Embed Size (px)
Citation preview

Injury, Int. J. Care Injured 44 (2013) 481–487
Proximal humeral fractures: The role of calcium sulphate augmentation andextended deltoid splitting approach in internal fixation using locking plates
K. Somasundaram *, C.P. Huber, V. Babu, H. Zadeh
West Middlesex University Hospital NHS Trust, Department of Orthopaedics, Twickenham Road, Isleworth, Middlesex TW7 6AF, UK
A R T I C L E I N F O
Article history:
Accepted 24 October 2012
Keywords:
Proximal humerus fractures
Internal fixation
Calcium sulphate bone substitute
Extended deltoid splitting approach
Proximal humerus locking plates
A B S T R A C T
The aim of our study is to analyse the results of our surgical technique for the treatment of proximal
humeral fractures and fracture dislocations using locking plates in conjunction with calcium sulphate
bone-substitute augmentation and tuberosity repair using high-strength sutures. We used the extended
deltoid-splitting approach for fracture patterns involving displacement of both lesser and greater
tuberosities and for fracture-dislocations. Optimal surgical management of proximal humeral fractures
remains controversial. Locking plates have become a popular method of fixation. However, failure of
fixation may occur if they are used as the sole method of fixation in comminuted fractures, especially in
osteopenic bone.
Methods: We retrospectively analysed 22 proximal humeral fractures in 21 patients; 10 were male and
11 female with an average age of 64.6 years (range 37–77). Average follow-up was 24 months. Eleven of
these fractures were exposed by the extended deltoid-splitting approach. Fractures were classified
according to Neer and Hertel systems. Preoperative radiographs and computed tomography (CT) scans in
three- and four-part fractures were done to assess the displacement and medial calcar length for
predicting the humeral head vascularity. According to the Neer classification, there were five two-part,
six three-part, five four-part fractures and six fracture-dislocations (two anterior and four posterior).
Results were assessed clinically with disabilities of the arm, shoulder and hand (DASH) scores, modified
Constant and Murley scores and serial postoperative radiographs.
Results: The mean DASH score was 16.18 and the modified Constant and Murley score was 64.04 at the
last follow-up. Eighteen out of twenty-two cases achieved good clinical outcome. All the fractures united
with no evidence of infection, failure of fixation, malunion, tuberosity failure, avascular necrosis or
adverse reaction to calcium sulphate bone substitute. There was no evidence of axillary nerve injury.
Four patients had a longer recovery period due to stiffness, associated wrist fracture and elbow
dislocation. The CaSO4 bone substitute was replaced by normal appearing trabecular bone texture at an
average of 6 months in all patients.
Conclusion: In our experience, we have found the use of locking plates, calcium sulphate bone substitute
and tuberosity repair with high-strength sutures to be a safe and reliable method of internal fixation for
complex proximal humeral fractures and fracture-dislocations. Furthermore, we have also found the use
of the extended deltoid-splitting approach to be safe and to provide excellent exposure facilitating
accurate reduction for fixation of the fracture patterns involving displacement of both lesser and greater
tuberosities and for fracture-dislocations.
� 2012 Elsevier Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Fractures of the proximal humerus are relatively commoninjuries, accounting for approximately 4–5% of all fractures.1 Thereis a steady increase in the incidence of this type of fracture in theosteoporotic population.2 Optimal surgical management of these
* Corresponding author. Tel.: +44 7954173802; fax: +44 2083215371.
E-mail addresses: [email protected], [email protected]
(K. Somasundaram), [email protected] (C.P. Huber),
[email protected] (V. Babu), [email protected] (H. Zadeh).
0020–1383/$ – see front matter � 2012 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.injury.2012.10.030
fractures remains controversial, with many advocating prostheticreplacement in elderly osteoporotic patients.3,4
Recent advances in implants and operative techniques seem tohave improved the outcome after open reduction and internalfixation of proximal humeral fractures compared with prostheticreplacement.5–7 However, despite the use of locking plates,significant rates of complications have been reported includingloss of fixation, humeral head perforation and impingement.8,9
The aim of our study is to analyse the results of our surgicaltechnique for the treatment of proximal humeral fractures and

K. Somasundaram et al. / Injury, Int. J. Care Injured 44 (2013) 481–487482
fracture dislocations using locking plates in conjunction withcalcium sulphate bone-substitute augmentation and tuberosityrepair using high-strength sutures. We used the extended deltoid-splitting approach as an alternative to the deltopectoral approachfor fracture patterns involving displacement of both lesser andgreater tuberosities and for fracture-dislocations.
