Embed Size (px)
Citation preview

Proportionality – regulate the banks, keep off the backs of clinical researchers
Charles Warlow, EdinburghCentre for Socio-legal studies, Oxford
March 2009

Bristol Heart Scandal
Harold Shipman
Alder Hey retained organs scandal
These were nothingwhatsoever to do with research approved by a Research Ethics Committee – and nor are eRecords

Types of clinical research – ie research on/with patients (and their tissues)
• Invasive - from biopsy to catheterising arteries to taking a blood sample – consent unarguable (almost)
• Non-invasive – from interviewing, to questionnaire, to medical records – consent perhaps not always necessary
• Interventional – randomised and non-randomised therapeutic interventions ie drugs (eg Northwick Park), surgery, physiotherapy, systems of care (eg stroke units) etc - consent surprisingly variable for non-randomised studies
The risks of harm are very different, but so too is the potential to affect larger or smaller numbers of patients – so get things into proportion

Increasing research regulation
•
UK Data Protection Act (1998)UK Human Rights Act (1998)Health and Social Care Act (2001) (England and Wales)Adults with Incapacity (Scotland) Act (2000)European Clinical Trials Directive (2001)Human Tissue Act (2004) (England and Wales)Mental Incapacity Act (2005) (England and Wales)Human Tissue Act (2006) (Scotland) •
•
Statutory regulation
Guidance from professional bodiesGeneral Medical CouncilConfidentiality & security advisory group for Scotland (CSAG)World Medical AssociationMedical Research CouncilBritish Medical AssociationDepartment of HealthRoyal College(s) of Physicians etc etc etc
Wasting researchers’ time, but this may if recorded and published change the
system

Research ethics committee practice in Scotland: a story from 1998
• Observational population-based study of incidence and prognosis of intracranial vascular malformations
• Multicentre Research Ethics Committee (MREC) approval July 1998
• Then to the Local Research Ethics Committees (LRECs) of 15 health boards
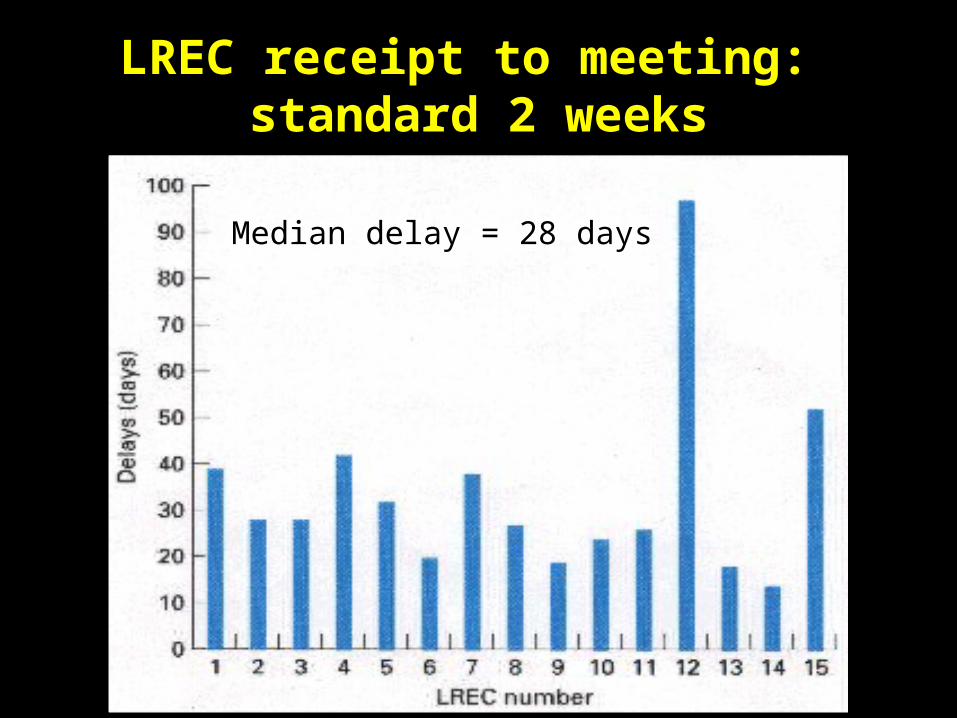
LREC receipt to meeting: standard 2 weeks
Median delay = 28 days

