Embed Size (px)
Citation preview

Hindawi Publishing CorporationEvidence-Based Complementary and Alternative MedicineVolume 2012, Article ID 850512, 14 pagesdoi:10.1155/2012/850512
Research Article
Proteomic Analysis Reveals the Deregulation ofInflammation-Related Proteins in Acupuncture-Treated Rats withAsthma Onset
Yu-Dong Xu,1, 2 Jian-Mei Cui,2 Yu Wang,1 Lei-Miao Yin,1 Chang-Ke Gao,2 Xiao-Yan Liu,1
Ying Wei,1 Yan-Yan Liu,1 Yong-Liang Jiang,1 Chun-Xiao Shan,1 and Yong-Qing Yang1, 2
1 Molecular Biology Laboratory, Shanghai Research Institute of Acupuncture and Meridian,Shanghai University of Traditional Chinese Medicine, Shanghai 200030, China
2 Yue Yang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
Correspondence should be addressed to Yong-Qing Yang, [email protected]
Received 29 June 2012; Revised 16 September 2012; Accepted 17 September 2012
Academic Editor: Alvin J. Beitz
Copyright © 2012 Yu-Dong Xu et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Although the beneficial effects of acupuncture in asthma treatment have been well documented, little is known regardingthe biological basis of this treatment. Changes in the lung proteome of acupuncture-treated rats with asthma onset werecomparatively analyzed using a two-dimensional gel electrophoresis (2DE) and mass-spectrometry- (MS-) based proteomicapproach. Acupuncture on specific acupuncture points appeared to improve respiratory function and reduce the total numberof leukocytes and eosinophils in bronchoalveolar lavage fluid in OVA-induced asthma onset. Image analysis of 2DE gels revealed32 differentially expressed acupuncture-specific protein spots in asthma onset; 30 of which were successfully identified as 28unique proteins using LC-MS/MS. Bioinformatic analyses indicated that these altered proteins are most likely involved ininflammation-related biological functions, and the functional associations of these proteins result in an inflammation signalingpathway. Acupuncture regulates the pathway at different levels by regulating several key nodal proteins, including downregulatingof proinflammatory proteins (e.g., S100A8, RAGE, and S100A11) and upregulating of anti-inflammatory proteins (e.g., CC10,ANXA5, and sRAGE). These deregulated inflammation-related proteins may mediate, at least in part, the antiasthmatic effect ofacupuncture. Further functional investigation of these acupuncture-specific effector proteins could identify new drug candidatesfor the prophylaxis and treatment of asthma.
1. Introduction
Asthma is a major public health problem that is charac-terized by an inflammatory disorder of the airways [1].The global prevalence, morbidity, mortality, and economicburden associated with asthma have increased worldwideover the past two decades. Approximately 300 millionpeople worldwide currently have asthma, and it is estimatedthat an additional 100 million people will be affected by2025 [2]. Although current allopathic treatments, includinganti-inflammatory and muscle-relaxing drugs, can providetemporary symptomatic relief, they do not prevent thenatural course of asthma [3, 4]. Because of unsatisfactorypharmacological interventions and adverse drug reactions,
many asthma sufferers turn to alternative or complementarytherapies for improved asthma management [5].
Acupuncture is an effective therapy that has been prac-ticed in China and other East Asian countries since 2000B.C. This technique uses fine needles that are inserted intospecific points of the body and manipulated with the intentof treating a wide variety of diseases. The World HealthOrganization endorses acupuncture for asthma and 42 otherindications [6], and the US National Institutes of Healthissued a consensus statement in 1997 proposing acupunctureas an effective treatment option for several health problems,including asthma [7]. We have previously reported thatacupuncture treatment, given according to the principlesof traditional Chinese medicine in patients with allergic

2 Evidence-Based Complementary and Alternative Medicine
asthma, has an immunomodulatory effect on inflammatorycells and cytokines and is associated with an improvementin general well-being [8], which is in good agreement witha study by Joos et al. [9]. Acupuncture can regulate thebalance of the Thl/Th2 response and reduce leukotriene B4and nitric oxide levels, which efficiently decreases immune-mediated lung inflammation in asthmatic rats [10, 11].Although findings from clinical and experimental studiesindicate that acupuncture has immunomodulatory and anti-inflammatory effects on asthma [12], little is known aboutthe biological basis of acupuncture treatment. A global pro-tein profiling study based on the effectiveness of acupuncturecould reveal the molecular basis of acupuncture treatmentand identify new therapeutic targets for asthma.
In recent years, a number of proteomic studies ofacupuncture in neurological disorders, including neuro-pathic pain, Parkinson’s disease, and spinal cord injury,have been published [13–15], and several candidate proteinsassociated with acupuncture effectiveness have been iden-tified. However, few proteomic studies have been designedto investigate the effects of acupuncture on asthma. Inthis study, a 2DE/MS-based proteomic analysis of lungtissues from acupuncture-treated rats with OVA-inducedasthma onset was performed to identify acupuncture-specificeffector proteins, which are expressed as a result of asthmatreatment, and elucidate the molecular mechanisms under-lying the antiasthma effect of acupuncture.
2. Materials and Methods
2.1. Animals. All animal experiments and procedures havebeen approved by the Committee on the Ethics of AnimalExperiments of Shanghai University of Traditional ChineseMedicine (approval ID: 08001) and were conducted inaccordance with the regulations set forth by the StateScience and Technology Commission. Pathogen-free, maleSprague-Dawley (SD) rats (four weeks old, 110–130 g, SLACLaboratory Animal Co. Ltd.; Shanghai, China) were raised ina pathogen-free rodent facility and provided with food andwater ad libitum. The rats were randomly divided into fourgroups: normal control rats (NC, n = 15), asthmatic rats(AS, n = 14), asthmatic rats treated with acupuncture (AA,n = 12), and normal rats treated with acupuncture (NA,n = 15). All rats were housed in animal facilities approved bythe Shanghai Committee for the Accreditation of LaboratoryAnimals for at least one week before the experiments wereinitiated.
2.2. Protocol for Sensitization and Allergen Challenge. Ratswere sensitized and challenged with ovalbumin (OVA, gradeV, Sigma, Taufkirchen, Germany) according to a previouslydescribed protocol [17]. Briefly, on day 0, the rats wereintraperitoneally injected with 1 mg of OVA precipitatedwith 10 mg of aluminum hydroxide gel and dissolved in1 mL saline (0.9% NaCl). On day 14, allergic rats wereanaesthetized with 1% sodium pentobarbitone (w/v) at adose of 50 mg/kg by intraperitoneal injection and werechallenged with 1 mL/kg of 5% OVA in saline (5 mg/kg) by
injection into the external jugular vein over a 10 s period(Figure 1(c)). The rats in the NC and NA groups received thesame treatment schedule but were sensitized and challengedwith saline instead of OVA.
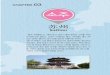
2.3. Acupuncture Treatment. The acupuncture points, GV14 (Dazhui, between the C7 and T1 vertebrae), bilateralBL12 (Fengmen, foveola laterally between the T2 and T3vertebrae), and bilateral BL13 (Feishu, foveola laterallybetween the T3 and T4 vertebrae), were selected based onthe theory of traditional Chinese medicine in treating asthma[8] (Figure 1(a) and Figure 1(b)). In accordance with ourclinical treatment of asthma [8], manual acupuncture wasperformed once every other day for two weeks beginningon the first day after sensitization (Figure 1(c)). Disposablestainless needles (13 mm long, 0.30 mm in diameter, SuzhouMedical Appliance Factory; Suzhou, China) were insertedthrough the skin to a depth of approximately 5 mm. Theneedles were twisted approximately 360◦ evenly at a rateof 60 times/min for 20 s, manipulated every 5 min, andwithdrawn after 20 min. To conveniently manipulate theacupuncture points on the back, the rat was placed on asuspended shelf (50 × 45 mm, approximately 50 cm highfrom the ground, Figure Supplemental 1 available online atdoi:10.1155/2012/850512), which calmed the rat and elim-inated the need for anesthesia [16]. The same experiencedpractitioner performed all needle manipulations, and theanimals were handled while awake. Special care was takento minimize stress. The rats in NC and AS groups werealso placed on the suspended shelf but did not receiveacupuncture treatment.
