Embed Size (px)
Citation preview

Prophylaxis of febrile neutropenia :experiences with adjuvant TAC
30th Apr, 2016 Jihyoun Lee Breast center, Department of Surgery Soonchunhyang University Hospital

Chemotherapy and the risk of febrile neutropenia
G-CSF administration in current guidelines
Prophylaxis of febrile neutropenia in breast cancer treatment
Experiences of long-acting G-CSF

Neutrophils
• First line of defense against the bacterial pathogens • Immediately able to recognize, attack, and kill invading organisms
• Recruits other cells Promotes inflammation Phagocytosis

Kolaczkowska et al. Nat Rev Immunol 2013

Chemotherapy and the immune system
• The administration of chemotherapy
Decrease the number of neutrophils Produce chemotactic and phagocytic defects
• Prolonged neutropenia is related to risk of infection • The risk of infection can be modified by Alterations of physical defense barriers patient’s cellular or humoral immune system Endogenous microflora
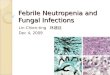
Lambertini et al. Expert Opi Biol Ther 2015
Mitotic pool Sensitivity to CT: very high Sensitivity to G-CSF: moderate
Maturation pool Sensitivity to CT: moderate Sensitivity to G-CSF: very high
Peripheral pool Sensitivity to CT: No Sensitivity to G-CSF: High

Toxicity grading for neutropenia
Toxicity Grade Definition
Grade 1 Mild ANC < LLN to 1.5 x 109/L
Grade 2 Moderate ANC < 1.5 to 1.0 x 109/L
Grade 3 Severe ANC < 1.0 to 0.5 x 109/L
Grade 4 Life threatening ANC < 0.5 x 109/L*
ANC, absolute neutrophil count; LLN, lower limit of normal. Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. Published June 14, 2010

Fever may be the sole Sx of infection
• Fever may not be present
in neutropenic infection: Steroids NSAIDs Clostridium septicum • endogenous cytokines (IL-6
and TNF) are released with the possible development of fever even in the absence of infection

Febrile Neutropenia(FN)
• Febrile neutropenia is defined as a single temperature of >38.3 °C (101 ° F) orally or sustained temperature of ≥38.0 °C (100.4 ° F) over >1 h <500 neutrophils/mcL or <1,000 neutrophils/mcL and a predicted decline to ≤500/mcL over the next 48 hours
NCCN guidelines ver. 1 2016
Myeloid growth factors

