Embed Size (px)
Citation preview
A Natural History Study of A Natural History Study of Atherosclerosis Using Multimodality Atherosclerosis Using Multimodality
Intracoronary Imaging to Prospectively Intracoronary Imaging to Prospectively Identify Vulnerable PlaqueIdentify Vulnerable Plaque
Gregg W. Stone, MDGregg W. Stone, MDPROSPECT InvestigatorsPROSPECT Investigators
PProviding roviding RRegional egional OObservations to bservations to SStudy tudy PPredictors redictors of of EEvents in the vents in the CCoronary oronary TTreeree
The The PROSPECTPROSPECT TrialTrial
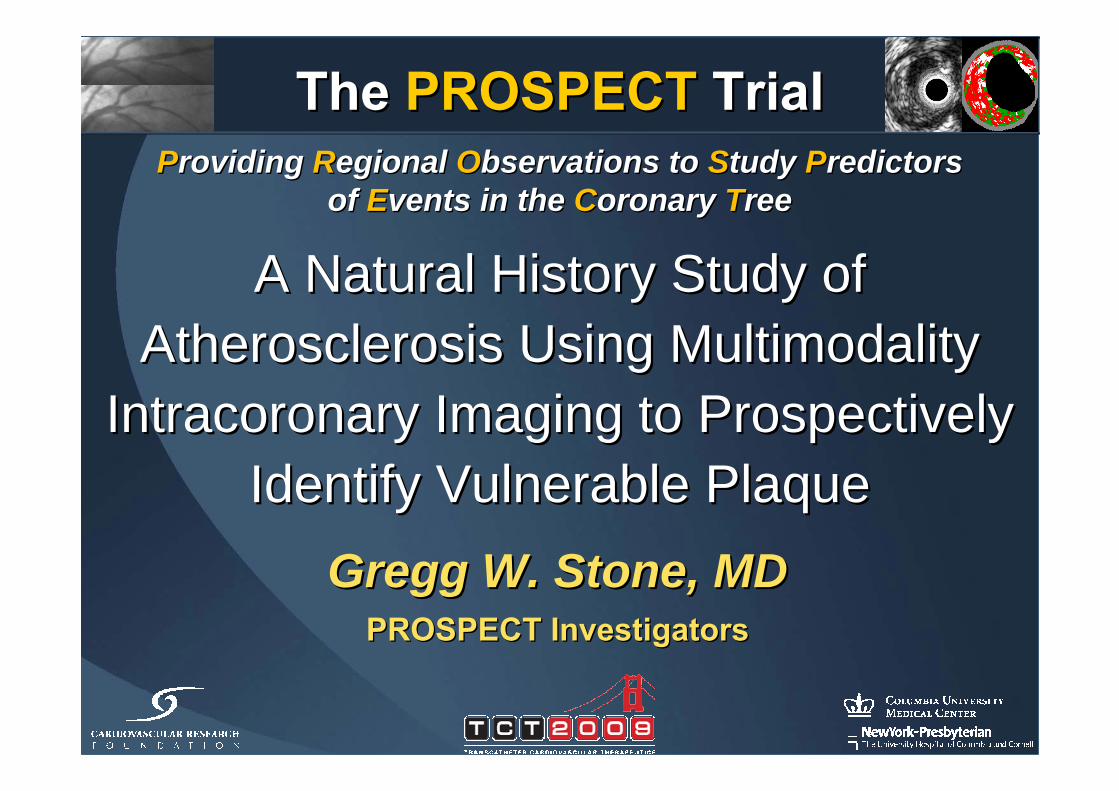
700 pts with ACS700 pts with ACSUA (with ECGUA (with ECG∆∆) ) oror NSTEMI NSTEMI oror STEMI >24STEMI >24ºº
undergoing PCI of 1 or 2 major coronary arteriesundergoing PCI of 1 or 2 major coronary arteriesat up to 40 sites in the U.S. and Europeat up to 40 sites in the U.S. and Europe
PCI of culprit lesion(s)PCI of culprit lesion(s)Successful and uncomplicatedSuccessful and uncomplicated
Formally enrolledFormally enrolled
Metabolic S.Metabolic S.•• Waist circumWaist circum•• Fast lipidsFast lipids•• Fast gluFast glu•• HgbA1CHgbA1C•• Fast insulinFast insulin•• CreatinineCreatinine
