Embed Size (px)
Citation preview

JournalofHepatology, 1988; 7:175-185 175 Elsevier
HEP 00440
Propranolol or endoscopic sclerotherapy in the prevention of recurrence of variceal bleeding
A prospective, randomized controlled trial*
Paula T. Alexandrino, M. Martins Alves and J. Pinto Correia Department of Medicine 2, Center of Gastroenterology (INIC), University Hospital of Santa Maria, Lisbon (Portugal)
'Received 30 December 1987) (Accepted 26 April 1988)
Summary
Endoscopic sc lerotherapy (ES) and continuous propranolol (P) t rea tment have both been proposed as useful
methods to prevent recurrent esophageal variceal bleeding. We report a prospective randomized trial in 65 pa-
tients with a previous history of endoscopical ly proven esophageal variceal bleeding_ Patients were randomized
by sealed envelopes stratified for Child 's A and B groups to receive either endoscopic sclerotherapy (n = 31) or
propranolo l (n = 34). The dose of oral propranolol was based on a reduction of the resting pulse rate by 25%. In-
t ravascular e thanolamine oleate was used for the endoscopic sclerotherapy in a 3-week schedule. The follow-up
per iod ranged from 17 to 57 months (median: ES = 31; P = 28 months). There was no difference in the cumula-
tive percentages of patients free of rebleeding from any source: esophageal and gastric varices, acute esophageal
and gastric ulcers or erosions (ES = 37%; P = 16%). Also, there was no difference in the cumulative survival (ES
= 69% ; P = 54%). However , patients in the propranolol group had significanily more variceal rebleeding from
the esophagus (n = 21) than did those in the sclerotherapy group (n = 9). The cumulative percentages of patients
free of esophageal variceal rebleeding after inclusion were 67% in the endoscopic sc lerotherapy group and 25%
in the propranolo l group ( log-rank test, P < 0.02). These differences indicated that sclerotherapy should be used
in 29% of the propranolol patients who rebled. Based on these results we recommend elective sc lerotherapy as
long-term therapy for preventing rebleeding of esophageal varices.
Introduction
Recurrent variceal bleeding is one of the main
causes of morbidi ty and poor quality of life in cirrhot-
ics; it is also responsible for their high mortal i ty [1].
Disappoint ing results were obta ined in trials compar-
* Part of the results were presented at the EASL and AASLD Meetings in 1986. Correspondence: Prof. J. Pinto Correia, Dept. Med. 2, Hospital Santa Maria, 1699 Lisbon Codex, Portugal.
0168-8278/88/$03.50(~) 1988 Elsevier Science Publishers B.V. (Biomedical Division)

176 P.T. ALEXANDRINO et al.
ing non-selective portal-systemic shunts with routine
medical therapy [2-4].
Lebrec et al. [5] demons t ra ted a significant reduc-
tion of recurrent variceal and non-variceal bleeding
and an increased survival in selected well-compen-
sated cirrhotic patients t reated with propranolol .
However , three subsequent studies in a less selected
populat ion [6-8] failed to confirm these results. On
the other hand, a few control led studies [9-11] re-
ported a beneficial effect of endoscopic sclerothera-
py in reducing the number of episodes of variceal re-
bleeding, and one of them claimed the addit ional
benefit of long-term survival [10].
Thus, in recent times, the most commonly used
non-surgical t rea tment al ternatives for prevention of
recurrent variceal bleeding are ei ther endoscopic
sclerotherapy or the long-term administrat ion of oral
propranolol . We designed a prospect ive randomized
trial to compare the short- and long-term results of
both therapies in patients with portal hypertension
who had bled from esophageal varices.
were a l ready in a sc lerotherapy group program, and
35 did not meet the above-ment ioned inclusion crite-
ria. Ano the r 27 were lost to immedia te follow-up_
The remaining 48 (17%) plus 17 referred from other
hospitals (meet ing the same selection criteria) in a to- tal of 65 were randomly al located ei ther to sclero-
therapy (n = 31) or to propranolol (17 = 34).
The characteristics of the two groups randomized
are summarized in Table 1_ There were no significant
differences in age and sex distr ibution, cause of por-
tal hyper tension (confirmed histologically in 61 of 65
pat ients) , previous episodes of bleeding or severi ty of
liver damage graded on randomizat ion by Camp-
bell 's modificat ion of the Chi ld-Turcot te classifica-
tion [12].
Study design Patients with clinically significant bleeding (hema-
temesis and/or melena requiring blood transfusion or
with a fall in hemoglobin of 3 g/dl or greater) under-
went emergency endoscopy.