Biomechanical and in vivo studies showed better stability andoutcome following internal fixation of comminuted proximalhumerus fractures when augmented with a calcium-phosphate(Ca3(PO4)2) bone substitute (Norion SRS, Skeletal Repair System;Norion, CA, USA).5,10 In our series we used a calcium-sulphate(CaSO4) injectable bone substitute instead (Stimulan, Biocompo-sites, Staffordshire, UK).11
Materials and methods
We retrospectively analysed proximal humeral fractures andfracture dislocations treated operatively at our hospital betweenJuly 2007 and November 2009. We excluded undisplaced orminimally displaced fractures (<5 mm), patients with low mentaltest scores (treated non-operatively) and cases where tuberosityrepair or bone-substitute augmentation was not required. Thisyielded 22 proximal humeral fractures/fracture dislocations in 21patients. All these fractures were treated with open reduction andinternal fixation using locking plates in conjunction with CaSO4
bone-substitute augmentation and tuberosity repair using high-strength sutures. The extended deltoid-splitting approach wasused to expose fractures involving displacement of both tuberosi-ties and fracture-dislocations in 11 fractures. During the studyperiod, only two cases were treated with hemiarthroplasty as theyhad high risk of humeral head ischaemia as predicted by Hertel’scriteria.12
The average age of patients was 61.6 years (range 45–77 years)and 15 were over the age of 60 years (Graph 1). There were 10 maleand 11 female patients. Nine patients had fractures on the rightside.
Fractures were assessed according to Neer’s classification basedon radiographs.13 There were five 2-part, six 3-part, five 4-partfractures and six fracture-dislocations (two anterior and fourposterior). Eighteen patients had computed tomography (CT) scansand fractures were further classified according to the Hertel’sLEGO-Codman classification.12 There were four Type I, one Type II,seven Type VII, one Type VIII, one Type IX, five Type XI and threeType XII fractures.
In accordance with Hertel’s criteria, the lengths of the intactmedial calcar and the medial hinge were used to predict the risk ofischaemia of the humeral head.12 Only one patient had combineddisruption of both the medial hinge and the medial calcar (<8 mmof length). All the others had either an intact medial hinge (5/22) ora calcar length >8 mm (20/22).
0
10
20
30
40
50
60
70
80
90
1 3 5 7 9 11 13 15 17 19 21
No. of Patients
Ag
e
Graph 1.
The specified operative technique as described below wasfollowed by all the senior authors performing the surgicalprocedures (B two cases, C nine cases and D 10 cases). The studydid not receive any funding from external sources and it was donein accordance with the rules of the audit and research departmentat our hospital.
Surgical technique
The deltopectoral approach was used in the Neer two-part andthree-part fractures. The Mackenzie shoulder approach14 wasevolved further by author D into extended deltoid-splittingapproach. This approach was used in four-part fractures andfracture-dislocations to facilitate exposure and reduction of thetuberosity fragments. The deltopectoral approach is well describedin the orthopaedic literature and is not discussed further. Wedescribe below the technique that we follow for the extendeddeltoid-splitting approach.
Position and fluoroscopic access
The patient is placed in the deckchair position. The surfacemarking of the acromion and lateral clavicle is drawn with a skinmarker (Fig. 1(a)). Adequate fluoroscopy access is ensured prior todraping.
Incision
The skin incision starts just posterior to the acromioclavicularjoint and is followed to the anterolateral corner of the acromionand then extended to a distance of 10–12 cm from the lateral edgeof the acromion in line with the interval between the anterior andmiddle bellies of the deltoid muscle. The subcutaneous tissue isdivided in line with the skin incision down to the deltotrapezialfascia.
Proximal deltoid split
After identifying the interval between the anterior and middlebellies, the proximal deltoid is initially split for a distance of lessthan 5 cm from the edge of the acromion (Fig. 1(b)). The axillarynerve generally runs 6 cm distal to the anterior acromion.15
Osteoperiosteal flaps are raised to release the proximal deltoidfrom its origin, thus exposing the anterolateral third of theacromion.
Identification of the axillary nerve
The next crucial step is to define the deep surface of the deltoidmuscle and mobilise it away from the fractured tuberosities andproximal shaft of the humerus. This is best achieved by palpatingthe deep surface of the acromion posteriorly using the index fingerand then sweeping the finger in a posteroinferior direction, thusbluntly lifting away the posterior and middle bellies of the deltoidfrom the proximal humerus (Fig. 1(c)). Often during thismanoeuvre, the axillary nerve can be palpated running trans-versely across the deep surface of the deltoid at the tip of one’sfinger inferiorly. A similar manoeuvre is used to mobilise theanterior deltoid from the lesser tuberosity.
