Embed Size (px)
Citation preview
A
aPoatiaw�wt©
K
1
fsaFba
3f
P
0d
International Journal of Antimicrobial Agents 30 (2007) 458–462
Short communication
Pseudomonas aeruginosa infections in the Intensive Care Unit: can theadequacy of empirical �-lactam antibiotic therapy be improved?
Sunil Bhat a, Shigeki Fujitani b, Brian A. Potoski a,c, Blair Capitano a,c,Peter K. Linden b, Kathleen Shutt a, David L. Paterson a,∗
a Division of Infectious Diseases, University of Pittsburgh Medical Center, Pittsburgh, PA, USAb Department of Critical Care Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
c Department of Pharmacy and Therapeutics, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
Received 12 December 2006; accepted 17 May 2007
bstract
Inadequate empirical antibiotic therapy for serious Pseudomonas aeruginosa infections has been linked to increased mortality. We performedretrospective cohort study of consecutive patients with ventilator-associated pneumonia, bacteraemia or other sterile-site infections caused by. aeruginosa occurring during Intensive Care Unit admissions. One hundred and fifty-eight episodes of serious infection with P. aeruginosaccurred in 140 patients. Empirical antibiotic therapy was microbiologically adequate in 67% of episodes of infection. Patients with P.eruginosa isolates resistant to piperacillin/tazobactam or cefepime were more likely to have received these antibiotics in the month prior tohe P. aeruginosa infection or to have had a Gram-negative bacillus resistant to these antibiotics isolated in the month prior to the P. aeruginosanfection. From these data, we have developed simple algorithms for empirical antibiotic choice in seriously ill patients with suspected P.eruginosa infections based on prior antibiotic exposure and prior isolation of antibiotic-resistant organisms. Application of these algorithmsould have improved the adequacy of empirical antibiotic therapy from 67% to 80–84%. Routine empirical addition of amikacin to the
-lactam would have increased the adequacy of the antibiotics to 96%. We conclude that knowledge of the prior receipt of �-lactam antibioticsith activity against P. aeruginosa and the isolation of Gram-negative bacilli resistant to such antibiotics in the recent past can readily increasehe adequacy of empirical antibiotic therapy for suspected P. aeruginosa infections.2007 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved.
py; Int
Gttda
(
eywords: Pseudomonas aeruginosa; Antimicrobial therapy; Empiric thera
. Introduction
�-Lactam, aminoglycoside or fluoroquinolone antibioticsorm the core of empirical antibiotic regimens in most Inten-ive Care Units (ICUs). Aminoglycosides are rarely useds monotherapy for serious infections such as pneumonia.luoroquinolones have been shown to be as good as, or
etter than, �-lactam therapy for infections such as ventilator-ssociated pneumonia (VAP) [1]. However, resistance of∗ Corresponding author. Present address: Suite 3A, Falk Medical Building,601 5th Avenue, Pittsburgh, PA 15213, USA. Tel.: +1 412 648 6478;ax: +1 412 648 6399.
E-mail addresses: [email protected],[email protected] (D.L. Paterson).
titthsir
924-8579/$ – see front matter © 2007 Elsevier B.V. and the International Societyoi:10.1016/j.ijantimicag.2007.05.022
ensive Care Unit
ram-negative bacilli (especially Pseudomonas aeruginosa)o fluoroquinolones has been rising steadily in ICUs acrosshe USA and in many other parts of the world over the lastecade [2]. This has greatly limited the usefulness of thisntibiotic class as empirical therapy.
Thus, piperacillin/tazobactam (PIP/TAZ), cefepimeCEFP), imipenem (IPM) and meropenem have emerged ashe most widely used empirical options for serious infectionsn ICUs. These antibiotics are particularly attractive sincehey have significant antipseudomonal activity and areherefore useful for empirical therapy of VAP. In some
ospitals, use of carbapenem antibiotics is restricted toituations where no other antibiotic options are available. Its likely that this restriction is enforced because of concernsegarding higher drug acquisition costs and the risk ofof Chemotherapy. All rights reserved.