Materials and Methods
Patients The study populat ion comprised 65 patients with
portal hypertension with at least one episode of
esophageal variceal bleeding. Cri ter ia for selection
to this study were: (a) recent episode of bleeding
from esophageal varices confirmed by emergency en-
doscopy (patients with suspicion of hemorrhage from
gastric erosions or o ther gastric or duodenal patholo-
gy were not included); (b) Child 's A and B groups;
(c) no contraindicat ions to the use of fl-blocking
agents, such as asthma or airway obstruct ion, left
ventricular failure, d iabetes mellitus type I; (d) no
previous sclerotherapy; (e) acceptance by the pa-
tients and/or his doctor to be included in the trial.
During a 3.5-year period, 277 patients with rup-
tured esophageal varices were admit ted to the
Gastroenterological Intensive Care Unit of our Hos-
pital_ Eighty-six died during the hospital admission
and 116 were excluded from randomizat ion: 81 were
submit ted to urgent endoscopic sc lerotherapy or
TABLE 1
CHARACTERISTICS OF THE TWO GROUPS AT ENTRY
Sclerolherapy Propranolol (n = 31) ( . = 34)
Age (yr. mean + S.D.) 44.9 + 11.3 49.9 + 11).9 Sex (M/F) 24/7 28/9 Diagnosis
alcoholic cirrhosis 26 26 non-alcoholic cirrhosis 2 6 nodular rcgcnerative hyperplasia I I
idiopathic portal thrombosis 2 1 Child's classification
Group A 23 24 Group B 8 10
No. o f previous b]eedings mean + S.D. 2.6 + 1.5 2.9 + 1.8 No. of patients 22 28
Transfusions (units) during the index bleeding episode (mean + S.D.) 2.8 + 2.4 3.8 _+ 2.8
Cardiac index" 5.(1 + 1.4 5.0 _+ 1.4 Portal pressure
(WHVP-FHVP)" 17.9 + 6.5 18.2 + 5 1 (n = 19) (n = 22)
Only in a subset of patients with liver cirrhosis.

PREVENTION OF VARICEAL REBLEEDING 177
Esophageal varices were considered the source of
bleeding when one of the following criteria was ob-
served: active bleeding from varices; signs of recent bleeding (clot or fibrin plug); no signs of recent
bleeding but no other potential source of bleeding. The hemorrhage was controlled by intravenous infu-
sion of vasopressin and/or Sengstaken-Blakemore balloon tamponade. Child's classification was estab-
lished at least 15 days after the end of the index bleeding episode, when the patients were hemodyna-
mically stable_ At that time, patients were classified
according to a numerical score: Child's A, 5 - 8 points; Child's B, 9-11 points [12]. Randomization
was done by a list of random numbers allocated to sealed envelopes in two separate groups for Child's A
and B patients: even numbers, sclerotherapy (n =
31); odd numbers, propranolol (n = 34). The mean interval between the end of bleeding and randomiza-
tion was 17.9 + 9.7 (mean + S.D.) days in the sclero- therapy group and 19.7 + 8.8 days in the propranolol
group.
After randomization, cardiac output and hepatic and systemic hemodynamic parameters were mea-
sured by a transjugular approach before starting
therapy, in 19 of 28 (68%) patients with cirrhosis in the sclerotherapy group and in 22 of 32 (69%) pa-
tients with cirrhosis in the propranolol group (Table 1). These studies were repeated after treatment in
some patients in both groups, and the results have
been published in part [13]. Sclerotherapy was carried out with intravascular
injection of 5% ethanolamine oleate through a later-
al-view Olympus endoscope (GIF-K 2 or Kl0 ) and NM-IK needle injector (Olympus)_ The procedure was performed under diazepam sedation, with a 'free-hand' technique, every 3 weeks, until the
esophageal varices had been obliterated at the
gastro-esophageal junction or were too small to re- ceive further injections. Endoscopic follow-up was performed every 3 months in the first year, and every
6 months after, and varices were reinjected if they re- curred, at similar intervals to the initial injections.
Propranolol was given orally, twice a day, in in- creasing doses, until the resting pulse rate was re- duced by 25%. Patients were seen every week for 1
month and then at intervals of 3 months and the dos-
age of propranolol was adjusted, if necessary, to maintain a reduction in resting pulse of approximate-
ly 25%. This expected response to the drug was used
as a measure of compliance which was also assessed by the discrepancy between the number of tablets is-
sued to the patients and patients' requests for further
supplies. All patients had a clinical and laboratory follow-up
and were systematically asked about drinking habits.
