Embed Size (px)
Citation preview

Prophylaxis of Rheumatic Fever
By EDWARD A. MORTIMER, JR., M.D., AND CHARLES H. RAMMELKAMP, JR., M.D.
G ROUP A streptococcal infection initiatesacute rheumatic fever; rheumatic val-vular heart disease is a sequela that
develops during or subsequent to the acuterheumatic episode. The mechanism by whichthe preceding streptococcal infection producesthe arthritic and constitutional symptoms andvalvular heart disease is unknown. Regardlessof the mechanism involved, there is little doubtthat prevention of the streptococcal infectioneliminates acute rheumatic fever and presum-ably rheumatic heart disease in any populationgroup. This fact has guided the management ofa selected group of individuals, namely thosepatients who have already had 1 attack ofrheumatic fever. The continuous prophylacticadministration of a sulfonamide drug or penicil-lin is a widely practised measure for ensuringfreedom from streptococcal infections andrheumatic recurrences.The establishment of the relationship of the
streptococcal infection to acute rheumaticfever led to the development of other methodsfor the control of rheumatic fever, since it waslogical to believe that successful treatment ofthe original streptococcal respiratory diseasemight alter the attack rate of this nonsuppura-tive complication. Treatment with sulfon-amides failed to prevent rheumatic fever" 2 inspite of the favorable influence it exerted onthe natural course of the acute respiratory ill-ness. Subsequently, penicillin was employed byMassell, Dow, and Jones3 for the therapy ofstreptococcal infections in patients who hadexperienced 1 or more rheumatic episodes andrecurrent attacks of rheumatic fever were
From the Departments of Pediatrics, Medicineand Preventive Medicine, Western Reserve Uni-versity School of Medicine and City Hospital, Cleve-land, Ohio.
This investigation was conducted under the spon-sorship of the Commission on Streptococcal Diseases,Armed Forces Epidemiological Board, and was sup-ported by the Office of The Surgeon General, Depart-ment of the Army, Washington, D. C., and Wyeth,Inc.
1144
eliminated. Similarly, initial attacks of rheu-matic fever may be prevented by successfultreatment of the streptococcal illness withpenicillin or other antibiotics.4On the basis of this and other information,
the American Heart Association' has maderecommendations for the control of rheumaticfever that are summarized in table 1. Minorchanges in the methods employed in prophy-laxis and treatment of streptococcal infectionsundoubtedly will be made as experience ac-cumulates. For example, the duration of pro-tection afforded by various doses of benzathinepenicillin has not been determined nor has thedaily oral dose of penicillin prophylaxis beenfinally established. Recent evidence' indicatesthat 1,200,000 units of benzathine penicillinwill protect against streptococcal infections for6 weeks and 900,000 units for 4 weeks. Like-wvise, oral penicillin probably should be admin-istered in doses of 200,000 units twice daily toinsure adequate prophylaxis.
It appears unlikely that major revisions inthese recommendations will be made unlessnew data become available that invalidateprevious conclusions. Recently, serious doubtshave been raised as to whether successful treat-ment of streptococcal infections does indeedprevent valvular heart disease. In addition,some physicians have questioned the desir-ability of continuing prophylaxis for life inthose individuals who have experienced 1 ormore rheumatic attacks. It is the purpose ofthe present discussion to review some of thedata and considerations presently availableregarding these 2 aspects of the problem ofrheumatic fever.
DOES TREATMENT OF THE STREPTOCOCCALINFECTION PREVENT RHEUMATIC HEARTDISEASE AS WELL AS SYMPTOMS OF ACUTERHEUMATIC FEVER?It is apparent from various studies that
treatment of the streptococcal illness results ina decreased incidence of the clinical manifesta-
Circulation, Volume XI V, December 1956
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from
PROPHYLAXIS OF RHEUMATIC FEVER
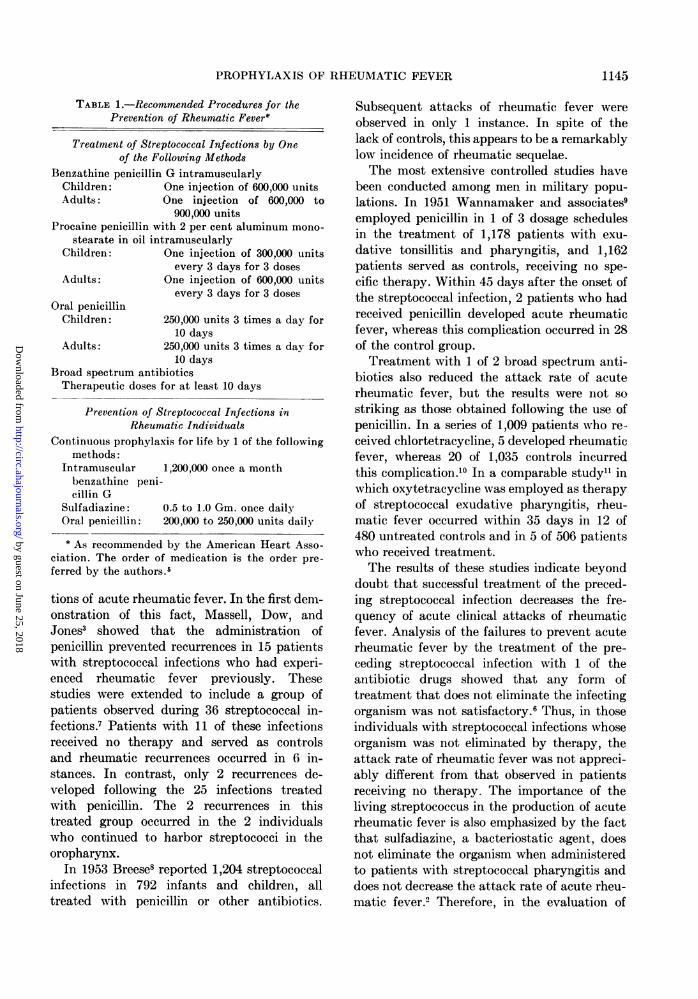
TABLE 1.-Recommended Procedures for thePrevention of Rheumatic Fever*
Treatment of Streptococcal Infections by Oneof the Following Methods
Benzathine penicillin G intramuscularlyChildren: One injection of 600,000 unitsAdults: One injection of 600,000 to
900,000 unitsProcaine penicillin with 2 per cent aluminum mono-
stearate in oil intramuscularlyChildren: One injection of 300,000 units
every 3 days for 3 dosesAdults: One injection of 600,000 units
every 3 days for 3 dosesOral penicillin
Children: 250,000 units 3 times a day for10 days
Adults: 250,000 units 3 times a day for10 days
Broad spectrum antibioticsTherapeutic doses for at least 10 days