Distal deltoid split
The deltoid is then split superficially to a distance of 10 cm fromthe lateral edge of the acromion. Note that the axillary nerve lies onthe deep surface of the deltoid and is closely related to the lateralcortex of the proximal humeral shaft.16 The deltoid split is carefully
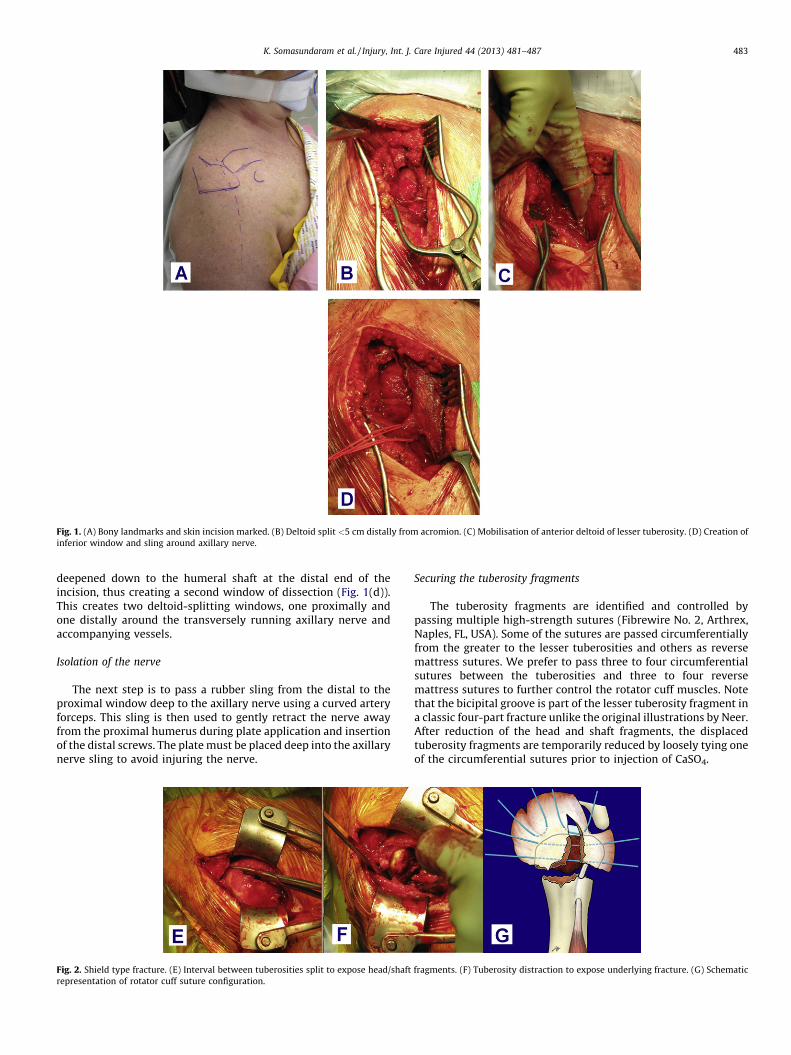
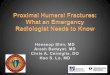
Fig. 1. (A) Bony landmarks and skin incision marked. (B) Deltoid split <5 cm distally from acromion. (C) Mobilisation of anterior deltoid of lesser tuberosity. (D) Creation of
inferior window and sling around axillary nerve.
K. Somasundaram et al. / Injury, Int. J. Care Injured 44 (2013) 481–487 483
deepened down to the humeral shaft at the distal end of theincision, thus creating a second window of dissection (Fig. 1(d)).This creates two deltoid-splitting windows, one proximally andone distally around the transversely running axillary nerve andaccompanying vessels.
Isolation of the nerve
The next step is to pass a rubber sling from the distal to theproximal window deep to the axillary nerve using a curved arteryforceps. This sling is then used to gently retract the nerve awayfrom the proximal humerus during plate application and insertionof the distal screws. The plate must be placed deep into the axillarynerve sling to avoid injuring the nerve.
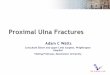
Fig. 2. Shield type fracture. (E) Interval between tuberosities split to expose head/shaft
representation of rotator cuff suture configuration.
Securing the tuberosity fragments
The tuberosity fragments are identified and controlled bypassing multiple high-strength sutures (Fibrewire No. 2, Arthrex,Naples, FL, USA). Some of the sutures are passed circumferentiallyfrom the greater to the lesser tuberosities and others as reversemattress sutures. We prefer to pass three to four circumferentialsutures between the tuberosities and three to four reversemattress sutures to further control the rotator cuff muscles. Notethat the bicipital groove is part of the lesser tuberosity fragment ina classic four-part fracture unlike the original illustrations by Neer.After reduction of the head and shaft fragments, the displacedtuberosity fragments are temporarily reduced by loosely tying oneof the circumferential sutures prior to injection of CaSO4.
fragments. (F) Tuberosity distraction to expose underlying fracture. (G) Schematic

Fig. 3. (H) Graft preparation. (I) Filling of metaphyseal void under fluoroscopic control using syringe and cannula. (J) Further void filling and addition of proximal locking
screws.
