Embed Size (px)
Citation preview
Promoting the Health and Wellbeing of
OSU’s Health Sciences Students through a New Wellness Onboarding Program
Bernadette Mazurek Melnyk, PhD, RN, CPNP/PMHNP, FAAN
Associate Vice President for Health Promotion University Chief Wellness Officer
Dean and Professor, College of Nursing Professor of Pediatrics and Psychiatry, College of Medicine
Special Thanks
• Jackie Hoying, PhD, RN, NEA-BC
• Lisa Militello, PhD, MPH, RN, CPNP
• Colleen McGovern, MPH, RN
• Caitlin Slevin, MHA, CCRP
• Alice Teall, MS, FNP, PNP, FAANP
Objectives
• Describe the state of health and wellness in health sciences students.
• Discuss a new wellness onboarding program for OSU health sciences students and its findings.
• Describe future plans for refinement and expansion of the program.
• Discuss strategies for enhancing wellbeing in OSU
health sciences students.
Transition into Graduate School Can be a Stressful Time for Many Students; Concerns about Performance,
Finances and Life Balance are Common
Health sciences colleges prepare students well to deliver high quality care to patients, yet few incorporate wellness and self-care into their academic programming
Although there are descriptive studies reporting the high prevalence of
mental health problems and unhealthy behaviors as students transition from high school into college, few studies have described the mental health, physical health and healthy lifestyle behaviors of health sciences students
There also is a paucity of intervention studies in this population to improve their healthy lifestyle behaviors during graduate school
The AAMC and IOM have emphasized the need to address physician
wellbeing in medical school programs
Background/Significance
Purpose • Purpose: To evaluate the feasibility, acceptability and
preliminary effects of a wellness on-boarding program for health sciences students, including dentistry, health and rehabilitation sciences, medicine, nursing, optometry, pharmacy, and veterinary medicine, on their healthy lifestyle beliefs, behaviors, anxiety and depressive symptoms
