Embed Size (px)
Citation preview

1Gut Month 2021 Vol 0 No 0
Proton- pump inhibitor use is not associated with severe COVID- 19- related outcomes: a propensity score- weighted analysis of a national veteran cohort
We read with interest the study by Lee et al.1 The authors conducted a propensity score (PS)- matched analysis of a national South Korean cohort evaluating the associ-ation between proton pump inhibitor (PPI) use and SARS- CoV- 2 susceptibility (primary outcome) and COVID- 19 clinical severity (secondary outcome). Between January and May 2020, 4785 patients tested positive for SARS- CoV- 2 (3.6% positivity); 267 current PPI users and 148 former PPI users were 1:1 PS- matched to non- users for the secondary outcomes. The authors reported current PPI use versus non- use was associated with a statistically significant increased risk of the composite endpoints: (1) oxygen therapy, intensive care unit (ICU) admission, mechan-ical ventilation use or death (composite OR 1.63; 95% CI, 1.03–2.53); and (2) ICU admission, mechanical ventilation or death (composite OR 1.79; 95% CI, 1.30 to 3.10).
We assembled a national retrospective cohort of US veterans who tested positive for SARS- CoV- 2 (index date). Current outpa-tient PPI use up to and including the index date (primary exposure) was compared with non- use, defined as no PPI prescrip-tion fill in the 365 days prior to the index date (online supplemental figure 1). The primary composite outcome was mechanical ventilation use or death within 60 days; the secondary composite outcome also included hospital or ICU admission. In contrast to PS matching, PS weighting allowed inclusion of all patients. Weighted logistic regres-sion models evaluated severe COVID- 19 outcomes between current PPI users versus non- users.
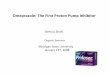
Our analytic cohort included 97 674 veterans with SARS- CoV- 2 testing, of whom 14 958 (15.3%) tested positive (6262 (41.9%) current PPI users, 8696 (58.1%) non- users). In the unweighted cohort, current PPI users were older, more often current or former smokers, and had more comorbidities than non- users. After weighting, all covariates were balanced (table 1, online supplemental figure 2). In the unweighted cohort, we observed higher odds of the primary (9.3% vs 7.5%; OR 1.27; 95% CI, 1.13- 1.43) and secondary (25.8% vs 21.4%; OR 1.27; 95% CI, 1.18- 1.37) composite outcomes among PPI users versus non- users (figure 1, online supplemental table 1). After PS weighting,
Letter
Table 1 Characteristics of veterans with positive SARS- CoV- 2 testing, stratified by current PPI user versus PPI non- user
Covariates
Unweighted cohort of veterans with positive SARS- CoV- 2 test
Weighted cohort of veterans with positive SARS- CoV- 2 test
PPI non- users(n=8696)
Current PPI users(n=6262)
PPI non- users (n=8696)
Current PPI users(n=6262) SMD†
VHA facility‡ ‡ ‡ ‡ ‡ 0.070
Age, mean years (SD) 60.46 (15.77) 64.37 (13.42) 61.94 (15.14) 62.15 (14.52) 0.014
Male sex, n (%) 7382 (84.9) 5578 (89.1) 7529 (86.6) 5441 (86.9) 0.009
Race/ethnicity, n (%) 0.033
Non- Hispanic white 4437 (51.0) 3885 (62.0) 4757 (54.7) 3527 (56.3)
Non- Hispanic black 2243 (25.8) 1315 (21.0) 2125 (24.4) 1477 (23.6)
Non- Hispanic other or unknown
794 (9.1) 515 (8.2) 764 (8.8) 540 (8.6)
Hispanic 1222 (14.1) 547 (8.7) 1049 (12.1) 717 (11.5)
Days from 1 January 2020 to index date, mean (SD)*
282 (82.8) 289 (78.7) 285 (81.5) 285 (81.2) 0.005
