Embed Size (px)
Citation preview

J Clin Pathol 1989;42:567-584
Proposals for the classification of chronic (mature) Band T lymphoid leukaemiasJ M BENNETT,* D CATOVSKY,I M-T DANIEL,$ G FLANDRIN,$D A G GALTON,¶ H R GRALNICK,§ C SULTAN,** THE FRENCH-AMERICAN-BRITISH (FAB) COOPERATIVE GROUP
From the * University ofRochester Cancer Center, Rochester, New York, United States ofAmerica; tAcademicDepartment ofHaematology, The Royal Marsden Hospital, London; $Institut de Recherches sur les Leucemieset les Maladies du Sang, Hopital Saint-Louis, Paris, France; ¶MRC Leukaemia Unit, Royal PostgraduateMedical School, London; §Hematology Service, National Institutes ofHealth, Bethesda, Maryland, UnitedStates ofAmerica; **Service Central d'Hematologie-Immunologie, Hopital Henri Mondor, Creteil, France
SUMMARY Peripheral blood, bone marrow films, and bone marrow biopsy specimens from 110patients, well characterised by clinical and laboratory studies, including electron microscopy, were
reviewed, to determine proposals for the classification of chronic (mature) B and T cell leukaemias.On the basis of cytology and membrane phenotype the following disorders were defined: (i) B celltype: chronic lymphocytic leukaemia (CLL); CLL ofmixed cell type, which includes cases with morethan 10% and less than 55% prolymphocytes (CLL/PL), and a less well defined form withpleomorphic lymphocytes but less than 10% prolymphocytes; prolymphocytic leukaemia (PLL);hairy cell leukaemia (HCL); HCL variant; splenic lymphoma with circulating villous lymphocytes;leukaemic phase of non-Hodgkin's lymphoma (follicular lymphoma, intermediate, or mantlezone lymphoma and others); lymphoplasmacytic lymphoma with peripheral blood disease (mostlyWaldenstr6m's macroglobulinaemia); and plasma cell leukaemia. (ii) T cell type: T/CLL, which wasdifferentiated from reactive T/lymphocytosis; T/PLL; adult T cell leukaemia/lymphoma; andSezary's syndrome.The recognition of distinct entities within the B and T cell leukaemias seems to have clinical and
epidemiological connotations. It is hoped that these proposals may serve as the basis for further work,discussion, and improved management of patients.
For many years chronic lymphocytic leukaemia (CLL)was thought to be a highly variable disease and theheterogeneity ofthe morphological appearances of thelymphocytes seen in blood films was accepted as partof the variability. Although it came to be accepted thatabnormal lymphoid cells could appear in the bloodduring the course of non-Hodgkin's lymphoma(NHL) and that these were sometimes distinctiveenough to merit special names such as "lymphosar-coma cells" and "notched-nucleus cells" found indiffuse lymphocytic lymphoma and follicular lym-phoma, respectively, and the Sezary cells of S6zary'ssyndrome, no systematic attempt was made to codifythe whole spectrum in relation to the pathological and
Accepted for publication 2 February 1989
clinical profiles. In the 1970s the advent of immuno-logical techniques for characterising a whole range ofmembrane molecules, usually glycoproteins, and somecytoplasmic constituents, introduced a new dimensioninto our understanding of the immune system and theprovenance and characterisation of many cell types.This new knowledge was rapidly applied to lympho-proliferative diseases.The first broad characterisation into B and T cells
soon led to the recognition that in most cases CLLaffected B lymphocytes. S&ary cells were alwaysfound to be T cells, while the cells of hairy cellleukaemia (HCL), whose origin was controversial formany years, were finally accepted as B cells. Prolym-phocytic leukaemia (PLL), first recognised on clinicaland cytomorphological grounds,' was of B cell originin most cases, but ofT cell origin in about 25%.2The discriminating power of immunological tech-
567
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

568niques was greatly strengthened by the use of mono-clonal antibodies against many cell surface epitopes.Some of these reagents were useful for identifying Band T cells while others helped to identify particularmaturation stages of T lymphocytes. The applicationof morphological and immunological methods hasreinforced the value of cytomorphology and hasproved advantageous in increasing our understandingof the heterogeneity of B CLL itself. Nevertheless, inpractice the cytological diagnosis of the chroniclymphoid leukaemias and allied conditions remainsdifficult because of their extreme variability. Certaincytomorphological features and immunologicalprofiles are so strongly associated that a specificdiagnosis can be suggested. In a few cases, however, aprecise assignment cannot be made with confidence.
Cytogenetic studies are becoming increasinglyimportant in the investigation of the lymphoid malig-nancies and point the way to the investigation of basicmolecular defects in the genome. Some of the mor-
phological types have been found to be constantlyassociated with particular chromosomal transloca-tions-for example, the translocation t(14;18)regularly found in follicular lymphoma3 and whichinvolves the fusion of an immunoglobulin coding genewith the bcl-2 sequence to yield a hybrid gene,4 trisomy12 in CLL,5 t(l 1; 14) in B cell PLL6 and inv(l4) in T cellPLL.7The conclusions resulting from the work so far
accomplished by the FAB group are necessarilyprovisional but go some way towards establishingguidelines in the cytological characterisation of thechronic lymphoid leukaemias. The extent to whichtheir more detailed categorisation will be clinicallyimportant remains to be worked out, although thebroad correlations are already well established.
Markers for B and T lymphocytes
The identification of specific markers for B and T cellshas provided the basis for two broad categories oflymphoid leukaemias. Two markers for B and Tlymphocytes were the first to be categorised-mem-brane immunoglobulins (SmIg), also shown in thecytoplasm (CyIg), and a rosette test with sheep
Bennett, Catovsky, Daniel, et al
erythrocytes, E-rosette, also recognised by mono-
clonal antibodies of the cluster of differentiation two(CD2). These methods and an increasing range ofmonoclonal antibodies are now essential for theclassification of leukaemias and lymphomas. In addi-tion to "pan-B" or "pan-T" reagents, which define thetwo main lines of differentiation, some antigens are
restricted to some maturation stages and thereforefulfil a useful role for the subclassification. Forexample, B lymphocytes ofCLL are characterised by a
distinct pattern of reactivity8 that consists of theexpression of SmIg (weakly) and of the CD5 antigen,high affinity for binding mouse erythrocytes (M-roset-tes), and low expression ofB maturation antigens suchas those detected by monoclonal antibodies FMC7 or
the CD22 group on the cell membrane.The methods to be used and the choice of reagents
will depend on the availability and experience ofindividual laboratories and are beyond the scope ofthis report. Viable cells are stained in suspension byimmunofluorescence methods and observations madeby flow cytometry or fluorescence microscopy. Thedetection of antigens or immunoglobulin on the cellsurface and cytoplasm is also possible on fixed cellpreparations-for example, those prepared by a
cytocentrifuge, or on frozen sections of lymphoidorgans prepared by immunocytochemical methods.The proposals for phenotyping B and T cell disordersare continuously improving with the introduction ofnew monoclonal antibodies.
B LYMPHOID LEUKAEMIASThis group ofdisorders has well characterised clinical,morphological, and histological features. The definingcriterion for diagnosis is the demonstration of amonoclonal population of B cells, shown byimmunoglobulin light chain restriction, and evidenceof B lineage differentiation shown by one or morespecific monoclonal antibodies such as CD19, CD20,or CD24.9The markers recommended for the diagnosis of
chronic B cell leukaemias, listed in tables 1 and 2, areintended only as guidelines. The patterns of reactivityobserved in the most common forms of B cell leuk-aemia and NHL with peripheral blood and bone
Table 1 Immunological methodsfor B cell markers
Reagent Method Designation Specificity
Anti-human Ig Cell suspensions SmIg B lymphocytes (light chain restricted)Fixed cells CyIg
Mouse erythrocytes Spontaneous rosetting M-rosettes B CLL cellsMonoclonal antibodies Cells in suspension or fixed on slides Immunofluorescence (Table 2)
ImmunoperoxidaseImmunoalkaline phosphatase
*Cryopreserved cells may also be used.