Prevention of Streptococcal Infections inRheumatic Individuals
Continuous prophylaxis for life by 1 of the followingmethods:
Intramuscular 1,200,000 once a monthbenzathine peni-cillin G
Sulfadiazine: 0.5 to 1.0 Gm. once dailyOral penicillin: 200,000 to 250,000 units daily
* As recommended by the American Heart Asso-ciation. The order of medication is the order pre-ferred by the authors.5
tions of acute rheumatic fever. In the first dem-onstration of this fact, Massell, Dow, andJones3 showed that the administration ofpenicillin prevented recurrences in 15 patientswith streptococcal infections who had experi-enced rheumatic fever previously. Thesestudies were extended to include a group ofpatients observed during 36 streptococcal in-fections.7 Patients with 11 of these infectionsreceived no therapy and served as controlsand rheumatic recurrences occurred in 6 in-stances. In contrast, only 2 recurrences de-veloped following the 25 infections treatedwith penicillin. The 2 recurrences in thistreated group occurred in the 2 individualswho continued to harbor streptococci in theoropharynx.
In 1953 Breese8 reported 1,204 streptococcalinfections in 792 infants and children, alltreated with penicillin or other antibiotics.
Subsequent attacks of rheumatic fever wereobserved in only 1 instance. In spite of thelack of controls, this appears to be a remarkablylow incidence of rheumatic sequelae.The most extensive controlled studies have
been conducted among men in military popu-lations. In 1951 Wannamaker and associates9employed penicillin in 1 of 3 dosage schedulesin the treatment of 1,178 patients with exu-dative tonsillitis and pharyngitis, and 1,162patients served as controls, receiving no spe-cific therapy. Within 45 days after the onset ofthe streptococcal infection, 2 patients who hadreceived penicillin developed acute rheumaticfever, whereas this complication occurred in 28of the control group.Treatment with 1 of 2 broad spectrum anti-
biotics also reduced the attack rate of acuterheumatic fever, but the results were not sostriking as those obtained following the use ofpenicillin. In a series of 1,009 patients who re-ceived chlortetracycline, 5 developed rheumaticfever, whereas 20 of 1,035 controls incurredthis complication.'0 In a comparable study1" inwhich oxytetracycline was employed as therapyof streptococcal exudative pharyngitis, rheu-matic fever occurred within 35 days in 12 of480 untreated controls and in 5 of 506 patientswho received treatment.The results of these studies indicate beyond
doubt that successful treatment of the preced-ing streptococcal infection decreases the fre-quency of acute clinical attacks of rheumaticfever. Analysis of the failures to prevent acuterheumatic fever by the treatment of the pre-ceding streptococcal infection with 1 of theantibiotic drugs showed that any form oftreatment that does not eliminate the infectingorganism was not satisfactory.6 Thus, in thoseindividuals with streptococcal infections whoseorganism was not eliminated by therapy, theattack rate of rheumatic fever was not appreci-ably different from that observed in patientsreceiving no therapy. The importance of theliving streptococcus in the production of acuterheumatic fever is also emphasized by the factthat sulfadiazine, a bacteriostatic agent, doesnot eliminate the organism when administeredto patients with streptococcal pharyngitis anddoes not decrease the attack rate of acute rheu-matic fever. Therefore, in the evaluation of
1145
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYMPOSIUM ON RHEUMATIC FEVER
various therapeutic regimens for prevention ofrheumatic fever by treatment of the precedingstreptococcal infection, it becomes necessary toexamine the bacteriologic results.
Primarily on the basis of the above studiesthe American Heart Association made recom-mendations for the prevention of rheumaticfever. Until evidence to the contrary is pro-duced, it was logical to assume that preventionof the acute joint and constitutional symptomsof rheumatic fever would result in a decreasedincidence of rheumatic valvular heart disease.Recently, Weinstein, Boyer, and Goldfield12have produced some data that indicate thattreatment of the preceding respiratory illnessprevents the symptoms of acute rheumaticfever but not valvular heart disease. In theirinitial studies' electrocardiographic abnor-malities developed in patients with scarletfever during early and late convalescence andthis was considered as evidence that rheumaticcarditis was not prevented by therapy. Subse-quent follow-up studies'2 confirmed this im-pression, since rheumatic valvular heart dis-ease appeared in most of those patients whoexhibited abnormalities and did not appear inthose with normal electrocardiograms.