Application to LREC approval
Median delay = 39 days

Each LREC required
• one copy of the protocol• a variable number of copies of:
– MREC application form 23 pages– Local investigator form & CV 8 pages– MREC correspondence 6 pages– Consent form & info. sheet 7 pages
_______
44 pages
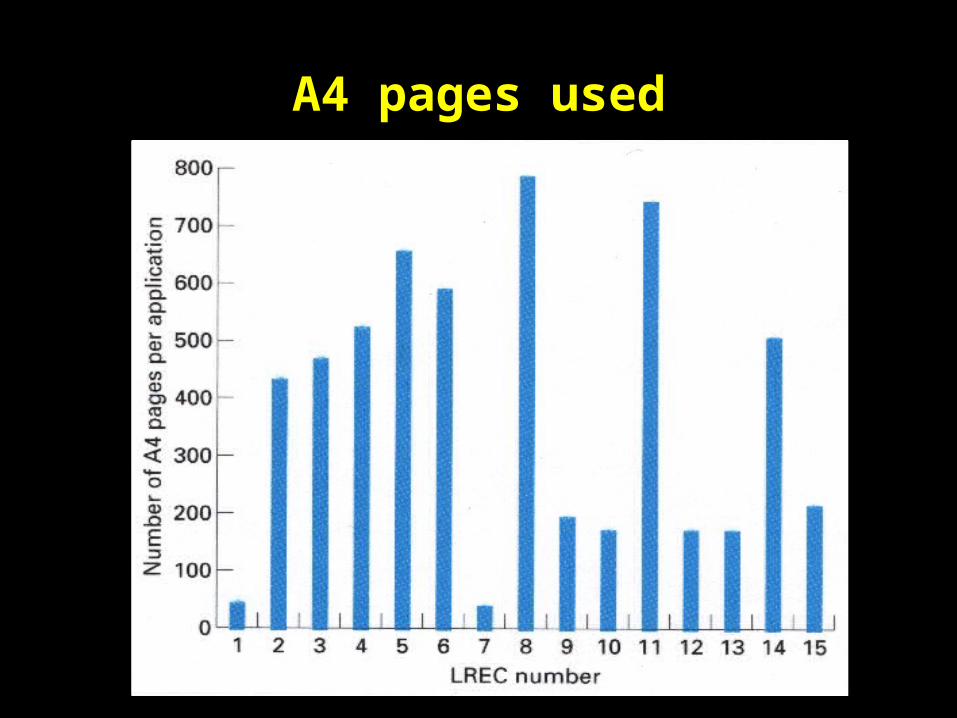
A4 pages used

5789 A4 pages, weighing 26.9 kg
….. and all for three trivial modifications, one not within the local committee’s jurisdiction
literally weighing…


A new era: Central Office for Research Ethics Committees (COREC) in 2000
COREC established by (English) Department of Health (UK liaison) in 2000– distributes decision-making to any resaerch ethics committee
(REC)– uniform on-line application form, albeit lengthy– extended jurisdiction of one REC decision– focus on process of REC review
• implement, develop, maintain, standardise & oversee process; training; appeals; information
• European Clinical Trials Directive (2001)• Good clinical practice (GCP) for all types of research, not just
trials

Another new era: National Research Ethics Service (NRES) 2007 –
The process of ethics approval is improving
• emphasis on national (UK) and service (with advice)• aims for consistency, between and within RECs • time lines (measurable but ?relevance – what about quality?)• not meant to review the science
But still no transparency such as release of minutes, or research into the process itself (variation in decision making?), or quality

