Embed Size (px)
Citation preview

BRIEF REPORT
Prophylactic Topically Applied Ice to PreventCutaneous Complications of Nontarget
Chemoembolization and Radioembolization
David S. Wang, MD, John D. Louie, MD, Nishita Kothary, MD,Rajesh P. Shah, MD, and Daniel Y. Sze, MD, PhD
ABSTRACT
Cutaneous complications can result from nontarget deposition during transcatheter arterial chemoembolization or radioembolization.
Liver tumors may receive blood supply from parasitized extrahepatic arteries (EHAs) that also perfuse skin or from hepatic arteries
located near the origin of the falciform artery (FA), which perfuses the anterior abdominal wall. To vasoconstrict cutaneous
vasculature and prevent nontarget deposition, ice packs were topically applied to at-risk skin in nine chemoembolization treatments
performed via 14 parasitized EHAs, seven chemoembolization treatments near the FA origin, and five radioembolization treatments in
cases in which the FA could not be prophylactically coil-embolized. No postprocedural cutaneous complications were encountered.
ABBREVIATIONS
EHA = extrahepatic artery, FA = falciform artery, HCC = hepatocellular carcinoma, ICA = intercostal artery, IMA = internalmammary artery, IPA = inferior phrenic artery
Transcatheter arterial chemoembolization and radioemboliza-
tion are technically demanding locoregional palliative treat-
ment options for primary liver tumors and liver-dominant
metastatic disease. Although uncommon, cutaneous complica-
tions from chemoembolization or radioembolization include
rash, pain, induration, ulceration, and necrosis caused by
nontarget delivery of chemoembolic agents or yttrium-90
(90Y) microspheres to terminal arterial branches supplying
skin (1,2).
Skin complications from transcatheter arterial therapies
are of particular concern in two scenarios. First, liver
tumors, especially if peripherally located or large, can
develop collateral blood supply parasitized from extrahepa-
tic arteries (EHAs) in 17%–27% of patients (3,4). Trans-
catheter arterial chemoembolization through parasitized
EHAs has been demonstrated to be an effective treatment
to control hepatic tumors (3–6), but may result in cutaneous
& SIR, 2013
J Vasc Interv Radiol 2013; 24:596–600
http://dx.doi.org/10.1016/j.jvir.2012.12.020
From the SIR 2012 Annual Meeting.
None of the authors have identified a conflict of interest.
From the Division of Interventional Radiology, Department of Radiology,
Stanford University Medical Center, 300 Pasteur Drive, H3630, Stanford, CA
94305-5642. Received November 12, 2012; final revision received and
accepted December 21, 2012. Address correspondence to D.S.W.; E-mail:
complications when involving the intercostal artery (ICA)
(1,5), internal mammary artery (IMA) (1,4,6), or inferior
phrenic artery (IPA) (7). Second, the falciform artery (FA),
which is visualized in 2%–25% of angiographic studies,
arises as a branch of the left or middle hepatic artery,
courses through the falciform ligament, and provides blood
supply to the anterior abdominal wall between the xiphoid
process and umbilicus (8). Administration of chemoembolic
agents (8,9) or 90Y microspheres (2,10) proximal to or in
proximity to the FA can result in skin complications. If the
FA is identified prospectively, prophylactic coil emboliza-
tion can be performed before chemoembolization (11) or
radioembolization (2,10), but this may not be possible if the
FA is diminutive or tortuous.
In such situations in which there was a recognized risk
for cutaneous complications, we applied topical ice packs
to the skin region susceptible to nontarget deposition to
induce vasoconstriction of the cutaneous vasculature (12)
and to limit dermal injury. We retrospectively studied the
outcomes after use of this simple adjunctive maneuver.
MATERIALS AND METHODS
Institutional review board approval was granted for this
retrospective study. All data were managed in accordance
with the Health Insurance Portability and Accountability
Act. A keyword database search of the radiology informatics
system was performed to identify chemoembolization and

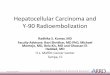
Figure 1. Images from a 65-year-old patient with HCC andresidual viable tumor in the anterolateral right hepatic lobe afterprevious transcatheter arterial chemoembolization. (a) Arterio-gram of the right 10th ICA revealed parasitized EHAs supplyinghypervascular tumor in the liver (arrows). Chemoembolizationwas performed via a microcatheter positioned near the origin ofthese parasitized branches, without topical application of icepacks. (b) Postembolization arteriogram showed stasis in theparasitized EHAs and avid uptake of chemoembolic emulsion(asterisk) and marked increase in prominence of musculocuta-neous chest wall branches (arrows), the normal and onlyresidual outflow of the ICA. This patient developed a painfulskin rash along the lateral right chest wall 2 days after theprocedure.