BiomarkersBiomarkers•• Hs CRPHs CRP•• ILIL--66•• sCD40LsCD40L•• MPOMPO•• TNFTNFαα•• MMP9MMP9•• LpLp--PLA2PLA2•• othersothers
PI: Gregg W. StonePI: Gregg W. StoneSponsor: Abbott Vascular; Partner: VolcanoSponsor: Abbott Vascular; Partner: Volcano
The The PROSPECTPROSPECT TrialTrial
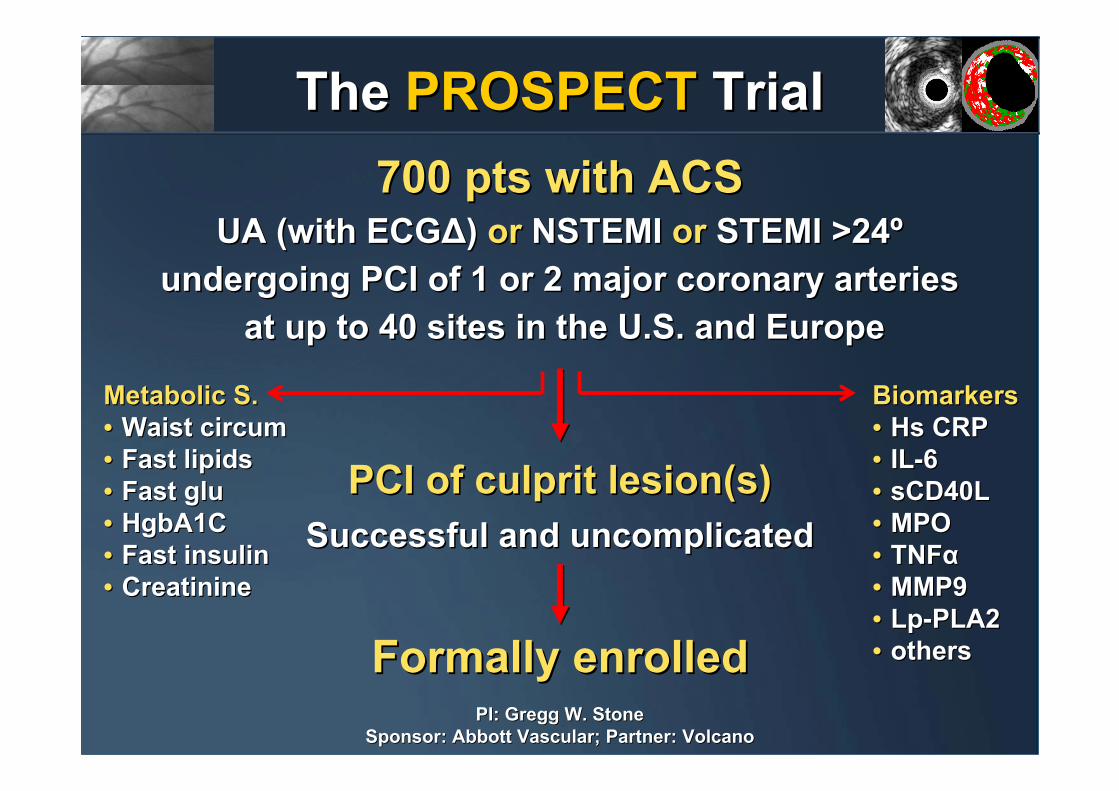
33--vessel imaging post PCIvessel imaging post PCICulprit artery, followed byCulprit artery, followed by
nonnon--culprit arteriesculprit arteries
Angiography (QCA of entire coronary tree)Angiography (QCA of entire coronary tree)IVUSIVUS
Virtual histologyVirtual histologyPalpography (n=~350)Palpography (n=~350)
Repeat imagingRepeat imagingin pts with events in pts with events
Meds recMeds recAspirinAspirinPlavix 1yrPlavix 1yrStatinStatinRepeat biomarkersRepeat biomarkers@ 30 days, 6 months @ 30 days, 6 months
Proximal 6-8 cm of each coronary
artery
Proximal 6Proximal 6--8 8 cm of each cm of each coronary coronary
arteryartery
MSCTMSCTSubstudySubstudyN=50N=50--100100F/U: 1 mo, 6 mo,
1 yr, 2 yr,±3-5 yrs
F/U: 1 mo, 6 mo,F/U: 1 mo, 6 mo,1 yr, 2 yr,1 yr, 2 yr,±±33--5 yrs5 yrs
The The PROSPECTPROSPECT TrialTrial