of Antim
tG
hfomwo
2
2
itt(dclwailtat
ovGcdtatdstods
paProtbswd
2
Calwm
3
3
ihpaw31Pd4t9tta
3
c(C(
3
bia((cPPwG
S. Bhat et al. / International Journal
he advent of resistance, particularly in non-fermentativeram-negative bacilli.The work described herein aimed to determine the likeli-
ood of inadequate empirical therapy with PIP/TAZ or CEFPor P. aeruginosa in an institution where carbapenem antibi-tics have been restricted. Furthermore, we aimed to deter-ine whether any simple algorithms could be applied thatould help to optimise empirical antibiotic therapy for seri-usly ill patients while maintaining diversity of antibiotic use.
. Methods
.1. Subjects and isolates
Pseudomonas aeruginosa infections occurring in patientsn ICUs in a tertiary referral centre from 1 January 2003o 31 December 2003 were identified. Only serious infec-ions, defined as those isolated from a normally sterile siteblood, cerebrospinal fluid (CSF), pleural fluid collectedirectly from a pleural fluid aspiration and peritoneal fluidollected directly during surgery) or from bronchoalveolaravage (BAL) (as long as more than 10 000 organisms/mLere present) were assessed. Consecutive infections were
ssessed and no records were missing. Antibiotic susceptibil-ty of the isolates was determined by the clinical microbiologyaboratory using microbroth dilution (for blood and CSF cul-ures) or disk diffusion (for all other sites). Interpretation ofntibiotic susceptibility was according to the guidelines ofhe Clinical and Laboratory Standards Institute [3].
The electronic medical records of the patients who devel-ped these infections were reviewed for the followingariables: receipt of antibiotics potentially active againstram-negative bacilli in the 30 days prior to the date of
ollection of the P. aeruginosa isolate (for the purpose ofetermining the impact of prior antibiotic use on the suscep-ibility of P. aeruginosa); receipt of antibiotics potentiallyctive against Gram-negative bacilli on the day on whichhe P. aeruginosa isolate was isolated and for 13 subsequentays (to determine the empirical therapy received); and theusceptibility profile of Gram-negative bacilli collected fromhe patient from any site during the 30 days prior to the datef collection of the P. aeruginosa isolate (for the purpose ofetermining the predictive effect of antibiotic resistance onubsequent P. aeruginosa isolates).
All information was collected for quality assurance pur-oses by the hospital’s Antibiotic Management Program tossess the impact of restrictions of antibiotics in the ICU.IP/TAZ, aminoglycosides and CEFP were available withoutestriction in ICUs during 2003, whilst carbapenems, aztre-nam and quinolones were only available after approval fromhe hospital’s Antibiotic Management Program. Use of car-
apenems had been restricted to Infectious Disease approvalince around 1996. The approved indication for carbapenemsas detection of Gram-negative organisms resistant to otherrug classes.ai1
icrobial Agents 30 (2007) 458–462 459
.2. Statistics
Data were entered into an Excel database (Microsoftorp.). Relationships between antibiotic resistance in P.eruginosa and prior use of PIP/TAZ or CEFP or prior iso-ation of PIP/TAZ- or CEFP-resistant Gram-negative bacilliere determined using the normal approximation to the bino-ial distribution.
. Results
.1. Isolates
One hundred and fifty-eight episodes of serious P. aerug-nosa infection were recorded in 140 patients (13 patientsad two episodes, 1 patient had three episodes and 1atient had four episodes) over the 1-year duration of thisssessment. The isolates responsible for these infectionsere from BAL (102/158; 64.6%), blood cultures (50/158;1.6%), pleural fluid (3/158; 1.9%), peritoneal fluid (2/158;.3%) and CSF (1/158; 0.6%). The percentages of the 158. aeruginosa isolates lacking susceptibility to antipseu-omonal antibiotics were: aztreonam, 51%; levofloxacin,2%; ciprofloxacin, 37%; PIP/TAZ, 27%; CEFP, 26%; gen-amicin, 26%; tobramycin, 20%; IPM, 18%; and amikacin,%. Fifty-four isolates (34.2%) were susceptible to all ofhese antibiotics, whereas four (2.5%) were resistant to all ofhese antibiotics and nine (5.7%) were resistant to all but onentibiotic.
.2. Cross-resistance
Isolates resistant to PIP/TAZ, CEFP or IPM had a >75%hance of being resistant to levofloxacin and ciprofloxacinTable 1). In contrast, <50% of isolates resistant to PIP/TAZ,EFP or IPM were resistant to tobramycin or amikacin
Table 1).