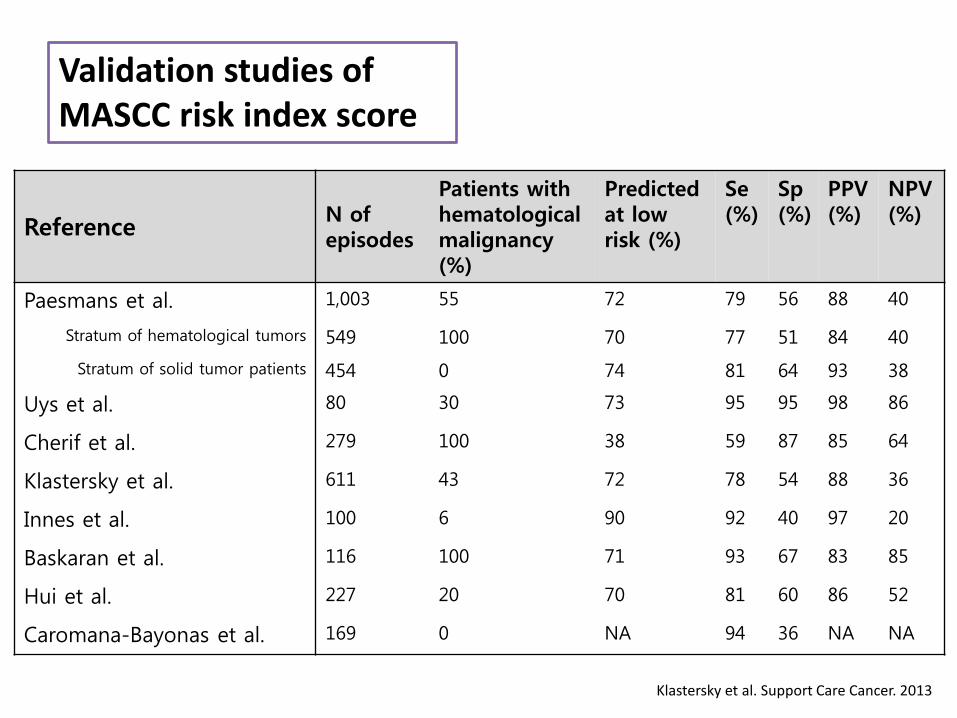
Chemotherapy regimens with a high risk of febrile neutropenia (>20%) CHEMOTHERAPY REGIMEN EORTC NCCN Doxorubicin, cyclophosphamide→docetaxel √
Docetaxel→doxorubicin, cyclophosphamide √
Doxorubicin and docetaxel √ √
Doxorubicin and paclitaxel √ √
Docetaxel, doxorubicin, and cyclophosphamide (TAC) √ √
DDb fluorouracil, epirubicin, and cyclophosphamide (FEC) √
DDb doxorubicin, cyclophosphamide, and paclitaxel (ACT) √ √
Docetaxel and trastuzumab √
Doxorubicin and cyclophosphamide (AC) √
Epirubicin and cyclophosphamide (EC) √
Doxorubicin, cyclophosphamide→docetaxel and trastuzumab √
Docetaxel √
Epirubicin √
Cyclophosphamide, methotrexate, and fluorouracil (CMF classic) √
Fluorouracil, epirubicin, and cyclophosphamide (FEC)→docetaxel √ √
Cyclophosphamide, epirubicin, and 5-FU (CEF) √
Capecitabine and docetaxel √
Cortes de Miguel et al. Support Care Cancer. 2015

Bozeuk et al. Support Care Cancer. 2015
Individual risk of FN
development of febrile neutropenia after a specific cycle of chemotherapy:

Identification of high risk patients
• The Multinational Association for Supportive
Care in Cancer(MASCC) risk index score a scoring system for identifying low-risk cancer patients with febrile neutropenia
(Klastersky et al. 2000)
• Predicting model for risk of neutropenic complications
clinical and biological parameters chemotherapy characteristics
(Lyman et al., 2011)
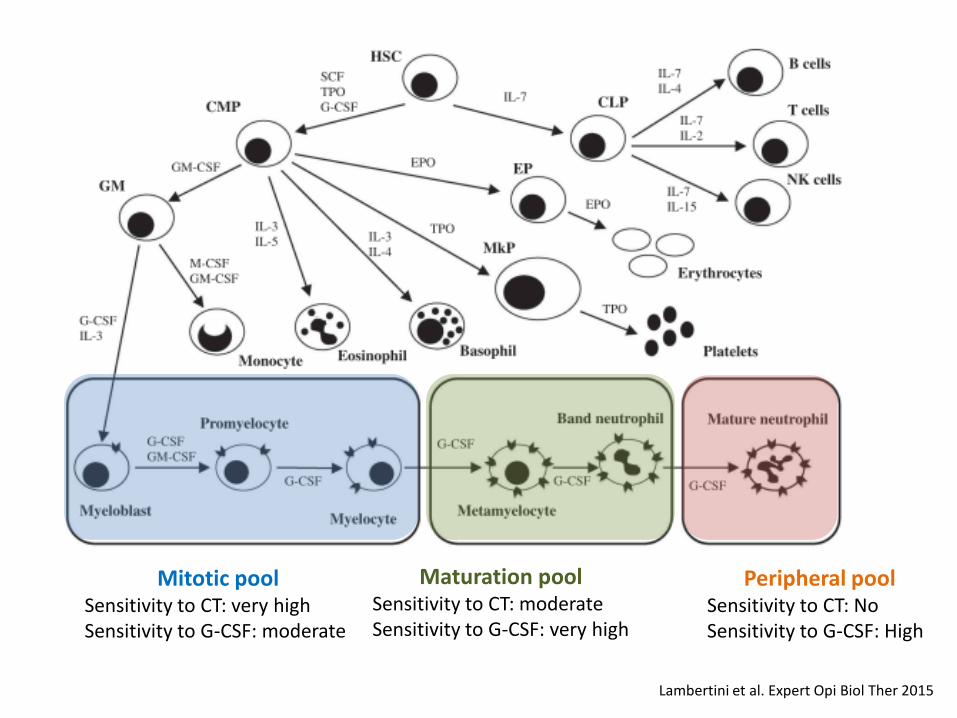
Validation studies of MASCC risk index score
Klastersky et al. Support Care Cancer. 2013
Reference N of episodes
Patients with hematological malignancy (%)
Predicted at low risk (%)
Se (%)
Sp (%)
PPV (%)
NPV (%)
Paesmans et al. 1,003 55 72 79 56 88 40
Stratum of hematological tumors 549 100 70 77 51 84 40
Stratum of solid tumor patients 454 0 74 81 64 93 38
Uys et al. 80 30 73 95 95 98 86
Cherif et al. 279 100 38 59 87 85 64
Klastersky et al. 611 43 72 78 54 88 36
Innes et al. 100 6 90 92 40 97 20
Baskaran et al. 116 100 71 93 67 83 85
Hui et al. 227 20 70 81 60 86 52
Caromana-Bayonas et al. 169 0 NA 94 36 NA NA