Adults with Incapacity (Scotland) Act 2000

No surgical, medical, nursing, dental or psychological research shall be carried out on any adult who is incapable in relation to a decision about participation in the research unless—
(1) research of a similar nature cannot be carried out on an adult who is capable in relation to such a decision; and the circumstances mentioned in subsection (2) are satisfied.
(2)The circumstances referred to in subsection (1) are that— (a) the purpose of the research is to obtain knowledge of—
the causes, diagnosis, treatment or care of the adult’s incapacity; or the effect of any treatment or care given during his incapacity to the adult which relates to that incapacity; and (b) the conditions mentioned in subsection (3) are fulfilled. (3) The conditions are— - the research is likely to produce real and direct benefit to the adult; - the adult does not indicate unwillingness to participate in the research; - the research has been approved by the Ethics Committee; - the research entails no foreseeable risk, or only a minimal foreseeable risk, to the adult; - the research imposes no discomfort, or only minimal discomfort, on the adult; and - consent has been obtained from any guardian or welfare attorney who has power to consent to the adult’s participation in research or, where there is no such guardian or welfare attorney, from the adult’s nearest relative.

Why it may be misleading to use the results of a trial in mild strokes to inform
the treatment of severe strokes
100 severe strokes: 60 die reduced by 10% to 54 by treatment
100 mild strokes: 30 die reduced by 10% to 27 by treatment – same relative risk reduction which is a reasonable expectation, but very different absolute risk reduction
But, treatment causes 2 fatal cerebral haemorrhages/100 treated irrespective of initial stroke severity
Therefore, for severe strokes:
Treatment avoids 4 deaths/100 treated (60 – 54 + 2): …..number-needed-to-treat to avoid one death = 25
but for mild strokes only 1 (30 – 27 + 2): …..number-needed-to-treat = 100
Amendment December 2006 of Adults with Incapacity (Scotland) Act, 2000Where the research consists of a clinical trial of a medicinal product, the research may be carried out b) without the consent of any guardian or welfare attorney, or the adult's nearest relative, if it has not been practicable to contact any such person before the decision to enter the adult as a subject of the clinical trial is made, and consent has been obtained from a person, other than a person connected with the conduct of the clinical trial, who is -(A) the doctor primarily responsible for the medical treatment provided to that adult, or (B) a person nominated by the relevant health care provider.(c) without the consent of any guardian or welfare attorney, or the adult's nearest relative, if treatment is being, or is about to be, provided for an adult who is incapable in relation to a decision about participation in the research as a matter of urgency;(ii) having regard to the nature of the clinical trial and of the particular circumstances of the case it is necessary to take action for the purposes of the clinical trial as a matter of urgency;(iii) it has not been reasonably practicable to obtain the consent of any such person;(iv) it has not been reasonably practicable to obtain the consent of any of the persons mentioned in paragraph (b) (A) or (B); and(v) the action to be taken is carried out in accordance with a procedure approved by the Ethics Committee

“Where the research consists of a clinical trial of a medicinal product………..”
So where does that leave a clinical trial of out of hospital defibrillation for cardiac arrest, or a study of a blood
biomarker for status epilepticus vs pseudo-status, for example?

Consent for observational studies – in particular medical records

Non-intrusive observational studies (research, audit, service planning,
public health monitoring, drug safety etc)
• Identifiable (non-anonymised) data are often required– for record linkage– to identify individuals during follow-up– to sort out diagnoses (eg epilepsy, migraine, even stroke)– to avoid double counting– to avoid consent bias– for control patients – for indirect follow up via GPs, hospital discharges, deaths
• Ideally consent should be obtained from patients for use of their identifiable data but this may be impractical or impossible (dead, demented, anxious, unaware of diagnosis, too many etc)
• Data Protection Act is a problem but its over-interpretation even more so (GMC, Section 60 Health & Social Care Act, England)

The underlying tension between patient confidentiality and the public health
Disclosure
collectivism
social responsibility
benefits of data
sharing
Confidentiality
individualism
autonomy
rights-based
citizenship
risk of disclosure
The key test is surely proportionality, but this requires judgement – not the application
of rigid rules by bureaucrats