• A pre-experimental pilot study was first conducted with 93 OSU health sciences students entering their health professional programs in 2014
• A second cohort experimental pilot study was conducted with 109 OSU health science students entering their health professional program in 2015
• Valid and reliable measures were collected at the start and end of the students’ semester oPatient Health Questionnaire-9 (PHQ-9) for depression oThe Generalized Anxiety Disorder Scale (GAD-7) oThe Brief Inventory of Perceived Stress (BIPS) oThe Healthy Lifestyle Beliefs Scale oThe Healthy Lifestyle Behaviors Scale
Methodology
Wellness Coaching is Evidence-Based
» ↑ Coping with stress and depression » ↓ Perceived stress » ↓ Depression » ↑ Quality of life in all domains » ↑ Physical well-being » ↑ Confidence & motivation to change » ↑ Activation & health status » Improvement maintained after coaching
completed » Interventions by phone equally effective
Clark et. al. (2014) Lawson et. al. (2013) Mettler et. al. (2014)

Wellness Coaching
» Partnership » Person-centered » Goal-directed » Focused on strengths » Grounded in Appreciative Inquiry » Uses Motivational Interviewing » Encourages self-discovery » Supports self-efficacy
Wolever et. al. (2013)
Wellness Coaching in the Onboarding Study
• Coaching is investment in the health of individuals who will be healthcare providers themselves
• Phone conversations individualized to student-participant goals • Texting encouragement as determined by student-participant
needs
mHEALTH • mHealth
– Wireless mobile technology accessed during normal daily activities – mHealth uses these technologies to monitor or improve health
outcomes
• mHealth for this project – Partnership with Memotext (HIPPA compliant) for software platform – Text messages (short message code, SMS<140 characters) used to