Multinational Association for Supportive Care in Cancer(MASCC) risk index score
MASCC Risk Index Factors and Weights CHARACTERISTIC WEIGHT
Burden of febrile neutropenia with no or mild symptoms 5
No hypotension (systolic BP>90 mmHg) 5
No chronic obstructive pulmonary disease 4
Solid tumor or hematological malignancy with no previous fungal infection 4
No dehydration requiring parenteral fluids 3
Burden of febrile neutropenia with moderate symptoms 3
Outpatients status 3
Age <60 years 2
<21

Identification of high risk patients
• Measurement of procalcitonin, CRP, IL-6 potential useful markers predicting severe infection in FN PCT had the best positive likelihood ratio
(Wu et al., 2015)
• Prognostic model for FN (Ahn et al., 2015)

Chemotherapy and the risk of febrile neutropenia
G-CSF administration in current guidelines
Prophylaxis of febrile neutropenia in breast cancer treatment
Experiences of long-acting G-CSF

The role of G-CSF
• G-CSF plays a central role in neutrophil formation
• Usually levels are low but may be increased during infections or
inflammatory status
• Enhances the proliferation and differentiation of neutrophils from progenitor cells
• Increase the survival and function of mature neutrophils resulting in peripheral neutrophilia

Lambertini et al. Expert Opi Biol Ther 2015
Mitotic pool Sensitivity to CT: very high Sensitivity to G-CSF: moderate
Maturation pool Sensitivity to CT: moderate Sensitivity to G-CSF: very high
Peripheral pool Sensitivity to CT: No Sensitivity to G-CSF: High

The role of G-CSF
• The use of G-CSFs before cytotoxic therapy should be avoided
since it renders the mitotic pool highly sensitive to chemotherapy
• all major guidelines recommend the use of G-CSFs 24 – 72 h after chemotherapy administration

Recombinant G-CSF
Lambertini et al. Expert Opi Biol Ther 2015
Balugrastim Empegfilgrastim

Pegylation: daily vs long acting G-CSF
Pegfilgrastim (Neulasta®) covalent attachment of a monomethoxy polyethylene glycol chain to the filgrastim Escape from renal clearance “self regulating” clearance by neutrophil
Filgrastim Recombinant methionyl human G-CSF