Smoking status, n (%) 0.067
Current smoker 1030 (11.8) 754 (12.0) 1047 (12.0) 762 (12.2)
Former smoker 3441 (39.6) 3085 (49.3) 3773 (43.4) 2780 (44.4)
Never smoker 3430 (39.4) 2180 (34.8) 3260 (37.5) 2376 (37.9)
Unknown 795 (9.1) 243 (3.9) 616 (7.1) 344 (5.5)
Comorbidities, n (%)
Asthma 629 (7.2) 685 (10.9) 747 (8.6) 571 (9.1) 0.018
Coronary artery disease 1645 (18.9) 1911 (30.5) 2034 (23.4) 1500 (24.0) 0.013
Cancer 1770 (20.4) 1750 (27.9) 2020 (23.2) 1508 (24.1) 0.020
Cardiomyopathy 255 (2.9) 279 (4.5) 309 (3.5) 228 (3.6) 0.005
Charlson comorbidity index, mean (SD)
1.82 (2.22) 2.55 (2.54) 2.12 (2.38) 2.17 (2.40) 0.022
Congestive heart failure 621 (7.1) 746 (11.9) 791 (9.1) 582 (9.3) 0.007
Chronic lung disease 2652 (30.5) 2757 (44.0) 3129 (36.0) 2315 (37.0) 0.020
Chronic neuromuscular disease
394 (4.5) 323 (5.2) 420 (4.8) 308 (4.9) 0.004
Chronic kidney disease 1161 (13.4) 1219 (19.5) 1390 (16.0) 1026 (16.4) 0.011
Chronic kidney failure 153 (1.8) 151 (2.4) 180 (2.1) 130 (2.1) 0.001
Chronic obstructive pulmonary disease
1316 (15.1) 1646 (26.3) 1694 (19.5) 1270 (20.3) 0.020
Cerebrovascular disease 2800 (32.2) 2966 (47.4) 3320 (38.2) 2453 (39.2) 0.021
Diabetes 3070 (35.3) 2815 (45.0) 3415 (39.3) 2469 (39.4) 0.003
Drug dependency 379 (4.4) 345 (5.5) 416 (4.8) 311 (5.0) 0.008
Emphysema 126 (1.4) 170 (2.7) 171 (2.0) 126 (2.0) 0.003
Heart disease 2093 (24.1) 2281 (36.4) 2533 (29.1) 1846 (29.5) 0.008
Heart failure (non- congestive)
790 (9.1) 898 (14.3) 988 (11.4) 709 (11.3) 0.001
Helicobacter pylori positive
1841 (21.2) 1138 (18.2) 1746 (20.1) 1232 (19.7) 0.022
HIV 120 (1.4) 51 (0.8) 105 (1.2) 78 (1.2) 0.003
Hypertension 5075 (58.4) 4620 (73.8) 5616 (64.6) 4149 (66.3) 0.035
Lower respiratory infection
1010 (11.6) 855 (13.7) 1076 (12.4) 796 (12.7) 0.010
Obstructive sleep apnea 2884 (33.2) 2773 (44.3) 3254 (37.4) 2454 (39.2) 0.037
Medications, n (%)
ACE inhibitors 2233 (25.7) 2152 (34.4) 2549 (29.3) 1887 (30.1) 0.018
ARBs 1170 (13.5) 1239 (19.8) 1378 (15.8) 1036 (16.6) 0.019
H2RAs 626 (7.2) 423 (6.8) 638 (7.3) 459 (7.3) 0.001
NSAIDs 5359 (61.6) 4745 (75.8) 5812 (66.8) 4358 (69.6) 0.059
Statins 4176 (48.0) 4249 (67.9) 4832 (55.6) 3656 (58.4) 0.057
*This variable represents the days from 1 January 2020 to the index date of SARS- CoV- 2 testing to account for temporal differences.†Only SMDs for the weighted cohort are provided in this table. Please refer to online supplemental figure 1 for the SMD plots for both the unweighted and weighted cohorts.‡All of the 127 VHA facilities were included as covariates in this analysis; however, the proportion of patients at each station for each group is not listed here due to space considerations. The SMD between PPI users and non- users in the unweighted cohort was 0.36, with balance achieved after weighting (SMD: 0.07).ACE, angiotensin- converting enzyme; ARBs, angiotensin II receptor blockers; H2Ras, histamine- 2 receptor antagonists; NSAIDs, non- steroidal anti- inflammatory agents; PPI, proton- pump inhibitor; SMD, standardised mean difference; VHA, Veterans Health Administration.
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from

2 Gut Month 2021 Vol 0 No 0
Letter
PPI use versus non- use was not associated with the primary (8.2% vs 8.0%; OR 1.03; 95% CI, 0.911.16) or secondary (23.4% vs 22.9%; OR 1.03; 95% CI, 0.95- 1.12) composite outcomes. There were no signifi-cant interactions between age and PPI use on composite or individual outcomes.
