Embed Size (px)
Citation preview
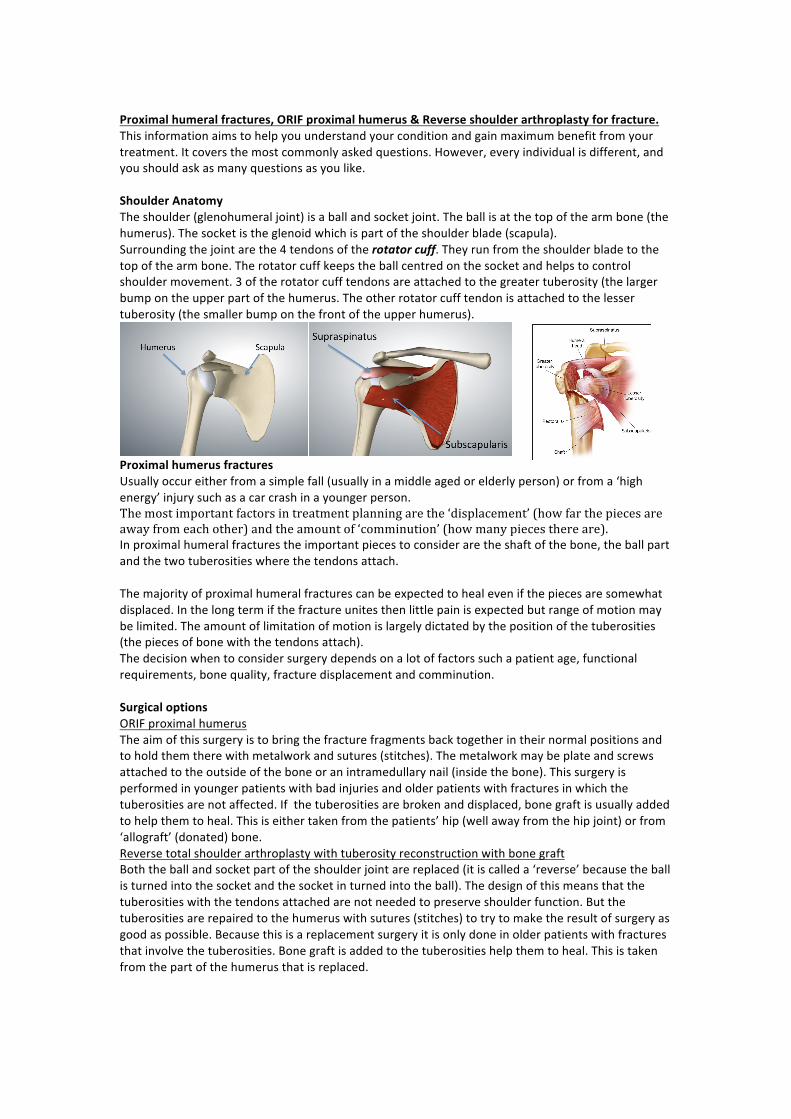
Proximalhumeralfractures,ORIFproximalhumerus&Reverseshoulderarthroplastyforfracture.Thisinformationaimstohelpyouunderstandyourconditionandgainmaximumbenefitfromyourtreatment.Itcoversthemostcommonlyaskedquestions.However,everyindividualisdifferent,andyoushouldaskasmanyquestionsasyoulike.ShoulderAnatomyTheshoulder(glenohumeraljoint)isaballandsocketjoint.Theballisatthetopofthearmbone(thehumerus).Thesocketistheglenoidwhichispartoftheshoulderblade(scapula).Surroundingthejointarethe4tendonsoftherotatorcuff.Theyrunfromtheshoulderbladetothetopofthearmbone.Therotatorcuffkeepstheballcentredonthesocketandhelpstocontrolshouldermovement.3oftherotatorcufftendonsareattachedtothegreatertuberosity(thelargerbumpontheupperpartofthehumerus.Theotherrotatorcufftendonisattachedtothelessertuberosity(thesmallerbumponthefrontoftheupperhumerus).