In Weinstein's study'2 167 patients withscarlet fever were treated with penicillin. Fortyof these received 800,000 units orally each dayfor 10 days; 127 were given 120,000 units intra-muscularly daily for 10 days. During con-valescence 12 patients (7.2 per cent) developedsymptoms and signs suggestive of rheumaticfever and of these, 2 met the diagnostic criteriaemployed by Jones.'4 The other 10 patientsdemonstrated electrocardiographic changes andin a few of these vague symptoms were alsorecorded. Seven years later 110 of the original167 patients returned for study, including 10of the original 12 suspected of having acuterheumatic fever. None of the 100 patientsavailable for examination who had had nofindings suggestive of rheumatic fever earliershowed findings indicative of valvular heartdisease. Of the 10 patients diagnosed as pos-sible rheumatic fever only 2 were thought tohave normal hearts at this follow-up examina-tion and 8 exhibited signs indicative of rheu-matic valvular heart disease.
The fact that valvular heart disease de-veloped in those patients exhibiting electro-cardiographic changes during the acute strepto-coccal infection and early convalescence ledthe authors to suggest that treatment of theoriginal streptococcal infection prevented theacute clinical manifestations of rheumaticfever but not valvular deformities. This situa-tion might be considered analogous to theeffects of ACTH and cortisone, which suppressthe clinical manifestations but not valvularheart disease when administered during an at-tack of acute rheumatic fever.'5 If these ob-servations of Weinstein12 are confirmed, thefailure to prevent valvular deformities bytreatment of the streptococcal infection withpenicillin suggests that the mechanisms of pro-duction of joint disease and heart disease aredifferent. Furthermore, if treatment of thestreptococcal infection does not reduce theincidence of valvular heart disease, other meth-ods of accomplishing this goal should be pur-sued vigorously. Although final answers arenot yet available, certain data would indicatethat adequate treatment of the acute respira-tory infection may alter the incidence ofrheumatic carditis.
There are a number of studies of electro-cardiographic changes subsequent to scarletfever and streptococcal pharyngitis. Faulkner,Place, and Ohlerl6 observed changes in theT wave in leads I or II or prolongation of theP-R interval to 0.20 sec. or longer in 6 per centof 171 patients with scarlet fever who receivedno specific treatment. Roelsenl7 found a pro-longed P-R interval of 0.20 sec. or more in 16per cent of 108 patients with scarlet fever andarthralgia and in 4 per cent of 99 scarlet feverpatients without arthralgia. In these 2 studiesno specific antibacterial treatment was em-ployed. Watson, Rothbard, and Swift'8 studied110 adults with scarlet fever who receivedeither sulfadiazine or no specific therapy.Twenty-two or 20 per cent showed electro-cardiographic abnormalities at some timeduring the illness. Fifteen of the 22 patientsexhibited an increase of the P-R interval of0.04 sec. or more. Seven showed inverted Twaves in leads I or II. In this total group of 22patients there were 6 definite and 2 probable
1146
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from
PROPHYLAXIS OF RHEUMATIC FEVER
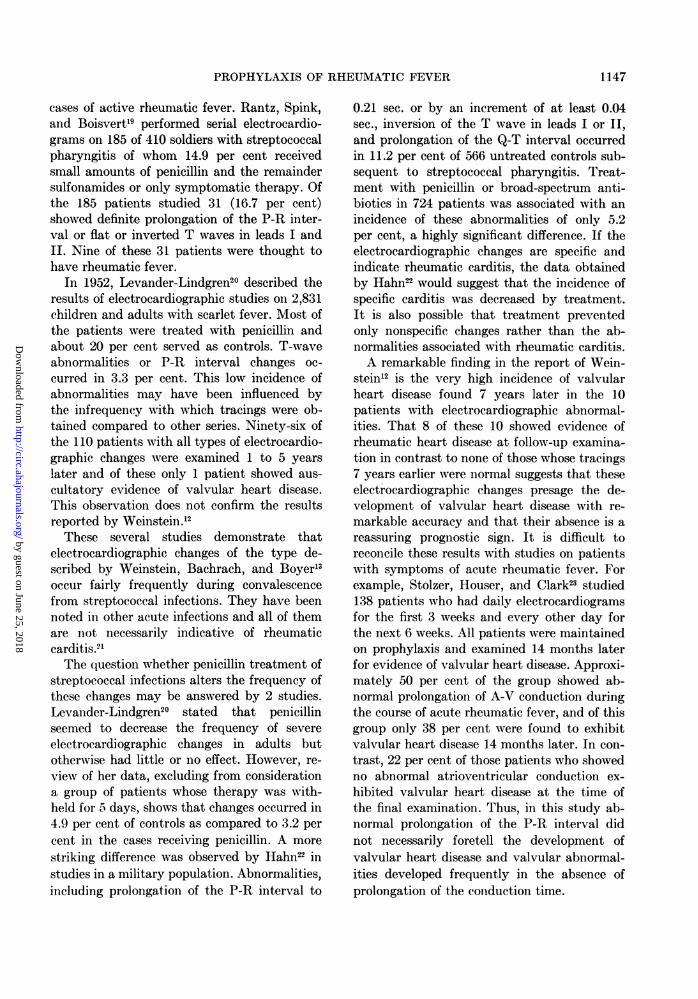
cases of active rheumatic fever. Rantz, Spink,and Boisvert'9 performed serial electrocardio-grams on 185 of 410 soldiers with streptococcalpharyngitis of whom 14.9 per cent receivedsmall amounts of penicillin and the remaindersulfonamides or only symptomatic therapy. Ofthe 185 patients studied 31 (16.7 per cent)showed definite prolongation of the P-R inter-val or flat or inverted T waves in leads I andII. Nine of these 31 patients were thought tohave rheumatic fever.