Table 1 . Demographic and Treatment Details of ProceduresPerformed with Topical Ice Packs Applied to At-risk SkinTerritories
Characteristic Value
Per patient (N ¼ 19)
Age (y)
Volume 24 ’ Number 4 ’ April ’ 2013 597
radioembolization procedures performed from October 2000
to October 2012 in which ice was topically applied.
Procedural digital subtraction angiography and cone-beam
C-arm computed tomography (CT) images and medical
records were retrospectively reviewed. Transcatheter arterial
chemoembolization and radioembolization techniques have
been previously described (13,14). Cone-beam C-arm CT
has been used routinely in these procedures since
March 2007.
In patients with parasitized EHAs, tumors were treated
with only chemoembolization, whereby chemoembolic mate-
rials were superselectively delivered directly into the EHAs
via a microcatheter. Chemoembolic materials consisted of
doxorubicin and/or cisplatinum solutions emulsified with
ethiodized oil (Ethiodol; Savage Laboratories, Melville,
New York; or Lipiodol; Guerbet, Villepinte, France), with
gelatin foam slurry or particulate embolic agents added when
arterioportal or arteriovenous shunting was detected; or drug-
eluting beads (100–300-mm LC Bead loaded with doxorubi-
cin; Biocompatibles, Oxford, Connecticut). The suspected
parasitized EHA was first evaluated by digital subtraction
angiography and/or contrast-enhanced cone-beam C-arm CT
imaging. If cutaneous branches originating from the EHA
were identified and the best achieved microcatheter position
for planned delivery was still deemed to present high risk
for nontarget embolization (Fig 1), plastic bags of crushed
or small cubed ice were topically applied to the skin in
the distribution of the identified cutaneous branches at least
10 minutes before and during transcatheter administration of
the chemoembolic materials. Arteriography was repeated
after topical application of ice and before chemoembolization
to assess for vasoconstriction.
In chemoembolization and radioembolization procedures
in which the FA was visualized angiographically and
susceptible to nontarget delivery but could not be prophy-
lactically coil-embolized, ice packs were applied to the
supraumbilical anterior abdominal wall in an identical
fashion before administration of chemoembolic materials
or 90Y microspheres (SIR-Sphere; Sirtex Medical, Lane
Cove, Australia; or TheraSphere; Nordion, Ottawa, Ontario,
Canada).
Mean 58.7Range 41–79
Sex
Male 13 (68.4)
Female 6 (31.6)
Liver tumor type
Hepatocellular carcinoma 15 (82.4)
Metastases (colorectal, thyroid, renal carcinoma) 4 (17.6)
Per procedure (N ¼ 21)
Chemoembolization
Parasitized extrahepatic arteries 9 (47.4)
Segment 4 arteryn 7 (31.6)
Radioembolization of LHA/segmental branchn 5 (21.1)
Values in parentheses are percentages.LHA ¼ left hepatic artery.n Falciform artery not prophylactically embolized.
RESULTS
Prophylactic topical application of ice packs was used to
prevent cutaneous complications in 16 transcatheter arterial
chemoembolization and five radioembolization procedures
in 19 patients (two underwent chemoembolization with
topical ice packs twice; Table 1). Mean patient age was
58.7 years (range, 41–79 y); 13 (68%) were men. Fifteen
patients (79%) were treated for hepatocellular carcinoma
(HCC) and the remaining four were treated for hepatic
metastases.
Nine procedures were transcatheter arterial chemoembo-
lization treatments delivered through 14 parasitized EHAs.