augment coaching – Coaches and participants picked topic(s) to be sent in messages “Your health coach hopes you are finding something relaxing to relieve your stress tonight! :)” – Push messages (one-way; e.g. reminder) “Don't forget to log your daily meals into your food log and review your fruit and vegetable intake ” – Coaches and participants determined frequency and timing of SMS
delivery
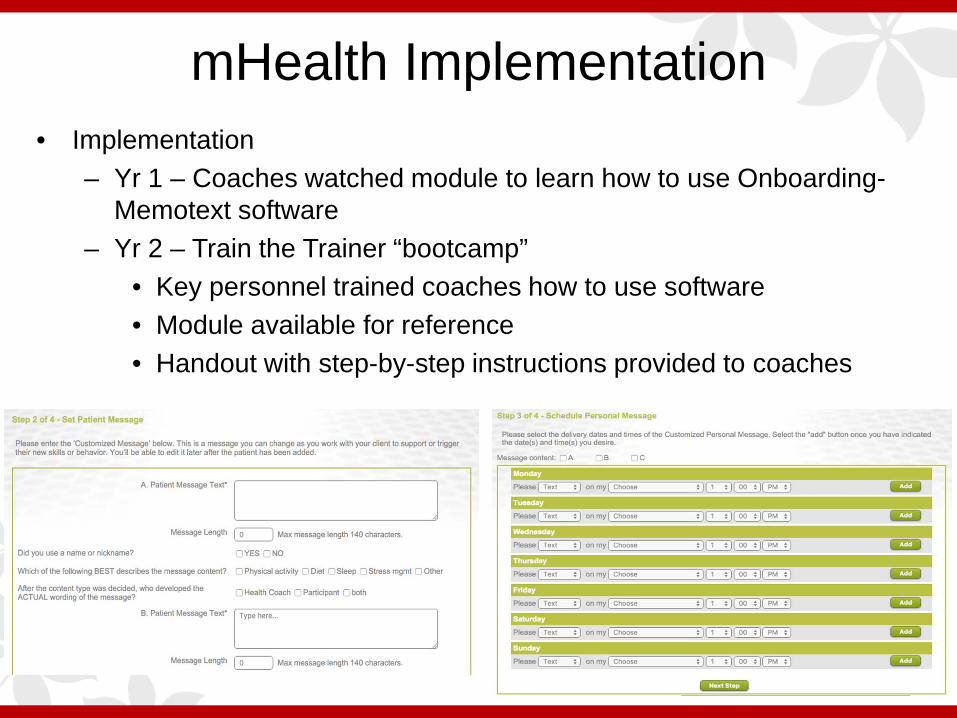
mHealth Implementation • Implementation
– Yr 1 – Coaches watched module to learn how to use Onboarding-Memotext software
– Yr 2 – Train the Trainer “bootcamp” • Key personnel trained coaches how to use software • Module available for reference • Handout with step-by-step instructions provided to coaches
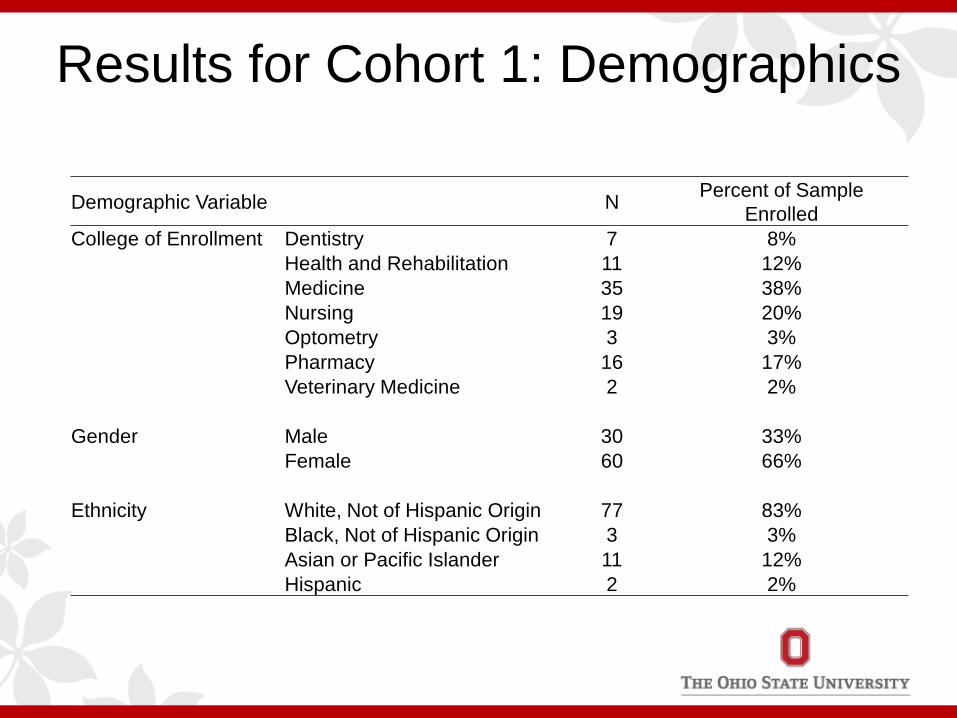
Results for Cohort 1: Demographics
Demographic Variable N Percent of Sample Enrolled
College of Enrollment Dentistry 7 8% Health and Rehabilitation 11 12% Medicine 35 38% Nursing 19 20% Optometry 3 3% Pharmacy 16 17% Veterinary Medicine 2 2%
Gender Male 30 33% Female 60 66%
Ethnicity White, Not of Hispanic Origin 77 83% Black, Not of Hispanic Origin 3 3% Asian or Pacific Islander 11 12%
Hispanic 2 2%
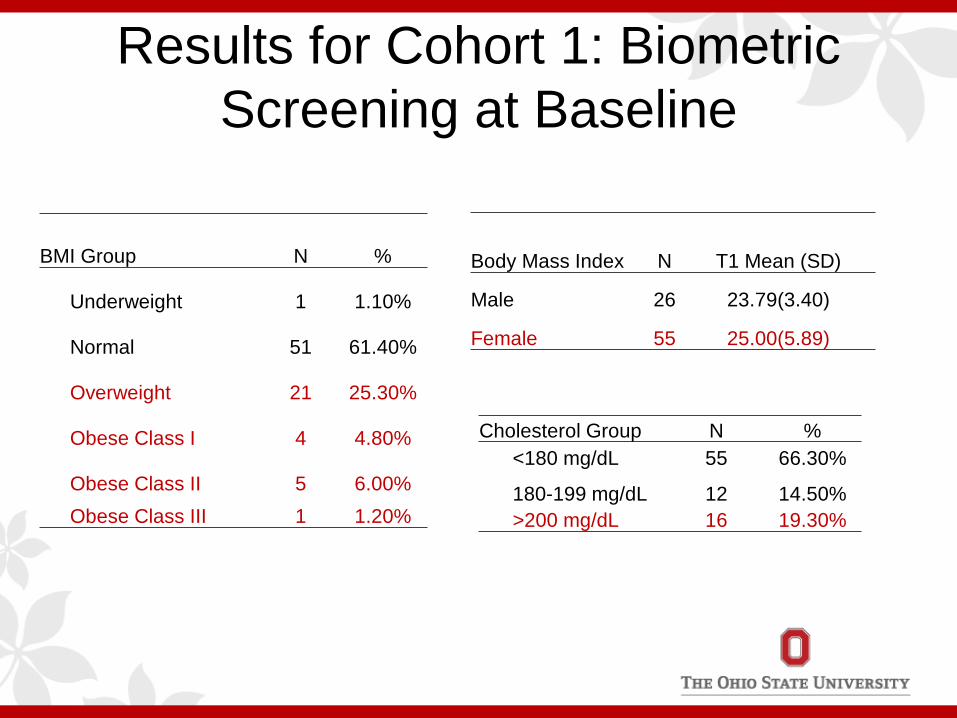
Results for Cohort 1: Biometric Screening at Baseline
Cholesterol Group N % <180 mg/dL 55 66.30%
180-199 mg/dL 12 14.50% >200 mg/dL 16 19.30%
BMI Group N %
Underweight 1 1.10%
Normal 51 61.40%
Overweight 21 25.30%
Obese Class I 4 4.80%
Obese Class II 5 6.00% Obese Class III 1 1.20%
Body Mass Index N T1 Mean (SD)
Male 26 23.79(3.40)
Female 55 25.00(5.89)
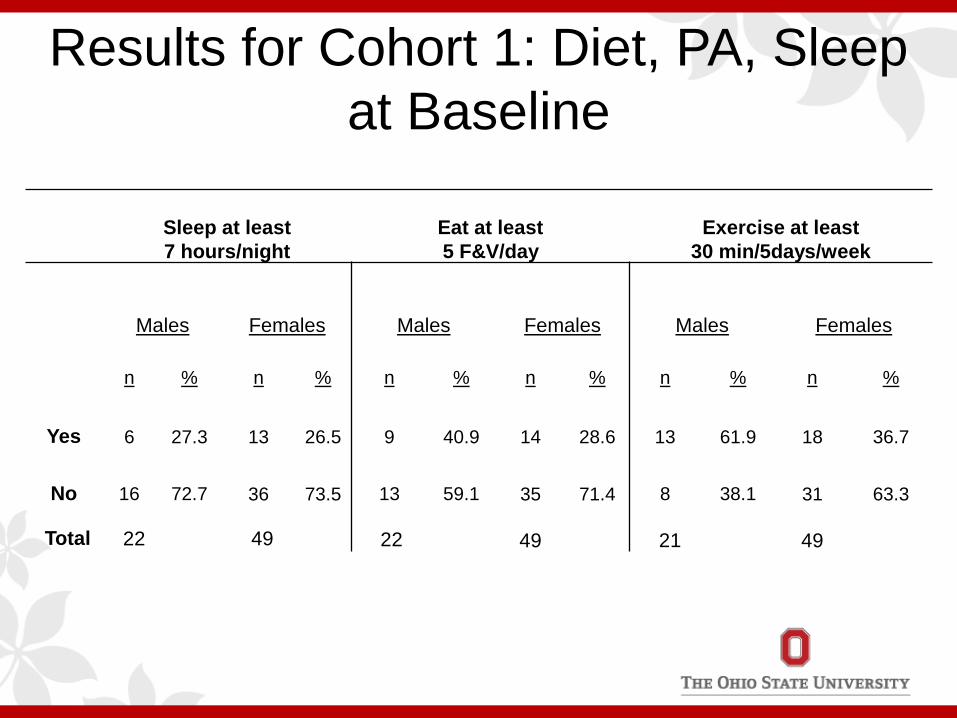
Results for Cohort 1: Diet, PA, Sleep at Baseline
Sleep at least 7 hours/night
Eat at least 5 F&V/day
Exercise at least 30 min/5days/week
Males Females Males Females Males Females
n % n % n % n % n % n %
Yes 6 27.3 13 26.5 9 40.9 14 28.6 13 61.9 18 36.7
No 16 72.7 36 73.5 13 59.1 35 71.4 8 38.1 31 63.3
49 49 Total 49 22 21 22
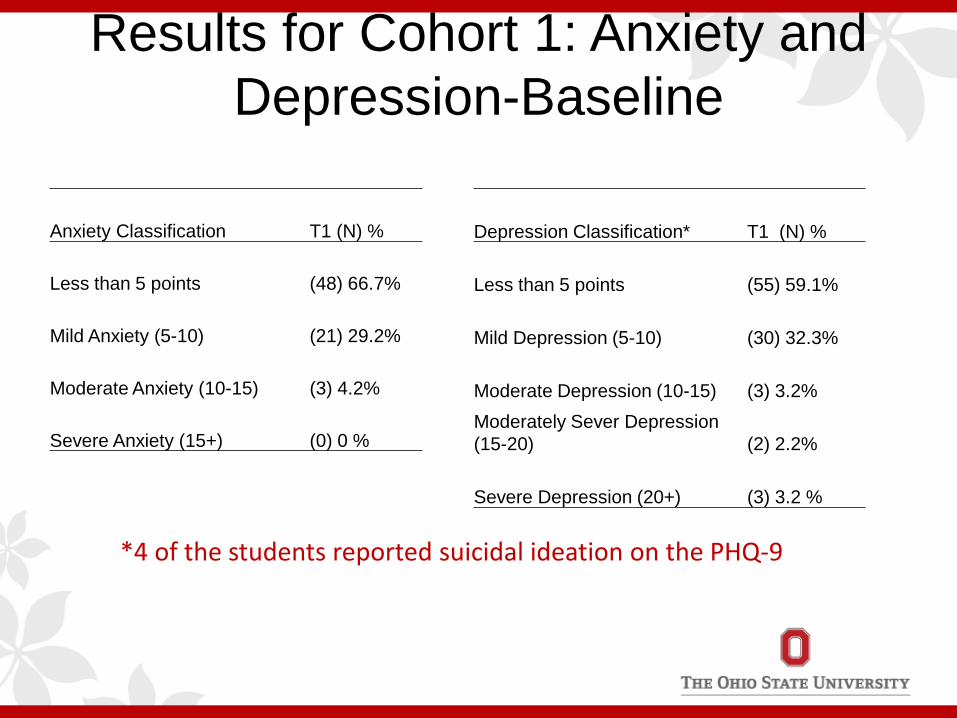
Results for Cohort 1: Anxiety and Depression-Baseline
Anxiety Classification T1 (N) %