All potential adverse side-effects were looked for
and registered. All clinical rebleeding episodes (hematemesis or
melena after a 24 h free interval) requiring blood transfusion or with a fall in hemoglobin of 3 g/dl or greater were treated in our GE Intensive Care Unit,
and endoscopically assessed to confirm the cause of
bleeding. In a case of no active bleeding from esoph-
ageal varices but where gastric varices or acute gas- tric or duodenal erosions were bleeding at the time of
endoscopy, the cause of rebleeding was ascribed to these associated lesions. Otherwise, the source of
bleeding was considered' unknown_ In the sclerothe- rapy group, esophageal variceal rebleeding was
treated with standard medical treatment and urgent
sclerotherapy, avoiding balloon tamponade when possible. In the propranolol group patients were treated with standard medical treatment and with ur-
gent sclerotherapy when they met the following crite- ria: either one single episode with shock or requiring
4 units of blood trarrsfusions or with a fall in hemoglo-
bin below 8 g/dl; or in any case after the second epi- sode of rebleeding. Patients who required urgent
sclerotherapy underwent further elective injections. Two patients were submitted to surgery after failure
of both therapies.
Statistical analysis This was performed on the basis of an 'intention to
treat' principle, so including in each group all clinical- ly evident rebleeding episodes and deaths after ran-
domization, irrespective of compliance and regular attendance. The data of 11 patients assigned to pro- pranolol, 10 of whom required emergency sclerothe-
rapy and 1 of whom had surgery, were analysed with

178 P.T. ALEXANDRINO et al.
the. data of the propranolol group. The data of one
patient assigned to the sclerotherapy group who was submitted to surgery was analysed with the data of
the sclerotherapy group. Two patients in the propra-
nolol group stopped taking the drug because of side-
effects and another two were lost to follow-up. They were censored at the time of stopping the drug or
when lost to follow-up. No patients in the sclerothe-
rapy group withdrew or were lost to follow-up. The percentages of patients free of rebleeding and
of patients surviving during the period after inclusion were calculated according to the Kaplan-Meier
method and were compared by means of a log-rank
test [14]. Results of continuous variables were ana-
lysed using Student's t test for paired or unpaired data, as indicated. The ~ test was used when analy-
sing discrete variables. Differences in P values less
than 0.05 were considered significant.
Results
The 65 patients were followed for between 17 and 57 months. Mean duration of follow-up (until pa-
tients were last seen, lost, withdrawn or dead) was
similar in both groups (sclerotherapy group 30.7 +
17.5; propranolol group 28.2 + 14.9 months). Of the 31 patients treated by sclerotherapy, vari-
ceal obliteration was achieved in 27 (87%) with a
mean of 4.5 + 1.5 courses in 3.7 + 2.8 months. The
remaining 4 patients died prior to this_ Of the 27 pa- tients with obliterated varices, 3 died without further
recurrence of varices. In 8 of the 24 (33%) patients
alive no further recurrence of varices was observed
over a median follow-up period of 35.9 + 15.5 months (range, 12-55 months). In 16 (66%), new
varices were observed, in 9 after a short interval (3-6
months) and in 7 after a long interval (12-30
months). A median of 1.8 + 1.6 further sclerothera- py courses were required for reobliteration, although
in 5 of the 16 patients further varices developed again after a median interval of 11.4 months (ranged from 6
to 24 months). A 25% decrease from base-line pulse rate was ob-
tained in 32 out of 34 patients in the propranolol
group (after 1.3 + 0.2 months) and was maintained
throughout the trial period with an average dosage of 130 + 65 mg daily (range 40- 360 mg daily). Mean
systolic blood pressure fell significantly from 124.0 +
12.9 mmHg to 105_3 + 13.2 mmHg. Failure to abstain from alcohol was observed in 11
of the 26 (42%) patients in the sclerotherapy group and in 9 of 26 (35%) patients in the propranolol
group. Alcoholic consumption was not significantly
different in patients who rebled or died in both
groups.
Rebleeding Rebleeding from esophageal varices was observed
in 9 of 31 (29%) patients in the sclerotherapy group
and in 21 of 34 (62%) in the propranolol group (Table
2). The percentages of patients free of rebleeding
from esophageal varices at 1, 2, 3 and 4 years after in-
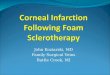
clusion were 77%, 73%, 67% and 67%, respectively, in the sclerotherapy group and 62%, 42%, 38% and
25%, respectively, in the propranolol group (Fig. 1). The overall differences between the two groups were
significant (~ = 5.746, P < 0_02), as well the differ- ences at 2, 3 and 4 years.
In the sclerotherapy group 7 patients had rebleed-
ing from esophageal varices within the first 6 months,
all before complete variceal obliteration. The two other patients had variceal rebleeding after 10 and
30 months following initial obliteration. In one, new
varices were not detected because he failed to attend
TABLE 2
FREQUENCY OF THE FIRST REBLEEDING EPISODE, ACCORDING TO CAUSES (NO. OF PATIENTS)
Sclerotherapy Propranolol (n = 31) (n = 34)
Esophageal varices 9 21 a'b
Gastric varices 2 ~ 0 Gastric erosions 5 2 Esophageal ulcer 1 0 Unknown 0 2
Total 17 25
One patient in each group underwent surgery because of un-- controlled bleeding.
b Ten patients changed to sclerotherapy.