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Table 2 Monoclonal antibodiesfor the study ofB cell disorders
CD No Reactivity Commonly used monoclonal antibodies
CD5 Mature T cells (strong) B CLL cells and some NHL cells (weak expression) Leul, TI01, T1, OKCLL, UCHT2CDIO Common ALL antigen, early B cells, and some NHL (follicular lymphoma) J5, OKB-CALLA, VIL-AI, NU-NI,
anti-CALLACDI9 All B lymphocytes from early to late maturation stages B4, Leul 2CD20 Most B lymphocytes BI, Leul6, RFB7, NU-B2CD21 Restricted to intermediate maturation stages B2, RFB6, BA-5CD22 Late B cells, hairy cells B3, Leul4, TO15, RFB4, CLB/BLyJFMC7* Late B cells, hairy cells, B prolymphocytes FMC7CD24 Most B lymphocytes BAICD25 Activated B and T cells; hairy cells Anti-Tac, Tacl, IL-2R1CD38 Activated B and T cells; plasma cells OKTIOAnti-class II MHC All B lymphocytes up to plasma cells; activated T cells and haemopoietic HLA-Dr, OKIa, GRBI, FMC4
antigens* precursors
*Not allocated to a particular cluster of differentiation; FMC7 is probably distinct from CD22, although findings in some of the B cellleukaemias suggest that both appear on the cell membrane at a relatively late stage of B cell maturation (table 3).
marrow disease are summarised in table 3. Thephenotype of a chronic B cell leukaemia is immuno-logically mature and should be distinguished from thatof early B lineage acute lymphoblastic leukaemiaswhich are immunologically immature-for example,positive for the enzyme terminal deoxynucleotidyltransferase (TdT). In the other extreme plasma cellsare associated with the loss ofB cell antigens and classII molecules and the appearance ofnew antigens suchas those detected by CD38 and other monoclonalantibodies such as PCA-l9 or BUl 1.'0 Other reagentsnot included in table 3 are anti-HC2" and LeuM5(CDl Ic)'2 which react with hairy cells. BecauseLeuM5 is also positive in monocytes, its value fordetecting hairy cells may depend on the simultaneousdemonstration of a B cell antigen, such as CD20 orCD24.CLL is the B cell leukaemia which can best be
defined by immunological phenotyping (table 3). Cellsof some NHL (intermediate or diffuse small cleaved),however, share with CLL lymphocytes the expressionof CD5 and have a weaker expression of SmIg than
other NHL and B cell PLL. "Deviation" from thetypical CLL phenotype is seen in cases with anincreased proportion of prolymphocytes or CLL/PL'3in which marker characteristics intermediate betweenCLL and PLL may be seen-for example, strongexpression of SmIg and reactivity with FMC7. '314 Iffour positive criteria for B cell CLL are set: weakSmIg, >30% M-rosettes, <50% CD5 + cells and< 30% FMC7 + cells, a combination of three or fourofthese markers is seen in 80% oftypical CLL, in 65%ofCLL/PL cases, and in none ofthose with a diagnosisof B PLL.'5 Two thirds of cases of B PLL have aphenotype quite different from that of CLL: strongSmIg, low M-rosettes and CD5, and >30% ofFMC7 + cells.'5From the above it is apparent that immunological
phenotyping provides useful information about celllineage and state of B cell maturation. The finaldiagnosis, however, depends on the composite infor-mation derived from clinical features, cell mor-phology, histology and membrane markers. It shouldbe recognised that even with optimal methods there
Table 3 Markers in chronic B cell leukaemias
NHL*
FolicularMarker CLL PLL HCL lymphoma Intermediate SLVL Plasma cell twnours**
SmIg Weak Strong . Moderate Strong Negative
M-irosettes ++ + -/+ -/ + - -CD5 ++ -+++CD19/20/24 ++ ++ ++ ++ ++ ++ -Anti-class II + + + + + + + + + + ++ -FMC7/CD22 -+ + + + + + + ++ -CDIO _ _ t + -CD25 - _ ++ _ _ _ +CD38 - - -/+ -/+ - _/+ + +
+ Indicate incidence at which a marker is positive in > 30% of cells in a particular B cell tumour (+ + 80-100%; + 40-80%; - + 10-40%;- 0-9% of cases).*Non-Hodgkin's lymphomas (NHL) with a high incidence of peripheral blood or bone marrow disease.**Myelomatosis and plasma ceil leukaemia; Waldenstr6m's marcoglobulinaemia cells show a similar phenotype except for sharing somefeatures with PLL, HCL, and NHL (expression of FMC7, CD22, and some other B cell antigens).
Classification ofB and T cell leukaemias 569
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

570are always some cases with atypical features that donot fit exactly in any of the named diagnoses, perhapsreflecting the great heterogeneity of the lymphoidsystem.
T LYMPHOID LEUKAEMIASThere is considerable heterogeneity in this group ofdisorders because of the existence ofmany functionalsubsets and stages of maturation of T lymphocytesfrom which the leukaemia may originate. The reagentsused for the diagnosis and classification of the T cellleukaemias are listed in table 4.The main distinguishing feature between the
immature (or thymic derived) and mature (or post-thymic) T cell disorders is the presence in the former,which comprises acute T lymphoblastic lymphoma, ofTdT and thymic antigens, such as those recognised byCDI a. Neither TdT nor CD Ia are found in chronic Tcell leukaemias (table 5). Important for their consis-tency as pan-T markers are E-rosettes and CD2 andCD3. The pan-T reagents CD5 and CD7 are more
consistently positive in thymic than in post thymic Tcell malignancies (table 5).Most types of mature T cell leukaemia involve
CD4+ cells; cases of T CLL and persistent T lym-phocytosis are often, but not always, CD8 + prolifera-tions. Even within CD4 + disorders the neoplasticcells may represent different functional subsets. Inaddition, other reagents may add further diagnosticinformation-for example, CD25 is characteristicallypositive in adult T cell leukaemia/lymphoma (ATLL)cells and rarely in otherT cell leukaemias. Monoclonalantibodies such as Leu7, CD16, and CD llb whichreact with larger granular lymphocytes and cytotoxiccells, including natural killer cells, can further identifyrare types ofT cell leukaemia, which often come underthe designation ofT CLL.As with the B cell disorders, immunological meth-
ods are necessary to define T cell leukaemias andprovide guidance to specific diagnoses, but are not
Table 4 Monoclonal antibodiesfor the study of Tcelldisorders
Commonly usedCD No Reactivity monoclonal antibodies
CDIa Cortical thymocytes; Leu6, T6, OKT6, NA134,T lymphoblasts NU-T2
CD2 Receptor for sheep TI1, OKTI 1, Leu5erythrocytes; most T cells
CD3 Mature T lymphocytes OKT3, Leu4, UCHT1, T3CD4 Helper/induced subset OKT4, T4, Leu3, NU-TH/lCD5 (Table 2)CD7 Mature and immature T cells 3A1, WT1, Leu9, OKT16CD8 Cytotoxic/suppressor subset T8, OKT8, Leu2
NU-T5/C, UCHT4CD25 (Table 2)
Bennett, Catovsky, Daniel, et alTable 5 Markers in chronic (mature) T cell leukaemias
Sezary'sMarker T-CLL T-PLL ATLL syndrome
TdTCDlaE-rosettes + + + + + + + +CD2 ++ ++ ++ ++CD3 ++ + ++ ++CD4 - + + + + +CD5 ++ ++ ++CD7 - ++ _ _CD8 ++ -1+ _ _CD25 - - ++ -CD38 - - - _
+Indicate rate at which a marker is positive in > 30% of cells inparticular T cell leukaemias (+ + 80-100%); -/+ 10-40%;- 0-9% of cases).
sufficient to define clinicopathological entities. Forthis, the immunological features need to be integratedwith cytomorphological and histopathological find-ings. Furthermore, monoclonal antibodies cannotestablish whether a T cell proliferation is clonal. This isnow possible by analysis of the rearrangement ofthe Tcell receptor ,B- and y-chain genes'6 and bychromosome studies.