In 1952, Levander-Lindgren20 described theresults of electrocardiographic studies on 2,831children and adults with scarlet fever. Most ofthe patients were treated with penicillin andabout 20 per cent served as controls. T-waveabnormalities or P-R interval changes oc-curred in 3.3 per cent. This low incidence ofabnormalities may have been influenced bythe infrequency with which tracings were ob-tained compared to other series. Ninety-six ofthe 110 patients with all types of electrocardio-graphic changes were examined 1 to 5 yearslater and of these only 1 patient showed aus-cultatory evidence of valvular heart disease.This observation does not confirm the resultsreported by Weinstein.'2These several studies demonstrate that
electrocardiographic changes of the type de-scribed by Weinstein, Bachrach, and Boyerl3occur fairly frequently during convalescencefrom streptococcal infections. They have beennoted in other acute infections and all of themare not necessarily indicative of rheumaticcarditis.9'The question whether penicillin treatment of
streptococcal infections alters the frequency ofthese changes may be answered by 2 studies.Levander-Lindgren20 stated that penicillinseemed to decrease the frequency of severeelectrocardiographic changes in adults butotherwise had little or no effect. However, re-view of her data, excluding from considerationa group of patients whose therapy was with-held for 5 days, shows that changes occurred in4.9 per cent of controls as compared to 3.2 percent in the cases receiving penicillin. A morestriking difference was observed by Hahn22 instudies in a military population. Abnormalities,including prolongation of the P-R interval to
0.21 sec. or by an increment of at least 0.04sec., inversion of the T wave in leads I or II,and prolongation of the Q-T interval occurredin 11.2 per cent of 566 untreated controls sub-sequent to streptococcal pharyngitis. Treat-ment with penicillin or broad-spectrum anti-biotics in 724 patients was associated with anincidence of these abnormalities of only 5.2per cent, a highly significant difference. If theelectrocardiographic changes are specific andindicate rheumatic carditis, the data obtainedby Hahn22 would suggest that the incidence ofspecific carditis was decreased by treatment.It is also possible that treatment preventedonly nonspecific changes rather than the ab-normalities associated with rheumatic carditis.A remarkable finding in the report of Wein-
stein12 is the very high incidence of valvularheart disease found 7 years later in the 10patients with electrocardiographic abnormal-ities. That 8 of these 10 showed evidence ofrheumatic heart disease at follow-up examina-tion in contrast to none of those whose tracings7 years earlier were normal suggests that theseelectrocardiographic changes presage the de-velopment of valvular heart disease with re-markable accuracy and that their absence is areassuring prognostic sign. It is difficult toreconcile these results with studies on patientswith symptoms of acute rheumatic fever. Forexample, Stolzer, Houser, and Clark23 studied138 patients who had daily electrocardiogramsfor the first 3 weeks and every other day forthe next 6 weeks. All patients were maintainedon prophylaxis and examined 14 months laterfor evidence of valvular heart disease. Approxi-mately 50 per cent of the group showed ab-normal prolongation of A-V conduction duringthe course of acute rheumatic fever, and of thisgroup only 38 per cent were found to exhibitvalvular heart disease 14 months later. In con-trast, 22 per cent of those patients who showedno abnormal atrioventricular conduction ex-hibited valvular heart disease at the time ofthe final examination. Thus, in this study ab-normal prolongation of the P-R interval didnot necessarily foretell the development ofvalvular heart disease and valvular abnormal-ities developed frequently in the absence ofprolongation of the conduction time.
1147
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYMPOSIUM ON RHEUMATIC FEVER
As mentioned above, in order to decrease theattack rate of rheumatic fever by treatment ofthe preceding respiratory infection, it is prob-ably necessary to eradicate the group A strepto-coccus. In the series of Weinsteinl2 33 per centof all patients with scarlet fever are known tohave developed a bacteriologic relapse or rein-fection after cessation of therapy with penicil-lin. It is not clear from their reports how manyof the 12 patients suspected of having rheu-matic fever incurred such relapses. However,upon re-examination of the data24 culturesfrom 8 patients showed no group A strepto-cocci at the time rheumatic fever was firstsuspected or during the rheumatic episode. In1 instance streptococci reappeared in thepharynx prior to the development of rheumaticsymptoms, and from 3 individuals streptococciwere isolated following the first sign of rheu-matic fever. Thus, in this small group of pa-
tients streptococci were isolated from thepharynx no more frequently in the suspectedrheumatic group than in the entire series.
Final answers to the disturbing questionsraised by the study of Weinstein12 are unavail-able at present. There is no doubt that treat-ment of the preceding streptococcal infectiondecreases the incidence of rheumatic fever pro-
viding the treatment is adequate to eliminatethe organism. It has also been shown byHahn22 that such treatment prevents, in largepart, the electrocardiographic changes fre-quently observed following streptococcal infec-tions. However, the answer to the questionwhether treatment of the streptococcal infec-tion prevents rheumatic valvular deformitiesmust await information that can be obtainedonly from a controlled study. Until such in-formation is available, it would seem advisableto continue to treat acute streptococcal diseaseswith therapy known to eliminate the organismin the majority of instances.
