Embed Size (px)
Citation preview
Prostate CryotherapyMinimally Invasive Cancer
Treatment
PM-3590 Rev A 08/11
This information is intended for general patient education purposes only in consultation with a physician.
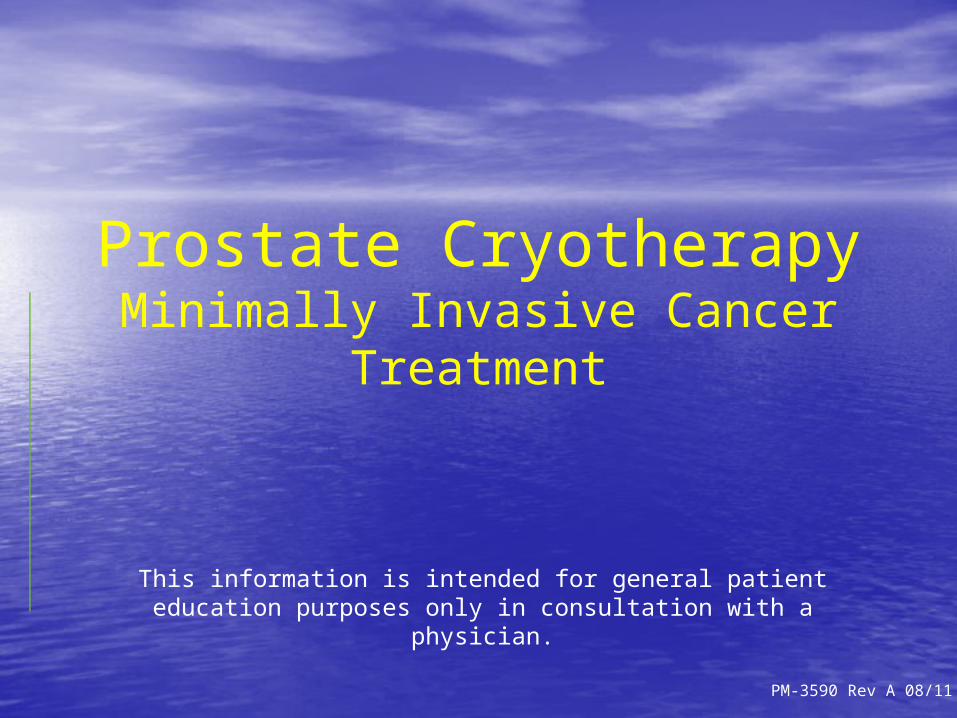
What is Cryotherapy?• Cryotherapy, Cryoablation,
Cryosurgery– Tissue Ablation (destruction) through the
localized delivery of extreme cold• Procedure Basics– Ultrasound-Guided
2.4 mm diameter probes percutaneously (without incision) introduced through the perineum
– Argon used to freeze– Helium used to thaw– Thermocouple
monitoring at key locations
2 PM-3590 Rev A 08/11

Tissue Effects of Cryoablation1
• Cell membranes are damaged along with intra & extracellular structures
• Microvascularity destroyed, disrupting oxygen supply to treated tissue
• Treated tissue necroses (dies) and is replaced by fibrotic mass
• Nerve bundles ablated, however, nerve sheaths remain intact, providing pathway for nerve regeneration
1Baust JG, et al; Current Opinion in Urology 2009, 19:127-132
3 PM-3590 Rev A 08/11

What will the patient experience?Cryotherapy• Minimally invasive, minimal blood loss, no incisions,
small probes inserted through the skin in the “bicycle seat” area
• The treatment will take place in the OR, under general or spinal anesthesia
• The entire treatment including recovery room will be around 6 hours
Recovery • Patients usually go home the same day• A Suprapubic tube (through the skin) or catheter is
usually necessary for about 1 to 2 weeks• Many patients report little discomfort and often
recover fully within days PM-3590 Rev A 08/114
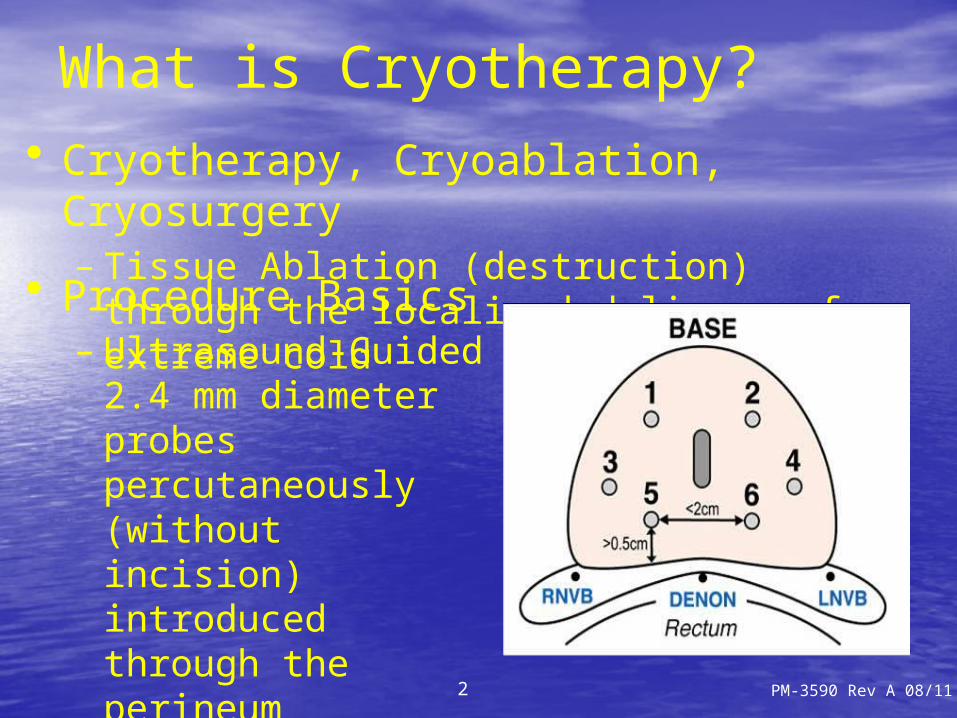
Freezing: 6-8 CryoProbe™ Devices
• 6-8 Variable/Adjustable length CryoProbes allow freezing of entire gland
• Temperature Monitoring within probes
• No probe over rectum• Argon Gas provides
rapid temperature drop PM-3590 Rev A 08/115