Disparate results are reported in studies analysing COVID- 19- related outcomes among PPI users versus non- users2–6 due to varied PPI exposure definitions; COVID- 19 severity outcomes; covariate assessment and adjustment; study design and populations; contemporaneous treatments; and health-care infrastructure. In our unweighted anal-ysis, we also observed an association between PPI use and severe COVID- 19 outcomes (separately and as composites) which was not demonstrated in the PS- weighted cohort, suggesting that the associations in previous studies might reflect incomplete covariate adjustment.7 Indeed, the low E- values (all <2.0) for the weak associa-tions between PPI exposure and COVID- 19 severity outcomes (although variably defined) that are demonstrated in previous studies suggest incomplete covariate adjust-ment and residual confounding (see online supplemental material).8 Similar to the Lee et al study, prior studies also include data from the first months of the COVID- 19 pandemic, when management and available treatments were rapidly evolving. Lee et al’s outcome definition also included oxygen therapy.
Oxygen administration may not correlate with COVID- 19 severity and may be consid-ered routine protocol, especially early in the pandemic. Similarly, ICU admission may be influenced by health system factors, such as bed availability. Our study was designed to avoid immortal time, lag time and proto-pathic biases, which have been present in some PPI studies (see online supplemental material).9 We further accounted for the pandemic timeframe and clinical manage-ment evolution by considering COVID- 19 prevalence and US geography.
In conclusion, with respect to COVID- 19, our robust PS- weighted analysis provides patients and providers with further evidence for PPI safety.
Shailja Shah ,1,2 Alese Halvorson,3 Brandon McBay,4 Chad Dorn,5 Otis Wilson,6,7 Sony Tuteja,8,9 Kyong- Mi Chang,8,9 Kelly Cho,10,11 Richard Hauger,12,13 Ayako Suzuki,14,15 Christine Hunt,14,15 Edward Siew,7,16 Michael Matheny,5,7,16 Adriana Hung ,6,16 Robert Greevy,3,6 Christianne Roumie6,17,18
1Gastroenterology Section, VA San Diego Healthcare System, San Diego, California, USA2Division of Gastroenterology, University of California, San Diego, California, USA3Department of Biostatistics, Vanderbilt University Medical Center, Nashville, Tennessee, USA4Department of Public Health, Harvard University T H Chan School of Public Health, Boston, Massachusetts, USA5Department of Biomedical Informatics, Vanderbilt University Medical Center, Nashville, Tennessee, USA
6Clinical Services Research and Development, VA Tennessee Valley, Nashville, TN, USA7Health Services Research and Development, VA Tennessee Valley, Nashville, Tennessee, USA8The Corporal Michael J. Crescenz VA Medical Center, Philadelphia, Pennsylvania, USA9University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA10VA Boston Healthcare System, Boston, Massachusetts, USA11Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA12Department of Psychiatry, University of California San Diego, La Jolla, California, USA13Center of Excellence for Stress & Mental Health, VA San Diego Healthcare System, San Diego, California, USA14Division of Gastroenterology, Duke University Medical Center, Durham, North Carolina, USA15Gastroenterology Section, Durham VA Health Care System, Durham, North Carolina, USA16Division of Nephrology & Hypertension, Vanderbilt University Medical Center, Nashville, Tennessee, USA17Department of Medicine, Vanderbilt University Medical Center, Nashville, Tennessee, USA18VA Geriatrics Research Education and Clinical Center (GRECC), VA Tennessee Valley Health System, Nashville, Tennessee, USA
Correspondence to Dr Shailja Shah, Gastroenterology, VA San Diego Healthcare System, La Jolla, CA 92161, USA; s6shah@ health. ucsd. edu
Acknowledgements Jason Denton (in memoriam): We would like to acknowledge and remember Jason Denton, a friend, colleague and team member, who contributed to database development and data stewardship.
Contributors SS helped in study concept, study design, dataset verification, interpretation of data and statistical analysis, drafting of initial manuscript and critical revision of the manuscript. AH and RG were responsible for study design, primary statistical analysis, dataset verification, interpretation of data and statistical analysis, critical revision of the manuscript and methodological oversight. CD and OW helped in dataset creation and stewardship. BM, ST, KC, AS, CH, ES, MM and AH performed manuscript revision. CR helped in study design, interpretation of data and statistical analysis, methodological and study oversight and critical revision of manuscript. All authors approved the final version of the manuscript.