Pegylation: daily vs long acting G-CSF
Green et al. J Clin Oncol 2003
Pegfilgrastim serum level vs ANC after single 6-mg Neulasta® dose
Serum concentration of Pegfilgrastim(Neulasta®)
ANC level

Filgrastim Pegfilgrastim (Neulasta®) Structure Human G-CSF produced by
recombinant DNA technology
Polyethylene glycol molecule bound to N-terminal of filgrastim
Pharmacokinetics Elimination half-life: Approximately 3.5 h
Elimination half-life: 15–80 h after subcutaneous injection
Dosing Starting dose of 5mcg/kg/day as a single daily injection by subcutaneous (SC) bolus, short IV infusion, or continuous SC or IV infusion
Once-per-cycle injections - A single subcutaneous injection of 6 mg administered once per cycle in adults
Clearance Primarily renal Pegylation enables self-regulating, neutrophil-mediated clearance
Cortes de Miguel et al. Support Care Cancer 2015

Pegylation: daily vs long acting G-CSF
Pegfilgrastim (Neulasta®) • Pegylation of filgrastim leads to reduced renal clearance and
sustained plasma concentration, which result in: Once-per-cycle subcutaneous dosing Self-regulated neutrophil-mediated clearance Given as a 6-mg fixed dose appropriate for adult patients across a wide range of body weights (≥ 45 kg) Given once per cycle and should not be administered in the period between 14 days before and 24 h after cytotoxic chemotherapy

Toxicity risks with myeloid growth factors
• Acute respiratory distress syndrome (ARDS) • Allergic reactions • Alveolar hemorrhage and hemoptysis • Bleomycin-containing regimens: pulmonary toxicity • Severe sickle cell crises • Splenic rupture • MDS and AML • Bone pain and pain in extremity

Mechanisms of bone pain
Lambertini et al. Crit Rev Oncol Hematol 2014

Lambertini et al. Crit Rev Oncol Hematol 2014

Pegylation: daily vs long acting G-CSF
Green et al. J Clin Oncol 2003
Pegfilgrastim
Daily filgrastim
• Doxorubicin and docetaxel(60 mg/m2 and 75 mg/m2)

Primary vs secondary prophylaxis
• Primary prophylaxis First and subsequent-cycle use of prophylactic antibiotics or growth factors • Secondary prophylaxis Addition of growth factors for patients who experienced a neutropenic complication from a prior cycle of chemotherapy (for which primary prophylaxis was not received)

Primary prophylaxis
• Primary prophylaxis Prevent FN, hospitalizations, infection-related deaths. Prophylactic use of G-CSF reduces the incidence, length, and severity of chemotherapy-induced neutropenia in breast cancer patients.

Lambertini et al. Expert Opi Biol Ther 2015

Primary prophylaxis

Chemotherapy and the risk of febrile neutropenia
G-CSF administration in current guidelines
Prophylaxis of febrile neutropenia in breast cancer treatment
Experiences of long-acting G-CSF

FN is related to RDI
NCCN guidelines ver. 1 2016 Myeloid growth factors

Reduced RDI and worse prognosis
HR,1.65; 95% CI, 1.18–2.30; p = 0.0029
HR, 1.73; 95% CI, 1.17–2.55; p = 0.0055
Overall Survival (years) Disease-Free Survival (years)
Chirivella et al. Breast Cancer Res Treat 2009
• 793 patients with early-stage breast cancer treated with anthracycline-based non-taxane adjuvant chemotherapy • Relative dose intensity (RDI) administered (≥85%, <85%).

