Embed Size (px)
Citation preview

FedericoBardazziResponsabileAmbulatorioPsoriasiSevereU.O.Dermatologia,PoliclinicoS.OrsolaMalpighi
Bologna
Psoriasi e Nutrizione: esistono cibi che la influenzano?

Cibo e psoriasi: relazione pericolosa?

Nel 2025 si s;mano 20 milioni di obesi

Anche se almeno in questo ancora ce la caviamo…
Associazione Internazionale di dermatologia ecologica
Anche se ancora ce la caviamo…

TuBavia anche in Italia hanno preso piede numerose diete alla moda
DietadelminestroneDietaazona Dietadissociata
DietadellearanceDietaDukan DietaLemme

E’ sempre più streBo e dimostrato il rapporto tra cibo e salute
Associazione Internazionale
di dermatologia ecologica
E’ sempre più stretto e dimostrato il legame che unisce il concetto di CIBO a quello di SALUTE
Associazione Internazionale
di dermatologia ecologica
E’ sempre più stretto e dimostrato il legame che unisce il concetto di CIBO a quello di SALUTE
Associazione Internazionale
di dermatologia ecologica
E’ sempre più stretto e dimostrato il legame che unisce il concetto di CIBO a quello di SALUTE
Associazione Internazionale
di dermatologia ecologica
E’ sempre più stretto e dimostrato il legame che unisce il concetto di CIBO a quello di SALUTE

Nutrizione e psoriasi
Associazione Internazionale di dermatologia ecologica
Associazione Internazionale di dermatologia ecologica

Psoriasi e sindrome metabolica • Spessopersemplificaresiparladiobesita,mainrealtalasindromemetabolicaèunapatologiaasé,unpo’piucomplessa
• E’caraHerizzatada:1. aumentodellacirconferenzadell’addome(superiorea88cmnelle
donneea102negliuomini),2. ipertensionearteriosa,3. ipertrigliceridemia(oltre150milligrammiditrigliceridiperdecilitro
disangue),4. rido;livellidicolesterolo“buono”HDL(menodi50nelle
femminee40neimaschi)5. aumentodellaglicemia(maggioredi100).
• Sesihannoanchesolotresucinquediquestecara0eris1chesisoffredisindromemetabolicaeipazienSconquestamalaUahannounrischioduevoltesuperioreallanormadimala]acoronarica,ictus,diabeteealcuniSpiditumori.
• Iricercatorihannoappuratochequasiil27percentodegliitalianipsoriasicipartecipanSallaloroindaginesoffrivadisindromemetabolica(controil15percentodeinonpsoriasici)echefralorolelesionidellapelleeranodiformapiusevera.

Insulinoresistenza
• LacirconferenzaaddominaleèconsideratofaHoreprediUvodiinsulino-resistenzasesuperiorea100cminentrambiisessi.
• Siparladiinsulino-resistenzaquandolecelluledell'organismodiminuisconolapropriasensibilitàall'azionedell’insulina;
• Ricordiamo,brevemente,chel'insulinaèunormoneessenzialeperconsenSreilpassaggiodelglucosiodalsangueallecellule,impedendochelasuaconcentrazioneemaSca(glicemia)sialzitroppo.
Diabete(comunementeosservatonelpzpsoriasico!)
Associazione Internazionale
di dermatologia ecologica
INSULINORESISTENZA
E la circonferenza addominale è considerato fattore predittivo di insulino-resistenza se superiore a 100cm in entrambi i sessi

Perche sindrome metabolica e psoriasi si associano?
• Lapsoriasièunapatologiainfiammatoriadellapelleelasindromemetabolicaèunacondizionechefavoriscel’infiammazionesistemicadell’organismo,invarimodieavarilivelliproducedellesostanzepro-infiammatorie.
• E’moltoimportanteunapproccioterapeuScoglobaledadedicarealpazienteconpsoriasi:ovverochel’obieUvosianonsoloatraHarelapatologiacutanea,maancheaprevenireoridurrelealtremalaUecorrelate,compresal’aHenzioneall’alimentazione.

All’aumento delle riserve energe;che segue una risposta cellulare da parte dell’adipocita che rilascia proteine
biologicamente aIve nell’infiammazione •LEPTINA(ormonecheinviasegnaledisazietaall’ipotalamoeregolaladistribuzionedeltessutoadiposo)•TNF-alfa(FactorediNecrosi)•Interleuchina6•CRP(proteinaCreaUva)
Associazione Internazionale
di dermatologia ecologica
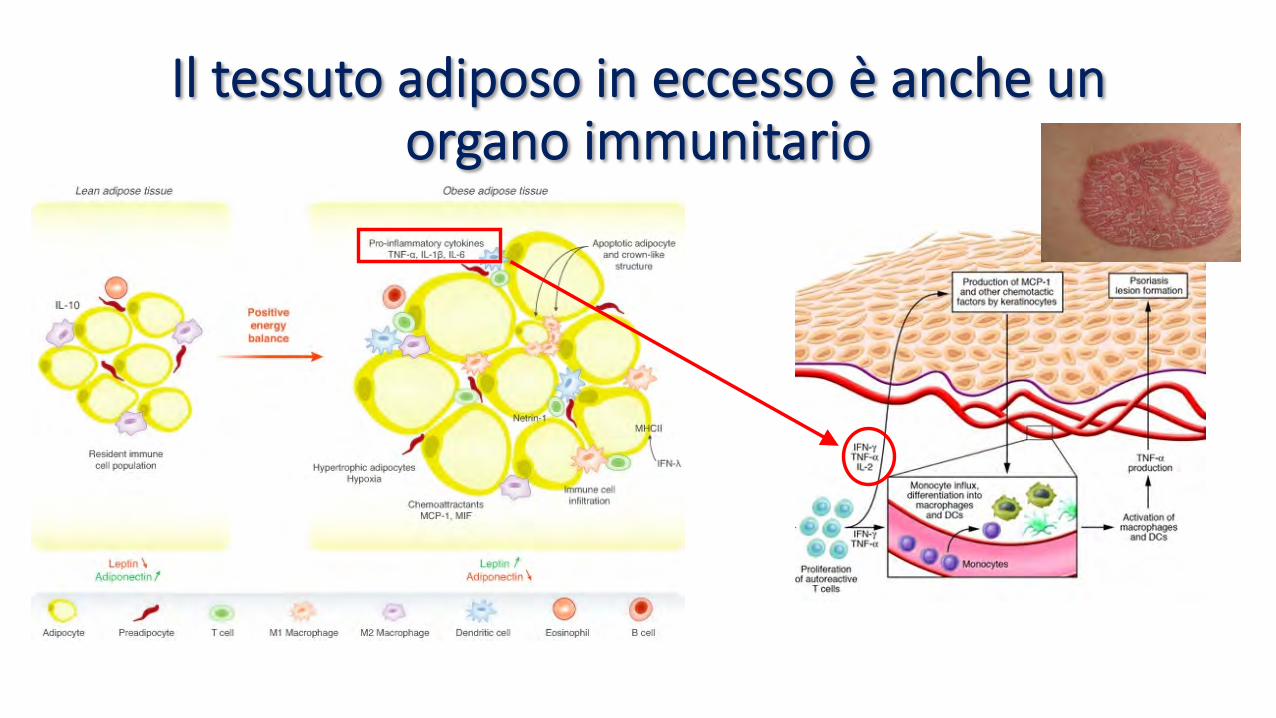
Il tessuto adiposo in eccesso è anche un organo immunitario
Lo stress ossida;vo • LostressossidaDvoèunacondizionepatologicacausatadallaroHuradell'equilibriofisiologico,inunorganismovivente,fralaproduzioneel'eliminazione,dapartedeisistemididifesaanSossidanS,dispeciechimicheossidanS.
• LespecieossidanSeiradicaliliberisvolgonoimportanSssimiruolifisiologici,qualiladifesaneiconfronSdeibaHeri,latrasmissionedeisegnalibiochimicifralecellule,ilcontrollodellapressionearteriosaecc.
• Èperòilloroeccesso,generalmenteriferitoaunaopiùclassidiossidanS,aessereimplicatonellostressossidaSvo,oggiritenutoassociatoaoltrecentopatologieumane(qualidiabetemellito,fibroblasiaretrolenScolare,malaUadiAlzheimer,aterosclerosi,ipertensionearteriosa,malaUadiParkinsonetc.),epotrebbeinoltreessereimportantenelprocessodiinvecchiamento.

Associazione Internazionale
di dermatologia ecologica

Stress ossida;vo e psoriasi

Ma quindi cosa dobbiamo mangiare?