K. Somasundaram et al. / Injury, Int. J. Care Injured 44 (2013) 481–487484
Shield-type fractures
Identification and reduction of the fragments could bedifficult in shield-type fractures as the intact soft tissue acrossthe tuberosities hides the tuberosity and anatomical headfracture lines. We recommend that the primary fracture linebetween the tuberosities (which usually lies 5–10 mm posteriorto the bicipital groove) is first identified with palpation using ablunt instrument and then split sharply with dissecting scissors(Fig. 2(e)). To achieve full visualisation of the head fragment, thisincision may need to be extended proximally to a distance of 1–2 cm into the supraspinatus tendon in line with its fibres,especially if dealing with a case of posterior fracture-dislocation(Fig. 2(f)). Separating the tuberosities then facilitates exposureof the head fragment. Next, multiple high-strength polyethylenesutures are passed as described in the previous section(Fig. 2(g)).
Reduction, fixation and CaSO4 bone-substitute augmentation
After checking the preliminary reduction with an imageintensifier, a proximal humeral locking plate is applied and heldusing a few distal screws, to act as a buttress before injectingCaSO4.
Once the head and neck fragments are anatomically reduced,a metaphyseal void becomes evident. At this point, the CaSO4
(Stimulan, Biocomposites, UK) is prepared and injected underfluoroscopy to ensure adequate filling of the void and toprevent extrusion into the surrounding soft tissues or joint(Fig. 3(h)–(j)).
The remaining locking screws are placed into the proximalhumerus after injecting CaSO4. On an average, we haveplaced five screws proximally into the head and three distallyinto the shaft. The proximal screws were kept 2–4 mm shortof the subchondral bone to minimise the risk of jointpenetration.
DASH Sco
0
10
20
30
40
50
1 2 3 4 5 6 7 8 9 10 11
Pati
Graph
Rotator cuff repair
The rotator cuff and tuberosities are meticulously repaired tothe plate through the suture holes on the plate using high-strengthsutures,17 which have been previously placed into the tuberositiesand the rotator cuff.
Wound closure
Closure of the deltoid proximally is achieved using transosseousnon-absorbable sutures to the acromion. The distal deltoid split isclosed with absorbable sutures.
Postoperative phase
Postoperatively, the arm is placed in a sling and early passiveshoulder stretching and pendulum exercises are started followedby active mobilisation after 6 weeks.
Results
Functional outcomes were assessed with DASH scores18 andmodified Constant and Murley scores by excluding powermeasurements, reducing the maximum total score to 75.19–21
The average follow-up of patients was 24 months. All patients wereassessed for axillary nerve sensation and anterior deltoidcontraction, during the follow-up.
The mean DASH score was 16.18 and the mean modifiedConstant and Murley score was 64.04 (Graphs 2 and 3). Allfractures united with no evidence of infection, failure of fixation,malunion, tuberosity failure, avascular necrosis or adverse reactionto CaSO4. There was no evidence of axillary nerve injury. Eighteenout of twenty-two patients achieved good clinical outcome. Fourpatients had prolonged recovery due to stiffness and associatedinjuries (ipsilateral wrist fracture/elbow dislocation).
res
12 13 14 15 16 17 18 19 20 21 22
ents
2.
Modified Constant & Murley Scores
0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Graph 3.