2.4. Measurement of Pulmonary Function. Pulmonary func-tion was assessed by measuring changes in the pulmonaryresistance (RL), dynamic compliance (Cdyn), and respira-tory rate (RR) in response to OVA challenge in anaesthetized,spontaneously breathing rats [16, 18]. Briefly, a rat wasplaced in a supine position and warmed with an incandescentlamp after anesthesia. At the upper part of the trachea, a T-shaped incision was made, and a T-shaped cannula, whichwas directly attached to a heater-controlled pneumotacho-graph (Fleisch model 000, Hans Rudolph; USA), was gentlyinserted into the trachea. Tidal flow was determined usinga pneumotachograph connected to a differential pressuretransducer (AutoTran, model 600D-011, ±2 cm H2O). Tomeasure the transpulmonary pressure, a water-filled PE-90tube was inserted into the esophagus to the mid-thoraxlevel (lower one-third of the esophagus) and coupled to apressure transducer (PT14MX, Jialong Teaching Equipment;Shanghai, China). The pneumotachograph tidal flow signalwas integrated with respect to time to obtain the tidalvolume. The pulmonary resistance (RL) and dynamic com-pliance (Cdyn) were calculated over a complete respiratorycycle using an integration method over flows, volumes, andpressures and were continuously recorded with software(Shanghai Medical College, Fudan University) designed forphysiology experiments. The respiratory parameters wereaveraged in 60 s segments, and the maximum RL, minimum

Evidence-Based Complementary and Alternative Medicine 3
Baseline recordOperation
d 1 d 3
Acupuncture treatment Measurement10 min 10 min5 min3–5 min
OVA challengein 10 s
(a) (b)
(c)
(a) (b)
OVA challenge and respiratory function measurement
Samplecollection
Day 14
Anaesthesis
d 5 d 7 d 9 d 11 d 13
Day 0
OVAsensitization
(b)(a)((
GV14 (Dazhui )
BL12 (Fengmen )
BL13 (Feishu )
Figure 1: Schematic localization of acupuncture points: GV14 (Dazhui), BL12 (Fengmen), and BL13 (Feishu) stimulated in rats (a), and thecorresponding equivalent acupuncture points in the human body (b). (c) Presentation of the experimental procedure; rats were sensitizedwith OVA at day 0. Acupuncture was repeatedly administered at specific acupuncture points on alternate days for 2 weeks from the first dayafter sensitization. On day 14, rats were anaesthetized and challenged with OVA by injection into the external jugular vein. The pulmonaryresistance (RL), dynamic compliance (Cdyn), and respiratory rate (RR) were recorded before the challenge for 10 min as the baselinevalues and immediately measured for another 10 min after the OVA challenge. The sample collections were performed immediately afterthe measurements were taken. Control rats were sensitized and challenged with saline instead of OVA.
Cdyn, and change in respiratory rate (RR) values weretaken and calculated as the differential value subtracted fromthe corresponding baseline value (Figure 1(c)). Experimentaloperators in lung function measurement, and the followingBALF analysis, 2DE-MS/MS, and western blot analysis didnot know the animal and sample allocation.
2.5. Bronchoalveolar Lavage Fluid (BALF) Collection andAnalysis. BALF collection was performed immediately fol-lowing the pulmonary function measurements. Each ratwas anesthetized and the lung and heart were surgicallyexposed. The trachea was cannulated and the lung waslavaged three times with a total volume of 10 mL of sterilesaline. The recovered lavage fluid was pooled and centrifugedat 300 g for 10 min at 4◦C. The cell pellet obtained from theBALF was resuspended in 100 μL PBS containing 1% BSA,and the BALF total leukocyte and differential cell countswere performed using a Hemavet 950 veterinary hematologysystem (Drew Scientific; Oxford, CT, USA).
2.6. Lung Tissue Sample Preparation. The excised right lobeof the lung was rinsed free of blood in ice-cold saline
and immediately frozen in liquid nitrogen. Protein fromeach lung tissue was extracted using a ReadyPrep SequentialExtraction Kit (Bio-Rad; Hercules, CA) with PMSF (1 mM),DNase (RNase-free; 20 μg/mL), and RNase (5 μg/mL) addedto Reagent 1 immediately before use. Protein concentrationswere determined using a modified Bradford assay. For the2DE analysis, protein extracts from animals in the samegroup were pooled equally according to protein quantity andstored at −80◦C until use.
2.7. 2DE Analysis. Protein (100 μg) was loaded onto 17 cmIPG strips with a linear separation range of pH 3–10 (Bio-Rad; Hercules, CA), which were subsequently rehydrated for12 h at 50 V at 20◦C. First-dimensional isoelectric focusing(IEF) was performed in a Protean IEF Cell (Bio-Rad).The IEF voltage was raised with a rapid ramp to 10,000 Vand strips were run at 20◦C with the current limitedto 50 mA/strip, until reaching 60,000 Vh. After IEF, thefocused IPG strips were equilibrated at room temperaturein buffer (50 mM Tris-HCl pH 8.8, 6 M urea, 20% glycerol,and 2% SDS) with 2% DTT (w/v) for 15 min followedby a second equilibration in the same buffer containing2.5% iodoacetamide (w/v) for 15 min. The strips were

4 Evidence-Based Complementary and Alternative Medicine
placed on 13% polyacrylamide gels and embedded in 1%agarose stacking gel. The second-dimensional SDS-PAGEwas performed at 24 mA per gel until the bromophenol bluedye front reached the bottom of the gels. The gels wererun in triplicate for each sample and stained with silvernitrate solution. For image analysis, the gels were scannedat a high resolution with a GS-800 densitometer (Bio-Rad),and PDQuest software version 7.1 (Bio-Rad) was used todetect altered protein expression levels. The automatic spotdetection and matching of the gels were followed by manualvalidation of the matched and unmatched protein spots. Theintensity volumes of individual spots were normalized withthe total intensity volume of all spots present in each gel(%V). Only those protein spots with intensity alterationsequal to or greater than twofold (t-test, P < 0.05) wereconsidered to demonstrate significant differential expression.
2.8. In-Gel Digestion and LC-MS/MS Analysis. Protein spotswith significant alterations in expression were manuallyexcised from the 2DE gels, destained for 20 min with equalvolumes of 30 mM potassium ferricyanide and 100 mMsodium thiosulfate at room temperature, and washed withMilli-Q water until the gels were destained. The spotswere maintained in 0.2 M NH4HCO3 for 20 min beforebeing lyophilized. Each spot was digested overnight with12.5 ng/mL trypsin in 0.1 M NH4HCO3 . The peptides wereextracted three times with 50% CAN and 0.1% TFA. Theidentification of the digested proteins was conducted usinga Finnigan LTQ mass spectrometer (ThermoQuest; San Jose,CA) coupled with a Surveyor HPLC system (ThermoQuest).First, a Microcore RP column (C18 0.15 mm × 120 mm;ThermoHypersil; San Jose, CA) was used to separate theprotein digests. Solvent A was 0.1% formic acid, and solventB was 0.1% formic acid in 99.9% ACN. The gradient washeld at 2% solvent B for 15 min and linearly increased to98% solvent B over 90 min. The peptides were eluted froma C18 microcapillary column at a flow rate of 150 μL/minand electrosprayed directly into the LTQ mass spectrometerwith an applied spray voltage of 3.2 kV. The scan rangedfrom m/z 400 to 2000. Protein identification using MS/MSraw data was performed using SEQUEST software (ThermoFinnigan) by searching against the Swiss-Prot rat proteindatabase. The identification results were filtered using Xcorr(1+≥1.9, 2+≥2.2, 3+≥3.75) and DelCn (≥0.1).
2.9. Bioinformatic Analysis. To highlight the potential bio-logical processes affected by acupuncture, differentiallyexpressed proteins were classified into groups according tobiological processes using the PANTHER (Protein ANalysisTHrough Evolutionary Relationships) Classification System(http://www.pantherdb.org/). Protein classifications werereviewed, and minor changes were made based on publisheddata regarding protein function (NCBI’s GeneRIFs and/orprotein data retrieval system iHOP). Proteins that did notmatch any entry in the PANTHER database or did not havean annotated function were assigned to one of PANTHER’sparent groups, with the aid of the online Gene Ontology toolAmiGO (http://amigo.geneontology.org). Protein-protein
interactions of proteins identified as having inflammatorybiological functions were investigated using the STRING(Search Tool for the Retrieval of Interacting Genes/Proteins)database of physical and functional interactions [19].