Parasitized EHAs included the right ICA (n ¼ 8; T8 to

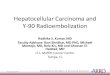
Figure 2. Images from a 51-year-old patient with HCC andresidual viable tumor along the lateral aspect of a segment6 lesion previously treated with transcatheter arterial chemoem-bolization. (a) Arteriogram of the right 11th ICA demonstrateda parasitized EHA supplying hypervascular tumor (arrow).(b) Fluoroscopic image after chemoembolization performedwith topical application of ice packs (note diffuse artifact) andthe microcatheter advanced into the parasitized branch vesselshowed uptake by the lesion (arrow). A static column ofcontrast medium was seen within a superficial side-branchvessel (arrowhead), reflecting hypothermia-induced vasocon-striction. This patient experienced no cutaneous complications.
Wang et al ’ JVIR598 ’ Ice to Prevent Cutaneous Complications of Nontarget Embolization
T11; Fig 2), right IMA (n ¼ 3; Fig 3), right IPA (n ¼ 2),
and left IMA (n ¼ 1; Table 2). These patients had
undergone an average of 3.6 previous chemoemboliza-
tions (range, two to six). Two patients exhibited occlusion
or severe attenuation of the hepatic arteries from previous
treatments.
Of the 12 cases in which the FA was visualized (Fig 4) but
prophylactic coil embolization was not feasible, seven were
chemoembolization procedures in which chemoembolic
agents were delivered in close proximity to the FA origin
and five were radioembolization administrations (SIR-
Sphere, n ¼ 3; TheraSphere, n ¼ 2) via the left hepatic
artery or a segmental branch proximal to the FA. As
comparison, prophylactic embolization of the FA was
successful in 20 chemoembolization or radioembolization
procedures performed during the same period of review.
Median follow-up was 5.7 months (range, 1.7–20.9 mo).
A minimum of 6 weeks follow-up—the period during
which cutaneous complications would be expected to
manifest—was obtained for all patients. Review of medical
records revealed no cutaneous complications in any patient.
All patients tolerated topical application of ice, but a few
required additional intravenous sedative medications
because of the discomfort caused by the cold ice. There
were no hypothermia-related adverse reactions, and
patients were kept warm and sedated enough to avoid
shivering and motion degradation of intraprocedural
imaging.
In the nine chemoembolization treatments of parasitized
EHAs in which skin-supplying vessels were identified,
arteriography performed after topical application of ice
demonstrated slower flow or stasis in superficial cutaneous
vessels and decreased body wall enhancement, with pre-
servation of flow into deeper parasitized arteries supplying
tumor (Fig 2b). Completion unenhanced cone-beam C-arm
CT was performed in 13 of the 16 chemoembolization
procedures; none showed evidence of nontarget uptake in
the at-risk skin or subcutaneous tissues (Fig 3c).
DISCUSSION
The principal technical objective of transcatheter arterial
interventions for hepatic malignancies is to deliver cyto-
toxic or radioactive agents selectively to tumors while
minimizing deposition in adjacent nonmalignant hepatic
and extrahepatic tissues. Safe and complete treatment
typically requires detailed angiographic evaluation of the
arterial pathways, use of microcatheters for superselective
catheterization of specific tumor-feeding arteries, and care-
ful administration of the therapeutic agents under vigilant
fluoroscopic monitoring to detect and prevent reflux.
Cutaneous complications can occur when the therapeutic
agents are delivered through or in proximity to an artery
that normally provides branches supplying skin and there is
inadvertent deposition in the terminal cutaneous branches
(1,2). Skin injury is thought to be caused by direct dermal
exposure to chemotherapeutic drugs or to b-irradiation,
possibly exacerbated by ischemia (1,9,10). Most skin
complications are mild and transient, and can be treated
with topical agents such as silver-containing ointments or
local corticosteroid injections. More severe complications
may present as fat and dermal necrosis and ulceration,
which may be complicated by infection. These severe cases
may require surgical debridement and/or skin grafting
(1,4,10).
Cutaneous complications can occur following trans-
catheter arterial chemoembolization of parasitized EHAs
originating from the ICA (1,5), IMA (1,4,6), and IPA (7),
as well as transcatheter arterial chemoembolization (8,9)
and radioembolization procedures (2,10) in which delivery
is performed proximal or in proximity to a patent FA. We
have described a simple, safe, and inexpensive method that
may reduce the risk of cutaneous nontarget chemoembo-
lization and radioembolization by using local hypothermia
to induce vasoconstriction of the superficial cutaneous
vasculature (12). Angiography confirmed decreased flow
into the at-risk skin, and completion cone-beam C-arm CT
showed no deposition of radiopaque agents in the at-risk
territories. On follow-up, there were no cutaneous compli-
cations following these high-risk procedures.
