Embed Size (px)
Citation preview

Research Methodology and Biostatistics
Introductory Course Workshop 4-6 March, 2005
Anita Das MBBS, MPHPharmasri www.pharmasri.com

Clinical Research Protocol1. What is a protocol? Definition2. Why a protocol? Can’t we do without
it?3. How to write a protocol? Protocol
development
Pharmasri www.pharmasri.com

Protocol is essentially….a written plan of the study
Well known devices for seeking grant fundsVital scientific function: help organise
research in a logical, focused & efficient way
Pharmasri www.pharmasri.com

Protocol definedICH GCP 1.49A document that describes the objective(s),
design, methodology, statistical considerations and organization of a trial.
All research should be conducted according to a written, clear, comprehensive and consistent protocol.
Pharmasri www.pharmasri.com

Example of Research ProtocolTitle of ProjectStatement of ProblemRelevance of problemLiterature reviewStatement of ObjectivesOutcome variablesStatement of research hypothesis
Health Research Methodology: A Guide for Training for Research Methods, WHO 2001Pharmasri www.pharmasri.com

Research MethodologySummaryResearch Design – Research strategies &
settingSamplingUse of controlsStudy instrumentsShort description of plans for data
collectionAnalysis and interpretation plan
Health Research Methodology: A Guide for Training for Research Methods, WHO 2001Pharmasri www.pharmasri.com

More Examples1. TITLE PAGE2. INVESTIGATORS AND STUDY
ORGANISATION3. SIGNATURE PAGE4. SYNOPSIS5. TABLE OF CONTENTS6. LIST OF ABBREVIATIONS7. GLOSSARY OF TERMS8. INTRODUCTION and BACKGROUND9. OBJECTIVES
ICH E6: Good Clinical Practice, Chapter 6 Pharmasri www.pharmasri.com

10. STUDY DESIGN11. STUDY POPULATION & SUBJECTS12. STUDY TREATMENT13. ASSESSMENT OF EFFICACY14. ASSESSMENT OF SAFETY & AE 15. CLINICAL ECONOMICS16. STUDY CONDUCT17. DATA MANAGEMENT18. STATISTICAL METHODS19. ETHICS & REGULATORTY20. ADMINISTRATIVE MATTERS21. REFERENCES22. APPENDIX
ICH E6: Good Clinical Practice, Chapter 6 Pharmasri www.pharmasri.com

2. Why a protocol? Can’t we do without it?
Why is a written, clear, comprehensive and consistent protocol so important to research?
1. Justification: justify the research2. Evaluation: basis for reviewing the research3. Specification: basis for agreement4. Blueprint: basis for planning &
implementation
Pharmasri www.pharmasri.com

1. JustificationAll research requires justification. The protocol is testimony to the fact that
the investigators have sufficiently thought through the proposed research concerning its justification, scientific quality and ethical propriety.
Pharmasri www.pharmasri.com

ICH GCP on trial justification
2.2 Before a trial is initiated, foreseeable risks and inconveniences should be weighed against the anticipated benefit for the individual subject and society. A trial should be initiated and continued only if the anticipated benefits justify the risks.
2.4 The available non clinical and clinical information on an investigational product should be adequate to support the proposed clinical trial.
These are summarized in rationale section of protocol.
Pharmasri www.pharmasri.com

2. EvaluationAll research requires review by both
external and internal parties.The protocol provides the basis for review.
Who might want to review a protocol?
Pharmasri www.pharmasri.com

Protocol reviewers
#. Who? Uses of protocol External 1. Funder/Sponsor Show research merit and utility, and researcher
capability. 2. Scientific community Show research is scientifically sound; hence
publishable. 3. Ethics committee Show ethical propriety 4. Regulatory agency Show compliance with applicable regulation
and laws. 5. Marketing authority Show validity of research results Internal 6. Co-investigators Secure collaboration 7. Internal QC Ensure protocol comply with GCP, regulation,
internal SOP. 8. Each key participant Ensure protocol is sufficient, clear and
consistent to each; ensure protocol a true reflection of practice.
Pharmasri www.pharmasri.com

3. Specificationbasis for agreement
All research requires collaboration. A protocol specifies how the research is to
be conducted by all parties involved.1. Contract between sponsor and
investigator on how the research is to be conducted. (Hence you sign and date a protocol.)
2. Agreement among investigators on uniform way to conduct a research.
Pharmasri www.pharmasri.com

4. Blueprint
All protocol eventually has to be operationalised to become actual research.
A protocol provides the basis for planning and implementing the research.
Pharmasri www.pharmasri.com