2.10. Western Blot. The same protein samples used for 2DEwere subjected to SDS-PAGE (12% to 15% polyacrylamidegels) and electrotransferred onto polyvinylidene fluoridemembranes (Millipore; Billerica, MA). The membranes wereblocked with PBS containing 5% nonfat milk and 0.1%Tween 20 for three hours at room temperature. The blockedmembranes were incubated overnight at 4◦C with specificprimary antibodies against CC10 (1 : 5000, Millipore 07–623), RhoGDI2 (1 : 2000, Abcam ab14230), S100A8 (1 : 3000,Santa Cruz sc-8113), sRAGE (1 : 5000, R&D AF1616), and β-actin (1 : 5000, Abcam) and were washed and incubated withthe appropriate horseradish-peroxidase- (HRP-) conjugatedsecondary antibodies for three hours at room tempera-ture. Immunocomplexes were visualized using enhancedchemiluminescence detection reagents (Beyotime; Shanghai,China) on X-ray films. Proteins were quantified usingoptical density analysis of protein bands using Quantity Onesoftware (Bio-Rad). Each protein band was normalized to thecorresponding β-actin band.
2.11. Statistical Analysis. Data were presented as the mean± SEM. A one-way analysis of variance (ANOVA) wasperformed to evaluate the differences among the groups. Posthoc comparisons, if applicable, were performed using theLeast Significant Difference (LSD) test. A value of P < 0.05was considered statistically significant.
3. Results
3.1. Effect of Acupuncture on Respiratory Function Variabilityin Asthma Onset in Rats. The allergen challenge in OVA-sensitized rats induced a significant increase in the RL at 1to 5 min (P < 0.05, Figure 2), and significant decreases in thesimultaneously measured Cdyn and RR (Table Supplemental1 available online at doi:10.1155/2012/850512) comparedwith control rats, thus indicating an OVA-induced asthmaonset. When acupuncture was performed on the OVA-sensitized rats in the AA group, the RL was significantlydecreased 2 to 5 min after the OVA challenge when comparedwith the AS group (P < 0.05, Figure 2), and Cdyn and RRwere increased 2 to 5 min after the challenge when comparedwith the AS group (Table Supplemental 1 available onlineat doi:10.1155/2012/850512). In addition, in acupuncture-treated normal rats, RL was unchanged after saline challengewhen compared with normal controls.
3.2. Effect of Acupuncture on the Total Leukocyte and Differen-tial Cell Counts in BALF. The total leukocyte, eosinophil, andbasophil counts in BALF recovered from OVA-challengedrats were significantly higher compared to normal controlrats (P < 0.05, P < 0.01, and P < 0.01, resp.). However,the numbers of neutrophils, lymphocytes, and monocyteswere unchanged after OVA challenge in OVA-sensitized rats.

Evidence-Based Complementary and Alternative Medicine 5
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
1 2 3 4 5 6 7 8 9 10
Ch
ange
s in
RL
afte
r ch
alle
nge
(kP
a/m
L/s)
Time (min) after OVA challenge
NCAS
AANA
−0.02
##
##
####
∗∗∗∗ ∗ ∗
#
Figure 2: Changes in the pulmonary resistance (RL) within 10 minafter challenge in NC (n = 15, sensitized and challenged withsaline), AS (n = 14, sensitized and challenged with OVA), AA(n = 12, sensitized and challenged with OVA + acupuncturetreatment) and NA (n = 15, sensitized and challenged with saline+ acupuncture treatment).The changes in the RL are expressedas differential values subtracted from the corresponding baselinevalues (Figure 1). Each point represents the mean± SEM. #P < 0.05,##P < 0.01 when comparing the AS group with the NC group and∗P < 0.05, ∗∗P < 0.01 when comparing the AA group with the ASgroup.
Treatment with acupuncture in the AA group significantlydecreased the total leukocyte, neutrophils, eosinophils, andbasophils in BALF compared with AS rats (all P < 0.01). TheBALF total and differential cell counts were not significantlydifferent between the normal control rats and acupuncture-treated normal rats (Figures 3(a) and 3(b)), which indicatedthat the changes in the cellular composition of the BALF byacupuncture is specific to asthma onset.
3.3. Changes in the Lung Proteome of Asthma Onset in RatsTreated with Acupuncture. The protein content in the samplefrom each group was measured using 2DE at least threetimes and was followed up by verifying that the same proteinpatterns within each group were obtained. We detectedapproximately 550–650 distinct protein spots in each 2DEgel and acquired a high overlap rate (>85%) for spots inthe parallel gels. Image analysis of the 2DE gels revealedthat acupuncture at specific points induced lung proteomechanges both in the normal rats (NA group versus NCgroup) and in rats with asthma onset (AA group versus ASgroup). However, the expression levels of 32 protein spotswere altered after acupuncture treatment in the rats withasthma onset but not changed after acupuncture treatmentin the normal rats (Figure 4(a)), which essentially indicatedthe pathology-specific regulation of acupuncture. These 32acupuncture-specific differentially expressed protein spotscould be divided according to their 2DE gel expression
patterns into six different categories, which are presentedin Table 1. Thirty protein spots were successfully identifiedby LC-MS/MS, which corresponded to 28 unique proteins(Table 1). Among them, 23 proteins had differential expres-sion levels in the AS group compared with the NC group,and the levels were restored to normal expression levelsafter acupuncture in the AA group, including the proteinsCC10 (uteroglobin), S100A8, RAGE (advanced glycosylationend product-specific receptor), and RhoGDI2 (Rho, GDPdissociation inhibitor (GDI) beta) (Figures 4(b), and 4(c)).ANXA5 (Annexin A5) and PRDX6 (Peroxiredoxin 6) didnot exhibit changes in expression in the AS group comparedwith the NC group; however, they did exhibit increased anddecreased levels, respectively, after acupuncture in the AAgroup.
3.4. Bioinformatic Analyses of Proteins Differentially Expressedfollowing Acupuncture. Using the PANTHER classificationsystem, proteins that were differentially expressed followingacupuncture in the AA group were classified by biologi-cal processes (Figure 5(a), Table Supplemental 2 availableonline at doi:10.1155/2012/850512). Protein classificationrevealed that many of the identified proteins are impli-cated in inflammation-related biological functions, includ-ing metabolic processes, inflammatory signal transduction,immune system processes, response to stimulus, and oxida-tion/reduction. The effect of Acupuncture on asthma may beassociated with the regulation of inflammatory processes.
Further analysis with the online tool STRING revealeda protein-protein interaction network among the proteinswith inflammation-related biological functions, and sevenproteins, including CC10, S100A8, S100A11, RAGE, ANXA5,RhoGDI2, and PRDX6, were associated either directly orindirectly by intermediate proteins (proteins that haveknown interactions with the identified proteins but werenot detected in our proteomic experiment) (Figure 5(b)).Notably, the intermediate protein S100A9, which is aninflammation-related protein related to S100A8 in terms ofbiological function, was regulated in asthmatic rats treatedwith acupuncture in our previous study [16]. The functionalassociations of these proteins indicate an inflammatorysignaling pathway in asthma that can be regulated byacupuncture.
3.5. Confirmation of the Differential Expression of Inflamma-tion-Related Proteins. To verify the deregulation of inflam-mation-related proteins following acupuncture, CC10,S100A8, RAGE, and RhoGDI2 were selected as representativeproteins and subjected to western blotting. In the AS group,the expression of S100A8 and RhoGDI2 were significantlyincreased (P < 0.01), whereas the expression of CC10 wassignificantly decreased (P < 0.01) when compared with theNC group. In the AA group, the expression of S100A8 andRhoGDI2 was downregulated (P < 0.01 and P < 0.05, resp.),and the expression of CC10 was upregulated (P < 0.01)relative to the AS group after acupuncture (Figures 6(a) and6(c)). These results are consistent with the results observedin the 2DE gels.

6 Evidence-Based Complementary and Alternative Medicine
0
4
8
12
16
20
NC AS AA NA
Tota
l leu
kocy
te c
oun
t (×
104/m
L)
∗
#
∗
(a)
0
10
20
30
40
50
60
70
Neu Lyc Mon Eos Bas
Cel
l nu
mbe
r (×
103/m
L)
NC
AA NA
#
∗
#
# #
∗ ∗∗
∗∗
AS
(b)
Figure 3: The effect of acupuncture on the cellular composition of BALF. BALFs were collected after OVA challenge. Total leukocyte (a)and differential cell counts (b) were performed. Neu, neutrophil; Lym, lymphocyte; Mon, monocyte; Eos, eosinophil; Bas, basophil. Valuesrepresent the mean ± SEM. #P < 0.05, ##P < 0.01 when comparing the AS group with the NC group, and ∗∗P < 0.01 when comparing theAA group with the AS group.