K. Somasundaram et al. / Injury, Int. J. Care Injured 44 (2013) 481–487 485
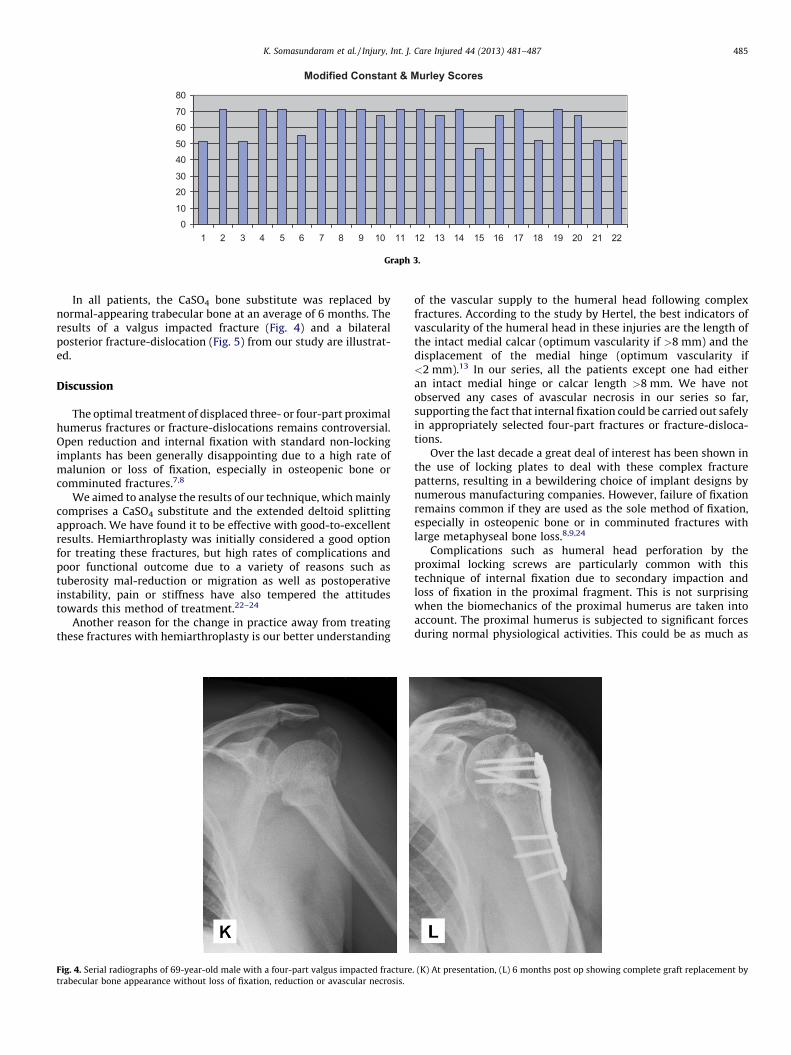
In all patients, the CaSO4 bone substitute was replaced bynormal-appearing trabecular bone at an average of 6 months. Theresults of a valgus impacted fracture (Fig. 4) and a bilateralposterior fracture-dislocation (Fig. 5) from our study are illustrat-ed.
Discussion
The optimal treatment of displaced three- or four-part proximalhumerus fractures or fracture-dislocations remains controversial.Open reduction and internal fixation with standard non-lockingimplants has been generally disappointing due to a high rate ofmalunion or loss of fixation, especially in osteopenic bone orcomminuted fractures.7,8
We aimed to analyse the results of our technique, which mainlycomprises a CaSO4 substitute and the extended deltoid splittingapproach. We have found it to be effective with good-to-excellentresults. Hemiarthroplasty was initially considered a good optionfor treating these fractures, but high rates of complications andpoor functional outcome due to a variety of reasons such astuberosity mal-reduction or migration as well as postoperativeinstability, pain or stiffness have also tempered the attitudestowards this method of treatment.22–24
Another reason for the change in practice away from treatingthese fractures with hemiarthroplasty is our better understanding
Fig. 4. Serial radiographs of 69-year-old male with a four-part valgus impacted fracture
trabecular bone appearance without loss of fixation, reduction or avascular necrosis.
of the vascular supply to the humeral head following complexfractures. According to the study by Hertel, the best indicators ofvascularity of the humeral head in these injuries are the length ofthe intact medial calcar (optimum vascularity if >8 mm) and thedisplacement of the medial hinge (optimum vascularity if<2 mm).13 In our series, all the patients except one had eitheran intact medial hinge or calcar length >8 mm. We have notobserved any cases of avascular necrosis in our series so far,supporting the fact that internal fixation could be carried out safelyin appropriately selected four-part fractures or fracture-disloca-tions.
Over the last decade a great deal of interest has been shown inthe use of locking plates to deal with these complex fracturepatterns, resulting in a bewildering choice of implant designs bynumerous manufacturing companies. However, failure of fixationremains common if they are used as the sole method of fixation,especially in osteopenic bone or in comminuted fractures withlarge metaphyseal bone loss.8,9,24
Complications such as humeral head perforation by theproximal locking screws are particularly common with thistechnique of internal fixation due to secondary impaction andloss of fixation in the proximal fragment. This is not surprisingwhen the biomechanics of the proximal humerus are taken intoaccount. The proximal humerus is subjected to significant forcesduring normal physiological activities. This could be as much as
. (K) At presentation, (L) 6 months post op showing complete graft replacement by