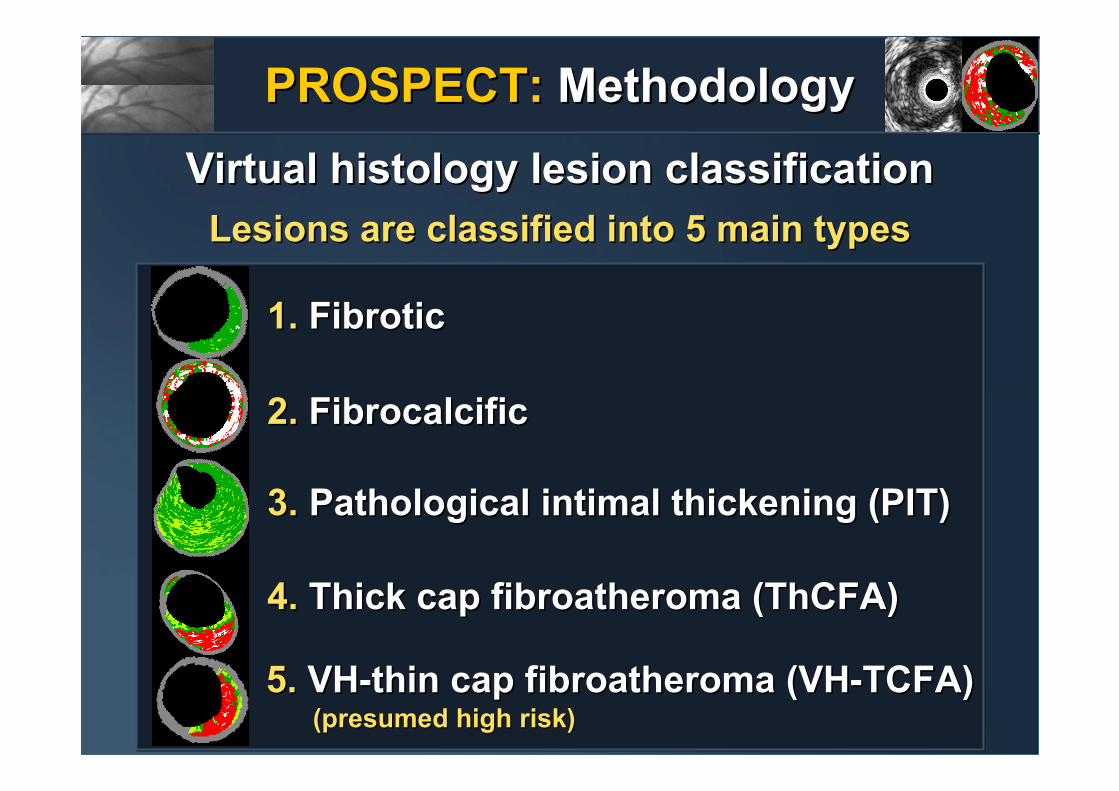
Lesions are classified into 5 main typesLesions are classified into 5 main types
1.1. FibroticFibrotic
2.2. FibrocalcificFibrocalcific
3.3. Pathological intimal thickening (PIT)Pathological intimal thickening (PIT)
4.4. Thick cap fibroatheroma (ThCFA)Thick cap fibroatheroma (ThCFA)
5. 5. VHVH--thin cap fibroatheroma (VHthin cap fibroatheroma (VH--TCFA)TCFA)(presumed high risk)(presumed high risk)
PROSPECT:PROSPECT: MethodologyMethodologyVirtual histology lesion classificationVirtual histology lesion classification
PROSPECT: PROSPECT: Primary EndpointPrimary Endpoint
MACE attributable to rapid angiographic progression of a non-culprit lesion*•Cardiac death•Cardiac arrest•Myocardial infarction•Unstable angina
- Requiring revascularization- Requiring rehospitalization
•Increasing angina- Requiring revascularization- Requiring rehospitalization
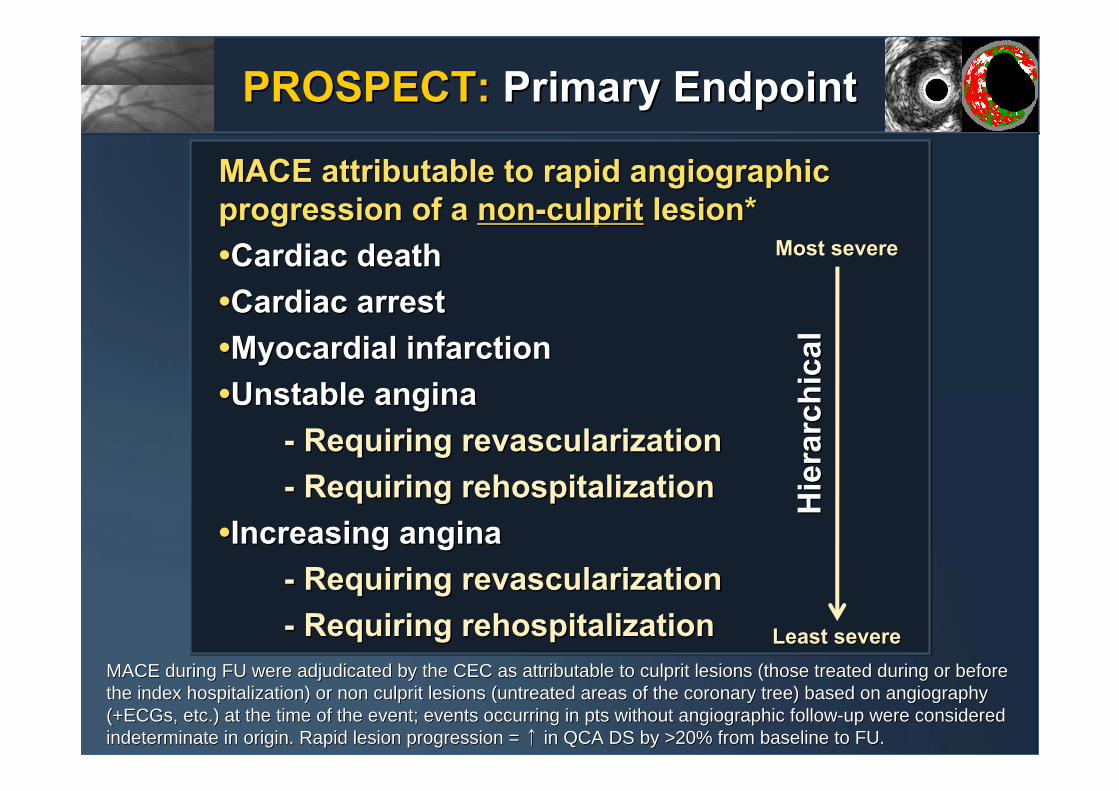
MACE attributable to rapid angiographic MACE attributable to rapid angiographic progression of a progression of a nonnon--culpritculprit lesion*lesion*••Cardiac deathCardiac death••Cardiac arrestCardiac arrest••Myocardial infarctionMyocardial infarction••Unstable anginaUnstable angina
-- Requiring revascularizationRequiring revascularization-- Requiring rehospitalizationRequiring rehospitalization
••Increasing anginaIncreasing angina-- Requiring revascularizationRequiring revascularization-- Requiring rehospitalizationRequiring rehospitalization
MACE during FU were adjudicated by the CEC as attributable to cuMACE during FU were adjudicated by the CEC as attributable to culprit lesions (those treated during or before lprit lesions (those treated during or before the index hospitalization) or non culprit lesions (untreated arethe index hospitalization) or non culprit lesions (untreated areas of the coronary tree) based on angiography as of the coronary tree) based on angiography (+ECGs, etc.) at the time of the event; events occurring in pts (+ECGs, etc.) at the time of the event; events occurring in pts without angiographic followwithout angiographic follow--up were considered up were considered indeterminate in origin. Rapid lesion progression = indeterminate in origin. Rapid lesion progression = ↑↑ in QCA DS by >20% from baseline to FU.in QCA DS by >20% from baseline to FU.