PREVENTION OF VARICEAL REBLEEDING 179
96
100 -
80.
6 0 -
40
20
L,
t I
N
k
i
I
4.
t
t - - - 3
h I
q . . . . - I~ L I - - - ~ I
1 Dead
* Lost to fo l low-up
"~ Withdrawn
• Surgery
' ' ' 1 +, ,,
. . . . 4 . 1 - - - - - 4 . . . . . . . - r l - . . . . . + l - . n
I i
I I I I
i
k . . . . . . . . i
ES J I I I
p<O,02
P P- . . . . " 4
years
P - 34 20 11 6 2
ES - 31 21 16 11 4
Fig. 1. Percentage of patients free of rebleeding from esophageal varices vs. time after randomization. ES = sclerotherapy (solid line); P = propranolol (hatched line). The short vertical bars represent trial times for patients free of rebleeding when last seen, lost to fol- low-up, withdrawn, submitted to surgery or dead. The numbers below the abscissa denote the number of patients at risk during the ob-
servation period in each group. The solid and hatched vertical bars represent the 95% confidence level (= 2 S_E.).
for follow-up endoscopies. In contrast, rebleeding in
the propranolol group was observed throughout the
42-month follow-up period. Two non-compliant pa-
tients were alcoholic and had early variceal rebleed-
ing complicated by death.
The 9 patients in the sclerotherapy group who had
variceal bleeding had a total of 15 episodes with a
mean of 0.06 rebleeding episodes per patient per
month of follow-up, and the 21 patients in the propra-
nolol group had a total of 39 episodes with a mean of
0.15 rebleeding episodes per patient per month of
follow-up. There was a significant difference be-
tween both the number of episodes of bleeding (P <
0.03) and the mean values per month (P < 0.05).
Mean blood transfusion requirements for each epi-
sode of rebleeding were similar for the two groups
(3.5 + 2.4 and 3.1 + 3.5 units, sclerotherapy and pro-
pranolol, respectively; Table 3).
TABLE 3
ANALYSIS OF THE REBLEEDING EPISODES
Sclerotherapy Propranolol (n = 31) (n = 34)
Mean follow-up (months) 30.7 + 17.5 28.2 __. 14.9
Rebleeding rate esophageal varices 33%* 75%* all sources 63% ~ 84% ~
No. of episodes of rebleeding esophageal varices 15"* 39** all sources 46 ~ 76 ~
Mean episodes/patient/month esophageal varices 0.06*** 0.15"** all sources 0.17 ~ 0.188
*P < 0.02.
**P < 0.03.
***P < 0.05
§ r l . s .

180 P.T. ALEXANDRINO et al.
Because of severe or repeated bleeding, 10 pa-
tients in the propranolol group received urgent and
elective sclerotherapy. In 8 patients variceal obliter- ation was achieved: 2 died after 12 and 19 months due
to rebleeding from 'new' varices and hepatic failure; in the 6 patients surviving the mean follow-up was 27
months from the time of initial sclerotherapy to the fi-
nal analysis of the trial_ In 2 patients obliteration was
not achieved: one of these died from variceal bleed- ing after three sessions of sclerotherapy and one was
submitted to surgery because of uncontrolled bleed-
ing. Two patients in the sclerotherapy group rebled
from gastric varices but none in the propranolol
group. In one of them, a severe rebleeding occurred
after complete obliteration of esophageal varices and
the patient was submitted to surgery. The percent-
ages of patients free of both esophageal and gastric variceal rebleeding in the sclerotherapy group at 1, 2,
3 and 4 years after inclusion were 74%, 66%, 61%
and 61%, respectively (Fig. 2). The overall differ- ences between the two groups were again significant
(X 2 = 3.863, P < 0.05). In the two figures, the curves of the sclerotherapy groups show a marked change at
6 months after entry, corresponding to the time when
complete esophageal variceal obliteration was achieved.
Gastric erosions were the origin of rebleeding in 5
patients (with seven episodes) with obliterated
esophageal varices in the sclerotherapy group and in
two fl-blockaded patients (with four episodes) in the propranolol group (Table 2). Half of the patients in
each group had heavy alcoholic consumption. In one
patient an esophageal ulcer causing three severe epi-
sodes of bleeding was observed 2 days after the initial sclerotherapy course and was complicated by an epi-
gastric peritonitis (see side-effects).