Material and methods
Peripheral blood and bone marrow films from a totalof 110 cases with a diagnosis of chronic B and T cellleukaemias were reviewed. We excluded from reviewcases of Burkitt's lymphoma/leukaemia and large celltransformation of T and B cell NHL. The group metfirst in May 1985 in London and analysed materialfrom 33 cases previously circulated to examine themorphological spectrum ofdisorders. No informationwas then made available on clinical and cell markerstudies. A preliminary classification proposal wasestablished and evaluated with subsequent analysis of59 new cases. These were discussed at a secondworkshop in Bethesda in April 1986. A set of slidesfrom 20 cases in which there was no consensus on thediagnosis was reviewed again and discussed with thehelp of a television projection microscope. Formaldiagnostic criteria, formulated after the immuno-logical information and available in all cases, were alsoconsidered. In a substantial number of cases, bonemarrow and lymph node biopsy specimens were alsoreviewed and in some cases of particular diagnosticdifficulty, electron microscopy photomicrographswere available. In October 1987 material from another18 cases was examined in London, with particularemphasis on the leukaemic phase ofNHL.
CLINICAL-MORPHOLOGICAL DISEASE ENTITIESThe group agreed that it was necessary to examine the
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemiasB and T leukaemias separately. It was recognised thatfor some of them, such as CLL, HCL, or ATLL, thediagnosis could be made by morphology alone, but forothers the B or T cell nature could not always beascertained without the appropriate cell markers.
B CELL LEUKAEMIAS-MORPHOLOGY OF THE
CELLSThe characteristics ofthe various types oflymphocytesseen in the most common chronic B cell leukaemias aresummarised in table 6. Here the main distinguishingfeatures between the small lymphocytes of typicalCLL and the large lymphocytes and prolymphocytesseen in CLL of mixed cell type are emphasised. Asubtle distinction can be made between the pleomor-phic prolymphocytes seen in CLL/PL and the moreuniform ones seen characteristically in B cell PLL. Inthe leukaemic forms ofNHL cleaved or cleft cells arecharacteristic of follicular lymphoma, and cells ofvariable morphology and some degree of nuclearirregularity are a feature of other types ofNHL.
Chronic lymphocytic leukaemiaPeripheral blood Defining criteria using the currentstaging systems for the disease suggest that a persistentlymphocytosis of > 10 x 109/l is sufficient for a diag-nosis of CLL. In adults with lymphocytosis between 5and 10 x 109/I cell marker studies are necessary toconfirm the presence of monoclonal B cells. In typicalcases of CLL the cells are small with a conspicuousthough narrow rim of cytoplasm (fig la). Both thenuclear and cytoplasmic outlines are regular, althougha small degree of nuclear irregularity with a kidneyshape or a small indentation is seen in some cases (figlb). The cytoplasm is homogeneous and weaklybasophilic and granules are not seen. The nuclear:cytoplasmic ratio is high. The nuclear chromatin ischaracteristically dense with clumps of darkchromatin separated by narrow pale spaces. With thestandard Romanovsky stains the nucleoli are eithernot visible or are inconspicuous and small. Some
571
morphological variation is seen from patient topatient. In some, the cytoplasm tends to be a littlemore abundant. When more than 10% of the lym-phocytes are large or are prolymphocytes the diag-nosis of mixed cell type CLL should be considered.Smudge cells are artefacts ofblood films, which are notdiagnostic, but nevertheless are characteristic of B cellCLL and in general tend to be more conspicuous witha high white cell count.Bone marrow Aspirates are generally hypercellularand show lymphocytic infiltration. Bone marrow
biopsy specimens are necessary to define the variouspatterns of infiltration and to exclude the diagnosis ofNHL such as follicular lymphoma. The extent ofinfiltration, which may be interstitial, nodular, mixedor diffuse, correlates with the clinical state.'7 18Lymph node biopsy Although lymph node disease inCLL is common, biopsies are not performed routinely.They are necessary in cases with low lymphocytecounts or when the membrane phenotype departsconsiderably from the typical pattern described intable 3, and, when the counts are high, if the mor-
phology suggests a diagnosis of NHL.
CLL, mixed cell typesIn several cases diagnosed as CLL the morphologicalfeatures are different from those described above. Twotypes of this form of CLL may be found: (i) a mixture(dimorphic picture) of small lymphocytes and prolym-phocytes (> 10% and less than 55%) designated CLL/PL; and (ii) a spectrum of small to large lymphocyteswith occasional (less than 10%) prolymphocytes.There is currently no clear evidence for a biologicaldisadvantage in the latter group with respect to typicalCLL, but data are accumulating which suggest refrac-toriness to treatment and a worse prognosis for theCLL/PL group.""
In two thirds of cases of CLL/PL the compositemembrane phenotype of B CLL (see above) is found,and in one third only one or two of the CLL markers(usually CD5 or high M-rosettes) are demonstrable.'5
Table 6 Types ofleukaemic B lymphoid cells
Cell type (disease) Size Chromatin Nucleolus Cytoplasm Otherfeatures
Small lymphocytes (CLL) < 2 red blood cells Clumpted in coarse Absent Scanty high Regular nuclear outlineblocks nuclear:
cytoplasmic ratioLarge lymphocytes (CLL, > 2 red blood cells Clumped Inconspicuous or small Low nuclear: Variable sizemixed cell) cytoplasmic
ratio, variableProlymphocytes (PLL) > 2 red blood cells Clumped One, prominent Low nuclear: Variable size
cytoplasmic ratioPleomorphicprolymphocytes > 2 red blood cells Clumped Central and prominent Variable nuclear: Variable size(CLL/PL) cytoplasmic ratio
Cleft cells (FL) 1-2 red blood cells Homogeneously Absent or one or two Scanty; not visible One or two shallow orcoarse inconspicuous or narrow rim deep narrow nuclear
clefts from angularbase
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Bennett, Catovsky, Daniel, et al
0
._.
.;*_
.-_' lb
Although clinical and laboratory features of CLL/PLare at least in some respects intermediate betweenthose ofCLL and PLL, marker studies suggest a closeraffinity with CLL.'3" The small lymphocytes ofCLL/PL tend to have a larger volume than those of CLL2'and the prolymphocytes tend to be more pleomorphicthan those seen in PLL (fig Ic). These cases areclinically heterogeneous and include patients withtypical CLL which evolves into a more aggressiveform, described as CLL in "prolymphocytoid" trans-formation,22 and others who present with an increased
proportion of prolymphocytes and whose course maynot be progressive.The cases in the second group ofCLL of mixed cell
type are less well defined and less common. These arecharacterised by larger cells than those seen in typicalCLL, tend to have a lower nuclear:cytoplasmic ratio,and a trend towards increased cytoplasmic basophilia.A clear distinction between two cell populations bysize (small and large) is not usually possible. Thepercentage of prolymphocytes is less than 10%. His-tological studies of lymph nodes and bone marrow
572
0lddk.
-Aod&6
i. n"i.Z,IF
ii.
1.
jilift Agibikri.
lqw:,Adbftf-,.d-..
'"W.
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemias
hg
r
.1. t A
n... .. .....5Y
I_0o,..
i
is-.....
k
biopsy specimens are important to distinguish thesecases from some forms of NHL.