.3. Predictors of resistance to PIP/TAZ
Sixty-eight (43%) of 158 episodes had been precededy use of PIP/TAZ in the month prior to the P. aeruginosanfection, 37% (25/68) of whom had a PIP/TAZ-resistant P.eruginosa strain causing this infection compared with 20%18/90) who had not been documented as receiving PIP/TAZP = 0.0191). Thirty-three (21%) of 158 episodes were pre-eded by isolation of a Gram-negative bacillus resistant toIP/TAZ, 64% (21/33) of whom were now infected with aIP/TAZ-resistant strain compared with 18% (22/125) whoere never known to be infected with a PIP/TAZ-resistantram-negative bacillus (P < 0.0001).
Of the 43 patients (27%) with a PIP/TAZ-resistant P.eruginosa isolate, 12 had prior use of PIP/TAZ and priorsolation of a PIP/TAZ-resistant Gram-negative bacillus,3 had prior use of PIP/TAZ but no prior isolation of a
460 S. Bhat et al. / International Journal of Antimicrobial Agents 30 (2007) 458–462
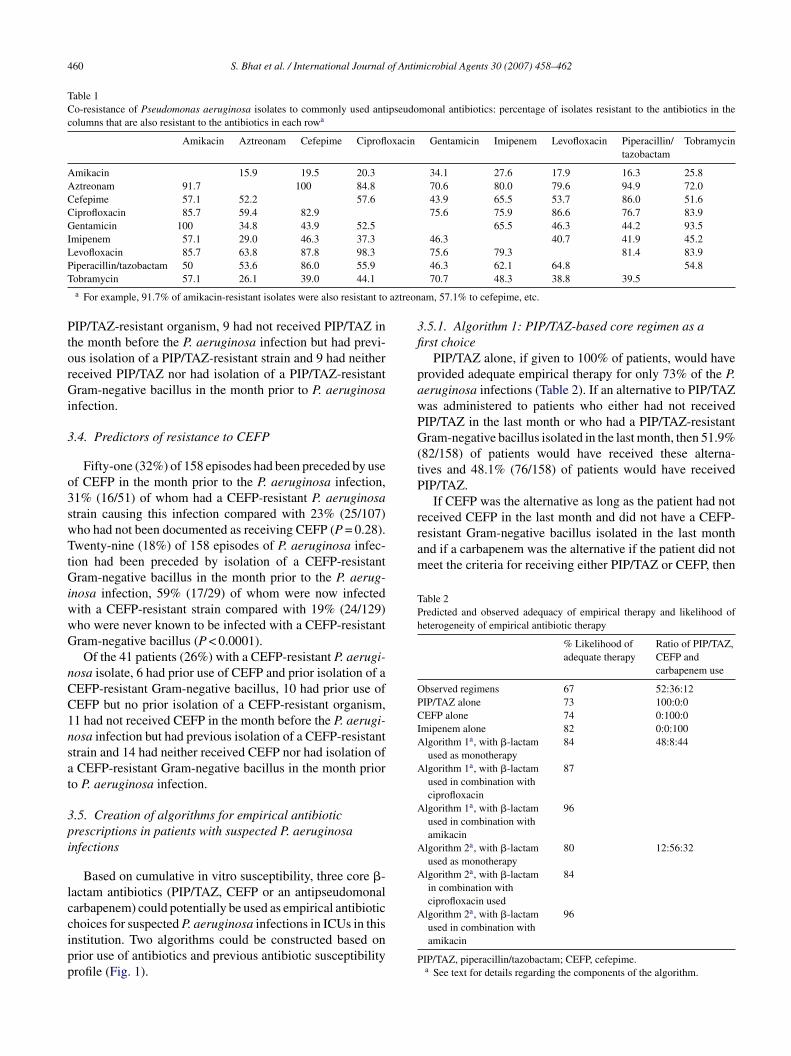
Table 1Co-resistance of Pseudomonas aeruginosa isolates to commonly used antipseudomonal antibiotics: percentage of isolates resistant to the antibiotics in thecolumns that are also resistant to the antibiotics in each rowa
Amikacin Aztreonam Cefepime Ciprofloxacin Gentamicin Imipenem Levofloxacin Piperacillin/tazobactam
Tobramycin
Amikacin 15.9 19.5 20.3 34.1 27.6 17.9 16.3 25.8Aztreonam 91.7 100 84.8 70.6 80.0 79.6 94.9 72.0Cefepime 57.1 52.2 57.6 43.9 65.5 53.7 86.0 51.6Ciprofloxacin 85.7 59.4 82.9 75.6 75.9 86.6 76.7 83.9Gentamicin 100 34.8 43.9 52.5 65.5 46.3 44.2 93.5Imipenem 57.1 29.0 46.3 37.3 46.3 40.7 41.9 45.2Levofloxacin 85.7 63.8 87.8 98.3 75.6 79.3 81.4 83.9PT