Analysing all sources of rebleeding (Table 2), 17 of
%
1 0 0 -
8 0 -
6 0 -
4 0
2 0 ¸
-f
i1 t l L - - - ~
L - - -
-f JJ JI
I .% L . . - 1
% H . . . . -I-i
L 4 - - - 1
1" Dead
Lost to f o l l ow-up
A W i t hd rawn
I I I ] t II
L _ ~
. . . . . ~x_ _ _ _ I - . . . . . . . . ! . . . . . . . I - I - - 1
i i ' ,, '
i .L
I I JI I I
P < 0 , 0 5 ',
i i i i , P
~. . . . . . . . ' t 4 . . . . . --t i I i I I
J .
ES l i
I I I I 1 2 3 4
y e a r s
P - 3 4 2 0 11 6 2
ES - 31 2 1 16 11 4
Fig. 2. Percentage of patients free of rebleeding from esophageal and gastric varices vs. time from randomization. ES = sclerotherapy (solid line); P = propranolol (hatched line). The short vertical bars represent trial times for patients free of rebleeding when last seen,
lost to follow-up, withdrawn or dead. The solid and hatched vertical bars represent the 95% confidence level (= 2 S.E.).

PREVENTION OF VARICEAL REBLEEDING 181
31 (54.8%) patients in the sclerotherapy group rebled, compared with 25 of 34 (73.6%) patients in the propranolol group. The percentages of patients free of rebleeding from any source at 1, 2, 3 and 4 years after inclusion were 60%, 43%, 37% and 37%, respectively, in the sclerotherapy group and 53%, 33%, 16% and 16%, respectively, in the propranolol group (Fig. 3). Although the curves show a distinct separation after 6 months, the difference between them was not significant ( ~ = 1.29, P < 0.21). In the sclerotherapy group a total of 46 episodes of rebleed- ing were observed in 17 patients (0.17 episodes per patient per month), whilst in the propranolol group there were 76 episodes in 25 patients (0.18 episodes per patient per month). This difference was not sig- nificant. The total and mean blood transfusion re- quirements for each episode of rebleeding were simi- lar for the two groups (1284 and 1485 units; 2.9 + 2.5 and 3.0 +_ 3.0 units for sclerotherapy and proprano- Iol, respectively).
Survival
In the sclerotherapy group 9 patients died: 4 died of liver failure (3 without further rebleeding 4.0, 5.5
and 20.0 months after inclusion; and one who had bled from gastric erosions, 36 months after entry); 4 died of complications related to a rebleeding episode 2.0, 2.5, 3.0 and 7.5 months after inclusion; and one died from uncontrolled hemorrhage 10 months after inclusion.
In the propranolol group 11 patients died after in- clusion: 2 of neoplasia (hepatocellular carcinoma and metastatic colon cancer) at 33 and 25 months; one of hepatic failure at 45.4 months; 3 from uncontrolled rebleeding at 6, 8 and 10 months; 5 from complica- tions related to rebleeding at 3.6, 4, 7, 12 and 22.3 months (Table 4).
The percentages of patients surviving at 1, 2, 3 and 4 years after inclusion were 77%, 74%, 69% and 69%, respectively, in the sclerotherapy group and 85%, 78%, 65% and 54%, respectively, in the pro-
%
1 0 0 -
8 0
6 0
4 0
2 0 -
L 1
L 1
L._.< 1. !l
.... t I " JL
i L
i
-]- D e a d
"A- L o s t t o f o l l o w - u p
, , ']
P 34
ES 31
. . . . I- . . . . i- l i i . . . . . . . . .
I I
i i i L . . . . . . .
i i
ES I I I I
NS
P I - . . . . -'1
Fig. 3. Percentage of patients free of rebleeding from any source vs. time after randomization. ES = sclerotherapy (solid line); P = propranolol (hatched line). No significant difference was found.
I I 2 3 4
years
17 9 4 2
17 10 6 5

182 P.T. A L E X A N D R I N O et al.
TABLE 4
MORTALITY TABLE, WITH CAUSES OF D E A T H IN B O T H G R O U P S
Sclerotherapy Propranolol (n = 31) (n = 34)
Total deaths 9 11 Group A (23/24) 6 6 Group B (8/10) 3 5
Causes of death bleeding 1 3" complications related to
bleeding 4 5 ~ hepatic failure 4 1 ~ others 0 2
" In each group, 1 patient after changing to sclerotherapy.
pranolol group (Fig. 4). These differences were not significant at any time. When differences in survival
were analysed according to Child's classification,
there was no statistically significant difference.
Side-effects In the propranolol group 2 patients stopped taking
the drug, because of bronchospasm and hepatic en-
cephalopathy in one, and left ventricular failure in the other. There was no rebleeding upon cessation or
subsequently. Both died, one from hepatic failure and the other from bladder cancer.