Prolymphocytic leukaemiaPLL is a distinct disorder characterised by a high whitecell count and splenomegaly without lymphaden-opathy.' The membrane phenotype of the prolym-phocyte is quite distinct from that ofCLL (table 3) buthas similarities to that of other B cell leukaemias. Theprolymphocyte is the predominant cell in peripheral
blood films (> 55%, usually > 70%) and is character-ised (table 6) by its large size, round nucleus with aprominent vesicular nucleolus, relatively well conden-sed nuclear chromatin and a lower nuclear:cytoplas-mic ratio than the small lymphocyte of CLL (figs ldand e). These morphological features must be soughtin well spread areas of blood films. The bone marrowinfiltration is diffuse, not very different from that ofCLL, or has a mixed interstitial-nodular pattern.Histological appearances oflymph nodes show diffuse
573
1;..A`wl-0
i
l
I
2
I
0
Cc- 'k-11-.. j-ff
Ill ...1".
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Bennett, Catovsky, Daniel, et al
I __2.___.
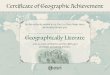
Fig 1 Peripheral bloodfilms ofB lymphoid leukaemias. (a and b) Chronic lymphocytic leukaemia (CLL). (c) CLL withmore than 10% prolymphocytes. (d and e) Prolymphocytic leukaemia. (fandg) Hairy cell leukaemia (HCL). (h) HCLvariant. (i andj) Splenic lymphoma with villous lymphocytes. (k and l) Follicular lymphoma. (m and n) Intermediate NHL.(o andp) Plasma cell leukaemia.
disease with or without a pseudo-nodular pattern.23The histological appearance of the spleen shows whiteand red pulp infiltration, with large proliferativenodules in the white pulp with a characteristic bizonalappearance-dense at the centre and lighter at theperiphery.24
Hairy cell leukaemiaThe hairy cell is the outstanding morphologicalfeature of this disease.' It has fine, irregular cytoplas-mic projections or villi and is, overall, larger than mostother lymphocytes. On peripheral blood films thecytoplasm stains light blue and has a poorly definedoutline (figs lf and g). Fine azurophilic granules areseen occasionally. Rod-shaped inclusions with a palecentre correspond to the ribosome-lamellar complexesseen at electron microscopic examination. Thenuclear:cytoplasmic ratio is low and the nucleus isexcentrically placed. The nucleus is oval, round, or
kidney-shaped. The nuclear chromatin has a finedispersed pattern and nucleoli are inconspicuous,small, and usually single. The bone marrow is alwaysaffected in HCL but may be difficult to aspiratebecause ofassociated fibrosis. Material available fromscanty aspirates or touch print preparations may beuseful to identify hairy cells. Bone marrow biopsysections are essential for diagnosis. These show varia-ble degrees of infiltration by hairy cells which can beidentified by the nuclear shape, the chromatin pattern,and the clear zone that separates one cell from anotherresulting from the abundant cytoplasm. The his-tological appearances of the spleen show a distinctivepattern of red pulp infiltration with the formation ofpseudo-sinuses and widening of the pulp cords. Mem-brane markers (table 3) support the diagnosis ofHCL,in particular the combined reactivity with CD25,LeuM5, and HC2. Tartrate-resistant acid phos-phatase (TRAP) is a typical cytochemical finding.26
574
AM&L
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemias
Hairy cell variantThis relatively rare disorder was described as havingmorphological features which are intermediate bet-ween hairy cells and prolymphocytes.2728 The charac-teristic cells have an abundant cytoplasm, more baso-philic than in hairy cells, but with similar villousprojections, moderately condensed heterochromatinwith a prominent nucleolus as in PLL cells, and aslightly higher nuclear:cytoplasmic ratio than typicalhairy cells (fig lh). The disease runs a chronic coursewith splenomegaly and a high white cell count (usually> 50 x 10/1, a rare finding in typical HCL) withoutmonocytopenia. As in HCL, the variant cells infiltratethe spleen mainly in the red pulp. The membranephenotype is close to that of prolymphocytes. Incontrast to typical hairy cells, HCL-V cells do notreact with CD25 and HC2 but some cases are LeuM5positive. Membrane IgG is often found on the cellmembrane and in some cases SmIg cannot be shown.
Splenic lymphoma with villous lymphocytes (SL VL)It hs been recognised that some patients suspected onclinical and laboratory grounds (splenomegaly andcirculating lymphocytes with villous projections) ashaving HCL, have, in fact, a predomantly splenic formof NHL, as established by analysis of the histologicalappearances of the spleen.2930 A small monoclonalband is shown in the serum or urine in two thirds ofcases. The white cell count is usually between 3 and 38x 109/129 and the circulating lymphocytes, whichcomprise most of the cells, are larger than CLLlymphocytes and are close to the size of prolym-phocytes. The nucleus is round or ovoid, has clumpedchromatin, and in half of the cases has also a distinct,small nucleolus (fig li). The amount of cytoplasm isvariable and is moderately basophilic. The mainfeatures are the presence of short villi, often localisedto one pole of the cell. The nuclear:cytoplasmic ratio ishigher than in hairy cells of HCL and HCL-V; a fewcells show lymphoplasmacytic features (fig lj).Membrane markers ofSLVL cases are similar to thoseofB PLL. Unlike HCL cells, these villous lymphocytesdo not react with HC2, CD25, LeuM5, or cyto-chemically with the TRAP reaction. The differentialdiagnoses to be considered are CLL, B PLL, HCL andHCL-variant. The histological appearances of thespleen show white pulp disease (in contrast to HCLand HCL-V), with or without clinically important redpulp infiltration.' 3 The bone marrow is not infiltratedin half of the cases; in others there is moderate topronounced diffuse or nodular infiltration.
Leukaemic manifestations ofNHLBefore the era of immunological markers severalconditions (B and T derived) were broadly describedas "lymphosarcoma cell leukaemia".3' These cases
575were thought to represent de novo lymphoid leu-kaemias, but it is clear that these are cases of NHLwhich present in a leukaemic phase of their disease orwhich have progressed to a leukaemic phase. The mostcommon form is follicular lymphoma in leukaemicphase.32"- Spiro et al reported that 38% of cases withhistologically confirmed follicular lymphoma pre-sented with a lymphocytosis greater than 5 x 109/lwhich was described as "CLL-like syndrome".32 In asignificant proportion of such cases, however, themorphological features were different from those ofCLL.Whenever it is suspected that a lymphocytosis is
associated with a NHL, bone marrow and lymph nodebiopsy sections are an essential part of the investiga-tion. When referring to this group of cases, only thosein which the disease presents in a leukaemic phase,which may be arbitrarily defined as > 5 1 09/l abnormallymphocytes, will be considered here. This does notpreclude the identification of a small percentage ofNHL cells in the peripheral blood. Although theabnormal circulating cells may be derived from severalhistological subtypes ofNHL,33 the most common andbest characterised form is the leukaemic phase offollicular lymphoma.34 Cases of stage IV NHL withbone marrow disease35 but no peripheral blood diseasewill not be discussed.
Leukaemic phase offollicular lymphomaAlthough in the series of Spiro et al the highestlymphocyte count recorded was 30 x 10Q/1,32 caseswith a higher white cell count (45-220 x 109/l) haverecently been recognised.3 The morphologicalfeatures of the circulating cells in follicular Iymphoma(table 6) are small, cleaved lymphocytes (often smallerthan CLL lymphocytes) with a high nuclear:cytoplas-mic ratio and very scanty cytoplasm, usually confinedto a thin rim visible between the concavities of thenucleus (figs ik and 1). The nuclear chromatin isuniformly condensed without clumping. Prominentbut usually very narrow nuclear clefts or fissures areseen in > 30% of cells; these clefts often arise in sharpangles from the nuclear surface and when they aredeep they divide the nucleus in two. These features ofthe nucleus are even more apparent by ultrastructuralanalysis (fig 2). The cell outline is often angular andnucleoli are eiher absent or barely visible. Membranemarkers (table 3) show differences with the findings inB CLL; SmIg is strong, the percentage of M-rosettes islow, FMC7 is positive, and CD5 is usually negativeand CDI0 is often positive. These findings are helpfulwhen the cytological features described above are nottypical and suggest a diagnosis of CLL. Bone marrowdisease is common and typically shows a para-trabecular localisation of lymphocytic infiltration,35although diffuse infiltration can also be found.