How LONG SHOULD PROPHYLAXIS BE MAIN-TAINED IN THE PATIENT WHO HAS HAD
RHEUMATIC FEVER?
In order to plan a rational method of man-
agement of the patient who has experiencedrheumatic fever the physician should be ac-
quainted with certain epidemiologic features of
streptococcal infections and rheumatic fever.Group A streptococci are maintained in naturein the upper respiratory tract of man. The mostdangerous source of infections is the carrierwho has recently acquired the organism.25Since streptococcal infections occur frequentlyin the young, school-age child, any situationthat places the individual in contact withchildren increases the risk of infection. Theorganism is transferred to the susceptible hostby intimate contact and not by droplet nuclei,contaminated dust, bedding, and other arti-cles.25Although adults apparently acquire fewer
streptococcal infections than children, it isprobably a fallacy to believe that this is due toacquired resistance. Immunity in man is type-specific and relatively long enduring.25 26 Sincemost adults probably have had experiencewith only a few serologic types during child-hood, they should become infected if ade-quately exposed to a carrier harboring a newtype of streptococcus. Experience in militarypopulations shows that young adults are verysusceptible to these infections when assignedto an installation experiencing an epidemic.Although type-specific immunity to strepto-
coccal infections may play a minor role in thedecreased incidence of both initial and recur-rent attacks of rheumatic fever in older agegroups, the major factor is most likely the lackof effective contacts with carriers of the organ-ism. Another factor that may contribute to thelow rates of initial attacks of rheumatic feverin the adult is decreased susceptibility torheumatic fever following a streptococcal in-fection.'2 Although the data are meager, avail-able information indicates that the rates arenot influenced by age,* once a streptococcalinfection develops.27 The situation in relationto the risk of recurrence of rheumatic activityas age progresses is poorly defined, but it isgenerally agreed that 1 attack confers a markedincrease in susceptibility.The reported rates of recurrence from 3
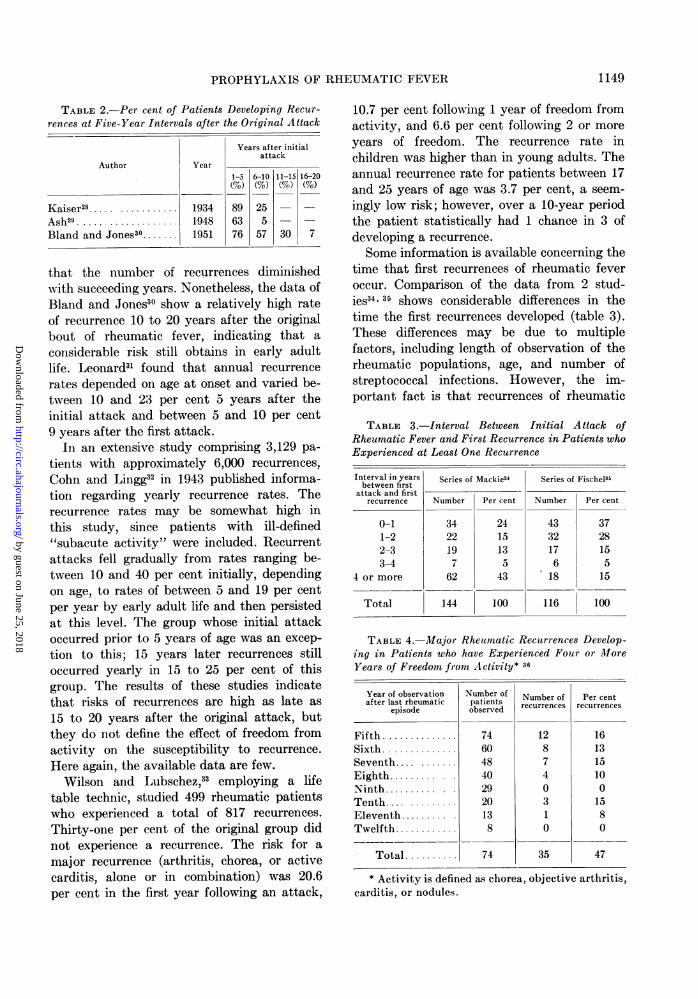
studies are shown in table 2. Although thefigures vary among the 3 studies, it is apparent
* Attack rates of rheumatic fever following thefirst experience with the organism are not available.
1148
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from
PROPHYLAXIS OF RHEUMATIC FEVER
Years after initialattack
1-5 6-10 11-15 16-20
89 25 -
63 5 -
76 57 30 7
that the number of recurrences diminishedwith succeeding years. Nonetheless, the data ofBland and Jones30 show a relatively high rateof recurrence 10 to 20 years after the originalbout of rheumatic fever, indicating that a
considerable risk still obtains in early adultlife. Leonard31 found that annual recurrence
rates depended on age at onset and varied be-tween 10 and 23 per cent 5 years after theinitial attack and between 5 and 10 per cent9 years after the first attack.
In an extensive study comprising 3,129 pa-
tients with approximately 6,000 recurrences,
Cohn and Lingg32 in 1943 published informa-tion regarding yearly recurrence rates. Therecurrence rates may be somewhat high inthis study, since patients with ill-defined"subacute activity" were included. Recurrentattacks fell gradually from rates ranging be-tween 10 and 40 per cent initially, dependingon age, to rates of between 5 and 19 per centper year by early adult life and then persistedat this level. The group whose initial attackoccurred prior to 5 years of age was an excep-
tion to this; 15 years later recurrences stilloccurred yearly in 15 to 25 per cent of thisgroup. The results of these studies indicatethat risks of recurrences are high as late as
15 to 20 years after the original attack, butthey do not define the effect of freedom fromactivity on the susceptibility to recurrence.