ProximalhumerusfracturesUsuallyoccureitherfromasimplefall(usuallyinamiddleagedorelderlyperson)orfroma‘highenergy’injurysuchasacarcrashinayoungerperson.Themostimportantfactorsintreatmentplanningarethe‘displacement’(howfarthepiecesareawayfromeachother)andtheamountof‘comminution’(howmanypiecesthereare).Inproximalhumeralfracturestheimportantpiecestoconsideraretheshaftofthebone,theballpartandthetwotuberositieswherethetendonsattach.Themajorityofproximalhumeralfracturescanbeexpectedtohealevenifthepiecesaresomewhatdisplaced.Inthelongtermifthefractureunitesthenlittlepainisexpectedbutrangeofmotionmaybelimited.Theamountoflimitationofmotionislargelydictatedbythepositionofthetuberosities(thepiecesofbonewiththetendonsattach).Thedecisionwhentoconsidersurgerydependsonalotoffactorssuchapatientage,functionalrequirements,bonequality,fracturedisplacementandcomminution.SurgicaloptionsORIFproximalhumerusTheaimofthissurgeryistobringthefracturefragmentsbacktogetherintheirnormalpositionsandtoholdthemtherewithmetalworkandsutures(stitches).Themetalworkmaybeplateandscrewsattachedtotheoutsideoftheboneoranintramedullarynail(insidethebone).Thissurgeryisperformedinyoungerpatientswithbadinjuriesandolderpatientswithfracturesinwhichthetuberositiesarenotaffected.Ifthetuberositiesarebrokenanddisplaced,bonegraftisusuallyaddedtohelpthemtoheal.Thisiseithertakenfromthepatients’hip(wellawayfromthehipjoint)orfrom‘allograft’(donated)bone.ReversetotalshoulderarthroplastywithtuberosityreconstructionwithbonegraftBoththeballandsocketpartoftheshoulderjointarereplaced(itiscalleda‘reverse’becausetheballisturnedintothesocketandthesocketinturnedintotheball).Thedesignofthismeansthatthetuberositieswiththetendonsattachedarenotneededtopreserveshoulderfunction.Butthetuberositiesarerepairedtothehumeruswithsutures(stitches)totrytomaketheresultofsurgeryasgoodaspossible.Becausethisisareplacementsurgeryitisonlydoneinolderpatientswithfracturesthatinvolvethetuberosities.Bonegraftisaddedtothetuberositieshelpthemtoheal.Thisistakenfromthepartofthehumerusthatisreplaced.
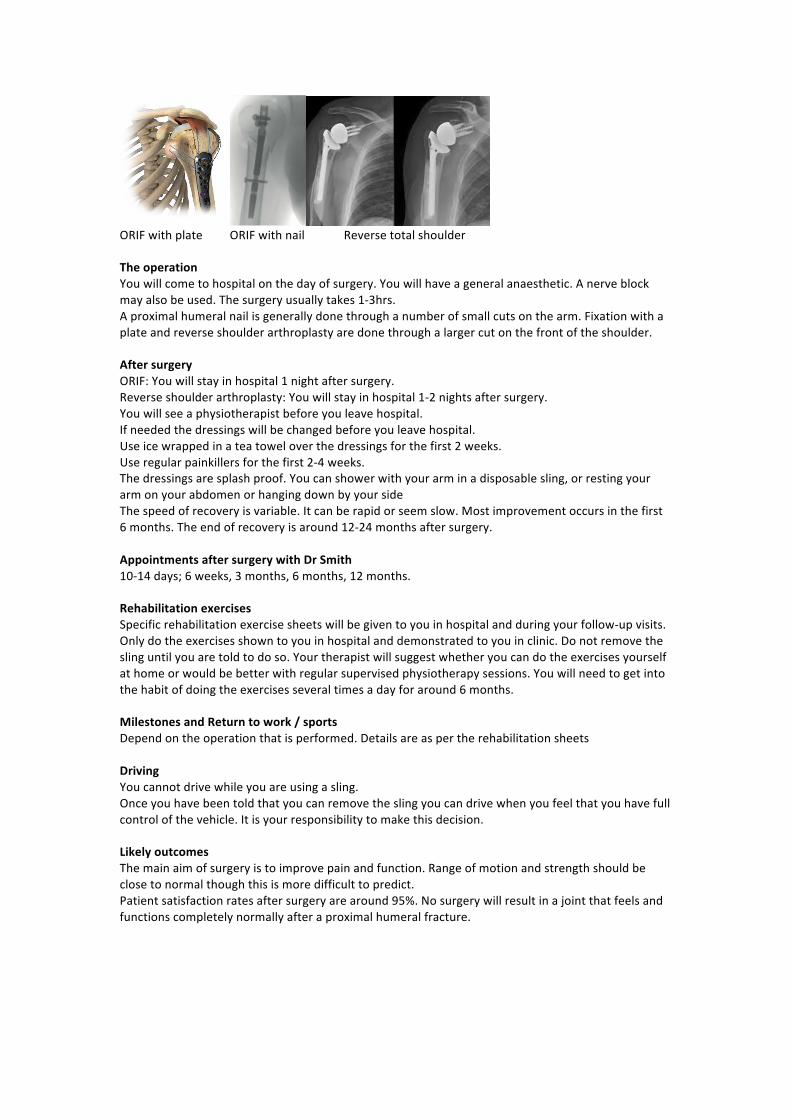