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Bennett, Catovsky, Daniel, et al
Fig 2 Electron microscopy oftwo circulating cellsfromfollicular lymphoma.
Intermediate NHL or mantle zone lymphomaThere are no detailed studies ofthe leukaemic manifes-tation of this lymphoma.3638 The most common cell isof medium size, has condensed chromatin, an incon-spicuous nucleolus with slight nuclear irregularitiesbest characterised as indentations and clefts (fig lm).The latter are not as pronounced or as deep as infollicular lymphoma cells. Larger cells with a highnuclear:cytoplasmic ratio and without a prominentnucleolus are seen (fig In). In a few cases the appearan-ces are those given above for CLL of mixed cell types,except that most cases of intermediate NHL have apaucity of small lymphocytes. Bone marrow biopsyspecimens show diffuse disease. The lymphoid popula-tion is monotonous and the cells are larger than CLLlymphocytes and tend to have an irregular nuclearoutline. The above morphological criteria werederived from the examination of blood and bonemarrow films from 12 cases in which there was aconsensus for the diagnosis ofNHL-intermediate typein leukaemic phase. The histopathological diagnosisof all these cases was made on the examination oflymph node biopsy specimens by independentobservers. Membrane marker studies show CD5+cells'39 and SmIg staining of moderate intensity withp and ( as the main heavy chain classes.39 CDIO ispositive when tested on all cell suspensions butnegative by immunocytochemistry.
Lymphoplasmacytic lymphomaThese are cases in which monoclonal immuno-globulin bands are present in the serum and includeWaldenstr6m's macroglobulinaemia and also cases ofSLVL, described above. In Waldenstr6m's macro-globulinaemia the paraprotein concentrations are> 20 g/l, while in SLVL the IgG or IgM paraproteinband concentrations are < 20 g/l while the white cellcount is usually > 10 x 109/l in SLVL and <10 x109/l in Waldenstr6m's macroglobulinaemia.9 Thecirculating lymphoid cells in Waldenstr6m'smacroglobulinaemia comprise a mixture of small andlarge lymphocytes, sometimes with an excentricnucleus and pronounced cytoplasmic basophilia andmorphological diversity. The bone marrow is oftendiseased in Waldenstr6m's macroglobulinaemia witha mixture of cells of different nuclear maturity, somewith dense chromatin and others with fine chromatin,and variable basophilia. A proportion of plasma cellsand of mast cells is characteristic of Waldenstr6m'smacroglobulinaemia.
Plasma cell leukaemia (PCL)PCL refers to patients with primary leukaemia and notthe terminal phase of myelomatosis (multiplemyeloma) in which abnormal plasma cells circulate in2% of cases.' PLC is usually an acute illnesssometimes resembling acute leukaemia. Hepato-.
576
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemiassplenomegaly is more common and bone lesions areless common than in myelomatosis, while hypercal-caemia and renal failure are common. We recognisetwo morphological types of PCL. In one, the cells aresmall and range from lymphocytes with basophiliccytoplasm to plasma cells, and in the other they areblast-like cells. In the former but not in the latter typethere is nuclear excentricity and a clear Golgi zone.Intense basophilia is a feature mainly of the smallplasmacytic type (figs lo and Ip). Membrane markerstudies (table 3) are helpful in recognising the plas-mablasts. Antigens normally found in B cells arelacking but new late B antigens appear. The presenceof monoclonal CyIg and expression of CD38 arediagnostic. Ultrastructural analysis often disclosesplasma cell features.4' Other laboratory investigations(Bence Jones proteinuria, hypercalcaemia) may alsocontribute towards a diagnosis of PCL.T CELL LEUKAEMIAS-MORPHOLOGY OF THECELLSOnce markers have assigned a lymphocytic prolifera-tion to the T cell series (see above) the next step is todefine the morphology ofthe cells, and it is on this thatthe classification will depend. The cells seen in themature T cell leukaemias include lymphocytes with arange of morphological types: (i) large granular lym-phocytes, characterised by abundant cytoplasm andazurophil granules; (ii) prolymphocytes with aprominent nucleolus, basophilic cytoplasm, and noazurophil granules; (iii) pleomorphic, polylobed cells;and (iv) small or large cerebriform cells. Lymphocyteswith a mature morphology but without azurophilgranules are present in normal peripheral blood butare very rarely seen as the predominant cell in T cellleukaemias. Such cells, however, may be seen in thesmall cell variant ofT cell PLL but, on ultrastructuralanalysis, the latter always show a distinct nucleolus.42T cell Iymphocytosis and T CLLThe upper limit of the absolute lymphocyte count inadults is about 4-8 x 109/l. Most normal lymphocytesare small to medium sized with a high nuclear:cyto-plasmic and a densely clumped nuclear chromatin;nucleoli are usually indistinct. Most cells are agranularwith a thin layer ofbasophilic or colourless cytoplasm.About 80% ofthe circulating lymphocytes are ofT cellorigin. Cases of reactive B cell lymphocytosis areextremely rare. More frequently, an absolute increasein the number of atypical T lymphocytes is seen as aresult of several infective processes. Reactive lym-phocytosis is selflimiting and is rarely above 5 x 109/l.The most common causes are viral infections, EpsteinBarr virus or cytomegalovirus in adults, and Bor-detella pertussis in children in which very high countsmay occur. The atypical cells have a lower nuclear:cytoplasmic ratio than normal, are often two to four
577times the size of normal lymphocytes, and havevariable cytoplasmic basophilia; sometimes thenucleus is irregular and resembles that of the mon-ocyte but almost always has the coarsely clumpedchromatin characteristic of lymphocytes.
In contrast to reactive lymphocytosis, chronic orpersistent (> 3 months) T lymphocytosis of unknowncause occurs and further study shows the proliferationto be clonal. The lymphocytosis tends to increasegradually over the ensuing months or years and isoften associated with cytopenias, usually neutropenia.If T lymphocytosis of >5 x 109/l persists for over sixmonths and consists of a relatively uniform popula-tion of lymphocytes, the diagnosis is likely to be TCLL; rarely, the white cell count is >20 x I09/1. Inmost cases the cells are large granular lymphocytes.43-5These have a low nuclear:cytoplasmic ratio and showseveral fine or sometimes coarse azurophil granules inthe abundant pale blue cytoplasm; occasional cellswith the same morphology are agranular. The nucleusis round or oval, slight excentric, and has clumpednuclear chromatin; nucleoli are rare, as are smudgecells (figs 3a and b). These lymphocytes, which con-situte 50-95% of the peripheral blood leucocytes,react strongly with cytochemical reactions for acidphosphatase and I glucuronidase, but weakly or not atall with a-naphthyl acetate esterase (ANAE).4 Ultras-tructural analysis shows that the azurophil granulesare distinct structures designated as parallel tubulararrays.4'
In addition to cases with a chronic course and stableT lymphocytosis, are those with more bulky disease ofliver and spleen and progressive course with risingwhite cell counts. In both types of T CLL thephenotype is that of the so-called Ty-lymphocyte witha spectrum of antigenic profiles; most cases with achronic course have a CD3 +, CD8 +, CD4-,Leu7 +, membrane phenotype (table 5). Cases withunusual phenotypes, representing granular lympho-cytes rarely seen in normal peripheral blood-forexample, CD4+, CD16+; CD8+, CDllb+, etc.,tend to have a more aggressive evolution. DNAanalysis with probes for the ( and 5 chain genes of theT cell receptor shows the genes to be in a rearrangedconfiguration'6 in most cases of chronic T celllymphocytosis as defined above, thus justifying theterm of T CLL or large granular lymphocyte leuk-aemia for this group of patients. Chronic T lympho-cytosis can be distinguished from T CLL only byproving clonality by DNA'6 or cytogenetic analysis inthe latter condition.45Bone marrow aspirates in cases of T CLL show
infiltration of variable degree; minor in the earlystages, >50% in later stages."445 Bone marrow tre-phine biopsy specimens show focal or more diffuseaccumulations which do not displace the normal bone
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Bennett, Catovsky, Daniel, et al
IS,--.