Primary prophylaxis in breast cancer Tx
GEPATRIO study • A phase III study of neoadjuvant TAC • Primary prophylaxis of Ciprofloxacin Daily G-CSF Pegfilgrastim Pegfilgrastim+ciprofloxacin
Von Mickwitz et al. Ann Oncol 2008

Mitchell et al. J Oncol Pharm Pract. 2016
Risks of FN and FN-Related complications were generally lower for prophylaxis with pegfilgrastim versus short-acting G-CSFs
Chemotherapy regimens with a high risk of febrile neutropenia (>20%) CHEMOTHERAPY REGIMEN EORTC NCCN Doxorubicin, cyclophosphamide→docetaxel √
Docetaxel→doxorubicin, cyclophosphamide √
Doxorubicin and docetaxel √ √
Doxorubicin and paclitaxel √ √
Docetaxel, doxorubicin, and cyclophosphamide (TAC) √ √
DDb fluorouracil, epirubicin, and cyclophosphamide (FEC) √
DDb doxorubicin, cyclophosphamide, and paclitaxel (ACT) √ √
Docetaxel and trastuzumab √
Doxorubicin and cyclophosphamide (AC) √
Epirubicin and cyclophosphamide (EC) √
Doxorubicin, cyclophosphamide→docetaxel and trastuzumab √
Docetaxel √
Epirubicin √
Cyclophosphamide, methotrexate, and fluorouracil (CMF classic) √
Fluorouracil, epirubicin, and cyclophosphamide (FEC)→docetaxel √ √
Cyclophosphamide, epirubicin, and 5-FU (CEF) √
Capecitabine and docetaxel √
Cortes de Miguel et al. Support Care Cancer. 2015

Discontinuing primary prophylaxis
• Increase in cost with primary G-CSF prophylaxis • 167 patients randomized to comparing primary prophylaxis
in first 2 cycles only and throughout all cycles
Aarts et al. J Clin Oncol 2013
OR 5.4 (95% CI, 2.3 to 12.6)
TAC, FEC-D, docetaxel, TC

The Korean National Health Insurance
• Filgrastim,lenograstim - neutropenia: administer <500/mm3 to 1,000/mm3
- febrile neutropenia: administer <1,000/mm3 to 3,000/mm3
• Pegfilgrastim (Neulasta®)
pegteograstim, tripegfilgrastim, lipegfilgrastim - adjuvant TAC(docetaxel + doxorubicin + cyclophosphamide) - neoadjuvant dose-dense FEC (fluorouracil + epirubicin + cyclophosphamide)
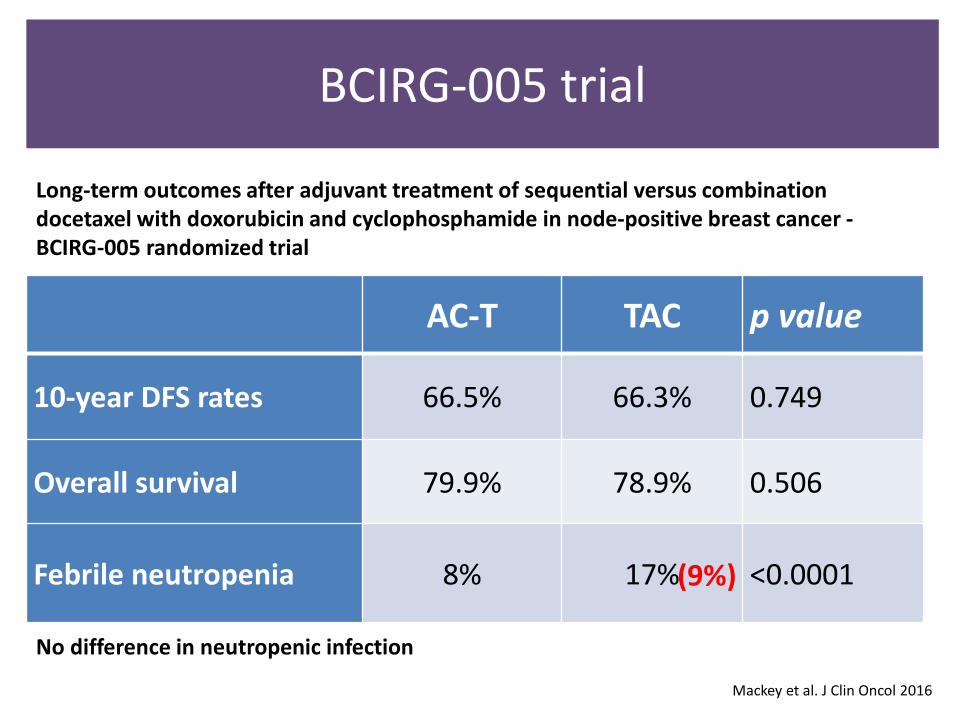
AC-T TAC p value
10-year DFS rates 66.5% 66.3% 0.749
Overall survival 79.9% 78.9% 0.506
Febrile neutropenia 8% 17% <0.0001
Mackey et al. J Clin Oncol 2016
BCIRG-005 trial
(9%)
Long-term outcomes after adjuvant treatment of sequential versus combination docetaxel with doxorubicin and cyclophosphamide in node-positive breast cancer - BCIRG-005 randomized trial
No difference in neutropenic infection