Less than 5 points (48) 66.7%
Mild Anxiety (5-10) (21) 29.2%
Moderate Anxiety (10-15) (3) 4.2%
Severe Anxiety (15+) (0) 0 %
Depression Classification* T1 (N) %
Less than 5 points (55) 59.1%
Mild Depression (5-10) (30) 32.3%
Moderate Depression (10-15) (3) 3.2% Moderately Sever Depression (15-20) (2) 2.2%
Severe Depression (20+) (3) 3.2 %
*4 of the students reported suicidal ideation on the PHQ-9
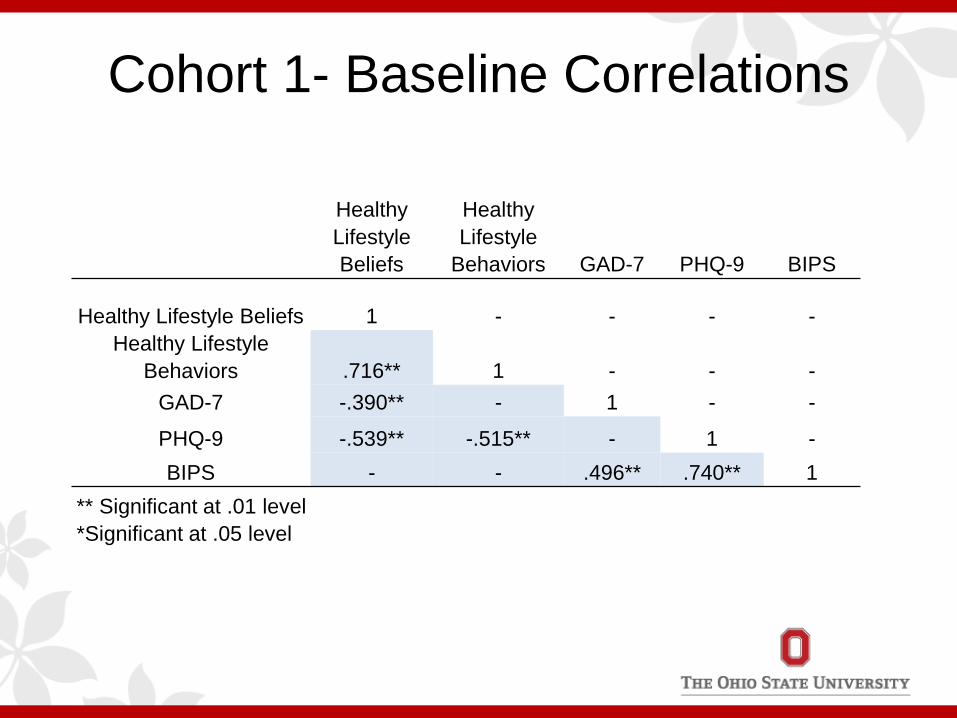
Cohort 1- Baseline Correlations
Healthy Lifestyle Beliefs
Healthy Lifestyle
Behaviors GAD-7 PHQ-9 BIPS
Healthy Lifestyle Beliefs 1 - - - - Healthy Lifestyle
Behaviors .716** 1 - - - GAD-7 -.390** - 1 - -
PHQ-9 -.539** -.515** - 1 - BIPS - - .496** .740** 1
** Significant at .01 level *Significant at .05 level
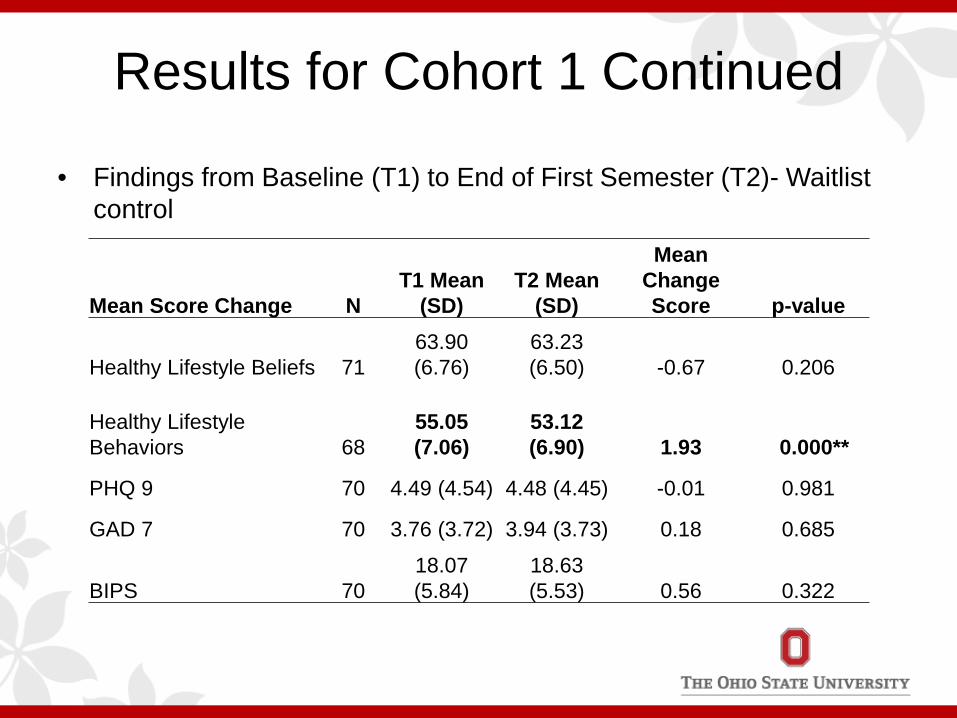
Results for Cohort 1 Continued
• Findings from Baseline (T1) to End of First Semester (T2)- Waitlist control
Mean Score Change N T1 Mean
(SD) T2 Mean
(SD)
Mean Change Score p-value
Healthy Lifestyle Beliefs 71 63.90 (6.76)
63.23 (6.50) -0.67 0.206
Healthy Lifestyle Behaviors 68
55.05 (7.06)
53.12 (6.90) 1.93 0.000**
PHQ 9 70 4.49 (4.54) 4.48 (4.45) -0.01 0.981
GAD 7 70 3.76 (3.72) 3.94 (3.73) 0.18 0.685
BIPS 70 18.07 (5.84)
18.63 (5.53) 0.56 0.322
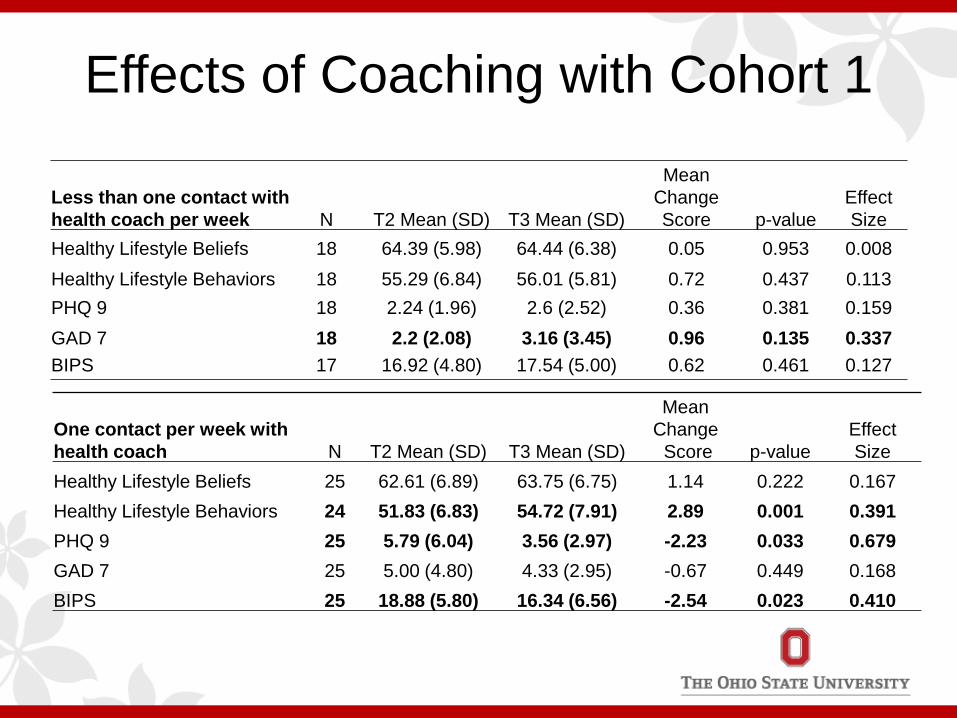
Effects of Coaching with Cohort 1
Less than one contact with health coach per week N T2 Mean (SD) T3 Mean (SD)
Mean Change Score p-value
Effect Size
Healthy Lifestyle Beliefs 18 64.39 (5.98) 64.44 (6.38) 0.05 0.953 0.008 Healthy Lifestyle Behaviors 18 55.29 (6.84) 56.01 (5.81) 0.72 0.437 0.113 PHQ 9 18 2.24 (1.96) 2.6 (2.52) 0.36 0.381 0.159 GAD 7 18 2.2 (2.08) 3.16 (3.45) 0.96 0.135 0.337 BIPS 17 16.92 (4.80) 17.54 (5.00) 0.62 0.461 0.127
One contact per week with health coach N T2 Mean (SD) T3 Mean (SD)
Mean Change Score p-value
Effect Size
Healthy Lifestyle Beliefs 25 62.61 (6.89) 63.75 (6.75) 1.14 0.222 0.167 Healthy Lifestyle Behaviors 24 51.83 (6.83) 54.72 (7.91) 2.89 0.001 0.391 PHQ 9 25 5.79 (6.04) 3.56 (2.97) -2.23 0.033 0.679 GAD 7 25 5.00 (4.80) 4.33 (2.95) -0.67 0.449 0.168 BIPS 25 18.88 (5.80) 16.34 (6.56) -2.54 0.023 0.410