aztreon
PtorGi
3
o3swTtGiwwG
nCC1nsat
3pi
lccipp
3fi
pawPG(tP
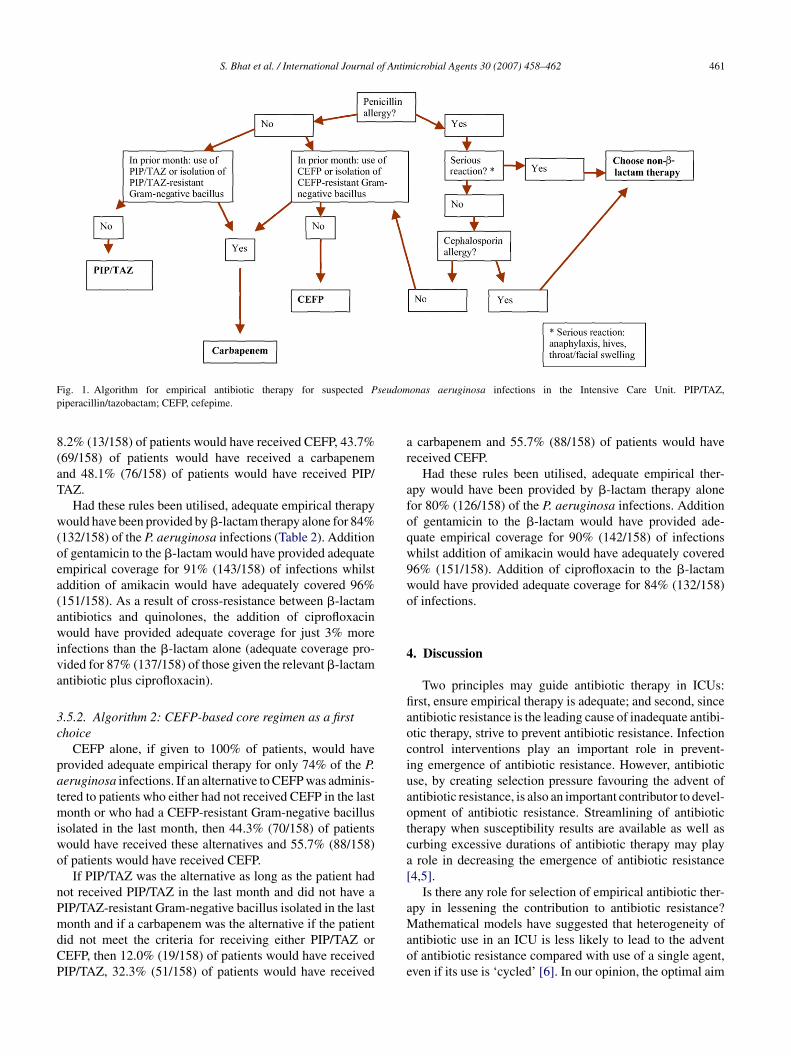
received CEFP in the last month and did not have a CEFP-resistant Gram-negative bacillus isolated in the last monthand if a carbapenem was the alternative if the patient did notmeet the criteria for receiving either PIP/TAZ or CEFP, then
Table 2Predicted and observed adequacy of empirical therapy and likelihood ofheterogeneity of empirical antibiotic therapy
% Likelihood ofadequate therapy
Ratio of PIP/TAZ,CEFP andcarbapenem use
Observed regimens 67 52:36:12PIP/TAZ alone 73 100:0:0CEFP alone 74 0:100:0Imipenem alone 82 0:0:100Algorithm 1a, with �-lactam
used as monotherapy84 48:8:44
Algorithm 1a, with �-lactamused in combination withciprofloxacin
87
Algorithm 1a, with �-lactamused in combination withamikacin
96
Algorithm 2a, with �-lactamused as monotherapy
80 12:56:32
Algorithm 2a, with �-lactamin combination withciprofloxacin used
84
iperacillin/tazobactam 50 53.6 86.0 55.9obramycin 57.1 26.1 39.0 44.1a For example, 91.7% of amikacin-resistant isolates were also resistant to
IP/TAZ-resistant organism, 9 had not received PIP/TAZ inhe month before the P. aeruginosa infection but had previ-us isolation of a PIP/TAZ-resistant strain and 9 had neithereceived PIP/TAZ nor had isolation of a PIP/TAZ-resistantram-negative bacillus in the month prior to P. aeruginosa
nfection.