People involvedMany professions are involved in Implementation:
1.CRA CRF development and data collection mechanism,
monitoring convention.2.CDM
data definition, database development, query generation
3.Site coordinator site management, data collection, specimen/material
handling etc4.Statistician
randomisation, data monitoring, analysis5.Investigator
techniques, schedule6.Reference centres
techniques, schedule.Pharmasri www.pharmasri.com

3. How to write a protocol? Protocol development
A protocol is a joint product of the different professions involved
The best way to write an impressive protocol is to “copy” another one.
Must have SOP and follow guideline.
Pharmasri www.pharmasri.com

Protocol development- 1
1. TITLE PAGEProtocol #AuthorProtocol DateAmendment # and DateAuthor’s and Reviewer’s signature and date
2. INVESTIGATORS & ORGANISATIONPrincipal and co-InvestigatorsSponsor and Research organisationReference centres, Study Committees etc
Pharmasri www.pharmasri.com

Protocol development- 2
3. SIGNATURE PAGE4. SYNOPSIS5. TABLE OF CONTENTS6. LIST OF ABBREVIATIONS7. GLOSSARY OF TERMSDefinition of common and technical terms
Pharmasri www.pharmasri.com

Protocol development- 3
8. INTRODUCTION and BACKGROUNDLiterature reviewRationale and motivational background
justifying the proposed research Make reference to Investigator’s brochure
for details
Pharmasri www.pharmasri.com

Protocol development- 4
9. OBJECTIVESA. Primary question: the major question the
investigators are most interested in.B. Secondary or subsidiary questions : relate to subsidiary end points.relate to subgroup hypotheses eg other than
overall contrast between each arm of trial.C. Ancillary questions: questions that do not
bear directly on the intervention being tested but which are nevertheless of interest; eg. natural history of disease in the control group, risk factor analysis.Pharmasri www.pharmasri.com

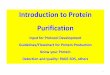
Protocol development- 5
10. STUDY DESIGNStudy design, # patients & DurationSchematic diagram of study design
Discussion of study design: Justify decision
Screen Baseline Randomise Rx
Wash-in/out End
Rx group
Control group
Pharmasri www.pharmasri.com

Protocol development- 6
11. STUDY POPULATION AND SUBJECTSInclusion criteriaExclusion criteriaSubject withdrawal & Drop-outScreening failures
Pharmasri www.pharmasri.com

Protocol development- 7
12. STUDY TREATMENTStudy DrugDosage and AdministrationConcomitant Medication/TreatmentTreatment Allocation and RandomisationBlinding & Emergency Unblinding proceduresAssessment of complianceInvestigational product handling
Pharmasri www.pharmasri.com

Protocol development- 8
13. ASSESSMENT OF EFFICACYSpecify efficacy parameterPrimary end-point(s): Rx effect for primary
objectiveSecondary end-point(s): supportive measures
related to Rx effect for secondary objectiveGlobal assessment variable: overall safety,
treatment effect and usefulness; requires judgement.
Surrogate variable: predictor of clinical benefitSpecify methods for assessing & recordingSpecify who and when assessed.
Pharmasri www.pharmasri.com

Protocol development- 9
14. ASSESSMENT OF SAFETY & AE Eliciting, Documenting and Reporting
Adverse EventsAssessment of Severity & CausalityFollow-up and Assessment of OutcomeSerious Adverse EventsTreatment of Adverse EventOverdosage & PregnancyBreaking the Study Blind
Pharmasri www.pharmasri.com

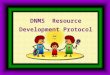
Protocol development- 10
15. CLINICAL ECONOMICS16. STUDY CONDUCTStudy procedures and FlowchartDetailed description of stages and visitsSample handling and Analysis
Pharmasri www.pharmasri.com

Screening
Baseline PCI In hospital
Follow up
Follow up
Final visit
Visit 1 2 3 3 4 5 6
Timeline (month) -4 -1 0 12-24 hrs
1 3 6
Procedures
Check eligibility X
Screening Coronary angiogram X*
Written informed consent X
Medical History X
Vital sign X
Blood sample for Hematology (10 ml)
X
Blood sample for Chemistry X
Randomization to treatment X
Blood sample for CK X X X X** X** X**
ECG X X X** X** X**
Efficacy assessment X X X X X
QCA X X** X** X** X
Report AE and SAE X X X
Complete CRF X X X X X X X
Flowchart
Pharmasri www.pharmasri.com

Protocol development- 12
18. STATISTICAL METHODSSample size and power considerationsRandomisationEnd-pointsAnalysis setsFinal analysisPlanned Interim analysis
Pharmasri www.pharmasri.com