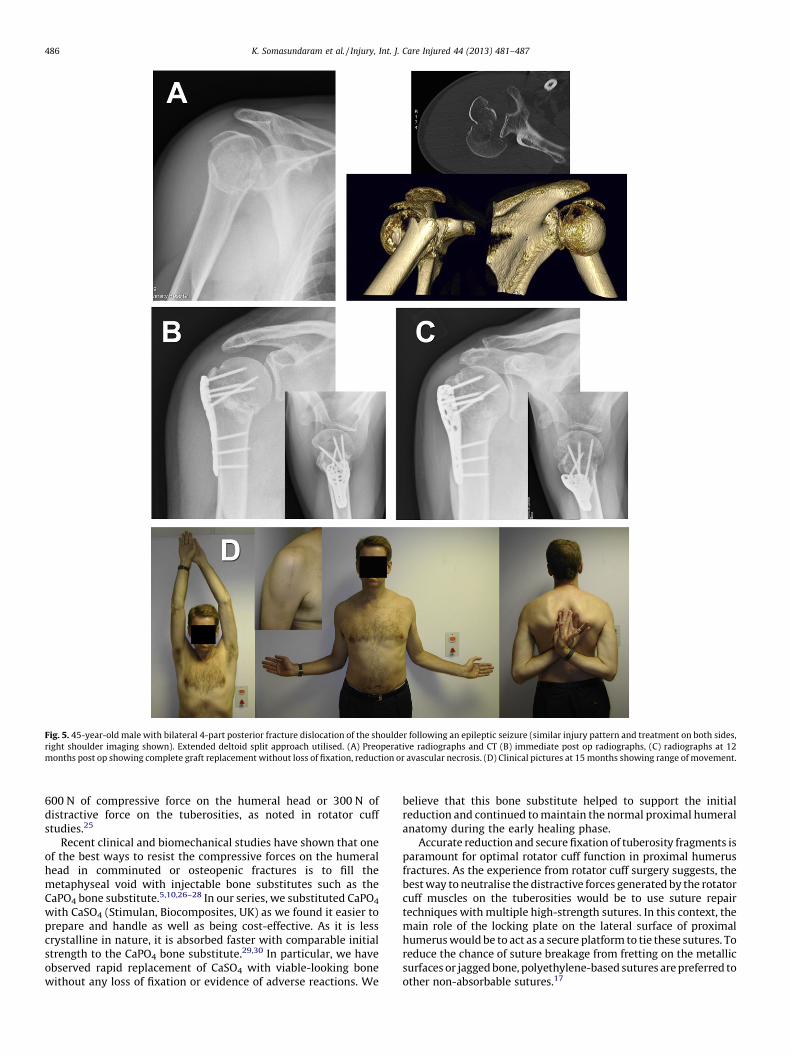
Fig. 5. 45-year-old male with bilateral 4-part posterior fracture dislocation of the shoulder following an epileptic seizure (similar injury pattern and treatment on both sides,
right shoulder imaging shown). Extended deltoid split approach utilised. (A) Preoperative radiographs and CT (B) immediate post op radiographs, (C) radiographs at 12
months post op showing complete graft replacement without loss of fixation, reduction or avascular necrosis. (D) Clinical pictures at 15 months showing range of movement.
K. Somasundaram et al. / Injury, Int. J. Care Injured 44 (2013) 481–487486
600 N of compressive force on the humeral head or 300 N ofdistractive force on the tuberosities, as noted in rotator cuffstudies.25
Recent clinical and biomechanical studies have shown that oneof the best ways to resist the compressive forces on the humeralhead in comminuted or osteopenic fractures is to fill themetaphyseal void with injectable bone substitutes such as theCaPO4 bone substitute.5,10,26–28 In our series, we substituted CaPO4
with CaSO4 (Stimulan, Biocomposites, UK) as we found it easier toprepare and handle as well as being cost-effective. As it is lesscrystalline in nature, it is absorbed faster with comparable initialstrength to the CaPO4 bone substitute.29,30 In particular, we haveobserved rapid replacement of CaSO4 with viable-looking bonewithout any loss of fixation or evidence of adverse reactions. We
believe that this bone substitute helped to support the initialreduction and continued to maintain the normal proximal humeralanatomy during the early healing phase.
Accurate reduction and secure fixation of tuberosity fragments isparamount for optimal rotator cuff function in proximal humerusfractures. As the experience from rotator cuff surgery suggests, thebest way to neutralise the distractive forces generated by the rotatorcuff muscles on the tuberosities would be to use suture repairtechniques with multiple high-strength sutures. In this context, themain role of the locking plate on the lateral surface of proximalhumerus would be to act as a secure platform to tie these sutures. Toreduce the chance of suture breakage from fretting on the metallicsurfaces or jagged bone, polyethylene-based sutures are preferred toother non-absorbable sutures.17

K. Somasundaram et al. / Injury, Int. J. Care Injured 44 (2013) 481–487 487
To further enhance the accuracy of the tuberosity reduction andfixation in displaced four-part fractures and fracture-dislocations,we advocate the use of the extended deltoid-splitting approach.Although we have not observed any cases of iatrogenic axillarynerve injury in our series, we emphasise the importance of carefulnerve isolation and protection throughout the procedure. In ouroperative technique, we have highlighted a number of key steps tominimise the chances of this devastating complication. Havingisolated and protected the nerve with the cuff of the deltoidbetween the two windows and the sling, safe access for fixation isprovided through the proximal and the distal windows.