Personal Wellness Plan Findings
• N= 55, 44 created 2 goals • 44% of primary goals and 43% of secondary
goals were related to physical activity • “I want to wake up a little earlier in the morning to
run for 20 minutes each day”
• “Maintaining at least 2 strenuous workouts a week and less strenuous workouts 3 of the remaining days (pushups and stretching before bed)”
Personal Wellness Plan Findings
• 34% of primary and 20% of secondary goals were nutrition related.
• “Eat two servings of fruits/vegetables a day”
• “Buy more food from the grocery store and
eat at home more” • “Decrease soda and sugary beverage
consumption to no more than 20 fl oz per day”
• 9% of primary or secondary goals were related to stress reduction.
• “I will give myself at least 1 hour per day away
from work and school. I will use that time to read or watch a TV show and zone out.”
• “I want to meditate for 20 minutes every day”
• “Write in a daily journal.”
Personal Wellness Plan Findings
Changes in Design and Study Protocol for Cohort 2 enrolled in August of 2015
• Randomized Controlled Pilot Trial - Group 1: Wellness plan with access to resources - Group 2: Wellness plan and health coaching
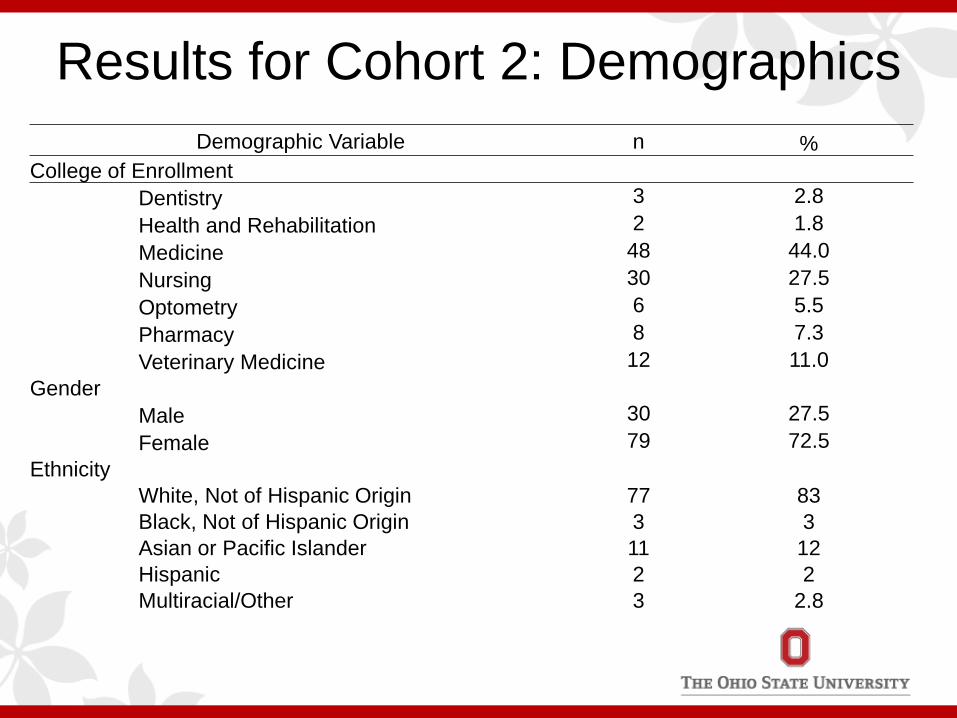
Results for Cohort 2: Demographics Demographic Variable n %
College of Enrollment Dentistry 3 2.8 Health and Rehabilitation 2 1.8 Medicine 48 44.0 Nursing 30 27.5 Optometry 6 5.5 Pharmacy 8 7.3 Veterinary Medicine 12 11.0
Gender Male 30 27.5 Female 79 72.5
Ethnicity White, Not of Hispanic Origin 77 83 Black, Not of Hispanic Origin 3 3 Asian or Pacific Islander 11 12
Hispanic 2 2 Multiracial/Other 3 2.8
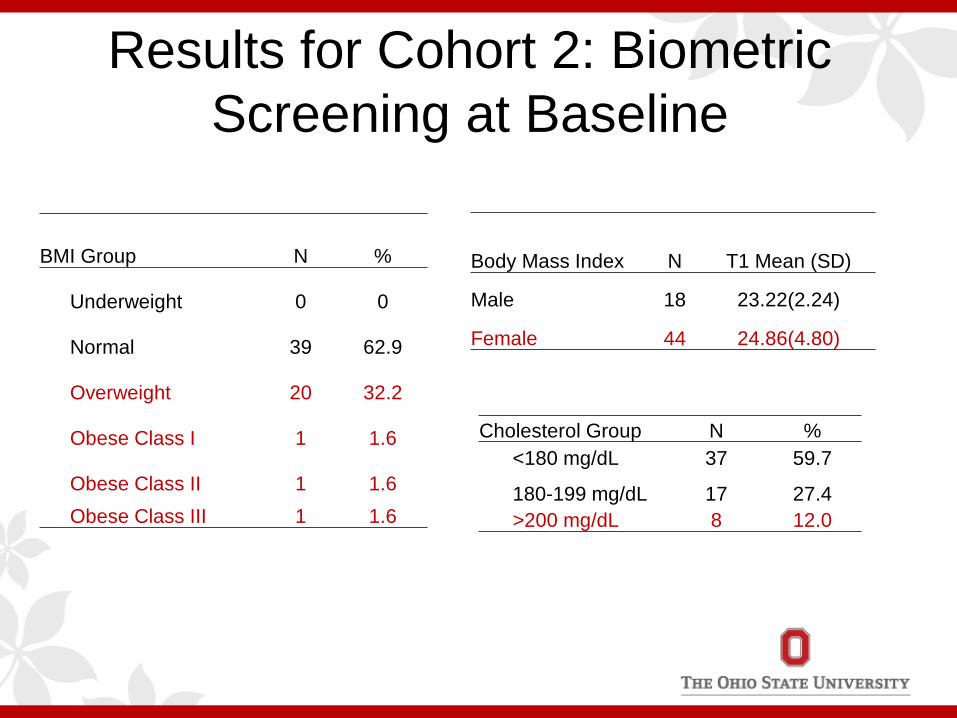
Results for Cohort 2: Biometric Screening at Baseline
Cholesterol Group N % <180 mg/dL 37 59.7
180-199 mg/dL 17 27.4 >200 mg/dL 8 12.0
BMI Group N %
Underweight 0 0
Normal 39 62.9
Overweight 20 32.2
Obese Class I 1 1.6