Although the present study did not have a control arm,
historical published data show that skin necrosis or
erythema occurred in 16.7% of patients who underwent
chemoembolization via parasitized ICAs (5) and in 8.9% of
patients who underwent chemoembolization via parasitized
IMAs (6). Although the right IPA is the most common

Figure 3. Images from a 54-year-old patient with medullary thyroid carcinoma and hepatic metastases supplied by parasitized EHAs.(a) Arteriogram of right IMA revealed multiple parasitized EHAs supplying several intrahepatic hypervascular tumors (arrows).(b) Maximum-intensity projection image reconstructed from cone-beam C-arm CT with contrast medium administered via the rightIMA demonstrated arterial supply to hypervascular lesions in the anterior right lobe (asterisk) and prominent branches supplying theright breast (arrow). Superselective transcatheter arterial chemoembolization was performed with topical ice packs applied to the rightbreast and anterior chest wall. (c) Maximum-intensity projection image reconstructed from completion unenhanced cone-beam C-armCT showed no uptake of the ethiodized oil emulsion in the right breast and overlying skin. This patient showed no symptoms ofcutaneous or chest wall deposition.
Volume 24 ’ Number 4 ’ April ’ 2013 599
source of parasitized collateral vessels to supply liver
tumors (3), to our knowledge, only one case of skin
complication following chemoembolization has been
reported (7). Although the IPA predominantly supplies
the diaphragm, it also provides branches that anastomose
with the ICA and IMA, which may allow for inadvertent
shunting of chemoembolic agents to the skin.
Just as individual parasitized branches supplying tumors
may be too small to select with microcatheters for
superselective treatment, cutaneous branches may also be
too numerous or small to coil or bland embolize for
prophylaxis. Some authors advocate for bland embolization
of parasitized EHAs as a safer alternative to chemoembo-
lization (4,6), particularly when superselective catheteriza-
tion of the tumor-supplying collateral vessels is not
possible. Our method of using topical ice packs to prevent
cutaneous complications may allow for safer use of
cytotoxic agents to exploit their possible improved efficacy.

Table 2 . Distribution of Parasitized EHAs Treated withChemoembolization with Ice Packs Applied (n ¼ 14)
Parasitized EHA Treated Arteries
Right intercostal artery 8 (57.1)
T8 2
T9 3
T10 1
T11 2
Right IMA 3 (21.4)
Right IPA 2 (14.3)
Left IMA 1 (7.1)
Values in parentheses are percentages.EHA ¼ extrahepatic artery, IMA ¼ internal mammary artery,IPA ¼ inferior phrenic artery.
Wang et al ’ JVIR600 ’ Ice to Prevent Cutaneous Complications of Nontarget Embolization
Another potential indication for the topical application
of ice is during chemoembolization or radioembolization
administration when there is a patent FA that cannot be
prophylactically embolized, which may result in nontarget
deposition in the anterior abdominal wall. The FA origin
may be tortuous, diminutive, duplicated, or even a diffuse
network, precluding selective catheterization and prophy-
lactic embolization. Although there is near-consensus in
favor of prophylactic microcoil embolization of a visua-
lized FA before radioembolization (2), prophylactic
embolization of a patent FA before chemoembolization
remains controversial because severe complications are
uncommon (15).
Limitations of the present retrospective study include
the small sample size and absence of a control group
Figure 4. Image from a 60-year-old patient with focal HCC inthe dome of segment 4a. Three-dimensional volume surfacerendering of cone-beam C-arm CT with contrast mediuminjected into the proper hepatic artery showed the segment 4atumor (arrowhead). The FA originated from the segment 4aartery and coursed toward the midline anterior abdomen(arrow). Its origin was extremely tortuous in this patient withcirrhosis and could not be catheterized for prophylactic coilembolization. Ice packs were topically applied as a chemother-apy–ethiodized oil emulsion was delivered just distal to the FAorigin. No cutaneous complications resulted.
for comparison. In addition, criteria for when to apply
ice and what was considered to represent high risk
for cutaneous complications were not prospectively or
strictly defined.