The Data Protection Act,1998 third schedule
Any use of identifiable data relating to the “physical or mental health or condition of a living individual requires his
or her informed consent”……..
but there is a qualification: or that the “processing is necessary for medical purposes” (which most have
assumed to include medical research)

“The [Data Protection Act 1998] itself does not necessarily require consent for the use of health information in medical research. The key is to ensure that people know what is happening with their information. The [Information Commissioner] takes the same view as that expressed by Mr Havers – namely, that researchers could be bolder. The statute sets out broad principles for handling personal information. It is not about absolutes.”
David Smith, Deputy Information Commissioner

Lothian Health Board: Information for Clinical Audit
We may record some of your personal health information in databases used by doctors and others for clinical audit. This is one way in which we maintain high-quality care; we will check a group of similar cases to your own against agreed standards to see where improvements can be made. Some of these audits are done over groups of hospitals, over Scotland or even the whole UK. In these cases we make every effort to use anonymous information. We are obliged to act on refusal to participate if possible.
ie ‘opt out’

Lothian Health Board: Information for Research
We may use some of your personal health information in research. This is when healthcare staff use information from their patients to help them find the causes of disease and the effects of treatment and for planning new treatments. If the research involves you personally you will be contacted and asked for your consent.
ie ‘opt in’

Law versus guidance
• Data Protection Act– personal data can be processed without consent
(exemptions for some forms of medical research)• NHS Code of Practice: Confidentiality (2003)
– “…do not use/disclose identifiable data, unless originally understood by confider, or + permission”
• GMC Confidentiality… (April 2004)– doctors should, “…seek patients’ express consent to
disclosure of information, where identifiable data is needed for any purpose other than the provision of care or for clinical audit…”

The future does not look promising…
“My board is quite clear: you can’t look at patients’ records and look at confidential clinical information without consent”
Harry Clayton, Chairman of the National Information Governance Board, 2009
A slightly odd view considering he wasonce CEO of the Alzheimer Disease Society!

"The problem about the Data Protection Act is that it is almost incomprehensible. It is very difficult to understand. The precise limits of it are problematic. There are constant difficulties about what information you are allowed to share between departments for instance. I just think it needs to be looked at again at some stage to make it more simple"
Lord Falconer (The Constitutional Affairs Secretary),reported in the Guardian, October 18th 2004

My own personal losses if unobtrusive health record data collection is prohibited, or subject
to consent in every case
• The broken leg story• The cancerous colon story• The gall bladder story

The emphasis throughout its history has been the empirical study of different areas of law with a view to understanding its place and role in society. Good empirical research, we believe, is based on well-developed theoretical ideas and traditions, and may lead to their adjustment and deepening.

Unique opportunity in the Scottish Intracranial Malformation Study (SIVMS)
to study the effects of consent bias• prospective, population-based cohort study of all IVMs
presenting in adults in Scotland from 1999, with complete prospective follow up
• we could not obtain consent from everyone (dead, consultant/GP refusal, no response to letter)
• yet at first we had Multicentre Research Ethics Committee approval to collect baseline and follow-up data on the whole cohort via GP and hospital records (Record Linkage available in Scotland)
• analysis of patients with brain AVMs enrolled 1999-2002 (n=187)