La dieta mediterranea: ancora aBuale
• IlDoH.AncelKeys,neglianni‘50,vivevanelnostromeravigliosoCilento(doveèrimastoper40anni!),aPioppi,unpaesinodi500abitanS,tuUincredibilmentesanielongevi.
• Ilmedicointuiscechei"poveri"deipaesinisperduSdelSudItalia,quellichemangiavanoancorapane,pasta,legumiepomodoro,eranomoltopiusaninonsolodeiciHadinidiNewYork,maanchedeilorostessiparenSemigraSormaidatemponegliStaSUniS.
Associazione Internazionale
di dermatologia ecologica
IlDoC.AncelKeys,neglianni‘50,vivevanelnostromeravigliosoCilento(doveèrimasto
per40anni!),aPioppi,unpaesinodi500abitanX,tu]incredibilmentesanielongevi.
IldoCintuiscecheI"poveri"deipaesinisperduXdelSudItalia,quellichemangiavano
ancorapane,pasta,legumiepomodoro,
eranomoltopiùsaninonsolodeiciCadinidiNewYork,maanchedeilorostessiparenX
emigraXormaidatemponegliStaXUniX.
IL PADRE DELLA DIETA MEDITERRANEA E’ UN AMERICANO…

In pra;ca intuisce la principale differenza
tra Europa e Usa
Associazione Internazionale di dermatologia ecologica
Associazione Internazionale di dermatologia ecologica
Associazione Internazionale di dermatologia ecologica
Associazione Internazionale di dermatologia ecologica
Associazione Internazionale di dermatologia ecologica

La dieta mediterranea oggi
Associazione Internazionale
di dermatologia ecologica
LAPIRAMIDEALIMENTARE:Lineeguida
Quellacheoggiciappareunasceltaobbligataperguadagnareinsalute,inseguiScomesiamodalterrorediipertensione,diabete,tumori,untempoloerapermoSviopposS:lemalaUedelbenessereeranosconosciuteaipiusemplicementepercheilbenessereeraunlusso,epersopravviverecisidovevaaccontentaredeglialimenSpiupoveriadisposizione,ovvero,farinegrezze,verdure,legumi,formaggi,pesce,(poveroanchelui)

E per uno psoriasico?
• E’statoscriHomolSssimosulruolodelladietanellapsoriasi,sebbenealcuniargomenSsianoancoraoggeHodidiscussione.CisonotuHaviaalcunecertezze…

1) La perdita di peso migliora la psoriasi
psoriasis improvement associated with gastricbypass surgery may not necessarily be caused bythe resulting decrease in weight, but perhaps causedby the hypersecretion of gut incretin hormoneglucagon-like peptide-1 that occurs after surgery.Interestingly, although glucagon-like peptide-1 hasbeen shown to reduce appetite and gastrointestinalmotility, it may also have anti-inflammatory effectsthat could contribute to psoriasis improvement aftergastric bypass surgery. This could explain improve-ment in psoriasis that is seen immediately aftersurgery and before substantial weight loss isachieved.
In summary, although gastric bypass is nottypically used as a first-line treatment for psoriasisalone, patients who undergo gastric bypass surgeryfor other indications may experience psoriasisimprovement. The exact mechanism of this improve-ment has yet to be determined.
DISCUSSIONThe effects of weight loss on psoriasis are of great
interest to physicians and patients alike. This reviewof the literature indicates elevated BMI is associatedwith increased psoriasis incidence and severity anddiminished therapeutic effect of certain medications.Interestingly, the effects of BMI on psoriasis maydepend on a person’s genetics: a recent study by Liet al40 found that the risk of developing psoriasis wasinfluenced by the interaction of BMI with 2 variantsin the IL12B and IL23R genes. This suggests that agene-environment interaction could play an impor-tant role in the development of psoriasis.41
Based on the studies cited, a BMI greater than 30kg/m2may potentially play a role in patients’ abilitiesto achieve the full therapeutic effect of psoriasistherapy. This could be for 2 possible reasons: it maybe a consequence of decreased drug distribution intothe body as a result of increased body mass, or it maybe a consequence of increased proinflammatorycytokine release as a result of increased adipocytecount. Given the potential correlation betweenelevated BMI with increasing psoriasis severity,weight loss has been considered as a potentialadjunct to other psoriasis therapies.
We found several prospective, controlled studiesexamining the impact of weight loss on psoriasis orpsoriatic arthritis. Weight loss in overweight or obesesubjects, through decreased caloric intake, appearsto have an added beneficial effect on psoriasis orpsoriatic arthritis when used in conjunction withother prescription medications. Interestingly, studieshave shown that caloric restriction in obese subjectslowers the level of circulating inflammatory cyto-kines.25,42 This may contribute to the observed
beneficial effect in psoriatic disease. Dietary weightloss may certainly be recommended as a lifestylechange by dermatologists for overweight and obesepatients with psoriasis. The evidence to support thisis currently graded as level IB, signifying evidencefrom at least 1 randomized controlled trial (Table I).
In addition, gastric bypass surgery is emerging asan intriguing treatment option and may be second-arily beneficial for psoriasis when performed forother medical conditions. Decreased need for treat-ment and general improvement of patients’ psoriasishave been reported in several case studies and arecent retrospective study.33-38 Similar to a hypo-caloric diet, it is an illustrative example of howweight loss may lead to psoriasis improvement.
ConclusionA number of studies suggest that weight loss may
be a useful preventative and adjunctive therapy forthe treatment of psoriasis or psoriatic arthritis. Gastricbypass surgery appears to be beneficial in selectpatients. However, additional larger, prospectiveclinical studies are needed to further delineate theefficacy of diet and weight loss interventions inpsoriasis improvement. Given the vast body ofpopular literature available to patients, it is importantfor clinical providers to familiarize themselves withthe evidence supporting various dietary plans.By doing so, they will be able to engage theirpatients and partner with them to maximize theimpact of pharmacologic and nonpharmacologicinterventions.
REFERENCES1. Koo J. Population-based epidemiologic study of psoriasis with
emphasis on quality of life assessment. Dermatol Clin 1996;14:485-96.
2. Stern RS. Psoriasis. Lancet 1997;350:349-53.3. Davidovici BB, Sattar N, Prinz JC, J€org PC, Puig L, Emery P, et al.
Psoriasis and systemic inflammatory diseases: potential mech-anistic links between skin disease and co-morbid conditions.J Invest Dermatol 2010;130:1785-96.
4. Sumarac-Dumanovic M, Stevanovic D, Ljubic A, Jorga J, SimicM, Stamenkovic-Pejkovic D, et al. Increased activity ofinterleukin-23/interleukin-17 proinflammatory axis in obesewomen. Int J Obes (Lond) 2009;33:151-6.
5. Choi J, Koo JY. Quality of life issues in psoriasis. J Am AcadDermatol 2003;49(Suppl):S57-61.
6. Wolk K, Mallbris L, Larsson P, Rosenblad A, Ving"ard E, St"ahle M.Excessive body weight and smoking associates with a high riskof onset of plaque psoriasis. Acta Derm Venereol 2009;89:492-7.
7. Kumar S, Han J, Li T, Qureshi AA. Obesity, waist circumference,weight change and the risk of psoriasis in US women. J EurAcad Dermatol Venereol 2013;27:1293-8.
8. Murray ML, Bergstresser PR, Adams-Huet B, Cohen JB.Relationship of psoriasis severity to obesity usingsame-gender siblings as controls for obesity. Clin ExpDermatol 2009;34:140-4.
J AM ACAD DERMATOL
VOLUME 71, NUMBER 1Debbaneh et al 139
J Am Acad Dermatol 2014;71:133-40.
• Ladietaipocaloricamiglioralapsoriasidipersé.
• Perdendopesosiaumentalarispostaalleterapie.
• Laperditadipesomiglioral’artritepsoriasica
• L’obesitàsevera(BMI>40)dovrebbeesseretraHataconbypassgastricoinpzselezionaS.