Funding American Gastroenterological Association 2019 Research Scholar Award (SS); US Dept of Veterans Affairs ICX002027A01 (SS), Million Veteran Programme Core MVP000 (KC); National Institute of Health K23HL143161A01 (ST).
Competing interests The authors report no conflicts of interest that are relevant to this article. Dr. Shah is an ad hoc consultant for Phathom Pharmaceuticals.
Patient consent for publication Not applicable.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible
Figure 1 Forest plot of primary and secondary COVID- 19 outcomes within 60 days of the index date, weighted and unweighted cohorts (semi- log scale, range 0.1 to 10). In the unweighted cohort, current outpatient PPI use compared with PPI non- use was associated with increased odds of severe COVID- 19 outcomes, defined based on composite (primary: death or mechanical ventilation; secondary: death, mechanical ventilation, ICU admission or hospitalisation) and individual component outcomes. Each of these associations were statistically non- significant after more fully accounting for covariates in the propensity- weighted cohort, including date of SARS- CoV- 2 testing and VHA facility location. Of note, there was no significant interaction between age group and PPI use on these outcomes. ICU, intensive care unit; PPI, proton pump inhibitor.
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from

3Gut Month 2021 Vol 0 No 0
Letter
for any error and/or omissions arising from translation and adaptation or otherwise.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid- 19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non- commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
© Author(s) (or their employer(s)) 2021. No commercial re- use. See rights and permissions. Published by BMJ.
► Additional supplemental material is published online only. To view, please visit the journal online (http:// dx. doi. org/ 10. 1136/ gutjnl- 2021- 325701).
To cite Shah S, Halvorson A, McBay B, et al. Gut Epub ahead of print: [please include Day Month Year]. doi:10.1136/gutjnl-2021-325701
Received 22 July 2021
Accepted 5 October 2021
Gut 2021;0:1–3. doi:10.1136/gutjnl-2021-325701
ORCID iDsShailja Shah http:// orcid. org/ 0000- 0002- 2049- 9959Adriana Hung http:// orcid. org/ 0000- 0002- 3203- 1608
REFERENCES 1 Lee SW, Ha EK, Yeniova Abdullah Özgür, et al. Severe
clinical outcomes of COVID- 19 associated with proton pump inhibitors: a nationwide cohort study with propensity score matching. Gut 2021;70:76–84.
2 Kamal F, Khan MA, Sharma S, et al. Lack of consistent associations between pharmacologic gastric acid suppression and adverse outcomes in patients with coronavirus disease 2019: meta- analysis of observational studies. Gastroenterology 2021;160:2588–90.
3 Kow CS, Hasan SS. Use of proton pump inhibitors and risk of adverse clinical outcomes from COVID- 19: a meta- analysis. J Intern Med 2021;289:125–8.
4 Hariyanto TI, Prasetya IB, Kurniawan A. Proton pump inhibitor use is associated with increased risk of severity and mortality from coronavirus disease 2019 (COVID- 19) infection. Dig Liver Dis 2020;52:1410–2.
5 Li G- F, An X- X, Yu Y, et al. Do proton pump inhibitors influence SARS- CoV- 2 related outcomes? a meta- analysis. Gut 2021;70:1806–8.
6 Israelsen SB, Ernst MT, Lundh A, et al. Proton pump inhibitor use is not strongly associated with SARS- CoV- 2 related outcomes: a nationwide study and meta- analysis. Clin Gastroenterol Hepatol 2021;19:1845–54.
7 Etminan M, Nazemipour M, Candidate MS, et al. Potential biases in studies of acid- suppressing drugs and COVID- 19 infection. Gastroenterology 2021;160:1443–6.
8 VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E- value. Ann Intern Med 2017;167:268–74.
9 Suissa S, Suissa A. Proton- pump inhibitors and increased gastric cancer risk: time- related biases. Gut 2018;67:2228–9.
