Embed Size (px)
DESCRIPTION
Prostate Cancer 2011-How Clinical Trials Have Led to New Options for Patients. Philip Kantoff MD Chief, Division of Solid Tumor Oncology Dana-Farber Cancer Institute Professor of Medicine Harvard Medical School. Background. 220,000 men diagnosed with prostate cancer in 2010 in US - PowerPoint PPT Presentation
Citation preview

Prostate Cancer 2011-How Clinical Trials Have Led to New Options for
Patients
Philip Kantoff MDChief, Division of Solid Tumor Oncology
Dana-Farber Cancer InstituteProfessor of Medicine
Harvard Medical School

Background
• 220,000 men diagnosed with prostate cancer in 2010 in US
• 1 in 6 men• 32,000 men will die of prostate cancer

Incidence of Prostate Cancer: Population Comparisons

Outline
• You can prevent prostate cancer
• Screening saves lives
• Many men who are diagnosed with prostate cancer do not need to be treated
• Many exciting new developments-results of clinical trials

Outline
• You can prevent prostate cancer

Finasteride Chemoprevention Study (PCPT)
18,000 Men>55 nl DRE and PSA<3
finasteride
placebo
CaP
CaP

Finasteride Chemoprevention Study (PCPT)

PCPT-Conclusions
• Finasteride reduces risk of prostate cancer
• Morbidity is minimal– Possible and slight increase in high grade
cancer in finasteride arm

REDUCE Trial• 8,200 men who had PSA between 2.5 ng/mL
and 10 ng/mL• All men had one negative prostate biopsy
within six months prior to study entry. • Participants were randomly assigned to
dutasteride or placebo; the study mandated 10 core biopsies at two and four years.
• Dutasteride was associated with a 23% reduction in prostate cancer cases compared with placebo.

FDA Approval of 5-ARIs?
• FDA advisory panel recommended against approval as chemoprevention
• Concern regarding increased incidence of high-grade tumors
• “Met an un-need”, reducing low-risk tumors• 60 men would need to be treated in order
for one man to avoid developing a clinically relevant prostate cancer

Outline
• You can prevent prostate cancer
• Screening saves lives

Does PSA based Screening Work? Does it Reduce Mortality
From Prostate Cancer?
• ERSPC study
• PLCO
• Scandinavian study

European Randomized Study of Screening for Prostate Cancer
(ERSPC) NEJM 2009• 162,243 men age 50 and 69 from seven
different European countries starting in the early 1990s
• Randomly assigned to a screening group or control
• Men in the screening group received a PSA test an average of once every 4 years and the men in the control group did not receive PSA tests at all.
• Median 9 years of follow up-20% reduction in prostate cancer mortality p=0.04

PLCO NEJM 2009
• 150,000 persons 55 to 74 years old at entry were randomized to two study arms, half to undergo cancer screening
• Screening was annual PSA and DRE
• 52% contamination
• Median follow-up 7 years
• No difference in prostate cancer mortality

Göteborg randomized prostate-cancer screening trial
• 20,000 men randomly sampled from the population register, were randomized to either a screening group invited for PSA testing every 2 years (n=10,000) or to a control group
• During a median follow-up of 14 years, 1,138 men in the screening group and 718 in the control group were diagnosed with prostate cancer
• The risk reduction of death from prostate cancer at 14 years was 60% (p=0·0002).

Conclusions
• Low mortality of prostate cancer in first 10 years (few events)
• PSA screening reduces mortality
• Large amount of overtreatment– Seen in numerous other studies

Outline
• You can prevent prostate cancer
• Screening saves lives
• Many men who are diagnosed with prostate cancer do not need to be treated

Who should consider active surveillance-NCCN Guidelines?
• Men with low risk prostate cancer (Gleason 6 and PSA<10) who have a life expectancy of less than 10 years.
• Men with “very low risk” prostate cancer when life expectancy is less than 20 years.– a Gleason score of 6 or below; a PSA <
10 and fewer than 3 positive biopsy cores (with <50% cancer in each); and a PSA density below 0.15 ng/mL per g.