2) Il consumo di alcol peggiora la psoriasi
E. Selenium and vitamin E supplementation for 8 weeks ledto an increase in antioxidant enzyme (glutathione peroxi-dase) levels in patients with psoriasis who showed decreasedglutathione peroxidase levels at the start of the study.34
Neither oral selenium monotherapy, nor selenium andvitamin E dual supplementation in patients with psoriasisand decreased plasma selenium levels resulted in anydiscernible clinical therapeutic benefit.35,36 Triple antioxi-dant therapy with selenium, coenzyme Q, and vitamin E,however, in patients with either erythrodermic psoriasis orsevere psoriatic joint disease, seemed to lessen time toclinical recovery.37
Fish oil
Fish oil has known beneficial effects when used as either amonotherapy or adjuvant therapy for treatment of psoriasisand its comorbidities. Intravenous (IV) formulations ofeicosapentaenoic acid (EPA) and docosahexaenoic acidgiven over 10 to 15 days produced consistent and dramaticimprovements in PASI scores; however, the significant costof IV therapy and inpatient treatment severely limits its useon a wide scale.38,39 Although blinded and controlled trialsof oral fish oil as monotherapy containing either 1.8 or 3 g ofEPA taken daily for 2 to 4 months yielded suboptimal results,revealing no significant changes between treatment andcontrol groups with respect to body surface area involve-ment, PASI score, or a patient subjective score, supplement-ing phototherapy or systemic retinoids with oral fish oil didproduce a greater therapeutic response than either therapyalone.40–44 Several authors also have suggested from theresults of small trials that oral fish oil mitigates retinoid-induced hypertriglyceridemia and cyclosporine-inducednephrotoxicity.45–47 By contrast, use of fish oil as a topicalformulation produced mixed results.48,49
Alcohol
Alcohol consumption can contribute to substantialmorbidity and mortality in patients with psoriasis. Alcoholintake has been associated with an increased risk fordeveloping psoriasis, treatment resistance, and increasedoverall mortality in Finnish patients admitted to the hospitalfor psoriasis.50–53 Objective measures of overconsumptionof alcohol, however, were not definitively linked to greaterpsoriasis severity.54 More studies on the effects of modifiedalcohol intake in psoriasis are needed.
Gluten-free diet
Although no randomized, controlled, prospective trialshave been conducted to provide more conclusive evidencewhether either celiac disease or the presence of autoanti-bodies associated with celiac disease are elevated in patientswith psoriasis, several studies have suggested an associa-
tion.55–58 Investigators have shown that adoption of a gluten-free diet in patients with psoriasis who have elevated anti-gliadin antibodies and/or celiac disease may result inimprovement in psoriasis.59,60 Based on this information, itmay be useful to screen psoriasis patients with bowelsymptoms for autoantibodies so that both the potentialunderlying celiac disease and psoriasis can receive appro-priate treatment.
Vitamin D, vitamin A, inositol, and zinc
Systemic vitamin D complexes with the vitamin Dreceptor, translocates to the nucleus, and binds responsiveDNA elements, ultimately regulating calcium homeostasis,the immune system, and cellular proliferation and differen-tiation.61 The use of high-dose systemic vitamin D, althoughsometimes beneficial in mitigating the clinical severity ofpsoriasis and psoriatic arthritis, is limited by the potential forhypercalcemia and hypercalciuria.62–65 Topical formula-tions, containing vitamin D analogues, however, have beenvery successful in the treatment of psoriasis and carry asignificantly lower risk for systemic side effects. The effectof vitamin D supplementation in patients with psoriasis withvitamin D deficiency is unclear, as randomized, controlledtrials are lacking. A recent case–control study conducted inSpain demonstrated that patients with psoriasis indeed havelower 25-hydroxyvitamin D (25[OH]D) levels than controlsand also are more likely to have 25(OH)D deficiency.66
Given that high-dose vitamin D supplementation to restore25(OH)D levels to normal is generally recommended inpatients with vitamin D deficiency, dermatologists shouldconsider screening at-risk patients and treating themappropriately. The effect on psoriasis and other potentialcomorbidities could be beneficial.
Vitamin A and its analogues also regulate cellularproliferation and differentiation.67 Vitamin A levels arenormal in the majority of patients with psoriasis; however, asubset of psoriatic patients may be at risk for developingvitamin A deficiency, including patients with particularlysevere forms of psoriasis.68–70 Although topical and systemicvitamin A derivatives are established, key elements in thetreatment of psoriasis, the potential deleterious side effects ofexcess systemic vitamin A are well known and limit its use ina variety of populations in dermatology. Interestingly, arecent study found that skin levels of carotenoids (vitamin Aprovitamins and antioxidants) were significantly decreased inpatients with psoriasis compared with controls, but thecarotenoid level showed no correlation with psoriasis severityscores.71 The significance of these findings is unclear and it isnot known whether skin carotenoid levels would aid inpredicting response to treatment with vitamin analogues.
Inositol, a polyhydric alcohol, supplementation in patientswith psoriasis taking lithium was effective in a randomized,blinded, controlled trial, whereas zinc supplementation hadno proven therapeutic benefit in psoriasis unrelated tolithium exposure.72,73
679The role of nutrition in dermatologic diseases
The role of nutrition in dermatologic diseases:Facts and controversiesNikita Lakdawala, MDa, Olubukola Babalola III, MS a, Flavia Fedeles, MDb,Meagen McCusker, MDa, Janelle Ricketts, MD, MBAa, Diane Whitaker-Worth, MDa,Jane M. Grant-Kels, MDa,⁎
aDepartment of Dermatology, University of Conneticut Health Center, Farmington, CT 06032, USAbDepartment of Dermatology, Alpert Medical School Providence, RI 02912, USA
Abstract Many dermatologic diseases are chronic with no definitive cure. For some diseases, theetiology is not completely understood, with treatment being difficult and associated with side effects. Insuch cases, patients may try alternative treatments to prevent onset, reduce symptom severity, or preventreoccurrence of a disease. Dietary modification, through supplementation and exclusion, is an extremelypopular treatment modality for patients with dermatologic conditions. It is, therefore, important fordermatologists to be aware of the growing body of literature pertaining to nutrition and skin disease toappropriately inform patients on benefits and harms of specific dietary interventions. We address therole of nutrition in psoriasis, atopic dermatitis, urticaria, and bullous diseases and specific dietarymodifications as an adjunct or alternative to conventional therapy.© 2013 Elsevier Inc. All rights reserved.
Psoriasis
Psoriasis is a chronic disease of abnormal keratinocyteproliferation and differentiation, as well as localized andsystemic inflammation. The pathogenesis is multifactorial,allowing for multiple therapeutic options, including vitaminA and D derivatives, corticosteroids, ultraviolet lightphototherapy, and immunosuppressive agents. Biologictherapies that target cytokines, including tumor necrosisfactor alpha (TNF-α), interleukin (IL)-12, IL-23, and IL-17,are now of particular importance in the therapeutic ladder.The association of various dietary factors and psoriasis,however, cannot be ignored. In particular, the associationbetween obesity and psoriasis deserves further consideration.The clinical course of psoriasis can be affected by obesity;dietary caloric modifications; and intake of antioxidants, ω-3
polyunsaturated fatty acids (PUFAs), alcohol, vitamin A andvitamin D derivatives, gluten, and inositol.1
Obesity
Investigators are still researching the numerous linksbetween obesity and psoriasis. Patients with psoriasis aremore overweight (body mass index [BMI] ≥ 25 kg/m2) orobese (BMI ≥ 30 kg/m2) than average.2–4 A higher BMI inpsoriasis correlates with the presence of severe (versus mild)disease and is suggested to be a risk factor for psoriasis.3,5 Aprospective study of nurses shows a positive associationbetween elevated waist circumference and BMI at least 35kg/m2 (relative risk [RR], 2.69; 95% confidence interval[CI], 2.12-3.40; P b .001) and risk for incident psoriasis.6
Despite these statistics, a causal relationship betweenobesity and psoriasis has not been clearly defined. Re-searchers have elucidated the roles of various cytokines inboth disease states, but the mechanisms leading to disease
⁎ Corresponding author.E-mail address: [email protected] (J.M. Grant-Kels).
0738-081X/$ – see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.clindermatol.2013.05.004
Clinics in Dermatology (2013) 31, 677–700