Hie
rarc
hica
lH
iera
rchi
cal
Most severeMost severe
Least severeLeast severe
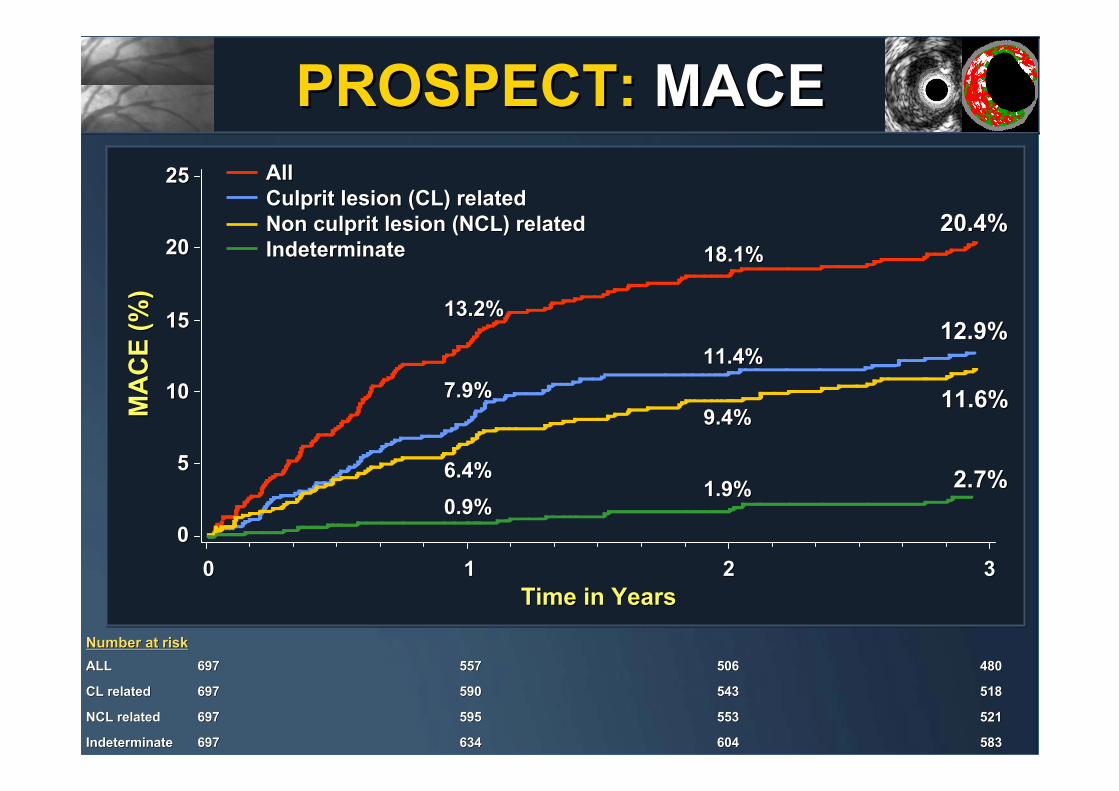
PROSPECT: PROSPECT: MACEMACEM
AC
E (%
)M
AC
E (%
)
Time in YearsTime in Years00 11 22 33
All All Culprit lesion (CL) relatedCulprit lesion (CL) relatedNon culprit lesion (NCL) relatedNon culprit lesion (NCL) relatedIndeterminateIndeterminate
00
55
1010
1515
2020
2525
Number at riskNumber at risk
20.4%20.4%
12.9%12.9%
11.6%11.6%
2.7%2.7%
13.2%13.2%
7.9%7.9%
6.4%6.4%
0.9%0.9%
18.1%18.1%
11.4%11.4%
9.4%9.4%
1.9%1.9%
ALLALL 697697 557 557 506 506 480480
CL relatedCL related 697697 590590 543543 518518
NCL relatedNCL related 697697 595595 553 553 521521
IndeterminateIndeterminate 697697 634634 604 604 583583
MA
CE
(%)
MA
CE
(%)
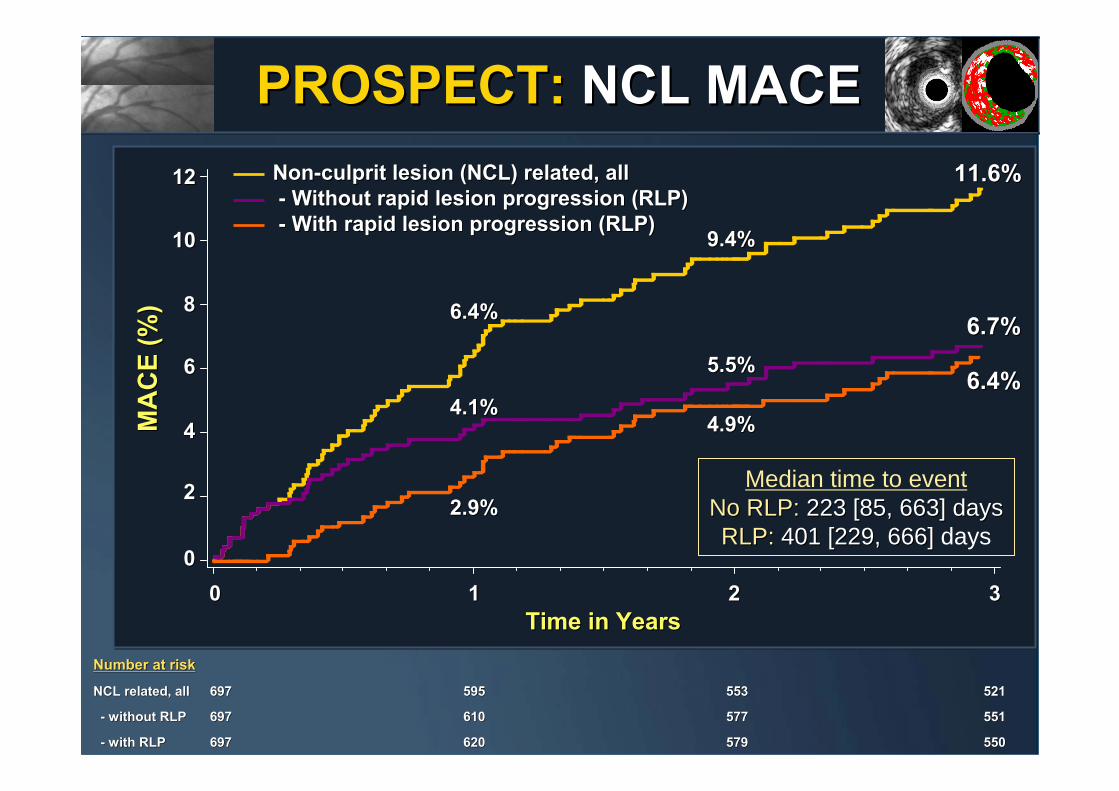
Time in YearsTime in Years00 11 22 33
Number at riskNumber at risk
NonNon--culprit lesion (NCL) related, allculprit lesion (NCL) related, all-- Without rapid lesion progression (RLP)Without rapid lesion progression (RLP)-- With rapid lesion progression (RLP)With rapid lesion progression (RLP)
00
22
44
66
88
1010
1212 11.6%11.6%
6.7%6.7%
6.4%6.4%
2.9%2.9%
4.1%4.1%
6.4%6.4%
5.5%5.5%
4.9%4.9%
9.4%9.4%
NCL related, allNCL related, all 697697 595595 553 553 521 521
-- without RLPwithout RLP 697697 610610 577 577 551 551
-- with RLPwith RLP 697697 620620 579 579 550 550
PROSPECT: PROSPECT: NCL NCL MACEMACE
Median time to eventNo RLP: No RLP: 223 [85, 663] days223 [85, 663] daysRLP: RLP: 401 [229, 666]401 [229, 666] days
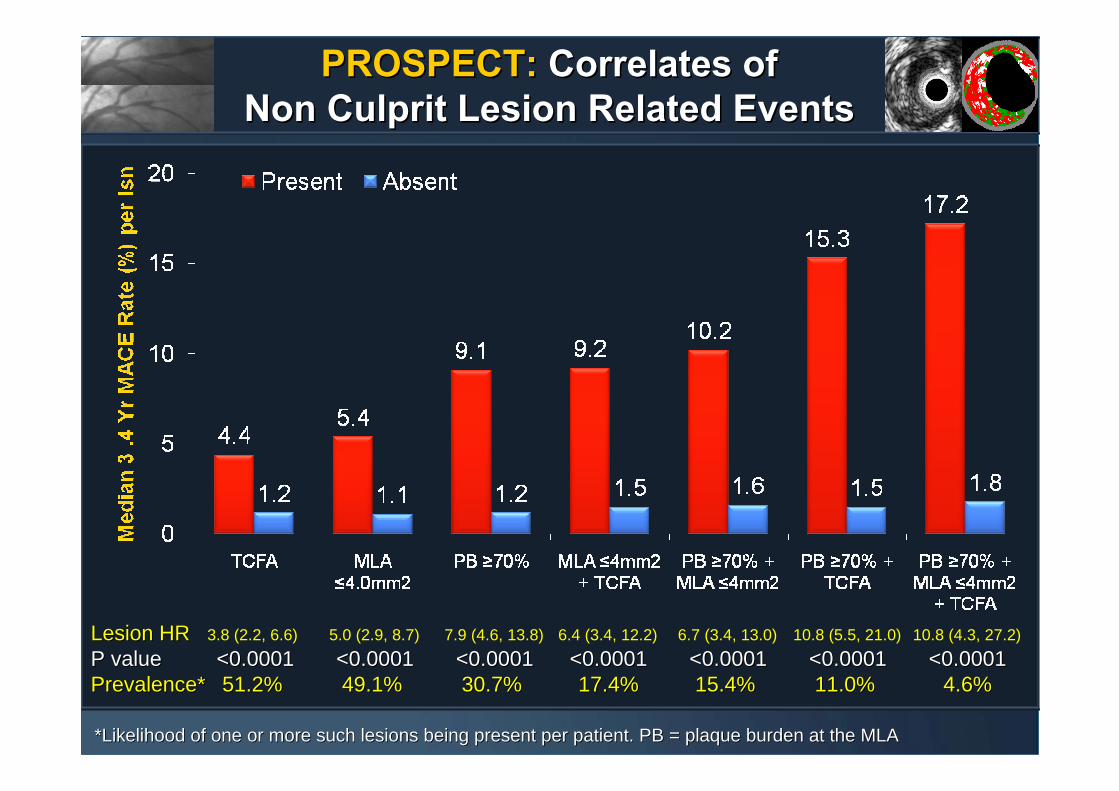
PROSPECT:PROSPECT: Correlates of Correlates of Non Culprit Lesion Related EventsNon Culprit Lesion Related Events
Lesion HRLesion HR 3.8 (2.2, 6.6) 5.0 (2.9, 8.7) 7.9 (4.6, 13.8) 6.4 (3.4, 12.2) 6.7 (3.4, 13.0) 10.8 (5.5, 21.0) 10.8 (4.3, 27.2) P valueP value <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001<0.0001 <0.0001<0.0001 <0.0001<0.0001 <0.0001<0.0001Prevalence*Prevalence* 51.2%51.2% 49.1%49.1% 30.7%30.7% 17.4% 17.4% 15.4%15.4% 11.0%11.0% 4.6%4.6%