GP/consultant approval sought to approach patient
n=187
Patient not approached
n=56
Patient approached
n=131
Consented n=111
No-response n=20
Refused n=0
CONSENTERS NON-CONSENTERS
Implicit non-consent
Proxy non-consent
Questionnaire Medical records & GP questionnaires
SIVMS
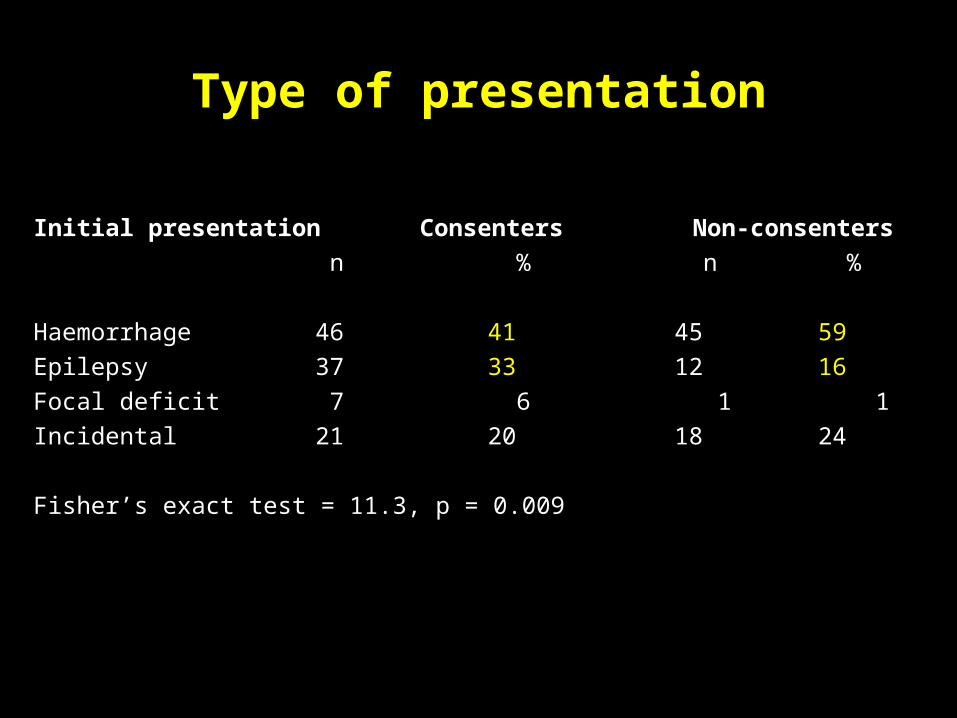
Type of presentation
Initial presentation Consenters Non-consenters
n % n %
Haemorrhage 46 41 45 59
Epilepsy 37 33 12 16
Focal deficit 7 6 1 1
Incidental 21 20 18 24
Fisher’s exact test = 11.3, p = 0.009
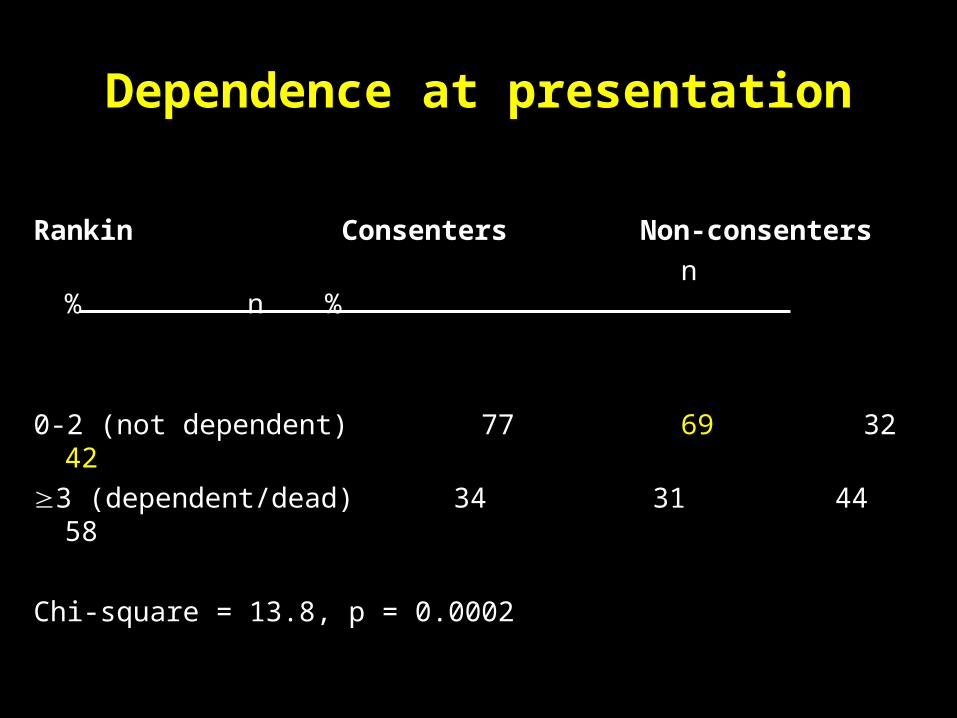
Dependence at presentation
Rankin Consenters Non-consenters
n % n %
0-2 (not dependent) 77 69 32 42
3 (dependent/dead) 34 31 44 58
Chi-square = 13.8, p = 0.0002