In conclusion, topical application of ice packs to
vasoconstrict superficial arterial branches when the skin
is susceptible to nontarget deposition of chemoembolic
agents or 90Y microspheres may provide an additional
measure of safety in the prevention of cutaneous complica-
tions. It should be considered specifically when transcath-
eter arterial chemoembolization is performed through
parasitized EHAs involving the ICA, IMA, and IPA, and
in chemoembolization and radioembolization administra-
tions in which a patent FA is visualized and cannot be
prophylactically embolized.
REFERENCES
1. Arora R, Soulen MC, Haskal ZJ. Cutaneous complications of hepatic
chemoembolization via extrahepatic collaterals. J Vasc Interv Radiol
1999; 10:1351–1356.
2. Riaz A, Lewandowski RJ, Kulik LM, et al. Complications following
radioembolization with yttrium-90 microspheres: a comprehensive litera-
ture review. J Vasc Interv Radiol 2009; 20:1121–1130.
3. Kim HC, Chung JW, Lee W, Jae HJ, Park JH. Recognizing extrahepatic
collateral vessels that supply hepatocellular carcinoma to avoid complica-
tions of transcatheter arterial chemoembolization. Radiographics 2005;
25(suppl):S25–S39.
4. Miyayama S, Matsui O, Taki K, et al. Extrahepatic blood supply to
hepatocellular carcinoma: angiographic demonstration and transcatheter
arterial chemoembolization. Cardiovasc Intervent Radiol 2006; 29:
39–48.
5. Park SI, Lee DY, Won JY, Lee JT. Extrahepatic collateral supply of
hepatocellular carcinoma by the intercostal arteries. J Vasc Interv Radiol
2003; 14:461–468.
6. Kim HC, Chung JW, Choi SH, et al. Hepatocellular carcinoma with
internal mammary artery supply: feasibility and efficacy of transarterial
chemoembolization and factors affecting patient prognosis. J Vasc Interv
Radiol 2007; 18:611–619.
7. Brennan DD, Farrelly C, Cooney R, Norris S, McEniff N. Abdominal rash
after transarterial chemoembolization via the right inferior phrenic artery.
J Vasc Interv Radiol 2005; 16:1269.
8. Gibo M, Hasuo K, Inoue A, Miura N, Murata S. Hepatic falciform artery:
angiographic observations and significance. Abdom Imaging 2001; 26:
515–519.
9. Baysal T, D’Agostino HB, Serra EE, Valji K, Rose SC, Kinney TB.
Supraumbilical dermal sclerosis and fat necrosis from chemoemboliza-
tion of hepatocellular carcinoma. J Vasc Interv Radiol 1998; 9:645–647.
10. Leong QM, Lai HK, Lo RG, Teo TK, Goh A, Chow PK. Radiation
dermatitis following radioembolization for hepatocellular carcinoma: a
case for prophylactic embolization of a patent falciform artery. J Vasc
Interv Radiol 2009; 20:833–836.
11. Ueno K, Miyazono N, Inoue H, Miyake S, Nishida H, Nakajo M. Embo-
lization of the hepatic falciform artery to prevent supraumbilical skin rash
during transcatheter arterial chemoembolization for hepatocellular carci-
noma. Cardiovasc Intervent Radiol 1995; 18:183–185.
12. Johnson JM, Kellogg DL Jr. Local thermal control of the human
cutaneous circulation. J Appl Physiol 2010; 109:1229–1238.
13. Tognolini A, Louie JD, Hwang GL, Hofmann LV, Sze DY, Kothary N.
Utility of C-arm CT in patients with hepatocellular carcinoma undergoing
transhepatic arterial chemoembolization. J Vasc Interv Radiol 2010; 21:
339–347.
14. Louie JD, Kothary N, Kuo WT, et al. Incorporating cone-beam CT into
the treatment planning for yttrium-90 radioembolization. J Vasc Interv
Radiol 2009; 20:606–613.
15. Kim DE, Yoon HK, Ko GY, Kwon JS, Song HY, Sung KB. Hepatic
falciform artery: Is prophylactic embolization needed before short-
term hepatic arterial chemoinfusion? Am J Roentgenol 1999; 172:
1597–1599.