Our study is the largest reported series of using CaSO4 bonesubstitute in proximal humeral fracture fixation. We performed a2-year follow-up of all our patients with outcome measured bywell-recognised scoring systems. The study comprised sameoperative technique performed by the three senior authorshighlighting the reproducibility of our technique. We understandthe limitations of our retrospective study with a limited number ofpatients. It leads us to the future scope of randomised controlledtrials comparing CaSO4 bone substitute with other substitutes.
In our experience we have found the use of locking plates,injectable CaSO4 bone-substitute augmentation and tuberosityrepair with high-strength sutures as well as the extended deltoid-splitting approach to be a safe and reliable method of internalfixation for complex proximal humeral fractures or fracturedislocations.
Based on our experience with this form of fixation for complexfractures of the proximal humerus, we recommend this techniquethat comprises:
1. A deltoid-splitting approach for more direct access and betterfracture visualisation in displaced four-part fractures andfracture-dislocations.
2. Internal fixation with locking plates and multi-planar screwsstaying short of sub-chondral bone by 2–4 mm.
3. Injectable CaSO4 to fill metaphyseal bone void to preventsecondary fracture collapse.
4. Accurate reduction and secure fixation of the tuberosityfragments with high-strength polyethylene sutures tied to theplate to restore rotator cuff function paving the way for earlyrehabilitation.
Conflict of interest statement
None.
References
1. Kristainsen B, Barfod G, Bredesen J, Erin-Madsen J, Grum B, Horsnaes MW, et al.Epidemiology of proximal humeral fractures. Acta Orthopaedica Scandinavica1987;58(February (1)):75–7. PMID 3577743/doi:10.1080/000164701753542023.
2. Kannus P, Palvanen M, Niemi S, Parkkari J, Jarvinen M, Vuori I. Increasingnumber and incidence of osteoporotic fractures of the proximal humerus inelderly people. BMJ 1996;313(October (7064)):1051–2. PMID 8898596.
3. Robinson CM, Page RS, Hill RM, Sanders DL, Court-Brown CM, Wakefield AE.Primary hemiarthroplasty for treatment of proximal humeral fractures. Journalof Bone and Joint Surgery American Volume 2003;85-A(July (7)):1215–23. PMID12851345.
4. Bosch U, Skutek M, Fremery RW, Tscerene H. Outcome after primary andsecondary hemiarthroplasty in fractures of proximal humeral fractures. Journalof Shoulder and Elbow Surgery 1998;7(September–October (5)):479–84. PMID9814926/doi:10.1016/S1058-2746(98)90198-7.
5. Robinson CM, Page RS. Severely impacted valgus proximal humeral fractures:results of operative treatment. Journal of Bone and Joint Surgery American Volume2003;85-A(September (9)):1647–55. PMID 12954821.
6. Brunner F, Sommer C, Bahrs C, Heuwinkel R, Hafner C, Rillman P, et al. Openreduction and internal fixation of proximal humeral fractures using a proximalhumeral locked plate: a prospective multicenter analysis. Journal of Orthopaedic
Trauma 2009;23(March (3)):163–72. PMID 19516088/doi:10.1097/BOT.0-b013e3185b1920.
7. Solberg BD, Moon CN, Franco DP, Paiement GD. Surgical treatment of three andfour part proximal humeral fractures. Journal of Bone and Joint Surgery AmericanVolume 2009;91(July (7)):1689–97. PMID 19571092/doi:10.2106/JBJS.H.00133.
8. Moonot P, Ashwood N, Hamlet M. Early results for treatment of three and fourpart fractures of humerus using the PHILOS plate system. Journal of Bone andJoint Surgery British Volume 2007;89(September (9)):1206–9. PMID 17905959/doi:10.1302/0301-620X.89B9.18528.
9. Owsley K, Gorczyca JT. Fracture displacement and screw cutout after openreduction and internal fixation proximal humeral fractures. Journal of Bone andJoint Surgery American Volume 2008;90(February (2)):233–40. PMID 18245580/doi:10.2106/JBJS.F.01351.
10. Kwon BK, Goertzen DJ, O’Brien PJ, Broekhuyse HM, Oxland TR. Biomechanicalevaluation of proximal humeral fracture fixation supplemented with calciumphosphate cement. Journal of Bone and Joint Surgery American Volume 2002;84-
A(June (6)):951–61. PMID 12063329.11. Coetzee AS. Regeneration of bone in the presence of calcium sulfate. Archives of
Otolaryngology 1980;106(July (7)):405–9. PMID 7387528.12. Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head
ischemia after intracapsular fracture of the proximal humerus. Journal ofShoulder and Elbow Surgery 2004;13(July–August (4)):427–33. PMID15220884/doi:10.1016/j.jse.2004.01.034.