3) Una dieta ricca di an;ossidan; (fruBa e verdura fresche) migliora la psoriasi
onset are not completely clear. Obesity and psoriasis sharesome pathogenic cytokines. Visceral adipose tissue containsinflammatory cytokines IL-6, TNF-α, adiponectin, andplasminogen activator inhibitor type 1 (PAI-1), amongothers. TNF-α, in particular, is known to play a key role inthe pathogenesis of psoriasis and is elevated in obesepatients. Patients with psoriasis show higher levels TNF-αand IL-6 in psoriatic skin lesion blister fluid compared withcontrols. These cytokine levels, furthermore, show asignificant correlation with disease severity.7 Also, immu-nohistochemical staining of normal skin and psoriaticplaques show more prominent staining for TNF-α in dermalmacrophages in the papillary dermis in psoriasis affectedskin.8 Circulating serum TNF-α levels are reportedly normalin psoriasis and do not correlate with disease activity;however, the involvement of different inflammatory medi-ators may differ by race/ethnicity. Egyptian patients withpsoriasis were found to have higher serum TNF-α levels thancontrols, and levels were positively associated with psoriasisseverity. TNF-α levels also were reported to correlate withdisease activity in Japanese patients.9 TNF-α also is a markerof inflammation in obese patients, who show significantlyhigher levels of both circulating serum TNF-α and solubleTNF-α receptors when compared with non-obese patients.10
As is well established, anti–TNF-α agents are very popularand effective in the treatment of moderate to severe psoriasis,although other agents, including anti-p40-IL12/23 agentsand anti-IL-17 agents currently are under investigation.
Adipokines are substances that regulate metabolicactivities and are secreted by different cellular componentsof white adipose tissue.11 Increased serum levels of resistin,an adipokine produced by macrophages in adipose tissue, arefound in psoriasis and are associated with more severepsoriasis. Resistin, not surprisingly, increases peripheralblood monocyte production of TNF-α in vitro.12 Although itis unclear whether serum resistin levels are elevated inobesity, resistin mRNA levels are elevated in obesepatients.12 Levels of leptin, a cytokine produced byadipocytes, also are significantly increased in obesity andin psoriasis.13,14 Leptin drives T cells toward the T helper(Th)-1 phenotype, while promoting TNF-α synthesis byperipheral blood monocytes.15–17 In patients with psoriasis,serum leptin also is positively associated with the PsoriasisArea and Severity Index (PASI) score (r = +0.59; P b .001)and BMI (r = +0.532; P b .001).18 Given that obesity andpsoriasis share many cytokines and inflammatory mediators,it is plausible that one disease state may influence thedevelopment and/or the clinical course of the other.
A higher BMI in psoriasis also is predictive of an inferiorresponse to both traditional systemic and biologic thera-pies.19,20 A prospective study of patients on methotrexate,cyclosporine, acitretin, systemic psoralen plus ultravioletlight, as well as efalizumab, etanercept, and infliximab showsthat a BMI of at least 30 kg/m2 may be associated with alower likelihood of achieving a PASI-75 at 16 weeks offollow-up.21
Given that altered body fat composition and an elevatedBMI are associated with a higher risk for psoriasis, moresevere psoriasis, and a mitigated response to systemictreatments, a few studies have explored the effect ofinterventions modifying body weight or calorie intake onthe clinical course of psoriasis. Some studies have shown ashort-term benefit of calorie restriction and a vegan diet inpsoriasis.22,23 A few case reports of obese patients withpsoriasis, furthermore, showed that weight loss after gastricbypass surgery led to an improvement in the condition.24
Calorie restriction also may have an effect on treatmentresponse in patients with an elevated BMI. In patients whoare either overweight or obese at the start of biologic therapy,a low-calorie diet may have helped increase responsivenessto therapy.25 Another study, evaluating the effect of caloricrestriction on response to cyclosporine in obese patients withpsoriasis, found that a calorie-restricted diet, resulting in anaverage 7 kg reduction in body weight, enhanced response totherapy.26
Metabolic syndrome includes insulin resistance, abnor-mal fat distribution, dyslipidemias, and elevated bloodpressure. Its incidence is increased in patients withpsoriasis.27,28 Interventions to improve comorbidities benefitpatients with psoriasis overall and also might result inimprovement in psoriasis, as suggested by controlled trialswith pioglitazone, which increases insulin sensitization inindividuals with diabetes and additionally has been shown toimprove PASI scores in psoriatics.29 Diet is already knownto benefit the components of metabolic syndrome. Does acalorie-restricted, low-fat, low-carbohydrate diet result insimultaneous improvement in psoriasis? One researchersuggested this based on a case report in which a patient withboth metabolic syndrome and psoriasis received 4 months ofrosiglitazone along with a hypoglycemic, hypocholestero-lemic diet. These changes resulted in improvement inpsoriasis (PASI score decreased from 5.6 to 2.1), hemoglo-bin A1c, and hypercholesterolemia.30 A low-protein, low-taurine diet, by contrast, has not been shown consistentlyeffective in the treatment of psoriasis.31
The associations between obesity and psoriasis arenumerous; however, more study on the effects of calorierestriction, weight loss, and the mechanisms of response todifferent treatments in obese patients is needed to moreeffectively counsel patients on diet modification.
Antioxidants
Antioxidants could potentially help in counteracting theoxidative stress that may play a role in the pathogenesis ofpsoriasis.32 Diets rich in fresh fruits, vegetables, and theirantioxidants may help reduce the risk for developing psoriasis.A case–control study linked increased consumption of carrots,tomatoes, and fresh fruit, as assessed by patient questionnaires,with a significantly decreased risk for psoriasis.33
Other antioxidants have been considered in the treatmentof psoriasis, including selenium, coenzyme Q, and vitamin
678 N. Lakdawala et al.
The role of nutrition in dermatologic diseases:Facts and controversiesNikita Lakdawala, MDa, Olubukola Babalola III, MS a, Flavia Fedeles, MDb,Meagen McCusker, MDa, Janelle Ricketts, MD, MBAa, Diane Whitaker-Worth, MDa,Jane M. Grant-Kels, MDa,⁎
aDepartment of Dermatology, University of Conneticut Health Center, Farmington, CT 06032, USAbDepartment of Dermatology, Alpert Medical School Providence, RI 02912, USA
Abstract Many dermatologic diseases are chronic with no definitive cure. For some diseases, theetiology is not completely understood, with treatment being difficult and associated with side effects. Insuch cases, patients may try alternative treatments to prevent onset, reduce symptom severity, or preventreoccurrence of a disease. Dietary modification, through supplementation and exclusion, is an extremelypopular treatment modality for patients with dermatologic conditions. It is, therefore, important fordermatologists to be aware of the growing body of literature pertaining to nutrition and skin disease toappropriately inform patients on benefits and harms of specific dietary interventions. We address therole of nutrition in psoriasis, atopic dermatitis, urticaria, and bullous diseases and specific dietarymodifications as an adjunct or alternative to conventional therapy.© 2013 Elsevier Inc. All rights reserved.
Psoriasis
Psoriasis is a chronic disease of abnormal keratinocyteproliferation and differentiation, as well as localized andsystemic inflammation. The pathogenesis is multifactorial,allowing for multiple therapeutic options, including vitaminA and D derivatives, corticosteroids, ultraviolet lightphototherapy, and immunosuppressive agents. Biologictherapies that target cytokines, including tumor necrosisfactor alpha (TNF-α), interleukin (IL)-12, IL-23, and IL-17,are now of particular importance in the therapeutic ladder.The association of various dietary factors and psoriasis,however, cannot be ignored. In particular, the associationbetween obesity and psoriasis deserves further consideration.The clinical course of psoriasis can be affected by obesity;dietary caloric modifications; and intake of antioxidants, ω-3
polyunsaturated fatty acids (PUFAs), alcohol, vitamin A andvitamin D derivatives, gluten, and inositol.1
Obesity
Investigators are still researching the numerous linksbetween obesity and psoriasis. Patients with psoriasis aremore overweight (body mass index [BMI] ≥ 25 kg/m2) orobese (BMI ≥ 30 kg/m2) than average.2–4 A higher BMI inpsoriasis correlates with the presence of severe (versus mild)disease and is suggested to be a risk factor for psoriasis.3,5 Aprospective study of nurses shows a positive associationbetween elevated waist circumference and BMI at least 35kg/m2 (relative risk [RR], 2.69; 95% confidence interval[CI], 2.12-3.40; P b .001) and risk for incident psoriasis.6
Despite these statistics, a causal relationship betweenobesity and psoriasis has not been clearly defined. Re-searchers have elucidated the roles of various cytokines inboth disease states, but the mechanisms leading to disease
⁎ Corresponding author.E-mail address: [email protected] (J.M. Grant-Kels).
0738-081X/$ – see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.clindermatol.2013.05.004
Clinics in Dermatology (2013) 31, 677–700

Mol; cibi vanno di moda…
Maancorasidiscute!