.4. Predictors of resistance to CEFP
Fifty-one (32%) of 158 episodes had been preceded by usef CEFP in the month prior to the P. aeruginosa infection,1% (16/51) of whom had a CEFP-resistant P. aeruginosatrain causing this infection compared with 23% (25/107)ho had not been documented as receiving CEFP (P = 0.28).wenty-nine (18%) of 158 episodes of P. aeruginosa infec-
ion had been preceded by isolation of a CEFP-resistantram-negative bacillus in the month prior to the P. aerug-
nosa infection, 59% (17/29) of whom were now infectedith a CEFP-resistant strain compared with 19% (24/129)ho were never known to be infected with a CEFP-resistantram-negative bacillus (P < 0.0001).Of the 41 patients (26%) with a CEFP-resistant P. aerugi-
osa isolate, 6 had prior use of CEFP and prior isolation of aEFP-resistant Gram-negative bacillus, 10 had prior use ofEFP but no prior isolation of a CEFP-resistant organism,1 had not received CEFP in the month before the P. aerugi-osa infection but had previous isolation of a CEFP-resistanttrain and 14 had neither received CEFP nor had isolation ofCEFP-resistant Gram-negative bacillus in the month prior
o P. aeruginosa infection.
.5. Creation of algorithms for empirical antibioticrescriptions in patients with suspected P. aeruginosanfections
Based on cumulative in vitro susceptibility, three core �-actam antibiotics (PIP/TAZ, CEFP or an antipseudomonalarbapenem) could potentially be used as empirical antibiotic
hoices for suspected P. aeruginosa infections in ICUs in thisnstitution. Two algorithms could be constructed based onrior use of antibiotics and previous antibiotic susceptibilityrofile (Fig. 1).A
P
46.3 62.1 64.8 54.870.7 48.3 38.8 39.5
am, 57.1% to cefepime, etc.
.5.1. Algorithm 1: PIP/TAZ-based core regimen as arst choice
PIP/TAZ alone, if given to 100% of patients, would haverovided adequate empirical therapy for only 73% of the P.eruginosa infections (Table 2). If an alternative to PIP/TAZas administered to patients who either had not receivedIP/TAZ in the last month or who had a PIP/TAZ-resistantram-negative bacillus isolated in the last month, then 51.9%
82/158) of patients would have received these alterna-ives and 48.1% (76/158) of patients would have receivedIP/TAZ.
If CEFP was the alternative as long as the patient had not
lgorithm 2a, with �-lactamused in combination withamikacin
96
IP/TAZ, piperacillin/tazobactam; CEFP, cefepime.a See text for details regarding the components of the algorithm.
S. Bhat et al. / International Journal of Antimicrobial Agents 30 (2007) 458–462 461
F seudomp
8(aT
w(oea(awiva
3c
patmiwo
nPmdCP
ar
afoqw9wo
4
fiaociuaotca[
a
ig. 1. Algorithm for empirical antibiotic therapy for suspected Piperacillin/tazobactam; CEFP, cefepime.
.2% (13/158) of patients would have received CEFP, 43.7%69/158) of patients would have received a carbapenemnd 48.1% (76/158) of patients would have received PIP/AZ.