Obese Class II 1 1.6 Obese Class III 1 1.6
Body Mass Index N T1 Mean (SD)
Male 18 23.22(2.24)
Female 44 24.86(4.80)
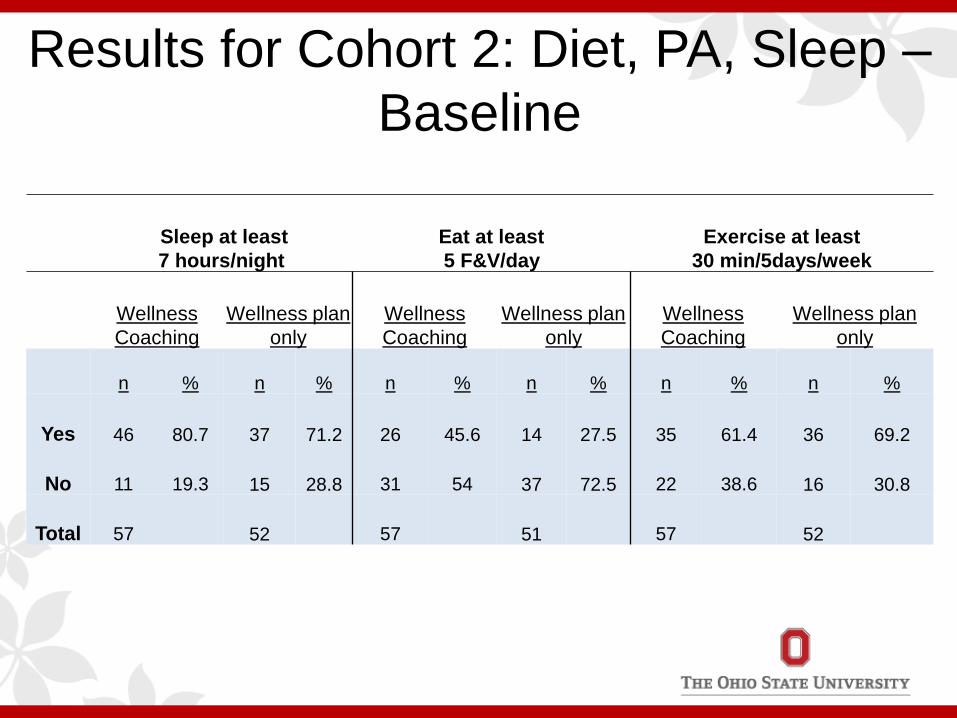
Results for Cohort 2: Diet, PA, Sleep –Baseline
Sleep at least 7 hours/night
Eat at least 5 F&V/day
Exercise at least 30 min/5days/week
Wellness Coaching
Wellness plan only
Wellness Coaching
Wellness plan only
Wellness Coaching
Wellness plan only
n % n % n % n % n % n %
Yes 46 80.7 37 71.2 26 45.6 14 27.5 35 61.4 36 69.2
No 11 19.3 15 28.8 31 54 37 72.5 22 38.6 16 30.8
Total 57 52 57 51 57 52
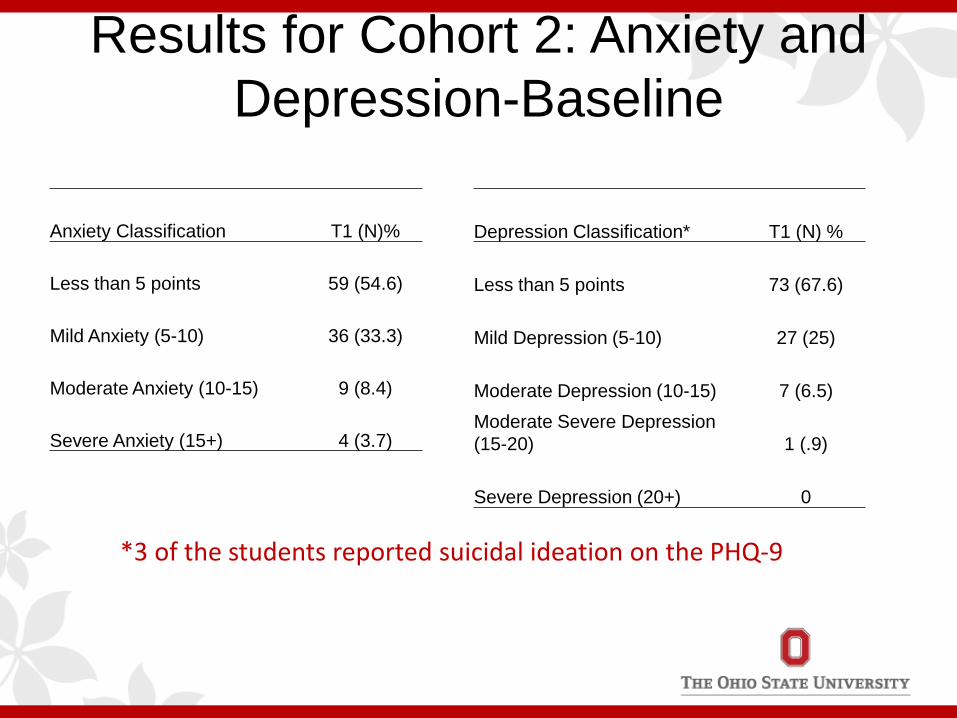
Results for Cohort 2: Anxiety and Depression-Baseline
Anxiety Classification T1 (N)%
Less than 5 points 59 (54.6)
Mild Anxiety (5-10) 36 (33.3)
Moderate Anxiety (10-15) 9 (8.4)
Severe Anxiety (15+) 4 (3.7)
Depression Classification* T1 (N) %
Less than 5 points 73 (67.6)
Mild Depression (5-10) 27 (25)
Moderate Depression (10-15) 7 (6.5) Moderate Severe Depression (15-20) 1 (.9)
Severe Depression (20+) 0
*3 of the students reported suicidal ideation on the PHQ-9
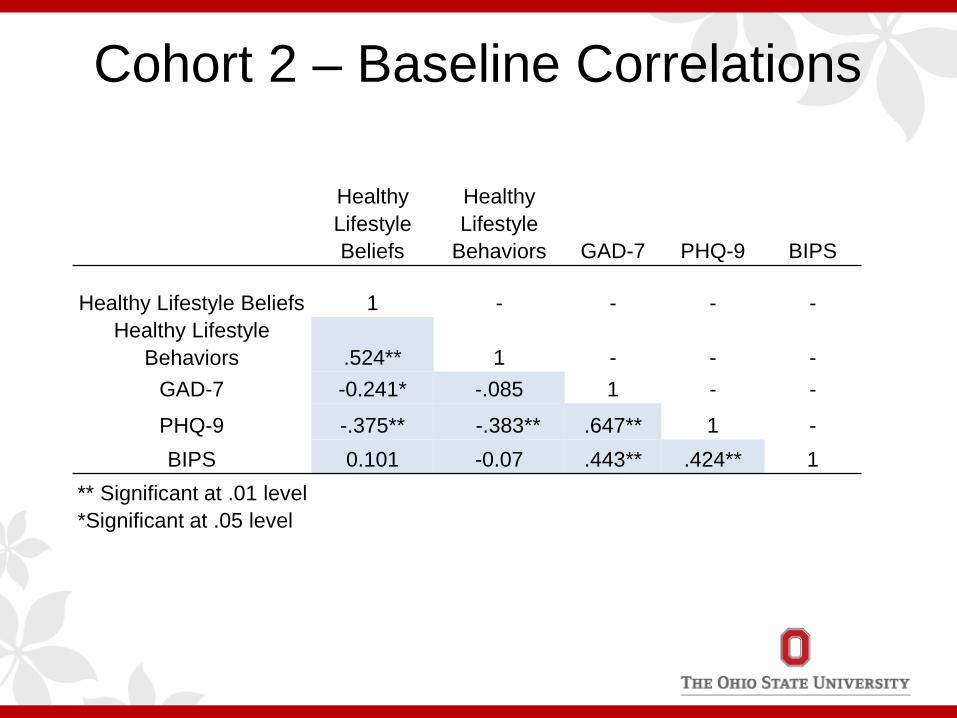
Cohort 2 – Baseline Correlations
Healthy Lifestyle Beliefs
Healthy Lifestyle
Behaviors GAD-7 PHQ-9 BIPS
Healthy Lifestyle Beliefs 1 - - - - Healthy Lifestyle
Behaviors .524** 1 - - - GAD-7 -0.241* -.085 1 - -
PHQ-9 -.375** -.383** .647** 1 - BIPS 0.101 -0.07 .443** .424** 1
** Significant at .01 level *Significant at .05 level
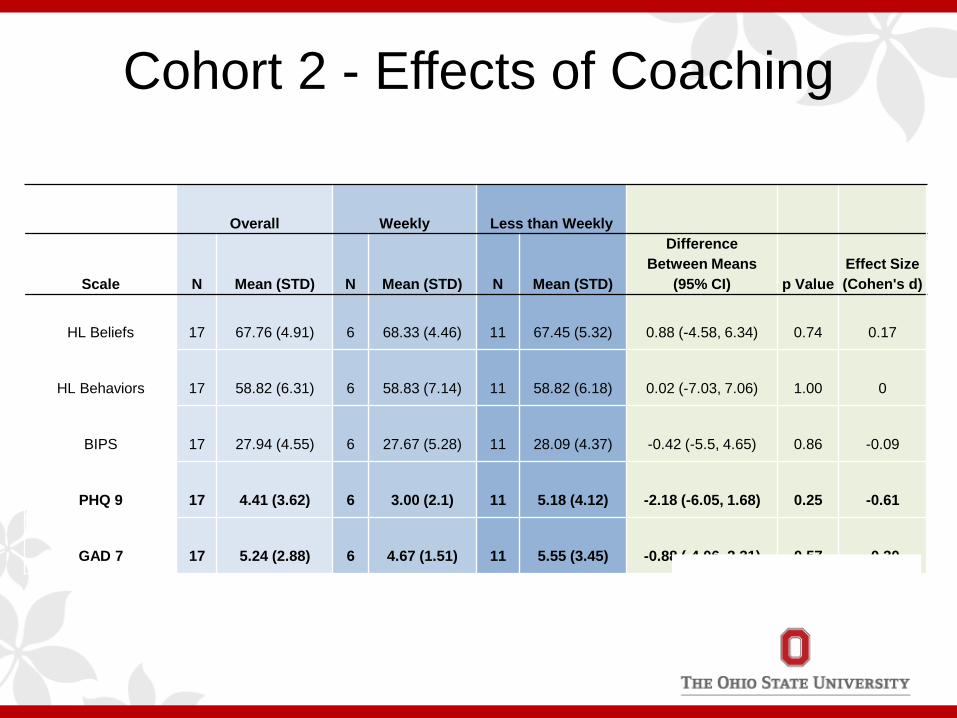
Cohort 2 - Effects of Coaching
Overall Weekly Less than Weekly
Scale N Mean (STD) N Mean (STD) N Mean (STD)
Difference Between Means
(95% CI) p Value Effect Size (Cohen's d)
HL Beliefs
17
67.76 (4.91)
6
68.33 (4.46)
11
67.45 (5.32)
0.88 (-4.58, 6.34)
0.74
0.17
HL Behaviors
17
58.82 (6.31)
6
58.83 (7.14)
11
58.82 (6.18)
0.02 (-7.03, 7.06)
1.00
0
BIPS
17
27.94 (4.55)
6
27.67 (5.28)
11
28.09 (4.37)
-0.42 (-5.5, 4.65)
0.86
-0.09
PHQ 9
17
4.41 (3.62)
6
3.00 (2.1)
11
5.18 (4.12)
-2.18 (-6.05, 1.68)
0.25
-0.61
GAD 7
17
5.24 (2.88)
6