**Likelihood of one or more such lesions being present per patientLikelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA. PB = plaque burden at the MLA
PROSPECT:PROSPECT: ConclusionsConclusions• From this trial, the first prospective, natural history study ofatherosclerosis using multimodality imaging to characterize the coronary tree, we can conclude that:• Approximately 20% of pts with ACS successfully treated with stents and contemporary medical Rx develop MACE within 3 years, with adverse events equally attributable to recurrence at originally treated culprit lesions (treatment failure) and topreviously untreated non culprit coronary segments
• Approximately 12% of pts develop MACE from non culprit lesions during 3 years of follow-up
• Patients treated with contemporary medical therapy who develop non culprit lesion events present most commonly with progressive or unstable angina, and rarely with cardiac death, cardiac arrest or MI
•• From this trial, the first prospective, natural history study ofFrom this trial, the first prospective, natural history study ofatherosclerosis using multimodality imaging to characterize the atherosclerosis using multimodality imaging to characterize the coronary tree, we can conclude that:coronary tree, we can conclude that:•• Approximately 20% of pts with ACS successfully treated with Approximately 20% of pts with ACS successfully treated with stents and contemporary medical Rx develop MACE within stents and contemporary medical Rx develop MACE within 3 years, with adverse events equally attributable to recurrence 3 years, with adverse events equally attributable to recurrence at originally treated culprit lesions (treatment failure) and toat originally treated culprit lesions (treatment failure) and topreviously untreated non culprit coronary segmentspreviously untreated non culprit coronary segments