Had these rules been utilised, adequate empirical therapyould have been provided by �-lactam therapy alone for 84%
132/158) of the P. aeruginosa infections (Table 2). Additionf gentamicin to the �-lactam would have provided adequatempirical coverage for 91% (143/158) of infections whilstddition of amikacin would have adequately covered 96%151/158). As a result of cross-resistance between �-lactamntibiotics and quinolones, the addition of ciprofloxacinould have provided adequate coverage for just 3% more
nfections than the �-lactam alone (adequate coverage pro-ided for 87% (137/158) of those given the relevant �-lactamntibiotic plus ciprofloxacin).
.5.2. Algorithm 2: CEFP-based core regimen as a firsthoice
CEFP alone, if given to 100% of patients, would haverovided adequate empirical therapy for only 74% of the P.eruginosa infections. If an alternative to CEFP was adminis-ered to patients who either had not received CEFP in the lastonth or who had a CEFP-resistant Gram-negative bacillus
solated in the last month, then 44.3% (70/158) of patientsould have received these alternatives and 55.7% (88/158)f patients would have received CEFP.
If PIP/TAZ was the alternative as long as the patient hadot received PIP/TAZ in the last month and did not have aIP/TAZ-resistant Gram-negative bacillus isolated in the last
onth and if a carbapenem was the alternative if the patientid not meet the criteria for receiving either PIP/TAZ orEFP, then 12.0% (19/158) of patients would have receivedIP/TAZ, 32.3% (51/158) of patients would have received
Maoe
onas aeruginosa infections in the Intensive Care Unit. PIP/TAZ,
carbapenem and 55.7% (88/158) of patients would haveeceived CEFP.
Had these rules been utilised, adequate empirical ther-py would have been provided by �-lactam therapy aloneor 80% (126/158) of the P. aeruginosa infections. Additionf gentamicin to the �-lactam would have provided ade-uate empirical coverage for 90% (142/158) of infectionshilst addition of amikacin would have adequately covered6% (151/158). Addition of ciprofloxacin to the �-lactamould have provided adequate coverage for 84% (132/158)f infections.
. Discussion
Two principles may guide antibiotic therapy in ICUs:rst, ensure empirical therapy is adequate; and second, sincentibiotic resistance is the leading cause of inadequate antibi-tic therapy, strive to prevent antibiotic resistance. Infectionontrol interventions play an important role in prevent-ng emergence of antibiotic resistance. However, antibioticse, by creating selection pressure favouring the advent ofntibiotic resistance, is also an important contributor to devel-pment of antibiotic resistance. Streamlining of antibioticherapy when susceptibility results are available as well asurbing excessive durations of antibiotic therapy may playrole in decreasing the emergence of antibiotic resistance
4,5].Is there any role for selection of empirical antibiotic ther-
py in lessening the contribution to antibiotic resistance?
athematical models have suggested that heterogeneity ofntibiotic use in an ICU is less likely to lead to the adventf antibiotic resistance compared with use of a single agent,ven if its use is ‘cycled’ [6]. In our opinion, the optimal aim

4 of Antim
oam
patgcWoa�wqwi
attiootarrrhwp
aosesieoebiqatom
lbc
drpoplrimt
WWssd
R
[
[
[
[
[
[
1997;94:12106–11.[7] El Amari EB, Chamot E, Auckenthaler R, Pechere JC, Van Delden C.
62 S. Bhat et al. / International Journal
f an empirical antibiotic policy in the ICU would be to ensuredequacy of empirical antibiotic choice and, if possible, toaintain heterogeneity of empirical antibiotic choice.In many hospitals, such as our own, antibiotic restriction
olicies are in place. Such policies may be useful to limitdministration of frequently misused therapies. However,here is also a risk in some settings of inhibiting hetero-eneity of empirical antibiotic choice as well as reducing thehance that empirical therapy is microbiologically adequate.e found that empirical therapy was adequate in only 67%
f episodes of serious infection with P. aeruginosa in ICUst our institution (Table 2). Eighty-eight percent of empirical-lactam use was with PIP/TAZ or CEFP. Both antibioticsere not subject to restriction in ICUs at the time of thisuality assurance project. In view of this, we investigatedhether empirical antibiotic choice could be improved in our
nstitution.Previous studies have suggested that prior use of an
ntipseudomonal antibiotic was a risk factor for resistance tohat antibiotic in P. aeruginosa bacteraemia [7]. We thereforeheorised that this would hold true in other serious P. aerug-nosa infections such as VAP. Our findings supported thesebservations. Patients who had previously received PIP/TAZr CEFP were more likely to have P. aeruginosa resistant tohe antibiotic that they had received. Additionally, there wasstriking association between prior isolation of an organism
esistant to PIP/TAZ or CEFP and isolation of P. aeruginosaesistant to these antibiotics. In a minority of patients, neitherisk factor for antibiotic resistance was identifiable. This mayave been the result of antibiotic use in the remote past (whiche did not record), antibiotic use in outside institutions orerson-to-person spread of antibiotic-resistant strains.
