristotle observes that responsibilityis only properly ascribed to actions that arevoluntary. See (Aristotle, 1999, 1110a ff).
33. K.A. De Ville, “God, Science, andHistory: The Cultural Origins of MedicalError.”
34. S. Gilbert, Wrongful Death (NewYork, Norton & Norton, 1997), p. 218-9.
35. J. Reason. Managing the Risks of Or-ganizational Accidents. p. 192.
36. Edmund Pellegrino, “Prevention ofMedical Error: Where Professional and Or-ganizational Ethics Meet.”
37. Edward A. Dauer, “Ethical Misfits:Mediation and Medical Malpractice Litiga-tion,” in Promoting Patient Safety: An Ethi-cal Basis for Policy Reform, ed. V.A. Sharpe(Washington, D.C.: Georgetown Universi-ty Press, in press).
38. The discussion of this distinction isdrawn from V. A. Sharpe, “Taking Respon-sibility For Medical Mistakes,” in S. Rubinand L. Zoloth, eds. Margin Of Error: TheEthics Of Mistakes in the Practice of Medi-cine. (Hagerstown, Md.: University Pub-lishing Group, 2000): 183-94.
39. Of course, failures of prospective re-sponsibility often result in holding someone

S18 September-October 2003 / HASTINGS CENTER REPORT
responsible retrospectively. The systems ap-proach is an attempt to expand the scope ofprospective responsibility so that concertedsteps toward safety can be taken and re-warded before there are specific outcomesto be assessed.
40. For example, are moral norms inher-ent to medicine, residing in the fiduciarynature of the healing relationship? Are theygrounded in a pragmatic concern to pro-duce “patient satisfaction?” Are they basedin theories of democratic citizenship? Or ismedicine simply like other market transac-tions that are based on contracts stipulatingspecific expectations and obligations?
41. Hippocrates. Epidemics I. In Hip-pocrates, trans., W.H.S. Jones. Loeb Classi-cal Library. (Cambridge, Mass.: HarvardUniversity Press, 1923-1988): 165.
42. L. May and S. Hoffman, CollectiveResponsibility: Five Decades of Debate in The-oretical and Applied Ethics (Savage, M: Row-man and Littlefield, 1991).
43. L.L Leape, D.W. Bates, D.J. Cullen,et al for the ADE Prevention Study Group.Systems Analysis of Adverse Drug Events.Journal of the American Medical Association274 (1995):35-43.
44. E. Pellegrino, “Prevention of MedicalError: Where Professional and Organiza-tional Ethics Meet.”
45. There is a large literature on the ex-tent to which people are responsible fortheir health and their health behaviors. Ourquestion is much narrower and concernsonly whether patients are responsible forthe safety and quality of health care deliv-ery.
46. R. Goeltz, “In Memory of My Broth-er, Mike,” in Promoting Patient Safety: AnEthical Basis for Policy Reform, ed. V.A.Sharpe (Washington, D.C.: GeorgetownUniversity Press, in press).
47. B. Liang, “Error Disclosure for Qual-ity Improvement: Authenticating a Team ofPatients and Providers to Promote PatientSafety,” in Promoting Patient Safety: An Eth-ical Basis for Policy Reform, ed. V.A. Sharpe(Washington, D.C.: Georgetown Universi-ty Press, in press).
48. This point is reflected in the JointCommission’s 2002 standards #3.7 on pa-tient education. Joint Commission on Ac-creditation of Health Care Organizations:2002 Comprehensive Accreditation Manualfor Hospitals: The Official Handbook (Oak-brook Terrace, IL, JCAHO, 2002).
49. D. Hilfiker, Facing Our Mistakes.New England Journal of Medicine 310(1984):118-122.
50. D. Studdert, “On Selling “No-Fault,” in Promoting Patient Safety: An Ethi-cal Basis for Policy Reform, ed. V.A. Sharpe(Washington, D.C.: Georgetown Universi-ty Press, in press); Edward A. Dauer, “Ethi-
cal Misfits: Mediation and Medical Mal-practice Litigation,” in Promoting PatientSafety: An Ethical Basis for Policy Reform, ed.V.A. Sharpe (Washington, D.C.: George-town University Press, in press); BryanLiang, “Error Disclosure for Quality Im-provement: Authenticating a Team of Pa-tients and Providers to Promote PatientSafety.”