•• Approximately 12% of pts develop MACE from Approximately 12% of pts develop MACE from non culprit non culprit lesionslesions during 3 years of followduring 3 years of follow--upup
•• Patients treated with contemporary medical therapy who Patients treated with contemporary medical therapy who develop non culprit lesion events present most commonly with develop non culprit lesion events present most commonly with progressive or unstable angina, and rarely with cardiac death, progressive or unstable angina, and rarely with cardiac death, cardiac arrest or MIcardiac arrest or MI
PROSPECT:PROSPECT: ConclusionsConclusions• While plaques which are responsible for unanticipated future MACE
are frequently angiographically mild, most untreated plaques which become symptomatic have a large plaque burden and a small lumen area (which are detectable by IVUS but not by angiography)
• Only about half of new events due to non culprit lesions exemplify the classic notion of vulnerable plaque (rapid lesion progression of mild angiographic lesions), while half are attributable to unrecognized and untreated severe disease with minimal change over time
• The prospective identification of non culprit lesions prone to develop MACE within 3 years can be enhanced by characterization of underlying plaque morphology with virtual histology, with VH-TCFAs representing the highest risk lesion type
• The combination of large plaque burden (IVUS) and a large necrotic core without a visible cap (VH-TCFA) identifies lesions which are at especially high risk for future adverse cardiovascular events