13. Neer CS. Displaced proximal humeral fractures I. Journal of Bone and JointSurgery American Volume 1970;52(September (6)):1077–89. PMID 5455339.
14. Mackenzie DB. Antero-superior exposure for total shoulder replacement. Jour-nal of Orthopaedic Trauma 1993;2(2):71–7. doi:10.1007/BF02620461.
15. Cetik O, Uslu M, Acar HI, Comert A, Tekdemir I, Cift H. Is there a safe area for theaxillary nerve in the deltoid muscle? A cadaveric study. Journal of Bone and JointSurgery American Volume 2006;88(November (11)):2395–9. PMID 17079396/doi:10.2106/JBJ.S.E.01375.
16. Loukas M, Grabska J, Tubbs RS, Apavdin N, Jordan R. Mapping the axillary nervewithin the deltoid muscle. Surgical and Radiologic Anatomy 2009;31(January(1)):43–7. PMID 18766295/doi:10.1007/s00276-008-0409-3.
17. Wust DM, Meyer DC, Favre P, Gerber C. Mechanical and handling properties ofbraided polyblend polyethylene suture in comparison to braided polyester andmonofilament polydiaxonone sutures. Arthroscopy 2006;22(November (11)).1146-53. PMID 17084288/doi:10.1016/j.arthro.2006.06.013.
18. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremityoutcome measure: the DASH (disabilities of the arm, shoulder and hand).American Journal of Industrial Medicine 1996;29(June (6)):602–8. PMID8773720/doi:10.1002/(SICI)1097-0274(199606)29:6<602:AID-AJIM4>3.0.CO;2-L.
19. Constant CR, Murley AH. A clinical method of functional assessment of theshoulder. Clinical Orthopaedics and Related Research 1987;214(January):160–4.PMID 3791738.
20. Othman A, Taylor G. Manipulation under anesthesia for frozen shoulder.International Orthopaedics 2002;26(5):268–70. PMID 12378350/doi:10.1007/s00264-002-0348.
21. Waszczykowski M, Fabis J. The results of arthroscopic capsular release in thetreatment of frozen shoulder – two year follow up. Ortopedia TraumatologiaRehabilitaija 2010;12(May–June (3)):216–24. PMID 20675863.
22. Antuna SA, Sperling JW, Cofield RH. Shoulder hemiarthroplasty for acutefractures of the proximal humerus, a minimum five year follow-up. Journalof Shoulder and Elbow Surgery 2008;17(March–April (2)):202–9. PMID18248746/doi:10.1016/j.jse.2007.06.025.
23. Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD. Functionaloutcome after humeral head replacement for acute three and four-part proxi-mal humeral fractures. Journal of Shoulder and Elbow Surgery 1995;4(March–April (2)):81–6. PMID 7600169.
24. Babst R, Sommer C, Bahrs C, Heuwinkel R, Hafner C, Rillman P, et al. Openreduction and internal fixation of proximal humeral fractures with a proximalhumeral locked plate: a prospective multicenter analysis. Journal of OrthopaedicTrauma 2009;23(March (3)):163–72. PMID 19516088/doi:10.1097/BOT.0-b013e31920185b.
25. Burkhart SS. A stepwise approach to arthroscopic rotator cuff repair based onbiomechanical principles. Arthroscopy 2000;16(January–February (1)):82–90.PMID 10627351/doi:10.1016/S0749-8063(00)90133-6.
26. Hall MC, Rosser M. The structure of upper end of the humerus with reference toosteoporotic changes in senescence leading to fractures. Canadian MedicalAssociation Journal 1963;88(February (6)):290–4. PMID 20327402.
27. Frankenburg EP, Goldstein SA, Bauer TW, Harris SA, Poser RD. Biomechanicaland histological evaluation of a calcium phosphate cement. Journal of Bone andJoint Surgery American Volume 1998;80:1112–24.
28. Robinson CM, Khan LA, Akhtar MA. Treatment of anterior fracture-dislocationsof the proximal humerus by open reduction and internal fixation. Journal ofBone and Joint Surgery British Volume 2006;88(April (4)):502–8. PMID16567786/doi:10.1302/0301-620X.88B4.17195.
29. Jamali A, Hilpert A, Debes J, Afshar P, Rahban S, Holmes R. Hydroxyapatite/calcium carbonate versus plaster of Paris. A histomorphometric and radio-graphic study in rabbit tibial defect model. Calcified Tissue International2002;71(August (2)):172–8. PMID 12200649/doi:10.1007/s00223-001-1087-x.
30. Beuerlein MJ, McKee MD. Calcium sulfate: what is the evidence? Journal ofOrthopaedic Trauma 2010;24(March (1)):46–51. PMID 20182236/doi:10.1097/BOT.0b013e3181cec48e.