RAGE typically consists of an extracellular immuno-globulin-like region, a short transmembrane domain, anda cytosolic tail. In addition to full-length RAGE, there is anisoform designated as soluble RAGE (sRAGE), which cor-responds to the extracellular domain of RAGE lacking thecytosolic and transmembrane domains [20]. AS to differen-tially expressed protein spot 24 (Figure 4), all six unique pep-tide sequences identified by mass spectrometry were mappedto the extracellular domain of RAGE (Table Supplemental3 available online at doi:10.1155/2012/850512). Therefore,it is possible that the identified protein corresponding tospot 24 was sRAGE as opposed to RAGE. To investigatethis possibility, we performed western blot experimentusing an anti-rat RAGE extracellular domain monoclonalgoat antibody (R&D Systems; Minneapolis, MN), whichdemonstrated that the lung tissue homogenate containedthree protein bands of approximately 55, 50, and 48 kD;the 48 kD band corresponds to sRAGE and the 55 kD and50 kD bands correspond to full-length RAGE as describedby Uchida et al. [21]. The resulting expression pattern isconsistent with the 2DE analysis that shows that sRAGE wasexpressed at a relatively low level in the AS group (P < 0.05versus NC) and was upregulated after acupuncture in the AAgroup (P < 0.05 versus AS). However, the expression patternof RAGE is completely opposite to that of sRAGE (Figures6(b) and 6(c)).
4. Discussion
Acupuncture is an integral part of traditional Chinese medi-cine and is used to treat variety of illnesses, including asthma.Over the past decade, several clinical trials have evaluated theefficacy of acupuncture therapy on asthma [22, 23]. In our
recent clinical research, we have reported that acupunctureat the Dazhui, Fengmen, and Feishu points of patients withallergic asthma has an immunomodulatory effect, whichresults in an improvement in general well-being [8]. Inview of the theory of traditional Chinese medicine, Dazhui,which is the crossing point of three yang meridians andthe governor vessel (GV), can strengthen the yang qi of theentire body and reinforce the vital qi to relieve asthmaticsymptoms. Fengmen always functions to regulate the flowof the meridian qi and is used to dredge and activate thelung meridian. Feishu is the site where the qi of the lungmeridian gathers in the back and is especially effective intreating respiratory disorders caused by either exogenousor endogenous pathogenic factors. The combination of thethree points can regulate the qi of the lung meridian, removeobstruction from the meridian, and disperse the lung qi tostop asthma.
Although the antiasthmatic effect of acupuncture hasbeen well documented, little is known about its molecularbasis. In the present study, acupuncture treatment appearedto improve the respiratory function and reduce the totalleukocyte and eosinophil number in the bronchoalveolarlavage fluid of sensitized rats after OVA challenge. Using a2DE/MS-based proteomic approach, the lung proteome ofacupuncture-treated rats with asthma onset was examined.Acupuncture at specific points led to lung proteome changesboth in the normal rats (NA group versus NC group) andthe rats with asthma onset (AA group versus AS group).However, the expression levels of 32 protein spots wereobserved to change after acupuncture treatment in ratswith asthma onset but were unchanged after acupuncturetreatment in normal rats. 30 of the 32 acupuncture-specific differentially expressed protein spots in asthmaonset were successfully identified as 28 unique proteins.

Evidence-Based Complementary and Alternative Medicine 7
1 2
3
7
8
9
10
11
12
13
14
15
18
19
20
76
66.2
43
36
31
21.5
17.5
3 PI 10
21
22
2324
25
26
27
2930
31
3216
17
45
6
28
MW (kD)
(a)
NC AS AA NA
S100A8
CC10
RhoGDI2
ANXA5
RAGE∗
(b)
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Opt
ical
den
sity
NCAS
AANA
S100A8CC10 RhoGDI2 ANXA5RAGE∗
∗
#∗
∗
∗
∗∗
##
#
(c)
Figure 4: Protein expression profiles in lung tissues. (a) A representative 2DE gel image of proteins isolated from the AA group. Thenumerically labeled spots indicate the differentially expressed protein spots among the NC, AS, and AA groups. The numbers correspondto the spot identification numbers listed in Table 1. The molecular weight standards and pH range are shown at the left and bottom of thegels, respectively. (b) Differential expression profiles of five inflammation-related proteins regulated by acupuncture: CC10, S100A8, RAGE∗
(which is actually sRAGE, Table 1), RhoGDI2, and ANXA5. The cropped images of 2DE gels were symmetrically boxed, and the arrows onthe images indicate the relative positions of the protein spots. (c) Quantitative analysis of the five inflammation-related proteins regulatedby acupuncture. Each spot volume was quantified from the intensity of the spots using PDQuest software. The bars represent the mean ±SEM of triplicate 2DE gels. #P < 0.05, ##P < 0.01 when comparing the AS group with the NC group. ∗P < 0.05, ∗∗P < 0.01 when comparingthe AA group with the AS group.
The identified proteins have been implicated in diverseinflammation-related biological functions, including inflam-matory signal transduction, immune system processes,response to stimulus, and oxidation/reduction. Of theseproteins, several proinflammatory proteins (e.g., S100A8,RAGE, and S100A11) were downregulated, and several anti-inflammatory proteins (e.g., CC10, ANXA5, and sRAGE)
were upregulated following acupuncture. The investigationof protein-protein interactions revealed a functional networkassociated with inflammatory signaling, and CC10, S100A8,RAGE, and RhoGDI2 acted as key node proteins. Westernblot analysis of CC10, S100A8, RAGE, and RhoGDI2 con-firmed the regulation of inflammation-related proteins andthe functional network by acupuncture treatment.

8 Evidence-Based Complementary and Alternative Medicine
Ta
ble
1:L
ist
of32
acu
pun
ctu
re-s
peci
fic
diff
eren
tial
lyex
pres
sed
prot
ein
sin
asth
ma
onse
t.
Spot
no.
aP
rote
inn
ame
Gen
esy
mbo
lSw
iss-
Pro
tn
o.E
xpre
ssio
nle
velr
atio
sT
heo
reti
cal
Mr(
kDa)
/PI
Pept
./co
v%
bA
S/N
CA
A/A
SN
A/N
C
Patt
ern
Iof
chan
ges
inex
pres
sion
NC
AS
AA
NC
AS
1P
rote
inS1
00-A
8S1
00a8
P50
115
4.44
90.
553
0.95
110
.2/5
.76/
56.1
8%2
Pro
tein
S100
-A8
S100
a8P
5011
513
.674
0.46
41.
669
10.2
/5.7
26/4
1.57
%3
Sim
ilar
tode
stri
nLO
C29
6197
XP
2158
62—
d0.
158
—d
18.5
/7.5
11/2
7.88
%4
Act
in,c
ytop
lasm
ic1
Act
bP
6071
12.
882
0g
4.16
841
.7/5
.313
/10.
67%
5R
ho,
GD
Pdi
ssoc
iati
onin
hib
itor
(GD
I)be
taA
rhgd
ibQ
5M86
0—
d0.
101
—d
22.9
/5.0
4/21
.00%
6A
ctin
,alp
ha
skel
etal
mu
scle
Act
a1P
6813
613
.250
0.14
54.
582
42.0
/5.2
8/11
.94%
7Se
rum
albu
min
prec
urs
orA
lbP
0277
0—
e0.
231
—e
68.7
/6.1
7/6.
58%
8A
TP
syn
thas
esu
bun
ital
pha,
mit
och
ondr
ial
prec
urs
orA
tp5a
1P
1599
9—
d0.
197
—d
59.8
/6.2
53/2
2.24
%
9G
lyce
rald
ehyd
e-3-
phos
phat
ede
hydr
ogen
ase
Gap
dhP
0479
7—
d0.
203
—d
35.8
/8.1
5/12
.31%
10G
lyce
rald
ehyd
e-3-
phos
phat
ede
hydr
ogen
ase
Gap
dhP
0479
73.
905
0.24
80.
828
35.8
/8.1
17/2
9.73
%11
An
ion
ictr
ypsi
n-1
prec
urs
orP
rss1
P00
762
—d
0.42
0—
d26
.0/4
.74/
8.13
%12
22kD
apr
otei
n—
—2.
288
0.44
20.
591
—6/
16.8
3%
13N
a+/K
+-t
ran
spor
tin
gA
TPa
sesu
bun
ital
pha-
1pr
ecu
rsor
Atp
1a1
P06
685
—d
0.47
1—
d11
.3/5
.316
/13.
29%
14Tu
bulin
alph
a-1A
chai
nTu
ba1a
P68
370
—d
0.42
5—
d50
.1/4
.911
/13.
53%
15P
hos
phog
lyce
rate
kin
ase
1P
gk1
P16
617
3.72
80.
369
1.12
144
.5/8
.09/
29.5
0%16
S100
a11
S100
a11
Q6B
345
4.19
00
g1.