1) Dieta gluten-free e psoriasi REVIEWS
Diet and psoriasis, part II: Celiac disease and roleof a gluten-free diet
Bhavnit K. Bhatia, BA,a,b Jillian W. Millsop, MD,a,c Maya Debbaneh, BA,a,d John Koo, MD,a
Eleni Linos, MD,a and Wilson Liao, MDa
San Francisco and Irvine, California; Chicago, Illinois; and Salt Lake City, Utah
Please see the September issue for the third part of this series.
Patients with psoriasis have been shown to have a higher prevalence of other autoimmune diseases includingceliac disease, a condition marked by sensitivity to dietary gluten. A number of studies suggest that psoriasisand celiac disease share common genetic and inflammatory pathways. Here we review the epidemiologicassociation between psoriasis and celiac disease and perform a meta-analysis to determine whether patientswith psoriasis more frequently harbor serologic markers of celiac disease. We also examine whether agluten-free diet can improve psoriatic skin disease. ( J Am Acad Dermatol 2014;71:350-8.)
Key words: antigliadin; celiac disease; celiac sprue; diet; gluten-free; nutrition; psoriasis.
P soriasis is a chronic inflammatory diseaseaffecting about 2% of the population andcharacterized by well-demarcated, erythem-
atous, scaly plaques.1 The pathogenesis of psoriasisinvolves the interplay among multiple genesusceptibility loci, the immune system, and variousenvironmental factors. Psoriasis is most commonlyunderstood as a T-cell-mediated disease involvinginterferon-g and tumor necrosis factor-alpha as keyproinflammatory players. More recently, T cellsexpressing cytokine interleukin 17 have been foundto play a major role in psoriasis.2
Patients with psoriasis are more likely to haveautoimmune diseases than the general population.In a recent study conducted by Wu et al3 examiningthe medical records of 25,341 patients with psoriasisfrom the Southern California Kaiser database,psoriasis was found to be significantly associatedwith 14 other autoimmune diseases. The linkbetween psoriasis and other autoimmune diseasesmay result from the shared abnormalities in cytokinepathways4,5 and genetic susceptibility loci.6
The association between psoriasis and celiacdisease has been of recent interest, and a numberof studies have evaluated a possible therapeuticeffect of a gluten-free diet (GFD) on psoriasis.Celiac disease is defined as a disease of the smallintestine characterized by mucosal inflammation,villous atrophy, and crypt hyperplasia uponexposure to dietary gluten, which is mainlycomposed of two groups of proteins called‘‘glutenins’’ and ‘‘gliadins.’’ Serum antibody levelsincluding IgA tissue transglutaminase antibody(tTG), IgA endomysial antibody (EMA), IgA anti-gliadin antibody (AGA), and IgG AGA are mostcommonly used as diagnostic markers for celiac
From the Department of Dermatology, University of California, SanFranciscoa; Rush Medical College, Rush University MedicalCenter, Chicagob; University of Utah School of Medicinec; andUniversity of California, Irvine, School of Medicine.d
Ms Bhatia and Dr Millsop contributed equally to this work.Dr Liao is supported in part by grants from the National Institutes
of Health (R01AR065174, K08AR057763). Dr Linos is supportedby the National Center for Research Resources (KL2RR024130)and Dermatology Foundation.
Disclosure: Dr Koo is a speaker for AbbVie and Leo. Dr Kooconducts research for Amgen, Janssen, Novartis, Photomedex,Galderma, Pfizer, and Merck. Dr Koo has no stocks,
employment, or board memberships with any pharmaceuticalcompany. None of the grants were directly related to thisstudy. Ms Bhatia, Ms Millsop, Ms Debbaneh, Dr Linos, andDr Liao have no conflicts of interest to declare.
Accepted for publication March 4, 2014.Reprint requests: Wilson Liao, MD, Department of Dermatology,
University of California, San Francisco, 515 Spruce St,San Francisco, CA 94118. E-mail: [email protected].
Published online April 28, 2014.0190-9622/$36.00! 2014 by the American Academy of Dermatology, Inc.http://dx.doi.org/10.1016/j.jaad.2014.03.017
Abbreviations used:
AGA: antigliadin antibodyEMA: endomysial antibodyGFD: gluten-free diettTG: tissue transglutaminase antibody
350
versus 5% of healthy control subjects. Moreover, in 2studies there was a positive correlation betweenceliac disease antibody positivity and severity ofpsoriasis or psoriatic arthritis. Interestingly, in thesepatients with psoriasis, elevated celiac diseaseantibodies did not necessarily correspond to abiopsy-confirmed diagnosis of celiac disease,suggesting that psoriasis may be associated withgluten sensitivity (marked by antibody positivity) butnot necessarily gluten enteropathy.
Regarding the benefit of a GFD in patients withpsoriasis, two small clinical trials showed a decreasein serologic markers of celiac disease after GFD andone showed a significant reduction in the PsoriasisArea Severity Index score. Three case reports alsodocumented resolution of psoriasis after GFD.
Based on the available evidence, we recommendthat providers verbally screen their patients withpsoriasis for symptoms of gluten sensitivity such asdiarrhea, flatulence, fatigue, and history of iron-deficiency anemia. Positive symptoms should befollowed up with antibody testing, with IgA EMAor IgA tTG recommended as the most sensitive andspecific tests. In patients with positive antibody tests,a trial of a GFD may be considered.
The pathogenesis of psoriasis and celiac diseasemay involve shared biological mechanisms.Genome-wide association studies of psoriasis andceliac disease have revealed that these two diseasesshare genetic susceptibility loci at 8 genes, includingat TNFAIP3, RUNX3, ELMO1, ZMIZ1, ETS1, SH2B3,SOCS1, andUBE2L3.34-36 These genes regulate innateand adaptive immune responses. Although celiacdisease is associated with autoantibody formationtypical of the Th2 axis, immunologic studies of celiacdisease indicate that Th1 cells,37,38 Th17 cells,39
gamma-delta T cells, and natural killer-like cellsplay an important role in disease pathogenesis.40
Psoriasis has been similarly linked to T helper (Th)1cells, Th17 cells, and gamma-delta T cells.
Additional hypotheses linking psoriasis to celiacdisease include increased intestinal permeabilitypresent in both conditions41,42 and the idea thatpsoriasis in patients with celiac disease can beinduced by vitamin-D deficiency.31,41-46
A pilot study by Skavland et al47 sought todetermine whether wheat antigens could serve asan immunologic trigger in patients with psoriasis.The study exposed peripheral blood mononuclearcells from 37 patients with psoriasis and 37 controlsubjects to various wheat proteins/peptides in vitroand measured proliferation responses. They foundthat the p62-75 peptide induced a significantresponse more frequently in the patients withpsoriasis compared with control subjects (P\ .05).
Several wheat antigens were able to induceexpression of the skin-homing marker cutaneouslymphocyte antigen. The authors concluded thatcertain wheat protein antigens may be important toa subgroup of patients with psoriasis, who couldbenefit from a GFD.47
ConclusionEpidemiologic and clinical studies suggest there is
an association among psoriasis, celiac disease, andceliac disease markers. There is early evidence tosuggest that a GFD may benefit some patients withpsoriasis, but further trials in defined populations areneeded. Still, clinicians may want to question theirpatients with psoriasis about symptoms of celiacdisease including diarrhea, flatulence, fatigue, andhistory of iron-deficiency anemia. Positive symptomsshould prompt clinicians to test for IgA EMA or IgAtTG antibodies, with positive antibody resultssuggesting the potential benefit of a GFD.
REFERENCES1. Elder JT, Bruce AT, Gudjonsson JE, Johnston A, Stuart PE,
Tejasvi T, et al. Molecular dissection of psoriasis: integratinggenetics and biology. J Invest Dermatol 2010;130:1213-26.
2. Lowes MA, Kikuchi T, Fuentes-Duculan J, Cardinale I, Zaba LC,Haider AS, et al. Psoriasis vulgaris lesions contain discretepopulations of Th1 and Th17 T cells. J Invest Dermatol 2008;128:1207-11.
3. Wu JJ, Nguyen TU, Poon KY, Herrinton LJ. The association ofpsoriasis with autoimmune diseases. J Am Acad Dermatol2012;67:924-30.
4. Makredes M, Robinson D, Bala M, Kimball AB. The burden ofautoimmune disease: a comparison of prevalence ratios inpatients with psoriatic arthritis and psoriasis. J Am AcadDermatol 2009;61:405-10.
5. Davidson A, Diamond B. Autoimmune diseases. N Engl J Med2001;345:340-50.
6. Cotsapas C, Voight BF, Rossin E, Lage K, Neale BM, Wallace C,et al. Pervasive sharing of genetic effects in autoimmunedisease. PLoS Genet 2011;7:e1002254.
7. Grodzinsky E, Hed J, Skogh T. IgA antiendomysium antibodieshave a high positive predictive value for celiac disease inasymptomatic patients. Allergy 1994;49:593-7.
8. Kelly CP, Feighery CF, Gallagher RB, Gibney MJ, Weir DG.Mucosal and systemic IgA anti-gliadin antibody in celiacdisease: contrasting patterns of response in serum, saliva,and intestinal secretions. Dig Dis Sci 1991;36:743-51.
9. Hopper AD, Hadjivassiliou M, Hurlstone DP, Lobo AJ,McAlindon ME, Egner W, et al. What is the role of serologictesting in celiac disease? A prospective, biopsy-confirmedstudy with economic analysis. Clin Gastroenterol Hepatol2008;6:314-20.
10. Rostom A, Dube C, Cranney A, Saloojee N, Sy R, Garritty C, et al.The diagnostic accuracy of serologic tests for celiac disease: asystematic review. Gastroenterology 2005;128:S38-46.
11. Birkenfeld S, Dreiher J, Weitzman D, Cohen AD. Celiac diseaseassociated with psoriasis. Br J Dermatol 2009;161:1331-4.
12. Ludvigsson JF, Lindel€of B, Zingone F, Ciacci C. Psoriasis in anationwide cohort study of patients with celiac disease.J Invest Dermatol 2011;131:2010-6.
J AM ACAD DERMATOL
VOLUME 71, NUMBER 2Bhatia et al 357
REVIEWS
Diet and psoriasis, part II: Celiac disease and roleof a gluten-free diet
Bhavnit K. Bhatia, BA,a,b Jillian W. Millsop, MD,a,c Maya Debbaneh, BA,a,d John Koo, MD,a
Eleni Linos, MD,a and Wilson Liao, MDa
San Francisco and Irvine, California; Chicago, Illinois; and Salt Lake City, Utah
Please see the September issue for the third part of this series.
Patients with psoriasis have been shown to have a higher prevalence of other autoimmune diseases includingceliac disease, a condition marked by sensitivity to dietary gluten. A number of studies suggest that psoriasisand celiac disease share common genetic and inflammatory pathways. Here we review the epidemiologicassociation between psoriasis and celiac disease and perform a meta-analysis to determine whether patientswith psoriasis more frequently harbor serologic markers of celiac disease. We also examine whether agluten-free diet can improve psoriatic skin disease. ( J Am Acad Dermatol 2014;71:350-8.)
Key words: antigliadin; celiac disease; celiac sprue; diet; gluten-free; nutrition; psoriasis.
P soriasis is a chronic inflammatory diseaseaffecting about 2% of the population andcharacterized by well-demarcated, erythem-
atous, scaly plaques.1 The pathogenesis of psoriasisinvolves the interplay among multiple genesusceptibility loci, the immune system, and variousenvironmental factors. Psoriasis is most commonlyunderstood as a T-cell-mediated disease involvinginterferon-g and tumor necrosis factor-alpha as keyproinflammatory players. More recently, T cellsexpressing cytokine interleukin 17 have been foundto play a major role in psoriasis.2
Patients with psoriasis are more likely to haveautoimmune diseases than the general population.In a recent study conducted by Wu et al3 examiningthe medical records of 25,341 patients with psoriasisfrom the Southern California Kaiser database,psoriasis was found to be significantly associatedwith 14 other autoimmune diseases. The linkbetween psoriasis and other autoimmune diseasesmay result from the shared abnormalities in cytokinepathways4,5 and genetic susceptibility loci.6
The association between psoriasis and celiacdisease has been of recent interest, and a numberof studies have evaluated a possible therapeuticeffect of a gluten-free diet (GFD) on psoriasis.Celiac disease is defined as a disease of the smallintestine characterized by mucosal inflammation,villous atrophy, and crypt hyperplasia uponexposure to dietary gluten, which is mainlycomposed of two groups of proteins called‘‘glutenins’’ and ‘‘gliadins.’’ Serum antibody levelsincluding IgA tissue transglutaminase antibody(tTG), IgA endomysial antibody (EMA), IgA anti-gliadin antibody (AGA), and IgG AGA are mostcommonly used as diagnostic markers for celiac
From the Department of Dermatology, University of California, SanFranciscoa; Rush Medical College, Rush University MedicalCenter, Chicagob; University of Utah School of Medicinec; andUniversity of California, Irvine, School of Medicine.d
Ms Bhatia and Dr Millsop contributed equally to this work.Dr Liao is supported in part by grants from the National Institutes
of Health (R01AR065174, K08AR057763). Dr Linos is supportedby the National Center for Research Resources (KL2RR024130)and Dermatology Foundation.
Disclosure: Dr Koo is a speaker for AbbVie and Leo. Dr Kooconducts research for Amgen, Janssen, Novartis, Photomedex,Galderma, Pfizer, and Merck. Dr Koo has no stocks,
employment, or board memberships with any pharmaceuticalcompany. None of the grants were directly related to thisstudy. Ms Bhatia, Ms Millsop, Ms Debbaneh, Dr Linos, andDr Liao have no conflicts of interest to declare.
Accepted for publication March 4, 2014.Reprint requests: Wilson Liao, MD, Department of Dermatology,
University of California, San Francisco, 515 Spruce St,San Francisco, CA 94118. E-mail: [email protected].
Published online April 28, 2014.0190-9622/$36.00! 2014 by the American Academy of Dermatology, Inc.http://dx.doi.org/10.1016/j.jaad.2014.03.017
Abbreviations used:
AGA: antigliadin antibodyEMA: endomysial antibodyGFD: gluten-free diettTG: tissue transglutaminase antibody
350