on May 4, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2021-325701 on 18 O
ctober 2021. Dow
nloaded from

SUPPLEMENTAL MATERIAL “Proton pump inhibitor use is not associated with severe COVID-19 related outcomes: A propensity score weighted analysis of a national veteran cohort.” Shah et al. Supplemental Methods The present study was designed to avoid exposure misclassification and immortal time, lag time, and protopathic biases, which have been present in some PPI studies as described by Suissa and Suissa (Gut 2018; 67;2228-2229). Immortal time bias related to exposure misclassification and latency bias pose potentially major issues for exposure (i.e. PPI)-outcome studies where the outcome is a long-term outcome, such as cancer. However, our study design avoids immortal time bias and our study question is not impacted by latency bias. Regarding immortal time, it is essential that exposure classification is restricted to exposures that occur on or before time 0, when follow-up begins. Both our exposed and unexposed statuses strictly meet these criteria—that is, PPI use after the index date was not considered for exposure classification since this would introduce potential immortal time bias. To be eligible for categorization as a current PPI user, a patient needed at least two outpatient PPI prescription fills prior to the index date. The drug persistence was calculated using the dates of the two most recent PPI prescription fills and the dispensed “days supply” of PPI therapy. The days supply was added to the date of the prescription fill, and if this persistence window included the date of the positive SARS-CoV-2 test, the person was categorized as a “current PPI user” (See Supplemental Figure 1 below). Patients were categorized as “PPI non-users” if they had not filled an outpatient PPI prescription for at least 365 days prior to the SARS-CoV-2 positive test date. Patients with PPI persistence windows that included -1 to -364 days prior to the index date were considered recent former users and excluded. PPI exposure was not analyzed as a time-varying exposure nor cumulative exposure, since doing so might misclassify active PPI use at the time of testing. Modeling PPI as a time-varying variable would not be appropriate for this present analysis since classifying PPI use after the index date (date of positive SARS-CoV-2 testing) as exposure would introduce bias into the analysis (patients with more comorbidities are more likely to be prescribed PPIs and are also more likely to be admitted to the hospital and have a more severe disease course), including immortal time bias (Suissa and Suissa, Gut 2018; 67;2228-2229). Cumulative exposure is most relevant for long-term outcomes, such as cancer outcomes, and would be less relevant for the present analysis focused on active PPI use and COVID-19 related outcomes out to 60 days of follow-up. Low pH deactivates most pathogens, including coronaviruses. The biological mechanism hypothesized to underlie an association between PPI use and severe COVID-19 related outcomes, if a true association did exist, is that PPI-mediated inhibition of gastric acid secretion would allow for a higher SARS-CoV-2 viral load to reach enterocytes, with subsequent downstream negative clinical consequences. The rigorous definition of PPI exposure in this study ensures a high probability of active PPI use at the time patients tested positive for COVID-19. Protopathic bias is a valid concern, which is why we required at least 2 PPI fills in the baseline year. To evaluate for protopathic bias among the current PPI users—that is, use of PPIs in response to symptoms that might be the result of COVID-19—we evaluated the number of days between the first and second PPI prescription fills, as well as the days between the date of the most recent PPI prescription fill and the date of SARS-CoV-2 positive testing. Among current PPI users, nearly all (>96%) current users had persistent PPI use with: 2 outpatient PPI
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) Gut
doi: 10.1136/gutjnl-2021-325701–3.:10 2021;Gut, et al. Shah S

prescriptions filled in the 365 days prior to the index date; at least 14 days between their first and second most recent PPI prescriptions; and at least 14 days between their first most recent PPI fill and their index date. Regarding latency bias, cancer is an excellent example of an outcome where this is a concern. Cancer begins long before it is diagnosed. Therefore, it is important to have a sufficient lag time after the start of exposure to ensure the exposure has sufficient time to influence any cancers being diagnosed. In the case of severe COVID-19 outcomes within 60 days of hospitalization and their association with PPI (the present study), both the outcomes and the exposure are acute. E-value calculation