I S
l'-I.
marrow cells. In some cases a maturation arrest of thegranulocytic series is seen and in others there iserythroid hypoplasia. The latter features are closelyassociated with the presence ofneutropenia or aregen-erative anaemia."45
Tprolymphocytic leukaemiaAbout 20% of patients who present with clinical andmorphological features of PLL have a T cell malig-nancy.2 Within the mature T cell leukaemias T PLLmay represent up to 40% of cases. Like B PLL, in T
PLL the white cell count is usually > 100 x 109/l atpresentation but, in contrast, there are usually lym-phadenopathy, skin lesions, and serous effusions aswell as splenomegaly, and the course is aggressive. Thecirculating cells in half of the cases ofT PLL resemblethose ofB PLL and unless cell markers are performed,it may be difficult to distinguish between these twodisorders. In other cases T PLL cells have lesscytoplasm and a higher nuclear:cytoplasmic ratio thanB PLL cells42; T prolymphocytes may also have anirregular nuclear outline (figs 3c and d). In some cases
578
.-AMIRLIddgmbk
A'Ibb
ti "
..Adfi.-
4-t-
Aft..
f,
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemias
-RAM r
h
'I
hA5->s.w.,
Fig 3 Peripheral bloodfilms ofchronic T cell leukaemias.J (a and b) T-CLL or proliferation oflarge granular
lymphocytes. (c and d) Tprolymphocytic leukaemia. (e,fandg) adult T cell leukaemia/ lymphoma. (h) large Sezarycell. (i) Small Sezary cells or Lutzner cells.
the cells are small and the nucleolus is not easily seenby light microscopy. In general, T prolymphocyteshave a deep basophilic cytoplasm which sometimeseven suggests plasma cell differentiation. As a result ofthis morphological heterogeneity some cases havebeen described as T CLL with "helper" phenotype orT CLL of "knobby" cell type (when nuclearirregularities are present). Thejustification for a singledisease entity in T PLL cases is threefold: (i) similarpresenting features and aggressive clinical course; (ii)similar ultrastructural features, in particular aprominent nucleolus (fig 4) and the presence of largeand dense localised granular structures4' whichcorrelate with the strong positivity with cytochemicalreactions for most acid hydrolases, including ANAEM;and (iii) a consistent chromosome abnormality,inv(14) in two thirds of the cases studied, with similarbreakpoints in 14ql1 and 14q32.7 Membrane markers(table 5) show that most T PLL are CD4 +, CD8 -proliferations; a minority coexpress CD4 and CD8and a few are CD4 -, CD8 +.242 Unlike other matureT cell leukaemias, in particular those with a CD4+phenotype, T PLL cells express strongly the CD7antigen.
There is little information on the histopathological
features of T PLL. The few cases studied showeddiffuse infiltration ofthe splenic red pulp with oblitera-tion of the white pulp. In lymph nodes the infiltrationis diffuse and affects predominantly paracortical areas.The bone marrow is usually diffusely infiltrated andshows increased fibrosis.4"
Adult T cell leukaemia/lymphomaOver a decade ago the first reports of an unusualsyndrome in Japanese adults appeared.49" Thepatients had manifestations of generalised lym-phadenopathy associated with circulating abnormallymphoid cells associated with hypercalcemia, bonelesions, skin lesions and bone marrow disease.The white cell count ranges widely and the percen-
tage of abnormal cells ranges from 10 to 80%.5°5I Thecells vary considerably in size from that of a smalllymphocyte to a large mononuclear cell (over 14 pm).The nuclear chromatin is relatively homogeneous andclumped or condensed. The nuclear outline has beendescribed variously as convoluted or "clover leafed".This conveys the most striking feature of the cells,pronounced polymorphism (figs 3e, f, and g). Nucleoliare uncommon and when present are small. Thecytoplasm is agranular and basophilic. Occasionally it
579
.; .7. 17.-'.t.i4, k,",... ..'r, 11.
.4
gl
t7"
04
i
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Bennett, Catovsky, Daniel, et al
Fig 4 Ultrastructure ofa prolymphocytefrom a case of T-PLL.
is difficult to distinguish the cells from those seen inSezary's syndrome; electron microscopy may help forthis purpose (fig 5). There are also instances in which TPLL may be confused withATLL because the promin-ent nucleolus normally seen in T PLL cells can beindistinct and the nuclear outline may be irregular.42 Inaddition to polylobed cells, some blastic cells withbasophilic cytoplasm are almost always seen in bloodfilms ofATLL. Positive cytochemical markers includeacid phosphatase, f1 glucuronidase, and ANAE. Themembrane phenotype is summarised in table 4. Thecells are CD4+ and, unlike other T cell disorders,consistently express the receptor for Interleukin-2(CD25).There is a spectrum of clinical syndromes in
ATLL.52 The most common, acute ATLL, presentswith a high white cell count, hypercalcaemia, and thesurvival is less than one year. In the more chronicATLL the white cell count is lower, there are fewercirculating abnormal cells, and the survival is morethan one year. The bone marrow is often normal in
these cases. Finally, a group of patients have normalwhite cell counts and few non-specific symptoms, anda low proportion of abnormal T lymphocytes in theblood films. Evidence of clonality in such cases can beshown by molecular methods with appropriateHTLV-I probes. This condition has been designated as"smouldering" ATLL.52ATLL has a distinct epidemiology which relates to
the distribution of its causative agent, the human typeC retrovirus HTLV-I." The asociation of HTLV-Iwith ATLL has been shown by serological andmolecular studies. Almost all patients with ATLLhave a high titre of antibodies to HTLV-I, and DNAanalysis shows clonal integration of HTLV-I in theneoplastic ATLL cells. Most cases have been found insouth western Japan,'52 the Caribbean region, and inCaribbean immigrants who reside in other countries.-'
Sezary's syndromeThis disorder is characterised by generalisedexfoliative erythroderma and an epidermal infiltrate of
580
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemias
a<.99 3I
Fig 5 Electron photomicrograph ofan atypical lymphocytefrom a case ofATLL.
atypical mononuclear cells. The abnormal circulatingcells in such cases are known as Sezary cells. Sezary'ssyndrome was the first disorder shown to be ofT cellorigin." I In peripheral blood films there are two typesofSezary cell: large (fig 3h) and small (fig 3i). The largeSezary cells, with near tetraploid chromosome num-ber, are less common. They are larger than neutrophilsand sometimes also larger than monocytes. Thenucleus is large and occupies four fifths of the cell witha round or oval profile and densely clumpedchromatin. A grooved pattern is apparent and thiscorresponds to the cerebriform nuclear shape shownat ultrastructural level.42 Nucleoli are small and rarelyvisible. The cytoplasm shows a clear basophilia, has anarrow rim around the nucleus, and lacks azurophilgranules.The small cell variant of Sezary cell (also known as
the Lutzner cell) is more common." The cell is the sizeofa small lymphocyte (fig 3i) but has the same groovednuclear chromatin pattern as the large Sezary cell (fig3h). Lutzner cells, however, usually have a highernuclear:cytoplasmic ratio than small lymphocytes andsometimes show cytoplasmic vacuoles (periodic acidSchiff positive) around the nucleus. Electron micros-copical examination is useful for the morphologicalidentification of small and large Sezary cells (fig 6).Bone marrow aspirates are either normal or showminimal infiltration; obvious disease is seen when thewhite cell count is high. Skin biopsy sectiops show thetypical pattern of infiltration in the upper dermis with
epidermotropism and Pautrier microabscesses. Themembrane phenotype of Sezary cells is that of amature T lymphocyte with CD3+, CD4+, CD8-markers (table 5).