Protocol development- 13
19. ETHICS & REGULATORTY CONSIDERATIONSInstitutional Review Board/Ethics CommitteesEthical conduct of the studySubject information and ConsentPatient protection procedures
Pharmasri www.pharmasri.com

Protocol development- 14
20. ADMINISTRATIVE MATTERSStudy documentation, CRF and Record
keepingFinance and InsuranceStudy TerminationConfidentiality and Publication policy
21. REFERENCES
Pharmasri www.pharmasri.com

Protocol development- 15
22. APPENDIXA. DECLARATION OF HELSINKIB. STUDY PROCEDURESC. QUESTIONNAIRE and CRFD. INVESTIGATIONAL PRODUCT LABELSE. ELEMENTS OF INFORMED CONSENTF. SAMPLE INFORMED CONSENT FORMG. PATIENT INFORMATION SHEETH. LETTER OF INDEMNITYI. INVESTIGATORS’ CURRICULUM VITAE
Pharmasri www.pharmasri.com

Case 1: To blind or not to blind
This is a multi-center, open label, parallel group randomized trial designed to demonstrate the equivalence of Staysafe/ANDY-disc® with the standard treatment Ultrabag® for a treatment period of 12 months. 260 patients on CAPD from 5 participating sites who meet inclusion/exclusion criteria will be enrolled into the trial. The primary efficacy variable is the incidence of peritonitis, and secondary efficacy variables are technique failure and technical problem encountered in using the products under investigation.
The investigational products here are Staysafe/ANDY-disc® and Ultrabag®. The nature of the treatment (CAPD) and the 2 products are such that it is not possible to blind study site personnel, study subjects, monitor, data management and sponsor personnel to the assigned treatment.
Questions for discussiona) What is at stake in the above situation?b) Why is the issue not a trivial matter?c) What would be your advice?
Pharmasri www.pharmasri.com

Case 2: Sample size is not always what it seems
For the above trial, the investigators intended to enroll 260 patients from 5 centres. Section 16.1 of the protocol on Sample size and power considerations reads as follows:
“Sample size was estimated based on the primary efficacy parameter, which is incidence of peritonitis rate. Based on literature data and our practice, an estimate of the incidence of peritonitis rate on CAPD is 0.05 episodes per patient month. We accept as equivalent 25% difference (delta) in risk of peritonitis at 1 year. For a power of 0.8 and alpha of 0.05 (one sided), the required sample size is 264 patients in each treatment groups followed-up for 1 year. No allowance is made for drop out.”
Questions for discussionDo you accept the statistician’s calculation above?Pharmasri www.pharmasri.com

Case 3: P value and p value
A trial was designed to compare the effect of a new
drug A, the standard drug B and placebo P. The p value for
treatment effect of A versus P was 0.001, for B versus P was 0.02 and for A versus B was 0.45.
Questions for discussiona) What is your take on the above results?b) Drug A is efficacious?c) Drug B is also efficacious?d) There is no difference in treatment effect between
drugs A and B in that study?e) However, since the p value for A vs P is much smaller
than p value of B vs P, A is likely to be more efficacious than B, though of course the study did not show that?
Pharmasri www.pharmasri.com

Case 4: It is not always possible to trialSmoking is suspected to increase the risk of certain indolent benign cancer (patients with the cancer don’t die quickly). The best design is to randomise subjects to smoking or non-smoking, then follow them up for many years to determine occurrence of the cancer. This is clearly not ethically acceptable, even if one could afford to do the trial. Questions for discussionTo address the above question, discuss the following design options:
a.Study a large group of smokers to determine how many of them have the cancer. If the incidence is higher than generally expected, we may conclude that smoking increases the risk of the cancer.
b. We can also follow up a group of smokers and a control group of non-smokers. If the incidence is higher among smokers than non-smokers, we may conclude that smoking increases the risk of the cancer
c. We can also assemble a group of patients with the cancer and a control group without cancer. If the proportion of smokers is higher among cancer group than non-cancer group, we may conclude that smoking increases the risk of the cancerPharmasri www.pharmasri.com

ReferencesFundamentals of Clinical Trials
by Lawrence M. Friedman, Curt Furberg, David L. Demets. Springer-Verlag; 3rd edition (November 1, 1998)
Health Research Methodology: A Guide for Training for Research Methods, WHO 2001. WHO Publications (Western Pacific Regional Office)
Good Clinical Practice, Chapter 6. International Committee on Harmonization E. http://www.ich.org
Pharmasri www.pharmasri.com