51. F. A. Sloan and C.R. Hsieh, “Vari-ability in Medical Malpractice Payments: IsThe Compensation Fair?” Law and SocietyReview 24 (1990):997-1039; N. Vidmar,Medical Malpractice and the American Jury:Confronting the Myths About Jury Incompe-tence, Deep Pockets, and Outrageous DamageAwards (Ann Arbor: University of MichiganPress, 1995); P.C. Weiler H.H. Hiatt, J.P.Newhouse , et al. A Measure of Malpractice:Medical Injury, Malpractice Litigation andPatient Compensation (Cambridge, Mass.:Harvard University Press, 1993); H.R.Burstin, W.G. Johnson, S.R. Lipsitz, T.A.Brennan. “Do the Poor Sue More? A Case-Control Study Of Malpractice Claims andSocioeconomic Status.” Journal of the Amer-ican Medical Association 13 (1993):1697-1701.
52. T.A. Brennan, C.A. Sox, H.R.Burstin, “Relation Between Negligent Ad-verse Events and the Outcomes of MedicalMalpractice Litigation,” New England Jour-nal of Medicine 335 (1996):1963-1967.
53. J.S. Kakalik and N.M. Pace, Costsand Compensation Paid in Tort Litigation(Santa Monica, CA: RAND, 1986 (R-3391-ICJ)).
54. P. Weiler, et al., A Measure of Mal-practice (Cambridge, Mass.: Harvard Uni-versity Press, 1993).
55. C. Levine. “Life But No Limb: TheAftermath of Medical Error.” Health Affairs21 (2002):237-41. Reprinted in PromotingPatient Safety: An Ethical Basis for Policy Re-form, ed. V.A. Sharpe (Washington, D.C.:Georgetown University Press, in press).
56. D. Kessler and M. McClellan. “DoDoctors Practice Defensive Medicine?”Quarterly Journal of Economics 111(1996):353-390.
57. S.C. Charles, “Sued and Non-SuedPhysicians’ Self-Reported Reactions to Mal-practice Litigation,” American Journal ofPsychiatry 142 (1985):437-440; T.Passineau, “Why Burned-Out Doctors GetSued More Often,” Medical Economics 75(1998):210-218; B.A. Liang, “The Effec-tiveness of Physician Risk Management:Potential Problems for Patient Safety,” RiskDecision Policy 5 (2000):183-202.
58. D. Studdert, “On Selling “No-Fault.”
59. H. Morreim, “Medical Errors: Pin-ning the Blame versus Blaming the Sys-tem,” in Promoting Patient Safety: An EthicalBasis for Policy Reform, ed. V.A. Sharpe
(Washington, D.C.: Georgetown Universi-ty Press, in press).
60. E.A. Dauer and L.J. Marcus, “Adapt-ing Mediation to Link Resolution of Med-ical Malpractice Disputes with Health CareQuality Improvement,” Law and Contem-porary Problems 60 (1997):185-218; W.Levinson, “Physician-Patient Communica-tion. A Key to Malpractice Prevention,”Journal of the American Medical Association.272 (1994):1619-20; W. Levinson, D.L.Roter, J.P. Mullooly, V.T. Dull, R.M.Frankel, “Physician-Patient Communica-tion. The Relationship with MalpracticeClaims Among Primary Care PhysiciansAnd Surgeons,” Journal of the AmericanMedical Association. 277 (1997):553-9.
61. W.M. Sage, “Reputation, Malprac-tice Liability, and Medical Error,” in Pro-moting Patient Safety: An Ethical Basis forPolicy Reform, ed. V.A. Sharpe (Washington,D.C.: Georgetown University Press, inpress); J. Soloski and R.P. Bezanson. Re-forming Libel Law. (New York: GuilfordPress, 1992).
62. E.A. Dauer, L.J. Marcus, and S.M.Payne, “Prometheus and the Litigators: AMediation Odyssey.” Journal of Legal Medi-cine 2000;21:159-186.
63. B. Liang, “Error Disclosure for Qual-ity Improvement: Authenticating a Team ofPatients and Providers to Promote PatientSafety.”
64. C.L. Bosk, Forgive and Remember:Managing Medical Failure (Chicago: Uni-versity of Chicago Press, 1979).
65. N.S. Berlinger, “’Missing the Mark’:Medical Error, Forgiveness, and Justice,” inPromoting Patient Safety: An Ethical Basis forPolicy Reform, ed. V.A. Sharpe (Washington,D.C.: Georgetown University Press, inpress).