4.67 (1.51)
11
5.55 (3.45)
-0.88 (-4.06, 2.31)
0.57
-0.30
mHealth data • Collectively for Years 1&2
– Range of topics covered • stress, physical activity, diet, water, reminders, self-monitoring, sleep
– Coaches and participants determined frequency of SMS delivery • Participants could text “STOP” at any time to opt-out
– Tone and verbiage varied by coach-participant dyad • General, funny, sarcastic
• Yr 1 – 26 participants – Total SMS sent = 2601 – SMS per participant = 8 to 428
• Yr 2 – 16 participants – Total SMS sent = 1210 SMS – SMS per participant = 6 to 212
Time for a good night's sleep. Relax and enjoy some quiet
moments before bed without distractions!
Sweet dreams!
Dessert? Really? Even after all that
we've been through?
YACHT WEEK is right around the corner!!!
Go pump some iron today to get that hott bod :)
mHealth Lessons Learned • Personal connection is important
– Goal of SMS: to be relevant and build upon personal connection – Simplicity is important
• One size does not fit all • Need to consider user comfort level learning/using the software • Coaches could “set it and forget it” Alert fatigue • Anecdotal
– One participant received 255 SMS before texting STOP » “Don't forget to add a veggie to dinner tonight. Enjoy ”
– That same participant replied at message 225 » “Thank you for your reminders ”
• Looking ahead Yr 3 – Reduce burden to coaches and participants
• Will automate SMS support from library of general wellness content (e.g. F&V, PA, Diet)
• Participants will get 1 weekly SMS delivered • Participants will get 1 monthly SMS assessing contact with health coach
Conclusion - Yrs 1 & 2 • Findings support the need to screen entering health sciences
students for depression, anxiety, healthy lifestyle beliefs and behaviors along with obtaining BMI and a biometric screen, although these strategies alone are not likely to result in improvements in outcomes
• Students with elevated depressive and anxiety symptoms need to receive evidence-based interventions, specifically cognitive-behavioral therapy (CBT) based programs