Monitoring: 4-6 TempProbe®
Sensors
• External Sphincter• Helps preserve
continence• Denonvillier’s Fascia
• Prevents freezing of rectum
• Neurovascular Bundles(see previous slide)• Confirms total gland
ablation
Ext. Sphincter
Denonvillier’s Fascia
PM-3590 Rev A 08/116

Probe Placement: CryoGuide®
System
Capture
Plan
Treat
Brachytherapy style planning system assures accurate and complete treatment PM-3590 Rev A 08/117

Clinical Data SummaryAvg Follow-Up
(months)Number of
PatientsTimeframe
(years)BDFS
FailureBasis
Rectal Injury
Incontinence Potency
31.8 4099 5 75%ASTRO
(3 cons ↑)0.4% 3.1%
32%(12 mo)1
100 117 7 73%Phoenix(Nadir +
2)N/A N/A 29%2
147±33 370 1080% (L)74% (M)46% (H)
Phoenix(Nadir +
2)N/A N/A N/A3
20.4±14.7 416 484% (L)82% (M)69% (H)
ASTRO(3 cons ↑)
0.0% 4.0% 51%
(48 mo)4
35 65 6 82% (H)ASTRO
(3 cons ↑)N/A 3.1% N/A5
50 76 575% (L)89% (M)76% (H)
>1.0 ng/mL
0.0% 1.3%47%
(36 mo)6
68 590 792% (L)89% (M)89% (H)
ASTRO(3 cons ↑)
<0.1% 4.3%5%
(Unaided)7
24±16.5 975 576% (L)67% (M)41% (H)
>1.0 ng/mL
0.5% 7.5%7%
(Unaided)8
1Dhar et al, J Urol 2010; 183(4 Supl):e184 Abstract 467. 2Donnelly et al, Cancer 2010; 116(2):323-30. 3Cohen et al, Urology 2008; 71(3):515-8. 4DiBlasio et al, IBJU 2008; 34:443-50. 5Ellis et al, Urology 2007; 69(2):306-10. 6Prepelica et al, Cancer 2005; 103(8):1625-30. 7Bahn et al, Urology 2002; 60(Supl 2A):3-11. 8Long et al, Urology 2001; 57(3):518-23.
PM-3590 Rev A 08/118
Clinical Data Highlights
• Timeframes up to 10 years3
• Over 6,000 patients studied1-8
• Overall BDFS = 73%-90%1-8
• Return to potency as high as 51% after 4 years3
– Utilized active rehabilitation
• Rectal injury ≤ 0.5%1,3,5-8
• Incontinence < 8%1,4-8
• Favorably compares to external beam radiation2
1Dhar et al, J Urol 2010; 183(4 Supl):e184 Abstract 467. 2Donnelly et al, Cancer 2010; 116(2):323-30. 3Cohen et al, Urology 2008; 71(3):515-8. 4DiBlasio et al, IBJU 2008; 34:443-50. 5Ellis et al, Urology 2007; 69(2):306-10. 6Prepelica et al, Cancer 2005; 103(8):1625-30. 7Bahn et al, Urology 2002; 60(Supl 2A):3-11. 8Long et al, Urology 2001; 57(3):518-23.
PM-3590 Rev A 08/119

Cryoablation of the Prostate
Before
During Probe
Placement
FrozenPM-3590 Rev A 08/1110
This information is intended for general patient education purposes only in consultation with a
physician.
![Dramatic Reduction of CEA Post Spray Cryotherapy in a Patient … · 2018-06-09 · chemotherapy with cryotherapy [2-5]. Standard, slow-energy transfer cryotherapy or cryosurgery](https://img.pdfslide.net/doc/110x75/5e852869e78a231248157db5/dramatic-reduction-of-cea-post-spray-cryotherapy-in-a-patient-2018-06-09-chemotherapy.jpg)