087
11.1
/5.6
3/26
.50%
17Si
mila
rto
Ras
supp
ress
orpr
otei
n1
Rsu
1D
3ZC
X0
2.21
10.
429
1.26
431
.5/8
.54/
10.8
3%
Patt
ern
IIof
chan
ges
inex
pres
sion
NC
AA
AS
18U
tero
glob
inpr
ecu
rsor
Scgb
1a1
P17
559
0.14
53.
830
0.50
210
.4/4
.97/
25.0
0%19
N-a
cety
lneu
ram
inic
acid
syn
thas
eN
ans
B1W
C26
0.28
12.
049
1.14
740
.0/6
.49/
17.8
3%20
Bif
un
ctio
nal
puri
ne
bios
ynth
esis
prot
ein
PU
RH
Ati
cO
3556
70
f—
f1.
623
64.2
/6.7
5/6.
42%
21C
reat
ine
kin
ase
B-t
ype
Ckb
P07
335
0f
—f
1.87
142
.7/5
.42/
4.46
%22
Car
bon
ican
hydr
ase
2C
a2P
2713
90.
227
3.43
61.
031
29.1
/6.9
32/5
0.38
%23
22kD
apr
otei
n—
—0.
129
5.82
31.
782
—5/
22.1
2%
24A
dvan
ced
glyc
osyl
atio
nen
dpr
odu
ct-s
peci
fic
rece
ptor
cA
ger
Q63
495
0.09
53.
334
1.03
542
.7/5
.825
/23.
38%
25Si
mila
rto
prot
easo
me
26S
AT
Pase
subu
nit
6Ps
mc6
Q32
PW
90
f—
f1.
152
45.8
/7.6
17/2
7.79
%26
Cofi
lin-1
Cfl
1P
4559
20f
—f
0.54
118
.5/8
.295
/78.
92%
27H
eat
shoc
k-re
late
d70
kDa
prot
ein
2H
spa2
P14
659
0.12
42.
798
0.66
069
.6/5
.56/
4.27
%

Evidence-Based Complementary and Alternative Medicine 9
Ta
ble
1:C
onti
nu
ed.
Spot
no.
aP
rote
inn
ame
Gen
esy
mbo
lSw
iss-
Pro
tn
o.E
xpre
ssio
nle
velr
atio
sT
heo
reti
cal
Mr(
kDa)
/PI
Pept
./co
v%
bA
S/N
CA
A/A
SN
A/N
C
Patt
ern
III
ofch
ange
sin
expr
essi
on
NC
AS
AA
NC
AS
AA
28A
nn
exin
A5
An
xa5
P14
668
—h
—h
—h
35.7
/4.9
14/2
3.20
%
Patt
ern
IVof
chan
ges
inex
pres
sion
NC
AS
AA
29Pe
roxi
redo
xin
-6P
rdx6
O35
244
1.24
50.
263
1.01
824
.8/5
.613
/26.
34%
Patt
ern
Vof
chan
ges
inex
pres
sion
NC
AS
AA
30G
amm
a-en
olas
eE
no2
P07
323
0.28
00
g0.
553
47.0
/7.0
2/5.
07%
31P
rote
indi
sulfi
deis
omer
ase
asso
ciat
ed6
Pdi
a6Q
6308
10.
311
0.41
31.
224
48.8
/5.0
20/2
6.07
%
Patt
ern
VI
ofch
ange
sin
expr
essi
onN
CA
S
AA
32M
yotr
oph
inM
tpn
P62
775
—d
2.05
4—
d12
.9/5
.36/
25.4
2%
Th
e32
acu
pun
ctu
re-s
pec
ific
diff
eren
tial
lyex
pres
sed
prot
ein
spot
sin
asth
ma
onse
tca
nbe
divi
ded
into
six
diff
eren
tca
tego
ries
acco
rdin
gto
thei
rex
pres
sion
patt
ern
son
2DE
gels
(NC
:nor
mal
con
trol
,AS:
asth
ma
mod
el,A
A:a
sth
ma
mod
eltr
eate
dw
ith
acu
pun
ctu
re,a
nd
NA
:nor
mal
rats
trea
ted
wit
hac
upu
nct
ure
).Pa
tter
ns
Ian
dII
,pro
tein
sth
atex
hib
ited
eith
erin
crea
sed
orde
crea
sed
leve
lsin
AS
com
pare
dw
ith
NC
that
wer
ere
stor
edto
nor
mal
expr
essi
onle
vels
byac
upu
nct
ure
;Pat
tern
sII
Ian
dIV
,pro
tein
sth
atdi
dn
otex
hib
itch
ange
dle
vels
inA
Sco
mpa
red
wit
hN
Cbu
tdid
exh
ibit
eith
erin
crea
sed
orde
crea
sed
leve
lsaf
ter
acu
pun
ctu
re;
Patt
ern
sV
and
VI,
prot
ein
sth
atex
hib
ited
eith
erin
crea
sed
orde
crea
sed
leve
lsin
AS
com
pare
dw
ith
NC
and
exh
ibit
edsi
mila
rex
pres
sion
patt
ern
saf
ter
acu
pun
ctu
rein
AA
com
pare
dw
ith
NC
.a T
he
spot
nu
mbe
rfr
om2D
Ege
lan
alys
is(F
igu
re3)
;bth
en
um
ber
ofm
atch
ing
pept
ides
(Pep
t.)
and
perc
enta
geof
the
tota
lam
ino
acid
sequ
ence
cove
red
byth
epe
ptid
es(%
Seq.
Cov
)fr
omth
em
ass
map
pin
gex
per
imen
ts;
c prot
ein
spot
24is
actu
ally
the
solu
ble
rece
ptor
for
adva
nce
dgl
ycat
ion
end
prod
uct
s(s
RA
GE
),w
hic
hco
rres
pon
dsto
the
extr
acel
lula
rdo
mai
nof
full-
len
gth
RA
GE
lack
ing
the
cyto
solic
and
tran
smem
bran
edo
mai
ns,
asre
veal
edby
BLA
STan
dve
rifi
edby
wes
tern
blot
anal
ysis
;dsp
otn
otde
tect
edin
gels
from
the
NC
and
NA
sam
ples
;e spot
not
dete
cted
inge
lsfr
omth
eN
Csa
mpl
es;f sp
otn
otde
tect
edin
gels
from
the
AS
sam
ples
;gsp
otn
otde
tect
edin
gels
from
the
AA
sam
ples
;hsp
otde
tect
edon
lyin
the
AA
sam
ples
.

10 Evidence-Based Complementary and Alternative Medicine
Immunesystem
process9%
Other6%
Signaltransduction
10%Oxidationreduction
3%
Cellularprocess
14%
Transport10%
Cellularcomponentorganization
6%
Response tostimulus
4%
Developmentalal process
8%
Metabolicprocess
22%
Cell cycle7%
(a)
TTF-1
CC10
PRDX6S100A11
S100A8
S100A9
ANXA5
RAGECDC42
GDI2
RhoGDI2
RAC2
ANXA6
(b)
Figure 5: Bioinformatic analysis of the acupuncture-specific differentially expressed proteins in asthma onset. (a) Functional classificationof the identified proteins using the PANTHER classification system. Proteins that were differentially expressed following acupuncture wereclassified into diverse functional categories according to biological process. (b) The STRING network of known protein-protein interactionsamong the seven inflammation-related proteins (marked by colored rectangles) regulated by acupuncture. Circle nodes indicate intermediateproteins not detected in the proteomic study (RAC2, RAS-related C3 botulinum substrate 2; GDI2, Rab GDI beta; CDC42, Cell divisioncontrol protein 42 homolog; ANXA6, Annexin A6; TTF-1, Thyroid transcription factor 1). S100A9 (green circle) is an inflammation-relatedprotein regulated by acupuncture, which was determined in our previous study [16]. The network edges represent the predicted functionalassociations, and stronger associations are represented by darker lines.
CC10
S100A8
RhoGDI2
NC
AS
AA
NA
β-actin
(a)
RAGE sRAGE
NC AS AA NA
55 kD50 kD48 kD
β-actin
(b)
0
0.4
0.8
1.2
1.6
2
CC10 S100A8 RhoGDI2 RAGE sRAGE
Rel
ativ
e qu
anti
ty
NC ASAA NA
##
##
##
##
∗∗
#∗∗∗
∗ ∗
(c)
Figure 6: Validation of the expression profiles of five inflammation-related proteins by western blot analysis. (a) A representative westernblot visualizing the expression levels of CC10, S100A8, and RhoGDI2. β-actin was used to demonstrate equal loading. (a) Western blotanalysis using the anti-rat RAGE extracellular domain monoclonal goat antibody demonstrates that the lung homogenate contains threebands that were approximately 48, 50, and 55 kD in size; the 48-kD band corresponds to sRAGE and the 55 and 50 kD bands correspondto full-length RAGE. (b) The densitometric quantification of individual proteins is expressed as the fold change compared to β-actin. Eachbar represents the mean ± SEM of triplicate experiments, and similar results were observed in all experiments. #P < 0.05, ##P < 0.01 whencomparing the AS group with the NC group; ∗P < 0.05, ∗∗P < 0.01 when comparing the AA group with the AS group.