Discussion
In contrast to reliance on the cytomorphological andcytochemical features used in our previous proposalsfor the classification of acute leukaemia, other thanmegakaryoblastic leukaemia (M7)," we consider thata reproducible classification ofthe chronic B and T cellleukaemias required determination of the membranephenotype of the neoplastic cells as well as a descrip-tion of their morphological features. In both the B andT cell lineages several well defined disease entities cannow be recognised in which the peripheral blood(leukaemic phase) and the bone marrow are affected.Some of the entities described here are well known butour proposals have emphasised the subtle phenotypicand morphological differences which allow disorderswith specific clinical features, cell biology, and naturalhistory to be defined more precisely than in the past. Inaddition to the morphological analysis of blood andbone marrow aspirates, the value of bone marrow
trephine biopsies and, in the case ofNHL in leukaemicphase, of the histological assessment of lymph nodesor spleen, has been emphasised.Advances in treatment-for example, the specific
response to a-interferon in HCL and not in the HCL-
:..P,; .-;
581
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

582 Bennett, Catovsky, Daniel, et al
.:X;:stf z 4^ s~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.I
Fig 6 Cerebriform appearance ofa Sezary cell as seen by electron microscopy.
variant form (G Flandrin and D Catovsky, unpubli-shed observation)-clearly justify the identification ofthe latter as a special subtype. Similarly, differences inthe natural history and prognosis of CLL and PLLjustify the separate identification of these forms of Bcell lymphocytic leukaemia. Confusion with CLL andHCL often arises with some types of NHL in leuk-aemic phase. Again, the combined information ofmorphology and membrane phenotype helps in theidentification of follicular lymphoma presenting witha leukaemic blood picture, and of splenic B celllymphoma whose circulating cells are often confusedwith hairy cells.The recognition of distinct entities within the T cell
leukaemias has important epidemiological and patho-physiological connotations as illustrated by ATLL,the T cell leukaemia caused by HTLV-I and T-PLLwhere a specific chromosome abnormality, inv(14)(qi 1q32), is often found.7
In the acute leukaemias morphological andimmunological features and cytogenetics have been
integrated to improve diagnostic precision and theobjective classification of human haemopoietic malig-nancies.59 It is hoped that in the field of the chronic Band T cell leukaemias our proposals will serve as thebasis for further work, discussion, and improvedclinical practice.
We thank Dr ES Jaffe for the review of the histopath-ological material; DrM Imbert for helpful discussions;Drs JV Melo, E Matutes, and MS Pombo de Oliveirafor assistance in preparing blood, bone marrow slides,and electron micrographs of selective cases for review.
References
I Galton DAG, Goldman JM, Wiltshaw E, Catovsky D, Kenry K,Goldenberg GJ. Prolymphocytic leukaemia. Br J Haematol1974;27:7-23.
2 Catovsky D, Weschler A, Matutes E, et al. The membranephenotype of T-prolymphocytic leukaemia. Scand J Haematol1982;29:398-404.
3 Koduru PRK, Filippa DA, Richardson ME, et al. Cytogenetic and
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

Classification ofB and T cell leukaemias 583histologic correlations in malignant lymphoma. Blood 1987;69:97-102.
4 Croce CM, Nowell PC. Molecular basis ofhuman B cell neoplasia.Blood 1985;65:1-7.
5 Gahrton G, Robert K-H, Friberg K, Zech L, Bird AG. Non-random chromosomal aberrations in chronic lymphocyticleukaemia revealed by polyclonal B-cell-mitogen stimulation.Blood 1980;56:640-7.
6 Brito-Babapulle V, Pittman S, Melo JV, Pomfret M, Catovsky D.Cytogenetic studies on prolymphocytic leukaemia. I. B-cellprolymphocytic leukaemia. Hematol Pathol 1987;1:27-33.
7 Brito-Babapulle V, Pomfret M, Matutes E, Catovsky D. Cytogen-etic studies on prolymphocytic leukaemia. II. T-cell prolym-phocytic leukaemia. Blood 1987;70:926-31.
8 Catovsky D, Melo JV, Matutes E. Biological markers in lym-phoproliferative disorders. In: Bloomfield CD, ed. Chronic andacute leukaemias in adults. The Hague: Martinus NijhoffPublishers, 1985:69-112.
9 Anderson KC, Bates MP, Slaughenhoupt BL, Pinkus GS,Schlossman SF, Nadler LM. Expression of human B cell-associated antigens in leukaemias and lymphomas: a model ofhuman b cell differentiation. Blood 1984;63:1424-33.
10 Natham PD, Walker L, Hardie D, et al. An antigenic study ofhuman plasma cells in normal tissue and in myeloma identifica-tion ofa novel plasma cell associated antigen. Clin Exp Immunol1986;65:1 12-9.
1 1 Posnett DN, Wang C-Y, Chiorazzi N, Crow MK, Kunkel HG. Anantigen characteristic of hairy cell leukaemia cells expressed oncertain activated B cells. J Immunol 1984;133:163540.
12 Schwarting R, Stein H, Want CY. The monoclonal antibodies S-HCL 1 (leu-14) and S-HCL 3 (leu-M5) allow the diagnosis ofhairy cell leukaemia. Blood 1985,65:974-83.
13 Melo JV, Catovsky D, Galton DAG. The relationship betweenchronic lymphocytic leukaemia and prolymphocytic leukaemia.I. Clinical and laboratory features of300 patients and character-isation of an intermediate group. Br J Haematol 1986;63:377-87.
14 Scott CS, Limbert HJ, Roberts BE, Stark AN. Prolymphocytoidvariants of chronic lymphocytic leukaemia: an immunologicaland morphological survey. Leuk Res 1987;11:135-40.
15 Melo JV, Brito-Babapulle V, Oliveira MSP, Galton DAG,Catovsky D. The relationship between chronic lymphocyticleukaemia and prolymphocytic leukaemia. In: Gale RP, Rai K,eds. Chronic lymphocytic leukaemia. Recent progress andfuture direction. New York: Alan R Liss Inc, 1987:205-14.
16 Minden MD, Mak TW. The structure of the T-cell antigenreceptor genes in normal and malignant T cells. Blood 1986;68:327-36.
17 Rozman C, Montserrat E, Rodriguez-Fernandez JM, et al. Bonemarrow histologic pattern. The best single prognosticparameter in chronic lymphocytic leukaemia: a multivariatesurvival analysis of 329 cases. Blood 1984;64:642-8.
18 Pangalis GA, Roussou PA, Kittas C, Kokkinou S, Fessas P. B-chronic lymphocytic leukaemia. Prognostic implication of bonemarrow histology in 120 patients experience from a singlehematology unit. Cancer 1987;69:767-71.
19 Melo JV, Catovsky D, Gregory WM, Galton DAG. The relation-ship between chronic lymphocytic leukaemia and prolym-phocytic leukaemia. IV. Analysis of survival and prognosticfeatures. Br J Haematol 1987;65:23-9.
20 Vallespi T, Torrabadella M, Julia A, et al. Chronic lymphocyticleukaemia: a multivariate survival analysis including mor-phological types of lymphoid cells in peripheral blood. In: GaleRP, Rai KR, eds. Chronic lymphocytic leukaemia. Recentprogress andfuture direction. New York: Alan R Liss Inc, 1987:277-88.
21 Melo JV, Wardle J, Chetty M, et al. The relationship betweenchronic lymphocytic leukaemia and prolymphocytic leukaemia.III. Evaluation of cell size by morphology and volumemeasurements. Br J Haematol 1986;64:469-78.
22 Enno A, Catovsky D, O'Brien M, et al. "Prolymphocytoid"transformation of chronic lymphocytic leukaemia. Br JHaematol 1979;41:9-18.
23 Owens MR, Strauchen JA, Rowe JM, Bennett JM. Prolym-phocytic leukaemia: histologic findings in atypical cases.Hematol Oncol 1984;2:249-57.