Using knowledge of these risk factors, we were able to cre-te simple algorithms that could have improved the adequacyf empirical antibiotic therapy in our ICUs. Furthermore,uch algorithms would have maintained or increased het-rogeneity of antibiotic use. There is unlikely to be anyuperiority of the PIP/TAZ- or CEFP-based algorithm. Leav-ng choice of algorithm open to physician preference forither antibiotic may also aid in heterogeneity of antibi-tic choice while maintaining high levels of adequacy ofmpirical therapy. Importantly, empirical availability of car-apenems (as dictated by the algorithm) appears to havencreased the chance that empirical therapy would be ade-uate. Empirical combination of a �-lactam antibiotic with
n aminoglycoside or a fluoroquinolone would also increasehe adequacy of empirical regimens (Table 2). Additionf aminoglycosides appears to be more likely to increaseicrobiological adequacy since co-resistance between �-icrobial Agents 30 (2007) 458–462
actam antibiotics and quinolones was more frequent thanetween �-lactam antibiotics and aminoglycosides (espe-ially amikacin).
A criticism of our approach is that it has not been vali-ated prospectively. A number of variables, such as failure ofecognition of the possibility of a P. aeruginosa infection, theresence of penicillin allergy, renal dysfunction, recent onsetf seizures or changes in institutional antibiotic susceptibilityrofiles, may reduce the adequacy of empirical therapy fromevels that we have predicted. We have incorporated our algo-ithms into an order set for suspected VAP in an attempt tomprove the adequacy of empirical antibiotic therapy while
aintaining antibiotic diversity. The effectiveness of usinghis order set is currently under study.
Funding: None.Competing interests: Brian Potoski: speaker’s bureau
yeth; grant support Pfizer. Blair Capitano: speaker’s bureauyeth. Peter Linden: speaker’s bureau Enzon. David Pater-
on: grant support from AstraZeneca, Merck and Elan;peaker’s bureau of Merck and Cubist. All other authorseclared no competing interests.
Ethical approval: Not required.
eferences
1] Fink MP, Snydman DR, Niederman MS, et al. Treatment of severepneumonia in hospitalized patients: results of a multicenter, ran-domized, double-blind trial comparing intravenous ciprofloxacin withimipenem–cilastatin. The Severe Pneumonia Study Group. AntimicrobAgents Chemother 1994;38:547–57.
2] Neuhauser MM, Weinstein RA, Rydman R, Danziger LH, KaramG, Quinn JP. Antibiotic resistance among gram-negative bacilli inUS intensive care units: implications for fluoroquinolone use. JAMA2003;289:885–8.
3] National Committee for Clinical Laboratory Standards. Performancestandards for antimicrobial susceptibility testing. Fourteenth Informa-tional Supplement. Wayne, PA: NCCLS; 2004.
4] Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibi-otic therapy for ventilator-associated pneumonia in adults: a randomizedtrial. JAMA 2003;290:2588–98.
5] Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-courseempiric antibiotic therapy for patients with pulmonary infiltrates in theintensive care unit. A proposed solution for indiscriminate antibioticprescription. Am J Respir Crit Care Med 2000;162:505–11.
6] Bonhoeffer S, Lipsitch M, Levin BR. Evaluating treatment pro-tocols to prevent antibiotic resistance. Proc Natl Acad Sci USA
Influence of previous exposure to antibiotic therapy on the susceptibilitypattern of Pseudomonas aeruginosa bacteremic isolates. Clin Infect Dis2001;33:1859–64.





