ORIFwithplateORIFwithnailReversetotalshoulderTheoperationYouwillcometohospitalonthedayofsurgery.Youwillhaveageneralanaesthetic.Anerveblockmayalsobeused.Thesurgeryusuallytakes1-3hrs.Aproximalhumeralnailisgenerallydonethroughanumberofsmallcutsonthearm.Fixationwithaplateandreverseshoulderarthroplastyaredonethroughalargercutonthefrontoftheshoulder.AftersurgeryORIF:Youwillstayinhospital1nightaftersurgery.Reverseshoulderarthroplasty:Youwillstayinhospital1-2nightsaftersurgery.Youwillseeaphysiotherapistbeforeyouleavehospital.Ifneededthedressingswillbechangedbeforeyouleavehospital.Useicewrappedinateatoweloverthedressingsforthefirst2weeks.Useregularpainkillersforthefirst2-4weeks.Thedressingsaresplashproof.Youcanshowerwithyourarminadisposablesling,orrestingyourarmonyourabdomenorhangingdownbyyoursideThespeedofrecoveryisvariable.Itcanberapidorseemslow.Mostimprovementoccursinthefirst6months.Theendofrecoveryisaround12-24monthsaftersurgery.AppointmentsaftersurgerywithDrSmith10-14days;6weeks,3months,6months,12months.RehabilitationexercisesSpecificrehabilitationexercisesheetswillbegiventoyouinhospitalandduringyourfollow-upvisits.Onlydotheexercisesshowntoyouinhospitalanddemonstratedtoyouinclinic.Donotremovetheslinguntilyouaretoldtodoso.Yourtherapistwillsuggestwhetheryoucandotheexercisesyourselfathomeorwouldbebetterwithregularsupervisedphysiotherapysessions.Youwillneedtogetintothehabitofdoingtheexercisesseveraltimesadayforaround6months.MilestonesandReturntowork/sportsDependontheoperationthatisperformed.Detailsareaspertherehabilitationsheets
DrivingYoucannotdrivewhileyouareusingasling.Onceyouhavebeentoldthatyoucanremovetheslingyoucandrivewhenyoufeelthatyouhavefullcontrolofthevehicle.Itisyourresponsibilitytomakethisdecision.LikelyoutcomesThemainaimofsurgeryistoimprovepainandfunction.Rangeofmotionandstrengthshouldbeclosetonormalthoughthisismoredifficulttopredict.Patientsatisfactionratesaftersurgeryarearound95%.Nosurgerywillresultinajointthatfeelsandfunctionscompletelynormallyafteraproximalhumeralfracture.





