•• While plaques which are responsible for unanticipated future MACWhile plaques which are responsible for unanticipated future MACE E are frequently angiographically mild, most untreated plaques whiare frequently angiographically mild, most untreated plaques which ch become symptomatic have a large plaque burden and a small lumen become symptomatic have a large plaque burden and a small lumen area (which are detectable by IVUS but not by angiography)area (which are detectable by IVUS but not by angiography)
•• Only about half of new events due to non culprit lesions exempliOnly about half of new events due to non culprit lesions exemplify the fy the classic notion of vulnerable plaque (rapid lesion progression ofclassic notion of vulnerable plaque (rapid lesion progression of mild mild angiographic lesions), while half are attributable to unrecognizangiographic lesions), while half are attributable to unrecognized and ed and untreated severe disease with minimal change over timeuntreated severe disease with minimal change over time
•• The prospective identification of non culprit lesions prone to dThe prospective identification of non culprit lesions prone to develop evelop MACE within 3 years can be enhanced by characterization of MACE within 3 years can be enhanced by characterization of underlying plaque morphology with virtual histology, with VHunderlying plaque morphology with virtual histology, with VH--TCFAs TCFAs representing the highest risk lesion typerepresenting the highest risk lesion type
•• The combination of large plaque burden (IVUS) and a large necrotThe combination of large plaque burden (IVUS) and a large necrotic ic core without a visible cap (VHcore without a visible cap (VH--TCFA) identifies lesions which are at TCFA) identifies lesions which are at especially high risk for future adverse cardiovascular eventsespecially high risk for future adverse cardiovascular events