Here again, the available data are few.Wilson and Lubschez,33 employing a life
table technic, studied 499 rheumatic patientswho experienced a total of 817 recurrences.
Thirty-one per cent of the original group didnot experience a recurrence. The risk for a
major recurrence (arthritis, chorea, or activecarditis, alone or in combination) was 20.6per cent in the first year following an attack,
10.7 per cent following 1 year of freedom fromactivity, and 6.6 per cent following 2 or moreyears of freedom. The recurrence rate inchildren was higher than in young adults. Theannual recurrence rate for patients between 17and 25 years of age was 3.7 per cent, a seem-ingly low risk; however, over a 10-year periodthe patient statistically had 1 chance in 3 ofdeveloping a recurrence.Some information is available concerning the
time that first recurrences of rheumatic feveroccur. Comparison of the data from 2 stud-ies34 35 shows considerable differences in thetime the first recurrences developed (table 3).These differences may be due to multiplefactors, including length of observation of therheumatic populations, age, and number ofstreptococcal infections. However, the im-portant fact is that recurrences of rheumatic
TABLE 3.-Interval Between Initial Attack ofRheumatic Fever and First Recurrence in Patients whoExperienced at Least One Recurrence
Interval in yearsbetween first
attack and firstrecurrence
0-11-22-33-4
4 or more
Total
Series of Mackie34
Number
3422197
62
144
Per cent
2415135
43
100
Series of Fischel35
Number
433217618
116
Per cent
372815515
100
TABLE 4.-Major Rheumatic Recurrences Develop-ing in Patients who have Experienced Four or MoreYears of Freedom front Activity* 36
Year of observation Number of Number of Per cent
episode patients recurrences recurrences
Fifth .74 12 16Sixth .60 8 13Seventh . 48 7 15Eighth ..... 40 4 10Ninth. ....... 29 0 0Tenth .... ......... 20 3 15Eleventh..... 13 1 8Twelfth .8 0 0
Total .74 35 47
* Activity is defined as chorea, objective arthritis,carditis, or nodules.
TABLE 2.-Per cent of Patients Developing Recur-rences at Five-Year Intervals after the Original Attack
Author
Kaiser2 ..... ...........
Ash29 ...................Bland and Jones30.......
Year
193419481951
1149
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYMPOSIUM ON RHEUMATIC FEVER
fever do occur after long periods of freedomfrom activity.An earlier study of Wilson, Lingg, and Crox-
ford36 supports the concept that the risk ofrecurrence after a number of years of freedomis high. Data were presented regarding each of412 rheumatic subjects followed for varyingperiods of time after their original attacks.There were 72 patients who experienced a totalof 74 periods of more than 4 years of freedomfrom major activity. The recurrences that de-veloped in these patients subsequent to 4 years
of freedom are shown by year of observation intable 4. It is again evident that recurrences
may occur many years after the original attackin spite of long intervals without rheumaticactivity.
It is obvious that a rational method of man-agement of the rheumatic patient cannot beestablished unless susceptibility to recurrence
can be defined in relation to other factors suchas age, period of freedom from activity, andthe role of streptococcal infections. As men-
tioned previously, the decreased incidence ofstreptococcal infections in the adult may ac-
count for the decreased occurrence of rheu-matic attacks recorded in the studies reviewed.Some information concerning the susceptibilityto recurrence following an observed strepto-coccal infection at age 17 to 25 was obtainedfrom an analysis of 216 patients admitted to a
military hospital.* A total of 216 patients were
seen who had a respiratory illness and who ex-
hibited group A streptococci in the cultures ofthe oropharynx. Seventy-seven of these 216patients received no specific treatment andwere observed for signs of rheumatic activityfor a minimum of 3 weeks from onset of theirstreptococcal infection. A diagnostic increasein the antistreptolysin titer was demonstratedin the convalescent serum as compared to thetiter of the serum obtained at the onset of therespiratory illness in 71 per cent of the patientsstudied. Pharyngeal or tonsillar exudate was
observed in 45 of the 77 patients. The attackrate for rheumatic fever in this group is re-
corded in table 5 according to the number of
* The authors are indebted to the professionalstaff of the Streptococcal Disease Laboratory for thecollection of these data.
TABLE 5.-Frequency of Rheumatic Fever Recur-rences in Young Adults Observed During a Strepto-coccal Infection*
Recurrence of rheumatic fever
Years since Numberlast attack of of Definite Possible Totalrheumatic fever infec-
Num- Per Num- Per Num- Perber cent ber cent ber cent
0-4 15 2 13 2 13 4 275-9 32 6 19 1 3 7 22
10 or more 17 2 12 0 0 2 12Unknown 13 0 0 1 8 1 8
Total 77 10 13 4 5 14 18
* No specific therapy was administered for therespiratory illness.
years that had elapsed since the last rheu-matic episode.Rheumatic fever, according to criteria for
diagnosis previously defined,9 developed in atotal of 14 or 18 per cent of the 77 patientsobserved during and following a streptococcalinfection. The attack rate according to thenumber of years that had elapsed since thelast rheumatic episode was 27, 22, and 12 percent for less than 5, 5 to 9, and 10 or moreyears of freedom, respectively. Although thetotal number of cases studied was small, it isapparent that susceptibility to a recurrencefollowing a streptococcal infection did not de-crease greatly as the period of freedom fromactivity increased. Certainly, one should notdiscontinue the prophylactic regimen justbecause a recurrence had not been observedfor a period of 5 or 10 years.*
It has been suggested that in the adult pro-tection from recurrences might be obtained bytreatment of the streptococcal infection. Thedata presented in table 6 show that reliance onthis method is not justified. In this study, 139patients with a past history of rheumaticfever received treatment for the respiratory ill-ness with antibiotics and were followed for signsof recurrences. All these patients exhibitedexudative tonsillitis or pharyngitis and cul-
* It is possible that freedom from experience withthe group A streptococcus afforded by prophylaxisfor a period of 5 or more years may alter the attackrate after a proved streptococcal infection, but nodata are available for analysis.