Ma aBenzione…
• NonvuoldirecheglipsoriasicidebbanomangiaresenzagluSne!• SembrasolocheipazienSconlapsoriasiabbianounamaggiorepredisposizioneasvilupparelaceliachia,cosìcomehannounamaggioretendenzaasvilupparealtremalaUeautoimmuni(es.artritereumatoide,sindromediSjorgen,malaUeinfiammatoriecronicheintesSnali)
• Percui,incasodisintomiintesSnali(flatulenza,alterazionidell’alvo,doloriaddominali)ènecessarioconsultareilmedicoedeventualmente,sepersistono,effeHuareesamiadeguaS.

2) Vitamina D e psoriasi
• SembracheildeficitdivitaminaDsiaassociatoallapsoriasi.• AlcunistudirandomizzaSecontrollaS,tuHavia,nonhannoconfermatochelasupplementazionedivitaminaDmiglioridavverolapsoriasi.
• Inoltre,laassunzionedivitaminaDsenzaunaveraepropriacarenza,puòdeterminarenellungoperiodoipocalcemia,ipercalciuria,calcolirenaliedemineralizzazioneossea.
• RicordiamochelavitaminaD(adifferenzadialtrevitaminecomelaColevitaminedelgruppoB)seineccessoNONvieneescretaconleurinemasiaccumulanell’organismo! REVIEWS
Diet and psoriasis, part III: Roleof nutritional supplements
Jillian W. Millsop, MD,a,b Bhavnit K. Bhatia, BA,a,c Maya Debbaneh, BA,a,d
John Koo, MD,a and Wilson Liao, MDa
San Francisco and Irvine, California; Chicago, Illinois; and Salt Lake City, Utah
Patients with psoriasis are increasingly turning to the use of alternative and complementary medicineto manage their psoriasis. Patients often inquire about what dietary supplements may be beneficial,including the use of oral vitamin D, vitamin B12, selenium, and omega-3 fatty acids in fish oils. Inthis review we examine the extent to which each of these common nutritional interventions has beenstudied for the treatment of psoriasis. We weighed evidence from both controlled and uncontrolledprospective trials. The evidence of benefit was highest for fish oils. For other supplements, there is needfor additional large, randomized clinical trials to establish evidence of efficacy. ( J Am Acad Dermatol2014;71:561-9.)
Key words: diet; fish oil; nutrition; omega-3; oral vitamin D; psoriasis; selenium; vitamin B12;1,25-dihydroxycholecalciferol; 1,25-dihydroxyvitamin D3; 1,25-(OH)2D3.
T he use of alternative and complementarymedicine has soared in popularity withpatients, not just for improvement of baseline
health, but even in the management of chronicconditions such as psoriasis.1,2 There is a growingbody of popular and scientific literature for the use ofnutritional supplementation in the treatment ofpsoriasis. With this information readily available,patients often perform independent research andask their dermatologists about what they can add totheir diets to make their conditionmoremanageable.Here we sought to explore some of the mostcommon nutritional supplements and explore towhat extent the scientific literature has evaluatedtheir respective clinical efficacies. We review studiesthat have examined oral vitamin D, vitamin B12,selenium, and omega-3 fatty acids.
METHODSWe performed our literature search in June 2013
using the electronic MEDLINE database via PubMed.Search terms included ‘‘psoriasis’’ combined with
‘‘oral vitamin D,’’ ‘‘1,25-(OH)2D3,’’ ‘‘1,25-dihydroxyvitamin D3,’’ ‘‘1,25-dihydroxycholecalciferol,’’ ‘‘fishoil,’’ ‘‘omega,’’ ‘‘B12,’’ ‘‘vitamin B,’’ and ‘‘selenium,’’respectively. In addition, abstracts containing thekey words ‘‘alternative therapies’’ and ‘‘nonstandardtreatment’’ were reviewed. We limited our search toarticles available in English and those publishedbetween 1960 and 2013. Manual searches ofbibliographies of the articles were also performedto identify additional studies to be included.Exclusion criteria included topical regimens andstudies that did not specify supplement dosage.The primary outcome evaluated was a statisticallysignificant reduction in Psoriasis Area and Severity
From the Department of Dermatology, University of California, SanFranciscoa; University of Utah School of Medicineb; RushMedical College, Rush University Medical Center, Chicagoc;and University of California, Irvine, School of Medicine.d
Dr Millsop and Ms Bhatia contributed equally to this work.Dr Liao is supported in part by grants from the National Institutes
of Health (R01AR065174, K08AR057763).Disclosure: Dr Koo is a speaker for AbbVie and Leo. Dr Koo
conducts research for Amgen, Janssen, Novartis, Photomedex,Galderma, Pfizer, and Merck. Dr Koo has no stocks, employ-ment, or board memberships with any pharmaceutical
company. None of the grants were directly related to thisstudy. Dr Millsop, Ms Bhatia, Ms Debbaneh, and Dr Liao have noconflicts of interest to declare.
Accepted for publication March 7, 2014.Reprint requests: Wilson Liao, MD, Department of Dermatology,
University of California, San Francisco, 515 Spruce St,San Francisco, CA 94118. E-mail: [email protected].
Published online April 28, 2014.0190-9622/$36.00! 2014 by the American Academy of Dermatology, Inc.http://dx.doi.org/10.1016/j.jaad.2014.03.016
Abbreviations used:
DHA: docosahexaenoic acidEPA: eicosapentaenoic acidPASI: Psoriasis Area Severity IndexUV: ultraviolet
561

3) Vitamina B12 e psoriasi
• Ancheinquestocaso,sebbenelacarenzadivitaminaB12siaassociataallapsoriasi,nonsembrachelasomministrazioneintramuscolareditalevitaminasiaassociataadunmigliroamentoclinicodellapsoriasi.
• TuHavia,almenoinquestocaso,l’eventualeassunzionedivitaminaB12nonpresentaeffeUcollaterali,datochel’eccessovieneescretoconleurine.
• PuòessereuSleunasupplementazioneinparScolareinqueipazienScheseguonounadietavegetariana,inquantoessaèprevalentementecontenutanellacarneoneiderivaS. REVIEWS
Diet and psoriasis, part III: Roleof nutritional supplements
Jillian W. Millsop, MD,a,b Bhavnit K. Bhatia, BA,a,c Maya Debbaneh, BA,a,d
John Koo, MD,a and Wilson Liao, MDa
San Francisco and Irvine, California; Chicago, Illinois; and Salt Lake City, Utah
Patients with psoriasis are increasingly turning to the use of alternative and complementary medicineto manage their psoriasis. Patients often inquire about what dietary supplements may be beneficial,including the use of oral vitamin D, vitamin B12, selenium, and omega-3 fatty acids in fish oils. Inthis review we examine the extent to which each of these common nutritional interventions has beenstudied for the treatment of psoriasis. We weighed evidence from both controlled and uncontrolledprospective trials. The evidence of benefit was highest for fish oils. For other supplements, there is needfor additional large, randomized clinical trials to establish evidence of efficacy. ( J Am Acad Dermatol2014;71:561-9.)
Key words: diet; fish oil; nutrition; omega-3; oral vitamin D; psoriasis; selenium; vitamin B12;1,25-dihydroxycholecalciferol; 1,25-dihydroxyvitamin D3; 1,25-(OH)2D3.
T he use of alternative and complementarymedicine has soared in popularity withpatients, not just for improvement of baseline
health, but even in the management of chronicconditions such as psoriasis.1,2 There is a growingbody of popular and scientific literature for the use ofnutritional supplementation in the treatment ofpsoriasis. With this information readily available,patients often perform independent research andask their dermatologists about what they can add totheir diets to make their conditionmoremanageable.Here we sought to explore some of the mostcommon nutritional supplements and explore towhat extent the scientific literature has evaluatedtheir respective clinical efficacies. We review studiesthat have examined oral vitamin D, vitamin B12,selenium, and omega-3 fatty acids.
METHODSWe performed our literature search in June 2013
using the electronic MEDLINE database via PubMed.Search terms included ‘‘psoriasis’’ combined with
‘‘oral vitamin D,’’ ‘‘1,25-(OH)2D3,’’ ‘‘1,25-dihydroxyvitamin D3,’’ ‘‘1,25-dihydroxycholecalciferol,’’ ‘‘fishoil,’’ ‘‘omega,’’ ‘‘B12,’’ ‘‘vitamin B,’’ and ‘‘selenium,’’respectively. In addition, abstracts containing thekey words ‘‘alternative therapies’’ and ‘‘nonstandardtreatment’’ were reviewed. We limited our search toarticles available in English and those publishedbetween 1960 and 2013. Manual searches ofbibliographies of the articles were also performedto identify additional studies to be included.Exclusion criteria included topical regimens andstudies that did not specify supplement dosage.The primary outcome evaluated was a statisticallysignificant reduction in Psoriasis Area and Severity
From the Department of Dermatology, University of California, SanFranciscoa; University of Utah School of Medicineb; RushMedical College, Rush University Medical Center, Chicagoc;and University of California, Irvine, School of Medicine.d
Dr Millsop and Ms Bhatia contributed equally to this work.Dr Liao is supported in part by grants from the National Institutes
of Health (R01AR065174, K08AR057763).Disclosure: Dr Koo is a speaker for AbbVie and Leo. Dr Koo
conducts research for Amgen, Janssen, Novartis, Photomedex,Galderma, Pfizer, and Merck. Dr Koo has no stocks, employ-ment, or board memberships with any pharmaceutical
company. None of the grants were directly related to thisstudy. Dr Millsop, Ms Bhatia, Ms Debbaneh, and Dr Liao have noconflicts of interest to declare.
Accepted for publication March 7, 2014.Reprint requests: Wilson Liao, MD, Department of Dermatology,
University of California, San Francisco, 515 Spruce St,San Francisco, CA 94118. E-mail: [email protected].
Published online April 28, 2014.0190-9622/$36.00! 2014 by the American Academy of Dermatology, Inc.http://dx.doi.org/10.1016/j.jaad.2014.03.016
Abbreviations used:
DHA: docosahexaenoic acidEPA: eicosapentaenoic acidPASI: Psoriasis Area Severity IndexUV: ultraviolet
561