24 Lampert I, Catovsky D, Marsh GW, Child JA, Galton DAG. Thehistopathology of prolymphocytic leukaemia with particularreference to the spleen: a comparison with chronic lymphocyticleukaemia. Histopathology 1980;4:3-19.
25 Bouroncle BA. Leukemic reticuloendotheliosis (hairy cell leuk-aemia). Blood 1979;53:412-36.
26 Yam LT, Janckila AJ, Li C-Y, Lam WKW. Cytochemistry oftartrate-resistant acid phosphatase: 15 years' experience. Leuk-aemia 1987;1:285-8.
27 Cawley JC, Burns GF, Hayhoe RGH. A chronic lym-phoproliferative disorder with distinctive features: a distinctvariant of hairy-cell leukemia. Leuk Res 1980;4:547-59.
28 Catovsky D, O'Brien M, Melo JV, Wardle J, Brozovic M. Hairycell leukaemia (HCL) variant: an intermediate disease betweenHCL and B-prolymphocytic leukaemia. Semin Oncol 1984;11:362-9.
29 Melo JV, Hegde U, Parreira A, Thompson I, Lampert IA,Catovsky D. Splenic B cell lymphoma with circulating villouslymphocytes: differential diagnosis of B cell leukaemias withlarge spleens. J Clin Pathol 1987;40:642-51.
30 Neiman RS, Sullivan AL, Jaffe R. Malignant lymphoma simulat-ing leukaemic reticuloendotheliosis. A clinicopathologic studyof ten cases. Cancer 1979;43:329-42.
31 Isaacs R. Lymphosarcoma cell leukaemia. Ann Intern Med 1937;11:657-62.
32 Spiro S, Galton DAG, Wiltshaw E, Lohmann RC. Follicularlymphoma: a survey of 75 cases with special reference to thesyndrome resembling chronic lymphocytic leukaemia. Br JCancer 1975;31 (Suppl II):60-72.
33 Come SE, Jaffe ES, Anderson JC, Mann RB, et al. Non Hodgkin'slymphomas in leukemic phase: clinicopathologic correlations.Am J Med 1980;69:667-74.
34 Melo JV, Robinson DSF, de Oliveira MP, et al. Morphology andimmunology of circulating cells in leukaemic phase of follicularlymphoma. J Clin Pathol 1988;41:951-9.
35 Bennett JM, Cain KC, Glick JH, Johnson GT, et al. Thesignificance of bone marrow involvement in non Hodgkin'slymphomas: The Eastern Cooperative Oncology Experience.J Clin Oncol 1986;4:1462-9.
36 Swerdlow SH, Habeshaw JA, Murray LJ, Dhaliwal HS, et al.Centrocytic lymphoma: a distinct clinicopathologic andimmunologic entity. A multiparameter study of 18 cases atdiagnosis and relapse. Am J Pathol 1983;113:181-97.
37 Jaffe S, Bookman MA, Longo DL. Lymphocytic lymphoma ofintermediate differentiation. Mantle zone lymphoma: a distinctsubtype of B-cell lymphoma. Hun Pathol 1987;18:877-80.
38 Weisenburger DD, Sanger WG, Armitage JO, Purtilo DT.Intermediate lymphocytic lymphoma: immunophenotypic andcytogenetic findings. Blood 1987;69:1617-21.
39 Harris NL, Nadler LM, Bhan AK. Immunohistologic character-isation of two malignant lymphomas of germinal center type(centroblastic/centrocytic and centrocytic) with monoclonalantibodies. Am J Pathol 1984;117:262-72.
40 Kyle RA, Maldonado JE, Bayrd ED. Plasma cell leukemia: reporton 17 cases. Arch Intern Med 1974;133:813-18.
41 Parreira A, Robinson DSF, Melo JV, et al. Primary plasma cellleukaemia: immunological and ultrastructural studies in 6 cases.Scand J Haematol 1985;35:570-8.
42 Matutes E, Garcia Talavera J, O'Brien M, Catovsky D. Themorphological spectrum of T-prolymphocytic leukaemia. Br JHaematol 1986;64: 111-24.
43 BrouetJC, FlandrinG, Sasportes M, Preud'hommeJL, SeligmannM. Chronic lymphatic leukaemia ofT cell origin. Lancet 1975;ii:890-3.
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from

584 Bennett, Catovsky, Daniel, et al44 Newland AC, Catovsky D, Linch D, et al. Chronic T cell
lymphocytosis: a review of 21 cases. Br J Haematol 1984;58:433-46.
45 Louhran TP Jr, Kadin ME, Starkebaum G, et al. Leukemia oflarge granular lymphocytes: association with clonalchromosomal abnormalities and autoimmune neutropenia,thrombocytopenia and hemolytic anemia. Ann Intern Med1985;102:169-75.
46 Crockard AD, Chalmers D, Matutes E, Catovsky D. Cytochemis-try of acid hydrolases in chronic B and T cell leukaemias. Am JClin Pathol 1982;78:437-44.
47 Costello C, Catovsky D, O'Brien M, Morilla R, Varadi S. ChronicT-cell leukaemias. I. Morphology, cytochemistry and ultra-structure. Leuk Res 1980;4:463-76.
48 Hernandez Nieto L, Lampert IA, Catovsky D. Bone marrowhistological patterns in B and T prolymphocytic leukaemia.Hematol Pathol 1989;3 (in press).
49 Yodoi J, Takatsuki K, Masuda T. Two cases of T cell chroniclymphocytic leukemia in Japan. N EnglJ Med 1974;290:572-3.
50 Uchiyama T, Yodoi J, Sagawa K, Takatsuki K, Uchino H. AdultT-cell leukemia: clinical and hematologic features of 16 cases.Blood 1977;50:481-92.
51 Kinoshita K, Kamihira S, Ikeda S, et al. Clinical, hematologic andpathologic features of leukemic T-cell lymphoma. Cancer1982;50:1554-62.
52 Abrams MB, Sidawy M, Novich M. Smoldering HTLV-associated T-cell leukemia. Arch Intern Med 1985;145:2257-8.
53 Poiesz BJ, Rusctti FW, Gazdar AF, et al. Detection and isolationof type C retrovirus particles from fresh and cultured lym-phocytes of a patient with cutaneous T-cell lymphoma. ProcNatl Acad Sci USA 1980;77:7415-19.
54 BlattnerWA, Blayney DW, Robert-GuroffM, et al. Epidemiologyof human T-cell leukemia/lymphoma virus. J Infect Dis1983;147:406-16.
55 Brouet J-C, Flandrin G, Seligmann M. Indications of the thymus-derived nature of the proliferating cells in six patients withSezary's syndrome. N EnglJ Med 1973;289:341-4.
56 Flandrin G, Brouet J-C. The Sezary cell: cytologic, cytochemicaland immunologic studies. Mayo Clin Proc 1974;49:575-83.
57 Lutzner MA, Emerit I, Durepaire R, Flandrin G, Grupper CH,Prunieras M. Cytogenetic, cytophotometric and ultrastructuralstudy of large cerebriforn cells of the Sezary syndrome anddescription of a small-cell variant. JNCI 1973;50:1145-62.
58 Bennett JM, Catovsky D, Daniel MT, et al. Criteria for thediagnosis ofacute leukaemia ofmegakaryocyte lineage. Ann IntMed 1985;103:460-2.
59 First MIC Cooperative Study Group. Morphologic, immunologicand cytogenetic (MIC) working classification of acute lym-phoblastic leukemias. Cancer Genet Cytogenet 1986;23:189-97.
Requests for reprints to: Professor D Catovsky, AcademicDepartment of Haematology and Cytogenetics, The RoyalMarsden Hospital, Fulham Road, London SW3 6JJ,England.
copyright. on N
ovember 6, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.42.6.567 on 1 June 1989. Dow
nloaded from