1150
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from

PROPHYLAXIS OF RHEUMATIC FEVER
TABLE 6.-Frequency of Rheumatic Recurrencesin Young Adults Observed During a StreptococcalInfection Treated with Antibiotics
Years sincelast attackof rheumatic
fever
0-45-9
10 or more
Unknown
Total
Numberof
infec-tions
35454712
139
Recurrence of rheumatic fever
Definite
Num- Per
ber cent
2 62 41 20 0
5 4
Possible
Num- Per
ber cent
6 172 43 60 0
11 8
Total
Num- Per
ber cent
8 234 94 90 0
16 12
tures showed group A streptococci. The attackrate in this group was 3.6 per cent, but an
additional 8 per cent showed some signs or
symptoms of a recurrent attack. Since many
streptococcal infections are inapparent, it isobvious that individuals such as those includedin table 5 should be under continuous prophy-laxis.
In summary, rheumatic recurrences occur inadult life in spite of freedom from activity formany years and the risk of recurrent activityin adult life following a streptococcal infectionis high. Therefore, the risk of a recurrent at-tack of acute rheumatic fever in adults dependsprimarily on effective contacts with a carrierof the group A streptococcus. Thus, estimationof the risk of recurrence of rheumatic fever isan individual problem and the decision as tohow long prophylaxis should be continuedmust be based on many factors. In the opinionof the authors, it is mandatory to continueprophylaxis as long as the patient is in schoolor serving in the armed services. Likewise, theadult, especially the parent, who is exposed tochildren should be protected. Those whose oc-
cupations demand intimate exposure to many
people undoubtedly experience an increasedrisk. In contrast, a chauffeur-driven executivewho is exposed to few people, other than hissecretary and other chauffeur-driven execu-
tives, has less opportunity to contract infection.All these variable and individual factors mustbe considered by the physician in making thedecision as to how long prophylaxis should becontinued in an individual patient. It is notsufficient to rely on antibiotic treatment of a
streptococcal infection, since many are inap-parent or cause few symptoms and therapydoes not prevent all recurrences. In addition,there is still some doubt whether therapy ofthe respiratory infection prevents cardiac dam-age. Therefore, prophylaxis should be main-tained indefinitely except in those few indi-viduals in whom the risk of contracting astreptococcal infection is negligible.
REFERENCESCommission on Acute Respiratory Diseases. A
study of a food-borne epidemic of tonsillitis andpharyngitis due to B-hemolytic streptococcus,type 5. Bull. Johns Hopkins Hosp. 77: 143, 1945.
2 MORRIS, A. J., CHAMOVITZ, R., CATANZARO, F. J.,AND RAMMELKAMP, C. H., JR.: Prevention ofrheumatic fever by treatment of previousstreptococcal infections. Effect of sulfadiazine.J. A. M. A. 160: 114, 1956.
3 MASSELL, B. F., Dow, J. W., AND JONES, T. D.:Orally administered penicillin in patients withrheumatic fever. J. A. M. A. 138: 1030, 1948.
4 DENNY, F. W., WANNAMAKER, L. W., BRINK,W. R., RAMMELKAMP, C. H., JR., AND CUSTER,E. A.: Prevention of rheumatic fever. Treat-ment of the preceding streptococcal infection..1. A. M. A. 143: 151, 1950.
Committee on Prevention of Rheumatic Feverand Bacterial Endocarditis of the AmericanHeart Association: Prevention of rheumaticfever and bacterial endocarditis through controlof streptococcal infections. Circulation 11: 317,1955.
6 Streptococcal Disease Laboratory: Unpublishedobservations.
7 MASSELL, B. F., STURGIS, G. P., KNOBLOCK, J. D.,STREEPER, R. B., HALL, T. N., AND NORCROSS,P.: Prevention of rheumatic fever by promptpenicillin therapy of hemolytic streptococcicrespiratory infections. J. A. M. A. 146: 1469,1951.
8 BREESE, B. B.: Treatment of beta hemolyticstreptococeic infections in the home. Relativevalue of available methods. J. A. M. A. 152:10, 1953.
9 WANNAMAKER, L. W., RAMMELKAMP, C. H., JR.,DENNY, F. W., BRINK, W. R., HOUSER, H. B.,HAHN, E. 0., AND DINGLE, J. H.: Prophylaxisof acute rheumatic fever by treatment of thepreceding streptococcal infection with variousamounts of depot penicillin. Am. J. Med. 10:673, 1951.
10 HouSER, H. B., ECKHARDT, G. C., HAHN, E. O.,DENNY, F. W., WANNAMAKER, L. W., ANDRAMMELKAMP, C. H., JR.: Effect of aureomyeintreatment of streptococcal sore throat on thestreptococcal carrier state, the immunologic
1151
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYMPOSIUM ON RHEUMATIC FEVER
response of the host, and the incidence of acuterheumatic fever. Pediatrics 12: 593, 1953.