S100 proteins, which are characterized by two EF-handcalcium-binding motifs, have received increased attentionin the study of asthma because of their close associationwith inflammation [24, 25]. We previously reported thatthe increased mRNA expression of S100A9 (also known ascalgranulin B; MRP14), a calcium-binding protein in theS100 protein family, was downregulated to control levels afteracupuncture [16]. In the current study, a similar regulationof the expression of two S100 proteins, S100A8 (also known
as calgranulin A, MRP8) and S100A11 (also known ascalgizzarin, S100C), was observed in acupuncture-treatedOVA-induced asthma onset rats. S100A8 and S100A9 aresmall calcium-binding proteins that are highly expressed inneutrophil and monocyte cytosols and generally form a het-erodimer (S100A8/A9, calprotectin) in a calcium-dependentmanner [25]. Increasing evidence indicates that S100A8and S100A9 are involved in intracellular and extracellularregulatory activities. Within cells, S100A8 and S100A9 play

Evidence-Based Complementary and Alternative Medicine 11
important roles in regulating enzyme activities, cytoskele-ton dynamics, transcription factors, Ca2+ homeostasis, andthe inflammatory response [26]. In addition, S100A8 andS100A9 are secreted into the extracellular space by unknownmechanisms [26, 27]. Secreted S100A8 and S100A9 proteinscan act in a cytokine-like manner as extracellular ligandsfor cell surface receptors, including RAGE, which activatessignaling cascades and initiates cellular responses [27].Furthermore, S100A8 and S100A9 are involved in a novelproinflammatory signaling pathway where they contributeto the activation of central cellular pathways, including p38or p44/42 MAP kinases and NF-κB signaling components,which induce the expression of many proinflammatorymolecules [27, 28]. Elevated levels of S100A8 and S100A9in human asthmatic BALF are strongly linked to allergicinflammation [29]. Moreover, the inhibition of S100A8 andS100A9 reduced the migration of inflammatory cells into thelungs in a mouse model of asthma [30]. These observationssuggest an association between pulmonary inflammationand S100A8 and S100A9. In our studies, the increasedexpression levels of S100A8, S100A9, and S100A11 in asthmaonset in rats were downregulated after acupuncture, whichsuggests that acupuncture had an effect on the regulation ofinflammatory reactions in asthma.
RAGE is a member of the immunoglobulin superfamilyof cell surface receptors. RAGE binds to multiple ligands,including S100 proteins, which leads to the activation ofproinflammatory signaling pathways, such as Cdc42/Rac,MAPK (ERK, p38, and JNK) [27], PI3 K, and Rho/Rho-kinase [31], as well as the up-regulation of RAGE itself.Although RAGE binds many S100 proteins, such as S100B,S100A1, and S100A12, it is unknown if RAGE directlybinds to S100A8, S100A9, or S100A8/A9 heterodimers [32].Recent studies have provided evidence that these interactionsare likely [27, 33, 34] and may explain the similaritiesbetween the expression patterns of RAGE, S100A8 andS100A9 in our study, which were increased in the ASgroup relative to the NC group and were downregulated tocontrol levels after acupuncture in the AA group. Notably,acupuncture simultaneously restored the expression level ofsRAGE, a secretory isoform of RAGE that was expressedat a relatively low level in the AS group. sRAGE lacks thetransmembrane domain found in intact RAGE and acts as anendogenous inhibitor of RAGE by binding circulating ligandsand inhibiting RAGE-induced proinflammatory signaling,tissue damage, and dysfunction [20]. Treatment of animalswith sRAGE can prevent and even reverse RAGE-mediatedpathological processes [31, 35]. Acupuncture could inhibitthe S100 protein/RAGE-mediated inflammatory signalingpathway by downregulating the proteins S100A8, S100A9,and RAGE while upregulating sRAGE expression, whichwould to reverse the inflammatory process of asthma.
Protein CC10 (also known as uteroglobin, and secre-toglobin 1A member 1) is a steroid-inducible, evolutionarilyconserved, secreted protein of the secretoglobin family [36].CC10 is mainly produced from Clara cells, which arenonciliated cells located mainly in the bronchioles, andfunctions as an important anti-inflammatory mediator inthe lung [37]. There is a marked decrease in the synthesis
and secretion of CC10 during LPS-induced acute lunginflammation [38]. Increased levels of IL-4, IL-5, and IL-13 [39] as well as a severe inflammatory response [40] havebeen observed in the lungs of CC10-deficient mice afterallergen challenge, which confirms the functional relevanceof CC10 in allergic inflammation. Treatment with CC10could improve airway conditions where inflammation is partof the pathophysiology [41, 42]. CC10 plays a key role as animportant endogenous regulator that modulates pulmonaryinflammatory reactions. In the present study, acupunctureupregulated CC10 expression, which was decreased in OVA-sensitized/challenged rats relative to normal control rats andindicates an anti-inflammatory effect of acupuncture onasthma. In agreement with the reported functional associa-tions among CC10, S100A8, S100A9, and RAGE in CC10-knockout mice [43], our study showed that the asthma onsetin rats with decreased expression of CC10 overexpressedtwo calcium-binding proteins, S100A8 and S100A9, whichwere coupled with increased RAGE expression. These resultssuggest an inflammatory pathway in asthma consistingof CC10, RAGE, S100A8, and S100A9. Acupuncture inasthma appears to exert an anti-inflammatory effect byregulating these inflammation-related proteins and inhibitsthis pathway.
Using the PANTHER classification system, seven ofthe identified proteins (Table Supplemental 2 availableonline at doi:10.1155/2012/850512) were classified as beinginvolved in signal transduction processes, which includecell-cell signaling, S100 protein/RAGE signaling, and Rho(Rho GTPase proteins)/Rho-kinase signaling. The Rho/Rho-kinase-mediated signaling pathway plays a crucial role inseveral pathophysiological processes of asthma, includingairway smooth muscle contraction, airway remodeling,and airway inflammation [44]. Inactivation of Rho/Rho-kinase signaling could inhibit the infiltration of airways byinflammatory cells and airway hyperresponsiveness inducedby allergen challenge [45]. Several compounds, such asY-27632 and fasudil, have been developed to prevent orblock the inflammatory response in asthma by inhibitingthe Rho/Rho-kinase signaling pathway [44, 46]. RhoGDI2plays a role in the regulation of Rho/Rho-kinase signaling bynegatively regulating the biological function of Rho GTPases[47]. In contrast, RhoGDIs may act as positive regulatorsrequired for the correct targeting and regulation of RhoGTPases [48]. In the asthmatic lung proteome, significantlyincreased RhoGDI2 expression was downregulated afteracupuncture, indicating an association between Rho/Rho-kinase signaling and the antiasthma effect of acupuncture;however, the precise role of RhoGDI2 in the Rho/Rho-kinase-mediated signaling pathway is not clear. Furtherstudies of RhoGDI2 and the effects on Rho/Rho-kinasesignaling will determine if RhoGDI2 is a novel therapeutictarget for asthma.
We also detected decreased expression of PRDX6 andincreased expression of ANXA5 in the acupuncture-treatedmodel; however, these two proteins did not exhibit alteredexpression in asthma onset in rats when compared with thecontrols. ANXA5 is a member of the annexins superfamily ofcalcium- and phospholipid-binding, which have been linked

12 Evidence-Based Complementary and Alternative Medicine
RhoGEF
Acute and chronic inflammation
Innate immune response
Other pathological response
Cytosol
Nuclues
RAGE
Stimulatory modificationInhibitory modification
CC10 2-DE and western blottingidentified proteins
CC10 S100A8/A9
RhoGDI2
AP-1 NF-κB
sRAGE
Rho kinase
GAP
Rho inact Rho act.