Side-effects occurred early in the course of treat-
ment: 3 patients had transient hepatic encepha- lopathy, 2 developed ascites, and 10 had dizziness
and fatigue. Two male patients experienced reduced sexual activity. Transient bronchospasm was ob-
served in 7 patients. No notable deterioration was
observed in routine liver function tests and serum electrolytes. Urea and creatinine did not change sig-
nificantly from base-line values at 1 or 2 years after inclusion.
In the sclerotherapy group ulceration was the most
frequent complication, occurring in 8 patients (5
%
lOO - ~ - - , ~, - - ~ , ~ * t
. . . . . . . H I - q - - I" ~" I
8 0 - I III I
60 l
4 0 -
Lost to f o l l o w - u p 20-
z~ Wi thdrawn
t F o l l o w - u p a f te r su rge ry
L I - - - I ~ i
I - - . - , } - - , , ~ I I I I t l I I I I I I • " , • i
L. . . . . . F - -~ - . . . . H - f - - - h . . . . NS
:" p i L - - - J - q - I ' - . . . . I-"~
F o l l o w - u p a f te r s c l e r o t h e r a p y
I I I I
1 2 3 4 years
P - 3 4 2 8 2 0 12 4
ES 31 2 4 2 0 14 4
Fig. 4. Cumulative survival curves for patients randomly assigned to sclerotherapy (ES) or propranolol (P). The short vertical bars represent trial times for patients when last seen (after surgery or after sclerotherapy in propranolol patients), lost to follow-up, or with-
drawn. No significant difference was found.

PREVENTION OF VARICEAL REBLEEDING 183
were asymptomatic, in 2 ulceration was confirmed endoscopically to be the site of rebleeding, following rebleeding from esophageal varices, and in 1 the bleeding ulcer was complicated by localised peritoni-
tis; this resolved with conservative management). Transient fever (/>38 °C) developed in 7 patients; cultures of blood and urine were sterile and the chest X-ray was normal. Seven patients had transient chest pain; 5 had pleural effusions, which were transient and asymptomatic in 4 but required medical therapy in one. Three patients had transient dysphagia due to narrowing of the esophageal lumen, diagnosed by re- sistance to passage of the endoscope. In two patients a prolonged hemorrhage after needle injection ne- cessitated blood transfusion. One patient developed aspiration pneumonia after emergency sclerothera- py. There were no fatal side-effects in any of the
groups.
Discussion
The present trial shows that long-term oral propra- nolol is less effective in reducing the frequency of variceal rebleeding as compared to repeated sclero- therapy. However, the frequency of rebleeding, whatever the sourcc, is the same with either propra- nolol or sclerotherapy. There was no difference in
survival over a 4-year period. Similar results have been observed in a trial recent-
ly published by Fleig et al. [15]. In this trial the re-
bleeding rate in both groups was much lower, around 30%, but the follow-up time was approximately only
half as long as in our study. The majority of our propranolol-treated patients
(60%) had variceal rebleeding distributed through- out the period of follow-up. This is similar to the re- suits in propranolol-treated patients of three recent randomized controlled trials reported by Burroughs et al. [6] in London, Villeneuve [7] in Montreal or Queuniet [8] in Rouen. Our results differ from those reported by Lebrec et al. [5] in Paris, despite the pa- tients' characteristics being very similar: 80% were alcoholic cirr~,otics in a good condition; 72% of pa- tients were class A and 28% class B, using the Child-
Campbell score [12]; the interval between the initial episode of bleeding and randomization and the mean dose of propranolol used were similar. Our selection was due to the inclusion criteria, and in addition ex-
cluded almost 30% of the total population already submitted to other therapies. When the study was de- signed, propranolol was supposed to be used only af- ter the bleeding episode was controlled and the pa- tient was hemodynamically stable. This excluded pa- tients who died in the first 2 weeks of the index epi- sode, approximately 30%. In the remaining Child's C patients, the potential danger offl-receptor blockade producing hypotension [16] was another reason for exclusion. Patients who had known contraindications to fl-receptor blockade were similarly excluded
(13%). The discrepancy between the results of the three
studies comparing propranolol with placebo [6-8] and the study of Lebrec et al. [5] has been related to the difference in patient selection: Burrough's and Villeneuve's patients had more advanced cirrhosis and the majority had nonalcoholic cirrhosis [6,7]. This does not apply to our study. The major differ- ence between our trial and the French trial [5] is the inclusion of patients who had bled from nonvariceal lesions. However, exclusion of this subgroup still shows effective prevention of variceal rebleeding in patients randomized by Lebrec et al. [5]. Their pa- tients who bled but did not die were withdrawn from the study and this may explain the differences ob- served [17].