• Health coaching can not only improve outcomes in those
being coached, but also those who are coaching • Intervention studies are needed to determine the best healthy
lifestyle interventions for health sciences students
The 7-session COPE Cognitive Behavioral Therapy-based Program will be delivered to students with elevated anxiety
and/or depressive symptoms
CBT Consists of cognitive restructuring, problem solving and behavioral change
The thinking/feeling/behaving triangle
Feeling
Thinking
Behaving
STRESSOR (Activator) ↓
NEGATIVE THOUGHT TO STOP (Belief)
↓
REPLACE THE NEGATIVE WITH A POSITIVE THOUGHT
↓ POSITIVE EMOTION &
BEHAVIOR
The ABCs are Taught in the COPE CBT Program
An essential component of CBT, allows the individual to put into practice the skills they are learning Skills Building or Homework reinforces the content and allows practicing of the skills
Skills Building Activities in COPE
A Sustainable Culture of Wellness
is Being Built at Ohio State
Remember, Culture Eats Strategy!
In God We Trust, Everyone Else
Must Bring Data!
Our Tactics Must be Evidence-based

Students Sit for Prolonged Periods of Time - More Movement Recovery
Breaks are Needed
The College of Nursing’s Faculty Wellness Toolbox
• Designed for faculty by faculty with the goal of incorporating wellness into curricula
• Contains 11 sections • Provides quick links and resources
for faculty to use in their courses • OSU faculty can be provided
access by emailing CON
The College of Nursing’s Faculty
Wellness Toolbox
• Exercise/movement
• Self care • Mental Health • Nutrition • Hydration • Sleep
• Crazy Inspiring stuff • Maximize study activities • Time management • Seasonal • Faculty Wellness
Resources

We do have time for wellness!

We must prioritize self-care with our students as much as taking great care of others and we need to role model
wellness
The Dream
All faculty, staff, students and clinicians excited about coming to work/school