Outline
• You can prevent prostate cancer
• Screening saves lives
• Many men who are diagnosed with prostate cancer do not need to be treated
• Many exciting new developments-results of clinical trials

Sipuleucel-T (Provenge) for Metastatic CRPC

Provenge: Mechanism of Action
INFUSE PATIENT
sipuleucel-T activates T-cells in the body
APC takes up the antigen
Antigen (PAP-GMCSF) is exposed to an Antigen Presenting Cell (APC)
Fully activated, the APC is now sipuleucel-T and is collected
Antigen is processed and presented on surface of the APC
T-cells proliferate and attack cancer cells

22
Sipuleucel-T: Logistics of TherapyDay 1
LeukapheresisDay 2-3
sipuleucel-T is manufacturedDay 3-4
Patient is infused
Apheresis Center Central Processing Doctor’s Office
COMPLETE COURSE OF THERAPY:Weeks 0, 2, 4

23
Randomized Phase 3 IMPACT Trial (IMmunotherapy Prostate AdenoCarcinoma Treatment)(IMmunotherapy Prostate AdenoCarcinoma Treatment)
Asymptomatic or Minimally
Symptomatic mCRPC (N=512)
Asymptomatic or Minimally
Symptomatic mCRPC (N=512)
Placebo Q 2 weeks
x 3
Placebo Q 2 weeks
x 3
Sipuleucel-T Q 2 weeks x 3
Sipuleucel-T Q 2 weeks x 3
2:1
Treated at Physician Discretion
and/or Salvage Protocol
Treated at Physician Discretion
and/or Salvage Protocol
Treated at Physician Discretion
Treated at Physician Discretion
Primary Endpoint: Overall SurvivalSecondary Endpoint: Objective Disease Progression
PROGRESSION
PROGRESSION
SURVIVAL
SURVIVAL

24
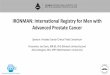
IMPACT Overall SurvivalFinal Analysis (349 events)
36.5 mo median f/u HR = 0.759 (95% CI: 0.606, 0.951)p = 0.017 (Cox model)Median Survival Benefit = 4.1 months
Sipuleucel-T (n = 341)Median Survival: 25.8 mo.36 mo. survival: 32.1%
Placebo (n = 171)Median Survival: 21.7 mo.36 mo. survival: 23.0%
No. at Risk
Sipuleucel-T 341 274 142 56 18 3
Placebo 171 123 59 22 5 2 Kantoff et al

Under-represented clinical trial populations
25
• African American patient population
• 5.8% of patients
• Positive sipuleucel-T treatment effect in patient subgroup
• AE profile comparable
HR 0.288 (0.125, 0.662)
African American Subgroup -Overall SurvivalIMPACT, D9901, D9902A

PROSTVAC VF-Tricom

27
Background-The Development of PROSTVAC-VF-Tricom
• Inactivated smallpox and fowlpox virus carrying PSA gene
Schlom et al

28

Randomized Phase II Study
Primary endpoint: Progression Free SurvivalSecondary endpoint: Overall Survival
Asymptomatic or Minimally
Symptomatic Metastatic Castrate Resistant
Prostate Cancer (N=125)
Asymptomatic or Minimally
Symptomatic Metastatic Castrate Resistant
Prostate Cancer (N=125)
Empty Vector + placebo
Empty Vector + placebo
PROSTVAC-VF Tricom + GM
PROSTVAC-VF Tricom + GM
P R O
G R E S
S I O N
P R O
G R E S
S I O N
2:1
SURVIVAL
SURVIVAL
Treated at physician discretion
and/or Salvage Protocol
Treated at physician discretion
and/or Salvage Protocol
Treated at physician discretion
Treated at physician discretion

30
Overall Survival
P = 0.006 (stratified logrank)Hazard Ratio = 0.56 (95% CI 0.37 to 0.85)
0
20
40
60
80
100
0 12 24 36 48 60Months
ControlPROSTVAC
N4082
Deaths3765
Median16.625.1
Kantoff et al

Newer Hormonal Agents
• Lyase inhibitors-block all hormone production from testicles, adrenals and from the tumor– Abiraterone

COU-AA-301• Phase III initiated in April 2008, enrollment
completed.
• Post-docetaxel mCRPC
• (n = 1158)R 2:1
Primary endpoint is OS
Abiraterone acetate, 1000 mg/day (4 x 250 mg tablets) PO,5 mg prednisone/prednisolone
BID
Placebo plus 5 mg prednisone/prednisolone BID
32

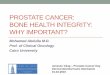
COU-AA-301: Abiraterone Acetate Improves OS in mCRPC
HR=0.646 (0.54-0.77) P <0.0001
Placebo: 10.9 months (95% CI: 10.2, 12.0)
0 100 200 300 400 500 600 700
0
20
40
60
80
100
Ove
rall
Su
rviv
al,
%
Days from Randomization
Abiraterone: 14.8 months (95% CI: 14.1, 15.4)
Abiraterone 797 728 631 475 204 25 0
Placebo 398 352 296 180 69 8 1

Outline
• You can prevent prostate cancer
• Screening saves lives
• Many men who are diagnosed with prostate cancer do not need to be treated
• Many exciting new developments-results of clinical trials

Thank you