In both treatment groups we analysed rebleeding (both esophageal variceal rebleeding or all clinically important rebleeding) in terms of the first occurrence of rebleeding subsequent to randomization, irrespec- tive of compliance, as noncompliance is an integral part of therapy [17]. Clearly, with a predominantly alcoholic population it is likely that strict compliance was not observed all of the time. Whatever the rea- son, all the 39 rebleeding episodes in the propranolol group occurred before changing to sclerotherapy.
Our results showed that sclerotherapy was su- perior to propranolol for the prevention of both esophageal and gastric variceal rebleeding. The number of patients who rebled and the number of ep-

184 P.T. ALEXANDRINO et al.
isodes were significantly less. The benefit of sclero- therapy in reducing the incidence of variceal rebleed- ing has also been reported in a number of controlled
trials comparing long-term sclerotherapy with place-
bo and/or medical therapy [9-11]. However, we did
not observe any difference between sclerotherapy and propranolol when the total rebleeding episodes,
from varices and other causes, were analysed. Nei-
ther the number of patients with rebleeding nor the number of episodes was statistically different. A dis-
tinct separation of the curves of patients free of re- bleeding is observed after the first year of follow-up.
The overall rebleeding rate during sclerotherapy is
63%, and 84% whilst taking propranolol_ The causes
of rebleeding were different: 84% of the propranolol
patients who rebled did so from varices and 50% of
the rebleeding sclerotherapy patients rebled from varices, but patients with obliterated varices rebleed-
ing from gastric erosions represent 29% of all re-
bleeders. This was unrelated to the continued con- sumption of alcohol.
It is a controversial issue as to whether bleeding
gastric erosions are related to portal hypertension.
The majority of controlled trials comparing sclero- therapy with other therapies did not consider it as a
• cause of rebleeding. Shunt surgery was proposed as a
therapy of bleeding gastritis, but on the other hand surgical trials report an incidence of rebleeding from
nonvariceal causes ranging from 9% [18], 13% [3],
15% [2] and 19% [19], despite patency of the shunts in the checked patients.
In a recent paper comparing sclerotherapy with distal splenorenal shunt [20], the authors reported an
overall rebleeding rate with sclerotherapy of 53% at
4 years of follow-up, with 26% of the total number of
patients rebleeding due to 'portal hypertension gas-
tritis'. Our patients who rebled from gastric erosions did well with medical treatment and all but one are
alive at the time of the trial analysis.
The cumulative survival of both groups of patients
was calculated according to the group into which they
were randomized, even if the patients who rebled had been offered other treatments. This was the case
for 10 patients in the propranolol group submitted to
chronic sclerotherapy after rebleeding and one pa-
tient in each group submitted to surgery. There is no difference in cumulative survival rate at any time or
between the Child's classes between the two thera-
pies.
The results are also no different if the two patients withdrawn from propranolol are included, or if the
analysis is performed according to treatment re- ceived rather than an intention to treat. It must be re-
membered, however, that this trial deals with a sub-
group of patiens who survived for 2 weeks after the
index bleeding episode and with a good general con- dition, which increases survival [1]. In general our
patients are not dissimilar to those reported in a num-
ber of controlled trials of other forms of elective ther-
apy of variceal bleeding. The characteristics of our
population explain the 2-year survival rate of over 70% observed in both the sclerotherapy and propra-
nolol groups. These figures are very similar to the 2-
year survival rate in sclerotherapy groups reported
by Westaby et al. [10] and the Copenhagen group,
among patients who survive the initial period [21], all of them reporting that sclerotherapy markedly im-
proved survival. Although propranolol patients rebled more from esophageal varices than sclerothe-
rapy patients, if they were then treated with an alter-
native therapy, they had the same survival. As there
was no standard medically treated (placebo) group, it
cannot be ascertained whether both therapies are similar with respect to survival, because both are su-
perior to standard medical treatment, or whether the
reduction in variceal rebleeding did not affect surviv-
al in this particular subgroup of patients_ The other
clinical trial comparing propranolol with paravari-
ceal sclerotherapy [15] did not show any difference in variceal rebleeding and survival during 2 years of fol- low-up.
A final word about the number of patients- It
would be very difficult to design a trial with a suffi-
cient number of patients to avoid both type I and type
II errors: to demonstrate a reduction of 20% in all
causes of rebleeding we would need 212 patients, in retrospective analysis we admit a type II error in rela-
tion to that difference, but there is power enough in
the significant difference between bleeding from esophageal and/or gastric varices.

PREVENTION OF VARICEAL REBLEEDING 185
Since 2 9 % of the p a t i e n t s u n d e r p r o p r a n o l o l re-
q u i r e d e m e r g e n c y s c l e r o t h e r a p y for acu t e r e b l e e d -
ing, we r e c o m m e n d the use of s c l e r o t h e r a p y as long-
t e r m e lec t ive t h e r a p y in p a t i e n t s w h o h a v e b led f r o m
e s o p h a g e a l var ices . Th i s s e e m s to be the bes t m e t h o d
of p r e v e n t i n g va r i cea l r e b l e e d i n g .