Mackey et al. J Clin Oncol 2016

Lee et al. Breast Cancer 2014
FN in Korean patients without primary prophylaxis

Chemotherapy and the risk of febrile neutropenia
G-CSF administration in current guidelines
Prophylaxis of febrile neutropenia in breast cancer treatment
Experiences of long-acting G-CSF

Woo et al. J Breast Cancer 2012
Grade 3/4 neutropenia
80 patients with adjuvant TAC (docetaxel plus doxorubicin and cyclophosphamide) (75/50/500 mg/m2 , every 3 weeks for 6 cycles)
SCH Experiences of Adjuvant TAC

SCH Experiences of Adjuvant TAC
Lee et al. Breast Cancer 2014
AC-D
TAC
Global health status(EORTC QLQ-C30)

TAC with Long-acting G-CSF(Neulasta®)
Adjuvant treatment of Node-positive breast cancer
38 patients(220 cycles) received TAC
ANC profile Day 0,2 and 5 to 10
NRS report Day 1 to 10

0
1000
2000
3000
4000
5000
6000
7000
day0 day1 day2 day3 day4 day5 day6 day7 day8 day9 day10
106±23
ANC profile and nadir

0
1000
2000
3000
4000
5000
6000
7000
day0 day1 day2 day3 day4 day5 day6 day7 day8 day9 day10
ANC profile and nadir
0
1000
2000
3000
4000
5000
6000
7000
day0 day1 day2 day3 day4 day5 day6 day7 day8 day9 day10 day11 day12 day13
235 146 90 944
662 106 606
TAC without primary prophylaxis(N=20)
(Data not shown in paper)

0
1
2
3
4
5
6
7
8
9
10
day0 day1 day2 day3 day4 day5 day6 day7 day8 day9 day10 day21
Bone pain (NRS)
Treatment-related events
• Incidence of FN: 15.7% • Incidence of reduced RDI (<85%): 2.2% • No treatment delay and treatment interruption • Neutropenic infection: 0.9% (1 pneumonia and 1 UTI)

FN in Korean patients without primary prophylaxis
15.7%

F/46 breast cancer patients Primary prophylaxis for Doxorubicin and docetaxel
• Left breast cancer with clinical stage IIIc (T3N2M0) • Doxorubicin and docetaxel chemotherapy • Primary prophylaxis of pegfilgrastim reimbursed by private insurance
1st cycle Day 0 Day 2 Day 6 Day 7 Day 8 Day9 Day10
ANC(mcl) 3,175 5,630 527 1,153 3,583 5,495
2ndcycle Day 0 Day 2 Day 6
ANC(mcl) 5,916 5,295 104
TA chemotherapy myalgia from day 5 to 7 In admission
Outpatient visit

Summary
• Patients that have high risk of complication from FN should be identified and closely monitored
• Primary prophylaxis is recommended if the risk of FN is expected
• Primary prophylaxis of FN with long-acting G-CSF was useful during TAC treatment

Thank you for your attention