Figure 7: A possible inflammatory signaling pathway that results from the functional associations of the identified inflammation-relatedproteins (marked with an underline), which is regulated by acupuncture in asthma. Acupuncture can downregulate the proteins S100A8,S100A9, RAGE, and RhoGDI2 and upregulate the expression of CC10 and sRAGE. This pathway may explain the anti-inflammatory effectof acupuncture in asthma. Rho inact, inactivated Rho GTPase; Rho act, activated Rho GTPase; RhoGEF, Rho-specific guanine nucleotideexchange factors; GAP, GTPase-activating proteins; NF-κB, nuclear factor-κB; AP1, activator protein-1.
to fibrinolysis, coagulation, apoptosis, and inflammation[49]. The anti-inflammatory properties of ANXA5 affect thefunctional consequences of inflammation in the vessel wall[50]. PRDX6 is a novel antioxidant enzyme that is highlyexpressed in the lung and plays an important role in thedefense against oxidative lung damage [51]. Deregulations ofANXA5 and PRDX6 suggest a regulatory effect of acupunc-ture on pulmonary inflammation and oxidative stress.
Airway inflammation is the dominant pathophysiologi-cal process in the natural course of asthma [1]. We previ-ously reported a proinflammatory process during the earlyasthmatic response, and calcium binding played a centralrole in this process [18]. In this study, several inflammation-related proteins were regulated in the lungs of rats treatedwith acupuncture, including downregulated proinflamma-tory proteins and upregulated anti-inflammatory proteins.The functional association of these deregulated proteinssuggests an inflammatory signaling pathway that might playa crucial role in the inflammatory reactions of asthma(Figure 7). In this pathway, the low level of CC10 likelystimulates the production of S100A8 and S100A9, whichactivates the S100 protein/RAGE-mediated proinflammatorysignaling pathway in the lungs of asthmatic rats. The bindingof RAGE to its S100 ligands provides a channel for thetransduction of inflammatory signals into the cell, whichfurther activates the intracellular Rho/Rho-kinase signalingpathway mediates the activation and nuclear translocationof transcription factors, such as nuclear factor (NF)-κB
and activator protein (AP)-1, and eventually leads tothe inception of the early airway inflammatory process.Acupuncture can systematically regulate this inflammatorysignaling pathway at different levels through the regulation ofseveral key nodal proteins, including CC10, S100A8, S100A9,RAGE, sRAGE, and RhoGDI2 (Figure 7), which may explain,at least in part, the anti-inflammatory effect of acupuncturein asthma.
In summary, this paper is the first to report the use ofa proteomic approach to analyze the protein profile of anasthma model treated with acupuncture. Our results indicatethat acupuncture downregulates the expression of proin-flammatory proteins (e.g., S100A8, RAGE, and S100A11)and upregulates the expression of anti-inflammatory pro-teins (e.g., CC10, ANXA5, and sRAGE) in the lung tissuesof rats with asthma onset. Characterizing the balance andinteraction between these inflammation-related proteinsmay contribute to a better understanding of the molec-ular mechanisms that underlie the antiasthmatic effect ofacupuncture. Moreover, further functional investigations ofthese acupuncture-specific effector proteins could identifynew drug candidates for the prophylaxis and treatment ofasthma.
Conflict of Interests
The authors have declared that no competing interests exist.

Evidence-Based Complementary and Alternative Medicine 13
Acknowledgments
This work was supported by the National Natural ScienceFoundation of China (no. 81173332, 30873299, 81001548,81173341, and 81202753), the Innovation Program ofShanghai Municipal Education Commission (09ZZ128), theShanghai Leading Academic Discipline Project (S30304),Shanghai Municipal Education Commission budget item(2011JW49), and the Key Program of State Administrationof Traditional Chinese Medicine of China.
References
[1] Global Initiative for Asthma (GINA), GINA Report, GlobalStrategy for Asthma Management and Prevention, 2010,http://www.ginasthma.org.
[2] K. Bahadori, M. M. Doyle-Waters, C. Marra et al., “Economicburden of asthma: a systematic review,” BMC PulmonaryMedicine, vol. 9, article 24, 2009.
[3] C. Fang, C. J. Corrigan, and S. Ying, “The treatment targetsof asthma: from laboratory to clinic,” Inflammation & AllergyDrug Targets, vol. 7, no. 2, pp. 119–128, 2008.
[4] P. J. Barnes, “New therapies for asthma: is there any progress?”Trends in Pharmacological Sciences, vol. 31, no. 7, pp. 335–343,2010.
[5] L. A. Marino and J. Shen, “Characteristics of complementaryand alternative medicine use among adults with currentasthma, 2006,” Journal of Asthma, vol. 47, no. 5, pp. 521–525,2010.
[6] “Use of acupuncture in modern health care,” WHO Chron, vol.280, no. 7-8, pp. 294–301, 1980.
[7] “NIH consensus conference. acupuncture,” JAMA, vol. 280,no. 17, pp. 1518–1524, 1998.
[8] Y. Q. Yang, H. P. Chen, Y. Wang, L. M. Yin, Y. D. Xu, and J.Ran, “Considerations for use of acupuncture as supplementaltherapy for patients with allergic asthma,” Clinical Reviews inAllergy and Immunology. In press.
[9] S. Joos, C. Schott, H. Zou, V. Daniel, and E. Martin, “Immu-nomodulatory effects of acupuncture in the treatment ofallergic asthma: a randomized controlled study,” Journal ofAlternative and Complementary Medicine, vol. 6, no. 6, pp.519–525, 2000.
[10] E. R. Carneiro, R. A. N. Xavier, M. A. P. D. Castro, C. M.O. D. Nascimento, and V. L. F. Silveira, “Electroacupuncturepromotes a decrease in inflammatory response associatedwith Th1/Th2 cytokines, nitric oxide and leukotriene B4modulation in experimental asthma,” Cytokine, vol. 50, no. 3,pp. 335–340, 2010.
[11] E. R. Carneiro, C. R. W. Carneiro, M. A. P. De Castro, Y.Yamamura, and V. L. F. Silveira, “Effect of electroacupunctureon bronchial asthma induced by ovalbumin in rats,” Journalof Alternative and Complementary Medicine, vol. 11, no. 1, pp.127–134, 2005.
[12] F. J. Zijlstra, I. Van Den Berg-De Lange, F. J. P. M. Huygen,and J. Klein, “Anti-inflammatory actions of acupuncture,”Mediators of Inflammation, vol. 12, no. 2, pp. 59–69, 2003.
[13] H. J. Sung, Y. S. Kim, I. S. Kim et al., “Proteomic analysisof differential protein expression in neuropathic pain andelectroacupuncture treatment models,” Proteomics, vol. 4, no.9, pp. 2805–2813, 2004.
[14] S. Jeon, J. K. Youn, S. T. Kim et al., “Proteomic analysis of theneuroprotective mechanisms of acupuncture treatment in a
Parkinson’s disease mouse model,” Proteomics, vol. 8, no. 22,pp. 4822–4832, 2008.
[15] W. J. Li, S. Q. Pan, Y. S. Zeng et al., “Identificationof acupuncture-specific proteins in the process of electro-acupuncture after spinal cord injury,” Neuroscience Research,vol. 67, no. 4, pp. 307–316, 2010.
[16] L. M. Yin, G. H. Jiang, Y. Wang et al., “Use of serial analysisof gene expression to reveal the specific regulation of geneexpression profile in asthmatic rats treated by acupuncture,”Journal of Biomedical Science, vol. 16, no. 1, article 46, 2009.
[17] L. M. Yin, G. H. Jiang, Y. Wang et al., “Serial analysis of geneexpression in a rat lung model of asthma,” Respirology, vol. 13,no. 7, pp. 972–982, 2008.
[18] Y. D. Xu, J. M. Cui, Y. Wang et al., “The early asthmaticresponse is associated with glycolysis, calcium binding andmitochondria activity as revealed by proteomic analysis inrats,” Respiratory Research, vol. 11, article 107, 2010.
[19] L. J. Jensen, M. Kuhn, M. Stark et al., “STRING 8—a globalview on proteins and their functional interactions in 630organisms,” Nucleic Acids Research, vol. 37, no. 1, pp. D412–D416, 2009.
[20] H. Maillard-Lefebvre, E. Boulanger, M. Daroux, C. Gaxatte, B.I. Hudson, and M. Lambert, “Soluble receptor for advancedglycation end products: a new biomarker in diagnosis andprognosis of chronic inflammatory diseases,” Rheumatology,vol. 48, no. 10, pp. 1190–1196, 2009.
[21] T. Uchida, M. Shirasawa, L. B. Ware et al., “Receptor foradvanced glycation end-products is a marker of type I cellinjury in acute lung injury,” American Journal of Respiratoryand Critical Care Medicine, vol. 173, no. 9, pp. 1008–1015,2006.