4) Selenio e psoriasi
• IlseleniohaproprietàimmunoregolatorieedanSproliferaSve.• Lasuacarenzapareessereassociataadunamaggioreseveritàdellapsoriasi.
• Alcunistudihannodimostratochelasomministrazionediselenio,coenzimaQ10evitaminaEmiglioranoirisultaSdelleterapieperlapsoriasi,altriancorainvecenonevidenzianonessunmiglioramentoinseguitoall’assunzionediquestesostanze.
• GlieffeUavversidellasomministrazionediselenioalungotermineincludononausea,vomito,irritabilitàeperditadicapelli(similiall’intossicazionedaarsenico).
The role of nutrition in dermatologic diseases:Facts and controversiesNikita Lakdawala, MDa, Olubukola Babalola III, MS a, Flavia Fedeles, MDb,Meagen McCusker, MDa, Janelle Ricketts, MD, MBAa, Diane Whitaker-Worth, MDa,Jane M. Grant-Kels, MDa,⁎
aDepartment of Dermatology, University of Conneticut Health Center, Farmington, CT 06032, USAbDepartment of Dermatology, Alpert Medical School Providence, RI 02912, USA
Abstract Many dermatologic diseases are chronic with no definitive cure. For some diseases, theetiology is not completely understood, with treatment being difficult and associated with side effects. Insuch cases, patients may try alternative treatments to prevent onset, reduce symptom severity, or preventreoccurrence of a disease. Dietary modification, through supplementation and exclusion, is an extremelypopular treatment modality for patients with dermatologic conditions. It is, therefore, important fordermatologists to be aware of the growing body of literature pertaining to nutrition and skin disease toappropriately inform patients on benefits and harms of specific dietary interventions. We address therole of nutrition in psoriasis, atopic dermatitis, urticaria, and bullous diseases and specific dietarymodifications as an adjunct or alternative to conventional therapy.© 2013 Elsevier Inc. All rights reserved.
Psoriasis
Psoriasis is a chronic disease of abnormal keratinocyteproliferation and differentiation, as well as localized andsystemic inflammation. The pathogenesis is multifactorial,allowing for multiple therapeutic options, including vitaminA and D derivatives, corticosteroids, ultraviolet lightphototherapy, and immunosuppressive agents. Biologictherapies that target cytokines, including tumor necrosisfactor alpha (TNF-α), interleukin (IL)-12, IL-23, and IL-17,are now of particular importance in the therapeutic ladder.The association of various dietary factors and psoriasis,however, cannot be ignored. In particular, the associationbetween obesity and psoriasis deserves further consideration.The clinical course of psoriasis can be affected by obesity;dietary caloric modifications; and intake of antioxidants, ω-3
polyunsaturated fatty acids (PUFAs), alcohol, vitamin A andvitamin D derivatives, gluten, and inositol.1
Obesity
Investigators are still researching the numerous linksbetween obesity and psoriasis. Patients with psoriasis aremore overweight (body mass index [BMI] ≥ 25 kg/m2) orobese (BMI ≥ 30 kg/m2) than average.2–4 A higher BMI inpsoriasis correlates with the presence of severe (versus mild)disease and is suggested to be a risk factor for psoriasis.3,5 Aprospective study of nurses shows a positive associationbetween elevated waist circumference and BMI at least 35kg/m2 (relative risk [RR], 2.69; 95% confidence interval[CI], 2.12-3.40; P b .001) and risk for incident psoriasis.6
Despite these statistics, a causal relationship betweenobesity and psoriasis has not been clearly defined. Re-searchers have elucidated the roles of various cytokines inboth disease states, but the mechanisms leading to disease
⁎ Corresponding author.E-mail address: [email protected] (J.M. Grant-Kels).
0738-081X/$ – see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.clindermatol.2013.05.004
Clinics in Dermatology (2013) 31, 677–700

5) Vitamina A e psoriasi
• L’uSlizzodeiderivaSdellavitaminaA(reSnoidi)nellapsoriasièampiamentedimostratoedèallabasedeltraHamentoditalepatologia.
• LavitaminaAeisuoiderivaShannoeffeUsulladifferenziazioneesullaproliferazionecellulare.
• AlcunistudievidenzianolacarenzadivitaminaAneipzconpsoriasi,tuHavianessunodiessihadimostratounrealebeneficiodell’assunzionedisupplemenSdivitaminaAnellemanifestazioniclinichedellapsoriasi.
The role of nutrition in dermatologic diseases:Facts and controversiesNikita Lakdawala, MDa, Olubukola Babalola III, MS a, Flavia Fedeles, MDb,Meagen McCusker, MDa, Janelle Ricketts, MD, MBAa, Diane Whitaker-Worth, MDa,Jane M. Grant-Kels, MDa,⁎
aDepartment of Dermatology, University of Conneticut Health Center, Farmington, CT 06032, USAbDepartment of Dermatology, Alpert Medical School Providence, RI 02912, USA
Abstract Many dermatologic diseases are chronic with no definitive cure. For some diseases, theetiology is not completely understood, with treatment being difficult and associated with side effects. Insuch cases, patients may try alternative treatments to prevent onset, reduce symptom severity, or preventreoccurrence of a disease. Dietary modification, through supplementation and exclusion, is an extremelypopular treatment modality for patients with dermatologic conditions. It is, therefore, important fordermatologists to be aware of the growing body of literature pertaining to nutrition and skin disease toappropriately inform patients on benefits and harms of specific dietary interventions. We address therole of nutrition in psoriasis, atopic dermatitis, urticaria, and bullous diseases and specific dietarymodifications as an adjunct or alternative to conventional therapy.© 2013 Elsevier Inc. All rights reserved.
Psoriasis
Psoriasis is a chronic disease of abnormal keratinocyteproliferation and differentiation, as well as localized andsystemic inflammation. The pathogenesis is multifactorial,allowing for multiple therapeutic options, including vitaminA and D derivatives, corticosteroids, ultraviolet lightphototherapy, and immunosuppressive agents. Biologictherapies that target cytokines, including tumor necrosisfactor alpha (TNF-α), interleukin (IL)-12, IL-23, and IL-17,are now of particular importance in the therapeutic ladder.The association of various dietary factors and psoriasis,however, cannot be ignored. In particular, the associationbetween obesity and psoriasis deserves further consideration.The clinical course of psoriasis can be affected by obesity;dietary caloric modifications; and intake of antioxidants, ω-3
polyunsaturated fatty acids (PUFAs), alcohol, vitamin A andvitamin D derivatives, gluten, and inositol.1
Obesity
Investigators are still researching the numerous linksbetween obesity and psoriasis. Patients with psoriasis aremore overweight (body mass index [BMI] ≥ 25 kg/m2) orobese (BMI ≥ 30 kg/m2) than average.2–4 A higher BMI inpsoriasis correlates with the presence of severe (versus mild)disease and is suggested to be a risk factor for psoriasis.3,5 Aprospective study of nurses shows a positive associationbetween elevated waist circumference and BMI at least 35kg/m2 (relative risk [RR], 2.69; 95% confidence interval[CI], 2.12-3.40; P b .001) and risk for incident psoriasis.6
Despite these statistics, a causal relationship betweenobesity and psoriasis has not been clearly defined. Re-searchers have elucidated the roles of various cytokines inboth disease states, but the mechanisms leading to disease
⁎ Corresponding author.E-mail address: [email protected] (J.M. Grant-Kels).
0738-081X/$ – see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.clindermatol.2013.05.004
Clinics in Dermatology (2013) 31, 677–700