Acknowledgement
W e are g ra t e fu l to Dr . A . B u r r o u g h s for r e a d i n g
and c o r r e c t i n g the E n g l i s h of this p a p e r .
References
1 Graham DY, Smith JL. The course of patients after vari- ceal hemorrhage. Gastroenterology 1981~ 80: 800-809.
2 Reynolds TB, Donovan A J, Mikkelsen WP, et al. Results of a 12 year randomized trial of portocaval shunl in patients with alcoholic cirrhosis and bleeding varices. Gastroenter- ology 1981; 80:1005-1011.
3 Resnick RH, Iber FL, Ishihara AM, et al. A controlled study of the therapeutic portocaval shunt. Gastroenter- ology 1974; 67: 843-857.
4 Rueff, B, Prandi D, Degos F, et al. A controlled study of therapeutic portocaval shunt in alcoholic cirrhosis. Lancet 1976; i: 655-659.
5 Lebrec D, Poynard .T, Bernuau J, et al. A randomized con- trolled study of propranolol for prevention of recurrent gastrointestinal bleeding in patients with cirrhosis: a final report. Hepatology 1984; 4: 355-358.
6 Burroughs AK, Jenkins W J, Sherlock S, et al. Controlled trial of propranolol for the prevention of recurrent variceal hemorrhage in patients with cirrhosis. N Engl J Med 1983: 309: 1539-1542.
7 Villeneuve JP, Layrargues GP, Rivard CI, et al. Proprano- 1ol for the prevention of recurrent variceal hemorrhage; a controlled trial. Hepatology 1986; 6: 1239-1243.
8 Queuniet AM, Czernichow P, Lereboughrs E, Ducrotte P, Tranvouez JL, Colin R. Etude controllde du propranolol dans la prdvention des r~cidives h6morragiques chez les pa- tients cirrhotiques. Gastroentero[ Clin Biol 1987; 11: 41-47.
9 Terblanche J, Bornman PC, Kahn D, et al. Failure of re- peated injection sclerotherapy to improve tong-term sur- vival after oesophageal variceal bleeding: a five year pro- spective controlled trial. Lancet 1983; ii: 1328-1332.
10 Westaby D, MacDouga[l BRD, Williams R. Improved sur- vival following injection sclerotherapy for oesophageal vat- ices: final analysis of a controlled trial. Hepato[ogy 1985; 5: 827-830.
11 Korula J, Balart LA, Radvan G, et al. A prospective ran- domized controlled trial of chronic oesophageal variceal sclerotherapy. Hepatology 1985; 5: 584-589.
12 Campbell DP, Parker DE, Anagustapoulos CE. Survival prediction in porto-caval shunts: a computorised statistical analysis. Am J Surg 1973; 126: 748-751.
13 Grima N, Alexandrino P, Diogo AN, Alves MM, Cotter J, Pinto Correia J. Hemodynamic effects of endoscopic scle- rotherapy (ES) in patients with portal hypertension [Ab- stract]. Dig Dis Sci 1986; 31 (suppl): 196S.
14 Peto R, Pike MC, Armitage P, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. Analysis and examples. Br J Cancer 1977; 35: 1-39.
15 Fleig WE, Stange EF, Hunecke R, et al. Prevention of re- current bleeding in cirrhotics with recent variceal hem- orrhage: prospective, randomized comparison of proprano- lol and sclerotherapy. Hepatology 1987; 7: 355-361.
16 Wilkinson SP. Propranolol and portal hypertension in cir- rhosis [Letter]. Lancet 1980; ii: 429.
17 Corm H. Propranolol in portal hypertension: problems in paradise? Hepatology 1984; 4: 560-564.
18 Harley HA J, Morgan T, Redeker AG, et al. Results of a randomized trial of end-to-side portocaval shunt and distal splenorenal shunt in alcoholic liver disease and variceal bleeding. Gastroenterology 1986; 91: 802-809.
19 Conn HQ, Resnick RH, Grace ND, et al. Distal splenore- nal shunts vs portal-systemic shunt: current status of a con- trolled trial. Hepatolo~v 1981: l- |'~1-160.
20 Warren WD, Henderson JM, Millikan W J, et al. Distal splenorenal shunt versus endoscopic sclerotherapy [or long-term management of variceal bleeding. Ann Surg 1986; 203: 454-462.
21 The Copenhagen Oesophageal Varices Sclerotherapy Pro- ject. Sclerotherapy after first variceal hemorrhage in cir- rhosis. A randomized multicenter trial. N Engl J Meal 1984; 311: 1594-1600.