[22] T. C. Medici, E. Grebski, J. Wu, G. Hinz, and B. Wuthrich,“Acupuncture and bronchial asthma: a long-term randomizedstudy of the effects of real versus sham acupuncture comparedto controls in patients with bronchial asthma,” Journal ofAlternative and Complementary Medicine, vol. 8, no. 6, pp.737–750, 2002.
[23] C. R. Schott and E. Martin, “Controlled trial of acupuncturein the treatment of bronchial asthma,” Focus on Alternative andComplementary Therapies, vol. 6, no. 1, pp. 91–92, 2001.
[24] C. Gebhardt, J. Nemeth, P. Angel, and J. Hess, “S100A8 andS100A9 in inflammation and cancer,” Biochemical Pharmacol-ogy, vol. 72, no. 11, pp. 1622–1631, 2006.
[25] A. J. Halayko and S. Ghavami, “S100A8/A9: a mediator ofsevere asthma pathogenesis and morbidity?” Canadian Journalof Physiology and Pharmacology, vol. 87, no. 10, pp. 743–755,2009.
[26] R. Donato, “Intracellular and extracellular roles of S100proteins,” Microscopy Research and Technique, vol. 60, no. 6,pp. 540–551, 2003.
[27] A. Hermani, B. De Servi, S. Medunjanin, P. A. Tessier, and D.Mayer, “S100A8 and S100A9 activate MAP kinase and NF-κB signaling pathways and trigger translocation of RAGE inhuman prostate cancer cells,” Experimental Cell Research, vol.312, no. 2, pp. 184–197, 2006.
[28] K. Sunahori, M. Yamamura, J. Yamana et al., “The S100A8/A9heterodimer amplifies proinflammatory cytokine productionby macrophages via activation of nuclear factor kappa B andp38 mitogen-activated protein kinase in rheumatoid arthritis,”Arthritis Research and Therapy, vol. 8, no. 3, article R69, 2006.
[29] J. Wu, M. Kobayashi, E. A. Sousa et al., “Differential pro-teomic analysis of bronchoalveolar lavage fluid in asthmaticsfollowing segmental antigen challenge,” Molecular and CellularProteomics, vol. 4, no. 9, pp. 1251–1264, 2005.

14 Evidence-Based Complementary and Alternative Medicine
[30] K. J. Greenlee, D. B. Corry, D. A. Engler et al., “Proteomic iden-tification of in vivo substrates for matrix metalloproteinases 2and 9 reveals a mechanism for resolution of inflammation,”Journal of Immunology, vol. 177, no. 10, pp. 7312–7321, 2006.
[31] Y. Chen, S. S. Yan, J. Colgan et al., “Blockade of late stagesof autoimmune diabetes by inhibition of the receptor foradvanced glycation end products,” Journal of Immunology, vol.173, no. 2, pp. 1399–1405, 2004.
[32] E. Leclerc, G. Fritz, S. W. Vetter, and C. W. Heizmann,“Binding of S100 proteins to RAGE: an update,” Biochimicaet Biophysica Acta, vol. 1793, no. 6, pp. 993–1007, 2009.
[33] S. Ghavami, I. Rashedi, B. M. Dattilo et al., “S100A8/A9 at lowconcentration promotes tumor cell growth via RAGE ligationand MAP kinase-dependent pathway,” Journal of LeukocyteBiology, vol. 83, no. 6, pp. 1484–1492, 2008.
[34] J. H. Boyd, B. Kan, H. Roberts, Y. Wang, and K. R. Walley,“S100A8 and S100A9 mediate endotoxin-induced cardiomy-ocyte dysfunction via the receptor for advanced glycation endproducts,” Circulation Research, vol. 102, no. 10, pp. 1239–1246, 2008.
[35] A. M. Karam, L. M. Nayak, and S. M. Lam, “Short-scar purse-string facelift,” Facial Plastic Surgery Clinics of North America,vol. 17, no. 4, pp. 549–556, 2009.
[36] A. B. Mukherjee, Z. Zhang, and B. S. Chilton, “Uteroglobin:a steroid-inducible immunomodulatory protein that foundedthe secretoglobin superfamily,” Endocrine Reviews, vol. 28, no.7, pp. 707–725, 2007.
[37] C. F. Lee, “Thermal breakage of a discrete one-dimensionalstring,” Physical Review E Statistical Nonlinear Soft MatterPhysics, vol. 80, no. 3, part 1, Article ID 031134, 2009.
[38] K. Arsalane, F. Broeckaert, B. Knoops, M. Wiedig, G. Toubeau,and A. Bernard, “Clara cell specific protein (CC16) expres-sion after acute lung inflammation induced by intratracheallipopolysaccharide administration,” American Journal of Res-piratory and Critical Care Medicine, vol. 161, no. 5, pp. 1624–1630, 2000.
[39] S. Z. Wang, C. L. Rosenberger, T. M. Espindola et al., “CCSPmodulates airway dysfunction and host responses in an Ova-challenged mouse model,” American Journal of Physiology, vol.281, no. 5, pp. L1303–L1311, 2001.
[40] L. C. Chen, Z. Zhang, A. C. Myers, and S. K. Huang, “Cuttingedge: altered pulmonary eosinophilic inflammation in micedeficient for clara cell secretory 10-kDa protein,” Journal ofImmunology, vol. 167, no. 6, pp. 3025–3028, 2001.
[41] C. R. Levine, I. H. Gewolb, K. Allen et al., “Safety, phar-macokinetics, and anti-inflammatory effects of intratrachealrecombinant human Clara cell protein in premature infantswith respiratory distress syndrome,” Pediatric Research, vol. 58,no. 1, pp. 15–21, 2005.
[42] T. L. Miller, B. N. Shashikant, A. L. Pilon, R. A. Pierce, T.H. Shaffer, and M. R. Wolfson, “Effects of an intratracheallydelivered anti-inflammatory protein (rhCC10) on physiolog-ical and lung structural indices in a juvenile model of acutelung injury,” Biology of the Neonate, vol. 89, no. 3, pp. 159–170,2006.
[43] A. Saha, Y. C. Lee, Z. Zhang, G. Chandra, S. B. Su, andA. B. Mukherjee, “Lack of an endogenous anti-inflammatoryprotein in mice enhances colonization of B16F10 melanomacells in the lungs,” Journal of Biological Chemistry, vol. 285, no.14, pp. 10822–10831, 2010.
[44] D. Schaafsma, R. Gosens, J. Zaagsma, A. J. Halayko, andH. Meurs, “Rho kinase inhibitors: a novel therapeuticalintervention in asthma?” European Journal of Pharmacology,vol. 585, no. 2-3, pp. 398–406, 2008.
[45] F. Taki, H. Kume, T. Kobayashi, H. Ohta, H. Aratake,and K. Shimokata, “Effects of Rho-kinase inactivation oneosinophilia and hyper-reactivity in murine airways by aller-gen challenges,” Clinical and Experimental Allergy, vol. 37, no.4, pp. 599–607, 2007.
[46] D. Schaafsma, I. S. T. Bos, A. B. Zuidhof, J. Zaagsma, and H.Meurs, “The inhaled Rho kinase inhibitor Y-27632 protectsagainst allergen-induced acute bronchoconstriction, airwayhyperresponsiveness, and inflammation,” American Journal ofPhysiology, vol. 295, no. 1, pp. L214–L219, 2008.
[47] H. J. Cho, K. E. Baek, and J. Yoo, “RhoGDI2 as a therapeutictarget in cancer,” Expert Opinion on Therapeutic Targets, vol.14, no. 1, pp. 67–75, 2010.
[48] H. Zhang, S. Tasaka, Y. Shiraishi et al., “Role of solublereceptor for advanced glycation end products on endotoxin-induced lung injury,” American Journal of Respiratory andCritical Care Medicine, vol. 178, no. 4, pp. 356–362, 2008.
[49] V. Gerke and S. E. Moss, “Annexins: from structure tofunction,” Physiological Reviews, vol. 82, no. 2, pp. 331–371,2002.
[50] M. M. Ewing, M. de Vries, M. Nordzell et al., “AnnexinA5 reduces inflammation mediated vascular remodellingand post-interventional atherosclerosis and improves vascularfunction in hypercholesterolemic mice,” Circulation, vol. 120,no. 18, pp. S1113–S1113, 2009.
[51] Y. Wang, S. A. Phelan, Y. Manevich, S. I. Feinstein, and A. B.Fisher, “Transgenic mice overexpressing peroxiredoxin 6 showincreased resistance to lung injury in hyperoxia,” AmericanJournal of Respiratory Cell and Molecular Biology, vol. 34, no.4, pp. 481–486, 2006.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com