The topic of residual confounding is relevant, particularly with studies of PPIs, irrespective of the outcome per se. In their 2017 publication in Annals of Internal Medicine, VanderWeele and Ding introduced a new measure, known as the “E-value”. (VanderWeele and Ding. Ann Intern Med 2017; 167: 268–74.) The E-value is defined as “the minimum strength of association, on the risk ratio scale, that an unmeasured confounder would need to have with both the treatment and the outcome to fully explain away a specific treatment-outcome association, conditional on the measured covariates.” A large E-value is interpreted as considerable unmeasured confounding is needed to explain away an effect estimate and render the treatment-outcome association null (i.e. the findings are robust); whereas a small E-value indicates that only slight unmeasured confounding is sufficient to explain away an effect estimate and render the association null. Importantly, according to VanderWeele and Ding, “if the confidence interval (CI) includes the null of a risk ratio of 1, then the E-value for the CI is simply 1 because no confounding is needed to move the CI to include 1.” The E-value is typically calculated for the adjusted analysis. Because our adjusted analyses (i.e. the weighted analyses) were all null findings—that is, the CIs all included 1.0 (see Figure 1)—all of the E-values would be 1 by definition. To help interpret the magnitude of confounding needed to render the unadjusted (unweighted) analyses null, we calculated the E-value for each. The E-values for the analyses of the association between PPI use vs. non-use and 60-day primary (mechanical ventilation or death) were 1.51 for the effect estimate and 1.32 for the confidence interval; for the secondary (hospitalization, ICU admission, mechanical ventilation, or death) composite outcomes the E-values were 1.51 for the effect estimate and 1.39 for the confidence interval (source: https://www.evalue-calculator.com/evalue/, derived from VanderWeele and Ding. Ann Intern Med 2017; 167: 268–74.). This is interpreted as: the observed OR of 1.27 for the primary and secondary composite outcomes could be explained away by unmeasured confounding that was associated with both the treatment and the outcome by an OR of 1.5-fold each, but weaker confounding cannot do so. Since these are unweighted analyses, the measured confounders are not accounted for; if these were weighted, i.e. adjusted analyses, then the interpretation would be 1.5-fold above and beyond the measured confounders. That our weighted analyses all demonstrated null associations suggests that we did at least sufficiently address (measured) confounding. Certainly we cannot account for all unmeasured residual confounding, but given the null findings, this should not impact the overall conclusion that active PPI use is not associated with significantly increased likelihood of adverse COVID-19 related outcomes.
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) Gut
doi: 10.1136/gutjnl-2021-325701–3.:10 2021;Gut, et al. Shah S

BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) Gut
doi: 10.1136/gutjnl-2021-325701–3.:10 2021;Gut, et al. Shah S

BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) Gut
doi: 10.1136/gutjnl-2021-325701–3.:10 2021;Gut, et al. Shah S

Supplemental Table 1. Associations between current PPI use vs. PPI non-use and COVID-19-related disease severity outcomes (primary analysis, unweighted and weighted cohorts)
OUTCOMES
PPI non-users
Current PPI
users
Odds Ratio (95% CI)
N in WEIGHTED COHORT 8,696 6,262
Primary Composite- Composite of death or
mechanical ventilation within 60 days from index date N with outcome (%)
691 (8.0%)
511 (8.2%)
1.03 (0.91-1.16)
Secondary Composite- Composite of hospitalization,
admission to intensive care unit, mechanical ventilation or death within 60 days from index date
N with outcome (%)
1,990 (22.9%)
1,467 (23.4%)
1.03 (0.95-1.12)
Individual Components- within 60 days from index date, N with outcome (%)
Death 598 (6.9%) 418 (6.7%) 0.97 (0.85-1.10) Mechanical ventilation 233 (2.7%) 202 (3.2%) 1.21 (0.99-1.48) ICU admission 631 (7.3%) 507 (8.1%) 1.13 (0.99-1.28)
Hospitalization 1,655 (19.0%) 1,244 (19.9%) 1.05 (0.97-1.15)
N in UNWEIGHTED COHORT 8,696 6,262
Primary Composite- Composite of death or mechanical ventilation within 60 days from index date
N with outcome (%)
649 (7.5%)
582 (9.3%) 1.27 (1.13-1.43)
Secondary Composite- Composite of hospitalization, admission to intensive care unit, mechanical ventilation
or death within 60 days from index date N with outcome (%)
1,863 (21.4%)
1,613 (25.8%) 1.27 (1.18-1.37)
Individual Components- within 60 days from index date, N with outcome (%)
Death 565 (6.5%) 482 (7.7%) 1.20 (1.06-1.36) Mechanical ventilation 209 (2.4%) 226 (3.6%) 1.52 (1.26-1.84) ICU admission 582 (6.7%) 559 (8.9%) 1.37 (1.21-1.54)
Hospitalization 1,543 (17.7%) 1,363 (21.8%) 1.29 (1.19-1.40)
*Note: p-interaction between age and PPI use on each of the composite and separate outcomes was >0.05, indicating no statistically significant interaction.
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) Gut
doi: 10.1136/gutjnl-2021-325701–3.:10 2021;Gut, et al. Shah S