All cause mortality
Consenters (red) and non-consenters (black)
Time (days)
1825146010957303650
Pro
po
rtio
n a
live
1.1
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Log rank=15.8 p=0.0001
2 outcomes
12 outcomes

Impact on an important study finding
• All participants– Haemorrhagic presentation of a brain AVM conferred a
higher subsequent risk of haemorrhage during untreated follow-up
• 95 unruptured brain AVMs: 2 bleeds log rank=8.4
• 92 ruptured brain AVMs: 8 bleeds p=0.004
• Consenters only– The relationship disappeared
• 59 unruptured brain AVMs: 1 bleed log rank=1.3
• 52 ruptured brain AVMs: 2 bleeds p=0.26

Time to first seizure
Consenters (red) and non-consenters (black)
Time (days)
1825146010957303650
Pro
po
rtio
n w
itho
ut
a s
eiz
ure
1.1
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Non-consenters 76 49 37 23 6 1
Time to first seizure
Consenters (red) and non-consenters (black)
Time (days)
1825146010957303650
Pro
po
rtio
n w
itho
ut
a s
eiz
ure
1.1
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Log rank=4.1 p=0.04
42 outcomes
13 outcomes

Conclusions• Consenters are systematically different from non-consenters in unpredictable
ways: this cannot be estimated in advance• The only way to measure consent bias is by obtaining data from non-consenters –
Catch 22• Insistence on consent from everyone will:
– be increasingly difficult and costly, waste investigator time on REC forms and delay research, and waste time with designing and administering consent forms
– harm some individual patients (over-consent)– bias non-intrusive observational research – which will then get the wrong result– which will damage individual and public health– and waste public money on research and practice– less observational research will be doneWhat better way to waste money and damage patients?

To cut the red tape
• do not over react to the law (like many ethics committees)• better organise and fund only necessary bureaucracy and have
it dealt with by well resourced support staff (NRES)• greater research professionalism (governance issues)• better involve patients (eg James Lind Alliance)• better inform the media (double-edged sword)• exploit +++ your own experiences as a patient• evidence based criticism, or anecdotes, depending on the
audience • rebadge research as audit – SIVMS was saved by SAIVMS –
Scottish Audit of Intracranial Vascular Malformations

We are swimming in a bureaucratic sludge, awash with consultancies, incomprehensible accountancy language, over-management, juvenile debate on aims and strategies, pseudo business practice and the dreaded “mission”
Gerry Mulgrew, New Communicado Theatre Company, letter to the Scotsman on 1st June 1999
Medical researchers are not alone………

• Irritated - because of the constant trivia brought up by minor bureaucrats, and the huge opportunity costs of keeping them happy
• Exhausted - because of the extreme effort to get through all the regulation from ethics to R&D to insurance issues, to sponsorship problems, to contracts with all and sundry
• Insulted - to be told how to do clinical research by people who have done little if any themselves
• Angry - because (over) regulation can force researchers either to do bad research with misleading results, or to give up research altogether (private practice can be very tempting)
• Even angrier - because my own health is being compromised by over-regulation, as well as the health of countless others
So how do I feel?
I want to be trusted……

Despite their very occasional failings, today I put mytrust in…
There has never in the UK been a successful prosecution for the inappropriate use of medical records for research – so again, get regulation in proportion to the risk of harm and trust researchers, regulated by ethics committees and the GMC, not to abuse confidential medical records

But we researchers do need to be responsible, professional and
careful….The Herald, 27th October 2008


Allen Stanford
Bernie Madoff Fred the shred Goodwin
Would you trustthese people….regulate the bankers!





