6) Olio di pesce (acido eicosapentenoico)
• DituHelesupplementazionifinoraviste,quelladell’oliodipesceappareesserelapiùpromeHente.
• L’assunzioneelevatadioliodipesceediacidigrassiomega3appareineffeUesserecorrelataconunmiglioramentodellelesionipsoriasiche,sebbeneancoraalcunidaSsianoincorsodivalidazione.
• Inoltre,propriol’elevataassunzionenelladietaditalisostanze,sembrerebbeesserelacausadellabassapercentualedipsoriasinellepopolazionidell’AfricaoccidentalecosìcomenellepopolazioniEschimesi.
• L’oliodipesce,infine,migliorerebbeancheglieffeUcollateralidialcunifarmaciuSlizzaSneltraHamentodellapsoriasi,comel’ipertrigliceridemiaindoHadaireSnoidielanefrotossicitàdaciclosporina. REVIEWS
Diet and psoriasis, part III: Roleof nutritional supplements
Jillian W. Millsop, MD,a,b Bhavnit K. Bhatia, BA,a,c Maya Debbaneh, BA,a,d
John Koo, MD,a and Wilson Liao, MDa
San Francisco and Irvine, California; Chicago, Illinois; and Salt Lake City, Utah
Patients with psoriasis are increasingly turning to the use of alternative and complementary medicineto manage their psoriasis. Patients often inquire about what dietary supplements may be beneficial,including the use of oral vitamin D, vitamin B12, selenium, and omega-3 fatty acids in fish oils. Inthis review we examine the extent to which each of these common nutritional interventions has beenstudied for the treatment of psoriasis. We weighed evidence from both controlled and uncontrolledprospective trials. The evidence of benefit was highest for fish oils. For other supplements, there is needfor additional large, randomized clinical trials to establish evidence of efficacy. ( J Am Acad Dermatol2014;71:561-9.)
Key words: diet; fish oil; nutrition; omega-3; oral vitamin D; psoriasis; selenium; vitamin B12;1,25-dihydroxycholecalciferol; 1,25-dihydroxyvitamin D3; 1,25-(OH)2D3.
T he use of alternative and complementarymedicine has soared in popularity withpatients, not just for improvement of baseline
health, but even in the management of chronicconditions such as psoriasis.1,2 There is a growingbody of popular and scientific literature for the use ofnutritional supplementation in the treatment ofpsoriasis. With this information readily available,patients often perform independent research andask their dermatologists about what they can add totheir diets to make their conditionmoremanageable.Here we sought to explore some of the mostcommon nutritional supplements and explore towhat extent the scientific literature has evaluatedtheir respective clinical efficacies. We review studiesthat have examined oral vitamin D, vitamin B12,selenium, and omega-3 fatty acids.
METHODSWe performed our literature search in June 2013
using the electronic MEDLINE database via PubMed.Search terms included ‘‘psoriasis’’ combined with
‘‘oral vitamin D,’’ ‘‘1,25-(OH)2D3,’’ ‘‘1,25-dihydroxyvitamin D3,’’ ‘‘1,25-dihydroxycholecalciferol,’’ ‘‘fishoil,’’ ‘‘omega,’’ ‘‘B12,’’ ‘‘vitamin B,’’ and ‘‘selenium,’’respectively. In addition, abstracts containing thekey words ‘‘alternative therapies’’ and ‘‘nonstandardtreatment’’ were reviewed. We limited our search toarticles available in English and those publishedbetween 1960 and 2013. Manual searches ofbibliographies of the articles were also performedto identify additional studies to be included.Exclusion criteria included topical regimens andstudies that did not specify supplement dosage.The primary outcome evaluated was a statisticallysignificant reduction in Psoriasis Area and Severity
From the Department of Dermatology, University of California, SanFranciscoa; University of Utah School of Medicineb; RushMedical College, Rush University Medical Center, Chicagoc;and University of California, Irvine, School of Medicine.d
Dr Millsop and Ms Bhatia contributed equally to this work.Dr Liao is supported in part by grants from the National Institutes
of Health (R01AR065174, K08AR057763).Disclosure: Dr Koo is a speaker for AbbVie and Leo. Dr Koo
conducts research for Amgen, Janssen, Novartis, Photomedex,Galderma, Pfizer, and Merck. Dr Koo has no stocks, employ-ment, or board memberships with any pharmaceutical
company. None of the grants were directly related to thisstudy. Dr Millsop, Ms Bhatia, Ms Debbaneh, and Dr Liao have noconflicts of interest to declare.
Accepted for publication March 7, 2014.Reprint requests: Wilson Liao, MD, Department of Dermatology,
University of California, San Francisco, 515 Spruce St,San Francisco, CA 94118. E-mail: [email protected].
Published online April 28, 2014.0190-9622/$36.00! 2014 by the American Academy of Dermatology, Inc.http://dx.doi.org/10.1016/j.jaad.2014.03.016
Abbreviations used:
DHA: docosahexaenoic acidEPA: eicosapentaenoic acidPASI: Psoriasis Area Severity IndexUV: ultraviolet
561

Le nuove fron;ere: il microbiota intes;nale
ILMICROBIOTAINTESTINALE• 1,5kgdibaHeri
presenSall’internodelnostroapparatodigerente...ilpesodiunorgano(ilfegato,peresempio)
• 10volteilnumerodellecelluledituHoilcorpo
• 3,3ovvero150volteilgenomaumano

• BaHeribuoniecaUvi:TuHoèparStodaunmanualedivulgaSvoamericano”THESKINNYGUTDIET”:
• BrendaWatsonpropone14menuricchidicibochecontenganoProbioSciePrebioScicheriduconol’assorbimento,modulandol’apportocalorico Associazione
Internazionale di dermatologia
ecologica
Batteri buoni e cattivi :
Tutto è partito da un manuale divulgativo americano ”THE SKINNY GUT DIET”
Brenda Watson propone 14 menu ricchi di cibo che contengano Probiotici e Prebiotici che riducono l’assorbimento, modulando l’apporto calorico
LoBe…intes;ne
• L’aumentodipesoquandosismeHedifumare,peresempio,sembrerebbedipenderedall’aumentodeibaHeriPHYLUMFIRMICUTES(quellipiuefficienSnell’assimilazionedeicibi)edalladiminuzionedeiPHYLUMBACTERIOIDI.
• EquestacomposizionebaHericacaraHerizzailMicrobiotadegliobesi
• InteoriasipotrebbemodularelaflorabaHericainterminiqualitaSviequanStaSvi:Intervenenedoadesempiosull’AKKERMANSIAMUCINIPHILAcheinfluenzailmetabolismoosulFECALIBACTERIUMPRAUSNITZIIchesembrafacilitareifenomeniinfiammatori
Associazione Internazionale
di dermatologia ecologica
LE NUOVE FRONTIERE ModularelaflorabaCericainterminiqualitaXviequanXtaXvi:Interveniresull’AKKERMANSIAMUCINIPHILAcheinfluenzailmetabolismo,
osulFECALIBACTERIUMPRAUSNITZIIchesembrafacilitareifenomeniinfiammatori
Associazione Internazionale
di dermatologia ecologica
LE NUOVE FRONTIERE ModularelaflorabaCericainterminiqualitaXviequanXtaXvi:Interveniresull’AKKERMANSIAMUCINIPHILAcheinfluenzailmetabolismo,
osulFECALIBACTERIUMPRAUSNITZIIchesembrafacilitareifenomeniinfiammatori

Vedremo cosa ci riserverà il futuro…

Concludendo… • Ladietadiognunodinoi,psoriasicoono,deveessereilpiùpossibilevariaedaUnenteallapiramidedelladietamediterranea!

• Diffidaredellediete“fai-da-te”o“dimoda”edegliintegratori“dabanco”!
• La perdita di peso, con una dieta bilanciata ed un’adeguata aIvità fisica, fa bene alla psoriasi!

Esempio di dieta bilanciata
RiparSzionenutrienS:• 55%dicarboidraS,• 15%diproteine,
• 30%dilipidi.

Carboidra; da preferire
ALIMENTIABASSOINDICEGLICEMICO•PASTADIGRANODUROITALIANA-PASTAEPANEINTEGRALE•RISOINTEGRALE•ORZO,FARRO,KAMUT,MIGLIO,AVENA•LEGUMI(lenScchie,ceci,fagioli,piselli,soia)•VERDUREAFOGLIAEDARADICE(distagione,3porzionialgiornovariamentecolorate)•FRUTTA(distagione,2porzionialgiornovariamentecolorate)

Lipidi da preferire
•OLIOEXTRAVERGINEDIOLIVA(2cucchiaialgiorno,crudo)•FRUTTASECCAAGUSCIO(2noci,o3mandorle,o3nocciolefonXdivitaminaEegrassipolinsaturi)•SEMIOLEAGINOSI(sesamo,girasole,semidizucca,semidilinofornisconoOmega3,cheriduconol’infiammazione)

Proteine da preferire
•PESCE(favorisceunbuonfunzionamentodell’insulina,fornisceOmega3,cheriduconol’infiammazione)•CARNIBIANCHE(nonsuperarei400gaseUmana)•LEGUMI•UOVA(2-4aseUmana)•LATTEEYOGURTSCREMATO

• La psoriasi NON è causata dall’alimentazione!!! (e nemmeno dallo stress)
CaraDelevingne,modella

Anche se la caIva alimentazione la può PEGGIORARE!

Invito a cena con…psoriasico!





