66. Kohn, et al., To Err is Human, p.101, 110.
67. These bills can be found on Thomas,the federal government’s legislative informa-tion site on the Internet,http://thomas.loc.gov/
68. Troyen Brennan, “The Institute ofMedicine Report on Medical Errors—Could it do Harm?”
69. Bryan Liang, “Error Disclosure forQuality Improvement: Authenticating aTeam of Patients and Providers to PromotePatient Safety.” Troyen A. Brennan andMichelle M. Mello, “Patient Safety andMedical Malpractice: A Case Study” Annalsof Internal Medicine 139 (2003): 267-273.
70. T. A. Brennan, “The Ethics of Confi-dentiality: The Special Case of Quality As-surance Research,” Clinical Research 38(1990):551-557.

S19SPECIAL SUPPLEMENT / Promoting Patient Safety: An Ethical Basis for Policy Deliberation
n Raymond S. Andrews, Jr.TrusteeThe Patrick and Catherine Weldon Donaghue Foundation
n Mary Ann BailyAssociate for Ethics and Health PolicyThe Hastings Center
n Carol BayleyVice President, Ethics and Justice EducationCatholic Healthcare West
n Nancy BerlingerDeputy Director and Associate for Religious StudiesThe Hastings Center
n Charles BoskProfessor, Department of SociologyUniversity of Pennsylvania
n Maureen ConnorDirector of Risk Management and Infection ControlDana-Farber Cancer Institute
n James ConwaySVP and Chief Operations OfficerDana-Farber Cancer Institute
n Edward DauerDean Emeritus and Professor of LawUniversity of Denver College of Law
n Kenneth De VilleSchool of MedicineDepartment of Medical HumanitiesEast Carolina University
n Allan FrankelDirector of Patient SafetyPartners Health Care System, Inc.
n Lynne GarnerExecutive Director The Patrick and Catherine Weldon Donaghue Foundation
n Sandra GilbertProfessor, Department of EnglishUniversity of Californis, Davis
n Roxanne GoeltzAir Traffic ControllerMinneapolis, Minn.
n Doni HaasFormer Risk Manager, Martin Memorial HospitalStuart, Fl.
n Curtis HartDirector of Pastoral Care and EducationNew York-Presbyterian HospitalWeill Cornell Center
n Bryan A. Liang, M.D., Ph.D., J.D.Professor, Law, Health Law & Policy InstituteUniversity of Houston Law CenterProfessor of Medicine, University of Texas School of Medicine
n Larry I. Palmer, LLBProfessor of LawCornell Law School
n Edmund D. Pellegrino, M.D.Emeritus Professor of Medicine
and Medical EthicsCenter for Clinical BioethicsGeorgetown University Medical Center
n E. Haavi MorreimCollege of MedicineUniversity of TennesseeHealth Science Center
n Erik ParensAssociate for Philosophical StudiesThe Hastings Center
n William S. SageProfessor of LawColumbia Law School
n Virginia Ashby SharpeFormer Deputy Director and Associate
for Biomedical and Enviornmental EthicsThe Hastings Center
n Scott A. SnookAssociate Professor Harvard Business School
n David StuddertAssistant Professor for Law & Public HealthDepartment of Health Policy & ManagementHarvard School of Public Health
n Karen TitlowProgram DirectorThe Leapfrog Group
n Albert WuAssociate ProfessorHealth Policy & ManagementSchool of Hygiene & Public HealthJohns Hopkins University
Project Working Group Members

The Hastings Center addresses fundamental ethicalissues in the areas of health, medicine, and the
environment as they affect individuals, communities,and societies. With a small staff of senior researchersat the Center and drawing upon an internationallyrenowned group of over 100 elected Fellows for theirexpertise, The Hastings Center pursues interdiscipli-nary research and education that includes both theoryand practice. Founded in 1969 by philosopher DanielCallahan and psychoanalyst Willard Gaylin, TheHastings Center is the oldest independent, nonparti-san, interdisciplinary research institute of its kind inthe world. From its earliest days The Hastings Centerhas understood that the moral problems arising fromrapid advances in medicine and biology are set withina broad intellectual and social context. The Center’scollaborations with policymakers, in the private as wellas the public sphere, assist them in analyzing the ethi-cal dimensions of their work.
ORDER IN F O R M ATION
For copies of this or other Hastings Center ReportSpecial Supplements, write or call: Membership DepartmentThe Hastings Center21 Malcolm Gordon RoadGarrison, NY 10524-5555(845) 424-4040(845) 424-4545 fax; [email protected] www.thehastingscenter.org.
ABOUT THE HASTINGS CENTER