11 CATANZARO, F. J., BROCK, L., CHAMOVITZ, R.,PERRY, WV. D., SIEGEL A. C., STETSON, C. A.,RAMMELKAMP, C. H., JR., HOUSER, H. B.,STOLZER, B. L., WANNAMAKER, L. W., ANDHAHN, E. 0.: Effect of oxytetracycline therapyof streptococcal sore throat on the incidence ofacute rheumatic fever. Ann. Int. Med. 42: 345,1955.
12 WEINSTEIN, L., BOYER, N. H., AND GOLDFIELD,M.: Rheumatic fever in scarlet-fever patientstreated with penicillin. A follow-up study afterseven years. New England J. Med. 253: 1, 1955.
13-, BACHRACH, L., AND BOYER, N. H.: Observa-tions on the development of rheumatic feverand glomerulonephritis in cases of scarlet fevertreated with penicillin. New England J. Mled.242: 1002, 1950.
14 JONES, T. D.: Diagnosis of rheumatic fever.J. A. M. A. 126: 481, 1944.
15 The Rheumatic Fever Working Party of theMedical Research Council of Great Britainand the Subcommittee of Principal Investigatorsof the American Council on Rheumatic Feverand Congenital Heart Disease, American HeartAssociation: The treatment of acute rheumaticfever in children. A cooperative clinical trialof ACTH, cortisone and aspirin. Circulation 11:343, 1955.
16 FAULKNER, J. WI., PLACE, E. H., AND OHLER, W.R.: The effect of scarlet fever on the heart. Am.J. M. Sc. 189: 352, 1935.
17 ROELSEN, E.: Electrocardiographic studies inscarlet fever. Acta med. scandinav. 106: 26,1941.
18 WATSON, R. F., ROTHBARD, S., AND SWIFT, H. F.:
The relationship of postscarlatinal arthritis andcarditis to rheumatic fever. J. A. M. A. 128:1145, 1945.
19 RANTZ, L. A., SPINK, WV. W., AND BOISVERT, P.J.: Abnormalities in the electrocardiogramfollowing hemolytic streptococcus sore throat.Arch. Int. Med. 77: 66,1946.
20 LEVANDER-LLNDGREN, M.: Electrocardiographicstudies in scarlet fever. Acta Paediat. Suppl.91: 1952.
21 GOLDFIELD, Al., BOYER, N. H., AND WEINSTEIN,
L.: Electrocardiographic changes during thecourse of measles. J. Pediat. 46: 30, 1955.
2HAHN, E. 0.: To be published.23 STOLZER, B. L., HOUSER, H. B., AND CLARK, E. J.:
Therapeutic agents in rheumatic carditis.Comparative effects of acetylsalicylic acid,corticotropin, and cortisone. Arch. Int. MIed.95: 677, 1955.
24 WEINSTEIN, L.: Personal communication.25 WANNAMAKER, L. W.: The epidemiology of strepto-
coccal infections. In, Streptococcal Infections,MI. McCarty, Ed., Chap. 12. New York, Co-lumbia University Press, 1954.
26 RAMMELKAMP, C. H., JR.: Glomerulonephritis.Proc. Inst. AMed. Chicago 19: 371, 1953.
27 -, WANNAMAKER, L. WV., AND DENNY, F. W.:The epidemiology and prevention of rheumaticfever. Bull. New York Acad. Med. 28: 321, 1952.
28 KAISER, A. D.: Factors that influence rheumaticdisease in children. J. A. M. A. 103: 886, 1934.
29 ASH, R.: The first ten years of rheumatic infectionin childhood. Am. Heart J. 36: 89, 1948.
30 BLAND, E. F., AND JONES, T. D.: Rheumatic feverand rheumatic heart disease. A twenty yearreport on 1,000 patients followed since child-hood. Circulation 4: 836, 1951.
31 LEONARD, M.: Puberty and prognosis in rheumaticfever. Am. Heart J. 14: 192, 1937.
32 COHN, A. E., AND LINGG, C.: The natural historyof rheumatic cardiac disease: a statistical study.II. Manifestations of rheumatic activity: Recur-rence, severity of infection, and prognosis.J. A. M. A. 121: 113, 1943.
33 WILSON, 1\I. G., AND LUBSCHEZ, R.: Recurrencerates in rheumatic fever. The evaluation ofetiologic concepts and consequent preventivetherapy. J. A. M. A. 126: 477, 1944.
34 MACKIE, T. T.: Rheumatic fever. An analyticalstudy of three hundred and ninety-three casesof rheumatic fever and eighty-nine cases ofchorea. Am. J. M. Sc. 172: 199, 1926.
35 FISCHEL, E. E.: quoted by Stollerman, G. H.: Theuse of antibiotics for the prevention of rheu-matic fever. Am. J. Med. 17: 757, 1954.
36 WILSON, M. G., LINGG, C., AND CROXFORD, G.:Statistical studies bearing on problems in theclassification of heart disease. III. Heart diseasein children. Am. Heart J. 4: 164, 1928.
1152
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from

EDWARD A. MORTIMER, JR. and CHARLES H. RAMMELKAMP, JR.Prophylaxis of Rheumatic Fever
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1956 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.14.6.11441956;14:1144-1152Circulation.
http://circ.ahajournals.org/content/14/6/1144.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 25, 2018http://circ.ahajournals.org/
Dow
nloaded from